
The Pharmacokinetics of CPZEN-45, a Novel Anti-Tuberculosis Drug, in Guinea Pigs
 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Animals
2.3. Treatments

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group # | Formulation—Route of Administration | Dose | Purpose in the Study |
|---|---|---|---|
| 1 | Solution—IV | 1 mg/kg | Obtain basic PK parameters in absence of drug absorption |
| 2 | Solution—SC | 1 mg/kg | Determine bioavailability of drug after administration by the conventional route |
| 3 | Powder—INS | 1 mg/kg | Determine pulmonary bioavailability by direct administration of the whole dose to the airways |
| 4 | Powder—Passive inhalation | * Single (80 mg) = 8 dosators over 24 min | Determine the size of an inhaled dose (number of dosators) that would maintain therapeutic concentrations for the longest period of time |
| 5 | Powder—Passive inhalation | * Double (160 mg) = 16 dosators over 48 min | |
| 6 | Powder—Passive inhalation | * Triple (240 mg) = 24 dosators over 72 min | |
| 7 | Powder—Passive inhalation | * Three sequential (80 mg) = 8 dosators every 5 h | Determine if there is powder accumulation after a single inhaled dose = 8 dosators |
2.3.1. Direct Administration of a Single Dose of CPZEN-45 by Different Routes
2.3.2. Passive Inhalation of Consecutive or Sequential Doses of CPZEN-45 Dry Powder Aerosols
2.4. Sample Collection and Determination of CPZEN-45 in Biological Samples
2.5. Data Analysis
2.5.1. Pharmacokinetic (PK) Analysis
2.5.2. Statistical Analysis
3. Results
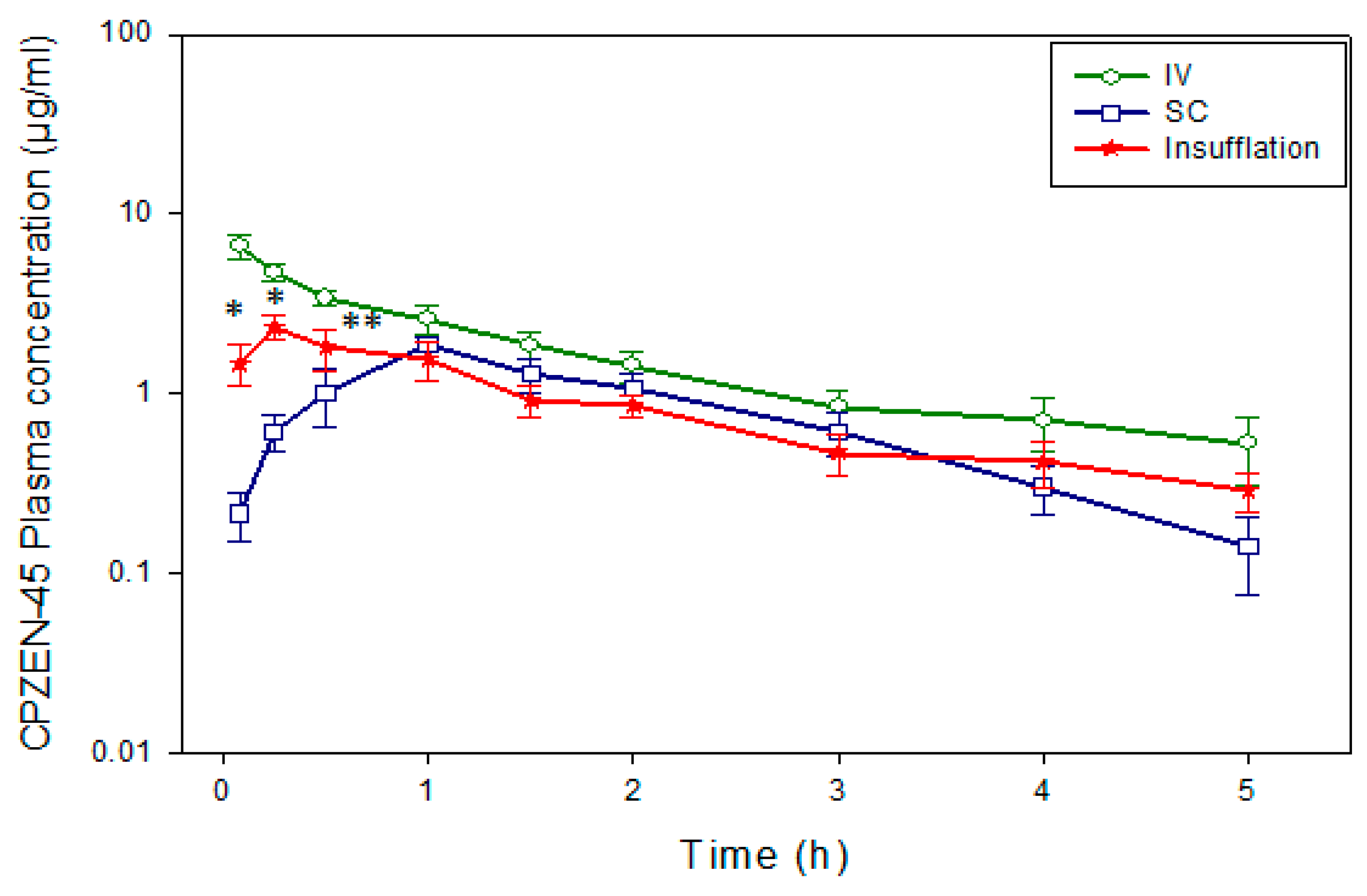
3.1. Disposition of a Single Dose of CPZEN-45 after Administration by the IV, SC, and Pulmonary (INS) Routes
3.2. Disposition of CPZEN-45 after Administration of Consecutive Doses by Passive Inhalation (Aerosol)
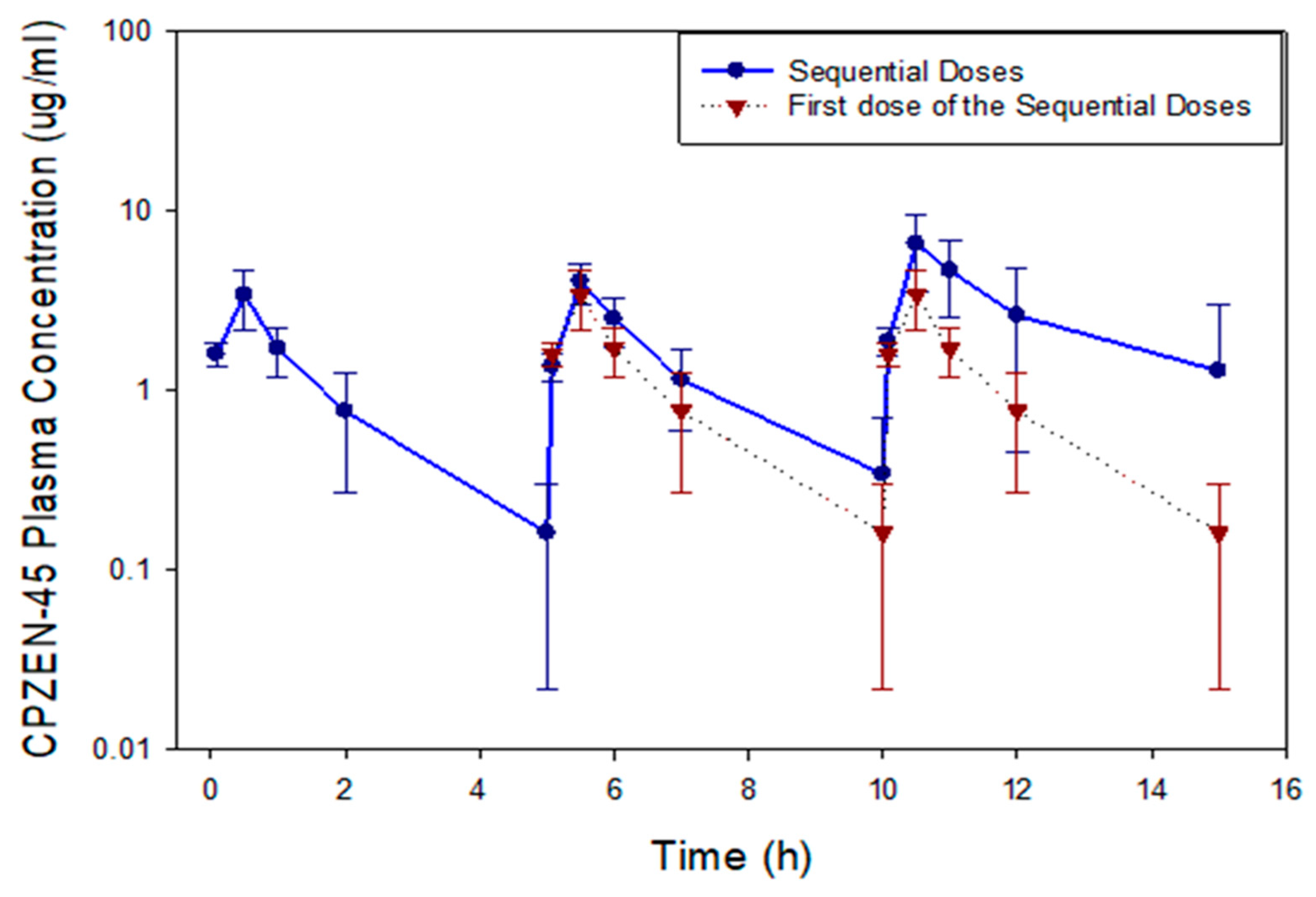
3.3. Disposition of CPZEN-45 after Administration of Sequential Doses by Passive Inhalation (Aerosol)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Tuberculosis Report 2021; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Crist, C. Worst TB Outbreak in 20 Years Reported in Washington State; Medscape: New York, NY, USA, 2022. [Google Scholar]
