

Intrathecal Pseudodelivery of Drugs in the Therapy of Neurodegenerative Diseases: Rationale, Basis and Potential Applications

 ,
,  ,
,  , ,
, ,
Abstract
:1. The BBB, the CSF, and the Neurodegenerative Diseases
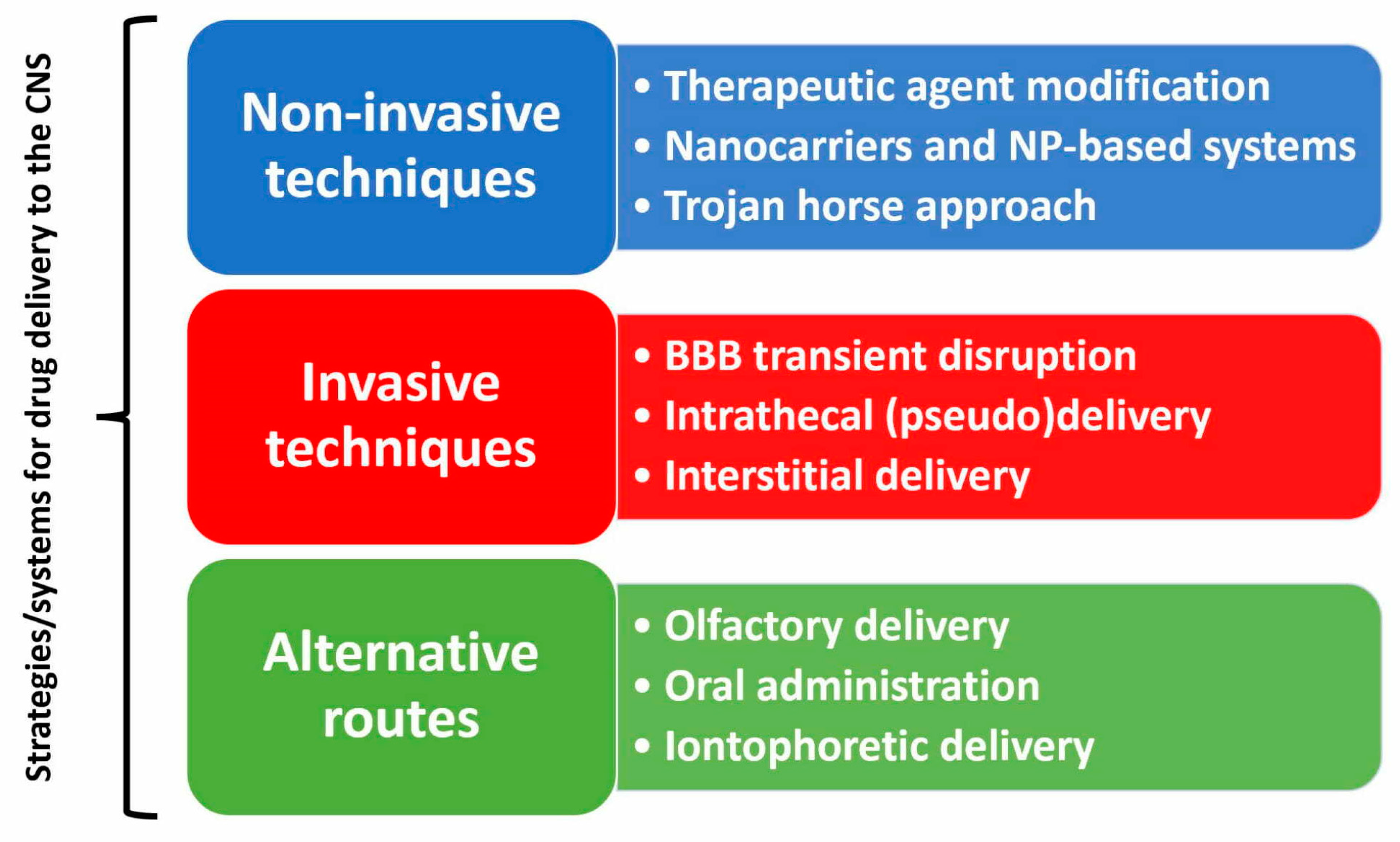
2. The Problem of Drug Delivery to the CNS and Its Many Explored Solutions
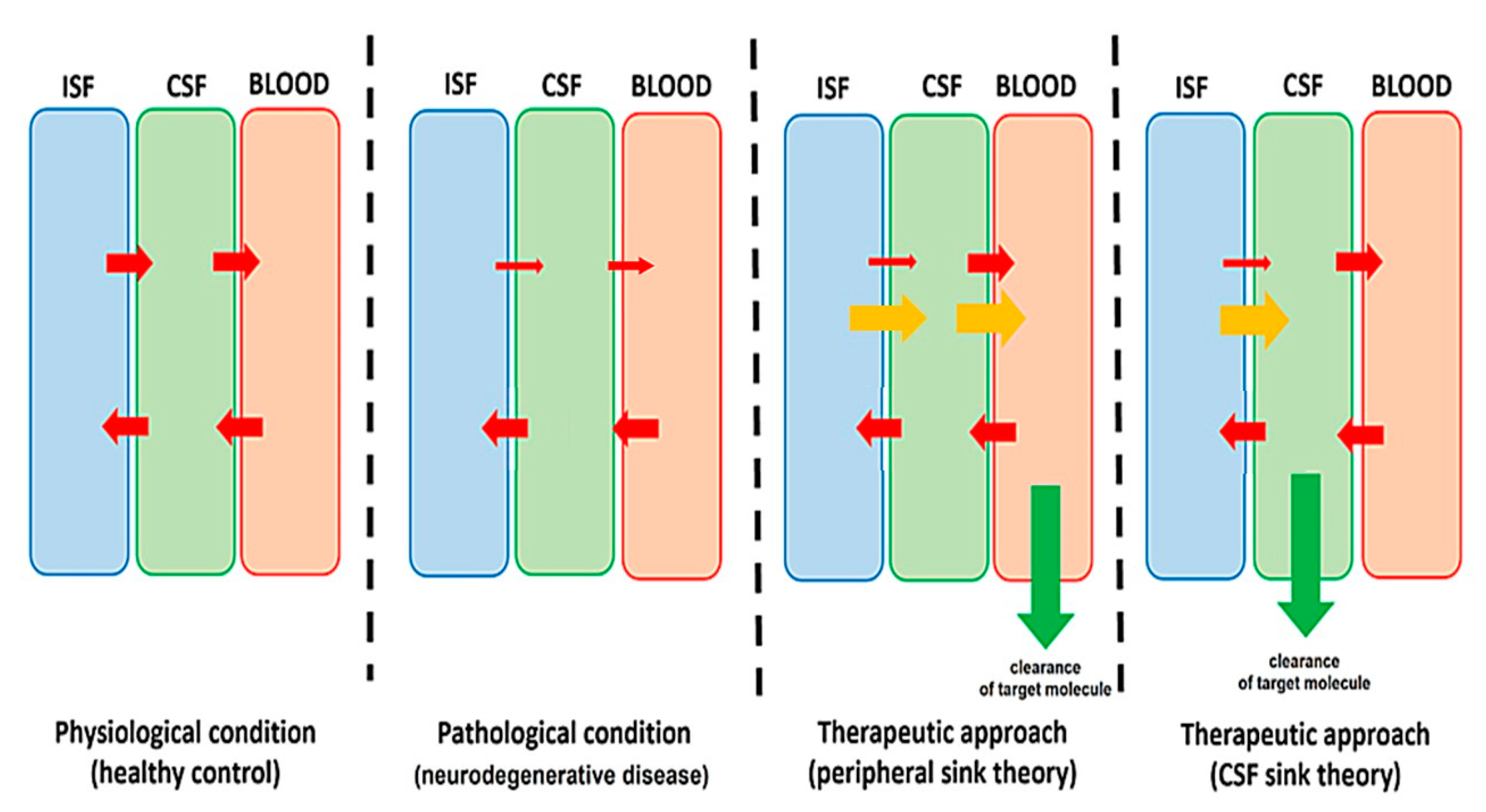
3. Clearing the CSF as a Therapeutic Strategy in Neurodegenerative Diseases
4. Intrathecal Pseudodelivery of Drugs: Concept, Advantages, and Disadvantages
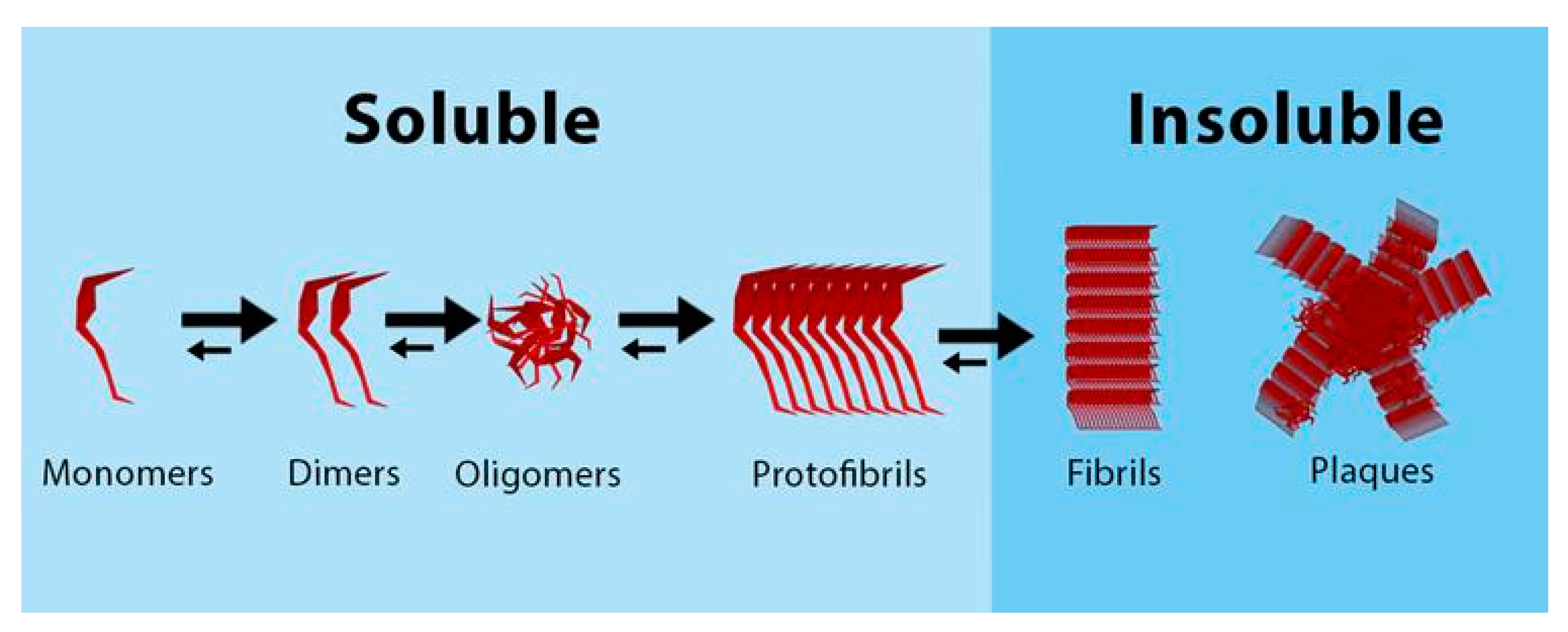
- A target molecule should be present in the CSF (soluble). This should be identified as potentially “toxic” or “pathogenic” and involved directly (aggregating proteins) or indirectly (mediators) in the physiopathology of the disease.
- A drug acting specifically on the target molecule is needed. This can be an antibody, an aptamer, an enzyme, or any other compound that has specificity over the target molecule and either binds or cleaves the target molecule.
- A significant size difference should exist between the target and drug molecules. While other physicochemical features may also play a role (such as electrostatic charge), the size difference is the main feature driving the selective molecular permeability through nanoporous membranes.
5. Potential Applications of Intrathecal Pseudodelivery of Drugs: Diseases, Targets, and Relevant Drugs
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kadry, H.; Noorani, B.; Cucullo, L. A blood–brain barrier overview on structure, function, impairment, and biomarkers of integrity. Fluids Barriers CNS 2020, 17, 69. [Google Scholar] [CrossRef] [PubMed]
- Katt, M.E.; Xu, Z.S.; Gerecht, S.; Searson, P.C. Human brain microvascular endothelial cells derived from the BC1 iPS cell line exhibit a blood-brain barrier phenotype. PLoS ONE 2016, 11, e0152105. [Google Scholar] [CrossRef] [Green Version]
- Alajangi, H.K.; Kaur, M.; Sharma, A.; Rana, S.; Thakur, S.; Chatterjee, M.; Singla, N.; Jaiswal, P.K.; Singh, G.; Barnwal, R.P. Blood–brain barrier: Emerging trends on transport models and new-age strategies for therapeutics intervention against neurological disorders. Mol Brain. 2022, 15, 49. [Google Scholar] [CrossRef]
- Solár, P.; Zamani, A.; Kubíčková, L.; Dubový, P.; Joukal, M. Choroid plexus and the blood-cerebrospinal fluid barrier in disease. Fluids Barriers CNS 2020, 17, 35. [Google Scholar] [CrossRef] [PubMed]
- Ayub, M.; Jin, H.K.; Bae, J.S. The blood cerebrospinal fluid barrier orchestrates immunosurveillance, immunoprotection, and immunopathology in the central nervous system. BMB Rep. 2021, 54, 196–202. [Google Scholar] [CrossRef]
- Kelley, D.H.; Thomas, J.H. Cerebrospinal Fluid Flow. Annu. Rev. Fluid Mech. 2023, 55, 237–264. [Google Scholar] [CrossRef]
- Schreiner, T.G.; Creangă-Murariu, I.; Tamba, B.I.; Lucanu, N.; Popescu, B.O. In Vitro Modeling of the Blood–Brain Barrier for the Study of Physiological Conditions and Alzheimer’s Disease. Biomolecules 2022, 12, 1136. [Google Scholar]
- Kok, F.K.; van Leerdam, S.L.; de Lange, E.C.M. Potential Mechanisms Underlying Resistance to Dementia in Non-Demented Individuals with Alzheimer’s Disease Neuropathology. J. Alzheimer’s Dis. 2022, 87, 51–81. [Google Scholar] [CrossRef]
- Fan, H.C.; Ho, L.I.; Chi, C.S.; Chen, S.J.; Peng, G.S.; Chan, T.M.; Lin, S.Z.; Harn, H.J. Polyglutamine (PolyQ) diseases: Genetics to treatments. Cell Transplant. 2014, 23, 441–458. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Vicente, M.; Cuervo, A.M. Autophagy and neurodegeneration: When the cleaning crew goes on strike. Lancet Neurol. 2007, 6, 352–361. [Google Scholar] [CrossRef] [PubMed]
- Nixon, R.A. The role of autophagy in neurodegenerative disease. Nat. Med. 2013, 19, 983–997. [Google Scholar] [CrossRef] [PubMed]
- Schweig, J.E.; Yao, H.; Beaulieu-Abdelahad, D.; Ait-Ghezala, G.; Mouzon, B.; Crawford, F.; Mullan, M.; Paris, D. Alzheimer’s disease pathological lesions activate the spleen tyrosine kinase. Acta Neuropathol. Commun. 2017, 5, 69. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Happonen, K.E.; Burrola, P.G.; O-Connor, C.; Hah, N.; Huang, L.; Nimmerjahn, A.; Lemke, G. Microglia use TAM receptors to detect and engulf amyloid β plaques. Nat. Immunol. 2021, 22, 586–594. [Google Scholar] [CrossRef]
