
Drug Utilization and Measurement of Medication Adherence: A Real World Study of Psoriasis in Italy

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Population
2.3. Adherence Measurement
2.4. Covariates
2.5. Statistical Analyses
2.6. Ethical Considerations
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Parisi, R.; Iskandar, I.Y.K.; Kontopantelis, E.; Augustin, M.; Griffiths, C.E.M.; Ashcroft, D.M. Global Psoriasis Atlas. National, regional, and worldwide epidemiology of psoriasis: Systematic analysis and modelling study. BMJ 2020, 369, m1590. [Google Scholar] [CrossRef] [PubMed]
- Italian Ministry of Health. Linea Guida Sulla Psoriasi, Presentato Aggiornamento Coordinato dall’ISS. 2013. Available online: https://www.salute.gov.it/portale/news/p3_2_1_1_1.jsp?lingua=italiano&menu=notizie&p=null&id=1072 (accessed on 10 September 2023).
- Vaengebjerg, S.; Skov, L.; Egeberg, A.; Loft, N.D. Prevalence, Incidence, and Risk of Cancer in Patients with Psoriasis and Psoriatic Arthritis: A Systematic Review and Meta-analysis. JAMA Dermatol. 2020, 156, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, A.; Fabbrocini, G.; Cinelli, E.; Ocampo Garza, S.S.; Camela, E.; Megna, M. Anti-interleukin-23 for psoriasis in elderly patients: Guselkumab, risankizumab and tildrakizumab in real-world practice. Clin. Exp. Dermatol. 2022, 47, 561–567. [Google Scholar] [CrossRef] [PubMed]
- Nijsten, T.; Margolis, D.J.; Feldman, S.R.; Rolstad, T.; Stern, R.S. Traditional systemic treatments have not fully met the needs of psoriasis patients: Results from a national survey. J. Am. Acad. Dermatol. 2005, 52 Pt 1, 434–444. [Google Scholar] [CrossRef]
- Stern, R.S.; Nijsten, T.; Feldman, S.R.; Margolis, D.J.; Rolstad, T. Psoriasis is common, carries a substantial burden even when not extensive, and is associated with widespread treatment dissatisfaction. J. Investig. Dermatol. Symp. Proc. 2004, 9, 136–139. [Google Scholar] [CrossRef]
- Storm, A.; Andersen, S.E.; Benfeldt, E.; Serup, J. One in 3 prescriptions are never redeemed: Primary nonadherence in an outpatient clinic. J. Am. Acad. Dermatol. 2008, 59, 27–33. [Google Scholar] [CrossRef]
- Storm, A.; Benfeldt, E.; Andersen, S.E.; Serup, J. A prospective study of patient adherence to topical treatments: 95% of patients underdose. J. Am. Acad. Dermatol. 2008, 59, 975–980. [Google Scholar] [CrossRef]
- Thorneloe, R.J.; Bundy, C.; Griffiths, C.E.; Ashcroft, D.M.; Cordingley, L. Nonadherence to psoriasis medication as an outcome of limited coping resources and conflicting goals: Findings from a qualitative interview study with people with psoriasis. Br. J. Dermatol. 2017, 176, 667–676. [Google Scholar] [CrossRef]
- Megna, M.; Cinelli, E.; Gallo, L.; Camela, E.; Ruggiero, A.; Fabbrocini, G. Risankizumab in real life: Preliminary results of efficacy and safety in psoriasis during a 16-week period. Arch. Dermatol. Res. 2022, 314, 619–623. [Google Scholar] [CrossRef]
- Egeberg, A.; Ottosen, M.B.; Gniadecki, R.; Broesby-Olsen, S.; Dam, T.N.; Bryld, L.E.; Rasmussen, M.K.; Skov, L. Safety, efficacy and drug survival of biologics and biosimilars for moderate-to-severe plaque psoriasis. Br. J. Dermatol. 2018, 178, 509–519. [Google Scholar] [CrossRef]
- Roche, H.; Bouiller, K.; Puzenat, E.; Deveza, E.; Roche, B.; Pelletier, F.; van de Laak, A.; Dupond, A.S.; Nardin, C.; Aubin, F. Efficacy and survival of biologic agents in psoriasis: A practical real-life 12-year experience in a French dermatology department. J. Dermatolog. Treat. 2019, 30, 540–544. [Google Scholar] [CrossRef] [PubMed]
