Stability of Oral Liquid Dosage Forms in Pediatric Cardiology: A Prerequisite for Patient’s Safety—A Narrative Review



Abstract
:1. Introduction
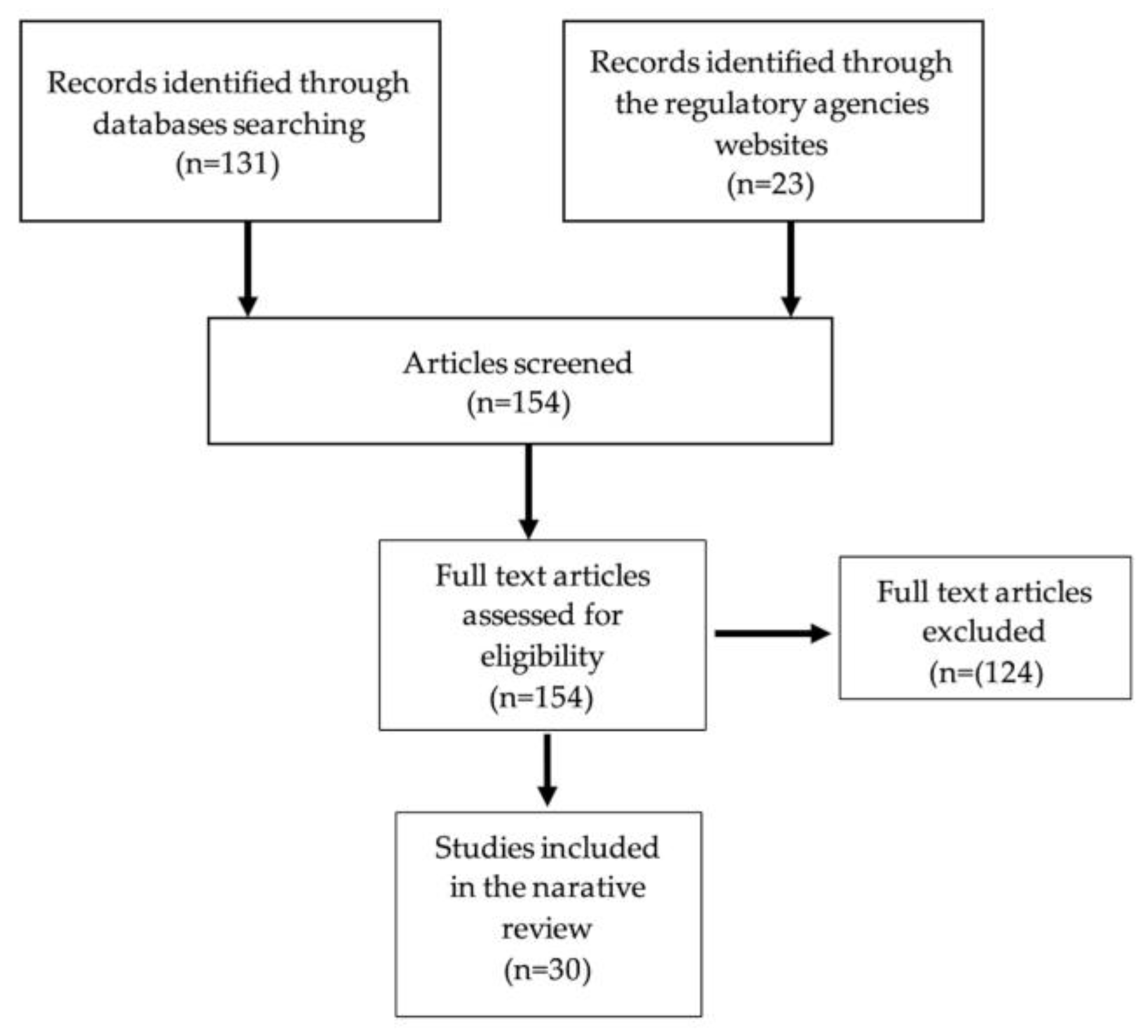
2. Materials and Methods
3. Results
3.1. Approved Medicines for Pediatric Use
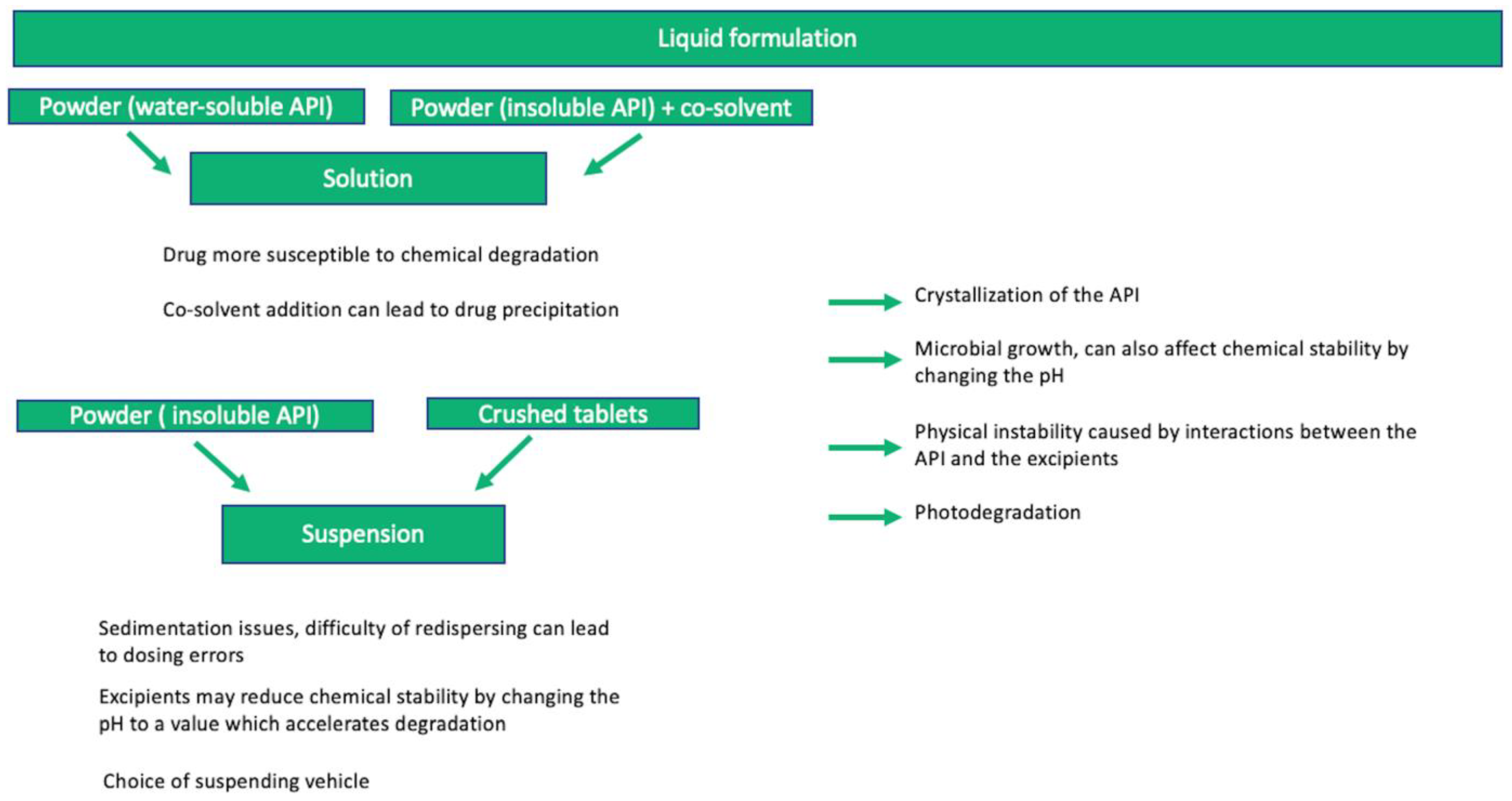
3.2. General Considerations on Compounding and Stability of Liquid Oral Dosage Forms for Substances Used in Pediatric Cardiology
3.3. Stability-Indicating Parameters and Guidelines
- formation of precipitate, clarity (for solutions), pH, viscosity, extractables, and level of microbial contamination;
- additionally for suspensions, dispersibility, rheological properties, mean size, and distribution of particles should be considered. In addition, polymorphic conversion may be examined, if applicable [71].
