

Radiolabeled Risperidone microSPECT/CT Imaging for Intranasal Implant Studies Development
 , ,
, ,  and
and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Risperidone Radiolabelling
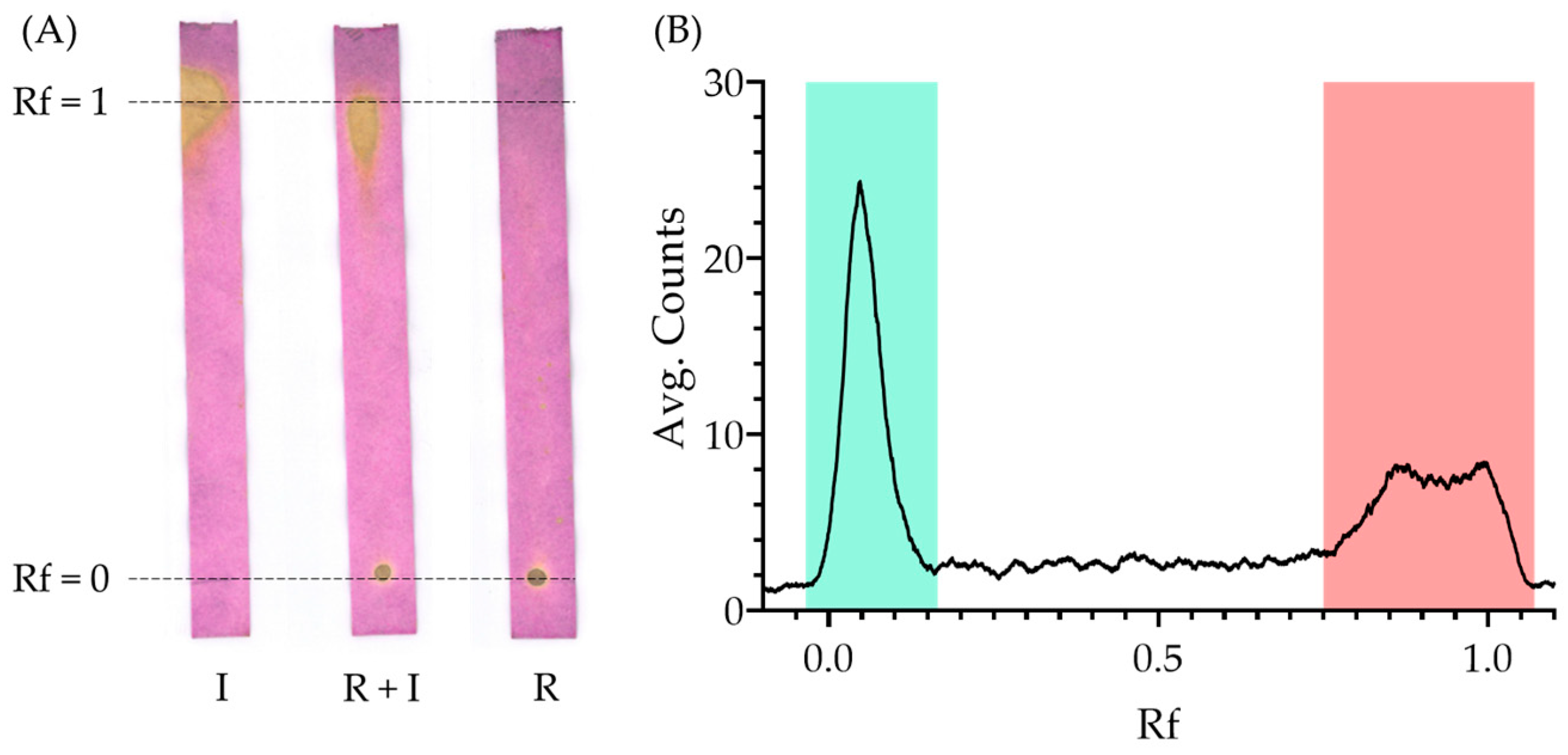
2.2. Quality Control
2.3. 125I-Risperidone Extraction and Purification
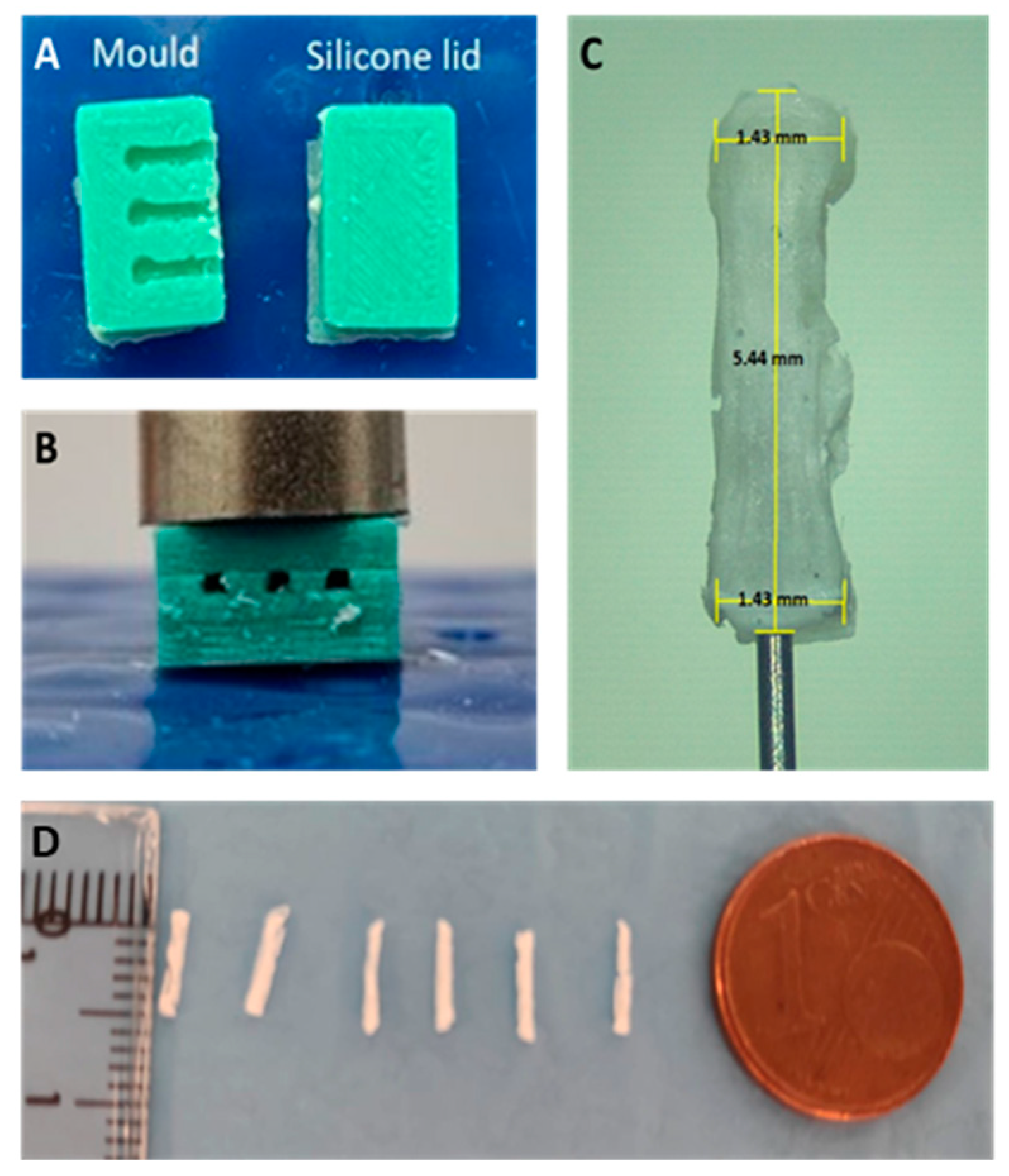
2.4. Preparation of Microimplants Containing 125I-RISP or [125I]INa
2.5. In Vitro Release Studies
2.6. Animal Studies
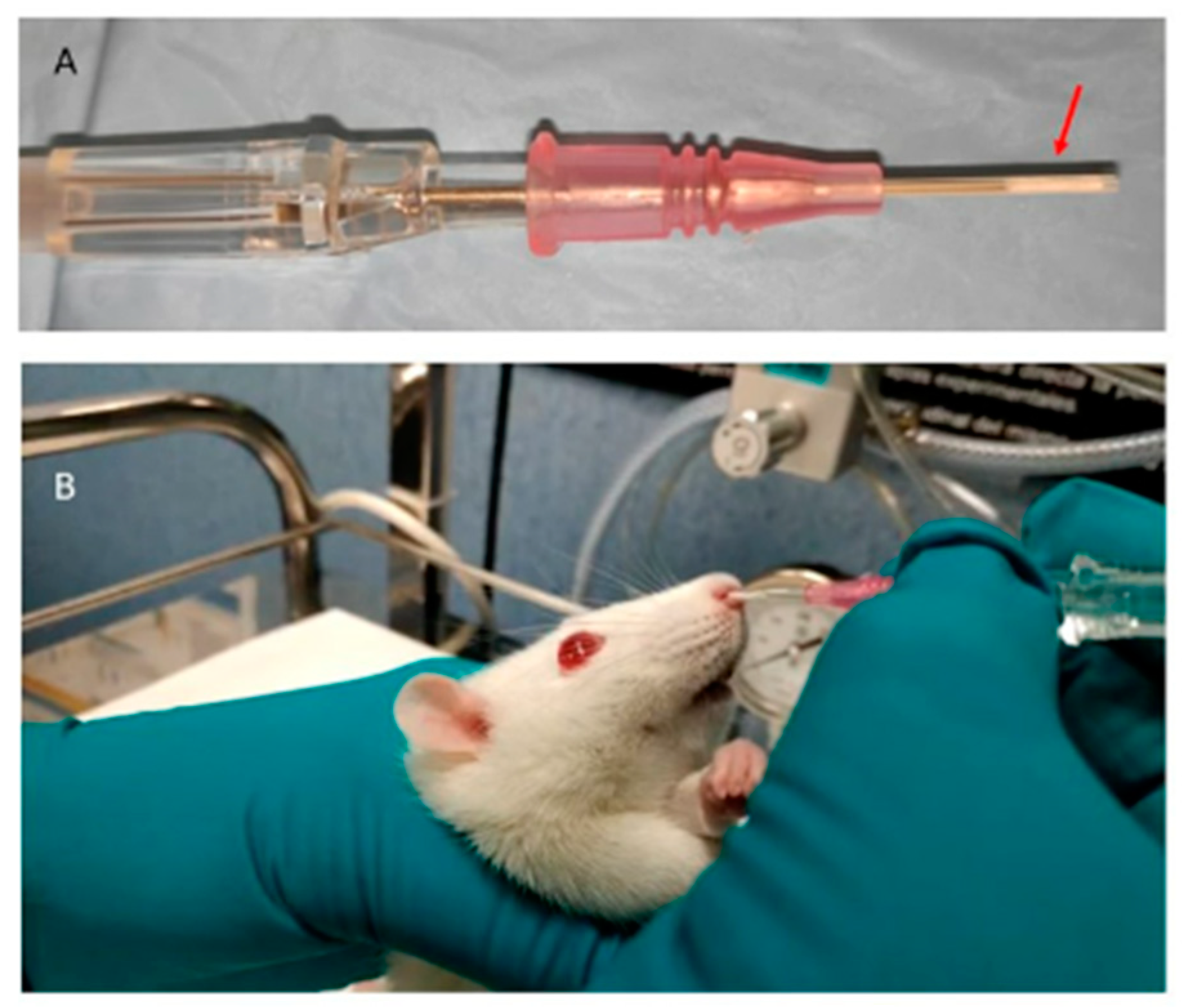
2.7. Microimplant Intranasal Administration and In Vivo Release Studies
3. Results and Discussion
3.1. Reaction Optimization and Radiolabelling Yield
3.2. Quality Control Validation
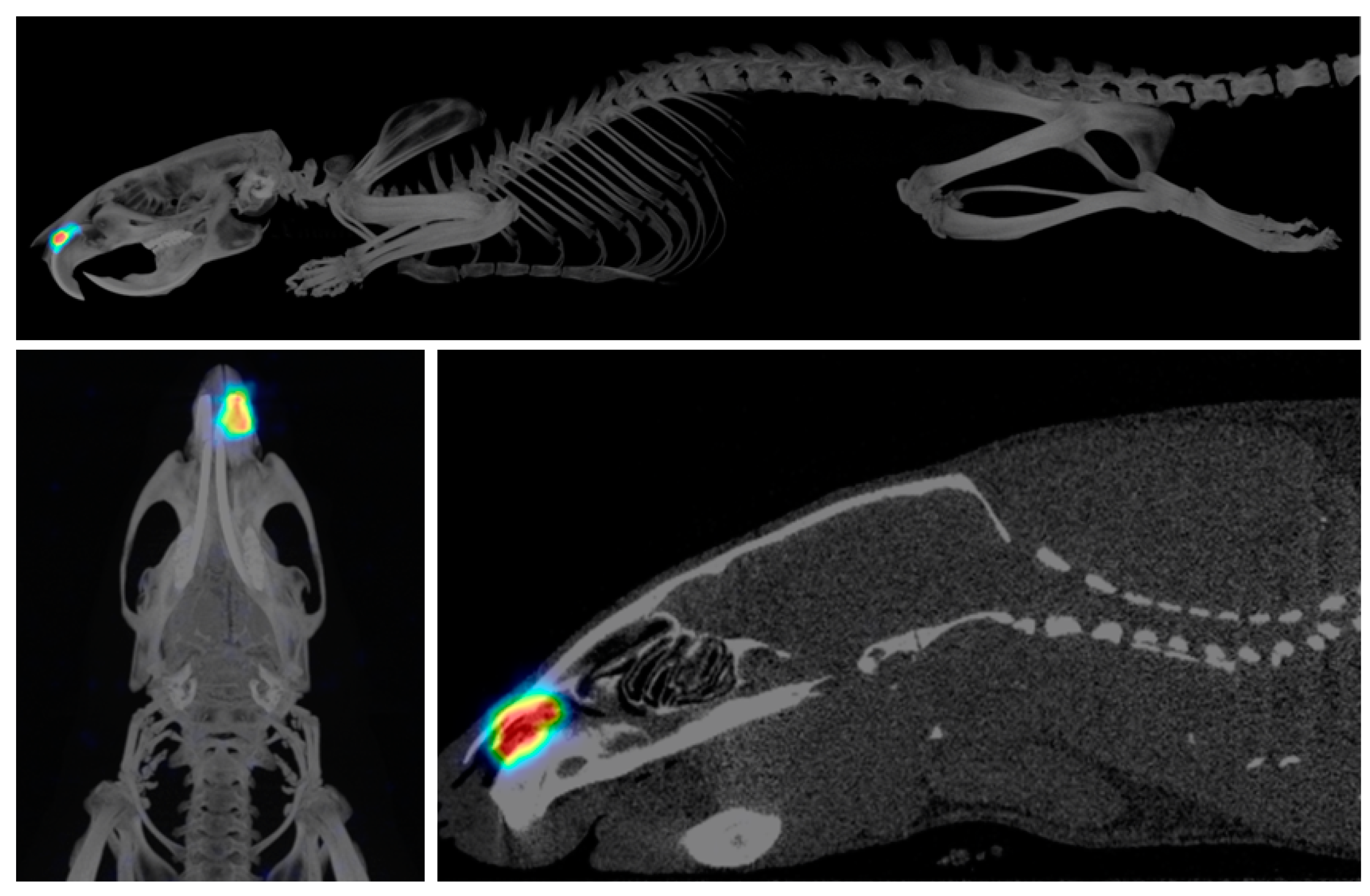
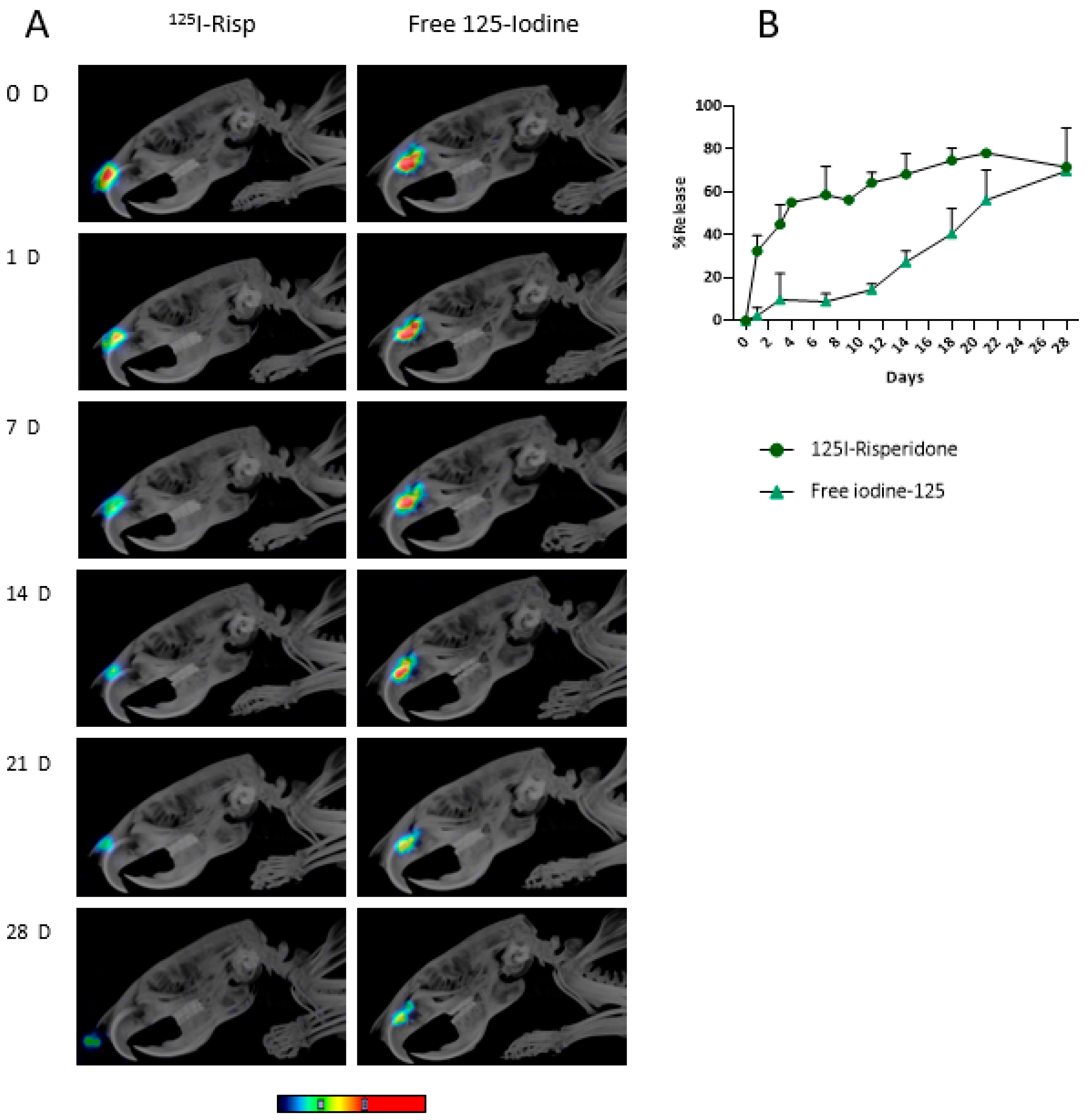
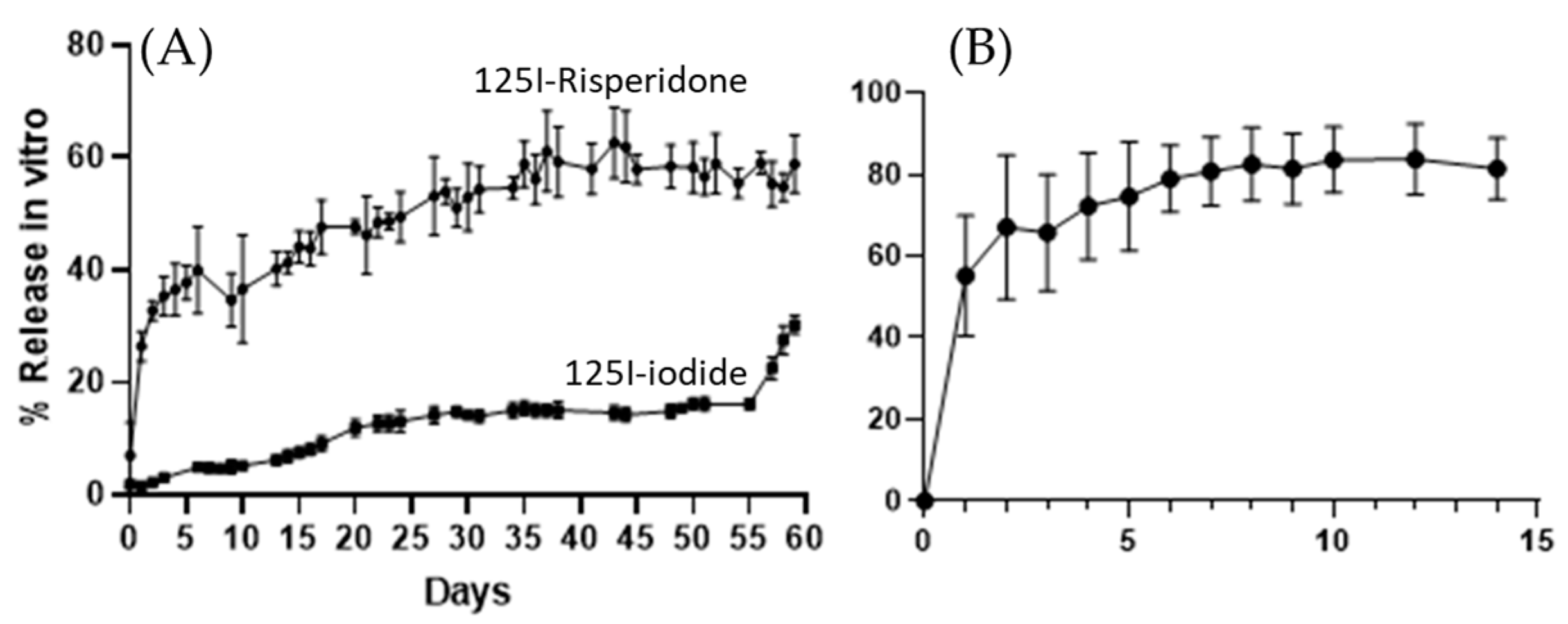
3.3. In Vivo and In Vitro Release Studies
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Quarterman, J.C.; Geary, S.M.; Salem, A.K. Evolution of drug-eluting biomedical implants for sustained drug delivery. Eur. J. Pharm. Biopharm. 2021, 159, 21–35. [Google Scholar] [CrossRef]
- Stewart, A.S.; Domínguez-Robles, J.; Donnelly, R.F.; Larrañeta, E. Implantable polymeric drug delivery devices: Classification, manufacture, materials, and clinical applications. Polymers 2018, 10, 1379. [Google Scholar] [CrossRef] [Green Version]
- Li, W.; Tang, J.; Lee, D.; Tice, T.R.; Schwendeman, S.P.; Prausnitz, M.R. Clinical translation of long-acting drug delivery formulations. Nat. Rev. Mater. 2022, 7, 406–420. [Google Scholar] [CrossRef]
- Chappel, E. Implantable drug delivery devices. In Drug Delivery Devices and Therapeutic Systems; Elsevier: Amsterdam, The Netherlands, 2021; pp. 129–156. [Google Scholar]
