
A Sustainable Solution to Skin Diseases: Ecofriendly Transdermal Patches

Abstract
:1. Introduction
2. Skin Diseases
2.1. Diabetic Wound
2.2. Skin Cancer
2.3. Psoriasis
2.4. Microbial and Viral Infections
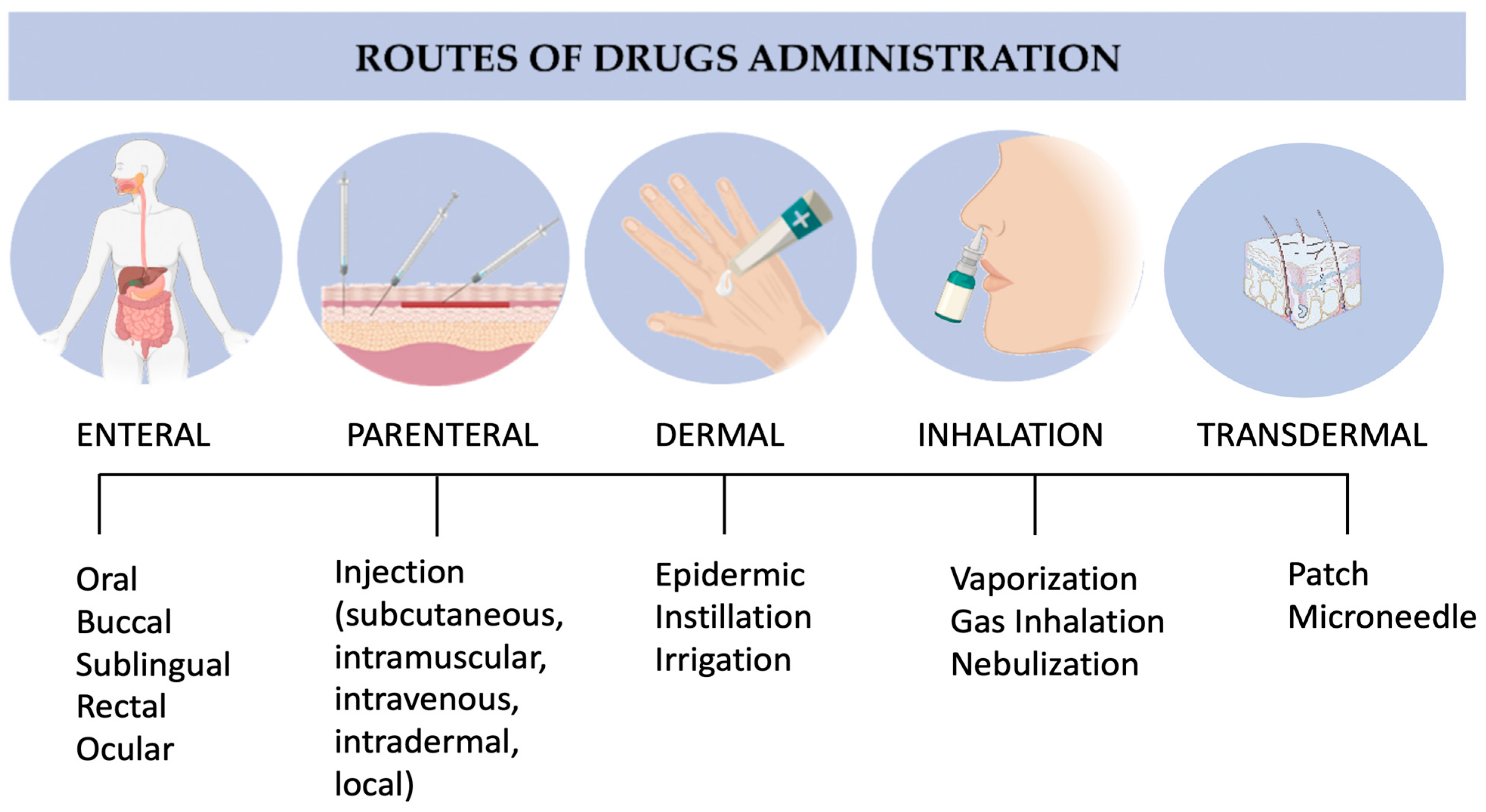
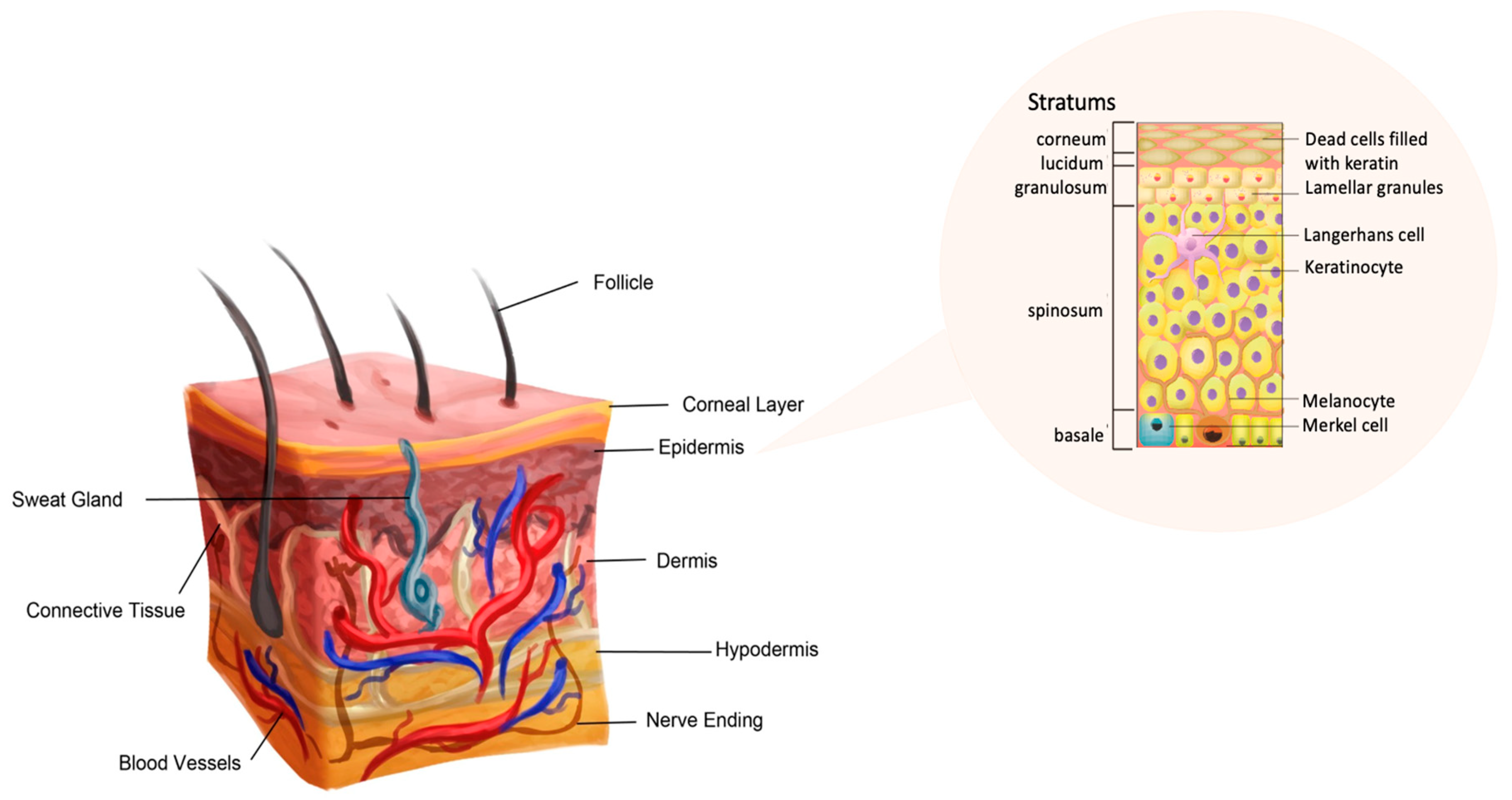
3. Dermal and Transdermal Drug Delivery and Design Parameters for Patches
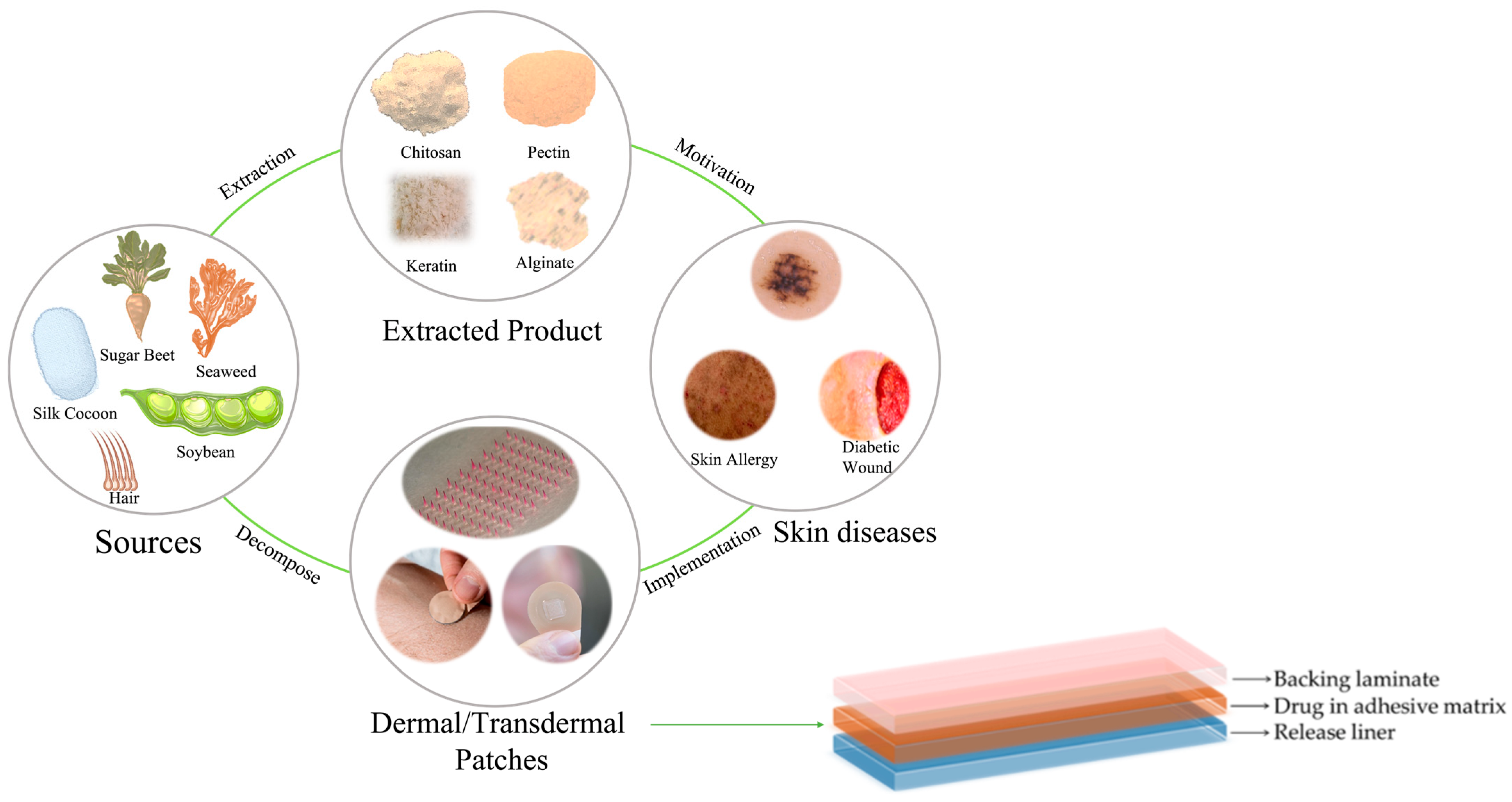
4. Sustainable Materials for Dermal and Transdermal Patches
4.1. Silk Fibroin
4.2. Chitosan/Chitin
4.3. Alginate
4.4. Keratin
4.5. Gelatin
4.6. Cellulose
4.7. Hyaluronic Acid
4.8. Pectin
4.9. Collagen
5. Commercial Products
6. Conclusions and Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gallo, R.L. Human skin is the largest epithelial surface for interaction with microbes. J. Investig. Dermatol. 2017, 137, 1213–1214. [Google Scholar] [CrossRef]
- Lehtimäki, J.; Sinkko, H.; Hielm-Björkman, A.; Salmela, E.; Tiira, K.; Laatikainen, T.; Mäkeläinen, S.; Kaukonen, M.; Uusitalo, L.; Hanski, I.; et al. Skin microbiota and allergic symptoms associate with exposure to environmental microbes. Proc. Natl. Acad. Sci. USA 2018, 115, 4897–4902. [Google Scholar] [CrossRef]
- Hay, R.J.; Johns, N.E.; Williams, H.C.; Bolliger, I.W.; Dellavalle, R.P.; Margolis, D.J.; Marks, R.; Naldi, L.; Weinstock, M.A.; Wulf, S.K.; et al. The global burden of skin disease in 2010: An analysis of the prevalence and impact of skin conditions. J. Investig. Dermatol. 2014, 134, 1527–1534. [Google Scholar] [CrossRef]
- Bickers, D.R.; Lim, H.W.; Margolis, D.; Weinstock, M.A.; Goodman, C.; Faulkner, E.; Gould, C.; Gemmen, E.; Dall, T. The burden of skin diseases: 2004: A joint project of the American Academy of Dermatology Association and the Society for Investigative Dermatology. J. Am. Acad. Dermatol. 2006, 55, 490–500. [Google Scholar] [CrossRef]
- Herman, T.F.; Santos, C. First pass effect. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2019. [Google Scholar]
- Sugibayashi, K.; Morimoto, Y. Polymers for transdermal drug delivery systems. J. Control. Release 1994, 29, 177–185. [Google Scholar] [CrossRef]
- Prausnitz, M.R.; Langer, R. Transdermal drug delivery. Nat. Biotechnol. 2008, 26, 1261–1268. [Google Scholar] [CrossRef]
- Prausnitz, M.R. Engineering microneedle patches for vaccination and drug delivery to skin. Annu. Rev. Chem. Biomol. Eng. 2017, 8, 177–200. [Google Scholar] [CrossRef]
- Kurczewska, J. Recent Reports on Polysaccharide-Based Materials for Drug Delivery. Polymers 2022, 14, 4189. [Google Scholar] [CrossRef]
- Nunes, D.; Andrade, S.; Ramalho, M.; Loureiro, J.; Pereira, M.C. Polymeric Nanoparticles-Loaded Hydrogels for Biomedical Applications: A Systematic Review on In Vivo Findings. Polymers 2022, 14, 1010. [Google Scholar] [CrossRef]
- Mathias, N.R.; Hussain, M.A. Non-invasive systemic drug delivery: Developability considerations for alternate routes of administration. J. Pharm. Sci. 2010, 99, 1–20. [Google Scholar] [CrossRef]
- Lee, S.B.; Geroski, D.; Prausnitz, M.; Edelhauser, H.F. Drug delivery through the sclera: Effects of thickness, hydration, and sustained release systems. Exp. Eye Res. 2004, 78, 599–607. [Google Scholar] [CrossRef]
- Li, Y.; Shawgo, R.S.; Tyler, B.; Henderson, P.T.; Vogel, J.S.; Rosenberg, A.; Storm, P.B.; Langer, R.; Brem, H.; Cima, M.J. In vivo release from a drug delivery MEMS device. J. Control. Release 2004, 100, 211–219. [Google Scholar] [CrossRef]
- Prausnitz, M.R.; Mitragotri, S.; Langer, R. Current status and future potential of transdermal drug delivery. Nat. Rev. Drug Discov. 2004, 3, 115–124. [Google Scholar] [CrossRef]
- Yanamandra, S.; Venkatesan, N.; Kadajji, V.; Wang, Z.; Issar, M.; Betageri, G. Proliposomes as a drug delivery system to decrease the hepatic first-pass metabolism: Case study using a model drug. Eur. J. Pharm. Sci. 2014, 64, 26–36. [Google Scholar] [CrossRef]
- Saboktakin, M.R.; Akhyari, S.; Nasirov, F.A. Synthesis and characterization of modified starch/polybutadiene as novel transdermal drug delivery system. Int. J. Biol. Macromol. 2014, 69, 442–446. [Google Scholar] [CrossRef]
- Zhang, H.; Zhang, J.; Streisand, J.B. Oral mucosal drug delivery: Clinical pharmacokinetics and therapeutic applications. Clin. Pharmacokinet. 2002, 41, 661–680. [Google Scholar] [CrossRef]
- Wokovich, A.M.; Prodduturi, S.; Doub, W.; Hussain, A.; Buhse, L.F. Transdermal drug delivery system (TDDS) adhesion as a critical safety, efficacy and quality attribute. Eur. J. Pharm. Biopharm. 2006, 64, 1–8. [Google Scholar] [CrossRef]
- Lopes, C.M.; Bettencourt, C.; Rossi, A.; Buttini, F.; Barata, P. Overview on gastroretentive drug delivery systems for improving drug bioavailability. Int. J. Pharm. 2016, 510, 144–158. [Google Scholar] [CrossRef]
- Gelperina, S.; Kisich, K.; Iseman, M.; Heifets, L. The Potential Advantages of Nanoparticle Drug Delivery Systems in Chemotherapy of Tuberculosis. Am. J. Respir. Crit. Care Med. 2012, 172, 1487–1490. [Google Scholar] [CrossRef]
