
The ClC-2 Chloride Channel Activator, Lubiprostone, Improves Intestinal Barrier Function in Biopsies from Crohn’s Disease but Not Ulcerative Colitis Patients
 ,
,
Abstract
:1. Introduction
2. Results
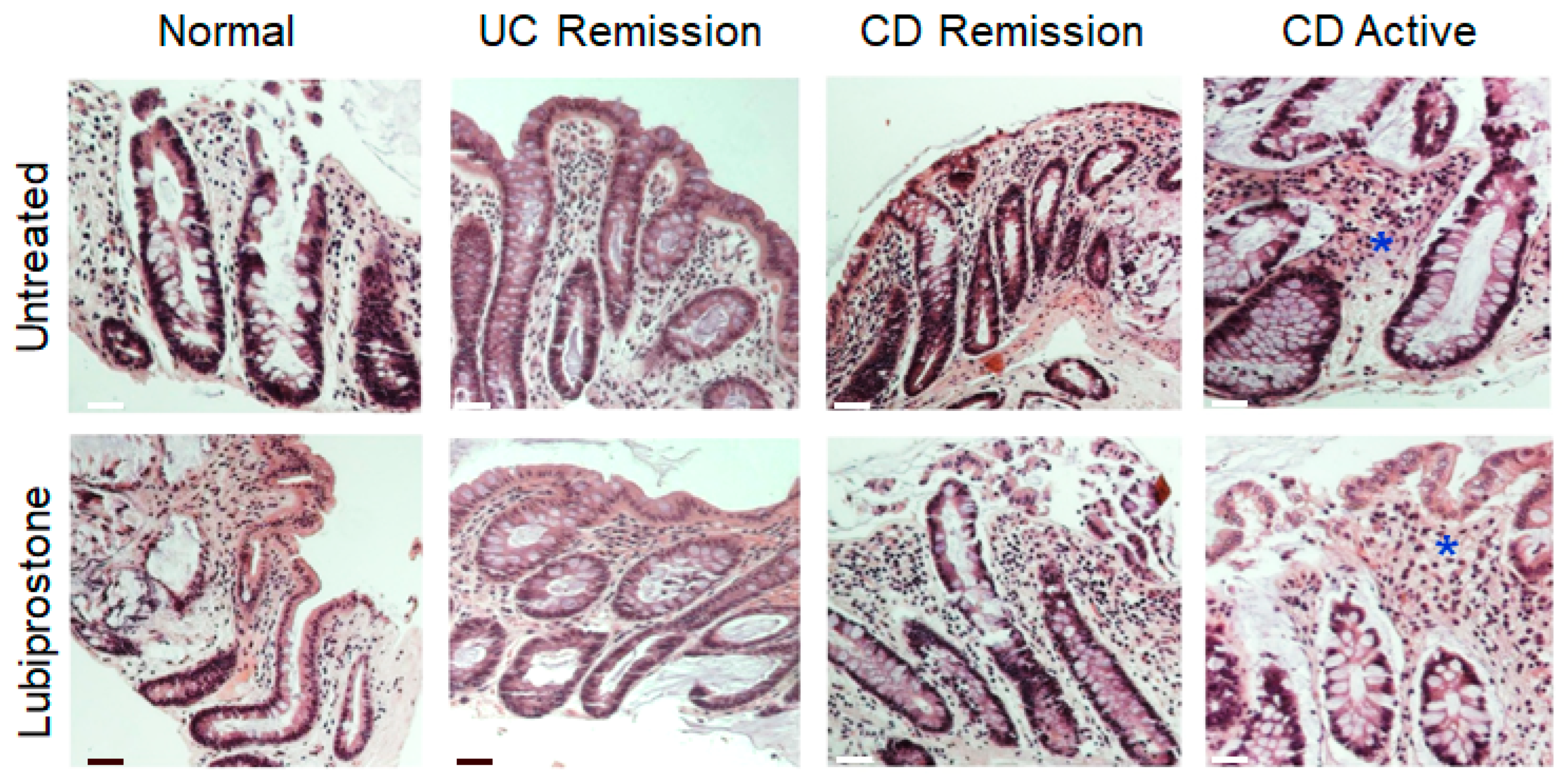
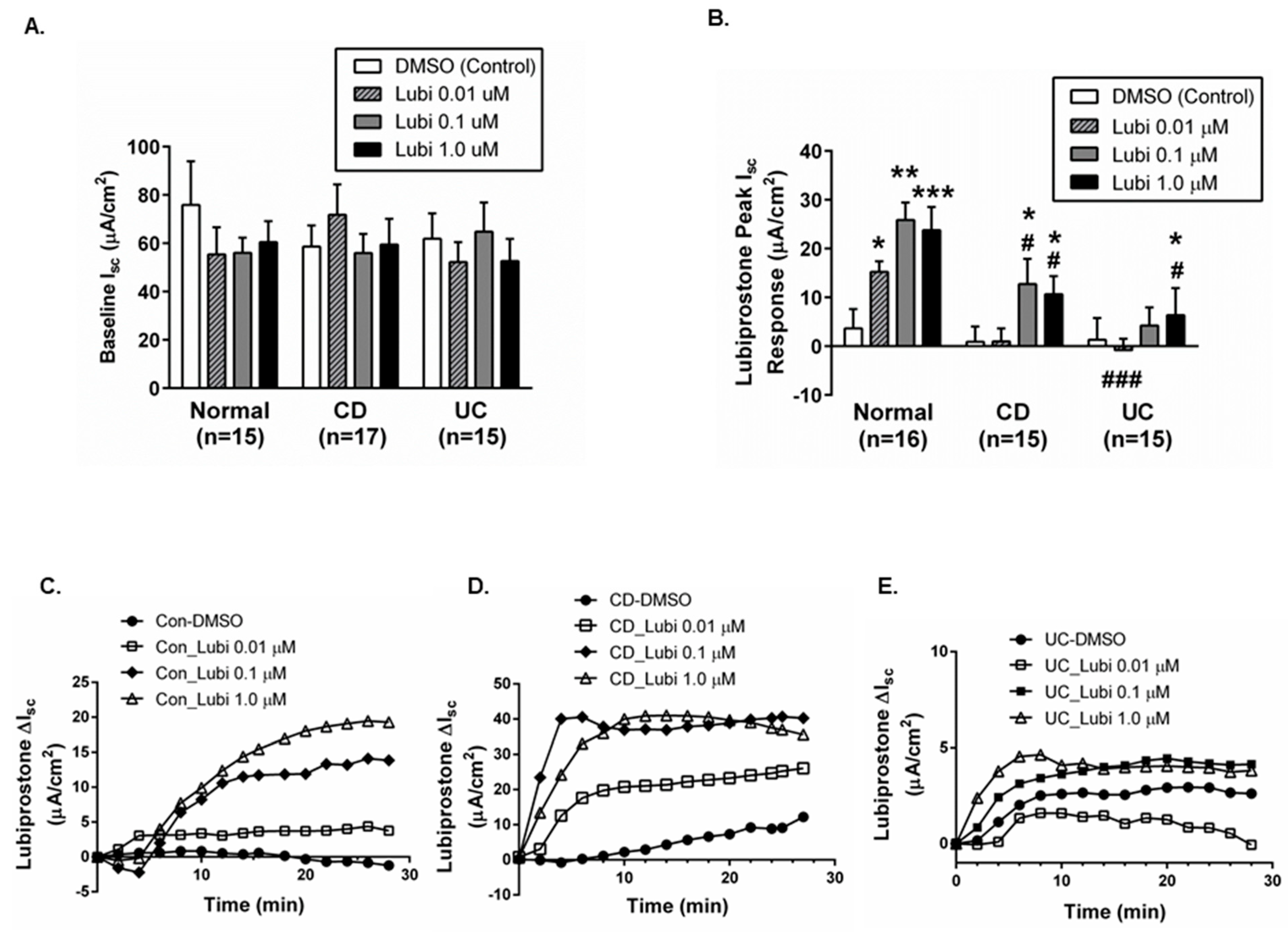
2.1. Colonic Biopsies from CD and UC Patients in Remission Have an Intact Epithelium and Display Normal Baseline Electrophysiological Parameters
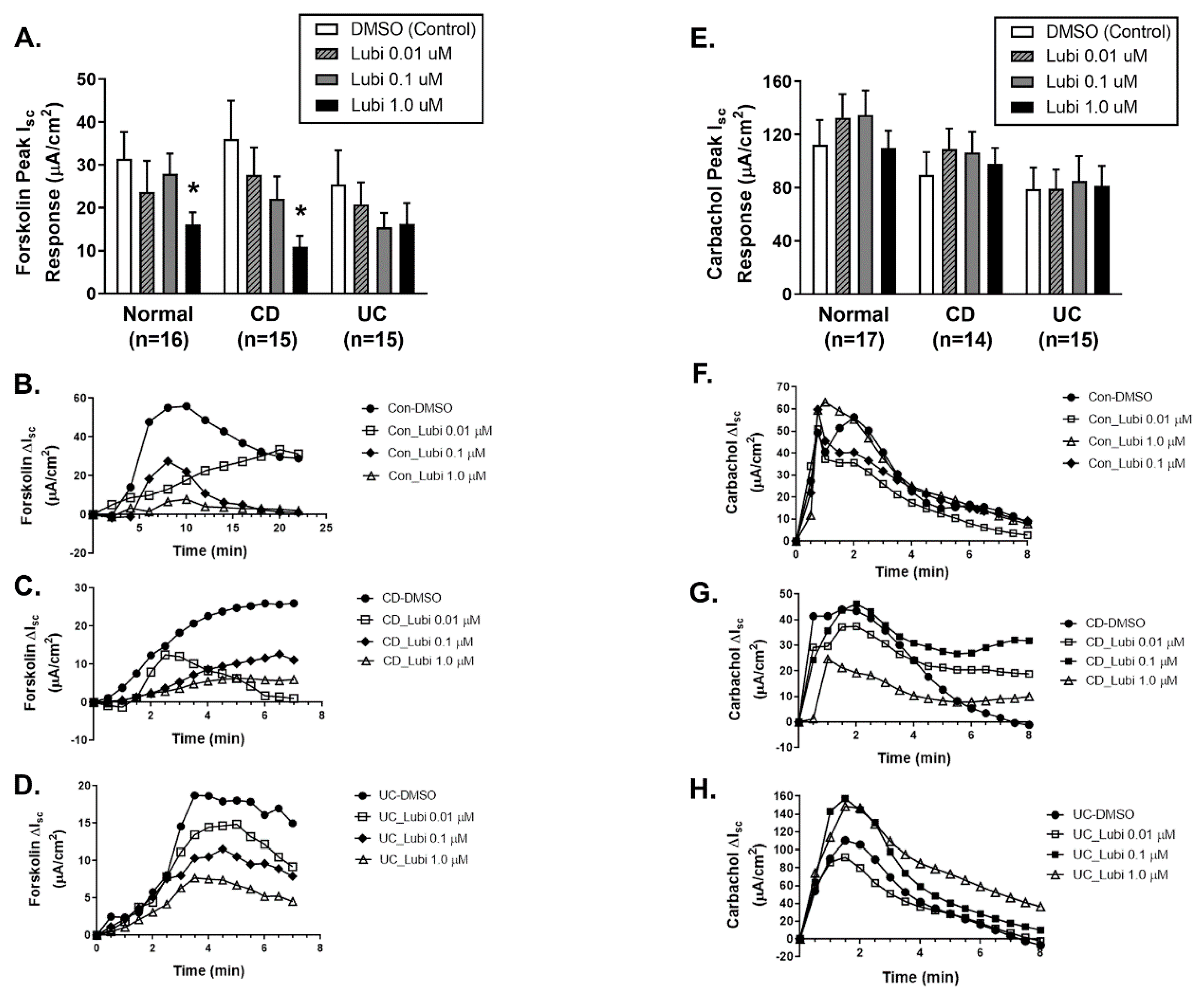
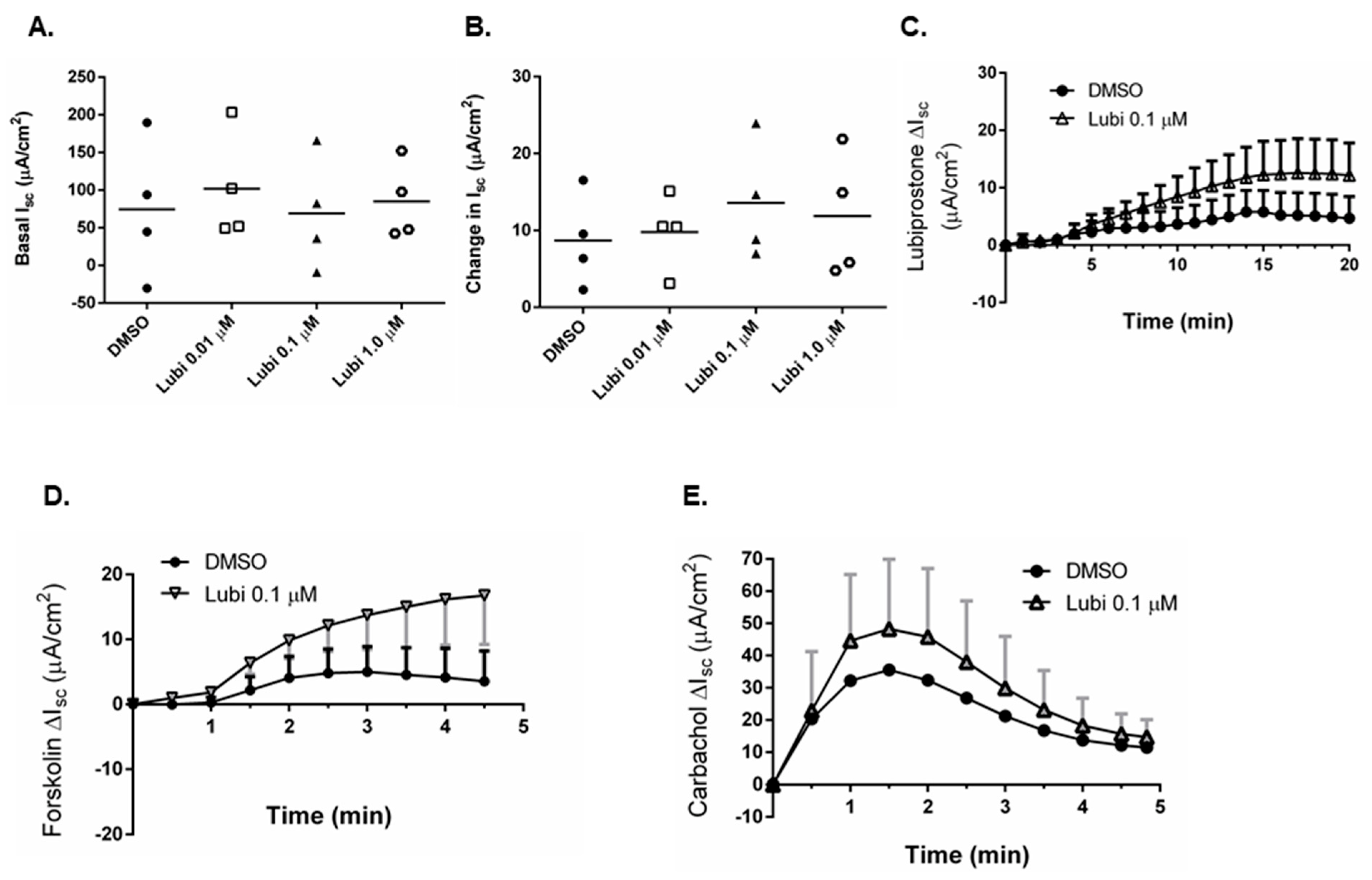
2.2. Colonic Biopsies from CD and UC Patients in Remission Show Differentially Reduced ion Transport Responsiveness to Lubiprostone
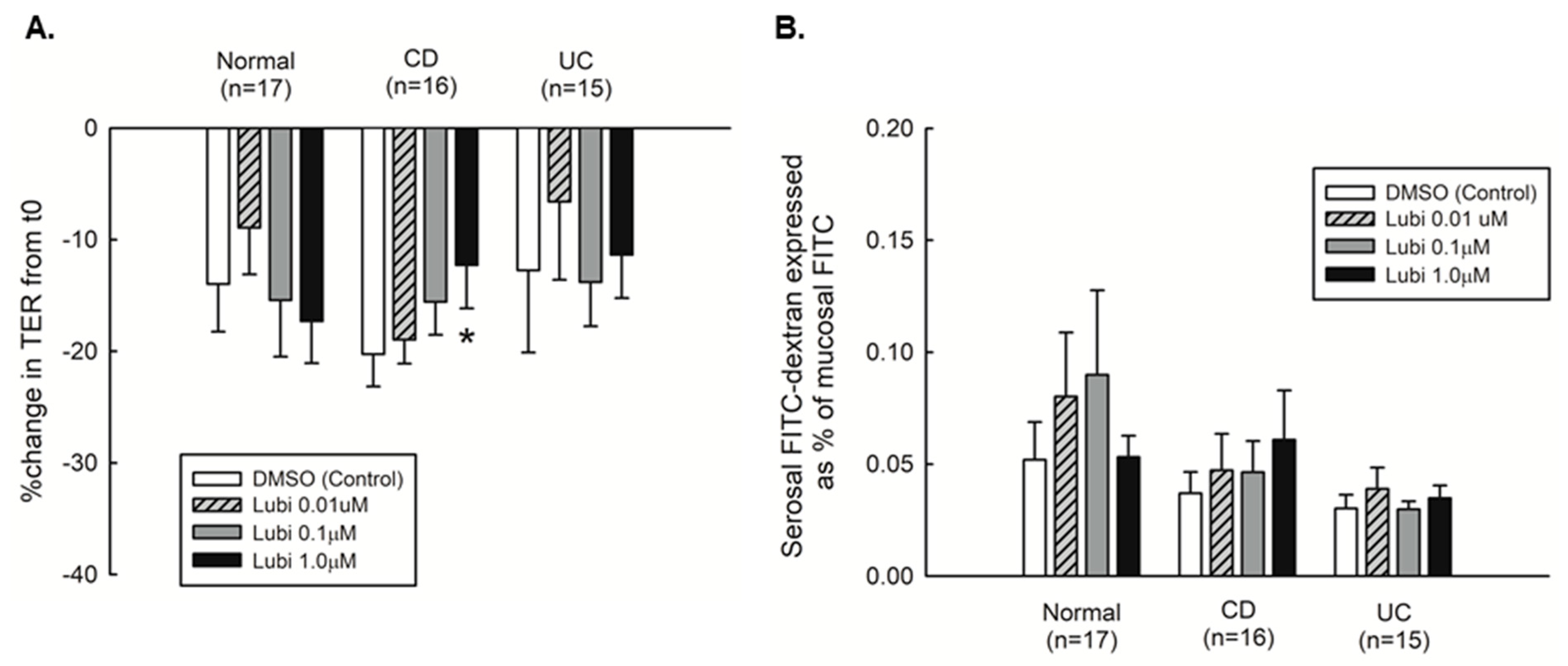
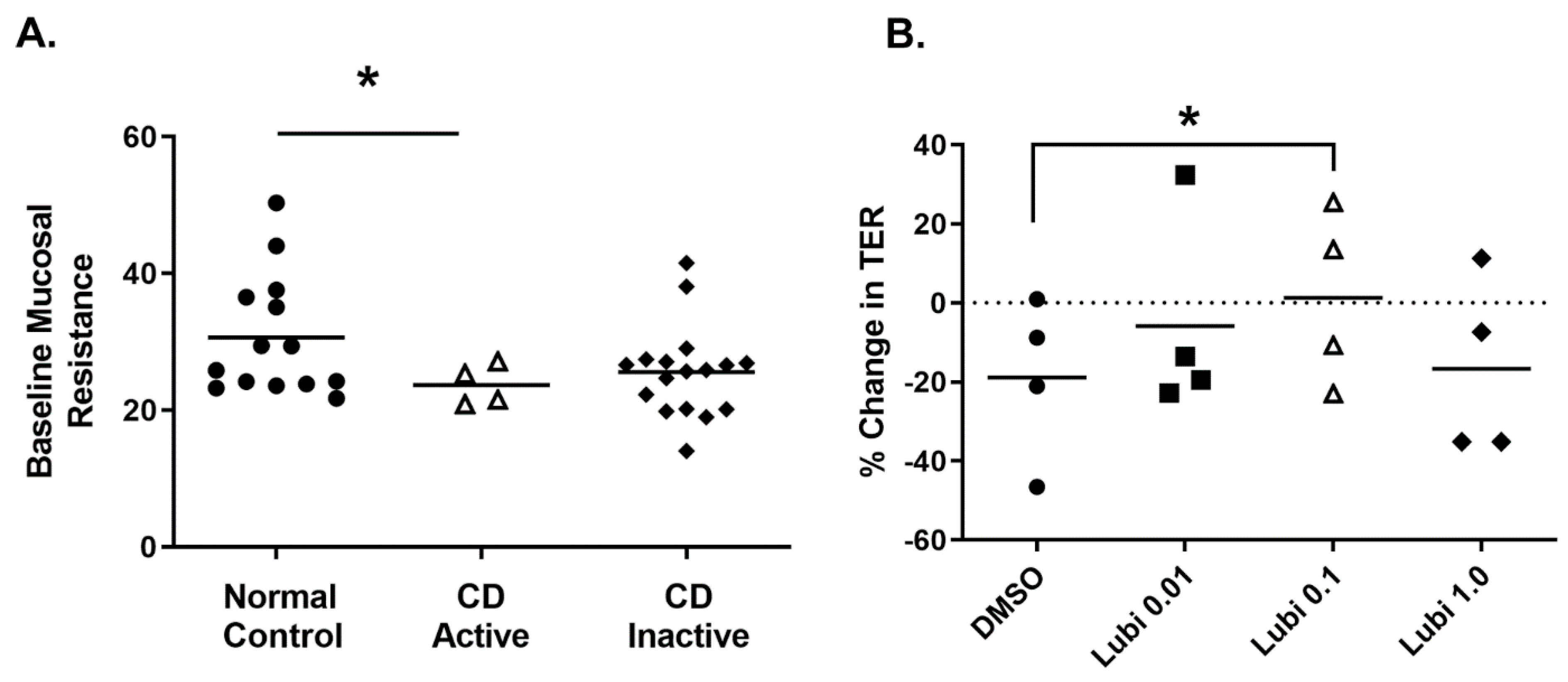
2.3. Mucosal Barrier Responsiveness to Lubiprostone in Quiescent Crohn’s Disease
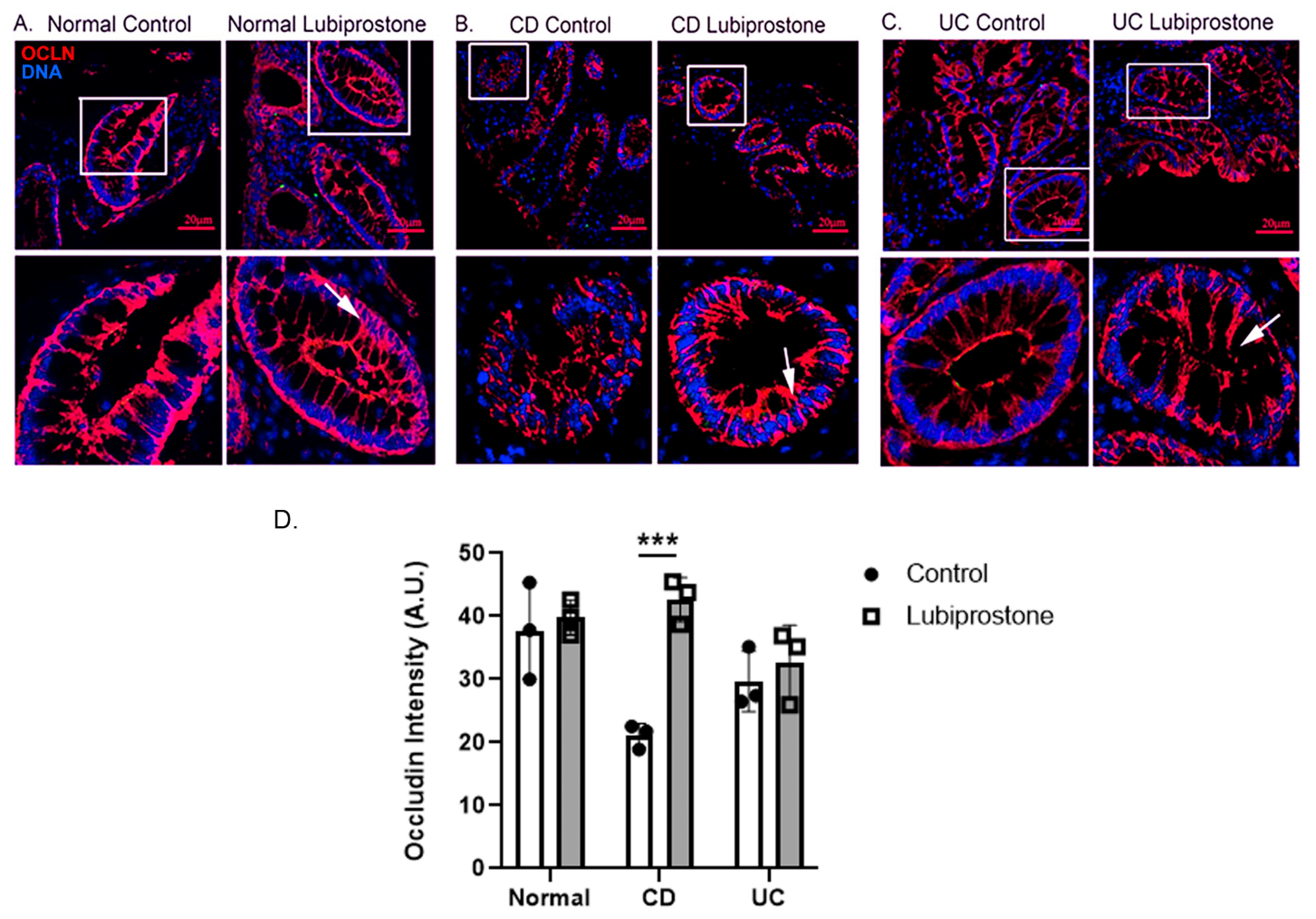
2.4. Lubiprostone Stimulates Occludin Relocalization in Colonic Biopsies from Crohn’s Disease Patients in Remission
2.5. Lubiprostone Stimulates Improved Colonic Barrier Function in Active Crohn’s Disease
2.6. Lubiprostone Effects on TER Are Independent of Ion Transport Stimulation
3. Discussion
4. Methods
4.1. Consent and Ethics Approval
4.2. Patient Criteria
4.3. Biopsy Collection
4.4. Immunohistochemical Staining
4.5. Immunofluorescence Imaging
4.6. Electrophysiological Studies of Human Colon
4.7. FITC-Dextran Permeability Measurements
4.8. Pharmacologic Challenge of Human Colonic Biopsies Ex Vivo
4.9. Data Analysis
4.10. Statistics
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CD | Crohn’s Disease |
| CFTR | Cystic Fibrosis Transmembrane conductance Regulator |
| cGMP | Cyclic Guanosine Monophosphate |
| CIC | Chronic Idiopathic Constipation |
| ClC-2 | Chloride Channel Type 2 |
| DSS | Dextran Sulfate Sodium |
| FD4 | FITC-Dextran 4kD |
| IBD | Inflammatory Bowel Disease |
| IBS-C | Constipation-Predominant Irritable Bowel Syndrome |
| IEC | Intestinal Epithelial Cell |
| Isc | Short-Circuit Current |
| TER | Transepithelial Electrical Resistance |
