
Levofloxacin HCl-Incorporated Zein-Based Solvent Removal Phase Inversion In Situ Forming Gel for Periodontitis Treatment
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
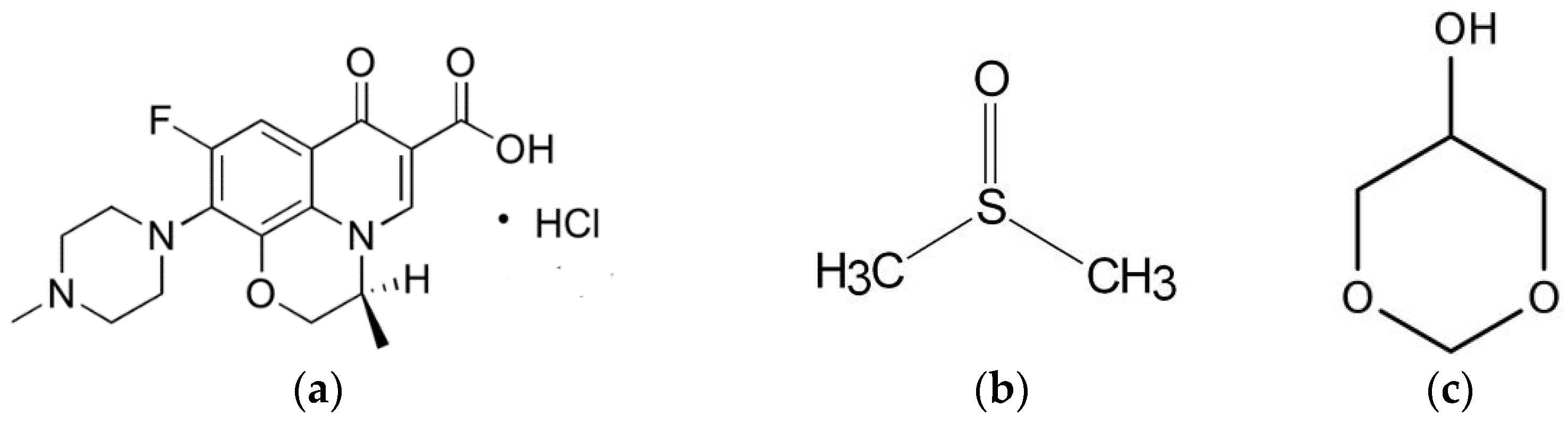
2.1. Materials
2.2. Preparation of In Situ Forming Gel
2.3. Rheology and Viscosity Characterization
2.4. Injectability
2.5. Gel Formation Study
2.6. Drug Content and In Vitro Drug Release Studies
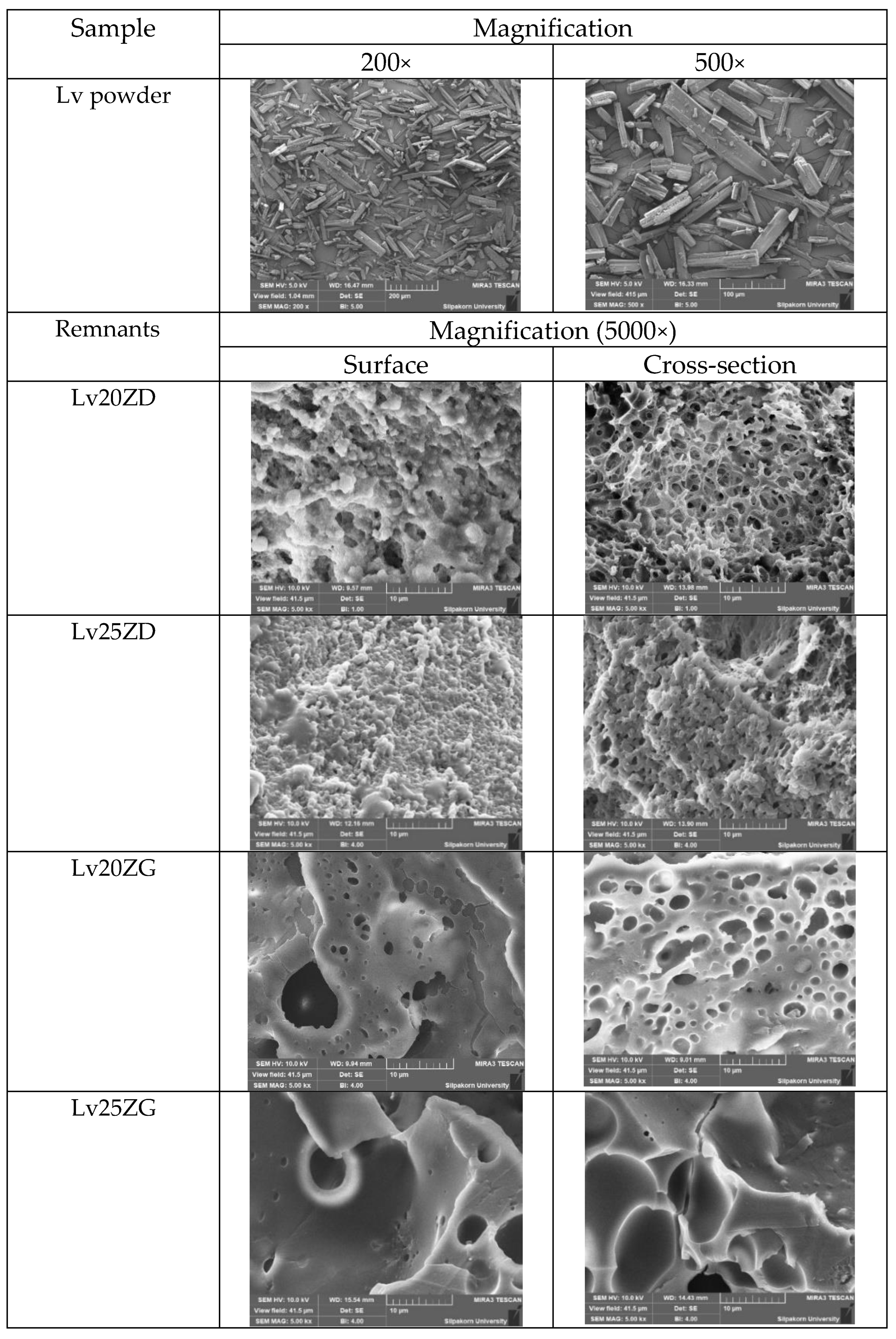
2.7. Scanning Electron Microscopy (SEM)
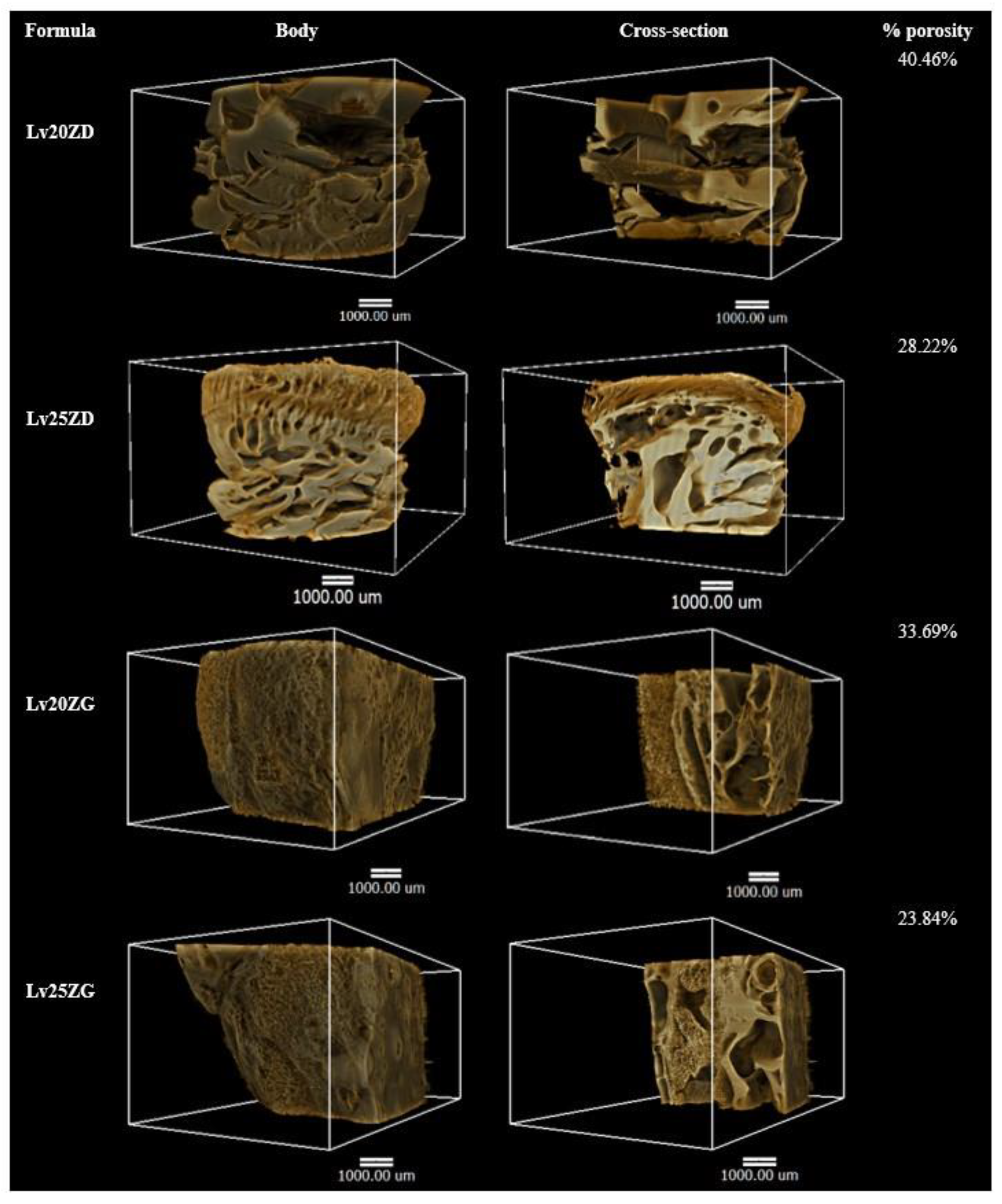
2.8. X-ray Imaging and X-ray Tomographic Microscopy
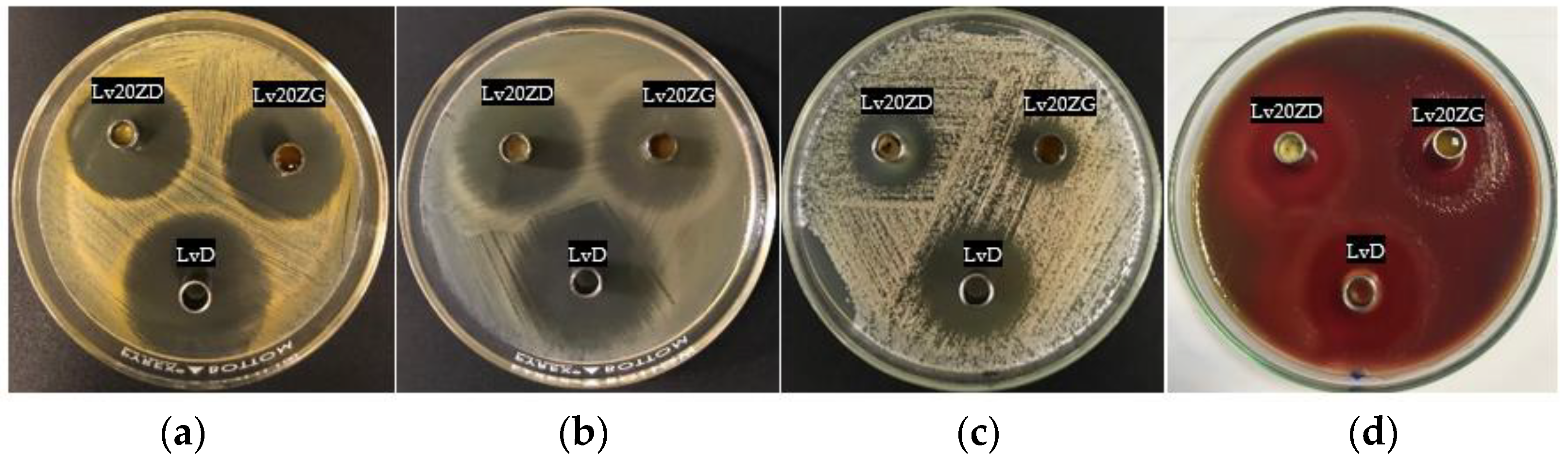
2.9. Antimicrobial Activities
2.10. Statistical Analysis
3. Results and Discussion
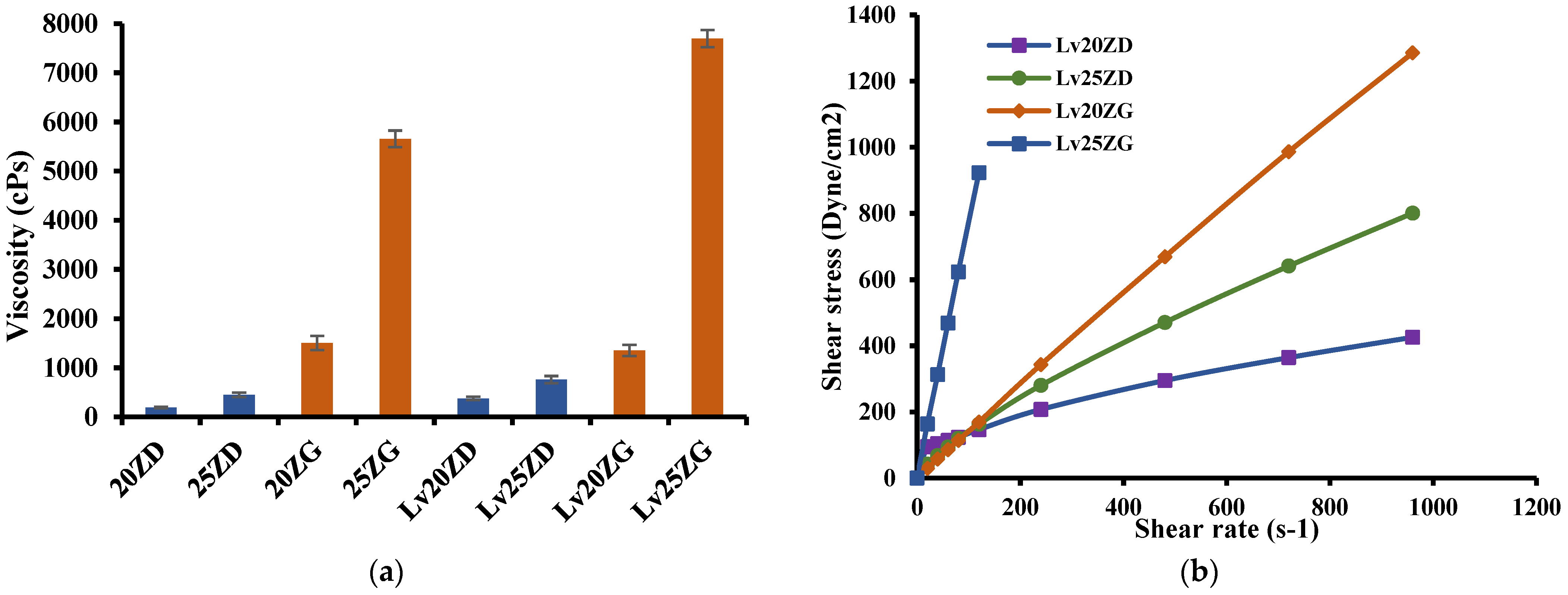
3.1. Viscosity and Rheological Behavior
3.2. Injectability
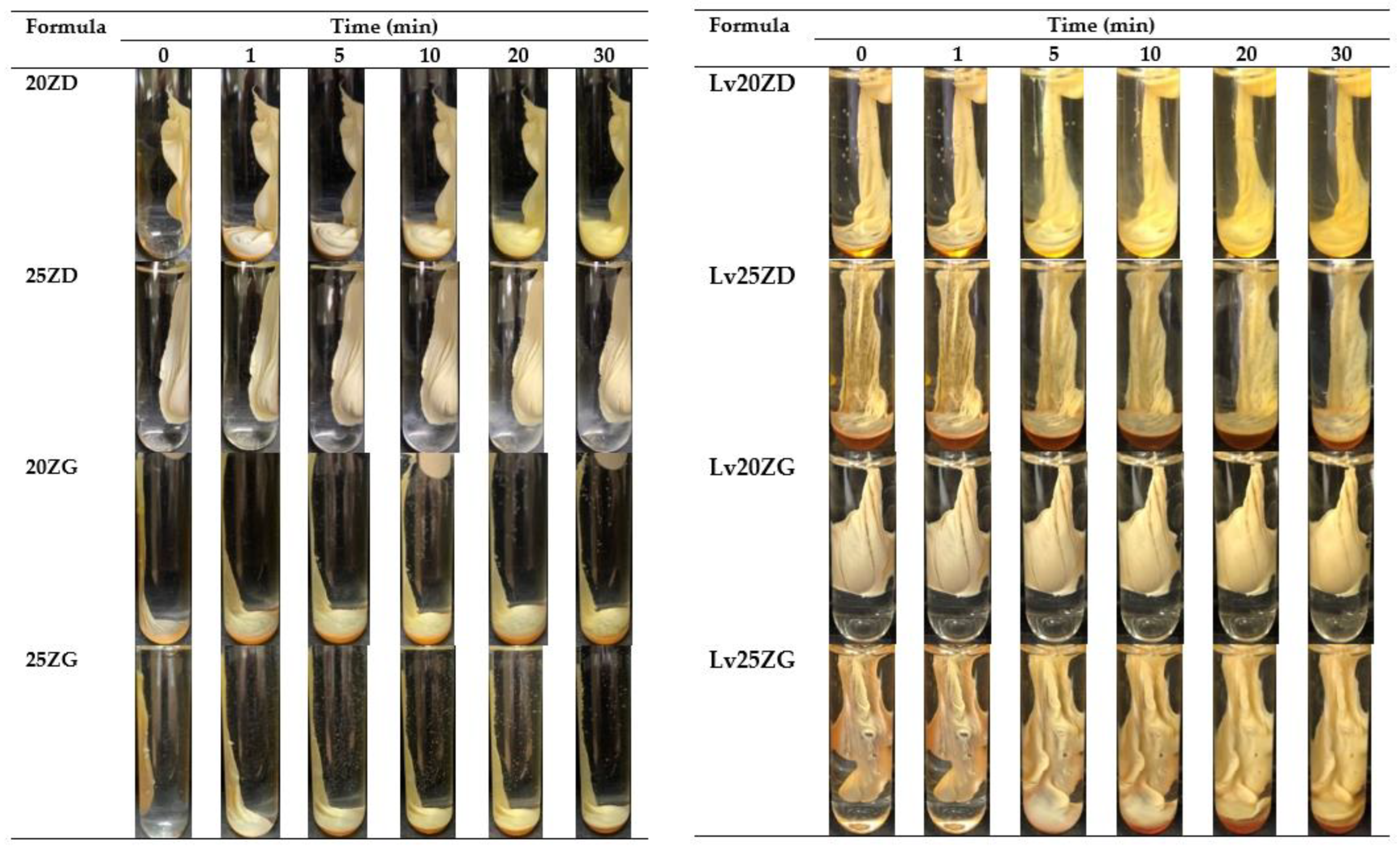
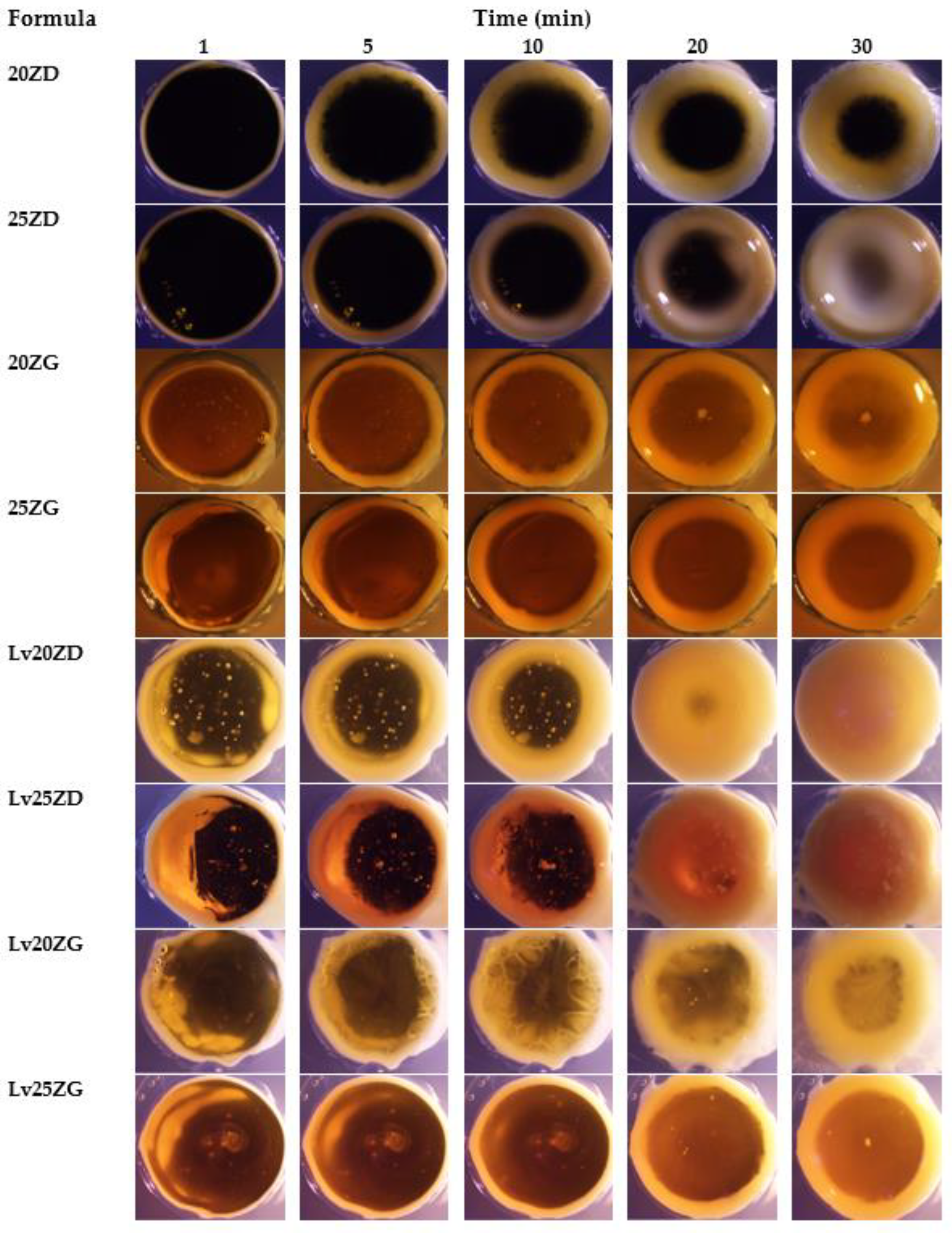
3.3. Gel Formation
3.4. Drug Content and In Vitro Drug Release Study
3.5. Scanning Electron Microscopy (SEM)
3.6. X-ray Computed Microtomography (μCT)
3.7. Antimicrobial Activities
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, S.Z.; Esen, A. Primary structure of a proline-rich zein and its cDNA. Plant Physiol. 1986, 81, 70–74. [Google Scholar] [CrossRef] [PubMed]
- Lawton, J.W. Zein: A history of processing and use. Cereal Chem. 2002, 79, 1–18. [Google Scholar] [CrossRef]
- Wang, Y.; Padua, G.W. Nanoscale characterization of zein self-assembly. Langmuir 2012, 28, 2429–2435. [Google Scholar] [CrossRef]
- Madeka, H.; Kokini, J.L. Effect of glass transition and cross-linking on rheological properties of zein: Development of a preliminary state diagram. Cereal Chem. 1996, 73, 433–438. [Google Scholar]
- Meyer, N.; Rivera, L.R.; Ellis, T.; Qi, J.; Ryan, M.P.; Boccaccini, A.R. Bioactive and antibacterial coatings based on zein/bioactive glass composites by electrophoretic deposition. Coatings 2018, 8, 27. [Google Scholar] [CrossRef] [Green Version]
- Weissmueller, N.T.; Lu, H.D.; Hurley, A.; Prud’homme, R.K. Nanocarriers from GRAS zein proteins to encapsulate hydrophobic actives. Biomacromolecules 2016, 17, 3828–3837. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Luo, Y.; Wang, Q. Antioxidant and antimicrobial properties of essential oils encapsulated in zein nanoparticles prepared by liquid–liquid dispersion method. LWT—Food Sci. Technol. 2012, 48, 283–290. [Google Scholar] [CrossRef]
- Brahatheeswaran, D.; Mathew, A.; Aswathy, R.G.; Nagaoka, Y.; Venugopal, K.; Yoshida, Y.; Maekawa, T.; Sakthikumar, D. Hybrid fluorescent curcumin loaded zein electrospun nanofibrous scaffold for biomedical applications. Biomed. Mater. 2012, 7, 045001. [Google Scholar] [CrossRef]
- Podaralla, S.; Averineni, R.; Alqahtani, M.; Perumal, O. Synthesis of novel biodegradable methoxy poly(ethylene glycol)-zein micelles for effective delivery of curcumin. Mol. Pharm. 2012, 9, 2778–2786. [Google Scholar] [CrossRef]