- Jain, N.K.; Mishra, V.; Mehra, N.K. Targeted drug delivery to macrophages. Expert Opin. Drug Deliv. 2013, 10, 353–367. [Google Scholar] [CrossRef]
- Benson, H.A.E. Transdermal drug delivery: Penetration enhancement techniques. Curr. Drug Deliv. 2005, 2, 23–33. [Google Scholar] [CrossRef]
- Priyanka, K.; Onkar, S. Transdermal Drug Delivery Systems Market by Type of Delivery System (Passive, Active), by Application (Analgesics, Hormone Replacement Therapies, Hypertension, Motion Sickness, Smoking Cessation, Others): Global opportunity Analysis and Industry Forecast; Allied Market Research: Portland, OR, USA, 2022. [Google Scholar]
- Gunatillake, P.A.; Adhikari, R.; Gadegaard, N. Biodegradable synthetic polymers for tissue engineering. Eur. Cells Mater. 2003, 5, 1–16. [Google Scholar] [CrossRef]
- Balart, R.; Montanes, N.; Dominici, F.; Boronat, T.; Torres-Giner, S. Environmentally friendly polymers and polymer composites. Materials 2020, 13, 4892. [Google Scholar] [CrossRef]
- Chi, J.; Zhang, X.; Chen, C.; Shao, C.; Zhao, Y.; Wang, Y. Antibacterial and angiogenic chitosan microneedle array patch for promoting wound healing. Bioact. Mater. 2020, 5, 253–259. [Google Scholar] [CrossRef]
- Latif, M.S.; Azad, A.K.; Nawaz, A.; Rashid, S.A.; Rahman, M.H.; Al Omar, S.Y.; Bungau, S.G.; Aleya, l.; Abdel-Daim, M.M. Ethyl Cellulose and Hydroxypropyl Methyl Cellulose Blended Methotrexate-Loaded Transdermal Patches: In Vitro and Ex Vivo. Polymers 2021, 13, 3455. [Google Scholar] [CrossRef]
- Suksaeree, J.; Maneewattanapinyo, P.; Panrat, K.; Pichayakorn, W.; Monton, C. Solvent-Cast Polymeric Films from Pectin and Eudragit® NE 30D for Transdermal Drug Delivery Systems. J. Polym. Environ. 2021, 29, 3174–3184. [Google Scholar] [CrossRef]
- Zhou, Z.; Xing, M.; Zhang, S.; Yang, G.; Gao, Y. Process optimization of Ca2+ cross-linked alginate-based swellable microneedles for enhanced transdermal permeability: More applicable to acidic drugs. Int. J. Pharm. 2022, 618, 121669. [Google Scholar] [CrossRef]
- Zhang, Y.; Jiang, G.; Yu, W.; Liu, D.; Xu, B. Microneedles fabricated from alginate and maltose for transdermal delivery of insulin on diabetic rats. Mater. Sci. Eng. C 2018, 85, 18–26. [Google Scholar] [CrossRef]
- Chen, Y.J.; Cheng, H.W.; Yen, W.Y.; Tsai, J.H.; Yeh, C.Y.; Chen, C.J.; Liu, J.T.; Chen, S.Y.; Chang, S.J. The Treatment of Keloid Scars via Modulating Heterogeneous Gelatin-Structured Composite Microneedles to Control Transdermal Dual-Drug Release. Polymers 2022, 14, 4436. [Google Scholar] [CrossRef]
- Pineda-Álvarez, R.A.; Bernad-Bernad, M.; Rodríguez-Cruz, I.; Escobar-Chávez, J.J. Development and characterization of starch/gelatin microneedle arrays loaded with lecithin–gelatin nanoparticles of losartan for transdermal delivery. J. Pharm. Innov. 2022, 17, 71–84. [Google Scholar] [CrossRef]
- Bechelli, S.; Delhommelle, J. Machine Learning and Deep Learning Algorithms for Skin Cancer Classification from Dermoscopic Images. Bioengineering 2022, 9, 97. [Google Scholar] [CrossRef]
- Lázaro-Martínez, J.L.; Álvaro-Afonso, F.; Sevillano-Fernández, D.; García-álvarez, Y.; Sanz-Corbalan, I.; García-Morales, E. Cellular Proliferation, Dermal Repair, and Microbiological Effectiveness of Ultrasound-Assisted Wound Debridement (UAW) Versus Standard Wound Treatment in Complicated Diabetic Foot Ulcers (DFU): An Open-Label Randomized Controlled Trial. J. Clin. Med. 2020, 9, 4032. [Google Scholar] [CrossRef]
- Wang, C.C.Y.; Wu, H.H.L.; Ponnusamy, A.; Pye, I.; Woywodt, A. Pruritus in Chronic Kidney Disease: An Update. Allergies 2022, 2, 87–105. [Google Scholar] [CrossRef]
- O’Shea, J.; Prausnitz, M.; Rouphael, N. Dissolvable Microneedle Patches to Enable Increased Access to Vaccines against SARS-CoV-2 and Future Pandemic Outbreaks. Vaccines 2021, 9, 320. [Google Scholar] [CrossRef]
- Mattiello, S.; Guzzini, A.; Del Giudice, A.; Santulli, C.; Antonini, M.; Lupidi, G.; Gunnella, R. Physico-Chemical Characterization of Keratin from Wool and Chicken Feathers Extracted Using Refined Chemical Methods. Polymers 2023, 15, 181. [Google Scholar] [CrossRef]
- Panonnummal, R.; Kumar, V.; Jayakumar, R.; Sabitha, M. Application of Chitosan and Its Derivatives in Transdermal Drug Delivery. Adv. Polym. Sci. 2021, 288, 411–446. [Google Scholar] [CrossRef]
- Chen, Y.; Xian, Y.; Carrier, A.J.; Youden, B.; Servos, M.; Cui, S.; Luan, T.; Lin, S.; Zhang, X. A simple and cost-effective approach to fabricate tunable length polymeric microneedle patches for controllable transdermal drug delivery. RSC Adv. 2020, 10, 15541–15546. [Google Scholar] [CrossRef]
- Designing Polymeric Nanoparticles for Targeted Drug Delivery System. Available online: https://www.researchgate.net/publication/280858357_Designing_Polymeric_Nanoparticles_for_Targeted_Drug_Delivery_System (accessed on 26 January 2023).