- Silvin, A.; Uderhardt, S.; Piot, C.; Da Mesquita, S.; Yang, K.; Geirsdottir, L.; Mulder, K.; Eyal, D.; Liu, Z.; Bridlance, C.; et al. Dual ontogeny of disease-associated microglia and disease inflammatory macrophages in aging and neurodegeneration. Immunity 2022, 55, 1448–1465. [Google Scholar] [CrossRef]
- Lee, J.-H.; Yang, D.-S.; Goulbourne, C.N.; Im, E.; Stavrides, P.; Pensalfini, A.; Chan, H.; Bouchet-Marquis, C.; Bleiwas, C.; Berg, M.J.; et al. Faulty autolysosome acidification in Alzheimer’s disease mouse models induces autophagic build-up of Aβ in neurons, yielding senile plaques. Nat. Neurosci. 2022, 25, 688–701. [Google Scholar] [CrossRef]
- Sikanyika, N.L.; Parkington, H.C.; Smith, A.I.; Kuruppu, S. Powering Amyloid Beta Degrading Enzymes: A Possible Therapy for Alzheimer’s Disease. Neurochem. Res. 2019, 44, 1289–1296. [Google Scholar] [CrossRef]
- Elbert, D.L.; Patterson, B.W.; Lucey, B.P.; Benzinger, T.L.S.; Bateman, R.J. Importance of CSF-based Aβ clearance with age in humans increases with declining efficacy of blood-brain barrier/proteolytic pathways. Commun. Biol. 2022, 5, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Mestre, H.; Verma, N.; Greene, T.D.; Lin, L.A.; Ladron-de-Guevara, A.; Sweeney, A.M.; Liu, G.; Thomas, V.K.; Galloway, C.A.; de Mesy Bentley, K.L.; et al. Periarteriolar spaces modulate cerebrospinal fluid transport into brain and demonstrate altered morphology in aging and Alzheimer’s disease. Nat. Commun. 2022, 13, 3897. [Google Scholar] [CrossRef]
- Peng, W.; Achariyar, T.M.; Li, B.; Liao, Y.; Mestre, H.; Hitomi, E.; Regan, S.; Kasper, T.; Peng, S.; Ding, F.; et al. Suppression of glymphatic fluid transport in a mouse model of Alzheimer’s disease. Neurobiol. Dis. 2016, 93, 215–225. [Google Scholar] [CrossRef] [Green Version]
- da Mesquita, S.; Papadopoulos, Z.; Dykstra, T.; Brase, L.; Farias, F.G.; Wall, M.; Jiang, H.; Kodira, C.D.; de Lima, K.A.; Herz, J.; et al. Meningeal lymphatics affect microglia responses and anti-Aβ immunotherapy. Nature 2021, 593, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Rusinek, H.; Butler, T.; Glodzik, L.; Pirraglia, E.; Babich, J.; Mozley, P.D.; Nehmeh, S.; Pahlajani, S.; Wang, X.; et al. Decreased CSF clearance and increased brain amyloid in Alzheimer’s disease. Fluids Barriers CNS 2022, 19, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Klostranec, J.M.; Vucevic, D.; Bhatia, K.D.; Kortman, H.G.J.; Krings, T.; Murphy, K.P.; terBrugge, K.G.; Mikulis, D.J. Current concepts in intracranial interstitial fluid transport and the glymphatic system: Part i-anatomy and physiology. Radiology 2021, 301, 502–514. [Google Scholar] [CrossRef]
- Lee, M.K.; Cho, S.J.; Bae, Y.J.; Kim, J.M. MRI-Based Demonstration of the Normal Glymphatic System in a Human Population: A Systematic Review. Front. Neurol. 2022, 13, 827398. [Google Scholar] [CrossRef]
- Kato, D.; Takahashi, Y.; Iwata, H.; Hatakawa, Y.; Lee, S.H.; Oe, T. Comparative studies for amyloid beta degradation: “Neprilysin vs. insulysin”, “monomeric vs. aggregate”, and “whole Aβ40 vs. its peptide fragments. Biochem. Biophys. Rep. 2022, 30, 101268. [Google Scholar] [CrossRef]
- Zhao, A.; Jiao, Y.; Ye, G.; Kang, W.; Tan, L.; Li, Y.; Deng, Y.; Liu, J.; Alzheimer’s Disease Neuroimaging Initiative (ADNI). Soluble TREM2 levels associate with conversion from mild cognitive impairment to Alzheimer’s disease. J. Clin. Investig. 2022, 132, 158708. [Google Scholar] [CrossRef]
- Brown, G.C.; St George-Hyslop, P. Does Soluble TREM2 Protect Against Alzheimer’s Disease? Front. Aging Neurosci. 2022, 13, 834697. [Google Scholar] [CrossRef]
- Zhong, L.; Chen, X.F.; Wang, T.; Wang, Z.; Liao, C.; Wang, Z.; Huang, R.; Wang, D.; Li, X.; Wu, L.; et al. Soluble TREM2 induces inflammatory responses and enhances microglial survival. J. Exp. Med. 2017, 214, 597–607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.; Fu, Z.; Zhang, X.; Xiong, M.; Meng, L.; Zhang, Z. TREM2 ectodomain and its soluble form in Alzheimer’s disease. J. Neuroinflammation 2020, 17, 1–12. [Google Scholar] [CrossRef]
- Kwon, H.S.; Koh, S.H. Neuroinflammation in neurodegenerative disorders: The roles of microglia and astrocytes. Transl. Neurodegener. 2020, 9, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Piehl, N.; van Olst, L.; Ramakrishnan, A.; Teregulova, V.; Simonton, B.; Zhang, Z.; Tapp, E.; Channappa, D.; Oh, H.; Losada, P.M.; et al. Cerebrospinal fluid immune dysregulation during healthy brain aging and cognitive impairment. Cell 2022, 185, 5028–5039.e13. [Google Scholar] [CrossRef]