- Gong, S.J.; Sun, S.X.; Sun, Q.S.; Wang, J.Y.; Liu, X.M.; Liu, G.Y. Tablets based on compressed zein microspheres for sustained oral administration: Design, pharmacokinetics, and clinical study. J. Biomater. Appl. 2011, 26, 195–208. [Google Scholar] [CrossRef]
- Lin, T.; Lu, C.; Zhu, L.; Lu, T. The biodegradation of zein in vitro and in vivo and its application in implants. AAPS PharmSciTech 2011, 12, 172–176. [Google Scholar] [CrossRef]
- Corradini, E.; Curti, P.S.; Meniqueti, A.B.; Martins, A.F.; Rubira, A.F.; Muniz, E.C. Recent advances in food-packing, pharmaceutical and biomedical applications of zein and zein-based materials. Int. J. Mol. Sci. 2014, 15, 22438–22470. [Google Scholar] [CrossRef] [Green Version]
- Sun, Q.S.; Dong, J.; Lin, Z.X.; Yang, B.; Wang, J.Y. Comparison of cytocompatibility of zein film with other biomaterials and its degradability in vitro. Biopolymers 2005, 78, 268–274. [Google Scholar] [CrossRef]
- Wang, H.J.; Gong, S.J.; Lin, Z.X.; Fu, J.X.; Xue, S.T.; Huang, J.C.; Wang, J.Y. In vivo biocompatibility and mechanical properties of porous zein scaffolds. Biomaterials 2007, 28, 3952–3964. [Google Scholar] [CrossRef] [PubMed]
- Xiao, D.; Davidson, P.M.; Zhong, Q. Spray-dried zein capsules with coencapsulated nisin and thymol as antimicrobial delivery system for enhanced antilisterial properties. J. Agric. Food Chem. 2011, 59, 7393–7404. [Google Scholar] [CrossRef]
- Wongsasulak, S.; Puttipaiboon, N.; Yoovidhya, T. Fabrication, gastromucoadhesivity, swelling, and degradation of zein-chitosan composite ultrafine fibers. J. Food Sci. 2013, 78, N926–N935. [Google Scholar] [CrossRef]
- Raza, A.; Hayat, U.; Zhang, X.; Wang, J.Y. Self-assembled zein organogels as in situ forming implant drug delivery system and 3D printing ink. Int. J. Pharm. 2022, 627, 122206. [Google Scholar] [CrossRef] [PubMed]
- Tortorella, S.; Maturi, M.; Buratti, V.V.; Vozzolo, G.; Locatelli, E.; Sambri, L.; Franchini, M.C. Zein as a versatile biopolymer: Different shapes for different biomedical applications. RSC Adv. 2021, 11, 39004–39026. [Google Scholar] [CrossRef]
- Eldeeb, A.E.; Salah, S.; Mabrouk, M.; Amer, M.S.; Elkasabgy, N.A. Dual-drug delivery via zein in situ forming implants augmented with titanium-doped bioactive glass for bone regeneration: Preparation, in vitro characterization, and in vivo evaluation. Pharmaceutics 2022, 14, 274. [Google Scholar] [CrossRef]
- Gao, Z.; Ding, P.; Zhang, L.; Shi, J.; Yuan, S.; Wei, J.; Chen, D. Study of a pingyangmycin delivery system: Zein/Zein-SAIB in situ gels. Int. J. Pharm. 2007, 328, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Tang, Z.; Zhang, D.; Sun, H.; Liu, H.; Zhang, Y.; Zhang, Y.; Chen, X. Doxorubicin-loaded polysaccharide nanoparticles suppress the growth of murine colorectal carcinoma and inhibit the metastasis of murine mammary carcinoma in rodent models. Biomaterials 2015, 51, 161–172. [Google Scholar] [CrossRef]