- Korelidou, A.; Domínguez-Robles, J.; Magill, E.; Eleftheriadou, M.; Cornelius, V.A.; Donnelly, R.F.; Margariti, A.; Larrañeta, E. 3D-printed reservoir-type implants containing poly(lactic acid)/poly(caprolactone) porous membranes for sustained drug delivery. Biomater. Adv. 2022, 139, 213024. [Google Scholar] [CrossRef]
- Stewart, S.A.; Domínguez-Robles, J.; McIlorum, V.J.; Gonzalez, Z.; Utomo, E.; Mancuso, E.; Lamprou, D.A.; Donnelly, R.F.; Larrañeta, E. Poly(caprolactone)-based coatings on 3d-printed biodegradable implants: A novel strategy to prolong delivery of hydrophilic drugs. Mol. Pharm. 2020, 17, 3487–3500. [Google Scholar] [CrossRef]
- Kumar, A.; Pillai, J. Implantable drug delivery systems. In Nanostructures for the Engineering of Cells, Tissues and Organs; Elsevier: Amsterdam, The Netherlands, 2018; pp. 473–511. [Google Scholar]
- Abdelkader, H.; Fathalla, Z.; Seyfoddin, A.; Farahani, M.; Thrimawithana, T.; Allahham, A.; Alani, A.W.G.; Al-Kinani, A.A.; Alany, R.G. Polymeric long-acting drug delivery systems (ladds) for treatment of chronic diseases: Inserts, patches, wafers, and implants. Adv. Drug Deliv. Rev. 2021, 177, 113957. [Google Scholar] [CrossRef]
- Picco, C.J.; Utomo, E.; McClean, A.; Domínguez-Robles, J.; Kurnia Anjani, Q.; Volpe-Zanutto, F.; McKenna, P.E.; Acheson, J.; Malinova, D.; Donnelly, R.F.; et al. Development of 3d-printed subcutaneous implants using concentrated polymer/drug solutions. Int. J. Pharm. 2022, 631, 122477. [Google Scholar] [CrossRef]
- Simpson, S.M.; Widanapathirana, L.; Su, J.T.; Sung, S.; Watrous, D.; Qiu, J.; Pearson, E.; Evanoff, A.; Karunakaran, D.; Chacon, J.E.; et al. Design of a drug-eluting subcutaneous implant of the antiretroviral tenofovir alafenamide fumarate. Pharm. Res. 2020, 37, 83. [Google Scholar] [CrossRef]
- Stewart, S.A.; Domínguez-Robles, J.; Utomo, E.; Picco, C.J.; Corduas, F.; Mancuso, E.; Amir, M.N.; Bahar, M.A.; Sumarheni, S.; Donnelly, R.F.; et al. Poly(caprolactone)-based subcutaneous implant for sustained delivery of levothyroxine. Int. J. Pharm. 2021, 607, 121011. [Google Scholar] [CrossRef]