| UC | Ulcerative Colitis |
References
- Johanson, J.F.; Drossman, D.A.; Panas, R.; Wahle, A.; Ueno, R. Clinical trial: Phase 2 study of lubiprostone for irritable bowel syndrome with constipation. Aliment. Pharmacol. Ther. 2008, 27, 685–696. [Google Scholar] [CrossRef] [PubMed]
- Johanson, J.F.; Morton, D.; Geenen, J.; Ueno, R. Multicenter, 4-week, double-blind, randomized, placebo-controlled trial of lubiprostone, a locally-acting type-2 chloride channel activator, in patients with chronic constipation. Am. J. Gastroenterol. 2008, 103, 170–177. [Google Scholar] [CrossRef] [PubMed]
- Schey, R.; Rao, S.S. Lubiprostone for the treatment of adults with constipation and irritable bowel syndrome. Dig. Dis. Sci. 2011, 56, 1619–1625. [Google Scholar] [CrossRef] [PubMed]
- Ginzburg, R.; Ambizas, E.M. Clinical pharmacology of lubiprostone, a chloride channel activator in defecation disorders. Expert Opin. Drug. Metab. Toxicol. 2008, 4, 1091–1097. [Google Scholar] [CrossRef]
- Cuppoletti, J.; Malinowska, D.H.; Tewari, K.P.; Li, Q.J.; Sherry, A.M.; Patchen, M.L.; Ueno, R. SPI-0211 activates T84 cell chloride transport and recombinant human ClC-2 chloride currents. Am. J. Physiol. Cell Physiol. 2004, 287, C1173–C1183. [Google Scholar] [CrossRef]
- Cuppoletti, J.; Chakrabarti, J.; Tewari, K.P.; Malinowska, D.H. Differentiation between human ClC-2 and CFTR Cl- channels with pharmacological agents. Am. J. Physiol. Cell Physiol. 2014, 307, C479–C492. [Google Scholar] [CrossRef] [Green Version]
- Cuppoletti, J.; Tewari, K.P.; Chakrabarti, J.; Malinowska, D.H. Identification of the fatty acid activation site on human ClC-2. Am. J. Physiol. Cell Physiol. 2017, 312, C707–C723. [Google Scholar] [CrossRef] [Green Version]
- Bao, H.F.; Liu, L.; Self, J.; Duke, B.J.; Ueno, R.; Eaton, D.C. A synthetic prostone activates apical chloride channels in A6 epithelial cells. Am. J. Physiol. Gastrointest. Liver. Physiol. 2008, 295, G234–G251. [Google Scholar] [CrossRef] [Green Version]
