
Development and Optimization of Sildenafil Orodispersible Mini-Tablets (ODMTs) for Treatment of Pediatric Pulmonary Hypertension Using Response Surface Methodology


Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Design of Experiments and Statistical Analysis
2.3. Production of Granules and Tablets
2.4. Granules Characterization
2.4.1. Measurement of Granule Size
2.4.2. Measurement of Granules Bulk and Tapped Density
2.4.3. Measurement of Granules Flowability
2.5. Tablets Characterization
2.5.1. Weight and Content Uniformity
2.5.2. Crushing Strength/Breaking Force
2.5.3. Friability
2.5.4. Disintegration Time
2.5.5. In Vitro Dissolution Study
3. Results and Discussion
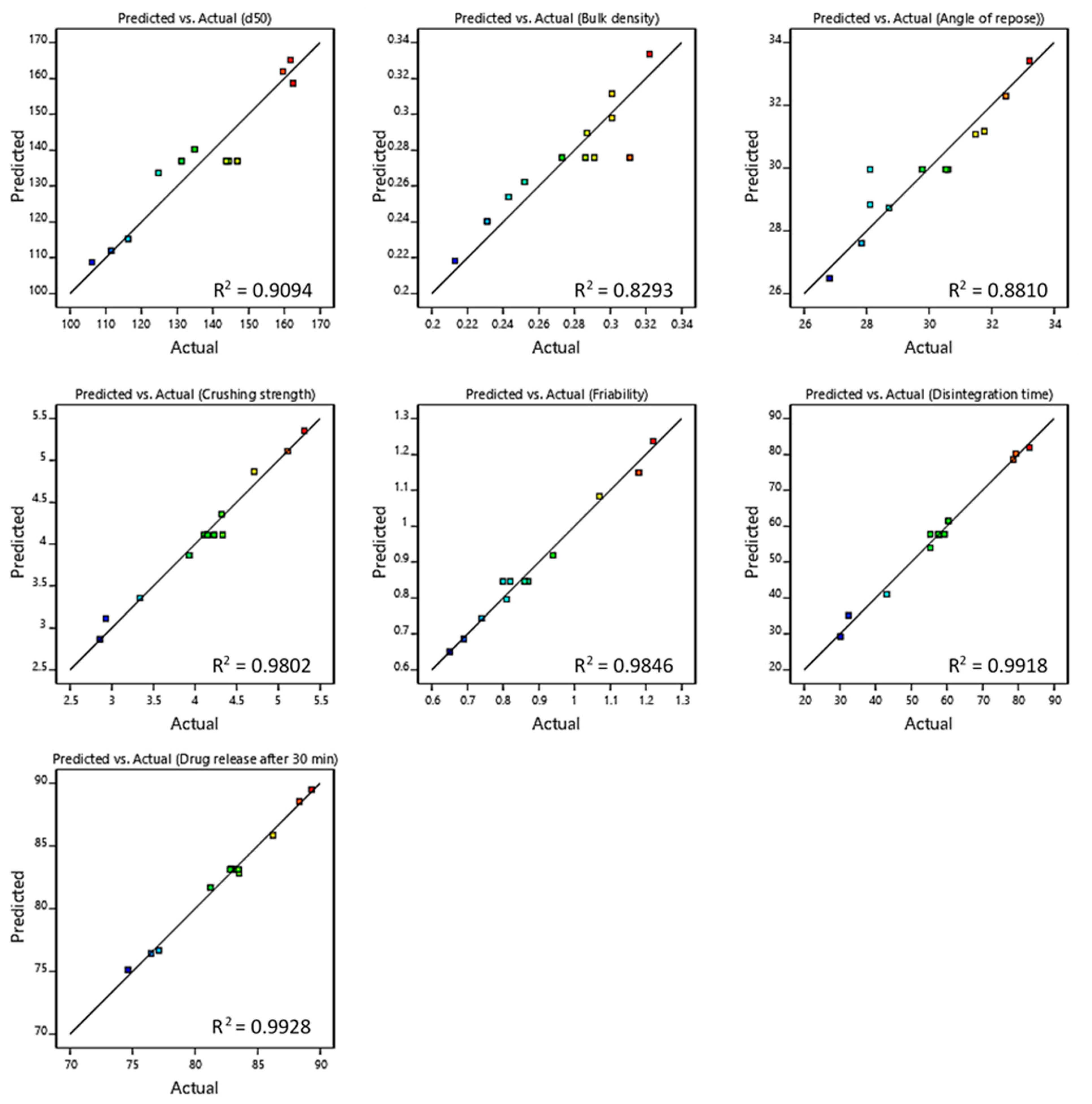
3.1. Fitting Data to the Models
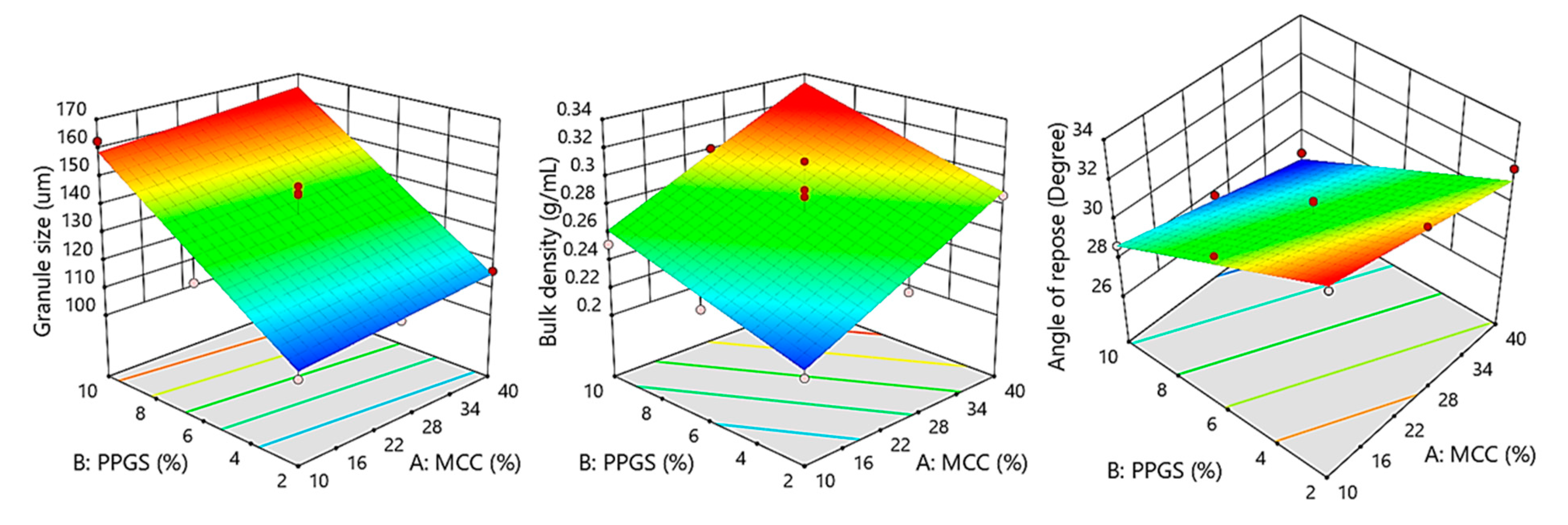
3.2. Influence of Independent Variables on Mean Granules Size
3.3. Effect of Independent Variables on Granules’ Bulk Density
3.4. Effect of Independent Variables on Granules Flowability
3.5. Weight Variability and CU of ODMTs
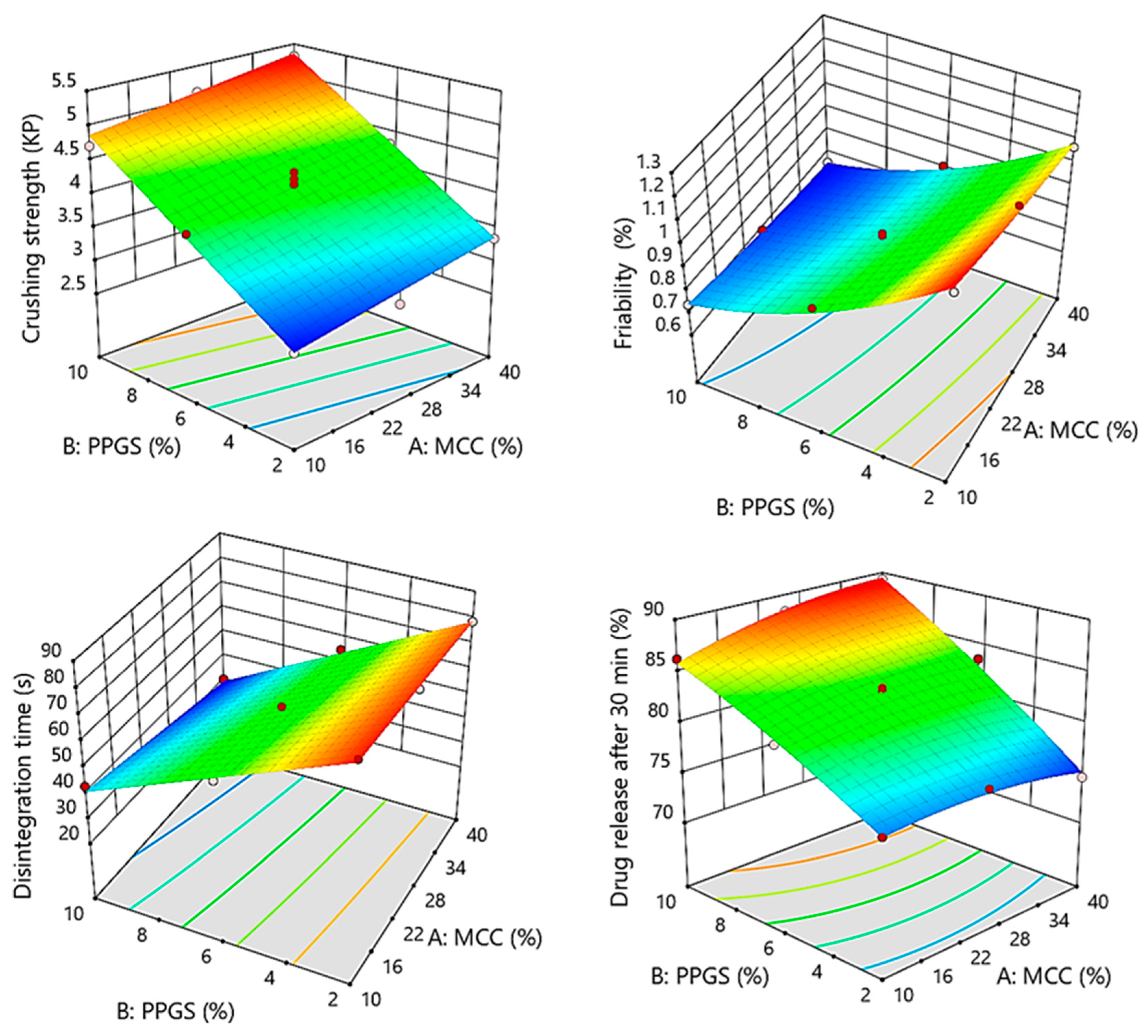
3.6. Influence of Independent Variables on Tablet Crushing Strength and Friability
3.7. Influence of Independent Variables on Disintegration Time of ODMTs
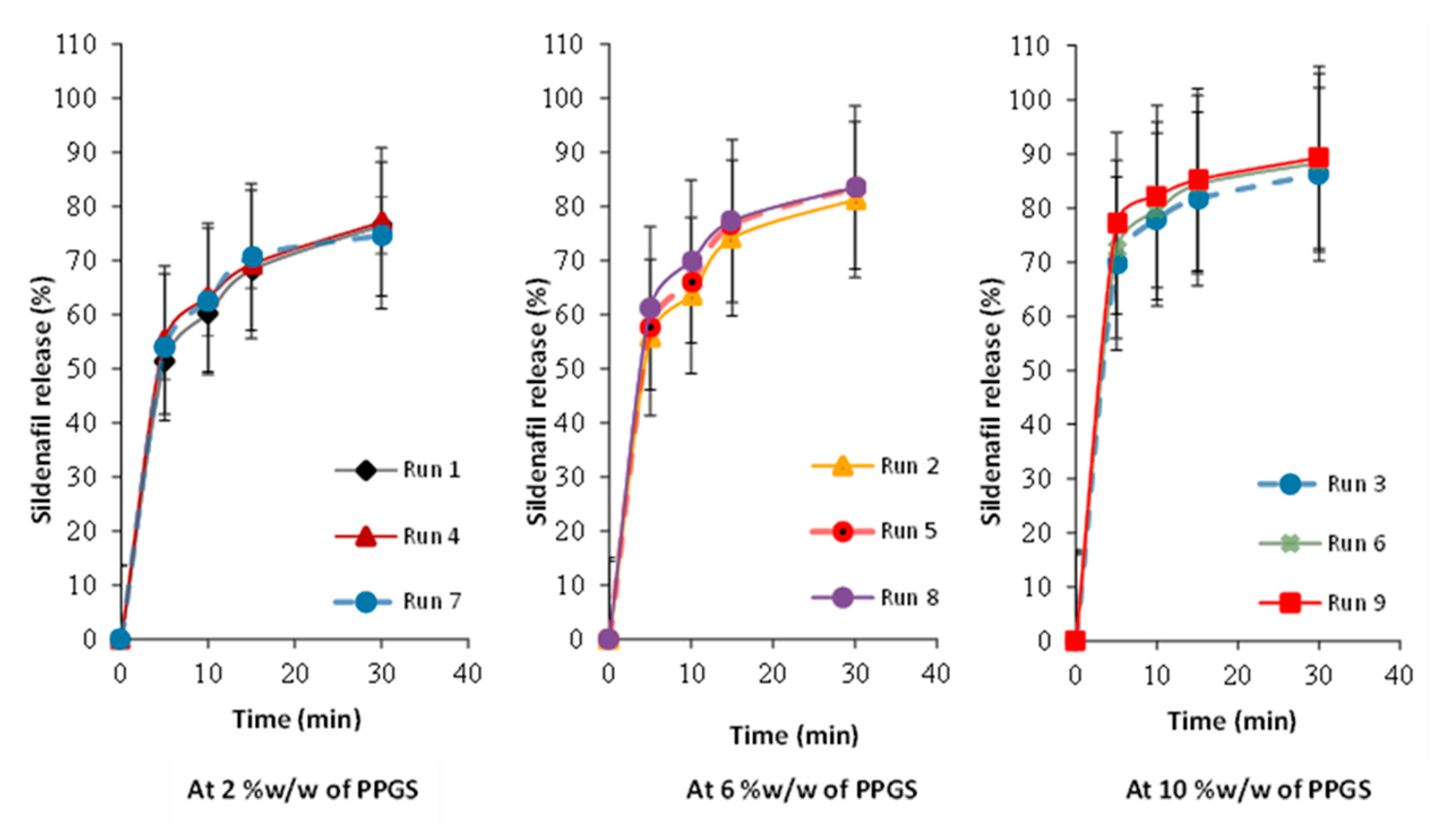
3.8. Influence of Independent Variables on Tablet Dissolution
3.9. Lack-of-Fit Test
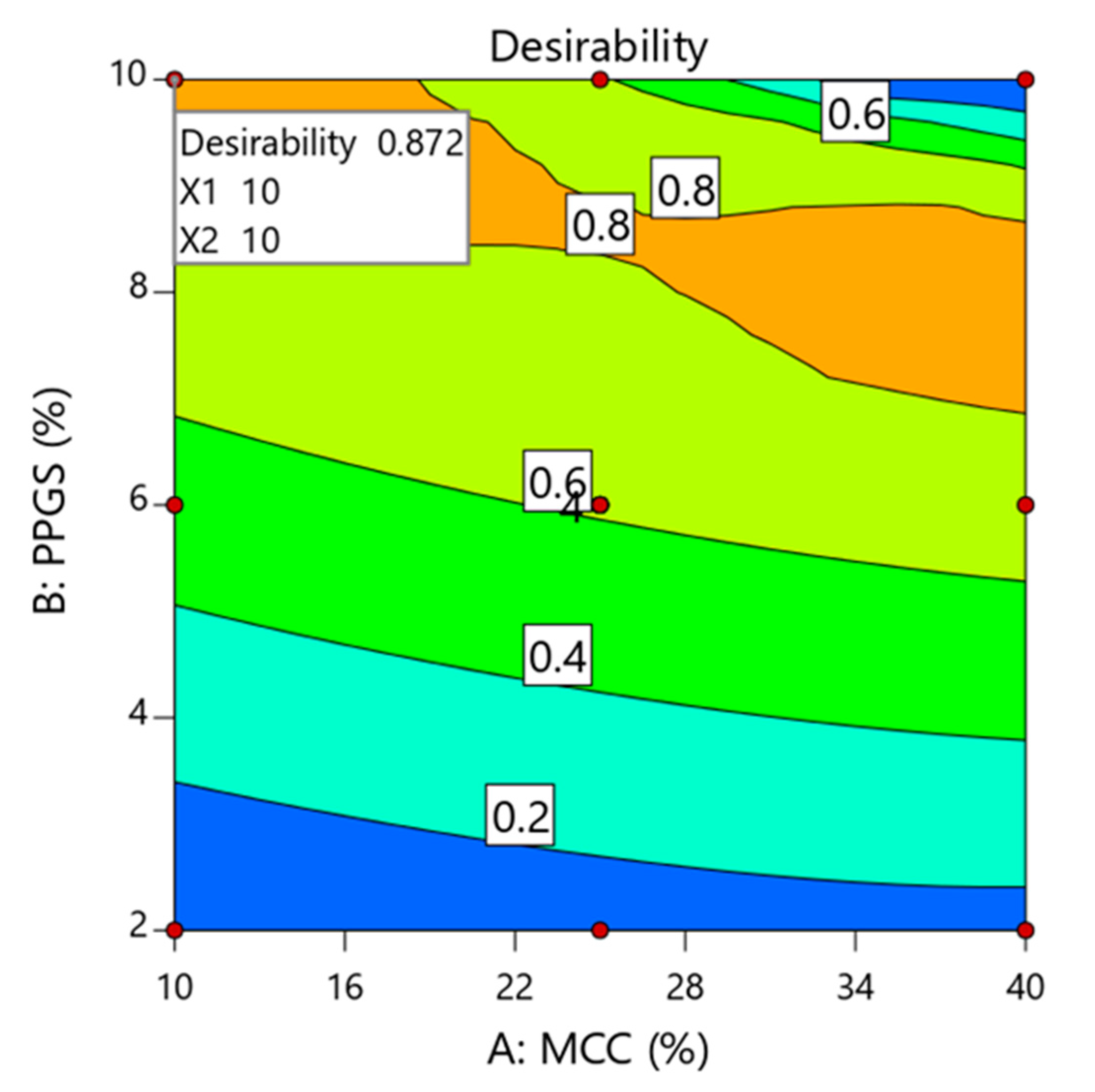