- Maghsoudi, S.; Taghavi Shahraki, B.; Rabiee, N.; Fatahi, Y.; Dinarvand, R.; Tavakolizadeh, M.; Ahmadi, S.; Rabiee, M.; Bagherzadeh, M.; Pourjavadi, A.; et al. Burgeoning Polymer Nano Blends for Improved Controlled Drug Release: A Review. Int. J. Nanomed. 2020, 15, 4363–4392. [Google Scholar] [CrossRef]
- Talebi, N.; Lopes, D.; Lopes, J.; Macário-Soares, A.; Kumar Dan, A.; Ghanbari, R.; Kahkesh, K.H.; Peixoto, D.; Giram, P.S.; Raza, F.; et al. Natural polymeric nanofibers in transdermal drug delivery. Appl. Mater. Today 2023, 30, 101726. [Google Scholar] [CrossRef]
- Srivastava, P.; Kalam, S.A. Natural Polymers as Potential Antiaging Constituents. In Pharmacognosy Medicinal Plants; InTech Open: London, UK, 2019. [Google Scholar] [CrossRef] [Green Version]
- Gaur, M.; Dobke, M.; Lunyak, V.V. Mesenchymal Stem Cells from Adipose Tissue in Clinical Applications for Dermatological Indications and Skin Aging. Int. J. Mol. Sci. 2017, 18, 208. [Google Scholar] [CrossRef]
- Vig, K.; Chaudhari, A.; Tripathi, S.; Dixit, S.; Sahu, R.; Pillai, S.; Dennis, V.A.; Singh, S.R. Advances in Skin Regeneration Using Tissue Engineering. Int. J. Mol. Sci. 2017, 18, 789. [Google Scholar] [CrossRef] [PubMed]
- Sampaio, A.L.; Bressan, A.; Vasconcelos, B.; Gri, A.C. Skin manifestations associated with systemic diseases—Part I. An. Bras. Dermatol. 2021, 96, 655–671. [Google Scholar] [CrossRef] [PubMed]
- Leal, J.M.; de Souza, G.; de Marsillac, P.; Gri, A.C. Skin manifestations associated with systemic diseases—Part II. An. Bras. Dermatol. 2021, 96, 672. [Google Scholar] [CrossRef] [PubMed]
- Franks, A.G. Skin Manifestations of Internal Disease. Med. Clin. N. Am. 2009, 93, 1265–1282. [Google Scholar] [CrossRef] [PubMed]
- Seth, D.; Cheldize, K.; Brown, D.; Freeman, E.E. Global Burden of Skin Disease: Inequities and Innovations. Curr. Dermatol. Rep. 2017, 6, 204. [Google Scholar] [CrossRef]
- Dolz-Pérez, I.; Sallam, M.A.; Masiá, E.; Morelló-Bolumar, D.; Pérez Del Caz, M.D.; Graff, P.; Abdelmonsif, D.; Hedtrich, S.; Nebot, V.J.; Vicent, M.J. Polypeptide-corticosteroid conjugates as a topical treatment approach to psoriasis. J. Control. Release 2020, 318, 210–222. [Google Scholar] [CrossRef]
- Youn, C.; Archer, N.; Miller, L.S. Research Techniques Made Simple: Mouse Bacterial Skin Infection Models for Immunity Research. J. Investig. Dermatol. 2020, 140, 1488–1497.e1. [Google Scholar] [CrossRef]
- Vijayakumar, V.; Samal, S.; Mohanty, S.; Nayak, S.K. Recent advancements in biopolymer and metal nanoparticle-based materials in diabetic wound healing management. Int. J. Biol. Macromol. 2019, 122, 137–148. [Google Scholar] [CrossRef]
- Khan, N.H.; Mir, M.; Qian, L.; Baloch, M.; Ali Khan, M.F.; Rehman, A.U.; Ngowi, E.E.; Wu, D.D.; Ji, X.Y. Skin cancer biology and barriers to treatment: Recent applications of polymeric micro/nanostructures. J. Adv. Res. 2021, 36, 223–247. [Google Scholar] [CrossRef]
- Cho, N.H.; Shaw, J.E.; Karuranga, S.; Huang, Y.; da Rocha Fernandes, J.D.; Ohlrogge, A.W.; Malanda, B. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res. Clin. Pract. 2018, 138, 271–281. [Google Scholar] [CrossRef]
- Spampinato, S.F.; Caruso, G.; de Pasquale, R.; Sortino, M.; Merlo, S. The Treatment of Impaired Wound Healing in Diabetes: Looking among Old Drugs. Pharmaceuticals 2020, 13, 60. [Google Scholar] [CrossRef]
- Geraghty, T.; LaPorta, G. Current health and economic burden of chronic diabetic osteomyelitis. Expert Rev. Pharmacoecon. Outcomes Res. 2019, 19, 279–286. [Google Scholar] [CrossRef]
- Boulton, A.J.; Vileikyte, L.; Ragnarson-Tennvall, G.; Apelqvist, J. The global burden of diabetic foot disease. Lancet 2005, 366, 1719–1724. [Google Scholar] [CrossRef]
- Moura, L.I.F.; Dias, A.; Carvalho, E.; de Sousa, H.C. Recent advances on the development of wound dressings for diabetic foot ulcer treatment—A review. Acta Biomater. 2013, 9, 7093–7114. [Google Scholar] [CrossRef]
- Gianino, E.; Miller, C.; Gilmore, J. Smart Wound Dressings for Diabetic Chronic Wounds. Bioengineering 2018, 5, 51. [Google Scholar] [CrossRef]
- Salazar, J.J.; Ennis, W.; Koh, T.J. Diabetes medications: Impact on inflammation and wound healing. J. Diabetes Complicat. 2016, 30, 746–752. [Google Scholar] [CrossRef]
- Barrientos, S.; Stojadinovic, O.; Golinko, M.; Brem, H.; Tomic-Canic, M. Growth factors and cytokines in wound healing. Wound Repair Regen. 2008, 16, 585–601. [Google Scholar] [CrossRef]
- Apalla, Z.; Nashan, D.; Weller, R.; Castellsagué, X. Skin Cancer: Epidemiology, Disease Burden, Pathophysiology, Diagnosis, and Therapeutic Approaches. Dermatol. Ther. 2017, 7 (Suppl. 1), 5–9. [Google Scholar] [CrossRef]
- Gruber, P.; Shah, M.; Zito, P.M. Skin Cancer. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK441949/ (accessed on 26 November 2022).