3.4. Stability Study Design
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lenk, C.; Duttge, G. Ethical and legal framework and regulation for off-label use: European perspective. Ther. Clin. Risk Manag. 2014, 10, 537–546. [Google Scholar] [CrossRef]
- Balan, S.; Hassali, M.A.A.; Mak, V.S.L. Two decades of off-label prescribing in children: A literature review. World J. Pediatr. 2018, 14, 528–540. [Google Scholar] [CrossRef] [PubMed]
- Palmaro, A.; Bissuel, R.; Renaud, N.; Durrieu, G.; Escourrou, B.; Oustric, S.; Montastruc, J.-L.; Lapeyre-Mestre, M. Off-Label Prescribing in Pediatric Outpatients. Pediatric 2015, 135, 49–58. [Google Scholar] [CrossRef]
- Rusz, C.-M.; Ősz, B.-E.; Jîtcă, G.; Miklos, A.; Bătrînu, M.-G.; Imre, S. Off-Label Medication: From a Simple Concept to Complex Practical Aspects. Int. J. Environ. Res. Public Health 2021, 18, 10447. [Google Scholar] [CrossRef]
- WHO. Report of the Paediatric Regulatory Network Meeting, 14–15 April 2021. Available online: https://www.who.int/publications/i/item/9789240050280 (accessed on 14 April 2023).
- FDA. Guidance Document for Industry, How to Comply with the Pediatric Research Equity Act. Available online: https://www.fda.gov/media/72274/download (accessed on 14 April 2023).
- EMA. 10-year Report to the European Comission Regarding the Paediatric Regulation. Available online: https://ec.europa.eu/health/system/files/2020-06/paediatrics_10_years_ema_technical_report_0.pdf (accessed on 23 February 2022).
- Thabet, Y.; Klingmann, V.; Breitkreutz, J. Drug Formulations: Standards and Novel Strategies for Drug Administration in Pediatrics. J. Clin. Pharmacol. 2018, 58, S26–S35. [Google Scholar] [CrossRef]
- Musko, M.; Sznitowska, M. Use of compounded dispersing media for extemporaneous pediatric syrups with candesartan cilexetil and valsartan. Acta Pharm. 2014, 64, 463–474. [Google Scholar] [CrossRef]
- WHO. Model List of Essential Medicines for Children, 8th List. 2021. Available online: https://www.who.int/publications/i/item/WHO-MHP-HPS-EML-2021.03 (accessed on 14 April 2023).
- EMA, Inventory of Paediatric Therapeutic Needs, Cardiovascular Therapeutic Area. Available online: https://www.ema.europa.eu/en/documents/other/inventory-paediatric-medicines-cardiovascular-therapeutic-area_en.pdf (accessed on 23 February 2022).
- Morri, M.; Castellano, P.; Leonardi, D.; Vignaduzzo, S. First Development, Optimization, and Stability Control of a Pediatric Oral Atenolol Formulation. AAPS PharmSciTech 2018, 19, 1781–1788. [Google Scholar] [CrossRef] [PubMed]
- Fuss, D.; Gondé, H.; Lamoureux, F.; Pereira, T.; Colnot, M.; Buchbinder, N.; Coquard, A.; Varin, R.; Hervouët, C. Stability study of a compounded oral solution of nicardipine for the treatment of hypertension in children. Eur. J. Pharm. Sci. 2021, 160, 105738. [Google Scholar] [CrossRef]
- Delmoral-Sanchez, J.-M.; Gonzalez-Alvarez, I.; Gonzalez-Alvarez, M.; Navarro-Ruiz, A.; Bermejo, M. Availability of Authorizations from EMA and FDA for Age-Appropriate Medicines Contained in the WHO Essential Medicines List for Children 2019. Pharmaceutics 2020, 12, 316. [Google Scholar] [CrossRef]
- Zahálka, L.; Klovrzová, S.; Matysová, L.; Šklubalová, Z.; Solich, P. Furosemide ethanol-free oral solutions for paediatric use: Formulation, HPLC method and stability study. Eur. J. Hosp. Pharm. 2018, 25, 144–149. [Google Scholar] [CrossRef] [PubMed]
- Mattos da Silva, M.R.; Pereira, D.L.; Pereira dos Santos, E.; Ricci Junior, E. Preparation of extemporaneous liquid in hospital pharmacy. Braz. J. Pharm. Sci. 2020, 56, 1–15. [Google Scholar] [CrossRef]
- Richey, R.H.; Shah, U.U.; Peak, M.; Craig, J.V.; Ford, J.L.; Barker, C.E.; Nunn, A.J.; Turner, M.A. Manipulation of drugs to achieve the required dose is intrinsic to paediatric practice but is not supported by guidelines or evidence. BMC Pediatr. 2013, 13, 81. [Google Scholar] [CrossRef]
- Binson, G.; Beuzit, K.; Migeot, V.; Marco, L.; Troussier, B.; Venisse, N.; Dupuis, A. Preparation and Physicochemical Stability of Liquid Oral Dosage Forms Free of Potentially Harmful Excipient Designed for Pediatric Patients. Pharmaceutics 2019, 11, 190. [Google Scholar] [CrossRef]
- Potier, A.; Voyat, J.; Nicolas, A. Stability study of a clonidine oral solution in a novel vehicle designed for pediatric patients. Pharm. Dev. Technol. 2018, 23, 1067–1076. [Google Scholar] [CrossRef]
- Mfoafo, K.A.; Omidian, M.; Bertol, C.D.; Omidi, Y.; Omidian, H. Neonatal and pediatric oral drug delivery: Hopes and hurdles. Int. J. Pharm. 2021, 597, 120296. [Google Scholar] [CrossRef]
- Belayneh, A.; Tessema, Z. A Systematic Review of the Stability of Extemporaneous Pediatric Oral Formulations. Sci. World. J. 2021, 2021, 8523091. [Google Scholar] [CrossRef]
- Stoltenberg, I.; Winzenburg, G.; Breitkreutz, J. Solid oral dosage forms for children—Formulations, excipients and acceptance issues. J. Appl. Ther. Res. 2010, 7, 141–146. [Google Scholar]
- Freerks, L.; Sommerfeldt, J.; Löper, P.C.; Klein, S. Safe, swallowable and palatable paediatric mini-tablet formulations for a WHO model list of essential medicines for children compound-A promising starting point for future PUMA applications. Eur. J. Pharm. Biopharm. 2020, 156, 11–19. [Google Scholar] [CrossRef]
- Lajoinie, A.; Henin, E.; Nguyen, K.A.; Malik, S.; Mimouni, Y.; Sapori, J.M.; Bréant, V.; Cochat, P.; Kassai, B. Oral drug dosage forms administered to hospitalized children: Analysis of 117,665 oral administrations in a French paediatric hospital over a 1-year period. Int. J. Pharm. 2016, 500, 336–344. [Google Scholar] [CrossRef]
- Galande, A.; Khurana, N.; Mutalik, S. Pediatric dosage forms—Challenges and recent developments: A critical review. J. Appl. Pharm. Sci. 2020, 10, 155–166. [Google Scholar]
- Bajcetic, M.; de Wildt, S.N.; Dalinghaus, M.; Breitkreutz, J.; Klingmann, I.; Lagler, F.B.; Keatley-Clarke, A.; Breur, J.M.; Male, C.; Jovanovic, I.; et al. Orodispersible minitablets of enalapril for use in children with heart failure (LENA): Rationale and protocol for a multicentre pharmacokinetic bridging study and follow-up safety study. Contemp. Clin. Trials Commun. 2019, 15, 100393. [Google Scholar] [CrossRef] [PubMed]
- Bebawy, G.; Sokar, M.; Abdallaha, O.Y. Novel risperidone orally disintegrating minitablets for pediatric use: Patient acceptance and dose adjustment. Drug Dev. Ind. Pharm. 2021, 47, 542–551. [Google Scholar] [CrossRef]
- Lopez, F.L.; Ernest, T.B.; Tuleu, C.; Gul, M.O. Formulation approaches to pediatric oral drug delivery: Benefits and limitations of current platforms. Expert Opin. Drug Deliv. 2015, 12, 1727–1740. [Google Scholar] [CrossRef]
- Aabed, W.J.; Radwan, A.H.; Zaid, A.N.; Shraim, N.Y. Extemporaneous Compounding and Physiological Modeling of Amlodipine/Valsartan Suspension. Int. J. Hypertens. 2021, 12, 6695744. [Google Scholar] [CrossRef]
- EMA. Formulations of Choice for the Paediatric Population-Scientific Guideline. Available online: https://www.ema.europa.eu/en/formulations-choice-paediatric-population (accessed on 23 February 2023).