- Washington State Department of Health. Tuberculosis Cases on the Rise Globally and in Washington State; Newsroom Washington State Department of Health: Washington, DC, USA, 2022.
- Conradie, F.; Diacon, A.H.; Ngubane, N.; Howell, P.; Everitt, D.; Crook, A.M.; Mendel, C.M.; Egizi, E.; Moreira, J.; Timm, J.; et al. Treatment of Highly Drug-Resistant Pulmonary Tuberculosis. N. Engl. J. Med. 2020, 382, 893–902. [Google Scholar] [CrossRef] [PubMed]
- Maartens, G.; Benson, C.A. Linezolid for Treating Tuberculosis: A Delicate Balancing Act. EBioMedicine 2015, 2, 1568–1569. [Google Scholar] [CrossRef] [PubMed]
- WHO. Rapid Communication: Key Changes to the Treatment of Drug-Resistant Tuberculosis; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- Takahashi, Y.; Igarashi, M.; Miyake, T.; Soutome, H.; Ishikawa, K.; Komatsuki, Y.; Koyama, Y.; Nakagawa, N.; Hattori, S.; Inoue, K.; et al. Novel semisynthetic antibiotics from caprazamycins A-G: Caprazene derivatives and their antibacterial activity. J. Antibiot. 2013, 66, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.; Manjunatha, U.; Boshoff, H.I.; Ha, Y.H.; Niyomrattanakit, P.; Ledwidge, R.; Dowd, C.S.; Lee, I.Y.; Kim, P.; Zhang, L.; et al. PA-824 kills nonreplicating Mycobacterium tuberculosis by intracellular NO release. Science 2008, 322, 1392–1395. [Google Scholar] [CrossRef]
- Huszar, S.; Singh, V.; Polcicova, A.; Barath, P.; Barrio, M.B.; Lagrange, S.; Leblanc, V.; Nacy, C.A.; Mizrahi, V.; Mikusova, K. N-Acetylglucosamine-1-Phosphate Transferase, WecA, as a Validated Drug Target in Mycobacterium tuberculosis. Antimicrob. Agents Chemother. 2017, 61, e01310-17. [Google Scholar] [CrossRef] [PubMed]
- Adhvaryu, M.; Vakharia, B. Drug-resistant tuberculosis: Emerging treatment options. Clin. Pharmacol. 2011, 3, 51–67. [Google Scholar] [CrossRef]
- Salomon, J.J.; Galeron, P.; Schulte, N.; Morow, P.R.; Severynse-Stevens, D.; Huwer, H.; Daum, N.; Lehr, C.M.; Hickey, A.J.; Ehrhardt, C. Biopharmaceutical in vitro characterization of CPZEN-45, a drug candidate for inhalation therapy of tuberculosis. Ther. Deliv. 2013, 4, 915–923. [Google Scholar] [CrossRef]