3.10. Formulation Optimization
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Epstein, R.; Krishnan, U.S. Management of Pulmonary Hypertension in the Pediatric Patient. Cardiol. Clin. 2022, 40, 115–127. [Google Scholar] [CrossRef] [PubMed]
- William, M.B.; Ali, M.A.S.; Farghaly, H.S.; Elfaham, T.H. Effectiveness and short-term survival associated with adding sildenafil to conventional therapy in the management of children with pulmonary hypertension. Prog. Pediatr. Cardiol. 2020, 56, 101168. [Google Scholar] [CrossRef]
- Provenza, N.; Calpena, A.C.; Mallandrich, M.; Halbaut, L.; Clares, B. Design and physicochemical stability studies of paediatric oral formulations of sildenafil. Int. J. Pharm. 2014, 460, 234–239. [Google Scholar] [CrossRef] [Green Version]
- Stoltenberg, I.; Breitkreutz, J. Orally disintegrating mini-tablets (ODMTs)—A novel solid oral dosage form for paediatric use. European J. Pharm. Biopharm. 2011, 78, 462–469. [Google Scholar] [CrossRef] [PubMed]
- WHO (World Health Organisation). 3, Flexible Solid Oral Dosage: Dispersible Formulations of Amoxicillin. In Revised WHO Classification and Treatment of Pneumonia in Children at Health Facilities: Evidence Summaries; World Health Organization: Geneva, Switzerland, 2014. Available online: https://www.ncbi.nlm.nih.gov/books/NBK264163/ (accessed on 19 February 2023).