- Xu, Y.; Wu, J.; Chen, Y.; Liu, J.; Li, N.; Yang, F. The use of zein and shuanghuangbu for periodontal tissue engineering. Int. J. Oral. Sci. 2010, 2, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Patil, V.; Mali, R.; Mali, A. Systemic anti-microbial agents used in periodontal therapy. J. Indian Soc. Periodontol. 2013, 17, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Slots, J. Selection of antimicrobial agents in periodontal therapy. J. Periodontal Res. 2002, 37, 389–398. [Google Scholar] [CrossRef] [Green Version]
- Vyas, S.P.; Sihorkar, V.; Mishra, V. Controlled and targeted drug delivery strategies towards intraperiodontal pocket diseases. J. Clin. Pharm. Ther. 2000, 25, 21–42. [Google Scholar] [CrossRef] [PubMed]
- Chuenbarn, T.; Chantadee, T.; Phaechamud, T. Doxycycline hyclate-loaded Eudragit® RS PO in situ-forming microparticles for periodontitis treatment. J. Drug Deliv. Sci. Technol. 2022, 71, 103294. [Google Scholar] [CrossRef]
- Chuenbarn, T.; Sirirak, J.; Tuntarawongsa, S.; Okonogi, S.; Phaechamud, T. Design and comparative evaluation of vancomycin HCl-loaded rosin-based in situ forming gel and microparticles. Gels 2022, 8, 231. [Google Scholar] [CrossRef]
- Khaing, E.M.; Mahadlek, J.; Okonogi, S.; Phaechamud, T. Lime peel oil–incorporated rosin-based antimicrobial in situ forming gel. Gels 2022, 8, 169. [Google Scholar] [CrossRef]
- Senarat, S.; Lwin, W.W.; Mahadlek, J.; Phaechamud, T. Doxycycline hyclate-loaded in situ forming gels composed from bleached shellac, Ethocel, and Eudragit RS for periodontal pocket delivery. Saudi Pharm. J. 2021, 29, 252–263. [Google Scholar] [CrossRef]
- Chantadee, T.; Sirirak, J.; Hoshino, T.; Phaechamud, T. Augmentative molecular aspect for phase inversion of vancomycin hydrochloride-loaded fatty acid in situ forming matrices. Mater. Des. 2021, 199, 109429. [Google Scholar] [CrossRef]
- Langtry, H.D.; Lamb, H.M. Levofloxacin. Its use in infections of the respiratory tract, skin, soft tissues and urinary tract. Drugs 1998, 56, 487–515. [Google Scholar] [CrossRef] [PubMed]
- Davis, R.; Bryson, H.M. Levofloxacin. A review of its antibacterial activity, pharmacokinetics and therapeutic efficacy. Drugs 1994, 47, 677–700. [Google Scholar] [CrossRef] [PubMed]
- Stein, G.E.; Goldstein, E.J.C. Review of the in vitro activity and potential clinical efficacy of levofloxacin in the treatment of anaerobic infections. Anaerobe 2003, 9, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Aksoy, F.; Dogan, R.; Ozturan, O.; Altuntas, E.; Yener, F.G.; Topcu, G.; Guler, B. Effect of a combination of mometasone furoate, levofloxacin, and retinyl palmitate with an in situ gel-forming nasal delivery system on nasal mucosa damage repair in an experimental rabbit model. Biomed. Pharmacother. 2017, 96, 603–611. [Google Scholar] [CrossRef]
- Bansal, M.; Mittal, N.; Yadav, S.K.; Khan, G.; Mishra, B.; Nath, G. Clinical evaluation of thermoresponsive and mucoadhesive chitosan in situ gel containing levofloxacin and metronidazole in the treatment of periodontal pockets—A split-mouth, clinical study. J. Pierre Fauchard Acad. 2016, 30, 6–14. [Google Scholar] [CrossRef]