- Pavel, T.I.; Chircov, C.; Rădulescu, M.; Grumezescu, A.M. Regenerative Wound Dressings for Skin Cancer. Cancers 2020, 12, 2954. [Google Scholar] [CrossRef]
- Kim, W.B.; Jerome, D.; Yeung, J. Diagnosis and management of psoriasis. Can. Fam. Physician 2017, 63, 278. Available online: https://pmc/articles/PMC5389757/ (accessed on 27 November 2022).
- Rendon, A.; Schäkel, K. Psoriasis Pathogenesis and Treatment. Int. J. Mol. Sci. 2019, 20, 1475. [Google Scholar] [CrossRef] [PubMed]
- Xue, Y.; Zhou, J.; Xu, B.N.; Li, Y.; Bao, W.; Cheng, X.L.; He, Y.; Xu, C.P.; Ren, J.; Zheng, Y.R.; et al. Global Burden of Bacterial Skin Diseases: A Systematic Analysis Combined with Sociodemographic Index, 1990–2019. Front. Med. 2022, 9, 875. [Google Scholar] [CrossRef] [PubMed]
- Jamaledin, R.; Yiu, C.K.; Zare, E.N.; Zhen, G.; Niu, L.-N.; Vecchione, R.; Chen, G.; Gu, Z.; Tay, F.R.; Makvandi, P. Advances in Antimicrobial Microneedle Patches for Combating Infections. Adv. Mater. 2020, 32, 2002129. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.; Russo, J.; Fiegel, J.; Brogden, N. Antibiotic Delivery Strategies to Treat Skin Infections When Innate Antimicrobial Defense Fails. Antibiotics 2020, 9, 56. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira, D.M.P.; Forde, B.M.; Kidd, T.J.; Harris, P.N.A.; Schembri, M.A.; Beatson, S.A.; Paterson, D.L.; Walker, M.J. Antimicrobial Resistance in ESKAPE Pathogens. Clin. Microbiol. Rev. 2020, 33, e00181-19. [Google Scholar] [CrossRef] [PubMed]
- Patrulea, V.; Borchard, G.; Jordan, O. An Update on Antimicrobial Peptides (AMPs) and Their Delivery Strategies for Wound Infections. Pharmaceutics 2020, 12, 840. [Google Scholar] [CrossRef]
- Rukavina, Z.; Klarić, M.Š.; Filipović-Grčić, J.; Lovrić, J.; Vanić, Ž. Azithromycin-loaded liposomes for enhanced topical treatment of methicillin-resistant Staphyloccocus aureus (MRSA) infections. Int. J. Pharm. 2018, 553, 109–119. [Google Scholar] [CrossRef]
- Dabija, D.; Tadi, P.; Danosos, G.N. Chronic urticaria. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK555910/ (accessed on 24 November 2022).
- Wang, F.-Y.; Chen, Y.; Huang, Y.-Y.; Cheng, C.-M. Transdermal drug delivery systems for fighting common viral infectious diseases. Drug Deliv. Transl. Res. 2021, 11, 1498–1508. [Google Scholar] [CrossRef]
- Almehmady, A.M.; Ali, S.A. Transdermal Film Loaded with Garlic Oil-Acyclovir Nanoemulsion to Overcome Barriers for Its Use in Alleviating Cold Sore Conditions. Pharmaceutics 2021, 13, 669. [Google Scholar] [CrossRef]
- Bader, M.S. Herpes zoster: Diagnostic, therapeutic, and preventive approaches. Postgrad. Med. 2013, 125, 78–91. [Google Scholar] [CrossRef]
- Garg, U.; Id, K.; Jain, I.D. Dermal and Transdermal Drug Delivery through Vesicles and Particles: Preparation and Applications. Adv. Pharm. Bull. 2022, 2022, 45–57. [Google Scholar] [CrossRef]
- Gugleva, V.; Ivanova, N.; Sotirova, Y.; Andonova, V. Dermal Drug Delivery of Phytochemicals with Phenolic Structure via Lipid-Based Nanotechnologies. Pharmaceuticals 2021, 14, 837. [Google Scholar] [CrossRef]
- Kolimi, P.; Narala, S.; Youssef, A.; Nyavanandi, D.; Dudhipala, N. A systemic review on development of mesoporous nanoparticles as a vehicle for transdermal drug delivery. Nanotheranostics 2023, 7, 70–89. [Google Scholar] [CrossRef]
- Ibaraki, H.; Kanazawa, T.; Oogi, C.; Takashima, Y.; Seta, Y. Effects of surface charge and flexibility of liposomes on dermal drug delivery. J. Drug Deliv. Sci. Technol. 2019, 50, 155–162. [Google Scholar] [CrossRef]
- Mishra, D.K.; Pandey, V.; Maheshwari, R.; Ghode, P.; Tekade, R.K. Cutaneous and Transdermal Drug Delivery: Techniques and Delivery Systems. In Basic Fundamentals of Drug Delivery; Academic Press: Cambridge, MA, USA, 2019; pp. 595–650. [Google Scholar] [CrossRef]
- Phatale, V.; Vaiphei, K.; Jha, S.; Patil, D.; Agrawal, M.; Alexander, A. Overcoming skin barriers through advanced transdermal drug delivery approaches. J. Control. Release 2022, 351, 361–380. [Google Scholar] [CrossRef]
- Pastore, M.N.; Kalia, Y.; Horstmann, M.; Roberts, M.S. Transdermal patches: History, development and pharmacology. Br. J. Pharmacol. 2015, 172, 2179–2209. [Google Scholar] [CrossRef]
- Dhiman, S.; Singh, T.; Rehni, A.K. Transdermal patches: A recent approach to new drug delivery system. Int. J. Pharm. Pharm. Sci. 2011, 3, 26–34. [Google Scholar]
- Gomaa, Y.; Prausnitz, M.R. Delivery of Drugs, Vaccines, and Cosmeceuticals to Skin Using Microneedle Patches. In Percutaneous Absorption; Taylor Francis: Abingdon, UK, 2021; pp. 585–608. [Google Scholar] [CrossRef]
- Lee, J.W.; Han, M.; Park, J.H. Polymer microneedles for transdermal drug delivery. J. Drug Target. 2013, 21, 211–223. [Google Scholar] [CrossRef]
- al Hanbali, O.A.; Khan, H.; Sarfraz, M.; Arafat, M.; Ijaz, S.; Hameed, A. Transdermal patches: Design and current approaches to painless drug delivery. Acta Pharm. 2019, 69, 197–215. [Google Scholar] [CrossRef] [Green Version]
- Godin, B.; Touitou, E. Dermal and Transdermal Delivery. In Encyclopedia of Nanotechnology; Springer: Dordrecht, The Netherlands, 2012; pp. 517–526. [Google Scholar] [CrossRef]
- Li, Q.Y.; Zhang, J.; Chen, B.; Wang, Q.; Guo, X.D. A solid polymer microneedle patch pretreatment enhances the permeation of drug molecules into the skin. RSC Adv. 2017, 7, 15408–15415. [Google Scholar] [CrossRef]
- Hwang, I.; Kim, H.N.; Seong, M.; Lee, S.H.; Kang, M.; Yi, H.; Bae, W.G.; Kwak, M.K.; Jeong, H.E. Multifunctional smart skin adhesive patches for advanced health care. Adv. Healthc. Mater. 2018, 7, 1800275. [Google Scholar] [CrossRef] [PubMed]
- Cilurzo, F.; Gennari, C.; Minghetti, P. Adhesive properties: A critical issue in transdermal patch development. Expert Opin. Drug Deliv. 2012, 9, 33–45. [Google Scholar] [CrossRef] [PubMed]
- Patel, D.; Chaudhary, S.; Parmar, B.; Bhura, N. Transdermal drug delivery system: A review. Pharm. Innov. 2012, 1, 66. [Google Scholar] [CrossRef]