- Fei, G.; Wang, Y.Z.; Liu, S.; Hu, H.Z.; Wang, G.D.; Qu, M.H.; Wang, X.Y.; Xia, Y.; Sun, X.; Bohn, L.M.; et al. Stimulation of mucosal secretion by lubiprostone (SPI-0211) in guinea pig small intestine and colon. Am. J. Physiol. Gastrointest. Liver. Physiol. 2009, 296, G823–G832. [Google Scholar] [CrossRef] [Green Version]
- Bijvelds, M.J.; Bot, A.G.; Escher, J.C.; De Jonge, H.R. Activation of intestinal Cl- secretion by lubiprostone requires the cystic fibrosis transmembrane conductance regulator. Gastroenterology 2009, 137, 976–985. [Google Scholar] [CrossRef]
- Ao, M.; Venkatasubramanian, J.; Boonkaewwan, C.; Ganesan, N.; Syed, A.; Benya, R.V.; Rao, M.C. Lubiprostone activates Cl- secretion via cAMP signaling and increases membrane CFTR in the human colon carcinoma cell line, T84. Dig. Dis. Sci. 2011, 56, 339–351. [Google Scholar] [CrossRef]
- Mizumori, M.; Akiba, Y.; Kaunitz, J.D. Lubiprostone stimulates duodenal bicarbonate secretion in rats. Dig. Dis. Sci. 2009, 54, 2063–2069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norimatsu, Y.; Moran, A.R.; MacDonald, K.D. Lubiprostone activates CFTR, but not ClC-2, via the prostaglandin receptor (EP(4)). Biochem. Biophys. Res. Commun. 2012, 426, 374–379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schiffhauer, E.S.; Vij, N.; Kovbasnjuk, O.; Kang, P.W.; Walker, D.; Lee, S.; Zeitlin, P.L. Dual activation of CFTR and CLCN2 by lubiprostone in murine nasal epithelia. Am. J. Physiol. Lung. Cell Mol. Physiol. 2013, 304, L324–L331. [Google Scholar] [CrossRef] [Green Version]
- Jakab, R.L.; Collaco, A.M.; Ameen, N.A. Lubiprostone targets prostanoid signaling and promotes ion transporter trafficking, mucus exocytosis, and contractility. Dig. Dis. Sci. 2012, 57, 2826–2845. [Google Scholar] [CrossRef] [PubMed]
- Arakawa, K.; Ishigami, T.; Nakai-Sugiyama, M.; Chen, L.; Doi, H.; Kino, T.; Minegishi, S.; Saigoh-Teranaka, S.; Sasaki-Nakashima, R.; Hibi, K.; et al. Lubiprostone as a potential therapeutic agent to improve intestinal permeability and prevent the development of atherosclerosis in apolipoprotein E-deficient mice. PLoS ONE 2019, 14, e0218096. [Google Scholar] [CrossRef]