- Hanif, S.N.M.; Hickey, A.J.; García-Contreras, L. Liquid chromatographic determination of CPZEN-45, a novel anti-tubercular drug, in biological samples. J. Pharm. Biomed. Anal. 2014, 88, 370–376. [Google Scholar] [CrossRef]
- Pitner, R.A.; Durham, P.G.; Stewart, I.E.; Reed, S.G.; Cassell, G.H.; Hickey, A.J.; Carter, D. A Spray-Dried Combination of Capreomycin and CPZEN-45 for Inhaled Tuberculosis Therapy. J. Pharm. Sci. 2019, 108, 3302–3311. [Google Scholar] [CrossRef] [PubMed]
- Stewart, I.E.; Durham, P.G.; Sittenauer, J.M.; Barreda, A.P.; Stowell, G.W.; Moody, C.; Mecham, J.B.; Simpson, C.; Daily, S.; Maloney, S.E.; et al. Optimization and Scale Up of Spray Dried CPZEN-45 Aerosol Powders for Inhaled Tuberculosis Treatment. Pharm. Res. 2022, 39, 3359–3370. [Google Scholar] [CrossRef]
- Hamed, K.; Debonnett, L. Tobramycin inhalation powder for the treatment of pulmonary Pseudomonas aeruginosa infection in patients with cystic fibrosis: A review based on clinical evidence. Ther. Adv. Respir. Dis. 2017, 11, 193–209. [Google Scholar] [CrossRef] [PubMed]
- Mortensen, N.P.; Durham, P.; Hickey, A.J. The role of particle physico-chemical properties in pulmonary drug delivery for tuberculosis therapy. J. Microencapsul. 2014, 31, 785–795. [Google Scholar] [CrossRef] [PubMed]
- Hanif, S.N.M.; Durham, P.; Hickey, A.J.; Garcia-Contreras, L. Pharmacokinetics of CPZEN-45 aerosol powders administered by passive inhalation. In Respiratory Drug Delivery 2014; Dalby, R.N., Byron, P.R., Peart, J., Suman, J.D., Farr, S., Traini, D., Young, P.M., Eds.; Davis Healthcare International Publishing, LCC: River Grove, IL, USA, 2014. [Google Scholar]
- Young, E.F.; Durham, P.G.; Perkowski, E.F.; Malik, S.; Hickey, A.J.; Braunstein, M. Efficacy of inhaled CPZEN-45 in treating tuberculosis in the guinea pig. Tuberculosis 2022, 135, 102207. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Contreras, L.; Fiegel, J.; Telko, M.J.; Elbert, K.; Hawi, A.; Thomas, M.; VerBerkmoes, J.; Germishuizen, W.A.; Fourie, P.B.; Hickey, A.J.; et al. Inhaled Large Porous Particles of Capreomycin for Treatment of Tuberculosis in a Guinea Pig Model. Antimicrob. Agents Chemother. 2007, 51, 2830–2836. [Google Scholar] [CrossRef] [PubMed]
