
Effects of Statin Combinations on Zika Virus Infection in Vero Cells

Abstract
:1. Introduction
2. Materials and Methods
2.1. Cells, Virus, and Reagents
2.2. Fixed-Ratio Combinations
2.3. Anti-ZIKV Activity of Statin Combinations in Vero Cells
2.4. Determination of Synergy
3. Results
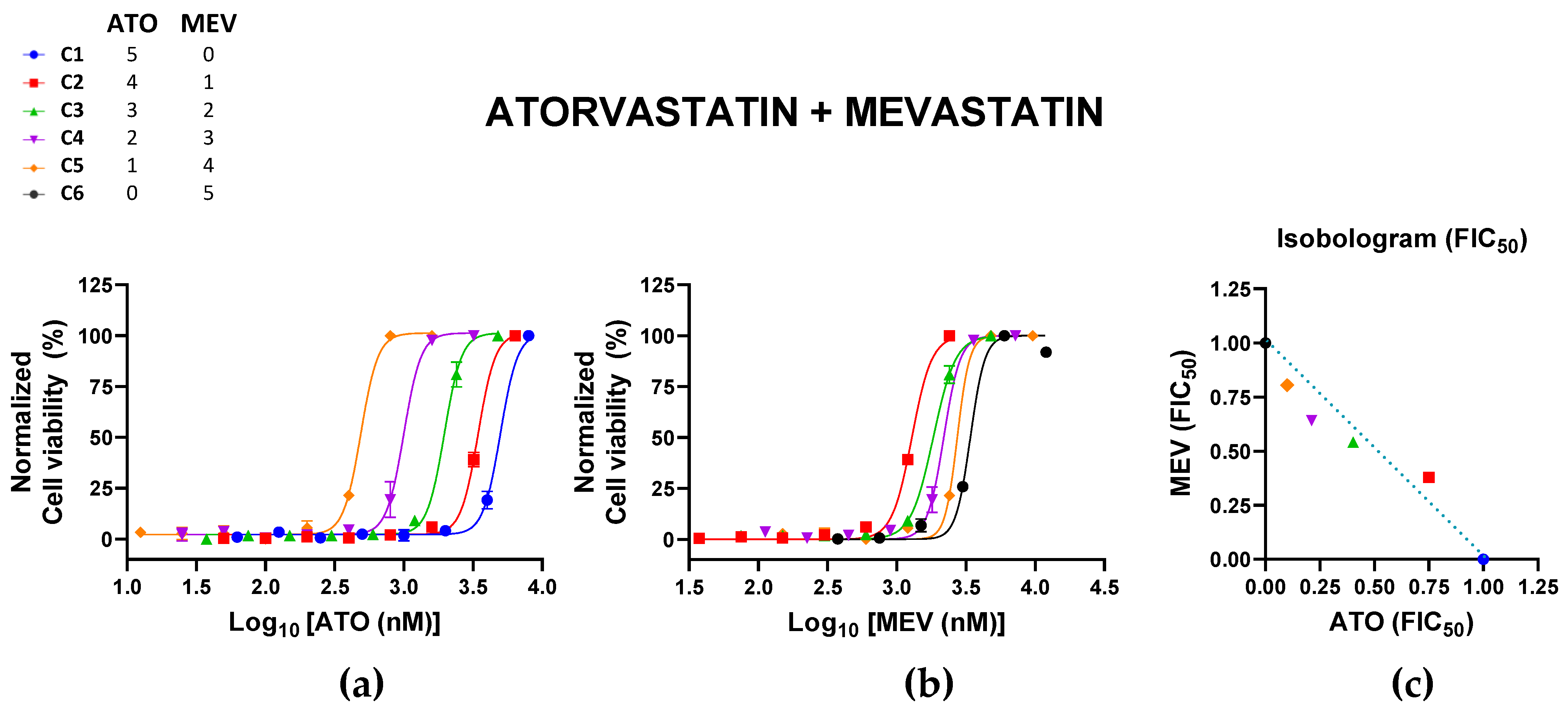
3.1. Atorvastatin and Mevastatin
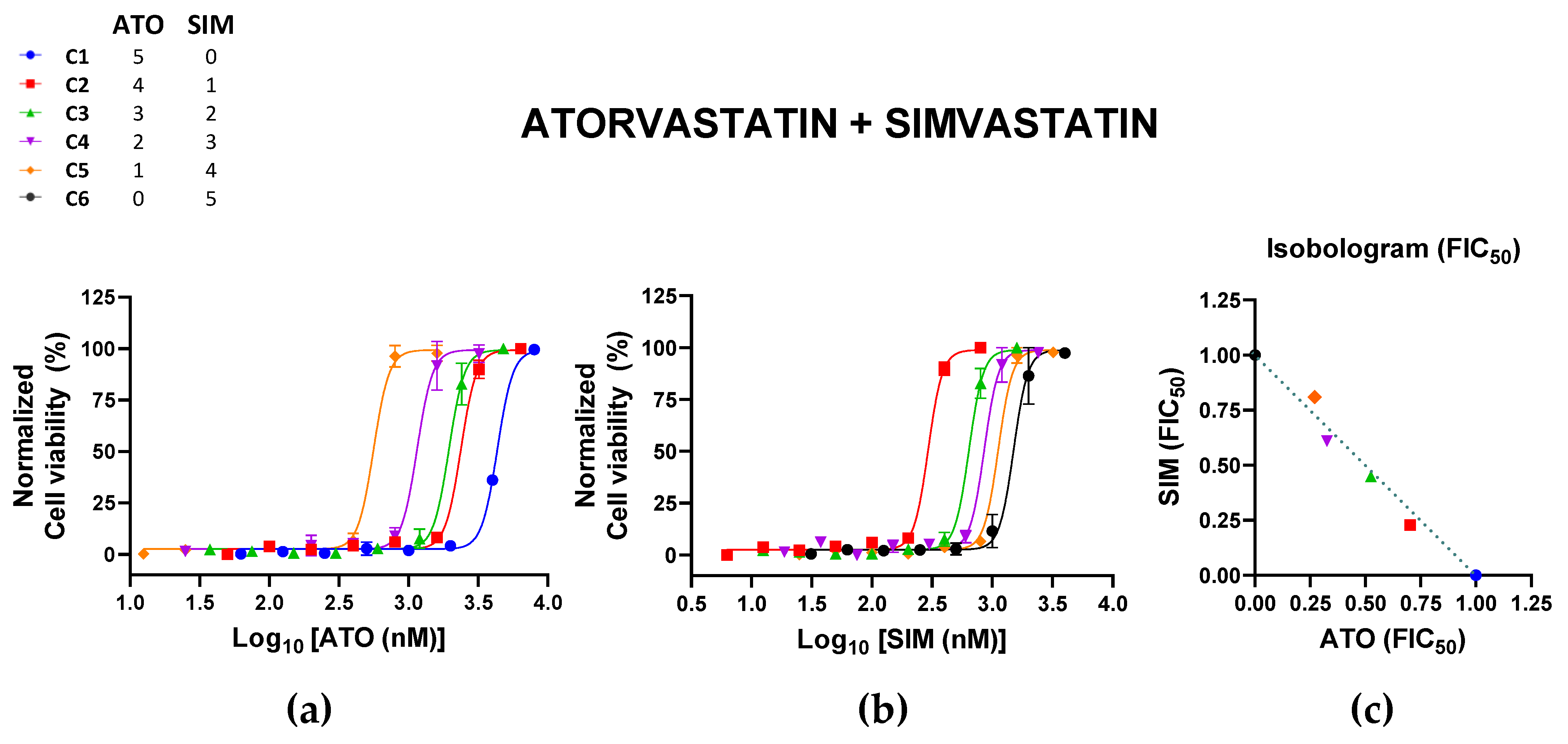
3.2. Atorvastatin and Simvastatin
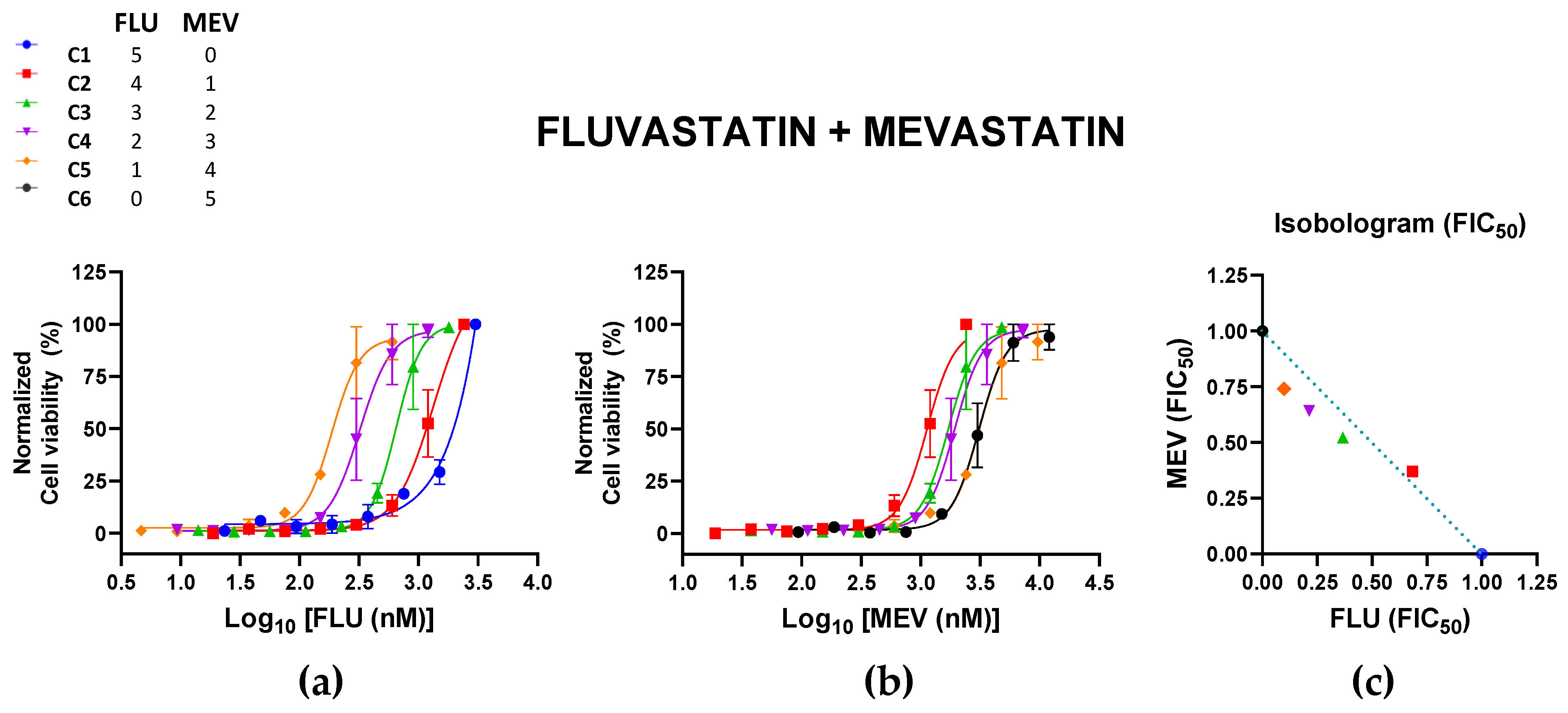
3.3. Fluvastatin and Mevastatin
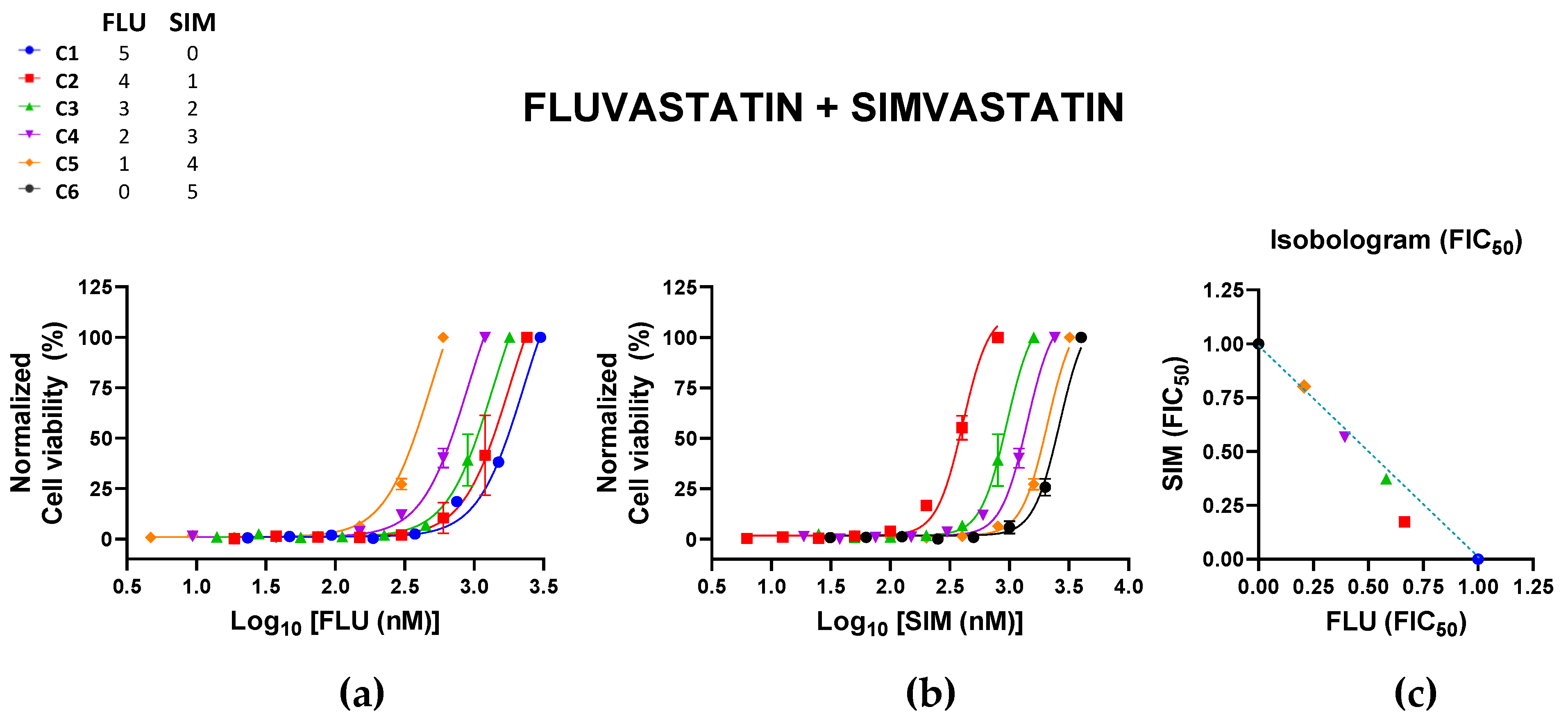
3.4. Fluvastatin and Simvastatin
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gutierrez-Bugallo, G.; Piedra, L.A.; Rodriguez, M.; Bisset, J.A.; Lourenco-de-Oliveira, R.; Weaver, S.C.; Vasilakis, N.; Vega-Rua, A. Vector-borne transmission and evolution of Zika virus. Nat. Ecol. Evol. 2019, 3, 561–569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boyer, S.; Calvez, E.; Chouin-Carneiro, T.; Diallo, D.; Failloux, A.B. An overview of mosquito vectors of Zika virus. Microbes. Infect. 2018, 20, 646–660. [Google Scholar] [CrossRef]