- Ng Kee Kwong, K.C.; Gregory, J.M.; Pal, S.; Chandran, S.; Mehta, A.R. Cerebrospinal fluid cytotoxicity in amyotrophic lateral sclerosis: A systematic review of in vitro studies. Brain Commun. 2020, 2, fcaa121. [Google Scholar] [CrossRef]
- Chang, R.; Yee, K.-L.; Sumbria, R.K. Tumor necrosis factor α Inhibition for Alzheimer’s Disease. J. Cent. Nerv. Syst. Dis. 2017, 9, 1179573517709278. [Google Scholar] [CrossRef]
- Tortelli, R.; Zecca, C.; Piccininni, M.; Benmahamed, S.; Dell—Abate, M.T.; Barulli, M.R.; Capozzo, R.; Battista, P.; Logroscino, G. Plasma Inflammatory Cytokines Are Elevated in ALS. Front. Neurol. 2020, 11, 552295. [Google Scholar] [CrossRef] [PubMed]
- Sun, Q.; Huo, Y.; Bai, J.; Wang, H.; Wang, H.; Yang, F.; Cui, F.; Song, H.; Huang, X. Inflammatory Cytokine Levels in Patients with Sporadic Amyotrophic Lateral Sclerosis. Neurodegener. Dis. 2022, 21, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Neumaier, F.; Zlatopolskiy, B.D.; Neumaier, B. Drug penetration into the central nervous system: Pharmacokinetic concepts and in vitro model systems. Pharmaceutics 2021, 13, 1542. [Google Scholar] [CrossRef]
- Pardridge, W.M. A Historical Review of Brain Drug Delivery. Pharmaceutics 2022, 14, 1283. [Google Scholar] [CrossRef] [PubMed]
- Meng, Y.; Reilly, R.M.; Pezo, R.C.; Trudeau, M.; Sahgal, A.; Singnurkar, A.; Perry, J.; Myrehaug, S.; Pople, C.B.; Davidson, B.; et al. MR-guided focused ultrasound enhances delivery of trastuzumab to Her2-positive brain metastases. Sci. Transl. Med. 2021, 13, abj4011. [Google Scholar] [CrossRef]
- Chu, C.; Jablonska, A.; Lesniak, W.G.; Thomas, A.M.; Lan, X.; Linville, R.M.; Li, S.; Searson, P.C.; Liu, G.; Pearl, M.; et al. Optimization of osmotic blood-brain barrier opening to enable intravital microscopy studies on drug delivery in mouse cortex. J. Control. Release 2020, 317, 312–321. [Google Scholar] [CrossRef]
- Poudel, P.; Park, S. Recent Advances in the Treatment of Alzheimer’s Disease Using Nanoparticle-Based Drug Delivery Systems. Pharmaceutics 2022, 14, 835. [Google Scholar] [CrossRef]
- Pinheiro, R.G.R.; Coutinho, A.J.; Pinheiro, M.; Neves, A.R. Nanoparticles for targeted brain drug delivery: What do we know? Int. J. Mol. Sci. 2021, 22, 11654. [Google Scholar] [CrossRef]
- Cano, A.; Muñoz-Morales, Á.; Sánchez-López, E.; Ettcheto, M.; Souto, E.B.; Camins, A.; Boada, M.; Ruíz, A. Exosomes-Based Nanomedicine for Neurodegenerative Diseases: Current Insights and Future Challenges. Pharmaceutics 2023, 15, 298. [Google Scholar] [CrossRef] [PubMed]
- Plassat, R.; Perrouin Verbe, B.; Menei, P.; Menegalli, D.; Mathé, J.F.; Richard, I. Treatment of spasticity with intrathecal baclofen administration: Long-term follow-up, review of 40 patients. Spinal Cord. 2004, 42, 686–693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koulousakis, A.; Kuchta, J. Intrathecal antispastic drug application with implantable pumps: Results of a 10 year follow-up study. In Operative Neuromodulation: Volume 1: Functional Neuroprosthetic Surgery An Introduction; Sakas Damianos, E., Simpson, B.A.K.E.S., Eds.; Springer Vienna: Vienna, Austria, 2007; pp. 181–184. [Google Scholar] [CrossRef]
- de Andres, J.; Hayek, S.; Perruchoud, C.; Lawrence, M.M.; Reina, M.A.; De Andres-Serrano, C.; Rubio-Haro, R.; Hunt, M.; Yaksh, T.L. Intrathecal Drug Delivery: Advances and Applications in the Management of Chronic Pain Patient. Front. Pain Res. 2022, 3, 900566. [Google Scholar] [CrossRef] [PubMed]
- Pope, J.E.; Deer, T.R.; Bruel, B.M.; Falowski, S. Clinical Uses of Intrathecal Therapy and Its Placement in the Pain Care Algorithm. Pain Pract. 2016, 16, 1092–1106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aartsma-Rus, A. FDA Approval of Nusinersen for Spinal Muscular Atrophy Makes 2016 the Year of Splice Modulating Oligonucleotides. Nucleic Acid Ther. 2017, 27, 67–69. [Google Scholar] [CrossRef]
- Kulkarni, J.A.; Witzigmann, D.; Thomson, S.B.; Chen, S.; Leavitt, B.R.; Cullis, P.R.; van der Meel, R. The current landscape of nucleic acid therapeutics. Nat. Nanotechnol. 2021, 16, 630–643. [Google Scholar] [CrossRef]