- Mitra, B.; Chang, J.; Wu, S.-J.; Wolfe, C.N.; Ternik, R.L.; Gunter, T.Z.; Victor, M.C. Feasibility of mini-tablets as a flexible drug delivery tool. Int. J. Pharm. 2017, 525, 149–159. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Thool, P.; Meruva, S.; Li, J.; Patel, J.; Agrawal, A.; Karki, S.; Bowen, W.; Mitra, B. Development of low dose micro-tablets by high shear wet granulation process. Int. J. Pharm. 2020, 587, 119571. [Google Scholar] [CrossRef]
- Hellberg, E.; Westberg, A.; Appelblad, P.; Mattsson, S. Evaluation of dissolution techniques for orally disintegrating mini-tablets. J. Drug Deliv. Sci. Technol. 2021, 61, 102191. [Google Scholar] [CrossRef]
- Suárez-González, J.; Magariños-Triviño, M.; Díaz-Torres, E.; Cáceres-Pérez, A.R.; Santoveña-Estévez, A.; Fariña, J.B. Individualized orodispersible pediatric dosage forms obtained by molding and semi-solid extrusion by 3D printing: A comparative study for hydrochlorothiazide. J. Drug Deliv. Sci. Technol. 2021, 66, 102884. [Google Scholar] [CrossRef]
- Naman, S.; Madhavi, N.; Singh, B.; Madan, J.; Baldi, A. Implementing risk-based quality by design for development and optimization of flavored oral disintegrating mini tablets. J. Drug Deliv. Sci. Technol. 2021, 66, 102799. [Google Scholar] [CrossRef]
- Mitra, B.; Thool, P.; Meruva, S.; Aycinena, J.A.; Li, J.; Patel, J.; Patel, K.; Agarwal, A.; Karki, S.; Bowen, W. Decoding the small size challenges of mini-tablets for enhanced dose flexibility and micro-dosing. Int. J. Pharm. 2020, 574, 118905. [Google Scholar] [CrossRef]
- Shukla, D.; Chakraborty, S.; Singh, S.; Mishra, B. Mouth Dissolving Tablets I: An Overview of Formulation Technology. Sci. Pharm. 2009, 77, 309–326. [Google Scholar] [CrossRef] [Green Version]
- Khafagy, E.-S.; Fayed, M.H.; Alrabahi, S.H.; Gad, S.; Alshahrani, S.M.; Aldawsari, M. Defining design space for optimization of escitalopram ultra-fast melting tablet using suspension spray-coating technique: In-vitro and in-vivo evaluation. J. Drug Deliv. Sci. Technol. 2020, 57, 101631. [Google Scholar] [CrossRef]
- Fayed, M.H.; Alalaiwe, A.; Almalki, Z.S.; Helal, D.A. Design Space Approach for the Optimization of Green Fluidized Bed Granulation Process in the Granulation of a Poorly Water-Soluble Fenofibrate Using Design of Experiment. Pharmaceutics 2022, 14, 1471. [Google Scholar] [CrossRef]
- AlAli, A.S.; Aldawsari, M.F.; Alalaiwe, A.; Almutairy, B.K.; Al-Shdefat, R.; Walbi, I.A.; Fayed, M.H. Exploitation of Design-of-Experiment Approach for Design and Optimization of Fast-Disintegrating Tablets for Sublingual Delivery of Sildenafil Citrate with Enhanced Bioavailability Using Fluid-Bed Granulation Technique. Pharmaceutics 2021, 13, 870. [Google Scholar] [CrossRef] [PubMed]
- Yogendrarajah, P.; Natalis, L.; Peys, W.; Lenaerts, M.; Lebrun, P.; Boon, J.-P.; Hellings, M. Application of Design Space and Quality by Design Methodologies combined with Ultra High-Performance Liquid Chromatography for the Optimization of the Sample Preparation of Complex Pharmaceutical Dosage Forms. J. Pharm. Biomed. Anal. 2022, 227, 115149. [Google Scholar] [CrossRef]
- Usta, D.Y.; Timur, B.; Teksin, Z.S. Formulation development, optimization by Box-Behnken design, characterization, in vitro, ex-vivo, and in vivo evaluation of bosentan-loaded self-nanoemulsifying drug delivery system: A novel alternative dosage form for pulmonary arterial hypertension treatment. Eur. J. Pharm. Sci. 2022, 174, 106159. [Google Scholar]