- Mukherjee, B.; Mahapatra, S.; Gupta, R.; Patra, B.; Tiwari, A.; Arora, P. A comparison between povidone-ethylcellulose and povidone-eudragit transdermal dexamethasone matrix patches based on in vitro skin permeation. Eur. J. Pharm. Biopharm. 2005, 59, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Thimmasetty, J.; Pandey, G.; Babu, P.R. Design and in vivo evaluation of carvedilol buccal mucoadhesive patches. Pak. J. Pharm. Sci. 2008, 21, 241–248. [Google Scholar] [PubMed]
- Chattopadhyay, P.; Dhiman, S.; Borah, S.; Rabha, B.; Chaurasia, A.; Veer, V. Essential oil based polymeric patch development and evaluating its repellent activity against mosquitoes. Acta Trop. 2015, 147, 45–53. [Google Scholar] [CrossRef]
- Gill, H.S.; Prausnitz, M.R. Coated microneedles for transdermal delivery. J. Control. Release 2007, 117, 227–237. [Google Scholar] [CrossRef]
- Erdem, Ö.; Eş, I.; Akceoglu, G.; Saylan, Y.; Inci, F. Recent Advances in Microneedle-Based Sensors for Sampling, Diagnosis and Monitoring of Chronic Diseases. Biosensors 2021, 11, 296. [Google Scholar] [CrossRef]
- Qi, Y.; Wang, H.; Wei, K.; Yang, Y.; Zheng, R.Y.; Kim, I.S.; Zhang, K.Q. A Review of Structure Construction of Silk Fibroin Biomaterials from Single Structures to Multi-Level Structures. Int. J. Mol. Sci. 2017, 18, 237. [Google Scholar] [CrossRef]
- Alheib, O.; da Silva, L.; Youn, Y.; Kwon, I.; Reis, R.; Correlo, V.M. 3D bioprinting: A step forward in creating engineered human tissues and organs. In Additive Manufacturing; Elsevier: Amsterdam, The Netherlands, 2021; pp. 599–633. [Google Scholar] [CrossRef]
- Lujerdean, C.; Baci, G.; Cucu, A.; Dezmirean, D.S. The Contribution of Silk Fibroin in Biomedical Engineering. Insects 2022, 13, 286. [Google Scholar] [CrossRef]
- Cheng, Y.; Koh, L.; Li, D.; Ji, B.; Han, M.; Zhang, Y.W. On the strength of β-sheet crystallites of Bombyx mori silk fibroin. J. R. Soc. Interface 2014, 11, 20140305. [Google Scholar] [CrossRef]
- Kaushik, S.; Thungon, P.; Goswami, P. Silk Fibroin: An Emerging Biocompatible Material for Application of Enzymes and Whole Cells in Bioelectronics and Bioanalytical Sciences. ACS Biomater. Sci. Eng. 2020, 6, 4337–4355. [Google Scholar] [CrossRef]
- Cao, Y.; Wang, B. Biodegradation of Silk Biomaterials. Int. J. Mol. Sci. 2009, 10, 1514. [Google Scholar] [CrossRef]
- Tomeh, M.A.; Hadianamrei, R.; Zhao, X. Silk Fibroin as a Functional Biomaterial for Drug and Gene Delivery. Pharmaceutics 2019, 11, 494. [Google Scholar] [CrossRef]
- Qi, Z.; Cao, J.; Tao, X.; Wu, X.; Kundu, S.; Lu, S. Silk Fibroin Microneedle Patches for the Treatment of Insomnia. Pharmaceutics 2021, 13, 2198. [Google Scholar] [CrossRef]
- Rojas, J.E.U.; de Oliveira, V.L.; de Araujo, D.R.; Tofoli, G.R.; de Oliveira, M.M.; Carastan, D.J.; Palaci, M.; Giuntini, F.; Alves, A.A. Silk Fibroin/Poly(vinyl Alcohol) Microneedles as Carriers for the Delivery of Singlet Oxygen Photosensitizers. ACS Biomater. Sci. Eng. 2022, 8, 128–139. [Google Scholar] [CrossRef]
- Lin, Z.; Li, Y.; Meng, G.; Hu, X.; Zeng, Z.; Zhao, B.; Lin, N.; Liu, X.Y. Reinforcement of Silk Microneedle Patches for Accurate Transdermal Delivery. Biomacromolecules 2021, 22, 5319–5326. [Google Scholar] [CrossRef]
- Bhattarai, N.; Gunn, J.; Zhang, M. Chitosan-based hydrogels for controlled, localized drug delivery. Adv. Drug Deliv. Rev. 2010, 62, 83–99. [Google Scholar] [CrossRef]
- Ahmadi, F.; Oveisi, Z.; Samani, M.; Amoozgar, Z. Chitosan based hydrogels: Characteristics and pharmaceutical applications. Res. Pharm. Sci. 2015, 10, 1–16. Available online: https://pmc/articles/PMC4578208/ (accessed on 25 January 2023).
- Norbury, W.; Herndon, D.; Tanksley, J.; Jeschke, M.; Finnerty, C.C. Infection in Burns. Surg. Infect. 2016, 17, 250–255. [Google Scholar] [CrossRef]
- Boucard, N.; Viton, C.; Agay, D.; Mari, E.; Roger, T.; Chancerelle, Y.; Domard, A. The use of physical hydrogels of chitosan for skin regeneration following third-degree burns. Biomaterials 2007, 28, 3478–3488. [Google Scholar] [CrossRef] [PubMed]
- Waibel, K.H.; Haney, B.; Moore, M.; Whisman, B.; Gomez, R. Safety of Chitosan Bandages in Shellfish Allergic Patients. Mil. Med. 2011, 176, 1153–1156. [Google Scholar] [CrossRef] [PubMed]
- Colobatiu, L.; Gavan, A.; Potarniche, A.V.; Rus, V.; Diaconeasa, Z.; Mocan, A.; Tomuta, I.; Mirel, S.; Mihaiu, M. Evaluation of bioactive compounds-loaded chitosan films as a novel and potential diabetic wound dressing material. React. Funct. Polym. 2019, 145, 104369. [Google Scholar] [CrossRef]
- Hao, Y.; Zhao, W.; Zhang, H.; Zheng, W.; Zhou, Q. Carboxymethyl chitosan-based hydrogels containing fibroblast growth factors for triggering diabetic wound healing. Carbohydr. Polym. 2022, 287, 119336. [Google Scholar] [CrossRef] [PubMed]
- Aderibigbe, B.; Buyana, B. Alginate in Wound Dressings. Pharmaceutics 2018, 10, 42. [Google Scholar] [CrossRef]
- He, L.; Shang, Z.; Liu, H.; Yuan, Z. Alginate-Based Platforms for Cancer-Targeted Drug Delivery. Biomed. Res. Int. 2020, 2020, 1487259. [Google Scholar] [CrossRef]
- Capeling, M.M.; Czerwinski, M.; Huang, S.; Tsai, Y.H.; Wu, A.; Nagy, M.S.; Juliar, B.; Sundaram, N.; Song, Y.; Han, W.M.; et al. Nonadhesive Alginate Hydrogels Support Growth of Pluripotent Stem Cell-Derived Intestinal Organoids. Stem Cell Rep. 2019, 12, 381–394. [Google Scholar] [CrossRef]
- Zhang, M.; Zhao, X. Alginate hydrogel dressings for advanced wound management. Int. J. Biol. Macromol. 2020, 162, 1414–1428. [Google Scholar] [CrossRef]
- Tan, B.; Huang, L.; Wu, Y.; Liao, J. Advances and trends of hydrogel therapy platform in localized tumor treatment: A review. J. Biomed. Mater. Res. A 2021, 109, 404–425. [Google Scholar] [CrossRef]
- Muthulakshmi, L.; Prabakaran, S.; Ramalingam, V.; Rajulu, A.V.; Rajan, M.; Ramakrishna, S.; Luo, H. Sodium alginate nanofibers loaded Terminalia catappa scaffold regulates intrinsic apoptosis signaling in skin melanoma cancer. Process Biochem. 2022, 118, 92–102. [Google Scholar] [CrossRef]
