
Efficacy and Safety Evaluation of Mometasone Furoate in Treating Ocular Inflammation
 and
and 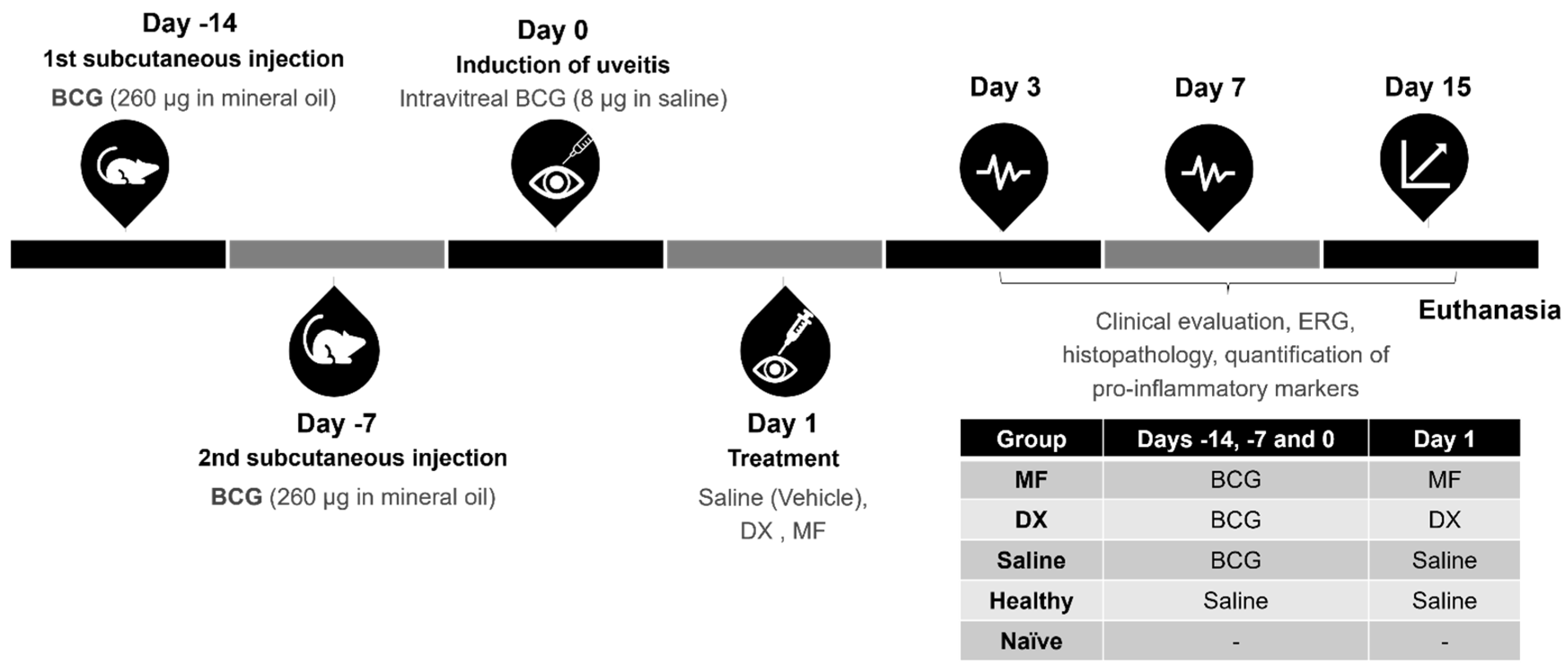