- Maturavongsadit, P.; Paravyan, G.; Kovarova, M.; Garcia, J.V.; Benhabbour, S.R. A New Engineering process of biodegradable polymeric solid implants for ultra-long-acting drug delivery. Int. J. Pharm. X 2021, 3, 100068. [Google Scholar] [CrossRef]
- Lee, S.H.; Wan, Q.; Wentworth, A.; Ballinger, I.; Ishida, K.; Collins, J.E.; Tamang, S.; Huang, H.-W.; Li, C.; Hess, K.; et al. Implantable system for chronotherapy. Sci. Adv. 2021, 7, eabj4624. [Google Scholar] [CrossRef]
- Myung, N.; Jin, S.; Cho, H.J.; Kang, H.-W. User-designed device with programmable release profile for localized treatment. J. Control. Release 2022, 352, 685–699. [Google Scholar] [CrossRef]
- Lee, D.-H.; Torre Hernandez, J.M. de la The newest generation of drug-eluting stents and beyond. Eur. Cardiol. Rev. 2018, 13, 54. [Google Scholar] [CrossRef]
- Domínguez-Robles, J.; Shen, T.; Cornelius, V.A.; Corduas, F.; Mancuso, E.; Donnelly, R.F.; Margariti, A.; Lamprou, D.A.; Larrañeta, E. Development of drug loaded cardiovascular prosthesis for thrombosis prevention using 3D printing. Mater. Sci. Eng. C 2021, 129, 112375. [Google Scholar] [CrossRef]
- Spadaccio, C.; Chello, M.; Trombetta, M.; Rainer, A.; Toyoda, Y.; Genovese, J.A. Drug releasing systems in cardiovascular tissue engineering. J. Cell. Mol. Med. 2009, 13, 422–439. [Google Scholar] [CrossRef]
- Khalaj, R.; Tabriz, A.G.; Okereke, M.I.; Douroumis, D. 3D printing advances in the development of stents. Int. J. Pharm. 2021, 609, 121153. [Google Scholar] [CrossRef]
- Huang, C.; Lan, Y.; Chen, S.; Liu, Q.; Luo, X.; Xu, G.; Zhou, W.; Lin, F.; Peng, Y.; Ng, E.Y.K.; et al. Patient-specific coronary artery 3d printing based on intravascular optical coherence tomography and coronary angiography. Complexity 2019, 2019, 5712594. [Google Scholar] [CrossRef] [Green Version]