- van der Vossen, A.C.; van der Velde, I.; Smeets, O.S.; Postma, D.J.; Vermes, A.; Koch, B.C.; Vulto, A.G.; Hanff, L.M. Design and stability study of an oral solution of amlodipine besylate for pediatric patients. Eur. J. Pharm. Sci. 2016, 92, 220–223. [Google Scholar] [CrossRef] [PubMed]
- Alessandrini, E.; Brako, F.; Scarpa, M.; Lupo, M.; Bonifazi, D.; Pignataro, V.; Cavallo, M.; Cullufe, O.; Enache, C.; Nafria, B.; et al. Children’s Preferences for Oral Dosage Forms and Their Involvement in Formulation Research via EPTRI (European Paediatric Translational Research Infrastructure). Pharmaceutics 2021, 13, 730. [Google Scholar] [CrossRef]
- Moreira, M.; Sarraguça, M. How can oral paediatric formulations be improved? A challenge for the XXI century. Int. J. Pharm. 2020, 590, 119905. [Google Scholar] [CrossRef]
- Mannan, A.; Jabeen, A.; Mubeen, H.; Nasiha, A.W. Challenges and advances in pediatric pharmaceutical dosage forms. Int. J. Pharm. Biol. Sci. 2018, 8, 5. [Google Scholar]
- Mohiuddin, A. Extemporaneous Compounding: Cautions, Controversies and Convenience. Inov. J. Med. Health Sci. 2019, 9, 252–264. [Google Scholar] [CrossRef]
- Thabet, Y.; Slavkova, M.; Breitkreutz, J. 10 years EU regulation of pediatric medicines—Impact on cardiovascular drug formulations. Expert Opin. Drug Deliv. 2018, 15, 261–270. [Google Scholar] [CrossRef]
- van Riet-Nales, D.A.; de Neef, B.J.; Schobben, A.F.; Ferreira, J.A.; Egberts, T.C.; Rademaker, C.M. Acceptability of different oral formulations in infants and preschool children. Arch. Dis. Child. 2013, 98, 725–731. [Google Scholar] [CrossRef] [PubMed]
- Spomer, N.; Klingmann, V.; Stoltenberg, I.; Lerch, C.; Meissner, T.; Breitkreutz, J. Acceptance of uncoated mini-tablets in young children—Results from a prospective exploratory cross-over study. Arch. Dis. Child. 2012, 97, 283–286. [Google Scholar] [CrossRef]
- FDA. Pediatric Labeling Changes. Available online: https://www.fda.gov/science-research/pediatrics/pediatric-labeling-changes (accessed on 14 April 2023).
- EMA. Summary of Product Characteristics. Available online: https://www.ema.europa.eu/en/documents/product-information/stayveer-epar-product-information_en.pdf (accessed on 14 April 2023).
- EMA. Summary of Product Characteristics. Available online: https://www.ema.europa.eu/en/documents/product-information/hemangiol-epar-product-information_en.pdf (accessed on 14 April 2023).
- EMA. Summary of Product Characteristics. Available online: https://www.ema.europa.eu/en/documents/product-information/inomax-epar-product-information_en.pdf (accessed on 14 April 2023).
- EMA. Summary of Product Characteristics. Available online: https://www.ema.europa.eu/en/documents/product-information/revatio-epar-product-information_en.pdf (accessed on 14 April 2023).
- EMA. Summary of Product Characteristics. Available online: https://www.ema.europa.eu/en/documents/product-information/tracleer-epar-product-information_en.pdf (accessed on 14 April 2023).
- Kochanowska-Karamyan, A.J. Pharmaceutical Compounding: The Oldest, Most Symbolic, and Still Vital Part of Pharmacy. Int. J. Pharm. Compd. 2016, 20, 367–374. [Google Scholar]
- Minghetti, P.; Pantano, D.; Gennari, C.G.; Casiraghi, A. Regulatory framework of pharmaceutical compounding and actual developments of legislation in Europe. Health Policy 2014, 117, 328–333. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, M.; Almeida, I.F. The Role of Pharmaceutical Compounding in Promoting Medication Adherence. Pharmaceuticals 2022, 15, 1091. [Google Scholar] [CrossRef]
- FDA. Compounding Progress Report. Available online: https://www.fda.gov/media/102493/download (accessed on 23 February 2023).
- Allen, L.V., Jr. Basics of Compounding: Standardization of Compounded Medications. Int. J. Pharm. Compd. 2019, 23, 35–44. [Google Scholar]
- Greeson, N.M.H.; Mixon, W.; Allan, W.C. Safety Standards in Pharmaceutical Compounding, Part 1: The Occupational Safety and Health Administration. Int. J. Pharm. Compd. 2020, 24, 270–276. [Google Scholar] [PubMed]
- Hossain, M.F.; Levesque, D.; Frye, J.; Rashid, M. Incorporating Quality Assurance in Pharmaceutical Compounding-related Courses in the PharmD Curricula. Int. J. Pharm. Compd. 2020, 24, 322–326. [Google Scholar]
- ICH. Q2 (R1) Guideline, Validation of Analytical Procedures. Available online: https://database.ich.org/sites/default/files/Q2%28R1%29%20Guideline.pdf (accessed on 23 February 2023).