- Adepu, S.; Ramakrishna, S. Controlled drug delivery systems: Current status and future directions. Molecules 2021, 26, 5905. [Google Scholar] [CrossRef]
- Rafiee, M.H.; Rasool, B.K.A. An Overview of Microparticulate Drug Delivery System and its Extensive Therapeutic Applications in Diabetes. Adv. Pharm. Bull. 2022, 12, 730–746. [Google Scholar] [CrossRef]
- Nunes, D.; Loureiro, J.A.; Pereira, M.C. Drug Delivery Systems as a Strategy to Improve the Efficacy of FDA-Approved Alzheimer’s Drugs. Pharmaceutics 2022, 14, 2296. [Google Scholar]
- Ericson, T.; Singla, P.; Kohan, L. Intrathecal Pumps. Phys. Med. Rehabil. Clin. 2022, 33, 409–424. [Google Scholar] [CrossRef]
- Peck, D.; Diwan, S. Programmable versus Fixed-Rate Pumps for Intrathecal Drug Delivery. In Intrathecal Drug Delivery for Pain and Spasticity, 1st ed.; Saunders: Philadelphia, PA, USA, 2011; pp. 84–89. [Google Scholar]
- Delhaas, E.M.; Huygen, F.J.P.M. Complications associated with intrathecal drug delivery systems. BJA Educ. 2020, 20, 51–57. [Google Scholar] [CrossRef]
- Gevirtz, C. Complications Associated With Intrathecal Pumps. Top. Pain Manag. 2012, 27, 1–7. [Google Scholar]
- Zhang, Y.; Lee, D.H.S. Sink hypothesis and therapeutic strategies for attenuating Aβ levels. Neuroscientist 2011, 17, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Lacorte, E.; Ancidoni, A.; Zaccaria, V.; Remoli, G.; Tariciotti, L.; Bellomo, G.; Sciancalepore, F.; Corbo, M.; Lombardo, F.L.; Bacigalupo, I.; et al. Safety and Efficacy of Monoclonal Antibodies for Alzheimer’s Disease: A Systematic Review and Meta-Analysis of Published and Unpublished Clinical Trials. J. Alzheimer’s Dis. 2022, 87, 101–129. [Google Scholar] [CrossRef] [PubMed]
- Söderberg, L.; Johannesson, M.; Nygren, P.; Laudon, H.; Eriksson, F.; Osswald, G.; Möller, C.; Lannfelt, L. Lecanemab, Aducanumab, and Gantenerumab—Binding Profiles to Different Forms of Amyloid-Beta Might Explain Efficacy and Side Effects in Clinical Trials for Alzheimer’s Disease. Neurotherapeutics 2022, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Menéndez-González, M.; Padilla-Zambrano, H.S.; Tomás-Zapico, C.; García, B.F. Clearing extracellular alpha-synuclein from cerebrospinal fluid: A new therapeutic strategy in parkinson’s disease. Brain Sci. 2018, 8, 52. [Google Scholar] [CrossRef] [Green Version]
- Menendez-Gonzalez, M.; Padilla-Zambrano, H.S.; Alvarez, G.; Capetillo-Zarate, E.; Tomas-Zapico, C.; Costa, A. Targeting beta-amyloid at the CSF: A new therapeutic strategy in Alzheimer’s disease. Front. Aging Neurosci. 2018, 10, 100. [Google Scholar] [CrossRef]
- Schreiner, T.G.; Menéndez-González, M.; Popescu, B.O. The “Cerebrospinal Fluid Sink Therapeutic Strategy” in Alzheimer’s Disease-From Theory to Design of Applied Systems. Biomedicines 2022, 10, 1509. [Google Scholar] [CrossRef]
- Gao, I.; Griffin, R.; Celestin, N.; Wong, J.; Sadiq, S. Filtration attenuates sporadic ALS CSF-induced motor neuron death in vitro (P1-13.007). Neurology 2022, 98, 2154. [Google Scholar]
- Celestin, N.; Shue, T.; Beaty, J.; Wong, J.; Sadiq, S. Filtration reduces neurotoxicity of sporadic ALS cerebrospinal fluid in a mouse model (2264). Neurology 2021, 96, 2264. [Google Scholar]
- Finsterer, J.; Mamoli, B. Cerebrospinal fluid filtration in amyotrophic lateral sclerosis. Eur. J. Neurol. 1999, 6, 597–600. [Google Scholar] [CrossRef]
- Finsterer, J.; Mamoli, B. Liquorpheresis (CSF filtration) in familial amyotrophic lateral sclerosis. Spinal Cord. 1999, 37, 592–593. [Google Scholar] [CrossRef] [Green Version]
- Menéndez González, M. Mechanical Dilution of Beta-amyloid Peptide and Phosphorylated Tau Protein in Alzheimer’s Disease: Too Simple to be True? Cureus 2017, 9, e1062. [Google Scholar] [CrossRef] [PubMed]
- Moriya, M.; Miyajima, M.; Nakajima, M.; Ogino, I.; Arai, H. Impact of Cerebrospinal Fluid Shunting for Idiopathic Normal Pressure Hydrocephalus on the Amyloid Cascade. PLoS ONE 2015, 10, e0119973. [Google Scholar] [CrossRef] [Green Version]
- Silverberg, G.D.; Levinthal, E.; Sullivan, E.v.; Bloch, D.A.; Chang, S.D.; Leverenz, J.; Flitman, S.; Winn, R.; Marciano, F.; Saul, T.; et al. Assessment of low-flow CSF drainage as a treatment for AD: Results of a randomized pilot study. Neurology 2002, 59, 1139–1145. [Google Scholar] [CrossRef] [PubMed]