- Bakola, V.; Karagkiozaki, V.; Tsiapla, A.R.; Pappa, F.; Moutsios, I.; Pavlidou, E.; Logothetidis, S. Dipyridamole-loaded biodegradable pla nanoplatforms as coatings for cardiovascular stents. Nanotechnology 2018, 29, 275101. [Google Scholar] [CrossRef] [Green Version]
- Martin, N.K.; Domínguez-Robles, J.; Stewart, S.A.; Cornelius, V.A.; Anjani, Q.K.; Utomo, E.; García-Romero, I.; Donnelly, R.F.; Margariti, A.; Lamprou, D.A.; et al. Fused deposition modelling for the development of drug loaded cardiovascular prosthesis. Int. J. Pharm. 2021, 595, 120243. [Google Scholar] [CrossRef]
- Suhardi, V.J.; Bichara, D.A.; Kwok, S.J.J.; Freiberg, A.A.; Rubash, H.; Malchau, H.; Yun, S.H.; Muratoglu, O.K.; Oral, E. A Fully functional drug-eluting joint implant. Nat. Biomed. Eng. 2017, 1, 0080. [Google Scholar] [CrossRef] [Green Version]
- Ma, X.; Gao, Y.; Zhao, D.; Zhang, W.; Zhao, W.; Wu, M.; Cui, Y.; Li, Q.; Zhang, Z.; Ma, C. Titanium implants and local drug delivery systems become mutual promoters in orthopedic clinics. Nanomaterials 2021, 12, 47. [Google Scholar] [CrossRef]
- Parikh, A.; Anand, U.; Ugwu, M.C.; Feridooni, T.; Massoud, E.; Agu, R.U. Drug-eluting nasal implants: Formulation, characterization, clinical applications and challenges. Pharmaceutics 2014, 6, 249–267. [Google Scholar] [CrossRef] [Green Version]
- Keller, L.-A.; Merkel, O.; Popp, A. Intranasal Drug Delivery: Opportunities and toxicologic challenges during drug development. Drug Deliv. Transl. Res. 2022, 12, 735–757. [Google Scholar] [CrossRef]
- Utomo, E.; Domínguez-Robles, J.; Moreno-Castellanos, N.; Stewart, S.A.; Picco, C.J.; Anjani, Q.K.; Simón, J.A.; Peñuelas, I.; Donnelly, R.F.; Larrañeta, E. Development of intranasal implantable devices for schizophrenia treatment. Int. J. Pharm. 2022, 624, 122061. [Google Scholar] [CrossRef]