- Yi, E.-J.; Kim, J.-Y.; Rhee, Y.-S.; Kim, S.-H.; Lee, H.-J.; Park, C.-W.; Park, E.-S. Preparation of sildenafil citrate microcapsules and in vitro/in vivo evaluation of taste masking efficiency. Int. J. Pharm. 2014, 466, 286–295. [Google Scholar] [CrossRef] [PubMed]
- Alalaiwe, A.; Fayed, M.H.; Alshahrani, S.M.; Alsulays, B.B.; Alshetaili, A.S.; Tawfeek, H.M.; Khafagy, E.-S. Application of design of experiment approach for investigating the effect of partially pre-gelatinized starch on critical quality attributes of rapid orally disintegrating tablets. J. Drug Deliv. Sci. Technol. 2019, 49, 227–234. [Google Scholar] [CrossRef]
- Aodah, A.H.; Fayed, M.H.; Alalaiwe, A.; BAlsulays, B.; FAldawsari, M.; Khafagy, E.-S. Design, Optimization, and Correlation of In Vitro/In Vivo Disintegration of Novel Fast Orally Disintegrating Tablet of High Dose Metformin Hydrochloride Using Moisture Activated Dry Granulation Process and Quality by Design Approach. Pharmaceutics 2020, 12, 598. [Google Scholar] [CrossRef] [PubMed]
- Thoorens, G.; Krier, F.; Leclercq, B.; Carlin, B.; Evrard, B. Microcrystalline cellulose, a direct compression binder in a quality by design environment—A review. Int. J. Pharm. 2014, 473, 64–72. [Google Scholar] [CrossRef] [Green Version]
- Mimura, K.; Kanada, K.; Uchida, S.; Yamada, M.; Namiki, N. Formulation Study for Orally Disintegrating Tablet Using Partly Pregelatinized Starch Binder. Chem. Pharm. Bull. 2011, 59, 959–964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Desai, P.M.; Liew, C.V.; Heng, P.W.S. Review of Disintegrants and the Disintegration Phenomena. J. Pharm. Sci. 2016, 105, 2545–2555. [Google Scholar] [CrossRef] [Green Version]
- Morin, G.; Briens, L. A Comparison of Granules Produced by High-Shear and Fluidized-Bed Granulation Methods. AAPS PharmSciTech 2014, 15, 1039–1048. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mishra, S.M.; Rohera, B.D. An integrated, quality by design (QbD) approach for design, development and optimization of orally disintegrating tablet formulation of carbamazepine. Pharm. Dev. Technol. 2017, 22, 889–903. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| QTPP Element | Target | CQAs | Justification |
|---|---|---|---|
| Dosage form | Orodispersible mini-tablets | Breaking force | Hard enough |
| Appearance and size | Uncoated mini-tablets (round, 3 mm in diameter) | Friability | <1% |
| Strength Route of administration Proposed indications | 5 mg/mini-tablet Oral Pediatric pulmonary hypertension | Disintegration time Drug release - | <60 s Not less than 80% in 30 min - |
| Run | MCC (% w/w) | PPGS (% w/w) |
|---|---|---|
| 1 | 10 | 2 |
| 2 | 10 | 6 |
| 3 | 10 | 10 |
| 4 | 25 | 2 |
| 5 | 25 | 6 |
| 6 | 25 | 10 |
| 7 | 40 | 2 |
| 8 | 40 | 6 |
| 9 | 40 | 10 |
| Ingredients | Function | % w/w | Quantity (mg) |
|---|---|---|---|
| Sildenafil citrate | Drug | 33.33 | 5 |
| Microcrystalline cellulose PH-105 | Filler | 10–40 | 1.5–6 |
| Partially pre-gelatinized starch | Binder/Disintegrant | 2–10 | 0.3–1.5 |
| D-mannitol | Filler | Up to 100 | Up to 15 |
| Sodium saccharin | Sweating agent | 1 | 0.15 |
| FDA-approved flavor | Flavor | q.s. | q.s. |
| Sodium stearyl fumarate | Hydrophilic lubricant | 1 | 0.15 |
| Total | - | 100 | 15 |
| Responses | Suggested Model | p-Value | R2 | Adjusted R2 | Predicted R2 | Adequate Precision |
|---|---|---|---|---|---|---|
| Y1:D50 | Linear | <0.0001 | 0.9094 | 0.8893 | 0.2619 | 17.396 |