- Hadden, M.; Martinez-Martin, D.; Yong, K.-T.; Ramaswamy, Y.; Singh, G. Recent Advancements in the Fabrication of Functional Nanoporous Materials and Their Biomedical Applications. Materials 2022, 15, 2111. [Google Scholar] [CrossRef]
- Kapruwan, P.; Ferré-Borrull, J.; Marsal, L.F. Nanoporous Anodic Alumina Platforms for Drug Delivery Applications: Recent Advances and Perspective. Adv. Mater. Interfaces 2020, 7, 33. [Google Scholar] [CrossRef]
- Mabrouk, M.; Rajendran, R.; Soliman, I.E.; Ashour, M.M.; Beherei, H.H.; Tohamy, K.M.; Thomas, S.; Kalarikkal, N.; Arthanareeswaran, G.; Das, D.B. Nanoparticle- and nanoporous-membrane-mediated delivery of therapeutics. Pharmaceutics 2019, 11, 294. [Google Scholar] [CrossRef] [Green Version]
- Voskerician, G.; Shive, M.S.; Shawgo, R.S.; von Recum, H.; Anderson, J.M.; Cima, M.J.; Langer, R. Biocompatibility and biofouling of MEMS drug delivery devices. Biomaterials 2003, 24, 1959–1967. [Google Scholar] [CrossRef]
- Schreiner, T.G.; Tamba, B.I.; Mihai, C.T.; Lőrinczi, A.; Baibarac, M.; Ciobanu, R.C.; Popescu, B.O. Clinical Medicine Nanoporous Membranes for the Filtration of Proteins from Biological Fluids: Biocompatibility Tests on Cell Cultures and Suggested Applications for the Treatment of Alzheimer’s Disease. J. Clin. Med. 2022, 2022, 5846. [Google Scholar] [CrossRef] [PubMed]
- Mabrouk, M.; Das, D.B.; Salem, Z.A.; Beherei, H.H. Nanomaterials for biomedical applications: Production, characterisations, recent trends and difficulties. Molecules 2021, 26, 1077. [Google Scholar] [CrossRef] [PubMed]
- Coto-Vilcapoma, M.A.; Castilla-Silgado, J.; Fernández-García, B.; Pinto-Hernández, P.; Cipriani, R.; Capetillo-Zarate, E.; Menéndez-González, M.; Álvarez-Vega, M.; Tomás-Zapico, C. New, Fully Implantable Device for Selective Clearance of CSF-Target Molecules: Proof of Concept in a Murine Model of Alzheimer’s Disease. J. Mol. Sci. 2022, 23, 9256. [Google Scholar] [CrossRef]
- Menendez-Gonzalez, M.; Vilcapoma, A.C.; Silgado, J.C.; Alvarez-Vega, M.; Antuña-Ramos, A.; Fernandez-Garcia, B.; Prado, C.; Alvarez, G.; Rodriguez, M.; Perez, E.; et al. Intrathecal pseudodelivery of Ab-mAb alleviates pathology in an Alzheimer’s disease model. Alzheimer’s Dement. 2022, 18, e068697. [Google Scholar] [CrossRef]
- Mortada, I.; Farah, R.; Nabha, S.; Ojcius, D.M.; Fares, Y.; Almawi, W.Y.; Sadier, N.S. Immunotherapies for Neurodegenerative Diseases. Front. Neurol. 2021, 12, 654739. [Google Scholar] [CrossRef]
- van Dyck, C.H.; Swanson, C.J.; Aisen, P.; Bateman, R.J.; Chen, C.; Gee, M.; Kanekiyo, M.; Li, D.; Reyderman, L.; Cohen, S.; et al. Lecanemab in Early Alzheimer’s Disease. N. Engl. J. Med. 2023, 388, 9–21. [Google Scholar] [CrossRef]
- Perneczky, R.; Jessen, F.; Grimmer, T.; Levin, J.; Flöel, A.; Peters, O.; Froelich, L. Anti-amyloid antibody therapies in Alzheimer’s disease. Brain 2023, awad005. [Google Scholar] [CrossRef] [PubMed]
- Tampi, R.R.; Forester, B.P.; Agronin, M. Aducanumab: Evidence from clinical trial data and controversies. Drugs Context 2021, 10, 1–9. [Google Scholar] [CrossRef]
- Byun, J. Recent progress and opportunities for nucleic acid aptamers. Life 2021, 11, 193. [Google Scholar] [CrossRef] [PubMed]
- Menendez-Gonzalez, M.; Gasparovic, C. Albumin exchange in Alzheimer’s disease: Might CSF be an alternative route to plasma? Front. Neurol. 2019, 10, 1036. [Google Scholar] [CrossRef]
- Loktyushov Ev Litus, E.A.; Deryusheva, E.I. Systematic search for peptide and protein ligands of human serum albumin capable of affecting its interaction with amyloid-p peptide. Acta Biomed. Sci. 2022, 7, 19–26. [Google Scholar] [CrossRef]
- Murray, K.A.; Hu, C.J.; Griner, S.L.; Pan, H.; Bowler, J.T.; Abskharon, R.; Rosenberg, G.M.; Cheng, X.; Seidler, P.M.; Eisenberg, D.S. De novo designed protein inhibitors of amyloid aggregation and seeding. Proc. Natl. Acad. Sci. USA 2022, 119, e2206240119. [Google Scholar] [CrossRef] [PubMed]
- Chaudhary, H.; Iashchishyn, I.A.; Romanova, N.v.; Rambaran, M.A.; Musteikyte, G.; Smirnovas, V.; Holmboe, M.; Ohlin, C.A.; Svedružić, Ž.M.; Morozova-Roche, L.A. Polyoxometalates as Effective Nano-inhibitors of Amyloid Aggregation of Pro-inflammatory S100A9 Protein Involved in Neurodegenerative Diseases. ACS Appl. Mater. Interfaces 2021, 13, 26721–26734. [Google Scholar] [CrossRef] [PubMed]