- Suárez-González, J.; Santoveña-Estévez, A.; Armijo-Ruíz, S.; Castillo, A.; Fariña, J.B. A High-Demanding Strategy to Ensure the Highest Quality Standards of Oral Liquid Individualized Medicines for Pediatric Use. AAPS PharmSciTech 2019, 20, 208. [Google Scholar] [CrossRef]
- Glass, B.D.; Haywood, A. Stability considerations in liquid dosage forms extemporaneously prepared from commercially available products. J. Pharm. Pharm. Sci. 2006, 9, 398–426. [Google Scholar]
- Standing, J.F.; Tuleu, C. Paediatric formulations-getting to the heart of the problem. Int. J. Pharm. 2005, 300, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Pabari, R.M.; McDermott, C.; Barlow, J.; Ramtoola, Z. Stability of an alternative extemporaneous captopril fast-dispersing tablet formulation versus an extemporaneous oral liquid formulation. Clin. Ther. 2012, 34, 2221–2229. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Chan, S.Y.; Ho, P.C. Effects of sucrose, citric buffer and glucose oxidase on the stability of captopril in liquid formulations. J. Clin. Pharm. Ther. 1999, 24, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Mendes, C.; Costa, A.P.; Oliveira, P.R.; Tagliari, M.P.; Silva, M.A. Physicochemical and microbiological stability studies of extemporaneous antihypertensive pediatric suspensions for hospital use. Pharm. Dev. Technol. 2013, 18, 813–820. [Google Scholar] [CrossRef] [PubMed]
- de Goede, A.L.; Boedhram, R.R.; Eckhardt, M.; Hanff, L.M.; Koch, B.C.; Vermaat, C.H.; Vermes, A. Development and validation of a paediatric oral formulation of clonidine hydrochlorid. Int. J. Pharm. 2012, 433, 119–120. [Google Scholar] [CrossRef]
- Casiraghi, A.; Centin, G.; Selmin, F.; Picozzi, C.; Minghetti, P.; Zanon, D. Critical Aspects in the Preparation of Extemporaneous Flecainide Acetate Oral Solution for Paediatrics. Pharmaceutics 2021, 13, 1963. [Google Scholar] [CrossRef]
- Rigaud, S.; Mathiron, D.; Moufawad, T.; Landy, D.; Djedaini-Pilard, F.; Marçon, F. Cyclodextrin Complexation as a Way of Increasing the Aqueous Solubility and Stability of Carvedilol. Pharmaceutics 2021, 13, 1746. [Google Scholar] [CrossRef]
- Food and Drug Administration, Public Health Service, U.S. Department of Health and Human Services FDA Expands List of “Do Not Compound” Drug Products. J. Pain Palliat. Care Pharmacother. 2016, 31, 76–78. [Google Scholar] [CrossRef]
- Fiocchi, A.; Riva, E.; Giovannini, M. Ethanol in medicines and other products intended for children. Nutr. Res. 1999, 19, 373–379. [Google Scholar] [CrossRef]
- Cuzzolin, L. Neonates exposed to excipients: Concern about safety. J. Pediatr. Neonat. Individual. Med. 2018, 7, e070112. [Google Scholar]
- EMA. Reflection Paper on the Use of Methyl- and Propylparaben as Excipients in Human Medicinal Products for Oral Use. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/reflection-paper-use-methyl-propylparaben-excipients-human-medicinal-products-oral-use_en.pdf (accessed on 23 February 2023).
- EMA. Questions and Answers on Benzoic Acid and Benzoates Used as Excipients in Medicinal Products for Human Use. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/questions-answers-benzoic-acid-benzoates-used-excipients-medicinal-products-human-use_en.pdf (accessed on 23 February 2023).
- ICH. Q1A (R2), Stability Testing of New Drug Substances and Products. Available online: https://database.ich.org/sites/default/files/Q1A%28R2%29%20Guideline.pdf (accessed on 23 February 2023).
- ICH. Q6A, Specifications: Test Procedures and Acceptance Criteria for New Drug Substances and New Drug Products: Chemical Substances. Available online: https://database.ich.org/sites/default/files/Q6A%20Guideline.pdf (accessed on 23 February 2023).
- Chapter 7. Liquid preparations for oral use. In PhEur, 10th ed.; EDQM: Strasbourg, France, 2023.
- Chapter 3.2. Containers. In PhEur, 10th ed.; EDQM: Strasbourg, France, 2023.
- WHO. TRS 1001—52nd report of the WHO Expert Committee on Specifications for Pharmaceutical Preparations. Available online: https://www.who.int/publications/i/item/9789241210195 (accessed on 23 February 2023).
- EMA. Guideline on Pharmaceutical Development of Medicines for Paediatric Use. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-pharmaceutical-development-medicines-paediatric-use_en.pdf (accessed on 23 February 2023).
- USP. Strength and Stability Testing for Compounded Preparationsi. Available online: https://www.usp.org/sites/default/files/usp/document/FAQs/strength-stability-testing-compounded-preparations.pdf (accessed on 23 February 2023).
- Nahata, M.C.; Morosco, R.S.; Hipple, T.F. Stability of amlodipine besylate in two liquid dosage forms. J. Am. Pharm. Assoc. 1999, 39, 375–377. [Google Scholar] [CrossRef] [PubMed]
- Graves, R.A.; Mandal, T.K.; Bostanian, L.A.; Nguyen, A.T.; Swopes, D.; Morris, T.C.; Pramar, Y.V. Physicochemical Stability of Compounded Amlodipine Besylate Suspensions in PCCA Base, SuspendIt. Int. J. Pharm. Compd. 2019, 23, 519–527. [Google Scholar] [PubMed]
- Brustugun, J.; Lao, Y.E.; Fagernaes, C.; Braenden, J.; Kristensen, S. Long-term stability of extemporaneously prepared captopril oral liquids in glass bottles. Am. J. Health Syst. Pharm. 2009, 66, 1722–1725. [Google Scholar] [CrossRef] [PubMed]
- Imre, S.; Vancea, S.; Muntean, D.L.; Sipos, E.; Cocis, A.; Avrigeanu, V.; Mircia, E. Stability of some medicinal solutions with captopril. Rev. Med. Chir. Soc. Med. Nat. 2008, 112, 848–855. (In Romanian) [Google Scholar]