- Moeser, A.J.; Nighot, P.K.; Engelke, K.J.; Ueno, R.; Blikslager, A.T. Recovery of mucosal barrier function in ischemic porcine ileum and colon is stimulated by a novel agonist of the ClC-2 chloride channel, lubiprostone. Am. J. Physiol. Gastrointest. Liver. Physiol. 2007, 292, G647–G656. [Google Scholar] [CrossRef] [Green Version]
- Matsui, H.; Shimokawa, O.; Kaneko, T.; Nagano, Y.; Rai, K.; Hyodo, I. The pathophysiology of non-steroidal anti-inflammatory drug (NSAID)-induced mucosal injuries in stomach and small intestine. J. Clin. Biochem. Nutr. 2011, 48, 107–111. [Google Scholar] [CrossRef] [Green Version]
- Hayashi, S.; Kurata, N.; Yamaguchi, A.; Amagase, K.; Takeuchi, K. Lubiprostone prevents nonsteroidal anti-inflammatory drug-induced small intestinal damage by suppressing the expression of inflammatory mediators via EP4 receptors. J. Pharmacol. Exp. Ther. 2014, 349, 470–479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jin, Y.; Blikslager, A.T. ClC-2 regulation of intestinal barrier function: Translation of basic science to therapeutic target. Tissue Barriers 2015, 3, e1105906. [Google Scholar] [CrossRef] [Green Version]
- Kato, T.; Honda, Y.; Kurita, Y.; Iwasaki, A.; Sato, T.; Kessoku, T.; Uchiyama, S.; Ogawa, Y.; Ohkubo, H.; Higurashi, T.; et al. Lubiprostone improves intestinal permeability in humans, a novel therapy for the leaky gut: A prospective randomized pilot study in healthy volunteers. PLoS ONE 2017, 12, e0175626. [Google Scholar] [CrossRef] [Green Version]
- Gyomorey, K.; Yeger, H.; Ackerley, C.; Garami, E.; Bear, C.E. Expression of the chloride channel ClC-2 in the murine small intestine epithelium. Am. J. Physiol. Cell Physiol. 2000, 279, C1787–C1794. [Google Scholar] [CrossRef] [Green Version]
- Moeser, A.J.; Haskell, M.M.; Shifflett, D.E.; Little, D.; Schultz, B.D.; Blikslager, A.T. ClC-2 chloride secretion mediates prostaglandin-induced recovery of barrier function in ischemia-injured porcine ileum. Gastroenterology 2004, 127, 802–815. [Google Scholar] [CrossRef]