- Bansal, M.; Mittal, N.; Yadav, S.K.; Khan, G.; Gupta, P.; Mishra, B.; Nath, G. Periodontal thermoresponsive, mucoadhesive dual antimicrobial loaded in-situ gel for the treatment of periodontal disease: Preparation, in-vitro characterization and antimicrobial study. J. Oral Biol. Craniofac. Res. 2018, 8, 126–133. [Google Scholar] [CrossRef]
- Phaechamud, T.; Praphanwittaya, P.; Laotaweesub, K. Solvent effect on fluid characteristics of doxycycline hyclate-loaded bleached shellac in situ-forming gel and -microparticle formulations. J. Pharm. Investig. 2018, 48, 409–419. [Google Scholar] [CrossRef]
- Tsampanakis, I.; Orbaek White, A. The Mechanics of Forming Ideal Polymer–Solvent Combinations for Open-Loop Chemical Recycling of Solvents and Plastics. Polymers 2022, 14, 112. [Google Scholar] [CrossRef]
- Gandhi, K.S.; Williams, M.C. Solvent effects on the viscosity of moderately concentrated polymer solutions. J. Polym. Sci. Part C Polym. Symp. 2007, 35, 211–234. [Google Scholar] [CrossRef]
- Phaechamud, T.; Lertsuphotvanit, N.; Praphanwittaya, P. Viscoelastic and thermal properties of doxycycline hyclate-loaded bleached shellac in situ forming -gel and -microparticle. J. Drug Deliv. Sci. Technol. 2018, 44, 448–456. [Google Scholar] [CrossRef]
- Danzer, L.A.; Ades, H.; Rees, E.D. The helical content of zein, a water insoluble protein, in non-aqueous solvents. Biochim. Biophys. Acta 1975, 386, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, H.S.; Falcetta, J.J. Introduction to polymer science and technology. In SPE Textbook; John Wiley & Sons: New York, NY, USA, 1977; pp. 1–268. [Google Scholar]
- Gad, H.A.; El-Nabarawi, M.A.; Abd El-Hady, S.S. Formulation and evaluation of PLA and PLGA in situ implants containing secnidazole and/or doxycycline for treatment of periodontitis. AAPS PharmSciTech 2008, 9, 878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jagdale, P.P.; Li, D.; Shao, X.; Bostwick, J.B.; Xuan, X. Fluid rheological effects on the flow of polymer solutions in a contraction–expansion microchannel. Micromachines 2020, 11, 278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Q.; Fassihi, M.A.; Fassihi, R. Delivery considerations of highly viscous polymeric fluids mimicking concentrated biopharmaceuticals: Assessment of injectability via measurement of total work done “WT. ” AAPS PharmSciTech 2018, 19, 1520–1528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiong, W.; Gao, X.; Zhao, Y.; Xu, H.; Yang, X. The dual temperature/pH-sensitive multiphase behavior of poly(N-isopropylacrylamide-co-acrylic acid) microgels for potential application in in situ gelling system. Colloids Surf. B Biointerfaces 2011, 84, 103–110. [Google Scholar] [CrossRef]
- Christopher, J.; Rini, C.J.; Roberts, B.C.; Aojun, A.V.; Klug, L.R.; Shermana, D.B.; Pettis, R.J. Enabling faster subcutaneous delivery of larger volume, high viscosity fluids. Expert Opin. Drug Deliv. 2022, 19, 1165–1176. [Google Scholar] [CrossRef]