- Ji, C.; Sigurdsson, E.M. Current Status of Clinical Trials on Tau Immunotherapies. Drugs 2021, 81, 1135–1152. [Google Scholar] [CrossRef] [PubMed]
- Teng, E.; Manser, P.T.; Pickthorn, K.; Brunstein, F.; Blendstrup, M.; Sanabria Bohorquez, S.; Wildsmith, K.R.; Toth, B.; Dolton, M. Safety and Efficacy of Semorinemab in Individuals with Prodromal to Mild Alzheimer Disease: A Randomized Clinical Trial. JAMA Neurol. 2022, 79, 758–767. [Google Scholar] [CrossRef] [PubMed]
- Wischik, C.M.; Harrington, C.R.; Storey, J.M.D. Tau-aggregation inhibitor therapy for Alzheimer’s disease. Biochem. Pharmacol. 2014, 88, 529–539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wischik, C.M.; Bentham, P.; Gauthier, S.; Miller, S.; Kook, K.; Schelter, B.O. Oral Tau Aggregation Inhibitor for Alzheimer’s Disease: Design, Progress and Basis for Selection of the 16 mg/day Dose in a Phase 3, Randomized, Placebo-Controlled Trial of Hydromethylthionine Mesylate. J. Prev. Alzheimers Dis. 2022, 9, 780–790. [Google Scholar] [CrossRef]
- van Lengerich, B.; Zhan, L.; Xia, D.; Chan, D.; Joy, D.; Park, J.I.; Tatarakis, D.; Calvert, M.; Hummel, S.; Lianoglou, S.; et al. A TREM2-activating antibody with a blood–brain barrier transport vehicle enhances microglial metabolism in Alzheimer’s disease models. Nat. Neurosci. 2023, 1–14. [Google Scholar] [CrossRef]
- Ma, L.Z.; Tan, L.; Bi, Y.L.; Shen, X.N.; Xu, W.; Ma, Y.H.; Li, H.Q.; Dong, Q.; Yu, J.T. Dynamic changes of CSF sTREM2 in preclinical Alzheimer’s disease: The CABLE study. Mol. Neurodegener. 2020, 15, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elcioğlu, H.K.; Aslan, E.; Ahmad, S.; Alan, S.; Salva, E.; Elcioglu, Ö.H.; Kabasakal, L. Tocilizumab’s effect on cognitive deficits induced by intracerebroventricular administration of streptozotocin in Alzheimer’s model. Mol. Cell Biochem. 2016, 420, 21–28. [Google Scholar] [CrossRef]
- Tobinick, E.L.; Gross, H. Rapid cognitive improvement in Alzheimer’s disease following perispinal etanercept administration. J. Neuroinflamm. 2008, 5, 2. [Google Scholar] [CrossRef] [Green Version]
- Shi, J.Q.; Shen, W.; Chen, J.; Wang, B.R.; Zhong, L.L.; Zhu, Y.W.; Zhu, H.Q.; Zhang, Q.Q.; Zhang, Y.D.; Xu, J. Anti-TNF-α reduces amyloid plaques and tau phosphorylation and induces CD11c-positive dendritic-like cell in the APP/PS1 transgenic mouse brains. Brain Res. 2011, 1368, 239–247. [Google Scholar] [CrossRef] [PubMed]
- Shi, J.Q.; Wang, B.R.; Jiang, W.W.; Chen, J.; Zhu, Y.W.; Zhong, L.L.; Zhang, Y.D.; Xu, J. Cognitive improvement with intrathecal administration of infliximab in a woman with Alzheimer’s disease. J. Am. Geriatr. Soc. 2011, 59, 1142–1144. [Google Scholar] [CrossRef] [PubMed]
- Ou, W.; Ohno, Y.; Yang, J.; Chandrashekar, D.V.; Abdullah, T.; Sun, J.; Murphy, R.; Roules, C.; Jagadeesan, N.; Cribbs, D.H.; et al. Efficacy and Safety of a Brain-Penetrant Biologic TNF-α Inhibitor in Aged APP/PS1 Mice. Pharmaceutics 2022, 14, 2200. [Google Scholar] [CrossRef]
- Pagano, G.; Taylor, K.I.; Anzures-Cabrera, J.; Marchesi, M.; Simuni, T.; Marek, K.; Postuma, R.B.; Pavese, N.; Stocchi, F.; Azulay, J.P.; et al. Trial of Prasinezumab in Early-Stage Parkinson’s Disease. N. Engl. J. Med. 2022, 387, 421–432. [Google Scholar] [CrossRef]
- Schenk, D.B.; Koller, M.; Ness, D.K.; Griffith, S.G.; Grundman, M.; Zago, W.; Soto, J.; Atiee, G.; Ostrowitzki, S.; Kinney, G.G. First-in-human assessment of PRX002, an anti–α-synuclein monoclonal antibody, in healthy volunteers. Mov. Disord. 2017, 32, 16428896. [Google Scholar] [CrossRef] [PubMed]
- Bluhm, A.; Schrempel, S.; von Hörsten, S.; Schulze, A.; Roßner, S. Proteolytic α-synuclein cleavage in health and disease. Int. J. Mol. Sci. 2021, 22, 5450. [Google Scholar] [CrossRef]
- Das, S.; Pukala, T.L.; Smid, S.D. Exploring the structural diversity in inhibitors of α-Synuclein amyloidogenic folding, aggregation, and neurotoxicity. Front. Chem. 2018, 6, 181. [Google Scholar] [CrossRef] [Green Version]
- Pons-Espinal, M.; Blasco-Agell, L.; Fernandez-Carasa, I.; di Domenico, A.; Richaud, Y.; Mosquera, J.L.; Marruecos, L.; Espinosa, L.; Garrido, A.; Tolosa, E.; et al. Immunosuppressive Tocilizumab Prevents Astrocyte Induced Neurotoxicity in HiPSC-LRRK2 Parkinson’s Disease by Targeting Receptor Interleukin-6. bioRxiv. 2022. Available online: http://biorxiv.org/content/early/2022/08/25/2022.08.23.504918.abstract (accessed on 10. January 2023).