- Chiaoprakobkij, N.; Suwanmajo, T.; Sanchavanakit, N.; Phisalaphong, M. Curcumin-Loaded Bacterial Cellulose/Alginate/Gelatin as A Multifunctional Biopolymer Composite Film. Molecules 2020, 25, 3800. [Google Scholar] [CrossRef]
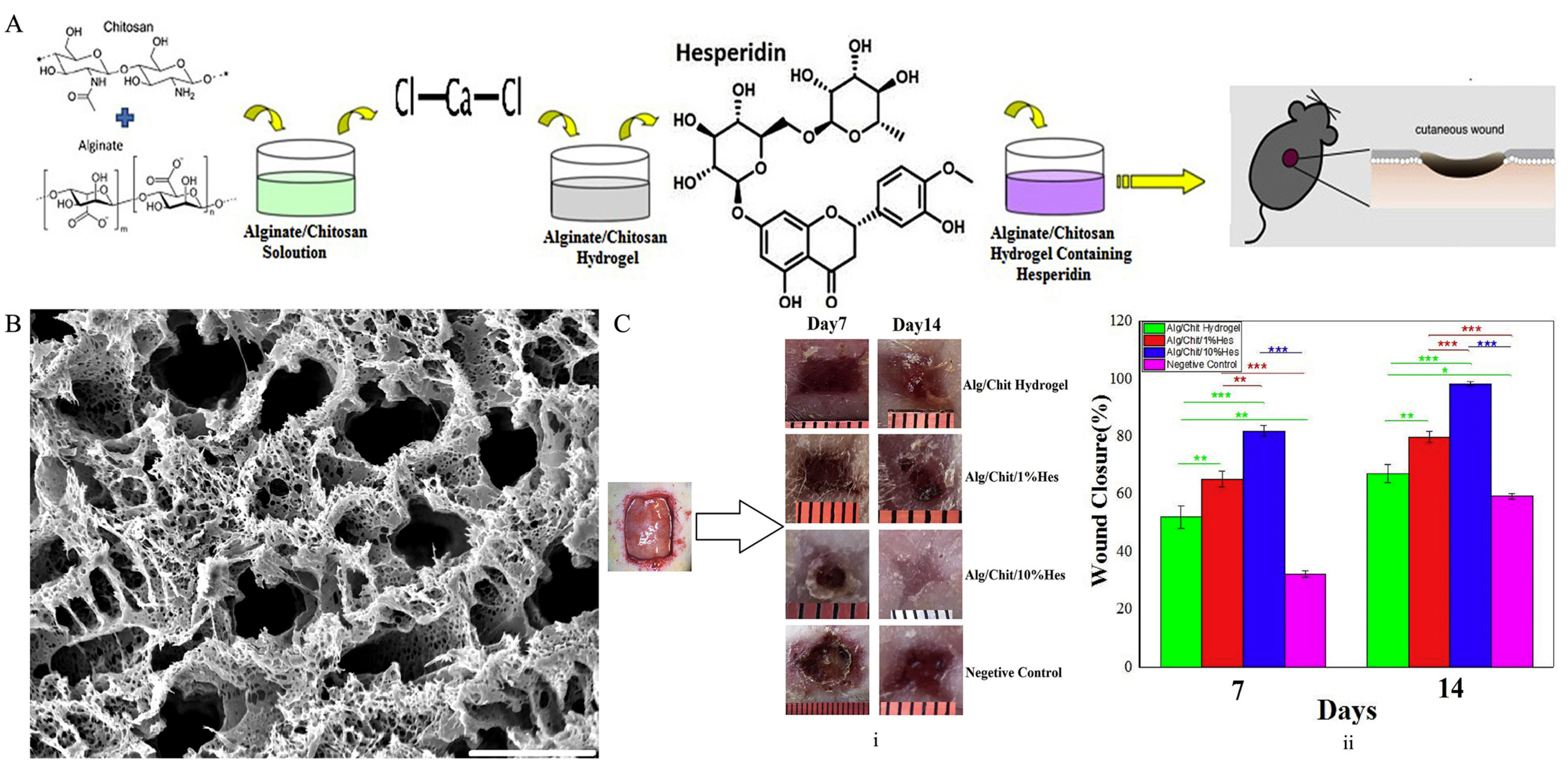
- Bagher, Z.; Ehterami, A.; Safdel, M.H.; Khastar, H.; Semiari, H.; Asefnejad, A.; Davachi, S.M.; Mirzaii, M.; Salehi, M. Wound healing with alginate/chitosan hydrogel containing hesperidin in rat model. J. Drug Deliv. Sci. Technol. 2020, 55, 101379. [Google Scholar] [CrossRef]
- Cleetus, C.M.; Alvarez Primo, F.; Fregoso, G.; Lalitha Raveendran, N.; Noveron, J.C.; Spencer, C.T.; Ramana, C.V.; Joddar, B. Alginate Hydrogels with Embedded ZnO Nanoparticles for Wound Healing Therapy. Int. J. Nanomed. 2020, 15, 5097–5111. [Google Scholar] [CrossRef]
- Feroz, S.; Muhammad, N.; Ranayake, J.; Dias, G. Keratin-based materials for biomedical applications. Bioact. Mater. 2020, 5, 496–509. [Google Scholar] [CrossRef]
- Wang, B.; Yang, W.; McKittrick, J.; Meyers, M.A. Keratin: Structure, mechanical properties, occurrence in biological organisms, and efforts at bioinspiration. Prog. Mater. Sci. 2016, 76, 229–318. [Google Scholar] [CrossRef]
- Lazarus, B.S.; Chadha, C.; Velasco-Hogan, A.; Barbosa, J.; Jasiuk, I.; Meyers, M.A. Engineering with keratin: A functional material and a source of bioinspiration. iScience 2021, 24, 102798. [Google Scholar] [CrossRef]
- Dou, Y.; Zhang, B.; He, M.; Yin, G.; Cui, Y. The structure, tensile properties and water resistance of hydrolyzed feather keratin-based bioplastics. Chin. J. Chem. Eng. 2016, 24, 415–420. [Google Scholar] [CrossRef]
- Fan, J.; Yu, M.Y.; Lei, T.D.; Wang, Y.H.; Cao, F.Y.; Qin, X.; Liu, Y. In Vivo Biocompatibility and Improved Compression Strength of Reinforced Keratin/Hydroxyapatite Scaffold. Tissue Eng. Regen. Med. 2018, 15, 145. [Google Scholar] [CrossRef]
- Nayak, K.K.; Gupta, P. Study of the keratin-based therapeutic dermal patches for the delivery of bioactive molecules for wound treatment. Mater. Sci. Eng. C 2017, 77, 1088–1097. [Google Scholar] [CrossRef]
- Chen, X.; Zhai, D.; Wang, B.; Hao, S.; Song, J.; Peng, Z. Hair keratin promotes wound healing in rats with combined radiation-wound injury. J. Mater. Sci. Mater. Med. 2020, 31, 28. [Google Scholar] [CrossRef]
- Liu, D.; Nikoo, M.; Boran, G.; Zhou, P.; Regenstein, J.M. Collagen and Gelatin. Annu. Rev. Food Sci. Technol. 2015, 6, 527–557. [Google Scholar] [CrossRef] [PubMed]
- Haug, I.J.; Draget, K.I. Gelatin. In Handbook of Hydrocolloids, 2nd ed.; Woodhead Publishing: Sawston, UK, 2009; pp. 142–163. [Google Scholar] [CrossRef]
- Mushtaq, F.; Raza, Z.A.; Batool, S.R.; Zahid, M.; Onder, O.C.; Rafique, A.; Nazeer, M.A. Preparation, properties, and applications of gelatin-based hydrogels (GHs) in the environmental, technological, and biomedical sectors. Int. J. Biol. Macromol. 2022, 218, 601–633. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Zeng, H.; Chen, Z.; Ge, Z.; Wang, B.; Liu, B.; Fan, Z. Sprayable methacrylic anhydride-modified gelatin hydrogel combined with bionic neutrophils nanoparticles for scar-free wound healing of diabetes mellitus. Int. J. Biol. Macromol. 2022, 202, 418–430. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Luo, Z.; Baidya, A.; Kim, H.J.; Wang, C.; Jiang, X.; Qu, M.; Zhu, J.; Ren, L.; Vajhadin, F.; et al. Biodegradable β-Cyclodextrin Conjugated Gelatin Methacryloyl Microneedle for Delivery of Water-Insoluble Drug. Adv. Healthc. Mater. 2020, 9, 2000527. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.H.; Lee, C.H.; Liang, H.K.; Huang, S.C.; Li, J.P.; Lin, C.J.; Chen, J.K. Integrating the microneedles with carboplatin to facilitate the therapeutic effect of radiotherapy for skin cancers. Biomater. Adv. 2022, 141, 213113. [Google Scholar] [CrossRef] [PubMed]
- Wohlert, M.; Benselfelt, T.; Wågberg, L.; Furó, I.; Berglund, L.; Wohlert, J. Cellulose and the role of hydrogen bonds: Not in charge of everything. Cellulose 2022, 29, 1–23. [Google Scholar] [CrossRef]
- Lee, W.J.; Clancy, A.; Kontturi, E.; Bismarck, A.; Shaffer, M.S.P. Strong and stiff: High-performance cellulose nanocrystal/poly(vinyl alcohol) composite fibers. ACS Appl. Mater. Interfaces 2016, 8, 31500–31504. [Google Scholar] [CrossRef] [Green Version]
- Sharif, F.; Muhammad, N.; Zafar, T. Cellulose based biomaterials: Benefits and challenges. In Biofibers and Biopolymers for Biocomposites: Synthesis, Characterization and Properties; Springer: Cham, Switzerland, 2020; pp. 229–246. [Google Scholar] [CrossRef]
- Dutta, S.D.; Patel, D.; Lim, K.T. Functional cellulose-based hydrogels as extracellular matrices for tissue engineering. J. Biol. Eng. 2019, 13, 55. [Google Scholar] [CrossRef]
- Alven, S.; Aderibigbe, B.A. Chitosan and Cellulose-Based Hydrogels for Wound Management. Int. J. Mol. Sci. 2020, 21, 9656. [Google Scholar] [CrossRef]
- de Amorim, J.D.P.; da Silva Junior, C.J.G.; de Medeiros, A.D.M.; do Nascimento, H.A.; Sarubbo, M.; de Medeiros, T.P.M.; Costa, A.F.d.S.; Sarubbo, L.A. Bacterial Cellulose as a Versatile Biomaterial for Wound Dressing Application. Molecules 2022, 27, 5580. [Google Scholar] [CrossRef]
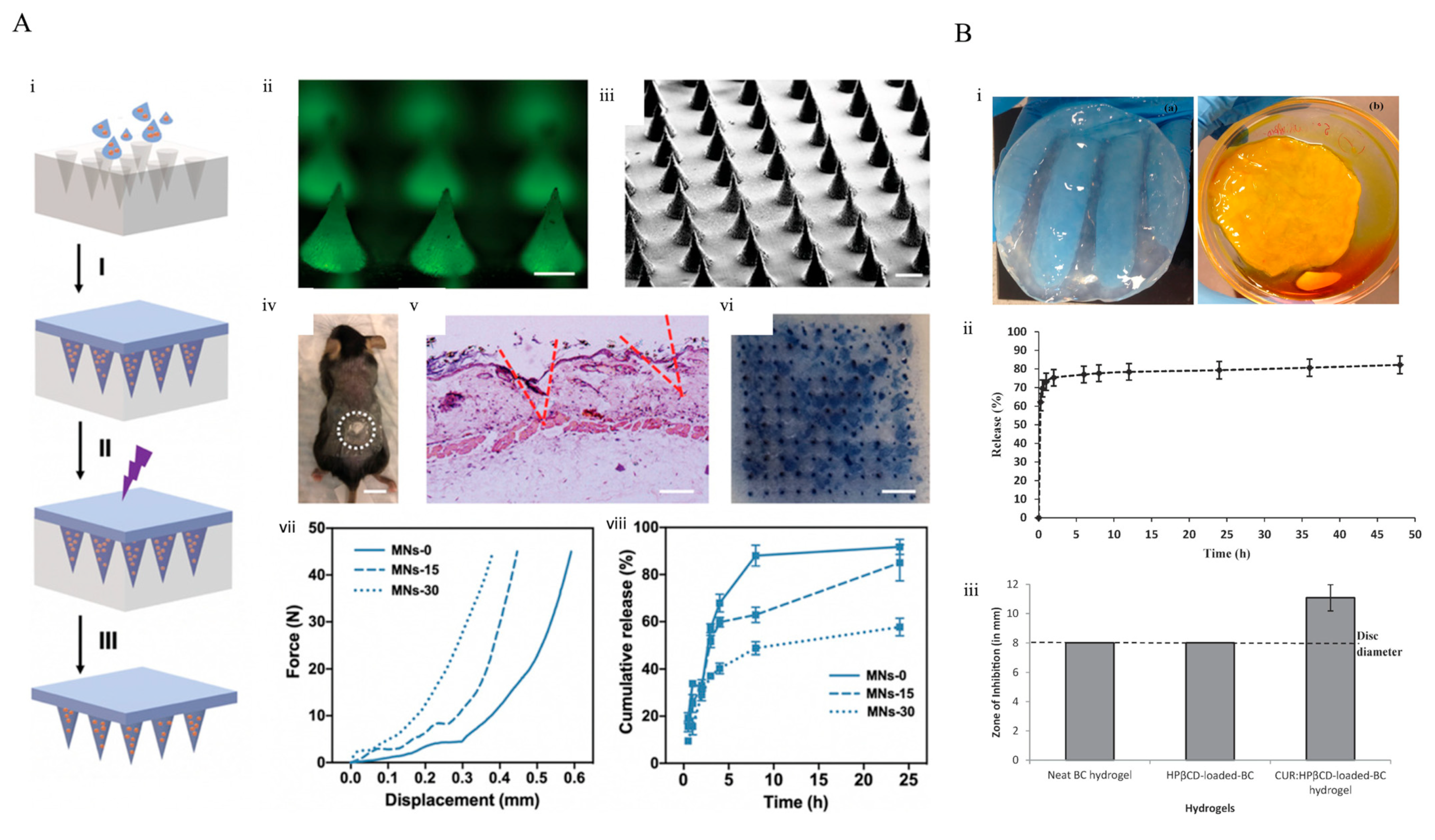
- Gupta, A.; Keddie, D.J.; Kannappan, V.; Gibson, H.; Khalil, I.R.; Kowalczuk, M.; Martin, C.; Shuai, X.; Radecka, I. Production and characterisation of bacterial cellulose hydrogels loaded with curcumin encapsulated in cyclodextrins as wound dressings. Eur. Polym. J. 2019, 118, 437–450. [Google Scholar] [CrossRef]
- Bulpitt, P.; Aeschlimann, D. New strategy for chemical modification of hyaluronic acid: Preparation of functionalized derivatives and their use in the formation of novel biocompatible hydrogels. J. Biomed. Mater. Res. 1999, 47, 152–169. [Google Scholar] [CrossRef]