- Rungseevijitprapa, W.; Bodmeier, R. Injectability of biodegradable in situ forming microparticle systems (ISM). Eur. J. Pharm. Sci. 2009, 36, 524–531. [Google Scholar] [CrossRef]
- Ibrahim, T.M.; Eissa, R.G.; El-Megrab, N.A.; El-Nahas, H.M. Morphological characterization of optimized risperidone-loaded in-situ gel forming implants with pharmacokinetic and behavioral assessments in rats. J. Drug Deliv. Sci. Technol. 2021, 61, 102195. [Google Scholar] [CrossRef]
- Chantadee, T.; Sawangsri, P.; Santimaleeworagun, W.; Phaechamud, T. Vancomycin hydrochloride-loaded stearic acid/lauric acid in situ forming matrix for antimicrobial inhibition in patients with joint infection after total knee arthroplasty. Mater. Sci. Eng. C 2020, 115, 110761. [Google Scholar] [CrossRef]
- Kirchner, B.; Reiher, M. The secret of dimethyl sulfoxide−water mixtures. A quantum chemical study of 1DMSO−nWater clusters. J. Am. Chem. Soc. 2002, 124, 6206–6215. [Google Scholar] [CrossRef]
- Philippot, P.; Lenoir, N.; D’Hoore, W.; Bercy, P. Improving patients’ compliance with the treatment of periodontitis: A controlled study of behavioural intervention. J. Clin. Periodontol. 2005, 32, 653–658. [Google Scholar] [CrossRef] [PubMed]
- Rein, S.M.T.; Intaraphairot, T.; Santimaleeworagun, W.; Chantadee, T.; Chuenbarn, T.; Phaechamud, T. Fluid properties of solvents and oils used in in situ forming microparticles. Thai J. Pharm. Sci. 2022, 46, 46–55. [Google Scholar]
- Rarokar, N.R.; Saoji, S.D.; Raut, N.A.; Taksande, J.B.; Khedekar, P.B.; Dave, V.S. Nanostructured cubosomes in a thermoresponsive depot system: An alternative approach for the controlled delivery of docetaxel. AAPS PharmSciTech 2015, 17, 436–445. [Google Scholar] [CrossRef] [Green Version]
- Phaechamud, T.; Mahadlek, J. Solvent exchange-induced in situ forming gel comprising ethyl cellulose-antimicrobial drugs. Int. J. Pharm. 2015, 494, 381–392. [Google Scholar] [CrossRef]
- Rein, S.M.T.; Lwin, W.W.; Tuntarawongsa, S.; Phaechamud, T. Meloxicam-loaded solvent exchange-induced in situ forming beta-cyclodextrin gel and microparticle for periodontal pocket delivery. Mater. Sci. Eng. C 2020, 115, 111275. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Mu, H.; Larsen, S.W.; Jensen, H.; Østergaard, J. An in vitro gel-based system for characterizing and predicting the long-term performance of PLGA in situ forming implants. Int. J. Pharm. 2021, 609, 121183. [Google Scholar] [CrossRef]
- Vandana, K.; Javali, M. A comparative evaluation of atrigel delivery system (10% doxycycline hyclate) Atridox with scaling and root planing and combination therapy in treatment of periodontitis: A clinical study. J. Indian Soc. Periodontol. 2012, 16, 43–48. [Google Scholar] [CrossRef]
- Schwach-Abdellaoui, K.; Vivien-Castioni, N.; Gurny, R. Local delivery of antimicrobial agents for the treatment of periodontal disease. Eur. J. Pharm. Biopharm. 2000, 50, 83–99. [Google Scholar] [CrossRef]