- Buontempo, F.; Bernabeu, E.; Glisoni, R.J.; Quiroga, E.; Bregni, C.; Chiappetta, D.A. Carvedilol stability in paediatric oral liquid formulations. Farm. Hosp. 2010, 34, 293–297. [Google Scholar] [CrossRef]
- Merino-Bohórquez, V.; Delgado-Valverde, M.; García-Palomo, M.; Dávila-Pousa, M.C.; Cañete, C.; Villaronga, M.; Rodriguez-Marrodán, B.; López-Rojas, R.; Cameán-Fernández, M. Pharmaceutical Technology Working Group and Pediatric Pharmacy Working Group of the Spanish Society of Hospital Pharmacy (SEFH), Physicochemical and microbiological stability of two news oral liquid formulations of clonidine hydrochloride for pediatric patients. Pharm. Dev. Technol. 2019, 24, 465–478. [Google Scholar]
- Santoveña, A.; Charola, I.; Suárez-González, J.; Teigell-Pérez, N.; García-van Nood, S.; Soriano, M.; Fariña, J.B. Development of a novel physico-chemically and microbiologically stable oral solution of flecainide for pediatrics. Pharm. Dev. Technol. 2018, 23, 978–985. [Google Scholar] [CrossRef]
- Cies, J.J.; Moore, W.S., II; Chopra, A.; Lu, G.; Mason, R.W. Stability of furosemide and chlorothiazide stored in syringes. Am. J. Health Syst. Pharm. 2015, 72, 2182–2188. [Google Scholar] [CrossRef]
- Cirri, M.; Maestrelli, F.; Mura, P.; Ghelardini, C.; Di Cesare Mannelli, L. Combined Approach of Cyclodextrin Complexation and Nanostructured Lipid Carriers for the Development of a Pediatric Liquid Oral Dosage Form of Hydrochlorothiazide. Pharmaceutics 2018, 10, 287. [Google Scholar] [CrossRef]
- Nahata, M.C.; Morosco, R.S. Stability of lisinopril in two liquid dosage forms. Ann. Pharmacother. 2004, 38, 396–399. [Google Scholar] [CrossRef]
- Foley, L.; Toney, J.; Barlow, J.W.; O’Connor, M.; Fitzgerald-Hughes, D.; Ramtoola, Z. Investigation of the Physical, Chemical and Microbiological Stability of Losartan Potassium 5 mg/mL Extemporaneous Oral Liquid Suspension. Molecules 2021, 26, 301. [Google Scholar] [CrossRef] [PubMed]
- Nahata, M.C.; Morosco, R.S.; Willhite, E.A. Stability of nifedipine in two oral suspensions stored at two temperatures. J. Am. Pharm. Assoc. 2002, 42, 865–867. [Google Scholar] [CrossRef] [PubMed]
- Muśko, M.; Sznitowska, M. Stability of extemporaneous pediatric oral liquids compounded from tablets and drug substance: Case of propranolol and theophylline. Acta Pol. Pharm. 2013, 70, 137–145. [Google Scholar] [PubMed]
- Russell, C.; Begum, S.; Hussain, Y.; Hussain, M.; Huen, D.; Rahman, A.S.; Perrie, Y.; Mohammed, A.R. Paediatric drug development of ramipril: Reformulation, in vitro and in vivo evaluation. J. Drug Target. 2015, 23, 854–863. [Google Scholar] [CrossRef] [PubMed]
- Provenza, N.; Calpena, A.C.; Mallandrich, M.; Halbaut, L.; Clares, B. Design and physicochemical stability studies of paediatric oral formulations of sildenafil. Int. J. Pharm. 2014, 460, 234–239. [Google Scholar] [CrossRef]
- Sae Yoon, A.; Sawatdee, S.; Woradechakul, C.; Sae Chee, K.; Atipairin, A. Physicochemical and Microbiological Stability of the Extemporaneous Sildenafil Citrate Oral Suspension. Sci. Pharm. 2015, 83, 659–670. [Google Scholar] [CrossRef]
- Klovrzová, S.; Zahálka, L.; Kříž, T.; Zahálková, O.; Matysová, L.; Šklubalová, Z.; Horák, P. Extemporaneous sotalol hydrochloride oral solutions for use in paediatric cardiology: Formulation and stability study. Eur. J. Hosp. Pharm. 2016, 23, 33–37. [Google Scholar] [CrossRef]
- Nahata, M.C.; Morosco, R.S. Stability of sotalol in two liquid formulations at two temperatures. Ann. Pharmacother. 2003, 37, 506–509. [Google Scholar] [CrossRef]
- El-Ragehy, N.A.; Hassan, N.Y.; Tantawy, M.A.; Abdelkawy, M. Stability-indicating chromatographic methods for determination of flecainide acetate in the presence of its degradation products; isolation and identification of two of its impurities. Biomed. Chromatogr. 2016, 30, 1541–1548. [Google Scholar] [CrossRef]
- Sajan, P.G.; Rohith, T.; Santosh, P.; Mantelingu, K.; Rangappa, K.S.; Kumara, M.N. Rapid, Highly efficient and stability indicating RP-UPLC method for the quantitative determination of potential impurities of carvedilol active pharmaceutical ingredient. Int. J. Pharm. Pharm. 2014, 6, 214–220. [Google Scholar]
- Baertschi, S.W.; Alsante, K.M.; Reed, R.A. (Eds.) Pharmaceutical Stress Testing: Predicting Drug Degradation, 2nd ed.; CRC Press: Boca Raton, FL, USA, 2011. [Google Scholar]
- de Diego, M.; Soto, J.; Mennickent, S. Stability-indicating LC method for the simultaneous determination of lisinopril and hydrochlorothiazide. J. Chromatogr. Sci. 2014, 52, 1193–1197. [Google Scholar] [CrossRef] [PubMed]
- Hassan, S.A.; Nashat, N.W.; Elghobashy, M.R.; Abbas, S.S.; Moustafa, A.A. Stability-Indicating RP-HPLC and CE Methods for Simultaneous Determination of Bisoprolol and Perindopril in Pharmaceutical Formulation: A Comparative Study. J. Chromatogr. Sci. 2020, 58, 747–758. [Google Scholar] [CrossRef] [PubMed]
- Roberto de Alvarenga Junior, B.; Lajarim Carneiro, R. Chemometrics Approaches in Forced Degradation Studies of Pharmaceutical Drugs. Molecules 2019, 24, 3804. [Google Scholar] [CrossRef] [PubMed]
- FDA. Oral Solutions and Suspensions. Available online: https://www.fda.gov/inspections-compliance-enforcement-and-criminal-investigations/inspection-guides/oral-solutions-and-suspensions-894 (accessed on 23 February 2023).