- Leach, J.B.; Bivens, K.; Patrick, C.; Schmidt, C.E. Photocrosslinked hyaluronic acid hydrogels: Natural, biodegradable tissue engineering scaffolds. Biotechnol. Bioeng. 2003, 82, 578–589. [Google Scholar] [CrossRef]
- Graça, M.F.P.; Miguel, S.; Cabral, C.; Correia, I.J. Hyaluronic acid—Based wound dressings: A review. Carbohydr. Polym. 2020, 241, 116364. [Google Scholar] [CrossRef]
- Du, H.; Liu, P.; Zhu, J.; Lan, J.; Li, Y.; Zhang, L.; Zhu, J.; Tao, J. Hyaluronic Acid-Based Dissolving Microneedle Patch Loaded with Methotrexate for Improved Treatment of Psoriasis. ACS Appl. Mater. Interfaces 2019, 11, 43588–43598. [Google Scholar] [CrossRef]
- Liu, S.; Zhang, Q.; Yu, J.; Shao, N.; Lu, H.; Guo, J.; Qiu, X.; Zhou, D.; Huang, Y. Absorbable Thioether Grafted Hyaluronic Acid Nanofibrous Hydrogel for Synergistic Modulation of Inflammation Microenvironment to Accelerate Chronic Diabetic Wound Healing. Adv. Healthc. Mater. 2020, 9, 2000198. [Google Scholar] [CrossRef]
- Rezvanian, M.; Ng, S.-F.; Alavi, T.; Ahmad, W. In-vivo evaluation of Alginate-Pectin hydrogel film loaded with Simvastatin for diabetic wound healing in Streptozotocin-induced diabetic rats. Int. J. Biol. Macromol. 2021, 171, 308–319. [Google Scholar] [CrossRef]
- Martău, G.A.; Mihai, M.; Vodnar, D.C. The Use of Chitosan, Alginate, and Pectin in the Biomedical and Food Sector—Biocompatibility, Bioadhesiveness, and Biodegradability. Polymers 2019, 11, 1837. [Google Scholar] [CrossRef]
- Liu, L.S.; Fishman, M.; Hicks, K.B. Pectin in controlled drug delivery—A review. Cellulose 2007, 14, 15–24. [Google Scholar] [CrossRef]
- Hasan, N.; Cao, J.; Lee, J.; Kim, H.; Yoo, J.-W. Development of clindamycin-loaded alginate/pectin/hyaluronic acid composite hydrogel film for the treatment of MRSA-infected wounds. J. Pharm. Investig. 2021, 51, 597–610. [Google Scholar] [CrossRef]
- Gazzi, R.P.; Frank, L.; Onzi, G.; Pohlmann, A.; Guterres, S.S. New pectin-based hydrogel containing imiquimod-loaded polymeric nanocapsules for melanoma treatment. Drug Deliv. Transl. Res. 2020, 10, 1829–1840. [Google Scholar] [CrossRef] [PubMed]
- Muthukumar, T.; Sreekumar, G.; Sastry, T.; Chamundeeswari, M. Collagen as a Potential Biomaterial in Biomedical Applications. Rev. Adv. Mater. Sci. 2018, 53, 29–39. [Google Scholar] [CrossRef]
- Antoine, E.E.; Vlachos, P.; Rylander, M.N. Review of Collagen I Hydrogels for Bioengineered Tissue Microenvironments: Characterization of Mechanics, Structure, and Transport. Tissue Eng. Part B Rev. 2014, 20, 683. [Google Scholar] [CrossRef] [PubMed]
- Khan, R.; Khan, M.H. Use of collagen as a biomaterial: An update. J. Indian Soc. Periodontol. 2013, 17, 539. [Google Scholar] [CrossRef]
- Terzopoulou, Z.; Michopoulou, A.; Palamidi, A.; Koliakou, E.; Bikiaris, D. Preparation and Evaluation of Collagen-Based Patches as Curcumin Carriers. Polymers 2020, 12, 2393. [Google Scholar] [CrossRef]
- Naomi, R.; Fauzi, M.B. Cellulose/Collagen Dressings for Diabetic Foot Ulcer: A Review. Pharmaceutics 2020, 12, 881. [Google Scholar] [CrossRef]
- Ulrich, D.; Smeets, R.; Unglaub, F.; Wöltje, M.; Pallua, N. Effect of oxidized regenerated cellulose/collagen matrix on proteases in wound exudate of patients with diabetic foot ulcers. J. Wound Ostomy Cont. Nurs. 2011, 38, 522–528. [Google Scholar] [CrossRef]
- Nguyen, T.P.; Nguyen, Q.V.; Nguyen, V.-H.; Le, T.-H.; Huynh, V.Q.N.; Vo, D.-V.N.; Trinh, Q.T.; Kim, S.Y.; Le, Q.V. Silk fibroin-based biomaterials for biomedical applications: A review. Polymers 2019, 11, 1933. [Google Scholar] [CrossRef]
- Raus, R.A.; Nawawi, W.W.; Nasaruddin, R.R. Alginate and alginate composites for biomedical applications. Asian J. Pharm. Sci. 2021, 16, 280–306. [Google Scholar] [CrossRef]
- Jaiswar, G.; Modak, S.; Singh, R.; Dabas, N. Functionalization of biopolymer keratin-based biomaterials and their absorption properties for healthcare application. In Polymeric Biomaterials for Healthcare Applications; Elsevier: Amsterdam, The Netherlands, 2022; pp. 257–270. [Google Scholar] [CrossRef]
- Al-Nimry, S.; Dayah, A.; Hasan, I.; Daghmash, R. Cosmetic, Biomedical and Pharmaceutical Applications of Fish Gelatin/Hydrolysates. Marine Drugs 2021, 19, 145. [Google Scholar] [CrossRef]
- Ghomi, E.R.; Nourbakhsh, N.; Kenari, M.A.; Zare, M.; Ramakrishna, S. Collagen-based biomaterials for biomedical applications. J. Biomed. Mater. Res. Part B Appl. Biomater. 2021, 109, 1986–1999. [Google Scholar] [CrossRef]
- Agarwal, C.; Csóka, L. Surface-modified cellulose in biomedical engineering. In Materials for Biomedical Engineering: Bioactive Materials, Properties, and Applications; Elsevier: Amsterdam, The Netherlands, 2019; pp. 215–261. [Google Scholar] [CrossRef]
- Azuma, K.; Ifuku, S.; Osaki, T.; Okamoto, Y.; Minami, S. Preparation and biomedical applications of chitin and chitosan nanofibers. J. Biomed. Nanotechnol. 2014, 10, 2891–2920. [Google Scholar] [CrossRef]
- de Oliveira, J.D.; Carvalho, L.; Gomes, A.; Queiroz, L.; Magalhães, B.; Parachin, N.S. Genetic basis for hyper production of hyaluronic acid in natural and engineered microorganisms. Microb. Cell Fact. 2016, 15, 119. [Google Scholar] [CrossRef]
- Eivazzadeh-Keihan, R.; Noruzi, E.B.; Aliabadi, H.A.M.; Sheikhaleslami, S.; Akbarzadeh, A.R.; Hashemi, S.M.; Gorab, M.G.; Maleki, A.; Cohan, R.A.; Mahdavi, M.; et al. Recent advances on biomedical applications of pectin-containing biomaterials. Int. J. Biol. Macromol. 2022, 217, 1–18. [Google Scholar] [CrossRef]
- Burkatovskaya, M.; Tegos, G.; Swietlik, E.; Demidova, T.; Castano, A.P.; Hamblin, M.R. Use of chitosan bandage to prevent fatal infections developing from highly contaminated wounds in mice. Biomaterials 2006, 27, 4157–4164. [Google Scholar] [CrossRef]
- Nazeer, N.; Ahmed, M. Polymers in medicine. In Polymer Science and Nanotechnology; Elsevier: Amsterdam, The Netherlands, 2020; pp. 281–323. [Google Scholar] [CrossRef]
- Nutricare. 2022. Available online: https://nutricare.co/pages/patch (accessed on 24 November 2022).