- Rajeshwari, H.R.; Dhamecha, D.; Jagwani, S.; Rao, M.; Jadhav, K.; Shaikh, S.; Puzhankara, L.; Jalalpure, S. Local drug delivery systems in the management of periodontitis: A scientific review. J. Control. Release 2019, 307, 393–439. [Google Scholar] [CrossRef]
- Kornman, K.S. Controlled-release local delivery antimicrobials in periodontics: Prospects for the future. J. Periodontol. 1993, 64, 782–791. [Google Scholar] [CrossRef]
- Ritger, P.L.; Peppas, N.A. A simple equation for description of solute release I. Fickian and non-fickian release from non-swellable devices in the form of slabs, spheres, cylinders or discs. J. Control. Release 1987, 5, 23–36. [Google Scholar] [CrossRef]
- Siepmann, J.; Siepmann, F. Mathematical modeling of drug delivery. Int. J. Pharm. 2008, 364, 328–343. [Google Scholar] [CrossRef] [PubMed]
- Shefeeq, T.; Ahmad, N. Mathematical Modelling for the Diffusional Release of a Dispersed Solute from a Cylindrical Polymer Matrix into Finite External Volume. Appl. Math. 2012, 3, 34–38. [Google Scholar] [CrossRef] [Green Version]
- Ghavami-Lahiji, M.; Shafiei, F.; Kashi, T.J.; Najafi, F. Drug release kinetics and biological properties of a novel local drug carrier system. Dent. Res. J. 2021, 18, 94. [Google Scholar] [CrossRef]
- Perioli, L.; Ambrogi, V.; Rubini, D.; Giovagnoli, S.; Ricci, M.; Blasi, P.; Rossi, C. Novel mucoadhesive buccal formulation containing metronidazole for the treatment of periodontal disease. J. Control. Release 2004, 95, 521–533. [Google Scholar] [CrossRef]
- Joiner, J.B.; Prasher, A.; Young, I.C.; Kim, J.; Shrivastava, R.; Maturavongsadit, P.; Benhabbour, S.R. Effects of drug physicochemical properties on in-situ forming implant polymer degradation and drug release kinetics. Pharmaceutics 2022, 14, 1188. [Google Scholar] [CrossRef]
- Parent, M.; Nouvel, C.; Koerber, M.; Sapin, A.; Maincent, P.; Boudier, A. PLGA in situ implants formed by phase inversion: Critical physicochemical parameters to modulate drug release. J. Control. Release 2013, 172, 292–304. [Google Scholar] [CrossRef]
- Ranch, K.M.; Maulvi, F.A.; Koli, A.R.; Desai, D.T.; Parikh, R.K.; Shah, D.O. Tailored doxycycline hyclate loaded in situ gel for the treatment of periodontitis: Optimization, in vitro characterization, and antimicrobial studies. AAPS PharmSciTech 2021, 22, 77. [Google Scholar] [CrossRef]
- Rawson, S.D.; Maksimcuka, J.; Withers, P.J.; Cartmell, S.H. X-ray computed tomography in life sciences. BMC Biol. 2020, 18, 21. [Google Scholar] [CrossRef] [Green Version]
- Rezaei, A.; Mohammadi, M.R. In vitro study of hydroxyapatite/polycaprolactone (HA/PCL) nanocomposite synthesized by an in situ sol-gel process. Mater. Sci. Eng. C 2013, 33, 390–396. [Google Scholar] [CrossRef]
- Lee, D.K.; Wang, D.P. Formulation development of allopurinol suppositories and injectable. Drug Dev. Ind. Pharm. 1999, 25, 1205–1208. [Google Scholar] [CrossRef] [PubMed]
- Strickley, R.G. Solubilizing excipients in oral and injectable formulations. Pharm. Res. 2004, 21, 201–230. [Google Scholar] [CrossRef] [PubMed]