- El-Kattan, M.M.; Rashed, L.A.; Shazly, S.R.; Ismail, R.S. Relation of serum level of tumor necrosis factor-alpha to cognitive functions in patients with Parkinson’s disease. Egypt. J. Neurol. Psychiatry Neurosurg. 2022, 58, 1–7. [Google Scholar] [CrossRef]
- Dam, T.; Boxer, A.L.; Golbe, L.I.; Höglinger, G.U.; Morris, H.R.; Litvan, I.; Lang, A.E.; Corvol, J.C.; Aiba, I.; Grundman, M.; et al. Safety and efficacy of anti-tau monoclonal antibody gosuranemab in progressive supranuclear palsy: A phase 2, randomized, placebo-controlled trial. Nat. Med. 2021, 27, 1451–1457. [Google Scholar] [CrossRef]
- Höglinger, G.U.; Litvan, I.; Mendonca, N.; Wang, D.; Zheng, H.; Rendenbach-Mueller, B.; Lon, H.K.; Jin, Z.; Fisseha, N.; Budur, K.; et al. Safety and efficacy of tilavonemab in progressive supranuclear palsy: A phase 2, randomised, placebo-controlled trial. Lancet Neurol. 2021, 20, 182–192. [Google Scholar] [CrossRef]
- Soeda, Y.; Takashima, A. New Insights Into Drug Discovery Targeting Tau Protein. Front. Mol. Neurosci. 2020, 13, 590896. [Google Scholar] [CrossRef] [PubMed]
- Francois-Moutal, L.; Scott, D.D.; Khanna, M. Direct targeting of TDP-43, from small molecules to biologics: The therapeutic landscape. RSC Chem. Biol. 2021, 2, 1158–1166. [Google Scholar] [CrossRef]
- Samanta, N.; Ruiz-Blanco, Y.B.; Fetahaj, Z.; Gnutt, D.; Lantz, C.; Loo, J.A.; Sanchez-Garcia, E.; Ebbinghaus, S. Superoxide Dismutase 1 Folding Stability as a Target for Molecular Tweezers in SOD1-Related Amyotrophic Lateral Sclerosis. ChemBioChem 2022, 23, e202200396. [Google Scholar] [CrossRef] [PubMed]
- Chantadul, V.; Wright, G.S.A.; Amporndanai, K.; Shahid, M.; Antonyuk, S.V.; Washbourn, G.; Rogers, M.; Roberts, N.; Pye, M.; O-Neill, P.M.; et al. Ebselen as template for stabilization of A4V mutant dimer for motor neuron disease therapy. Commun. Biol. 2020, 3, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pozzi, S.; Codron, P.; Soucy, G.; Renaud, L.; Cordeau, P.J.; Dutta, K.; Bareil, C.; Julien, J.P. Monoclonal full-length antibody against TAR DNA binding protein 43 reduces related proteinopathy in neurons. JCI Insight 2020, 5, 140420. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Yokoshi, M.; Okada, H.; Kawahara, Y. The cleavage pattern of TDP-43 determines its rate of clearance and cytotoxicity. Nat. Commun. 2015, 6, 6183. [Google Scholar] [CrossRef] [Green Version]
- Prasad, A.; Bharathi, V.; Sivalingam, V.; Girdhar, A.; Patel, B.K. Molecular mechanisms of TDP-43 misfolding and pathology in amyotrophic lateral sclerosis. Front. Mol. Neurosci. 2019, 12, 25. [Google Scholar] [CrossRef]
- Malik, R.; Wiedau, M. Therapeutic Approaches Targeting Protein Aggregation in Amyotrophic Lateral Sclerosis. Front. Mol. Neurosci. 2020, 13, 98. [Google Scholar] [CrossRef] [PubMed]
- Milligan, C.; Atassi, N.; Babu, S.; Barohn, R.J.; Caress, J.B.; Cudkowicz, M.E.; Evora, A.; Hawkins, G.A.; Wosiski-Kuhn, M.; Macklin, E.A.; et al. Tocilizumab is safe and tolerable and reduces C-reactive protein concentrations in the plasma and cerebrospinal fluid of ALS patients. Muscle Nerve 2021, 64, 309–320. [Google Scholar] [CrossRef]
- Wood, H. TNF—a potential therapeutic target for ALS. Nat. Rev. Neurol. 2022, 18, 317. [Google Scholar] [CrossRef]
- Ou, W.; Yang, J.; Simanauskaite, J.; Choi, M.; Castellanos, D.M.; Chang, R.; Sun, J.; Jagadeesan, N.; Parfitt, K.D.; Cribbs, D.H.; et al. Biologic TNF-α inhibitors reduce microgliosis, neuronal loss, and tau phosphorylation in a transgenic mouse model of tauopathy. J. Neuroinflammation 2021, 18, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Bartl, S.; Oueslati, A.; Southwell, A.L.; Siddu, A.; Parth, M.; David, L.S.; Maxan, A.; Salhat, N.; Burkert, M.; Mairhofer, A.; et al. Inhibiting cellular uptake of mutant huntingtin using a monoclonal antibody: Implications for the treatment of Huntington’s disease. Neurobiol. Dis. 2020, 141, 104943. [Google Scholar] [CrossRef]
- Margulis, B.A.; Vigont, V.; Lazarev, V.F.; Kaznacheyeva, E.V.; Guzhova, I.V. Pharmacological protein targets in polyglutamine diseases: Mutant polypeptides and their interactors. FEBS Lett. 2013, 587, 1997–2007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minakawa, E.N.; Nagai, Y. Protein Aggregation Inhibitors as Disease-Modifying Therapies for Polyglutamine Diseases. Front. Neurosci. 2021, 15, 621996. [Google Scholar] [CrossRef] [PubMed]
- Sirbu, C.; Ghinescu, M.; Axelerad, A.; Sirbu, A.M.; Ionita-Radu, F. A new era for monoclonal antibodies with applications in neurology (Review). Exp. Ther. Med. 2020, 21, 1. [Google Scholar] [CrossRef]
- Hampel, H.; Hardy, J.; Blennow, K.; Chen, C.; Perry, G.; Kim, S.H.; Villemagne, V.L.; Aisen, P.; Vendruscolo, M.; Iwatsubo, T.; et al. The Amyloid-β Pathway in Alzheimer’s Disease. Mol. Psychiatry. 2021, 26, 5481–5503. [Google Scholar] [CrossRef]