- Qualicare Burn Gel Dressing. Available online: https://easygoods.co.uk/product/qualicare-wound-burns-scalds-medium-size-10cm-x-10cm-first-aid-dressings/?attribute_pa_pack-of=10 (accessed on 26 November 2022).
- 3M. Available online: https://www.3m.com/3M/en_US/p/d/b00035951/ (accessed on 26 November 2022).









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Advantages | Disadvantages | REF |
|---|---|---|
|
| [11] |
|
| [12] |
|
| [13,14] |
|
| [15,16] |
|
| [17,18] |
| [19] | |
| [20] | |
| [21] |
| Natural Polymers | Synthetic Polymers | ||
|---|---|---|---|
| Advantages | Disadvantages | Advantages | Disadvantages |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| |
| |||
| Patch Design | ||
|---|---|---|
| Drug [84] | Polymer [86] | Adhesive [87] |
| Molecular weight | Tensile strength | Binding force with skin surface |
| Half-life | Endurance against folding | Resistance against shear adhesion |
| Skin permeation coefficient | Flatness | Force required to peel it off |
| Concentration | Moisture content | |
| Hydrophilic/hydrophobic nature | Solubility in different solvents | |
| Film-forming capacity | ||
| Sustainable Biomaterial | Source | Advantages | Application Type | Applications from Literature |
|---|---|---|---|---|
| Silk Fibroin | Silkworm (Bombyx mori) | Biocompatibility, easy processability, controllable biodegradation, versatile functionalization, adjustable drug release | Wound dressing, bone regeneration, drug delivery, gene therapy [160] | |
| Alginate | Brown seaweed | Biocompatibility, biodegradability, inexpensive, easily producible | Wound dressing, tissue engineering, drug delivery, bone regeneration [161] | |
| Keratin | Feathers, hooves, wool, horns, and hair | Biocompatibility, mechanic durability, easy availability, biodegradability | Drug delivery, wound dressing, cosmetics, implant filler [162] | |
| Gelatin | Mammalian bone and hide | Cell recognition, biocompatibility, biodegradability, easy processing | Wound dressing, gene therapy, tissue engineering, drug delivery, intrinsic activity [163] | |
| Collagen | Bovine skin and tendons | Good cell recognition, biodegradability, flexibility, easy availability, mechanical strength, biocompatibility | 3D printing, wound healing, cosmetics, drug delivery, dental applications [164] | |
| Cellulose | Plants and bacteria | Biocompatibility, high purity, water in-soluble | Wound healing, drug delivery, tissue bioscafolds, medical implants [165] | |
| Chitosan/Chitin | Shells of crustaceans, insects and fungi | Biologically renewable, biodegradability, biocompatibility, | Stem cell technology, drug delivery, wound dressing, cosmetic, functional foods [166] | |
| Hyaluronic Acid | Soy-based foods | Biocompatibility, biodegradability, easily functionalized | Wound healing, DNA carrier, cosmetics, aesthetic [167] | |
| Pectin | Apple, citrus fruits, sugar beets | Biocompatibility, biodegradability | Tissue engineering, drug delivery, wound healing [168] |
| Drugs/Molecules | Patch Type | Application Purpose | Model Skin/Organism | Highlights | Ref |
|---|---|---|---|---|---|
| Porphyrins | Silk Fibroin Microneedle | Skin Cancer Treatment | Ex vivo pig skin | Enhanced the penetration of drugs, pioneering study for photodynamic therapy. | [106] |
| Tetracycline Antibiotics | Reducing Local Infections | Escherichia coli | Rapid healing of wounds without infection | [107] | |
| Streptozotocin (STZ) | Chitosan Film | Diabetic Wound Treatment | Rat skin | Streptozotocin increased healing rate from 60% to 95% after 14 days. | [113] |
| Basic fibroblast growth factor (bFGF) | Chitosan Hydrogel | Mice Skin | Nutrition support with porous structure, healing enhancement from 80% to 100% after 14 days. | [114] | |
| Terminalia catappa (TC) | Sodium Alginate Fibers | Skin Cancer Treatment | Skin melanoma cell line (B16F10) | Cell growth rate of cancer cells decreased from 100% to 35%. | [120] |
| Curcumin | Cellulose/alginate/gelatin (BCAGG) film | Oral Cancer Treatment | Oral cancer cells (CAL-27) | Stretchable film provided easy-to-use advantage, Cell viability reduced from 100% to 40% without damaging human keratinocytes (HaCaT) and human gingival fibroblasts (GF), which are healthy cells. | [121] |
| Hesperidin | Alginate hydrogel | Wound Treatment | Rat skin | Wound repairing rate was improved from 60% to 95% after 14 days. | [122] |
| Zinc Oxide (ZnO) Nanoparticles | CF-1 MEF IRR 2M mammalian fibroblast cells | Enhancing wound treatment from 90% to 96% after 24 h with suppressing bacterial growth. | [123] | ||
| Glucose Oxidase | Keratin transdermal patch | Diabetic Wound Treatment | Human | The potential applicability of keratin-based dermal patches for reducing topical glucose level in diabetic wounds and especially foot ulcers. | [129] |
| Keratin | Keratin Based | Skin cancer treatment | HaCaT keratinocytes and rats | Faster recovery for radiated-wound healing. | [130] |
| Zeolitic imidazolate frameworks (ZIF-8) nanoparticles | Sprayable gelatin methacrylate hydrogel | Wound Treatment | Staphylococcus aureus and Escherichia coli | Decreasing viability of bacteria from 100% to approximately 20%. | [134] |
| β-cyclodextrin | Gelatin microneedle | Skin Cancer Treatment | Skin melanoma cell line (B16F10) | Increase in the release capacity and transdermal penetration of drugs, advancement in the release of drug with extending curing process of gelatin microneedle. | [135] |
| Carboplatin (CP) | Cancer cell viability dramatically decreased from 100% to 40% after 72 h. | [136] | |||
| Curcumin | Cellulose hydrogel | Microbial skin wounds and psoriasis-induced wounds treatment | A549, U251MG, MSTO and Panc1 adenocarcinoma cell lines | Increase in the humid environment with the porous structure of hydrogel and obtained slow and sustainable drug release capacity. | [143] |
| Methotrexate | Ethyl cellulose—hydrophilic hydroxypropyl methylcellulose (EC/HMPC) patch | Psoriasis Treatment | Albino rabbits | Drug was distributed uniformly, and its local effect increased. | [27] |
| Hyaluronic acid (HA) microneedle | Mice Skin | Reducing required treatment thickness from 90 µm to 60 µm. | [147] | ||
| Thioether grafting | Hyaluronic acid (HA) nanofibrous hydrogel | Diabetic Wound Treatment | 100% healing rate after 15 days in comparison to hydrogels without thioether, which demonstrated 85% healing rate. Elimination of reactive oxygen species (H2O2) and preventing inflammatory reactions with thioether application. | [148] | |
| Simvastatin | Alginate-Pectin hydrogel | Rat skin | Enhancing healing rate from 80% to 95% after 21 days. | [149] | |
| Clindamycin (Cly) | Pectin hydrogel | Methicillin-resistant Staphylococcus aureus (MRSA)-infected wounds | Methicillin-resistant Staphylococcus aureus (MRSA) | Cell viability of bacteria decreased from 109 to 102. | [152] |
| Nanocapsule imiquimod | Skin Cancer Treatment | SK-MEL-28 melanoma cell line | Advancement in permeability of imiquimod with nanocapsulation process. After 72 h, the viability of cells decreased dramatically from 100% to approximately 50%. | [153] | |
| Curcumin | Collagen hydrogel | Psoriasis Treatment | Keratinocytes and fibroblasts from the skin of Caucasian patient | Preventing the proliferation of psoriatic keratinocytes and sustaining such suppression over time. | [157] |
| Collagen type I | Collagen patch | Diabetic foot ulcer treatment | Human | Rapid wound healing and a significant reduction in the size of the wounds in patients. | [159] |
| Company | Active Material | Application | Highlights | Ref |
|---|---|---|---|---|
| Patch | Aloe Vera | Burns and blisters | Vegan product, sustainable, biocompatible, immediate applicability, and easy-to-use | [171] |
| Qualicare | Hydrogel | Burns and scalds | First-aid gel, nonadherent, sterile, biocompatible, and easy-to-use | [172] |
| 3M Tegaderm | Hydrocolloid Thin Dressing | Ulcers, wounds, and burns | Enhanced exudate control, offered in sacral, square, and oval-shaped dressings, and waterproof film | [173] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yilmaz, E.G.; Ece, E.; Erdem, Ö.; Eş, I.; Inci, F. A Sustainable Solution to Skin Diseases: Ecofriendly Transdermal Patches. Pharmaceutics 2023, 15, 579. https://doi.org/10.3390/pharmaceutics15020579
Yilmaz EG, Ece E, Erdem Ö, Eş I, Inci F. A Sustainable Solution to Skin Diseases: Ecofriendly Transdermal Patches. Pharmaceutics. 2023; 15(2):579. https://doi.org/10.3390/pharmaceutics15020579
Chicago/Turabian StyleYilmaz, Eylul Gulsen, Emre Ece, Özgecan Erdem, Ismail Eş, and Fatih Inci. 2023. "A Sustainable Solution to Skin Diseases: Ecofriendly Transdermal Patches" Pharmaceutics 15, no. 2: 579. https://doi.org/10.3390/pharmaceutics15020579