- Rowe, R.C.; Sheskey, P.J.; Quinn, M.E. Handbook of Pharmaceutical Excipients, 6th ed.; Pharmaceutical Press: London, UK, 2009. [Google Scholar]
- Ahmed, T.A.; Ibrahim, H.M.; Samy, A.M.; Kaseem, A.; Nutan, M.T.H.; Hussain, M.D. Biodegradable injectable in situ implants and microparticles for sustained release of montelukast: In vitro release, pharmacokinetics and stability. AAPS PharmSciTech 2014, 15, 772–780. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thakur, R.R.; McMillan, H.L.; Jones, D.S. Solvent induced phase inversion-based in situ forming controlled release drug delivery implants. J. Control. Release 2014, 176, 8–23. [Google Scholar] [CrossRef] [PubMed]
- Matschke, C.; Isele, U.; van Hoogevest, P.; Fahr, A. Sustained-release injectables formed in situ and their potential use for veterinary products. J. Control Release 2002, 85, 1–15. [Google Scholar] [CrossRef]
- Kim, K.-B.; Anand, S.S.; Muralidhara, S.; Kim, H.J.; Bruckner, J.V. Formulation-dependent toxicokinetics explains differences in the GI absorption, bioavailability and acute neurotoxicity of deltamethrin in rats. Toxicology 2007, 234, 194–202. [Google Scholar] [CrossRef]
- Spiegel, A.J.; Noseworthy, M.M. Use of nona-queous solvents in parenteral products. J. Pharm. Sci. 1963, 52, 917–927. [Google Scholar] [CrossRef]
- Seymour, R.A.; Heasman, P.A. Pharmacological control of periodontal disease. II. Antimicrobial agents. J. Dent. 1995, 23, 5–14. [Google Scholar] [CrossRef]
- Amel, Y.; Bouziane, D.; Leila, M.; Ahmed, B. Microbiological study of periodontitis in the west of Algeria. West Indian Med. J. 2015, 5, 7–12. [Google Scholar]
- Speck, S.; Wenke, C.; Feßler, A.T.; Kacza, J.; Geber, F.; Scholtzek, A.D.; Hanke, D.; Eichhorn, I.; Schwarz, S.; Rosolowski, M.; et al. Borderline resistance to oxacillin in Staphylococcus aureus after treatment with sub-lethal sodium hypochlorite concentrations. Heliyon 2020, 6, e04070. [Google Scholar] [CrossRef]
- Rattanaumpawan, P.; Nachamkin, I.; Bilker, W.B.; Roy, J.A.; Metlay, J.P.; Zaoutis, T.E.; Lautenbach, E. High fluoroquinolone MIC is associated with fluoroquinolone treatment failure in urinary tract infections caused by fluoroquinolone susceptible Escherichia coli. Ann. Clin. Microbiol. Antimicrob. 2017, 16, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koeth, L.M.; Good, C.E.; Appelbaum, P.C.; Goldstein, E.J.; Rodloff, A.C.; Claros, M.; Dubreuil, L.J. Surveillance of susceptibility patterns in 1297 European and US anaerobic and capnophilic isolates to co-amoxiclav and five other antimicrobial agents. J. Antimicrob. Chemother. 2004, 53, 1039–1044. [Google Scholar] [CrossRef] [PubMed] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Formula | Levofloxacin HCl (Lv) | Zein | DMSO | Glycerol Formal (GF) |
|---|---|---|---|---|
| (% w/w) | (% w/w) | (% w/w) | (% w/w) | |
| 20ZD | - | 20 | 80 | - |
| 25ZD | - | 25 | 75 | - |
| 20ZG | - | 20 | - | 80 |
| 25ZG | - | 25 | - | 75 |
| Lv20ZD | 1 | 20 | 79 | - |
| Lv25ZD | 1 | 25 | 74 | - |
| Lv20ZG | 1 | 20 | - | 79 |
| Lv25ZG | 1 | 25 | - | 74 |