- Durham, P.G.; Hanif, S.N.; Contreras, L.G.; Young, E.F.; Braunstein, M.S.; Hickey, A.J. Disposable Dosators for Pulmonary Insufflation of Therapeutic Agents to Small Animals. J. Vis. Exp. 2017, 55356. [Google Scholar] [CrossRef]
- Garcia-Contreras, L.; Sethuraman, V.; Kazantseva, M.; Hickey, A. Efficacy of Combined Rifampicin Formulations Delivered by the Pulmonary Route to Treat Tuberculosis in the Guinea Pig Model. Pharmaceutics 2021, 13, 1309. [Google Scholar] [CrossRef]
- Koul, A.; Arnoult, E.; Lounis, N.; Guillemont, J.; Andries, K. The challenge of new drug discovery for tuberculosis. Nature 2011, 469, 483–490. [Google Scholar] [CrossRef] [PubMed]
- Clark, S.; Hall, Y.; Williams, A. Animal models of tuberculosis: Guinea pigs. Cold Spring Harb. Perspect. Med. 2014, 5, a018572. [Google Scholar] [CrossRef]
- Basaraba, R.J. Experimental tuberculosis: The role of comparative pathology in the discovery of improved tuberculosis treatment strategies. Tuberculosis 2008, 88 (Suppl. S1), S35–S47. [Google Scholar] [CrossRef]
- Montgomery, S.A.; Young, E.F.; Durham, P.G.; Zulauf, K.E.; Rank, L.; Miller, B.K.; Hayden, J.D.; Lin, F.-C.; Welch, J.T.; Hickey, A.J.; et al. Efficacy of pyrazinoic acid dry powder aerosols in resolving necrotic and non-necrotic granulomas in a guinea pig model of tuberculosis. PLoS ONE 2018, 13, e0204495. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Contreras, L.; Padilla-Carlin, D.J.; Sung, J.; VerBerkmoes, J.; Muttil, P.; Elbert, K.; Peloquin, C.; Edwards, D.; Hickey, A. Pharmacokinetics of Ethionamide Delivered in Spray-Dried Microparticles to the Lungs of Guinea Pigs. J. Pharm. Sci. 2017, 106, 331–337. [Google Scholar] [CrossRef]
- Sung, J.C.; Garcia-Contreras, L.; Verberkmoes, J.L.; Peloquin, C.A.; Elbert, K.J.; Hickey, A.J.; Edwards, D.A. Dry powder nitroimidazopyran antibiotic PA-824 aerosol for inhalation. Antimicrob. Agents Chemother. 2009, 53, 1338–1343. [Google Scholar] [CrossRef] [PubMed]