- Formica, M.L.; Real, D.A.; Picchio, M.L.; Catlin, E.; Donnelly, R.F.; Paredes, A.J. On a highway to the brain: A review on nose-to-brain drug delivery using nanoparticles. Appl. Mater. Today 2022, 29, 101631. [Google Scholar] [CrossRef]
- Aderibigbe, B. In situ-based gels for nose to brain delivery for the treatment of neurological diseases. Pharmaceutics 2018, 10, 40. [Google Scholar] [CrossRef] [Green Version]
- Agrawal, M.; Saraf, S.; Saraf, S.; Dubey, S.K.; Puri, A.; Gupta, U.; Kesharwani, P.; Ravichandiran, V.; Kumar, P.; Naidu, V.G.M.; et al. Stimuli-responsive in situ gelling system for nose-to-brain drug delivery. J. Control. Release 2020, 327, 235–265. [Google Scholar] [CrossRef]
- Saddar, E.; El-Tawoosy, M.; Motaleb, H.A. Preparation and biological evaluation of radioiodinated risperidone and lamotrigine as models for brain imaging agents. J. Radioanal. Nucl. Chem. 2014, 301, 189–196. [Google Scholar] [CrossRef]
- Yuan, G.; Shoup, T.M.; Moon, S.-H.; Brownell, A.-L. A concise method for fully automated radiosyntheses of [ 18 F]jnj-46356479 and [ 18 F]fitm via cu-mediated 18 F-fluorination of organoboranes. RSC Adv. 2020, 10, 25223–25227. [Google Scholar] [CrossRef]
- Prieto, E.; Irazola, L.; Collantes, M.; Ecay, M.; Cuenca, T.; Martí-Climent, J.M.; Peñuelas, I. Performance evaluation of a preclinical SPECT/CT system for multi-animal and multi-isotope quantitative experiments. Sci. Rep. 2022, 12, 18161. [Google Scholar] [CrossRef]
- Patel, S.; Chavhan, S.; Soni, H.; Babbar, A.K.; Mathur, R.; Mishra, A.K.; Sawant, K. Brain targeting of risperidone-loaded solid lipid nanoparticles by intranasal route. J. Drug Target. 2011, 19, 468–474. [Google Scholar] [CrossRef]