| LvG | 1 | - | - | 99 |
| LvD | 1 | - | 99 | - |
| Formula | Injectability Force (N) | Work of Injectability (N.mm) |
|---|---|---|
| 20ZD | 1.02 ± 0.08 | 7.51 ± 0.15 c |
| 25ZD | 1.19 ± 0.05 | 9.13 ± 0.21 c,e |
| 20ZG | 1.07 ± 0.10 a | 13.75 ± 0.95 f |
| 25ZG | 3.02 ± 0.04 a | 42.31 ± 1.23 f |
| Lv20ZD | 1.00 ± 0.04 | 7.09 ± 0.17 d |
| Lv25ZD | 1.14 ± 0.03 | 12.34 ± 0.21 d,e |
| Lv20ZG | 1.15 ± 0.06 b | 15.20 ± 0.40 g |
| Lv25ZG | 3.07 ± 0.13 b | 44.75 ± 1.14 g |
| Formula | Zero-Order | First-Order | Higuchi’s | Korsmeyer–Peppas | ||
|---|---|---|---|---|---|---|
| r2 | r2 | r2 | r2 | n | Release Mechanism | |
| LvD | 0.9437 | 0.9693 | 0.9730 | 0.9809 | 0.599 ± 0.055 | non-Fickian diffusion |
| LvG | 0.9712 | 0.9336 | 0.9175 | 0.9774 | 0.797 ± 0.054 | non-Fickian diffusion |
| Lv20ZD | 0.8449 | 0.9930 | 0.9578 | 0.9597 | 0.530 ± 0.015 | non-Fickian diffusion |
| Lv25ZD | 0.7644 | 0.9774 | 0.9228 | 0.9542 | 0.387 ± 0.020 | non-Fickian diffusion |
| Lv20ZG | 0.8345 | 0.9855 | 0.9345 | 0.9451 | 0.574 ± 0.045 | non-Fickian diffusion |
| Lv25ZG | 0.7944 | 0.9622 | 0.9408 | 0.9418 | 0.477 ± 0.010 | non-Fickian diffusion |
| Formula | Inhibition Zone + S.D. (mm) | |||
|---|---|---|---|---|
| S. aureus ATCC 6538 | E. coli ATCC 8739 | C. albicans ATCC 10231 | P. gingivalis ATCC 33277 | |
| DMSO | 12.3 ± 0.5 a | 16.0 ± 0.8 a | 25.7 ± 1.2 a | 17.3 ± 0.5 a |
| GF | 15.7 ± 1.2 c | 16.3 ± 0.5 c | 31.3 ± 1.2 c | 13.3 ± 0.5 c |
| 20ZD | 11.3 ± 0.5 | 14.0 ± 0.0 | 13.7 ± 2.1 | 16.0 ± 0.8 |
| 25ZD | - | - | 10.3 ± 0.5 a | - |
| 20ZG | 12.7 ± 0.9 c | 15.0 ± 0.8 | 14.0 ± 1.4 c | 14.0 ± 0.8 |
| 25ZG | - | - | 14.7 ± 0.9 c | - |
| LvD | 37.7 ± 0.5 a,b | 38.3 ± 1.2 a,b | 19.7 ± 1.7 a | 39.7 ± 1.7 a,b |
| LvG | 37.0 ± 0.8 c, d | 35.7 ± 0.5 c, d | 27.3 ± 0.9 d | 33.7 ± 0.5 c,d |
| Lv20ZD | 34.3 ± 0.5 b | 32.0 ± 0.8 b | 16.7 ± 2.1 | 35.3 ± 1.2 b |
| Lv25ZD | 34.3 ± 0.5 b | 31.3 ± 0.5 b | - | 29.0 ± 0.8 b |
| Lv20ZG | 34.3 ± 0.5 d | 30.7 ± 0.5 d | 17.0 ± 1.4 d | 29.3 ± 1.7 d |
| Lv25ZG | 32.3 ± 0.5 d | 29.7 ± 0.5 d | 12.0 ± 1.6 d | 26.0 ± 0.8 d |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Senarat, S.; Rojviriya, C.; Puyathorn, N.; Lertsuphotvanit, N.; Phaechamud, T. Levofloxacin HCl-Incorporated Zein-Based Solvent Removal Phase Inversion In Situ Forming Gel for Periodontitis Treatment. Pharmaceutics 2023, 15, 1199. https://doi.org/10.3390/pharmaceutics15041199
Senarat S, Rojviriya C, Puyathorn N, Lertsuphotvanit N, Phaechamud T. Levofloxacin HCl-Incorporated Zein-Based Solvent Removal Phase Inversion In Situ Forming Gel for Periodontitis Treatment. Pharmaceutics. 2023; 15(4):1199. https://doi.org/10.3390/pharmaceutics15041199
Chicago/Turabian StyleSenarat, Setthapong, Catleya Rojviriya, Napaphol Puyathorn, Nutdanai Lertsuphotvanit, and Thawatchai Phaechamud. 2023. "Levofloxacin HCl-Incorporated Zein-Based Solvent Removal Phase Inversion In Situ Forming Gel for Periodontitis Treatment" Pharmaceutics 15, no. 4: 1199. https://doi.org/10.3390/pharmaceutics15041199