- Garcia Contreras, L.; Sung, J.; Ibrahim, M.; Elbert, K.; Edwards, D.; Hickey, A. Pharmacokinetics of Inhaled Rifampicin Porous Particles for Tuberculosis Treatment: Insight into Rifampicin Absorption from the Lungs of Guinea Pigs. Mol. Pharm. 2015, 12, 2642–2650. [Google Scholar] [CrossRef] [PubMed]
- Patton, J.S. Mechanisms of macromolecule absorption by the lungs. Adv. Drug Deliv. Rev. 1996, 19, 3–36. [Google Scholar] [CrossRef]
- Sung, J.C.; Padilla, D.J.; Garcia-Contreras, L.; Verberkmoes, J.L.; Durbin, D.; Peloquin, C.A.; Elbert, K.J.; Hickey, A.J.; Edwards, D.A. Formulation and pharmacokinetics of self-assembled rifampicin nanoparticle systems for pulmonary delivery. Pharm. Res. 2009, 26, 1847–1855. [Google Scholar] [CrossRef] [PubMed]
- Le Brun, P.P.; Vinks, A.A.; Touw, D.J.; Hekelaar, N.; Mannes, G.P.; Brimicombe, R.W.; Frijlink, E.H.; Heijerman, H.G. Can tobramycin inhalation be improved with a jet nebulizer? Ther. Drug Monit. 1999, 21, 618–624. [Google Scholar] [CrossRef]
- Sakagami, M. Insulin disposition in the lung following oral inhalation in humans: A meta-analysis of its pharmacokinetics. Clin. Pharmacokinet. 2004, 43, 539–552. [Google Scholar] [CrossRef] [PubMed]
- Surber, M.W.; Beck, S.; Pham, S.; Marsden, A.T.; Gandi, S.K.; Baily, J.; McElroy, M.C. Inhaled nintedanib is well-tolerated and delivers key pharmacokinetic parameters required to treat bleomycin-induced pulmonary fibrosis. Pulm. Pharmacol. Ther. 2020, 63, 101938. [Google Scholar] [CrossRef]
- Cryan, S.A.; Sivadas, N.; Garcia-Contreras, L. In vivo animal models for drug delivery across the lung mucosal barrier. Adv. Drug Deliv. Rev. 2007, 59, 1133–1151. [Google Scholar] [CrossRef]
- García-Contreras, L. In vivo models for controlled release pulmonary drug delivery. In Controlled Pulmonary Drug Delivery; Smyth, H.D.C., Hickey, A.J., Eds.; Springer Science and Business Media, LLC: New York, NY, USA, 2011. [Google Scholar]
- Hickey, A.J.; Smyth, H.D.C.; Telko, M.J. Dry Powder Aerosol Generator; U.S.P. Office, Ed.; The University of North Carolina: Chapel Hill, NC, USA, 2012; p. 18. [Google Scholar]