- Kumar, M.; Misra, A.; Babbar, A.K.; Mishra, A.K.; Mishra, P.; Pathak, K. Intranasal nanoemulsion based brain targeting drug delivery system of risperidone. Int. J. Pharm. 2008, 358, 285–291. [Google Scholar] [CrossRef]
- Rukmangathen, R.; Yallamalli, I.M.; Yalavarthi, P.R. Formulation and biopharmaceutical evaluation of risperidone-loaded chitosan nanoparticles for intranasal delivery. Drug Dev. Ind. Pharm. 2019, 45, 1342–1350. [Google Scholar] [CrossRef]
- Goshtasbi, K.; Abouzari, M.; Abiri, A.; Yasaka, T.; Sahyouni, R.; Bitner, B.; Tajudeen, B.A.; Kuan, E.C. Efficacy of steroid-eluting stents in management of chronic rhinosinusitis after endoscopic sinus surgery: Updated meta-analysis. Int. Forum Allergy Rhinol. 2019, 9, 1443–1450. [Google Scholar] [CrossRef]
- Gadkaree, S.K.; Rathi, V.K.; Scangas, G.A.; Naunheim, M.R.; Metson, R. Use of corticosteroid-eluting sinus stents between 2012 and 2017. JAMA Otolaryngol. Neck Surg. 2019, 145, 90. [Google Scholar] [CrossRef]
- Wang, C.; Yu, L.; Chu, X.; Wang, K.; Li, J.; Lai, Y.; Meng, C.; Wen, W.; Zhu, D.; Zhang, Y.; et al. Short-term postoperative efficacy of steroid-eluting stents for eosinophilic chronic rhinosinusitis with nasal polyps: A randomized clinical trial. Int. Forum Allergy Rhinol. 2022. [Google Scholar] [CrossRef]
- Huang, Z.; Zhou, B.; Wang, D.; Zang, H.; Zhang, H.; Wang, H.; Wang, S.; Cheng, L.; Li, J.; Wu, W.; et al. Comparison of bioabsorbable steroid-eluting sinus stents versus nasopore after endoscopic sinus surgery: A multicenter, randomized, controlled, single-blinded clinical trial. Ear Nose Throat J. 2022, 101, 260–267. [Google Scholar] [CrossRef]
- Larrañeta, E.; Raghu Raj Singh, T.; Donnelly, R.F. Overview of the clinical current needs and potential applications for long-acting and implantable delivery systems. In Long-Acting Drug Delivery Systems; Elsevier: Amsterdam, The Netherlands, 2022; pp. 1–16. [Google Scholar]