- Schmitt-Egenolf, M.; Freilich, J.; Stelmaszuk-Zadykowicz, N.M.; Apol, E.; Hansen, J.B.; Levin, L.Å. Drug Persistence of Biologic Treatments in Psoriasis: A Swedish National Population Study. Dermatol. Ther. 2021, 11, 2107–2121. [Google Scholar] [CrossRef]
- Girolomoni, G.; Strohal, R.; Puig, L.; Bachelez, H.; Barker, J.; Boehncke, W.H.; Prinz, J.C. The role of IL-23 and the IL-23/TH 17 immune axis in the pathogenesis and treatment of psoriasis. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 1616–1626. [Google Scholar] [CrossRef]
- Perrone, V.; Losi, S.; Sabatino, S.; Mezzetti, M.; Dovizio, M.; Sangiorgi, D.; Degli Esposti, L. Analysis of Drug Utilization in Patients with Psoriasis: A Real-World Retrospective Study Among the Italian Population. Psoriasis 2023, 13, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Blauvelt, A.; Shi, N.; Burge, R.; Malatestinic, W.N.; Lin, C.Y.; Lew, C.R.; Zimmerman, N.M.; Goldblum, O.M.; Zhu, B.; Murage, M.J. Comparison of real-world treatment patterns among patients with psoriasis prescribed ixekizumab or secukinumab. J. Am. Acad. Dermatol. 2020, 82, 927–935. [Google Scholar] [CrossRef]
- STROBE Statement—Checklist of Items that Should Be Included in Reports of Cohort Studies. Available online: www.strobe-statement.org/ (accessed on 11 October 2023).
- Guerrero-Fernández de Alba, I.; Orlando, V.; Monetti, V.M.; Mucherino, S.; Gimeno-Miguel, A.; Vaccaro, O.; Forjaz, M.J.; Poblador Plou, B.; Prados-Torres, A.; Riccardi, G.; et al. Comorbidity in an Older Population with Type-2 Diabetes Mellitus: Identification of the Characteristics and Healthcare Utilization of High-Cost Patients. Front. Pharmacol. 2020, 11, 586187. [Google Scholar] [CrossRef] [PubMed]
- Orlando, V.; Coscioni, E.; Guarino, I.; Mucherino, S.; Perrella, A.; Trama, U.; Limongelli, G.; Menditto, E. Drug-utilisation profiles and COVID-19. Sci. Rep. 2021, 11, 8913. [Google Scholar] [CrossRef]
- Orlando, V.; Mucherino, S.; Guarino, I.; Guerriero, F.; Trama, U.; Menditto, E. Gender Differences in Medication Use: A Drug Utilization Study Based on Real World Data. Int. J. Environ. Res. Public Health 2020, 17, 3926. [Google Scholar] [CrossRef]
- Arnone, M.; Takahashi, M.D.F.; Carvalho, A.V.E.D.; Bernardo, W.M.; Bressan, A.L.; Ramos, A.M.C.; Terena, A.C.; Souza, C.D.S.; Nunes, D.H.; Bortoletto, M.C.C.; et al. Diagnostic and therapeutic guidelines for plaque psoriasis—Brazilian Society of Dermatology. An. Bras. Dermatol. 2019, 94 (Suppl. S1), 76–107. [Google Scholar] [CrossRef]
- De Geest, S.; Zullig, L.L.; Dunbar-Jacob, J.; Helmy, R.; Hughes, D.A.; Wilson, I.B.; Vrijens, B. ESPACOMP Medication Adherence Reporting Guideline (EMERGE). Ann. Intern. Med. 2018, 169, 30–35. [Google Scholar] [CrossRef]
- Vrijens, B.; De Geest, S.; Hughes, D.A.; Przemyslaw, K.; Demonceau, J.; Ruppar, T.; Dobbels, F.; Fargher, E.; Morrison, V.; Lewek, P.; et al. A new taxonomy for describing and defining adherence to medications. Br. J. Clin. Pharmacol. 2012, 73, 691–705. [Google Scholar] [CrossRef] [PubMed]
- Mucherino, S.; Maffoni, M.; Cena, C.; Armando, L.G.; Guastavigna, M.; Orlando, V.; Orofino, G.; Traina, S.; Giardini, A.; Menditto, E.; et al. Italian Translation and Validation of the Original ABC Taxonomy for Medication Adherence. Healthcare 2023, 11, 846. [Google Scholar] [CrossRef] [PubMed]
- Mair, A.; Fernandez-Llimos, F.; Alonso, A.; Harrison, C.; Hurding, S.; Kempen, T.; Kinnear, M.; Michael, N.; McIntosh, J.; Wilson, M.; et al. Polypharmacy Management by 2030: A Patient Safety Challenge. 2017. Available online: https://www.isimpathy.eu/uploads/Polypharmacy-Handbook-2nd-Edition.pdf (accessed on 10 September 2023).