{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals’ Preparation and Intravitreal Injections
2.2. In Vivo Ocular Safety Evaluation
2.3. In Vivo Anti-Inflammatory Activity
2.3.1. Induction of Uveitis and Treatment with MF
2.3.2. Ophthalmic Evaluation
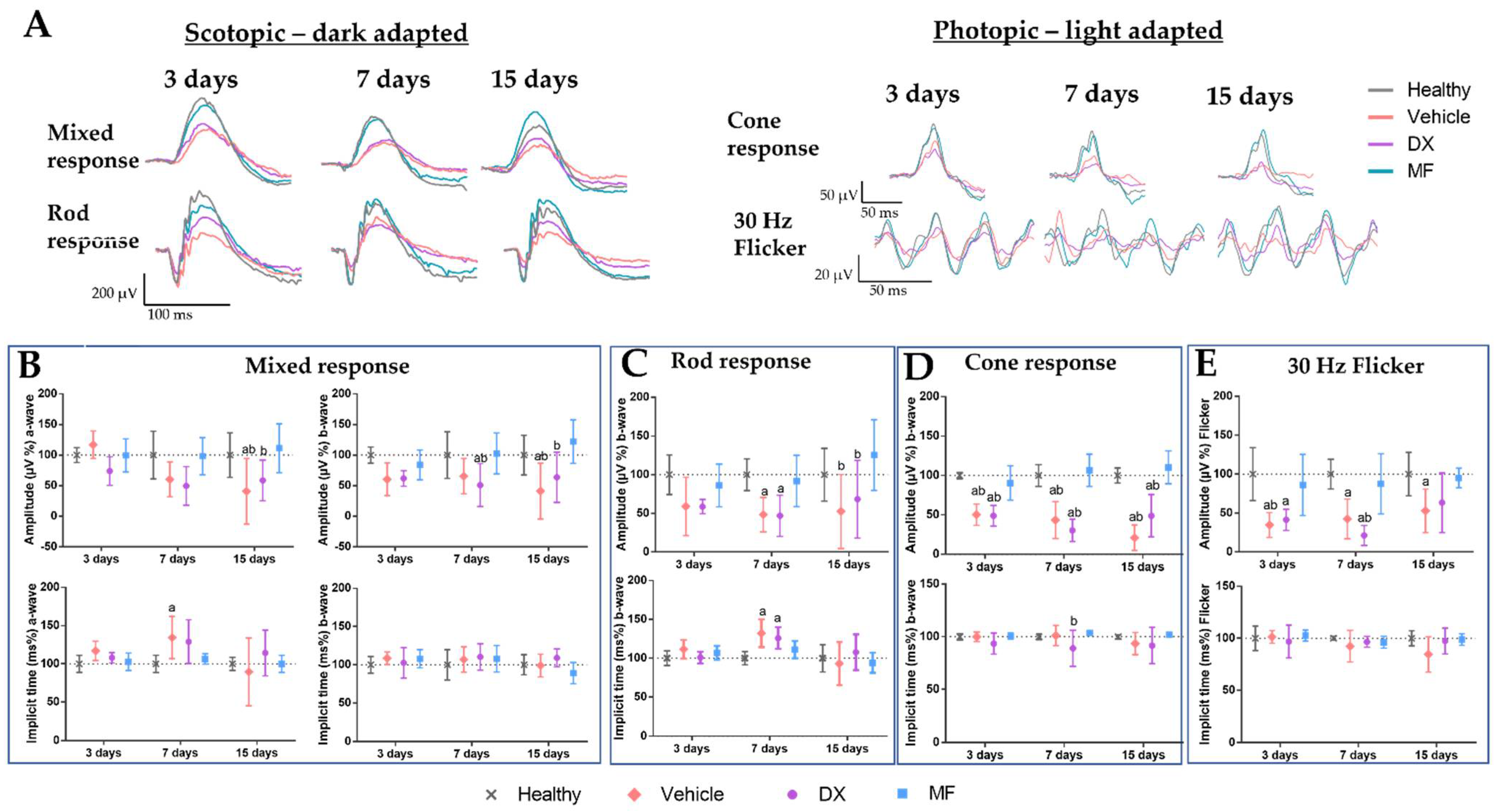
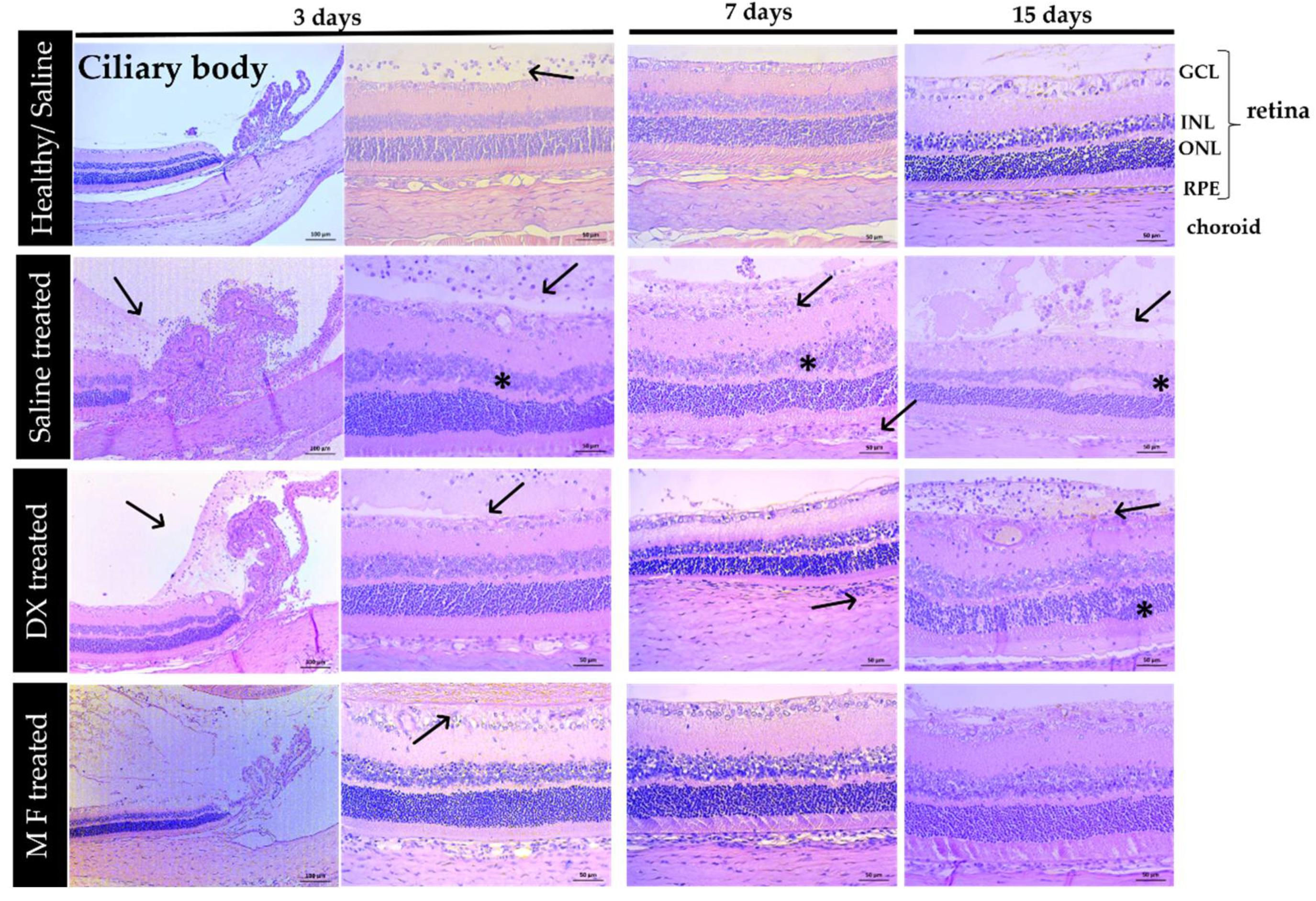
2.3.3. Electroretinography and Histopathological Analysis