- Muntean, D.L.; Imre, S.; Voda, C. The Influence of Some Factors on Spirolactone Stability in Solution. Rev. Chim. 2008, 59, 721–725. [Google Scholar] [CrossRef]
- Alarie, H.; Gaëlle Roullin, V.; Leclair, G. Development of a safe and versatile suspension vehicle for pediatric use: Formulation development. Int. J. Pharm. 2019, 569, 118552. [Google Scholar] [CrossRef]
- Deicke, A.; Süverkrüp, R. Dose uniformity and redispersibility of pharmaceutical suspensions 2: Assessment of three commercial erythromycin ethyl succinate oral liquids. Eur. J. Pharm. Biopharm. 2000, 49, 73–78. [Google Scholar] [CrossRef]
- USP. Chapter <795> Pharmaceutical Compounding—Nonsterile Preparations; The United States Pharmacopeial Convention: Rockville, MD, USA, 2010. [Google Scholar]
- Szakonyi, G.; Zelkó, R. The effect of water on the solid state characteristics of pharmaceutical excipients: Molecular mechanisms, measurement techniques, and quality aspects of final dosage form. Int. J. Pharm. Investig. 2012, 2, 18–25. [Google Scholar]
- Teraoka, R.; Otsuka, M.; Matsuda, Y. Effects of temperature and relative humidity on the solid-state chemical stability of ranitidine hydrochloride. J. Pharm. Sci. 1993, 82, 601–604. [Google Scholar] [CrossRef]
- Parmar, N.; Amin, S.; Singla, N.; Kohli, K. The solution, solid state stability and kinetic investigation in degradation studies of lercanidipine: Study of excipients compatibility of lercanidipine. Pharm. Dev. Technol. 2012, 17, 730–740. [Google Scholar] [CrossRef]
- Seburg, R.A.; Ballard, J.M.; Hwang, T.L.; Sullivan, C.M. Photosensitized degradation of losartan potassium in an extemporaneous suspension formulation. J. Pharm. Biomed. Anal. 2006, 42, 411–422. [Google Scholar] [CrossRef]
- Bonferoni, M.C.; Mellerio, G.; Giunchedi, P.; Caramella, C.; Conte, U. Photostability evaluation of nicardipine HCl solutions. Int. J. Pharm. 1992, 80, 109–117. [Google Scholar] [CrossRef]
- Sudesh, B.M.; Uttamrao, K.S. Determination and validation of valsartan and its degradation products by isocratic HPLC. J. Chem. Metrol. 2009, 3, 1–12. [Google Scholar]
- Lanzanova, F.A.; Argenta, D.; Arend, M.Z.; Junior, L.B.; Cardoso, S.G. LC and LC-MS Evaluation of Stress Degradation Behavior of Carvedilol. J. Liq. Chromatogr. Relat. Technol. 2009, 32, 526–543. [Google Scholar] [CrossRef]
- de Diego, M.; Godoy, G.; Mennickent, S.; Olivares, M.; Godoy, R. Stress degradation studies of ramipril by a validated stability-indicating liquid chromatographic method. J. Chil. Chem. Soc. 2010, 55, 450–453. [Google Scholar] [CrossRef]
- Ogbonna, J.D.N.; Cunha, E.; Attama, A.A.; Ofokansi, K.C.; Ferreira, H.; Pinto, S.; Gomes, J.; Marx, Í.M.G.; Peres, A.M.; Lobo, J.M.S.; et al. Overcoming Challenges in Pediatric Formulation with a Patient-Centric Design Approach: A Proof-of-Concept Study on the Design of an Oral Solution of a Bitter Drug. Pharmaceuticals 2022, 15, 1331. [Google Scholar] [CrossRef] [PubMed]
- Patel, V.P.; Tushar, R.D.; Chavda, B.G.; Katira, R.M. Extemporaneous dosage form for oral liquids. Pharmacophore 2011, 2, 49–66. [Google Scholar]
- Polonini, H.C.; Silva, S.L.; de Almeida, T.R.; Brandão, M.A.F.; Ferreira, A.O. Compatibility of caffeine, carvedilol, clomipramine hydrochloride, folic acid, hydrochlorothiazide, loperamide hydrochloride, methotrexate, nadolol, naltrexone hydrochloride and pentoxifylline in SyrSpend SF PH4 oral suspensions. Eur. J. Hosp. Pharm. 2016, 23, 352–358. [Google Scholar] [CrossRef]
- Uriel, M.; Gómez-Rincón, C.; Marro, D. Stability of regularly prescribed oral liquids formulated with SyrSpend® SF. Pharmazie 2018, 73, 196–201. [Google Scholar]
- Thrimawithana, T.R.; D’Amore, S.; Dib, Y.; Fadavi Firooz, N.; Fakhouri, W.; Saeed, A.; Allahham, A. Critical appraisal of commercially available suspending vehicles for extemporaneous compounding of cardiovascular medicines: Physical and chemical stability mini review. Pharm. Dev. Technol. 2019, 24, 529–538. [Google Scholar] [CrossRef]
- Haywood, A.; Glass, B.D. Liquid dosage forms extemporaneously prepared from commercially available products—Considering new evidence on stability. J. Pharm. Pharm. Sci. 2013, 16, 441–455. [Google Scholar] [CrossRef]
- de Saldanha Simon, E.; Wingert, N.R.; Gobetti, C.; Primieri, G.B.; Ayres, M.V.; de Almeida, S.H.O.; Volpato, N.M.; Steppe, M. Development, Quality by Design-Based Optimization, and Stability Assessment of Oral Liquid Formulations Containing Baclofen for Hospital Use. AAPS PharmSciTech 2022, 23, 301. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Active Substance | Age | Type of Approval | Dosage Form | Indication | Year of Approval |
|---|---|---|---|---|---|
| Bosentan [40] | 1–15 y | New medicine including pediatric indication | Film-coated tablets | PAH | 2013 |
| Propranolol [41] | 5 w–5 m | Oral solution | Hemangioma | 2014 | |
| Nitric oxide [42] | 0–17 y | Extension (new pediatric indication) | Gas for inhalation | PAH | 2011 |
| Sildenafil [43] | 1–17 y |
Film-coated tablets Solution for injection Powder for oral suspension | PAH | 2011 | |
| Bosentan [44] | 3 m–18 y | Extension of indication to include new age group | Film-coated tablets | PAH | 2015 |
| Nitric oxide | 0–17 y | Addition of a new dosage strength | Gas for inhalation | PAH | 2011 |
| Amlodipine 1,2 | 6–17 y | Nationally authorized medicine (HU) | Film-coated tablet | hypertension | 2011 |
| Losartan 1 |
2.5 mg/mL 6–16 y | Nationally authorized medicine (RO, HU) | Powder for oral suspension | hypertension | 2009/2011 |
| Losartan 1 | New pediatric indication (RO, IT, FI) | NS | 2009/2010 | ||
| Losartan 1 | New pharmaceutical formulation (CY, EE, IT, ES, UK) | Powder for oral solution/suspension | 2009 | ||
| Spironolactone 1,2 | 25 mg, 50 mg | Nationally authorized medicine (HU) | Film-coated tablet | Congestive heart failure | 2011 |
| Valsartan 2 |
3 mg/mL 1–18 y | Nationally authorized medicine (HU, CZ) | Oral solution | Hypertension | 2010 |