- Italian Data Protection Authority. General Authorisation to Process Personal Data for Scientific Research Purposes—1 March 2012. Available online: https://www.garanteprivacy.it/home/docweb/-/docweb-display/docweb/2485392 (accessed on 11 October 2023).
- Nast, A.; Smith, C.; Spuls, P.I.; Avila Valle, G.; Bata-Csörgö, Z.; Boonen, H.; De Jong, E.; Garcia-Doval, I.; Gisondi, P.; Kaur-Knudsen, D.; et al. EuroGuiDerm Guideline on the systemic treatment of Psoriasis vulgaris—Part 1: Treatment and monitoring recommendations. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 2461–2498. [Google Scholar] [CrossRef] [PubMed]
- Sbidian, E.; Chaimani, A.; Garcia-Doval, I.; Doney, L.; Dressler, C.; Hua, C.; Hughes, C.; Naldi, L.; Afach, S.; Le Cleach, L. Systemic pharmacological treatments for chronic plaque psoriasis: A network meta-analysis. Cochrane Database Syst. Rev. 2022, 5, CD011535. [Google Scholar] [CrossRef] [PubMed]
- Xu, C.; Teeple, A.; Wu, B.; Fitzgerald, T.; Feldman, S.R. Drug Adherence and Persistence of Patients with Moderate to Severe Psoriasis Treated with Biologic Medications in a US Commercially Insured Population. Dermatology 2022, 238, 438–447. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, A.W.; Patel, M.; Li, C.; Garg, V.; Mandava, M.R.; Wu, J.J. Real-world switching patterns and associated characteristics in patients with psoriasis treated with biologics in the United States. J. Dermatolog. Treat. 2023, 34, 2200870. [Google Scholar] [CrossRef]
- Giometto, S.; Tillati, S.; Baglietto, L.; De Bortoli, N.; Mosca, M.; Conte, M.; Tuccori, M.; Gini, R.; Lucenteforte, E. Use of Biological Drugs for Psoriasis: A Drug-Utilization Study Using Tuscan Administrative Databanks. Int. J. Environ. Res. Public Health 2022, 19, 6799. [Google Scholar] [CrossRef]
- Feldman, S.R.; Zhang, J.; Martinez, D.J.; Lopez-Gonzalez, L.; Marchlewicz, E.H.; Shrady, G.; Mendelsohn, A.M.; Zhao, Y. Real-world biologic and apremilast treatment patterns and healthcare costs in moderate-to-severe plaque psoriasis. Dermatol. Online J. 2021, 27, 2. [Google Scholar] [CrossRef]