- Moeser, A.J.; Nighot, P.K.; Roerig, B.; Ueno, R.; Blikslager, A.T. Comparison of the chloride channel activator lubiprostone and the oral laxative Polyethylene Glycol 3350 on mucosal barrier repair in ischemic-injured porcine intestine. World J. Gastroenterol. 2008, 14, 6012–6017. [Google Scholar] [CrossRef] [PubMed]
- Nighot, P.K.; Blikslager, A.T. Chloride channel ClC-2 modulates tight junction barrier function via intracellular trafficking of occludin. Am. J. Physiol. Cell Physiol. 2012, 302, C178–C187. [Google Scholar] [CrossRef] [PubMed]
- Nighot, P.K.; Leung, L.; Ma, T.Y. Chloride channel ClC- 2 enhances intestinal epithelial tight junction barrier function via regulation of caveolin-1 and caveolar trafficking of occludin. Exp. Cell Res. 2017, 352, 113–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nighot, P.K.; Moeser, A.J.; Ryan, K.A.; Ghashghaei, T.; Blikslager, A.T. ClC-2 is required for rapid restoration of epithelial tight junctions in ischemic-injured murine jejunum. Exp. Cell Res. 2009, 315, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Nighot, P.K.; Blikslager, A.T. ClC-2 regulates mucosal barrier function associated with structural changes to the villus and epithelial tight junction. Am. J. Physiol. Gastrointest. Liver. Physiol. 2010, 299, G449–G456. [Google Scholar] [CrossRef] [Green Version]
- Nighot, P.; Young, K.; Nighot, M.; Rawat, M.; Sung, E.J.; Maharshak, N.; Plevy, S.E.; Ma, T.; Blikslager, A. Chloride channel ClC-2 is a key factor in the development of DSS-induced murine colitis. Inflamm. Bowel. Dis. 2013, 19, 2867–2877. [Google Scholar] [CrossRef] [Green Version]
- McCole, D.F. IBD candidate genes and intestinal barrier regulation. Inflamm. Bowel. Dis. 2014, 20, 1829–1849. [Google Scholar] [CrossRef] [Green Version]
- Teshima, C.W.; Dieleman, L.A.; Meddings, J.B. Abnormal intestinal permeability in Crohn’s disease pathogenesis. Ann. N. Y. Acad. Sci. 2012, 1258, 159–165. [Google Scholar] [CrossRef]