- Kraemer, M.U.G.; Reiner, R.C., Jr.; Brady, O.J.; Messina, J.P.; Gilbert, M.; Pigott, D.M.; Yi, D.; Johnson, K.; Earl, L.; Marczak, L.B.; et al. Past and future spread of the arbovirus vectors Aedes aegypti and Aedes albopictus. Nat. Microbiol. 2019, 4, 854–863. [Google Scholar] [CrossRef] [Green Version]
- Duffy, M.R.; Chen, T.H.; Hancock, W.T.; Powers, A.M.; Kool, J.L.; Lanciotti, R.S.; Pretrick, M.; Marfel, M.; Holzbauer, S.; Dubray, C.; et al. Zika virus outbreak on Yap Island, Federated States of Micronesia. N. Engl. J. Med. 2009, 360, 2536–2543. [Google Scholar] [CrossRef] [PubMed]
- Musso, D.; Gubler, D.J. Zika Virus. Clin. Microbiol. Rev. 2016, 29, 487–524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao-Lormeau, V.M.; Blake, A.; Mons, S.; Lastere, S.; Roche, C.; Vanhomwegen, J.; Dub, T.; Baudouin, L.; Teissier, A.; Larre, P.; et al. Guillain-Barre Syndrome outbreak associated with Zika virus infection in French Polynesia: A case-control study. Lancet 2016, 387, 1531–1539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mier-y-Teran-Romero, L.; Delorey, M.J.; Sejvar, J.J.; Johansson, M.A. Guillain–Barré syndrome risk among individuals infected with Zika virus: A multi-country assessment. BMC Med. 2018, 16, 67. [Google Scholar] [CrossRef] [PubMed]