- Garcia-Contreras, L.; Sung, J.C.; Muttil, P.; Padilla, D.; Telko, M.; Verberkmoes, J.L.; Elbert, K.J.; Hickey, A.J.; Edwards, D.A. Dry powder PA-824 aerosols for treatment of tuberculosis in guinea pigs. Antimicrob. Agents Chemother. 2010, 54, 1436–1442. [Google Scholar] [CrossRef]
- Hickey, A.J.; Garcia-Contreras, L. Immunological and toxicological implications of short-term studies in animals of pharmaceutical aerosol delivery to the lungs: Relevance to humans. Crit. Rev. Ther. Drug Carrier Syst. 2001, 18, 387–431. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Contreras, L.; Muttil, P.; Fallon, J.K.; Kabadi, M.; Gerety, R.; Hickey, A.J. Pharmacokinetics of sequential doses of capreomycin powder for inhalation in guinea pigs. Antimicrob. Agents Chemother. 2012, 56, 2612–2618. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, M.; Garcia Contreras, L. Preclinical Pharmacokinetics of Antitubercular Drugs. In Drug Delivery Systems for Tuberculosis Prevention and Treatment; Hickey, A.J., Misra, A., Fourie, P.B., Eds.; John Wiley and Sons, Ltd.: Sussex, UK, 2016; pp. 131–155. [Google Scholar]








| Parameter | Intravenous (IV) (1 mg/kg, Solution) | Subcutaneous (SC) (1 mg/kg, Solution) | Insufflation (INS) (1 mg/kg, Powder) |
|---|---|---|---|
| Non-compartmental analysis | |||
| AUC (µgh/mL) | 8.18 ± 2.72 1 | 3.76 ± 1.84 2 | 4.61 ± 1.63 2 |
| AUC0-∞ (µgh/mL) | 8.50 ± 3.27 1 | 4.05 ± 2.01 2 | 5.76 ± 2.64 1,2 |
| CLSS_F (ml/hkg) | 136.07 ± 43.30 2 | 277.16 ± 121.09 1 | 236.70 ± 74.75 1,2 |
| Ke (h−1) | 0.64 ± 0.20 2 | 0.96 ± 0.24 1 | 0.39 ± 0.15 2 |
| t1/2 (h) | 1.14 ± 0.27 2 | 0.76 ± 0.22 2 | 2.06 ± 1.01 1 |
| MRT (h) | 1.66 ± 0.39 2 | 1.90 ± 0.37 2 | 2.83 ± 0.84 1 |
| MAT (h) | - | 0.42 ± 0.17 | 1.17 ± 0.84 |
| Cmax (µg/mL) | 6.89 ± 2.06 1 | 1.91 ± 0.48 2 | 2.35 ± 1.02 2 |
| Tmax (h) | 0.08 ± 0.00 3 | 0.83 ± 0.25 1 | 0.37 ± 0.18 2 |
| F_AUC | - | 46.01 ± 22.49 | 56.39 ± 19.94 |
| F_AUC0-∞ | - | 47.73 ± 23.72 | 67.78 ± 31.14 |
| One Compartment analysis | |||
| Ka (h−1) | - | 1.23 ± 0.55 | 12.94 ± 5.66 |
| Ke (h−1) | 0.43 ± 0.19 2 | 0.95 ± 0.35 1 | 0.47 ± 0.13 2 |
| Parameter | Insufflation (INS) (1 mg/kg) | Aerosol Single Dose (80 mg) | Aerosol Double Dose (160 mg) | Aerosol Triple Dose (240 mg) |
|---|---|---|---|---|