| Valsartan 2 |
New formulation (AU, CY, CZ, EE, FI, IT, RO, SI, ES, SW, UK) | Oral solution/divisibility of the tablet | |||
| Valsartan 2 | 6–18 y | New pediatric indication (CY, EE, RO, FI, SW) | Film-coated tablet | Hypertension | 2010 |
| Candesartan 2 | 6–18 y | New pediatric indication (CY) | Film-coated tablet | Hypertension | 2013 |
| Levamlodipine | 6–17 y | Labelling change | Tablet | Hypertension | 2019 |
| Amlodipine benzoate | >6 y | Labelling change | Oral suspension | Hypertension | 2019 |
| Aliskiren | >6 y | Labelling change | Pellets | Hypertension | 2017 |
| Sodium nitroprusside | NS | Labelling change | Injectable | Hypertensive crisis | 2013 |
| Olmesartan | >6 y | Labelling change | Tablet | Hypertension | 2010 |
| Candesartan | 1–17 y | Labelling change | Tablet | 2009 | |
| Eplerenone | 4–17 y 3 | Labelling change | Tablet | 2008 | |
| Valsartan | 6–16 y | Labelling change | Tablet | 2007 | |
| Metoprolol | 6–16 y 3 | Labelling change | ER Tablets | 2007 | |
| Carvedilol | 2 m–17 y | Labelling change | Tablet | Heart failure | 2007 |
| Irbesartan | 6–16 y 3 | Labelling change | Tablet | Hypertension | 2006 |
| Fenoldopam | <1–12 y | Labelling change | Injectable | In hospital, short-term reduction of hypertension | 2004 |
| Losartan | 6–16 y | Labelling change | Tablet | Hypertension | 2004 |
| Amlodipine | 6–17 y | Labelling change | Tablet | 2004 | |
| Lisinopril | 6–16 y | Labelling change | Tablet | 2003 | |
| Fosinopril | 6–16 y 3 | Labelling change | Tablet | 2003 | |
| Sotalol | 3 d–12 y 3 | Labelling change | Tablet | Arrhythmia | 2001 |
| Enalapril | 1 m–16 y | Labelling change | Tablet | Hypertension | 2001 |
| Stability Testing | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Appearance/Organoleptic Properties | pH | Assay of API/Preservatives | Degradation Products | MT | Redispersibility | Rheological Properties | Particle Size Distribution | Ref. | |
| Amlodipine besylate 1 mg/mL | + | + | + | + | − | − | − | − | [74] |
| Amlodipine besylate & 0.5 mg/mL and 10 mg/mL | + | + | + | + | − | − | + | − | [75] |
| Amlodipine besylate 0.5 mg/mL | + | + | + | + | + | NA | NA | NA | [31] |
| Amlodipine/Valsartan 5/80 mg/5 mL ^ | + | + | + | − | + | − | + | − | [29] |
| Atenolol | + | + | + | − | + | − | − | − | [12] |
| Candesartan 1 mg/mL | + | − | + ** | − | − # | + | + | + | [9] |
| Valsartan 4 mg/mL | |||||||||
| Captopril 1 mg/mL and 5 mg/mL | + | + | + | + | + | NA | NA | NA | [76] |
| Captopril 1 mg/mL | + | − | + | + | + | NA | NA | NA | [77] |
| Carvedilol + CD 5 mg/mL | − | − | + | + | − | NA | NA | NA | [61] |
| Carvedilol 1 mg/mL | − | − | + | + | − | − | − | − | [78] |
| Clonidine 50 μg/mL | + | + | + | − | − | NA | NA | NA | [59] |
| Clonidine 10 μg/mL | + | + | + | + | + | NA | NA | NA | [19] |
| Clonidine 20 μg/mL | + | + | + | + | + | NA | NA | NA | [79] |
| Flecainide acetate 10 mg/mL | + | + | + * | − | + | NA | NA | NA | [60] |
| Flecainide acetate 20 mg/mL | |||||||||
| Flecainide 20 mg/mL | + | − | + ** | − | + | + | + | − | [80] |
| Chlorothiazide 10 mg/mL + Furosemide 1 mg/mL | + | − | + | + | − | NA | NA | NA | [81] |
| Furosemide 5 mg/mL | − | + | + | − | + | + | − | + | [58] |
| Spironolactone 5 mg/mL | |||||||||
| Hydrochlorothiazide 5 mg/mL | |||||||||
| Furosemide 2 mg/mL | + | + | + | + | + | NA | NA | NA | [15] |
| Spironolactone 5 mg/mL | + | + | + ** | + | − | NA | NA | NA | [18] |
| Hydrochlorothiazide 2 mg/mL | |||||||||
| Hydrochlorothiazide + CD 2 mg/mL ^ | − | − | − | − | − | − | + | + | [82] |
| Lisinopril 1 mg/mL | + | + | + | − | − | − | − | − | [83] |
| Losartan 5 mg/mL | + | + | + | + | + | + | − | − | [84] |
| Nicardipine 2 mg/mL | + | + | + ** | − | + | NA | NA | NA | [13] |
| Nifedipine 4 mg/mL | + | + | + | + | − | + | − | − | [85] |
| Propranolol 2 mg/mL and Propranolol 5 mg/mL | + | + | + | − | + | + | + | − | [86] |
| Ramipril 1 mg/mL | + | + | + | + | − | + | + | + | [87] |
| Sildenafil 2 mg/mL | + | + | + | + | + | + | + | + | [88] |
| Sildenafil 2.5 mg/mL | + | + | + | + | + | + | + | − | [89] |
| Sotalol 5 mg/mL | + | + | + | − | − | NA | NA | NA | [90] |
| Sotalol 5 mg/mL | + | + | + | − | − | + | − | − | [91] |
| Design of Stability Study | ||||||||
|---|---|---|---|---|---|---|---|---|
| Drug Substance Dosage Strength | Formulation/ Number of Formulation | Source for Formulation/Vehicles | Study Type * | Duration | Storage Conditions | Testing Frequency | Assigned Shelf-Life | Ref. |
| Amlodipine besylate 0.5 mg/mL | Solution/3 | Crushed tablets/Purified water | Long-term | 12 months | 25 ± 2 °C | 0, 1, 2, 3, 6 months | NS | [31] |
| 40 ± 2 °C | ||||||||
| Accelerated | ||||||||
| In-use | 4 ± 2 °C | 0, 1, 2, 3, 6 9, 12 months | ||||||
| Amlodipine besylate 1 mg/mL | Suspension/2 | Crushed tablets/MC + syrup, | Long-term | 91 days | 4 °C | T0, 7, 14, 28, 42, 56, 70, 91 days | 91 days refrigeration | [74] |
| OraPlus® + OraSweet® | Accelerated | 56 days | 25 °C | |||||
| Amlodipine besylate 0.5 mg/mL and 10 mg/mL # | Suspension/2 | Powder/SuspendIt base | Long-term | 180 days | 5 °C | T0, 7, 14, 29, 46, 60, 90, 120, 180 days | 90 days | [75] |
| 25 °C | 7 days | |||||||
| Amlodipine/Valsartan 5/80 mg/5 mL | Suspension/1 | Crushed tablets/guar gum | Long-term | 4 weeks | RT | T0, week 1, week 2, week 3, week 4 | 4 weeks RT | [29] |
| Atenolol 1% and 4% | Syrup/3 | Powder/Syrup, Glycerin, or both | Long-term | 6 months | 4 ± 2 °C | T0, 6 months | 6 months | [12] |
| 25 ± 2 °C/60 ± 5%RH | 3 months @ | |||||||
| Accelerated | ||||||||
| 40 ± 2 °C/75 ± 5%RH | 6 months | |||||||
| Candesartan 1 mg/mL | Syrup/3 | Crushed tablets/Xanthan gum, vehicle for oral solution USP, sucrose syrup | Long-term | 35 days | 25 °C | T0, 7, 14, 28, 35 days | 14 days @ | [9] |
| Valsartan 4 mg/mL | Syrup/3 | 4 °C | ||||||
| Captopril 1 mg/mL and 5 mg/mL | Solution/1 | Powder/Sterile water for irrigation | Long-term | 12 months | 22 °C | T0, 3, 6, 9, 12 months | 12 months | [76] |