- Kaplan, D.L.; Ung, B.L.; Pelletier, C.; Udeze, C.; Khilfeh, I.; Tian, M. Switch rates and total cost associated with apremilast and biologics in biologic-naive patients with psoriatic arthritis. J. Comp. Eff. Res. 2021, 10, 989–998. [Google Scholar] [CrossRef]
- Wu, J.J.; Pelletier, C.; Ung, B.; Tian, M.; Khilfeh, I.; Curtis, J.R. Treatment Switch Patterns and Healthcare Costs in Biologic-Naive Patients with Psoriatic Arthritis. Adv. Ther. 2020, 37, 2098–2115. [Google Scholar] [CrossRef]
- Batta, S.; Khan, R.; Zaayman, M.; Limmer, A.; Kivelevitch, D.; Menter, A. IL-17 and -23 Inhibitors for the Treatment of Psoriasis. EMJ Allergy Immunol. 2023. [Google Scholar] [CrossRef]
- Menditto, E.; Cahir, C.; Malo, S.; Aguilar-Palacio, I.; Almada, M.; Costa, E.; Giardini, A.; Gil Peinado, M.; Massot Mesquida, M.; Mucherino, S.; et al. Persistence as a Robust Indicator of Medication Adherence-Related Quality and Performance. Int. J. Environ. Res. Public Health 2021, 18, 4872. [Google Scholar] [CrossRef] [PubMed]
- Gniadecki, R.; Bang, B.; Bryld, L.E.; Iversen, L.; Lasthein, S.; Skov, L. Comparison of long-term drug survival and safety of biologic agents in patients with psoriasis vulgaris. Br. J. Dermatol. 2015, 172, 244–252. [Google Scholar] [CrossRef]
- Esposti, L.D.; Perrone, V.; Sangiorgi, D.; Buda, S.; Andretta, M.; Rossini, M.; Girolomoni, G. Analysis of drug utilization and health care resource consumption in patients with psoriasis and psoriatic arthritis before and after treatment with biological therapies. Biologics 2018, 12, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Sbidian, E.; Mezzarobba, M.; Weill, A.; Coste, J.; Rudant, J. Persistence of treatment with biologics for patients with psoriasis: A real-world analysis of 16,545 biologic-naive patients from the French National Health Insurance database (SNIIRAM). Br. J. Dermatol. 2019, 180, 86–93. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Overall ° | Index Treatment | ||||||
|---|---|---|---|---|---|---|---|
| Apremilast | Etanercept | Adalimumab | Ustekinumab | Secukinumab | Ixekizumab | ||
| n = 801 | n = 165 (20.6%) | n = 56 (7.0%) | n = 132 (16.5%) | n = 124 (15.5%) | n = 183 (22.8%) | n = 141 (17.6%) | |
| Gender, N (%) | |||||||
| Males | 485 (60.5) | 91 (55.2) | 33 (58.9) | 77 (58.3) | 70 (56.5) | 122 (66.7) | 92 (65.2) |