- Musso, D.; Ko, A.I.; Baud, D. Zika Virus Infection—After the Pandemic. N. Engl. J. Med. 2019, 381, 1444–1457. [Google Scholar] [CrossRef]
- Hoen, B.; Schaub, B.; Funk, A.L.; Ardillon, V.; Boullard, M.; Cabie, A.; Callier, C.; Carles, G.; Cassadou, S.; Cesaire, R.; et al. Pregnancy Outcomes after ZIKV Infection in French Territories in the Americas. N. Engl. J. Med. 2018, 378, 985–994. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Prioritizing Diseases for Research and Development in Emergency Contexts. Available online: https://www.who.int/activities/prioritizing-diseases-for-research-and-development-in-emergency-contexts (accessed on 25 October 2022).
- Españo, E.; Nam, J.H.; Song, E.J.; Song, D.; Lee, C.K.; Kim, J.K. Lipophilic statins inhibit Zika virus production in Vero cells. Sci. Rep. 2019, 9, 11461. [Google Scholar] [CrossRef]
- Moghadasian, M.H. Clinical pharmacology of 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitors. Life Sci. 1999, 65, 1329–1337. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Gutierrez, M.; Castellanos, J.E.; Gallego-Gomez, J.C. Statins reduce dengue virus production via decreased virion assembly. Intervirology 2011, 54, 202–216. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Gutierrez, M.; Correa-Londono, L.A.; Castellanos, J.E.; Gallego-Gomez, J.C.; Osorio, J.E. Lovastatin delays infection and increases survival rates in AG129 mice infected with dengue virus serotype 2. PLoS ONE 2014, 9, e87412. [Google Scholar] [CrossRef]
- Wani, M.A.; Mukherjee, S.; Mallick, S.; Akbar, I.; Basu, A. Atorvastatin ameliorates viral burden and neural stem/ progenitor cell (NSPC) death in an experimental model of Japanese encephalitis. J. Biosci. 2020, 45, 77. [Google Scholar] [CrossRef] [PubMed]
- US FDA. FDA Requests Removal of Strongest Warning against Using Cholesterol-Lowering Statins during Pregnancy; Still Advises Most Pregnant Patients Should Stop Taking Statins: Breastfeeding Not Recommended in Patients Who Require Statins. 2021. Available online: https://www.fda.gov/drugs/drug-safety-and-availability/fda-requests-removal-strongest-warning-against-using-cholesterol-lowering-statins-during-pregnancy (accessed on 26 October 2022).