| In-use | 1 month | 4–8 °C | T0, 1 month | |||||
| Captopril 1 mg/mL | Solution/4 | Powder/Preservative solution | Long-term | 39 days | 22 °C | NS | 7 days | [77] |
| t < 8 °C | ||||||||
| Carvedilol + CD 5 mg/mL | Solution/2 | Powder/γCD or RAMEB in aqueous media | Long-term photostability | 6 months | 25 °C/60%RH + 7500 Lux and UV light | T0, 1, 2, 3, 6 months | 6 months | [61] |
| Carvedilol 1 mg/mL | Solution/2 | Powder/Propylene glycol and Polyvinylpyrrolidone | Long-term | 56 days | 4 °C | T0, 3, 7, 14, 28, 56 days | 56 days at RT | [78] |
| 25 °C | ||||||||
| Accelerated | ||||||||
| 40 °C | ||||||||
| Carvedilol 1 mg/mL | Suspension/1 | Powder/aqueous suspension vehicle | Long-term | 56 days | 4 °C | |||
| 25 °C | ||||||||
| Accelerated | 40 °C | |||||||
| Clonidine 50 μg/mL | Solution/1 | Powder/distilled water | Long-term | 9 months | RT | T0, 1, 2, 3 6, 9 months | 9 months | [59] |
| Clonidine 10 μg/mL | Solution/1 | Powder/Inorpha® | Long-term | 60 days | 5 ± 3 °C | T0, 15, 21, 30, 60 days | 60 days | [19] |
| In-use | 25 ± 2 °C | ~ | ||||||
| In-use | 36, 45, 51, 60 days | 5 ± 3 °C p.f.l | ||||||
| Clonidine 20 μg/mL | Solution/2 | Powder/Purified water + simple syrup | Long-term | 90 days | 5 ± 3 °C | T0, 2, 6, 10, 14, 20, 30, 40, 50, 70, 90 days | 90 d | [79] |
| 25 ± 2 °C | ||||||||
| 40 ± 2 °C | ||||||||
| In-use | ||||||||
| In-use | T0, 7, 14, 28, 42 days | 5 ± 3 °C p.f.l | ||||||
| Flecainide acetate 10 mg/mL | Solution/8 | Powder/Ultra pure water | Long-term | 56 days | 4 ± 1 °C | T0, 14, 28, 42, 56 days | & | [60] |
| Flecainide acetate 20 mg/mL | 25 ± 1 °C | 8 weeks | ||||||
| 40 ± 1 °C | / | |||||||
| Flecainide 20 mg/mL | Solution/4 | Powder/Simple syrup | Long-term | 60 days | 5 ± 0.1 °C | T0, 15, 30, 15 for physicochemical | NS | [80] |
| 25 ± 0.1 °C | T0, 10, 30, 60 for microbiology | |||||||
| 40 ± 0.1 °C | ||||||||
| Chlorothiazide 10 mg/mL + /Furosemide 1 mg/mL | Solution/2 | Powder/ Sol. for inj/Dextrose 5% USP | Photostability | 96 h | 25 °C/60% RH | T0, 24, 36, 48, 72, 96 h | 96 h p.f.l | [81] |
| Furosemide 5 mg/mL | Suspension/1 Suspension/2 for Hydrochlorothiazide | Powder/Aqueous suspension vehicle based on CMC Na as suspending agent | Short-term | 7 days | 25 ± 2 °C | T0, 7 days | 7 days; NS | [58] |
| Spironolactone 5 mg/mL | ||||||||
| 5 ± 3 °C | ||||||||
| Hydrochlorothiazide 5 mg/mL | ||||||||
| Furosemide 2 mg/mL | Solution/2 | Powder/Water for injection | Long-term | 9 months | 25 ± 3 °C | T0, 7, 30, 90, 180, 270 days | 9 months RT | [15] |
| 40 ± 0.5 °C | ||||||||
| Spironolactone 5 mg/mL | Suspension/1 | Powder/Syrspend®PH4 Dry | Long-term | 60 days | 22 ± 4 °C | T0, 7, 14, 30, 42, 60 days | 60 days @ | [18] |
| Hydrochlorothiazide 2 mg/mL | 5 ± 3 °C | |||||||
| Hydrochlorothiazide + CD 2 mg/mL | Solution/2 | Powder/HPβCD or SBEβCD and Nano-lipid carriers | Long-term | 3 months | 4 °C | T0, 1, 2, 3 months | NS | [82] |
| Lisinopril 1 mg/mL | Suspension/2 | Crushed tablets/MC 1% Syrup/OraPlus® + OraSweet® | Long-term | 91 days | 25 °C | T0, 7, 14, 28, 42, 56, 70, 91 days | NS | [83] |
| 4 °C in plastic prescription bottles | ||||||||
| Losartan 5 mg/mL | Suspension/2 | Crushed tablets/OraPlus® +OraSweet®/Deionised water | Long-term | 28 days | 4 °C | T0, 1, 3, 7, 10, 14, 21, 28 days | 28 days | [84] |
| RT | ||||||||
| Nicardipine 2 mg/mL | Solution/3 | Powder/InOrpha® ***/Orablend®/Syrspend SF® | Long-term | 90 days | 2–8 °C | T0, 1, 2, 7, 15, 30, 60, 90 days | 90 days | [13] |
| 25 °C | ||||||||
| Nifedipine 4 mg/mL | Suspension/2 | Capsules/MC 1% Syrup/OraPlus® + OraSweet® | Long-term | 91 days | 4 °C | T0, 7, 14, 28, 42, 56, 70, 91 days | NS | [85] |
| 25 °C/60 °C | ||||||||
| Propranolol 2 mg/mL and 5 mg/mL | Suspension/1 | Crushed tablets or Powder/OraSweet®/Vehicle for oral solution USP/Sucrose syrup | Long-term | 35 days | 4 °C | T0, 35 days | 35 days | [86] |
| Syrup/2 | 25 °C | |||||||
| Ramipril 1 mg/mL ** | Solution/2 | Powder/Acetic acid/HPβCD/Xanthan Gum | Accelerated | 6 months | 40 °C/75%RH | T0, 12 months ^ | @ | [87] |
| Suspension/1 | Long-term | 12 months | 25 °C/60%RH | 12 months | ||||
| Sildenafil 2 mg/mL | Suspension/1 Solution/2 | Powder/Bidistilled water | Long-term | 90 days | 4 °C | T0, 7, 15, 30, 60, 90 days | 15 days | [88] |
| 25 °C | 90 days | |||||||
| 40 °C | 60 days | |||||||
| Sildenafil 2.5 mg/mL | Suspension/1 | Crushed tablet/1% MC and syrup | Long-term | 90 days | 30 °C/75%RH | T0, 7, 14, 21, 28, 60, 90 days | 90 days | [89] |
| Accelerated | 40 °C/75%RH | |||||||
| In-use | RT | T0, 7, 14 | 14 days | |||||
| Sotalol 5 mg/mL | Solution/3 **** | Powder/Water for injection | Long-term | 180 days | 25 ± 2 °C | T0, 7, 14, 30, 60, 90, 120, 150, 180 days | 180 days under refrigeration | [90] |
| 5 ± 3 °C | ||||||||
| Sotalol 5 mg/mL | Suspension/2 | Crushed tablets/MC 1% Syrup/OraPlus® + OraSweet® | Long-term | 91 days | 4 °C | T0, 7, 14, 28, 42, 56, 70, 91 days | 3 months ^^ | [91] |
| 25 °C | ||||||||
| 25 °C | ||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jîtcă, C.-M.; Jîtcă, G.; Ősz, B.-E.; Pușcaș, A.; Imre, S. Stability of Oral Liquid Dosage Forms in Pediatric Cardiology: A Prerequisite for Patient’s Safety—A Narrative Review. Pharmaceutics 2023, 15, 1306. https://doi.org/10.3390/pharmaceutics15041306
Jîtcă C-M, Jîtcă G, Ősz B-E, Pușcaș A, Imre S. Stability of Oral Liquid Dosage Forms in Pediatric Cardiology: A Prerequisite for Patient’s Safety—A Narrative Review. Pharmaceutics. 2023; 15(4):1306. https://doi.org/10.3390/pharmaceutics15041306
Chicago/Turabian StyleJîtcă, Carmen-Maria, George Jîtcă, Bianca-Eugenia Ősz, Amalia Pușcaș, and Silvia Imre. 2023. "Stability of Oral Liquid Dosage Forms in Pediatric Cardiology: A Prerequisite for Patient’s Safety—A Narrative Review" Pharmaceutics 15, no. 4: 1306. https://doi.org/10.3390/pharmaceutics15041306