- Liaskoni, A.; Wildman, R.D.; Roberts, C.J. 3D printed polymeric drug-eluting implants. Int. J. Pharm. 2021, 597, 120330. [Google Scholar] [CrossRef]
- Kar, A.; Ahamad, N.; Dewani, M.; Awasthi, L.; Patil, R.; Banerjee, R. Wearable and implantable devices for drug delivery: Applications and challenges. Biomaterials 2022, 283, 121435. [Google Scholar] [CrossRef]
- Pons-Faudoa, F.P.; Ballerini, A.; Sakamoto, J.; Grattoni, A. Advanced implantable drug delivery technologies: Transforming the clinical landscape of therapeutics for chronic diseases. Biomed. Microdevices 2019, 21, 47. [Google Scholar] [CrossRef]
- Higashi, K.; Medic, G.; Littlewood, K.J.; Diez, T.; Granstrom, O.; De Hert, M. Medication adherence in schizophrenia: Factors influencing adherence and consequences of nonadherence, a systematic literature review. Ther. Adv. Psychopharmacol. 2013, 3, 200–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haddad, P.M.; Brain, C.; Scott, J. Nonadherence with antipsychotic medication in schizophrenia: Challenges and management strategies. Patient Relat. Outcome Meas. 2014, 5, 43–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warriach, Z.I.; Sanchez-Gonzalez, M.A.; Ferrer, G.F. Suicidal behavior and medication adherence in schizophrenic patients. Cureus 2021, 13, e12473. [Google Scholar] [CrossRef]
- Moges, S.; Belete, T.; Mekonen, T.; Menberu, M. Lifetime relapse and its associated factors among people with schizophrenia spectrum disorders who are on follow up at comprehensive specialized hospitals in amhara region, ethiopia: A cross-sectional study. Int. J. Ment. Health Syst. 2021, 15, 42. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Keenan, A.; Daskiran, M.; Mathews, M.; Nuamah, I.; Orman, C.; Joshi, K.; Singh, A.; Godet, A.; Pungor, K.; et al. Relapse and treatment adherence in patients with schizophrenia switching from paliperidone palmitate once-monthly to three-monthly formulation: A retrospective health claims database analysis. Patient Prefer. Adherence 2021, 15, 2239–2248. [Google Scholar] [CrossRef]