- Komarasamy, T.V.; Adnan, N.A.A.; James, W.; Balasubramaniam, V.R. Finding a chink in the armor: Update, limitations, and challenges toward successful antivirals against flaviviruses. PLoS Negl. Trop. Dis. 2022, 16, e0010291. [Google Scholar] [CrossRef]
- Taylor, B.A.; Thompson, P.D. Statin-Associated Muscle Disease: Advances in Diagnosis and Management. Neurotherapeutics 2018, 15, 1006–1017. [Google Scholar] [CrossRef] [Green Version]
- Rosenson, R.S.; Gandra, S.R.; McKendrick, J.; Dent, R.; Wieffer, H.; Cheng, L.-I.; Catapano, A.L.; Oh, P.; Kees Hovingh, G.; Stroes, E.S. Identification and Management of Statin-Associated Symptoms in Clinical Practice: Extension of a Clinician Survey to 12 Further Countries. Cardiovasc. Drugs Ther. 2017, 31, 187–195. [Google Scholar] [CrossRef] [Green Version]
- Dostal, L.A.; Schardein, J.L.; Anderson, J.A. Developmental toxicity of the HMG-CoA reductase inhibitor, atorvastatin, in rats and rabbits. Teratology 1994, 50, 387–394. [Google Scholar] [CrossRef]
- Minsker, D.H.; MacDonald, J.S.; Robertson, R.T.; Bokelman, D.L. Mevalonate supplementation in pregnant rats suppresses the teratogenicity of mevinolinic acid, an inhibitor of 3-hydroxy-3-methylglutaryl-coenzyme a reductase. Teratology 1983, 28, 449–456. [Google Scholar] [CrossRef]
- Ghidin, A.; Sicherer, S.; Willner, J. Congenital abnormalities (VATER) in baby born to mother using lovastatin. Lancet 1992, 339, 1416–1417. [Google Scholar] [CrossRef]
- Karadas, B.; Uysal, N.; Erol, H.; Acar, S.; Koc, M.; Kaya-Temiz, T.; Koren, G.; Kaplan, Y.C. Pregnancy outcomes following maternal exposure to statins: A systematic review and meta-analysis. Br. J. Clin. Pharmacol. 2022, 88, 3962–3976. [Google Scholar] [CrossRef] [PubMed]
- Winterfeld, U.; Allignol, A.; Panchaud, A.; Rothuizen, L.E.; Merlob, P.; Cuppers-Maarschalkerweerd, B.; Vial, T.; Stephens, S.; Clementi, M.; De Santis, M.; et al. Pregnancy outcome following maternal exposure to statins: A multicentre prospective study. BJOG 2013, 120, 463–471. [Google Scholar] [CrossRef] [PubMed]
- Taguchi, N.; Rubin, E.T.; Hosokawa, A.; Choi, J.; Ying, A.Y.; Moretti, M.E.; Koren, G.; Ito, S. Prenatal exposure to HMG-CoA reductase inhibitors: Effects on fetal and neonatal outcomes. Reprod. Toxicol. 2008, 26, 175–177. [Google Scholar] [CrossRef]
- Bateman, B.T.; Hernandez-Diaz, S.; Fischer, M.A.; Seely, E.W.; Ecker, J.L.; Franklin, J.M.; Desai, R.J.; Allen-Coleman, C.; Mogun, H.; Avorn, J.; et al. Statins and congenital malformations: Cohort study. BMJ 2015, 350, h1035. [Google Scholar] [CrossRef] [Green Version]
- Ward, N.C.; Watts, G.F.; Eckel, R.H. Statin Toxicity. Circ. Res. 2019, 124, 328–350. [Google Scholar] [CrossRef] [PubMed]
- Banach, M.; Rizzo, M.; Toth, P.P.; Farnier, M.; Davidson, M.H.; Al-Rasadi, K.; Aronow, W.S.; Athyros, V.; Djuric, D.M.; Ezhov, M.V.; et al. Position paper: Statin intolerance—An attempt at a unified definition. Position paper from an International Lipid Expert Panel. Arch. Med. Sci. 2015, 11, 1–23. [Google Scholar] [CrossRef]
- McKenney, J.M. Pharmacologic characteristics of statins. Clin. Cardiol. 2003, 26, 32–38. [Google Scholar] [CrossRef]
- Schachter, M. Chemical, pharmacokinetic and pharmacodynamic properties of statins: An update. Fundam. Clin. Pharmacol. 2005, 19, 117–125. [Google Scholar] [CrossRef]