| Mean age ± SD | 49.2 ± 16.3 | 60.9 ± 12.9 | 51.7 ± 14.5 | 37.0 ± 16.7 | 48.3 ± 14.9 | 48.9 ± 15.2 | 46.9 ± 13.8 |
| Polypharmacy, * N (%) | |||||||
| No polypharmacy (1–4 drugs) | 258 (32.2) | 34 (20.6) | 22 (39.3) | 47 (35.6) | 38 (30.6) | 69 (37.7) | 48 (34.0) |
| Polypharmacy (5–9 drugs) | 253 (31.6) | 32 (19.4) | 9 (16.1) | 55 (41.7) | 67 (54.0) | 61 (33.3) | 59 (41.8) |
| Excessive polypharmacy (≥10 drugs) | 290 (36.2) | 99 (60.0) | 25 (44.6) | 30 (22.7) | 49 (39.5) | 53 (29.0) | 34 (24.1) |
| 1-Year Adherence Estimation | Overall | Apremilast | Etanercept | Adalimumab | Ustekinumab | Secukinumab | Ixekizumab |
|---|---|---|---|---|---|---|---|
| n = 801 | n = 165 (20.6%) | n = 56 (7.0%) | n = 132 (16.5%) | n = 124 (15.5%) | n = 183 (22.8%) | n = 141 (17.6%) | |
| Initiation Phase | |||||||
| ∆% Ptp/Ptd | 93.0 | 84.6 | 96.7 | 94.7 | 93.3 | 94.5 | 91.2 |
| Implementation phase | |||||||
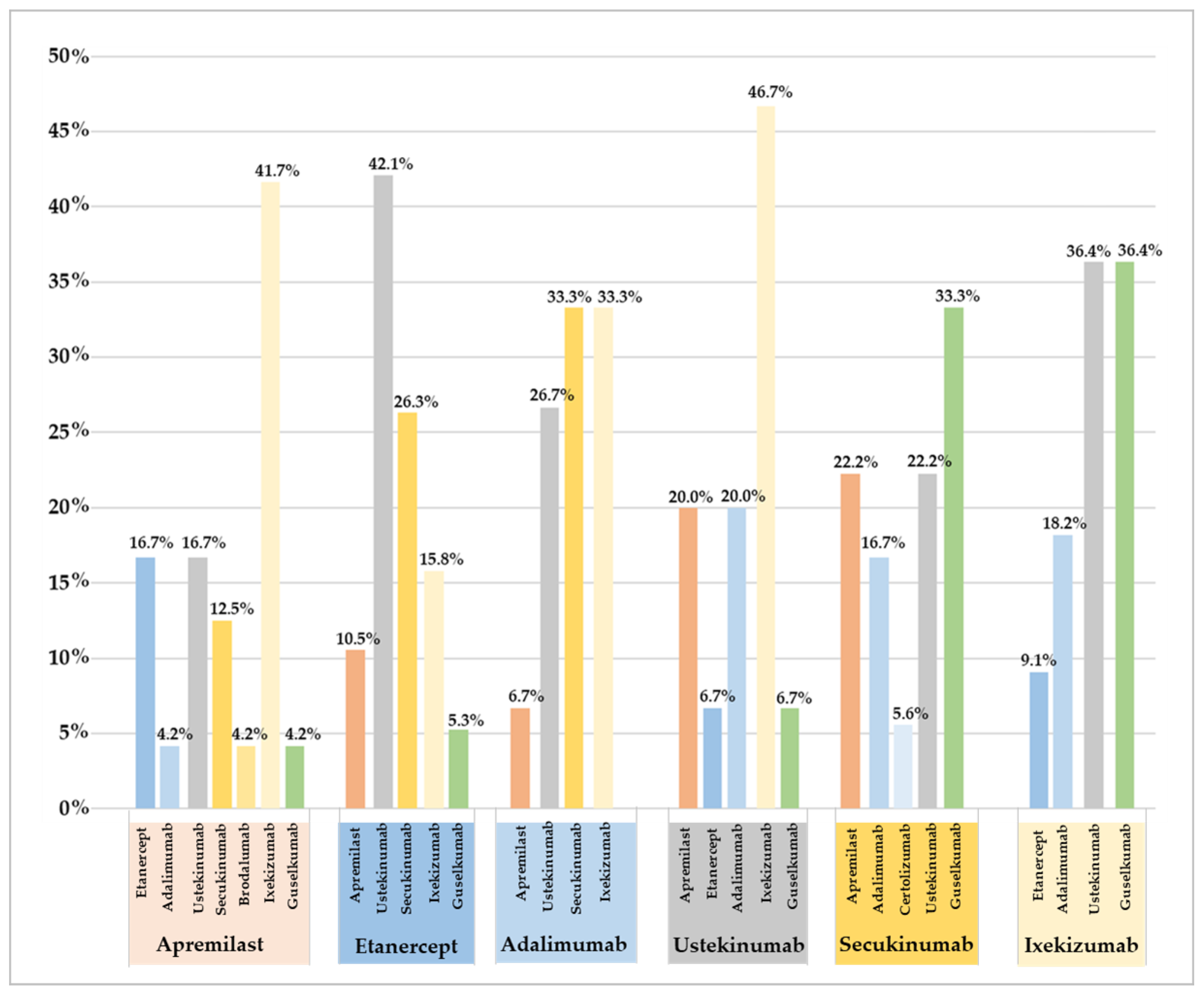
| Swap, N (%) | 106 (13.1) | 24 (14.5) | 19 (33.9) | 15 (11.4) | 15 (12.1) | 18 (9.8) | 11 (7.8) |
| Mean days ± SD | 29 ± 84.8 | 34.3 ± 93.9 | 58.8 ± 98.6 | 24.5 ± 77.5 | 20.3 ± 64.8 | 27.2 ± 88.9 | 21.7 ± 79.2 |
| Switch, N (%) | 12 (1.5) | - | 2 (3.6) | 3 (2.3) | - | 5 (2.7) | 2 (1.4) |
| Mean days ± SD | 4.1 ± 35.9 | - | 8 ± 49.9 | 7.4 ± 48.5 | - | 7.5 ± 49.1 | 3.9 ± 33.1 |
| Discontinuation phase | |||||||
| 30-day gap | |||||||
| Adherent, N (%) | 390 (48.7) | 78 (47.3) | 29 (51.8) | 66 (50.0) | 40 (32.3) | 110 (60.1) | 67 (47.5) |
| Mean days ± SD | 167.9 ± 107.1 | 163.9 ± 90 | 201.8 ± 110 | 164.9 ± 95.2 | 138.4 ± 109.3 | 182 ± 118.3 | 182.4 ± 115.5 |
| 60-day gap | |||||||
| Adherent, N (%) | 515 (64.3) | 93 (56.4) | 38 (67.9) | 81 (61.4) | 80 (64.5) | 135 (73.8) | 88 (62.4) |
| Mean days ± SD | 176.6 ± 101.7 | 161.3 ± 75.4 | 222.7 ± 110.1 | 163 ± 90.5 | 177.9 ± 120.8 | 195.8 ± 120.3 | 176.4 ± 101.6 |
| 90-day gap | |||||||
| Adherent, N (%) | 570 (71.2) | 99 (60.0) | 42 (75.0) | 89 (67.4) | 102 (82.3) | 142 (77.6) | 96 (68.1) |
| Mean days ± SD | 170 ± 90.9 | 153.1 ± 67.9 | 217.1 ± 103.3 | 152.7 ± 85.1 | 202.7 ± 95.4 | 183.5 ± 110 | 168.1 ± 93.9 |
| Characteristics | Unadjusted OR (95% CI) | p-Value | Adjusted OR (95% CI) | p-Value |