| AUC (µgh/mL) | 4.61 ± 1.63 2 | 9.14 ± 1.43 2 | 18.41 ± 7.72 1 | 15.65 ± 5.48 1,2 |
| AUC0-∞ (µgh/mL) | 5.76 ± 2.64 1,2 | 9.34 ± 1.37 2 | 19.52 ± 7.97 1 | 16.29 ± 5.91 1,2 |
| CLSS_F (ml/hkg) | 236.70 ± 74.75 1,2 | 215.68 ± 27.42 1 | 247.17 ± 134.43 1 | 226.20 ± 56.19 1 |
| Ke (h−1) | 0.39 ± 0.15 2 | 0.81 ± 0.14 1 | 0.65 ± 0.12 1 | 0.74 ± 0.12 1 |
| t1/2 (h) | 2.06 ± 1.01 1 | 0.86 ± 0.15 2 | 1.09 ± 0.26 2 | 0.94 ± 0.12 2 |
| MRT (h) | 2.83 ± 0.84 1 | 1.39 ± 0.27 2 | 1.83 ± 0.37 2 | 1.78 ± 0.26 2 |
| Cmax (µg/mL) | 2.35 ± 1.02 2 | 6.63 ± 1.80 1 | 10.30 ± 4.90 1 | 7.27 ± 2.32 1 |
| Tmax (h) | 0.37 ± 0.18 2 | 0.50 ± 0.00 2 | 1.00 ± 0.00 1 | 1.00 ± 0.44 1 |
| Parameter | Aerosol 8 × 8 × 8 Doses (5 h, 80 mg) | Aerosol 8 × 8 × 8 Doses (10 h, 80 mg) | Aerosol 8 × 8 × 8 Doses (15 h, 80 mg) |
|---|---|---|---|
| AUC (µgh/mL) | 5.40 ± 2.65 1 | 6.89 ± 2.27 1 | 14.14 ± 9.82 1 |
| AUC0-∞ (µgh/mL) | 5.67 ± 2.89 1 | 7.29 ± 2.45 1 | 20.69 ± 21.00 1 |
| CLSS_F (mL/hkg) | 245.07 ± 100.80 1 | 225.55 ± 77.26 1 | 256.69 ± 156.67 1 |
| Ke (h−1) | 0.70 ± 0.22 1 | 0.78 ± 0.20 1 | 0.49 ± 0.32 1 |
| t1/2 (h) | 1.03 ± 0.25 1 | 0.91 ± 0.24 1 | 2.01 ± 1.51 1 |
| MRT (h) | 1.39 ± 0.22 1 | 1.65 ± 0.38 1 | 2.92 ± 2.19 1 |
| Cmax (µg/mL) | 3.40 ± 1.25 2 | 4.05 ± 1.02 1,2 | 6.55 ± 3.05 1 |
| Tmax (h) | 0.50 ± 0.00 1 | 0.50 ± 0.00 1 | 0.50 ± 0.00 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garcia-Contreras, L.; Hanif, S.N.M.; Ibrahim, M.; Durham, P.; Hickey, A.J. The Pharmacokinetics of CPZEN-45, a Novel Anti-Tuberculosis Drug, in Guinea Pigs. Pharmaceutics 2023, 15, 2758. https://doi.org/10.3390/pharmaceutics15122758
Garcia-Contreras L, Hanif SNM, Ibrahim M, Durham P, Hickey AJ. The Pharmacokinetics of CPZEN-45, a Novel Anti-Tuberculosis Drug, in Guinea Pigs. Pharmaceutics. 2023; 15(12):2758. https://doi.org/10.3390/pharmaceutics15122758
Chicago/Turabian StyleGarcia-Contreras, Lucila, Shumaila Nida Muhammad Hanif, Mariam Ibrahim, Phillip Durham, and Anthony J. Hickey. 2023. "The Pharmacokinetics of CPZEN-45, a Novel Anti-Tuberculosis Drug, in Guinea Pigs" Pharmaceutics 15, no. 12: 2758. https://doi.org/10.3390/pharmaceutics15122758