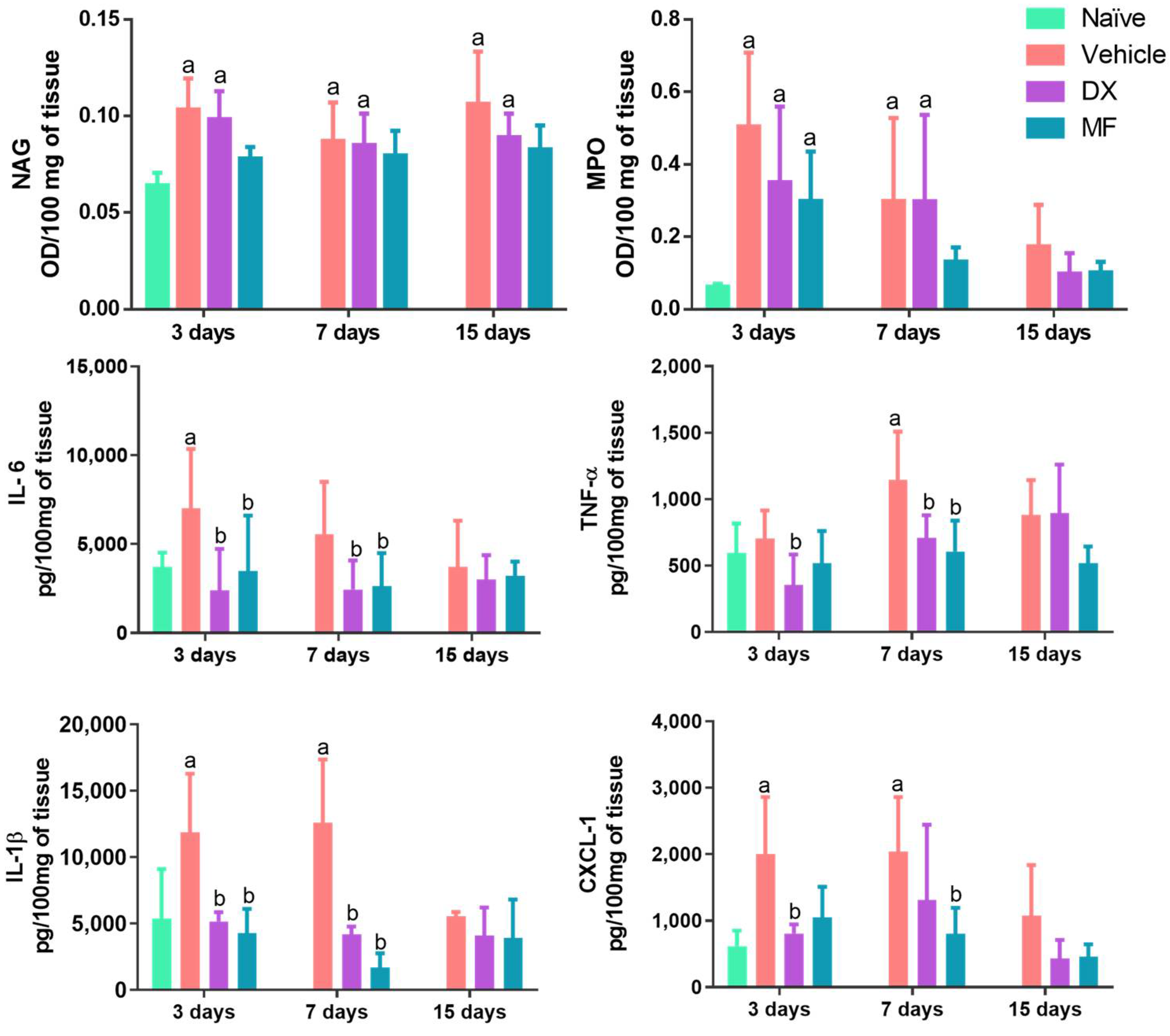
2.3.4. Quantification of Pro-Inflammatory Markers
2.3.5. Statistical Analysis
3. Results