|---|---|---|---|---|
| Men (vs. women) | 0.908 (0.686–1.203) | 0.501 | 0.922 (0.681–1.249) | 0.6 |
| Age | ||||
| 19–40 y (vs. under 18) | 1.644 (0.734–3.681) | 0.227 | 1.595 (0.663–3.838) | 0.298 |
| 41–65 y (vs. under 18) | 1.166 (0.533–2.549) | 0.701 | 1.146 (0.472–2.783) | 0.764 |
| Over 65 y (vs. under 18) | 1.5 (0.656–3.431) | 0.337 | 1.585 (0.595–4.225) | 0.357 |
| Regimen complexity | ||||
| Polypharmacy (5–9 drugs) (vs. no polytherapy) | 0.714 (0.505–1.010) | 0.057 | 0.743 (0.515–1.072) | 0.113 |
| Excessive polypharmacy (≥10 drugs) (vs. no polytherapy) | 0.76 (0.543–1.064) | 0.11 | 0.679 (0.453–1.016) | 0.06 |
| Therapy change | ||||
| Swap | 2.696 (1.723–4.219) | <0.001 * | 2.835 (1.774–4.529) | <0.001 * |
| Switch | 0.466 (0.139–1.561) | 0.216 | 0.534 (0.152–1.875) | 0.327 |
| Index PSO treatment | ||||
| Apremilast | 1.065 (0.756–1.499) | 0.719 | 0.817 (0.222–3.003) | 0.761 |
| Etanercept | 0.869 (0.505–1.496) | 0.613 | 0.606 (0.154–2.382) | 0.473 |
| Adalimumab | 0.932 (0.642–1.353) | 0.71 | 0.712 (0.191–2.651) | 0.612 |
| Ustekinumab | 2.226 (1.484–3.337) | <0.001 * | 1.574 (0.423–5.861) | 0.499 |
| Secukinumab | 0.546 (0.391–0.764) | <0.001 * | 0.482 (0.132–1.761) | 0.269 |
| Ixekizumab | 1.05 (0.73–1.51) | 0.793 | 0.819 (0.222–3.023) | 0.765 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mucherino, S.; Rafaniello, C.; Serino, M.; Zinzi, A.; Trama, U.; Capuano, A.; Menditto, E.; Orlando, V. Drug Utilization and Measurement of Medication Adherence: A Real World Study of Psoriasis in Italy. Pharmaceutics 2023, 15, 2647. https://doi.org/10.3390/pharmaceutics15122647
Mucherino S, Rafaniello C, Serino M, Zinzi A, Trama U, Capuano A, Menditto E, Orlando V. Drug Utilization and Measurement of Medication Adherence: A Real World Study of Psoriasis in Italy. Pharmaceutics. 2023; 15(12):2647. https://doi.org/10.3390/pharmaceutics15122647
Chicago/Turabian StyleMucherino, Sara, Concetta Rafaniello, Marianna Serino, Alessia Zinzi, Ugo Trama, Annalisa Capuano, Enrica Menditto, and Valentina Orlando. 2023. "Drug Utilization and Measurement of Medication Adherence: A Real World Study of Psoriasis in Italy" Pharmaceutics 15, no. 12: 2647. https://doi.org/10.3390/pharmaceutics15122647