| Y2: Bulk density | Linear | 0.0004 | 0.8293 | 0.7914 | 0.7442 | 14.861 |
| Y3: Angle of repose | Linear | <0.0001 | 0.8810 | 0.8545 | 0.8295 | 17.775 |
| Y4: Crushing strength | Linear | <0.0001 | 0.9802 | 0.9758 | 0.9658 | 41.670 |
| Y5: Friability | Quadratic | <0.0001 | 0.9846 | 0.9718 | 0.9362 | 26.967 |
| Y6: Disintegration time | 2FI | <0.0001 | 0.9918 | 0.9887 | 0.9716 | 50.402 |
| Y7: Percent release after 30 min | Quadratic | <0.0001 | 0.9929 | 0.9869 | 0.9381 | 39.195 |
| Formula | d50 (µm ± SD) | Bulk Density (g/mL ± SD) | Tapped Density (g/mL ± SD) | Carr’s Index % | Flow Character according to USP | Angle of Repose (Degree ± SD) |
|---|---|---|---|---|---|---|
| 1 | 106.13 ± 0.35 | 0.213 ± 0.014 | 0.251 ± 0.016 | 15.13 | Good | 33.21 ± 0.321 |
| 2 | 124.71 ± 0.32 | 0.231 ± 0.006 | 0.2626 ± 0.009 | 11.83 | Good | 31.49 ± 0.423 |
| 3 | 162.45 ± 0.21 | 0.252 ± 0.032 | 0.276 ± 0.037 | 8.69 | Excellent | 28.72 ± 0.127 |
| 4 | 111.56 ± 0.26 | 0.243 ± 0.034 | 0.281 ± 0.031 | 13.5 | Good | 32.46 ± 0.615 |
| 5 | 131.23 ± 0.21 | 0.273 ± 0.007 | 0.313 ± 0.009 | 12.77 | Good | 30.54 ± 0.247 |
| 6 | 159.58 ± 0.65 | 0.301 ± 0.033 | 0.323 ± 0.041 | 6.81 | Excellent | 27.84 ± 0.442 |
| 7 | 116.24 ± 0.24 | 0.287 ± 0.008 | 0.328 ± 0.008 | 12.5 | Good | 31.77 ± 0.361 |
| 8 | 134.85 ± 0.32 | 0.301 ± 0.047 | 0.326 ± 0.062 | 7.66 | Excellent | 28.11 ± 0.431 |
| 9 | 161.74 ± 0.45 | 0.322 ± 0.019 | 0.337 ± 0.017 | 4.45 | Excellent | 26.81 ± 0.392 |
| Variables | Coefficient Estimate | Sum of Squares | Standard Error | F-Value | p-Value | 95% CI Low | 95% CI High |
|---|---|---|---|---|---|---|---|
| Y1: D50 (Linear model) | |||||||
| Intercept | 136.95 | - | 1.87 | - | - | 132.71 | 141.18 |
| X1 | 3.26 | 63.64 | 2.65 | 1.51 | 0.2503 | −2.74 | 9.25 |
| X2 | 24.97 | 2742.00 | 2.65 | 88.81 | <0.0001 | 18.98 | 30.97 |
| Y2: Bulk density (Linear model) | |||||||
| Intercept | 0.2759 | - | 0.0045 | - | - | 0.2658 | 0.2961 |
| X1 | 0.0357 | 0.0076 | 0.0063 | 31.68 | 0.0003 | 0.0213 | 0.0500 |
| X2 | 0.0220 | 0.0029 | 0.0063 | 12.05 | 0.007 | 0.0077 | 0.0363 |
| Y3: Angle of repose (Linear model) | |||||||
| Intercept | 29.95 | - | 0.2252 | - | - | 29.44 | 30.46 |
| X1 | −1.12 | 7.55 | 0.3185 | 12.40 | 0.0065 | −1.84 | −0.4012 |
| X2 | −2.35 | 32.99 | 0.3185 | 54.22 | <0.0001 | −3.07 | −1.62 |
| Run | Weight (mg ± SD) | Drug Content (% ± SD) | Crushing Strength (KP ± SD) | Friability (% ± SD) | Disintegration Time (S ± SD) | %Release at 30 min (% ± SD) |
|---|---|---|---|---|---|---|
| 1 | 14.86 ± 1.31 | 100.32 ± 1.25 | 2.86 ± 0.61 | 1.22 ± 0.03 | 83.11 ± 1.13 | 76.49 ± 1.15 |
| 2 | 14.93 ± 1.27 | 99.13 ± 1.41 | 3.93 ± 0.14 | 0.94 ± 0.06 | 60.42 ± 1.33 | 81.24 ± 1.14 |
| 3 | 15.91 ± 1.21 | 101.33 ± 1.22 | 4.71 ± 0.61 | 0.74 ± 0.02 | 43.15 ± 1.28 | 86.24 ± 1.13 |
| 4 | 14.98 ± 1.05 | 100.66 ± 2.11 | 2.93 ± 0.33 | 1.18 ± 0.01 | 79.34 ± 1.63 | 77.11 ± 2.36 |
| 5 | 14.89 ± 1.15 | 98.89 ± 1.71 | 4.15 ± 0.28 | 0.86 ± 0.05 | 57.62 ± 1.61 | 83.47 ± 1.82 |
| 6 | 14.95 ± 1.29 | 101.56 ± 0.98 | 5.11 ± 0.71 | 0.69 ± 0.03 | 32.41 ± 1.32 | 88.35 ± 2.41 |
| 7 | 15.25 ± 0.88 | 100.88 ± 1.63 | 3.34 ± 0.31 | 1.07 ± 0.02 | 78.61 ± 2.18 | 74.63 ± 2.84 |
| 8 | 15.13 ± 0.74 | 98.76 ± 2.01 | 4.32 ± 0.39 | 0.81 ± 0.01 | 55.32 ± 0.57 | 83.52 ± 1.21 |
| 9 | 15.23 ± 0.48 | 100.93 ± 0.76 | 5.31 ± 0.26 | 0.65 ± 0.03 | 30.17 ± 0.81 | 89.31 ± 2.17 |
| Variables | Coefficient Estimate | Sum of Squares | Standard Error | F-Value | p-Value | 95% CI low | 95% CI High |
|---|---|---|---|---|---|---|---|