- Björkhem-Bergman, L.; Lindh, J.D.; Bergman, P. What is a relevant statin concentration in cell experiments claiming pleiotropic effects? Br. J. Clin. Pharmacol. 2011, 72, 164–165. [Google Scholar] [CrossRef] [Green Version]
- Ghim, J.L.; Phuong, N.T.T.; Kim, M.J.; Kim, E.J.; Song, G.S.; Ahn, S.; Shin, J.G.; Kim, E.Y. Pharmacokinetics of fixed-dose combination of atorvastatin and metformin compared with individual tablets. Drug Des. Dev. Ther. 2019, 13, 1623–1632. [Google Scholar] [CrossRef]
- Mysore, Y.; Del Amo, E.M.; Loukovaara, S.; Hagstrom, M.; Urtti, A.; Kauppinen, A. Statins for the prevention of proliferative vitreoretinopathy: Cellular responses in cultured cells and clinical statin concentrations in the vitreous. Sci. Rep. 2021, 11, 980. [Google Scholar] [CrossRef] [PubMed]
- Barilla, D.; Prasad, P.; Hubert, M.; Gumbhir-Shah, K. Steady-state pharmacokinetics of fluvastatin in healthy subjects following a new extended release fluvastatin tablet, Lescol XL. Biopharm. Drug Dispos. 2004, 25, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Siekmeier, R.; Lattke, P.; Mix, C.; Park, J.W.; Jaross, W. Dose dependency of fluvastatin pharmacokinetics in serum determined by reversed phase HPLC. J. Cardiovasc. Pharmacol. Ther. 2001, 6, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Fung, E.C.; Crook, M.A. Statin Myopathy: A Lipid Clinic Experience on the Tolerability of Statin Rechallenge. Cardiovasc. Ther. 2012, 30, e212–e218. [Google Scholar] [CrossRef]
- Corsini, A. The Safety of HMG-CoA Reductase Inhibitors in Special Populations at High Cardiovascular Risk. Cardiovasc. Drugs Ther. 2003, 17, 265–285. [Google Scholar] [CrossRef]
- Gorabi, A.M.; Kiaie, N.; Bianconi, V.; Jamialahmadi, T.; Al-Rasadi, K.; Johnston, T.P.; Pirro, M.; Sahebkar, A. Antiviral effects of statins. Prog. Lipid Res. 2020, 79, 101054. [Google Scholar] [CrossRef]
- Saheki, A.; Terasaki, T.; Tamai, I.; Tsuji, A. In vivo and in vitro blood-brain barrier transport of 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase inhibitors. Pharm. Res. 1994, 11, 305–311. [Google Scholar] [CrossRef]
- Wood, W.G.; Eckert, G.P.; Igbavboa, U.; Muller, W.E. Statins and neuroprotection: A prescription to move the field forward. Ann. N. Y. Acad. Sci. 2010, 1199, 69–76. [Google Scholar] [CrossRef] [Green Version]
- Guillot, F.; Misslin, P.; Lemaire, M. Comparison of Fluvastatin and Lovastatin Blood-Brain Barrier Transfer Using In Vitro and In Vivo Methods. J. Cardiovasc. Pharmacol. 1993, 21, 339–346. [Google Scholar] [CrossRef]
- Whitehorn, J.; Nguyen, C.V.V.; Khanh, L.P.; Kien, D.T.H.; Quyen, N.T.H.; Tran, N.T.T.; Hang, N.T.; Truong, N.T.; Tai, L.T.H.; Huong, N.T.C.; et al. Lovastatin for the Treatment of Adult Patients With Dengue: A Randomized, Double-Blind, Placebo-Controlled Trial. Clin. Infect. Dis. 2016, 62, 468–476. [Google Scholar] [CrossRef]
- Zapatero-Belinchon, F.J.; Moeller, R.; Lasswitz, L.; van Ham, M.; Becker, M.; Brogden, G.; Rosendal, E.; Bi, W.; Carriqui-Madronal, B.; Islam, K.; et al. Fluvastatin mitigates SARS-CoV-2 infection in human lung cells. iScience 2021, 24, 103469. [Google Scholar] [CrossRef] [PubMed]