- Wyatt, J.; Vogelsang, H.; Hübl, W.; Waldhöer, T.; Lochs, H. Intestinal permeability and the prediction of relapse in Crohn’s disease. Lancet 1993, 341, 1437–1439. [Google Scholar] [CrossRef] [PubMed]
- Hollander, D.; Vadheim, C.M.; Brettholz, E.; Petersen, G.M.; Delahunty, T.; Rotter, J.I. Increased intestinal permeability in patients with Crohn’s disease and their relatives. A possible etiologic factor. Ann. Intern. Med. 1986, 105, 883–885. [Google Scholar] [CrossRef] [PubMed]
- Marin, M.L.; Greenstein, A.J.; Geller, S.A.; Gordon, R.E.; Aufses, A.H., Jr. A freeze fracture study of Crohn’s disease of the terminal ileum: Changes in epithelial tight junction organization. Am. J. Gastroenterol. 1983, 78, 537–547. [Google Scholar] [PubMed]
- Weber, C.R.; Raleigh, D.R.; Su, L.; Shen, L.; Sullivan, E.A.; Wang, Y.; Turner, J.R. Epithelial myosin light chain kinase activation induces mucosal interleukin-13 expression to alter tight junction ion selectivity. J. Biol. Chem. 2010, 285, 12037–12046. [Google Scholar] [CrossRef] [Green Version]
- Zeissig, S.; Burgel, N.; Gunzel, D.; Richter, J.; Mankertz, J.; Wahnschaffe, U.; Kroesen, A.J.; Zeitz, M.; Fromm, M.; Schulzke, J.D. Changes in expression and distribution of claudin 2, 5 and 8 lead to discontinuous tight junctions and barrier dysfunction in active Crohn’s disease. Gut 2007, 56, 61–72. [Google Scholar] [CrossRef]
- Marchelletta, R.R.; Krishnan, M.; Spalinger, M.R.; Placone, T.W.; Alvarez, R.; Sayoc-Becerra, A.; Canale, V.; Shawki, A.; Park, Y.S.; Bernts, L.H.; et al. T cell protein tyrosine phosphatase protects intestinal barrier function by restricting epithelial tight junction remodeling. J. Clin. Investig. 2021, 131. [Google Scholar] [CrossRef]
- Nishii, N.; Oshima, T.; Li, M.; Eda, H.; Nakamura, K.; Tamura, A.; Ogawa, T.; Yamasaki, T.; Kondo, T.; Kono, T.; et al. Lubiprostone Induces Claudin-1 and Protects Intestinal Barrier Function. Pharmacology 2020, 105, 102–108. [Google Scholar] [CrossRef]