| Y4:Crushing strength (Linear model) | |||||||
| Intercept | 4.11 | - | 0.0345 | - | - | 4.03 | 4.19 |
| X1 | 0.245 | 0.3601 | 0.0488 | 25.22 | 0.0007 | 0.1346 | 0.3554 |
| X2 | 1.00 | 6.00 | 0.0488 | 420.10 | <0.0001 | 0.8896 | 1.11 |
| Y5:Friability (Quadratic model) | |||||||
| Intercept | 0.8462 | - | 0.0140 | - | - | 0.8119 | 0.8806 |
| X1 | −0.0617 | 0.0228 | 0.0126 | 24.11 | 0.0027 | −0.0924 | −0.0309 |
| X2 | −0.2317 | 0.3220 | 0.0154 | 340.21 | <0.0001 | −0.2624 | −0.2009 |
| X1 X2 | 0.0115 | 0.0009 | 0.0188 | 0.9508 | 0.3672 | −0.0226 | −0.0526 |
| Y6:Disintegration time (2FI model) | |||||||
| Intercept | 57.71 | - | 0.5222 | - | - | 56.50 | 58.91 |
| X1 | −3.76 | 84.98 | 0.7384 | 25.97 | 0.0009 | −5.47 | −2.06 |
| X2 | −22.56 | 3052.37 | 0.7384 | 932.92 | <0.0001 | −24.26 | −20.85 |
| X1 X2 | −2.12 | 17.98 | 0.9044 | 5.49 | 0.0471 | −4.21 | −0.0344 |
| Y7:Percent release at 30 min (Quadratic model) | |||||||
| Intercept | 83.14 | - | 0.2364 | - | - | 82.56 | 83.72 |
| X1 | 0.5817 | 2.03 | 0.2114 | 7.57 | 0.0333 | 0.0643 | 1.10 |
| X2 | 5.94 | 212.06 | 0.2114 | 790.49 | <0.0001 | 5.43 | 6.46 |
| X1 X2 | 1.23 | 6.08 | 0.2590 | 22.65 | 0.0031 | 0.5988 | 1.87 |
| Response | F-Value | p-Value | Comment |
|---|---|---|---|
| d50 | 0.7929 | 0.6313 | Not significant |
| Bulk density | 0.9518 | 0.5638 | Not significant |
| Flowability | 0.1755 | 0.9656 | Not significant |
| Crushing strength | 1.77 | 0.3419 | Not significant |
| Friability | 0.7341 | 0.5972 | Not significant |
| Disintegration time | 1.39 | 0.4180 | Not significant |
| Percent release after 30 min | 4.99 | 0.1098 | Not significant |
| Variables | Target | Range | Weight | Importance Co-Efficient |
|---|---|---|---|---|
| Input | ||||
| MCC | In range | 10–40% w/w | 1 | NA |
| PPGS | In range | 2–10% w/w | 1 | NA |
| Output | ||||
| Crushing strength (KP) | 5 | 2.86–5.31 | +++++ | |
| Friability (%) | 0.65 | 0.65–1.22 | 1 | +++ |
| Disintegration time (s) | 35 | 30.17–83.11 | 1 | +++++ |
| Percent release after 30 min (%) | 85 | 74.63–89.31 | 1 | +++ |
| Variables | Value | ||
|---|---|---|---|
| MCC (% w/w) | 10 | ||
| PPGS (% w/w) | 10 | ||
| Overall desirability = 0.872 | |||
| Responses | Predicted values | Experimental values * | Prediction error (%) |
| Crushing strength (KP) | 4.86 | 4.72 ± 0.34 | 2.88 |
| Friability (%) | 0.74 | 0.71 ± 0.04 | 4.22 |
| Disintegration time (s) | 41.03 | 39.11 ± 1.03 | 4.67 |
| Percent release after 30 min (%) | 85.85 | 86.21 ± 2.41 | −4.88 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alalaiwe, A.; Alsenaidy, M.A.; Almalki, Z.S.; Fayed, M.H. Development and Optimization of Sildenafil Orodispersible Mini-Tablets (ODMTs) for Treatment of Pediatric Pulmonary Hypertension Using Response Surface Methodology. Pharmaceutics 2023, 15, 923. https://doi.org/10.3390/pharmaceutics15030923
Alalaiwe A, Alsenaidy MA, Almalki ZS, Fayed MH. Development and Optimization of Sildenafil Orodispersible Mini-Tablets (ODMTs) for Treatment of Pediatric Pulmonary Hypertension Using Response Surface Methodology. Pharmaceutics. 2023; 15(3):923. https://doi.org/10.3390/pharmaceutics15030923
Chicago/Turabian StyleAlalaiwe, Ahmed, Mohammad A. Alsenaidy, Ziyad S. Almalki, and Mohamed H. Fayed. 2023. "Development and Optimization of Sildenafil Orodispersible Mini-Tablets (ODMTs) for Treatment of Pediatric Pulmonary Hypertension Using Response Surface Methodology" Pharmaceutics 15, no. 3: 923. https://doi.org/10.3390/pharmaceutics15030923