- Polacek, C.; Friebe, P.; Harris, E. Poly(A)-binding protein binds to the non-polyadenylated 3’ untranslated region of dengue virus and modulates translation efficiency. J. Gen. Virol. 2009, 90, 687–692. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, D.; Dastidar, D.G.; Roy, K.; Ghosh, A.; Mukhopadhyay, D.; Sikdar, N.; Biswas, N.K.; Chakrabarti, G.; Das, A. Computational prediction of the molecular mechanism of statin group of drugs against SARS-CoV-2 pathogenesis. Sci. Rep. 2022, 12, 6241. [Google Scholar] [CrossRef] [PubMed]
- Zapata-Cardona, M.I.; Florez-Alvarez, L.; Zapata-Builes, W.; Guerra-Sandoval, A.L.; Guerra-Almonacid, C.M.; Hincapie-Garcia, J.; Rugeles, M.T.; Hernandez, J.C. Atorvastatin Effectively Inhibits Ancestral and Two Emerging Variants of SARS-CoV-2 in vitro. Front. Microbiol. 2022, 13, 721103. [Google Scholar] [CrossRef]
- Cho, D.-H.; Choi, J.; Gwon, J.G. Atorvastatin Reduces the Severity of COVID-19: A Nationwide, Total Population-Based, Case-Control Study. COVID 2022, 2, 398–406. [Google Scholar] [CrossRef]
- Mason, R.P.; Walter, M.F.; Day, C.A.; Jacob, R.F. Intermolecular differences of 3-hydroxy-3-methylglutaryl coenzyme a reductase inhibitors contribute to distinct pharmacologic and pleiotropic actions. Am. J. Cardiol. 2005, 96, 11–23. [Google Scholar] [CrossRef]
- Galiullina, L.F.; Aganova, O.V.; Latfullin, I.A.; Musabirova, G.S.; Aganov, A.V.; Klochkov, V.V. Interaction of different statins with model membranes by NMR data. Biochim. Biophys. Acta Biomembr. 2017, 1859, 295–300. [Google Scholar] [CrossRef]
- Lin, C.P.; Hsiao, F.C.; Wu, C.T.; Lin, Y.S.; Chen, S.W.; Chu, P.H. Beneficial Effects of Fixed-Dose Combination of Amlodipine and Atorvastatin in Patients with Concomitant Hypertension and Hypercholesterolemia: A Multi-Institutional Cohort Study. Acta Cardiol. Sin. 2022, 38, 736–750. [Google Scholar] [CrossRef]
- Kim, B.K.; Hong, S.J.; Lee, Y.J.; Hong, S.J.; Yun, K.H.; Hong, B.K.; Heo, J.H.; Rha, S.W.; Cho, Y.H.; Lee, S.J.; et al. Long-term efficacy and safety of moderate-intensity statin with ezetimibe combination therapy versus high-intensity statin monotherapy in patients with atherosclerotic cardiovascular disease (RACING): A randomised, open-label, non-inferiority trial. Lancet 2022, 400, 380–390. [Google Scholar] [CrossRef]
- Park, M.S.; Youn, J.C.; Kim, E.J.; Han, K.H.; Lee, S.H.; Kim, S.H.; Kim, B.J.; Kwon, S.U.; Ryu, K.H. Efficacy and Safety of Fenofibrate-Statin Combination Therapy in Patients With Inadequately Controlled Triglyceride Levels Despite Previous Statin Monotherapy: A Multicenter, Randomized, Double-blind, Phase IV Study. Clin. Ther. 2021, 43, 1735–1747. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Combi. | Starting Conc. (µM) | EC50 a | FIC50 b | CI | |||
|---|---|---|---|---|---|---|---|
| (Ratio) | ATO | MEV | ATO (nM) | MEV (nM) | ATO | MEV | ΣFIC50 b |
| C1 (5:0) | 8 | 0 | 4568 (4102–5034) | 0 | 1.00 | 0 | 1.00 |
| C2 (4:1) | 6.4 | 2.4 | 3433 (3312–3554) | 1287 (1237–1337) | 0.750 (±0.003) | 0.378 (±0.007) | 1.129 (±0.011) |
| C3 (3:2) | 4.8 | 4.8 | 1837 (1770–1908) | 1837 (1764–1916) | 0.402 (±0.008) | 0.541 (±0.019) | 0.943 (±0.027) |
| C4 (2:3) | 3.2 | 7.2 | 971.7 (899–1044) | 2186 (2917–2355) | 0.212 (±0.002) | 0.642 (±0.017) | 0.854 (±0.019) |
| C5 (1:4) | 1.6 | 9.6 | 456.6 (412–501) | 2739 (2474–3004) | 0.100 (±0.002) | 0.805 (±0.0001) | 0.905 (±0.001) |