- Fernández-Miranda, J.J.; Díaz-Fernández, S.; López-Muñoz, F. Effectiveness of more personalized, case-managed, and multicomponent treatment for patients with severe schizophrenia compared to the standard treatment: A ten-year follow-up. J. Pers. Med. 2022, 12, 1101. [Google Scholar] [CrossRef] [PubMed]
- Pennington, M.; McCrone, P. The cost of relapse in schizophrenia. Pharmacoeconomics 2017, 35, 921–936. [Google Scholar] [CrossRef] [Green Version]
- Almond, S.; Knapp, M.; Francois, C.; Toumi, M.; Brugha, T. Relapse in schizophrenia: Costs, clinical outcomes and quality of life. Br. J. Psychiatry 2004, 184, 346–351. [Google Scholar] [CrossRef] [Green Version]







Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Simón, J.A.; Utomo, E.; Pareja, F.; Collantes, M.; Quincoces, G.; Otero, A.; Ecay, M.; Domínguez-Robles, J.; Larrañeta, E.; Peñuelas, I. Radiolabeled Risperidone microSPECT/CT Imaging for Intranasal Implant Studies Development. Pharmaceutics 2023, 15, 843. https://doi.org/10.3390/pharmaceutics15030843
Simón JA, Utomo E, Pareja F, Collantes M, Quincoces G, Otero A, Ecay M, Domínguez-Robles J, Larrañeta E, Peñuelas I. Radiolabeled Risperidone microSPECT/CT Imaging for Intranasal Implant Studies Development. Pharmaceutics. 2023; 15(3):843. https://doi.org/10.3390/pharmaceutics15030843
Chicago/Turabian StyleSimón, Jon Ander, Emilia Utomo, Félix Pareja, María Collantes, Gemma Quincoces, Aarón Otero, Margarita Ecay, Juan Domínguez-Robles, Eneko Larrañeta, and Iván Peñuelas. 2023. "Radiolabeled Risperidone microSPECT/CT Imaging for Intranasal Implant Studies Development" Pharmaceutics 15, no. 3: 843. https://doi.org/10.3390/pharmaceutics15030843