- Pasieka, A.; Panek, D.; Szałaj, N.; Espargaró, A.; Więckowska, A.; Malawska, B.; Sabaté, R.; Bajda, M. Dual Inhibitors of Amyloid-β and Tau Aggregation with Amyloid-β Disaggregating Properties: Extended in Cellulo, in Silico, and Kinetic Studies of Multifunctional Anti-Alzheimer’s Agents. ACS Chem. Neurosci. 2021, 12, 2057–2068. [Google Scholar] [CrossRef]
- Jang, D.I.; Lee, A.H.; Shin, H.Y.; Song, H.R.; Park, J.H.; Kang, T.B.; Lee, S.R.; Yang, S.H. The role of tumor necrosis factor alpha (Tnf-α) in autoimmune disease and current tnf-α inhibitors in therapeutics. Int. J. Mol. Sci. 2021, 22, 2719. [Google Scholar] [CrossRef]
- Hu, Y.; Huang, Z.; Yang, S.; Chen, X.; Su, W.; Liang, D. Effectiveness and safety of anti-tumor necrosis factor-alpha agents treatment in behcets’ disease-associated uveitis: A systematic review and meta-analysis. Front. Pharmacol. 2020, 11, 941. [Google Scholar] [CrossRef]
- Khanna, D.; McMahon, M.; Furst, D.E. Safety of tumour necrosis factor-α antagonists. Drug Saf. 2004, 27, 307–324. [Google Scholar] [CrossRef]
- Carreón Guarnizo, E.; Hernández Clares, R.; Castillo Triviño, T.; Meca Lallana, V.; Arocas Casañ, V.; Iniesta Martínez, F.; Olascoaga Urtaza, J.; Meca Lallana, J.E. Experience with tocilizumab in patients with neuromyelitis optica spectrum disorders. Neurol. (Engl. Ed.) 2022, 37, S0213–S4853. [Google Scholar] [CrossRef] [PubMed]
- Cabreira, V.; Dias, L.; Fernandes, B.; Aires, A.; Guimarães, J.; Abreu, P.; Azevedo, E. Tocilizumab for severe refractory primary central nervous system vasculitis: A center experience. Acta Neurol. Scand. 2022, 145, 479–483. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Li, L.; Wang, Q.; Jiang, F.; Zhang, P.; Guo, F.; Liu, H.; Huang, J. A Novel Humanized Anti-Interleukin-6 Antibody HZ0408b With Anti-Rheumatoid Arthritis Therapeutic Potential. Front. Immunol. 2022, 12, 816646. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Neurodegenerative Disease | Molecular Target | Proposed Classes of Therapeutic Agents |
|---|---|---|
| Alzheimer’s disease | Aβ | mAbs, aptamers [74,75,76,77,78,79,80] |
| Enzymes [24] | ||
| Albumin [81,82] | ||
| Protein conformation stabilizers and aggregation inhibitors [81,82,83,84] | ||
| Tau protein | mAbs, aptamers [85,86] | |
| Protein conformation stabilizers and aggregation inhibitors [87,88] | ||
| sTREM2 | mAbs, aptamers [89,90] | |
| IL-6 | mAbs [91] | |
| TNF-α | fusion protein by recombinant DNA, mAb [92,93,94,95] | |
| Parkinson’s disease and Dementia with Lewy bodies | α-synuclein | mAbs, aptamers [58,86,96,97] |
| Enzymes [98] | ||
| Protein conformation stabilizers and aggregation inhibitors [83,99] | ||
| IL-6 | mAbs [100] | |
| TNF-α | mAbs [101] | |
| Multisystem Atrophy | α-synuclein | mAbs, aptamers [58,86,96,97] |
| Protein conformation stabilizers and aggregation inhibitors [83,99] | ||
| Enzymes [98] | ||
| Progressive supranuclear palsy | Tau | mAbs, aptamers [102,103] |
| Protein conformation stabilizers and aggregation inhibitors [104] | ||
| Frontotemporal dementia | TDP43 | mAbs, aptamers [105] |
| Tau protein | mAbs, aptamers [85] | |
| Protein conformation stabilizers and aggregation inhibitors [104] | ||
| Amyotrophic lateral sclerosis | SOD | mAbs, aptamers [86] |
| Protein conformation stabilizers and aggregation inhibitors [86,106,107] | ||
| TDP43 | mAbs, aptamers [108] | |
| Enzymes [109] | ||
| Protein conformation stabilizers and aggregation inhibitors [110,111] | ||
| Tau protein | mAbs, aptamers [85] | |
| Protein conformation stabilizers and aggregation inhibitors [104] | ||
| IL-6 | mAbs [112] | |
| TNF-α | mAbs [113,114] | |
| Huntington’s disease and other diseases caused by polynucleotide-mutated repeats | mutant HTT protein and other polyQ-mutated proteins | mAbs, aptamers [115] |
| Protein conformation stabilizers and aggregation inhibitors [116,117] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manuel, M.-G.; Tamba, B.-I.; Leclere, M.; Mabrouk, M.; Schreiner, T.-G.; Ciobanu, R.; Cristina, T.-Z. Intrathecal Pseudodelivery of Drugs in the Therapy of Neurodegenerative Diseases: Rationale, Basis and Potential Applications. Pharmaceutics 2023, 15, 768. https://doi.org/10.3390/pharmaceutics15030768
Manuel M-G, Tamba B-I, Leclere M, Mabrouk M, Schreiner T-G, Ciobanu R, Cristina T-Z. Intrathecal Pseudodelivery of Drugs in the Therapy of Neurodegenerative Diseases: Rationale, Basis and Potential Applications. Pharmaceutics. 2023; 15(3):768. https://doi.org/10.3390/pharmaceutics15030768
Chicago/Turabian StyleManuel, Menéndez-González, Bogdan-Ionel Tamba, Maxime Leclere, Mostafa Mabrouk, Thomas-Gabriel Schreiner, Romeo Ciobanu, and Tomás-Zapico Cristina. 2023. "Intrathecal Pseudodelivery of Drugs in the Therapy of Neurodegenerative Diseases: Rationale, Basis and Potential Applications" Pharmaceutics 15, no. 3: 768. https://doi.org/10.3390/pharmaceutics15030768