| C6 (0:5) | 0 | 12 | 0 | 3404 (3020–3788) | 0 | 1.00 | 1.00 |
| Combi. | Starting Conc. (µM) | EC50 a | FIC50 b | CI | |||
|---|---|---|---|---|---|---|---|
| (Ratio) | ATO | SIM | ATO (nM) | SIM (nM) | ATO | SIM | ΣFIC50 b |
| C1 (5:0) | 8 | 0 | 4639 (3274–6574) | 0 | 1.00 | 0 | 1.00 |
| C2 (4:1) | 6.4 | 0.8 | 2391 (2257–2532) | 298.8 (282–317) | 0.703 (±0.163) | 0.228 (±0.027) | 0.930 (±−0.136) |
| C3 (3:2) | 4.8 | 1.6 | 1870 (1741–2009) | 623.5 (581–670) | 0.524 (±0.136) | 0.448 (±0.040) | 0.972 (±0.096) |
| C4 (2:3) | 3.2 | 2.4 | 1138 (973–1330) | 852.5 (738–985) | 0.327 (±0.110) | 0.609 (±0.003) | 0.934 (±0.106) |
| C5 (1:4) | 1.6 | 3.2 | 536.8 (446–644) | 1068 (907–1258) | 0.270 (±0.162) | 0.808 (±0.006) | 1.08 (±0.156) |
| C6 (0:5) | 0 | 4 | 0 | 1804 (1336–2435) | 0 | 1.00 | 1.00 |
| Combi. | Starting Conc. (µM) | EC50 a | FIC50 b | CI | |||
|---|---|---|---|---|---|---|---|
| (Ratio) | FLU | MEV | FLU (nM) | MEV (nM) | FLU | MEV | ΣFIC50 b |
| C1 (5:0) | 3 | 0 | 1726 (1544–1978) | 0 | 1.00 | 0 | 1.00 |
| C2 (4:1) | 2.4 | 2.4 | 1128 (992–1266) | 1128 (992–1266) | 0.684 (±0.051) | 0.371 (±0.118) | 1.054 (±0.169) |
| C3 (3:2) | 1.8 | 4.8 | 641.5 (911–1044) | 1711 (1498–1952) | 0.367 (±0.075) | 0.522 (±0.005) | 0.889 (±0.080) |
| C4 (2:3) | 1.2 | 7.2 | 641.9 (562–732.2) | 1952 (1651–2319) | 0.213 (±0.066) | 0.642 (±0.055) | 0.855 (±0.121) |
| C5 (1:4) | 0.6 | 9.6 | 325.3 (275–387) | 3053 (2513–3656) | 0.0.99 (±0.049) | 0.740 (±0.215) | 0.839 (±0.264) |
| C6 (0:5) | 0 | 12 | 0 | 3096 (2726–3519) | 0 | 1.00 | 1.00 |
| Combi. | Starting Conc. (µM) | EC50 a | FIC50 b | CI | |||
|---|---|---|---|---|---|---|---|
| (Ratio) | FLU | SIM | FLU (nM) | SIM (nM) | FLU | SIM | ΣFIC50 b |
| C1 (5:0) | 3 | 0 | 1630 (1513–1752) | 0 | 1.00 | 0 | 1.00 |
| C2 (4:1) | 2.4 | 0.8 | 1073 (995–1154) | 357.8 (331–385) | 0.664 (±0.056) | 0.174 (±0.026) | 0.838 (±0.082) |
| C3 (3:2) | 1.8 | 1.6 | 966.5 (911–1044) | 859.1 (810–928) | 0.582 (±0.053) | 0.373 (±0.027) | 0.955 (±0.080) |
| C4 (2:3) | 1.2 | 2.4 | 641.9 (601–684) | 1284 (1202–1368) | 0.393 (±0.022) | 0.567 (±0.022) | 0.956 (±0.043) |
| C5 (1:4) | 0.6 | 3.2 | 338.1 (315–361) | 1803 (1681–1925) | 0.208 (±0.004) | 0.802 (±0.003) | 1.01 (±0.007) |
| C6 (0:5) | 0 | 4 | 0 | 2259 (2091–2427) | 0 | 1.00 | 1.00 |
| Statin | EC50 (µM) | Cmax | Css | HMGCR IC50 (nM) |
|---|---|---|---|---|
| Atorvastatin | 4.6 | 8–40 nM | 31.9 ng/mL (57.10 nM) | 8.2 |
| Fluvastatin | 1.7 | 40 mg dose: 1.08 µM in males 1.58 µM in females | Lescol XL, 80 mg: 7.71–102.4 ng/mL (18–249 nM) Lescol XL, 160 mg: 25.3–258.8 (61–629 nM) Fluvastatin IR, 40 mg: 9.19–442.8 ng/mL (22–1077 nM) | 27.6 |
| Mevastatin | 3.4 | - | - | 23 |
| Simvastatin | 2.3 | 19–31 nM | 1.68 ng/mL (4.01 nM) | 11.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Españo, E.; Kim, J.-K. Effects of Statin Combinations on Zika Virus Infection in Vero Cells. Pharmaceutics 2023, 15, 50. https://doi.org/10.3390/pharmaceutics15010050
Españo E, Kim J-K. Effects of Statin Combinations on Zika Virus Infection in Vero Cells. Pharmaceutics. 2023; 15(1):50. https://doi.org/10.3390/pharmaceutics15010050
Chicago/Turabian StyleEspaño, Erica, and Jeong-Ki Kim. 2023. "Effects of Statin Combinations on Zika Virus Infection in Vero Cells" Pharmaceutics 15, no. 1: 50. https://doi.org/10.3390/pharmaceutics15010050