- Zong, Y.; Zhu, S.; Zhang, S.; Zheng, G.; Wiley, J.W.; Hong, S. Chronic stress and intestinal permeability: Lubiprostone regulates glucocorticoid receptor-mediated changes in colon epithelial tight junction proteins, barrier function, and visceral pain in the rodent and human. Neurogastroenterol. Motil. 2019, 31, e13477. [Google Scholar] [CrossRef]
- Jin, Y.; Pridgen, T.A.; Blikslager, A.T. Pharmaceutical Activation or Genetic Absence of ClC-2 Alters Tight Junctions During Experimental Colitis. Inflamm. Bowel. Dis. 2015, 21, 2747–2757. [Google Scholar] [CrossRef] [Green Version]
- Kang, S.B.; Marchelletta, R.R.; Penrose, H.; Docherty, M.J.; McCole, D.F. A comparison of linaclotide and lubiprostone dosing regimens on ion transport responses in human colonic mucosa. Pharmacol. Res. Perspect. 2015, 3, e00128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Selin, K.A.; Hedin, C.R.H.; Villablanca, E.J. Immunological Networks Defining the Heterogeneity of Inflammatory Bowel Diseases. J. Crohns. Colitis. 2021, 15, 1959–1973. [Google Scholar] [CrossRef] [PubMed]
- De Lisle, R.C. Lubiprostone stimulates small intestinal mucin release. BMC Gastroenterol. 2012, 12, 156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Musch, M.W.; Wang, Y.; Claud, E.C.; Chang, E.B. Lubiprostone decreases mouse colonic inner mucus layer thickness and alters intestinal microbiota. Dig. Dis. Sci. 2013, 58, 668–677. [Google Scholar] [CrossRef] [Green Version]
- Hemlin, M.; Jodal, M.; Lundgren, O.; Sjovall, H.; Stage, L. The importance of the subepithelial resistance for the electrical properties of the rat jejunum in vitro. Acta. Physiol. Scand. 1988, 134, 79–88. [Google Scholar] [CrossRef]
- Clarke, L.L. A guide to Ussing chamber studies of mouse intestine. Am. J. Physiol. Gastrointest. Liver. Physiol. 2009, 296, G1151–G1166. [Google Scholar] [CrossRef] [Green Version]
- McCole, D.F.; Rogler, G.; Varki, N.; Barrett, K.E. Epidermal growth factor partially restores colonic ion transport responses in mouse models of chronic colitis. Gastroenterology 2005, 129, 591–608. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control | CD-Remission | UC-Remission | CD-Active | |
|---|---|---|---|---|
| Number of patients | 17 | 16 | 15 | 4 |
| Sex (% female) | 57 | 73 | 67 | 50 |
| Age at enrollment (Years +/- SD) | 61.8 ± 10.9 | 39.5 ± 14.3 | 49 ± 14.8 | 50 ± 14.7 |
| Symptoms (% of total population) | ||||
| Diarrhea | 7 | 27 | 13 | 75 |
| Blood (rectum/stool) | 7 | 6.7 | 0 | 25 |
| Anemia | 0 | 0 | 7 | 0 |
| Abdominal pain | 0 | 33 | 25 | |
| Medical treatment (% of total popn.) | ||||
| Anti-inflammatories | 42.9 | 26.7 | 86.7 | 25 |
| Anti-TNF | 0 | 46.7 | 33 | 75 |
| Steroids | 0 | 0 | 6.7 | 25 |
| Immunosuppressives | 0 | 26.7 | 33 | 50 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, Y.S.; Kang, S.B.; Marchelletta, R.R.; Penrose, H.M.; Ruiter-Visser, R.; Jung, B.; Docherty, M.J.; Boland, B.S.; Sandborn, W.J.; McCole, D.F. The ClC-2 Chloride Channel Activator, Lubiprostone, Improves Intestinal Barrier Function in Biopsies from Crohn’s Disease but Not Ulcerative Colitis Patients. Pharmaceutics 2023, 15, 811. https://doi.org/10.3390/pharmaceutics15030811
Park YS, Kang SB, Marchelletta RR, Penrose HM, Ruiter-Visser R, Jung B, Docherty MJ, Boland BS, Sandborn WJ, McCole DF. The ClC-2 Chloride Channel Activator, Lubiprostone, Improves Intestinal Barrier Function in Biopsies from Crohn’s Disease but Not Ulcerative Colitis Patients. Pharmaceutics. 2023; 15(3):811. https://doi.org/10.3390/pharmaceutics15030811
Chicago/Turabian StylePark, Young Su, Sang Bum Kang, Ronald R. Marchelletta, Harrison M. Penrose, Roos Ruiter-Visser, Barbara Jung, Michael J. Docherty, Brigid S. Boland, William J. Sandborn, and Declan F. McCole. 2023. "The ClC-2 Chloride Channel Activator, Lubiprostone, Improves Intestinal Barrier Function in Biopsies from Crohn’s Disease but Not Ulcerative Colitis Patients" Pharmaceutics 15, no. 3: 811. https://doi.org/10.3390/pharmaceutics15030811