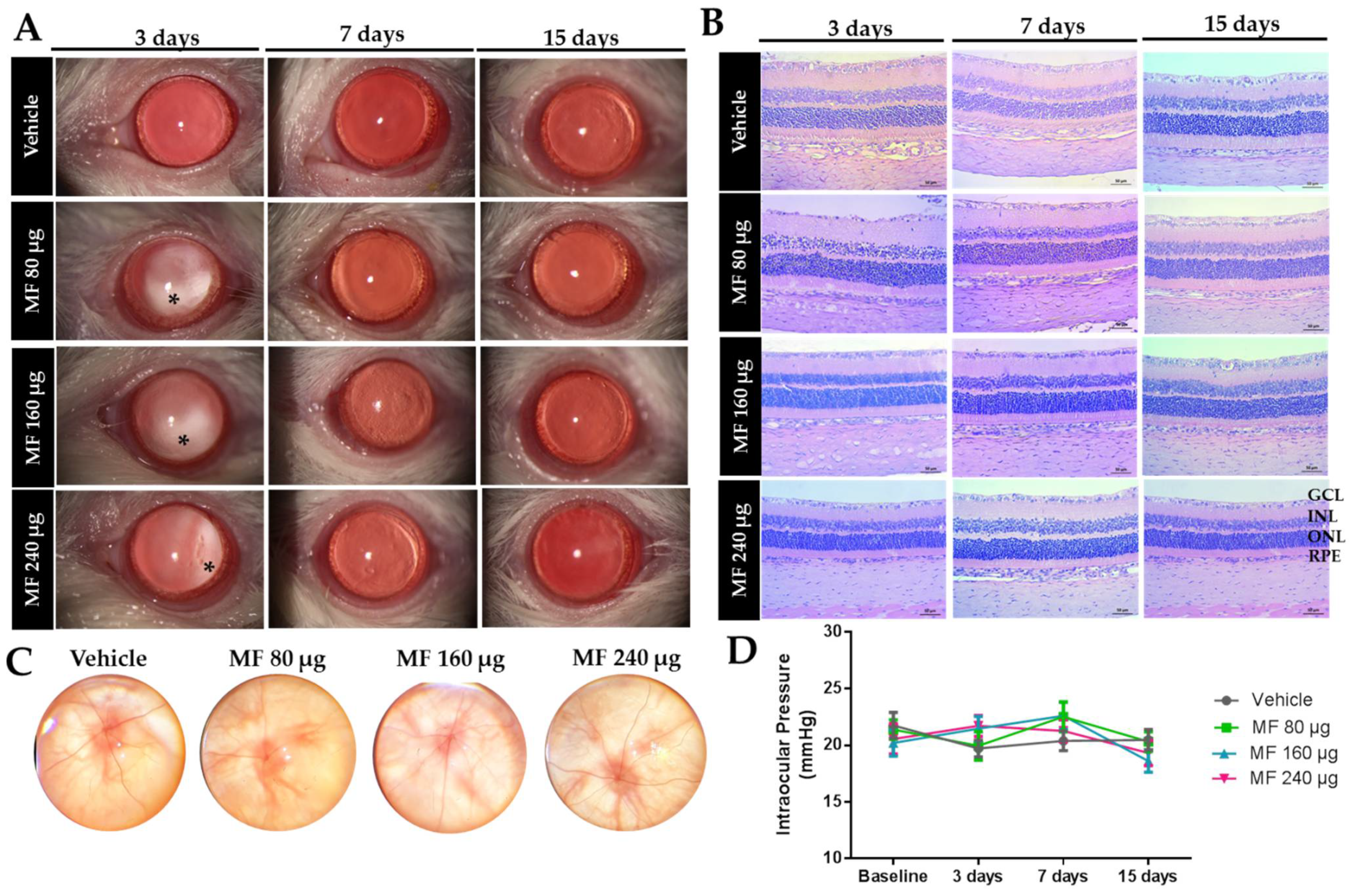
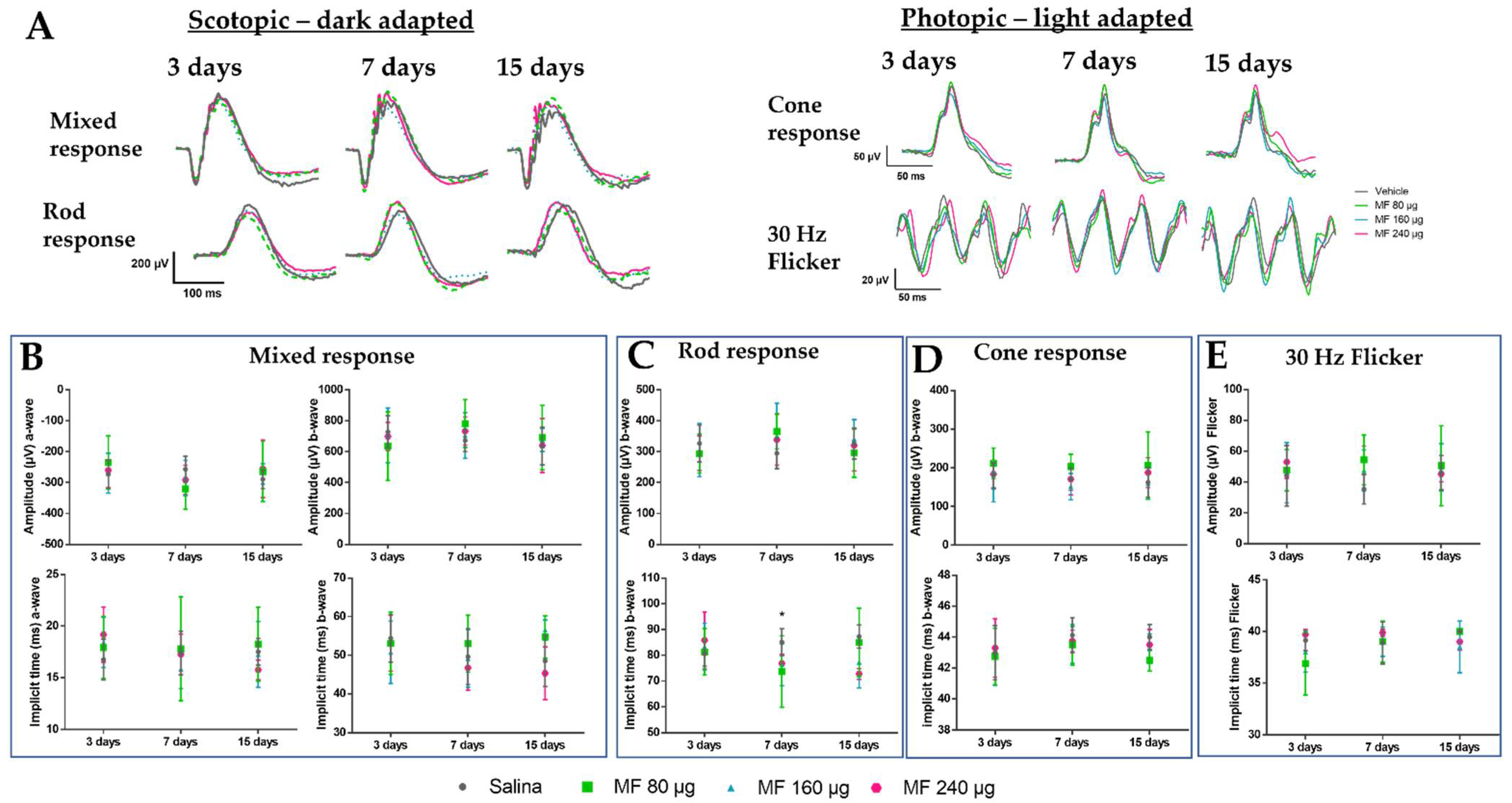
3.1. Safety Study of the Intraocular Administration of MF
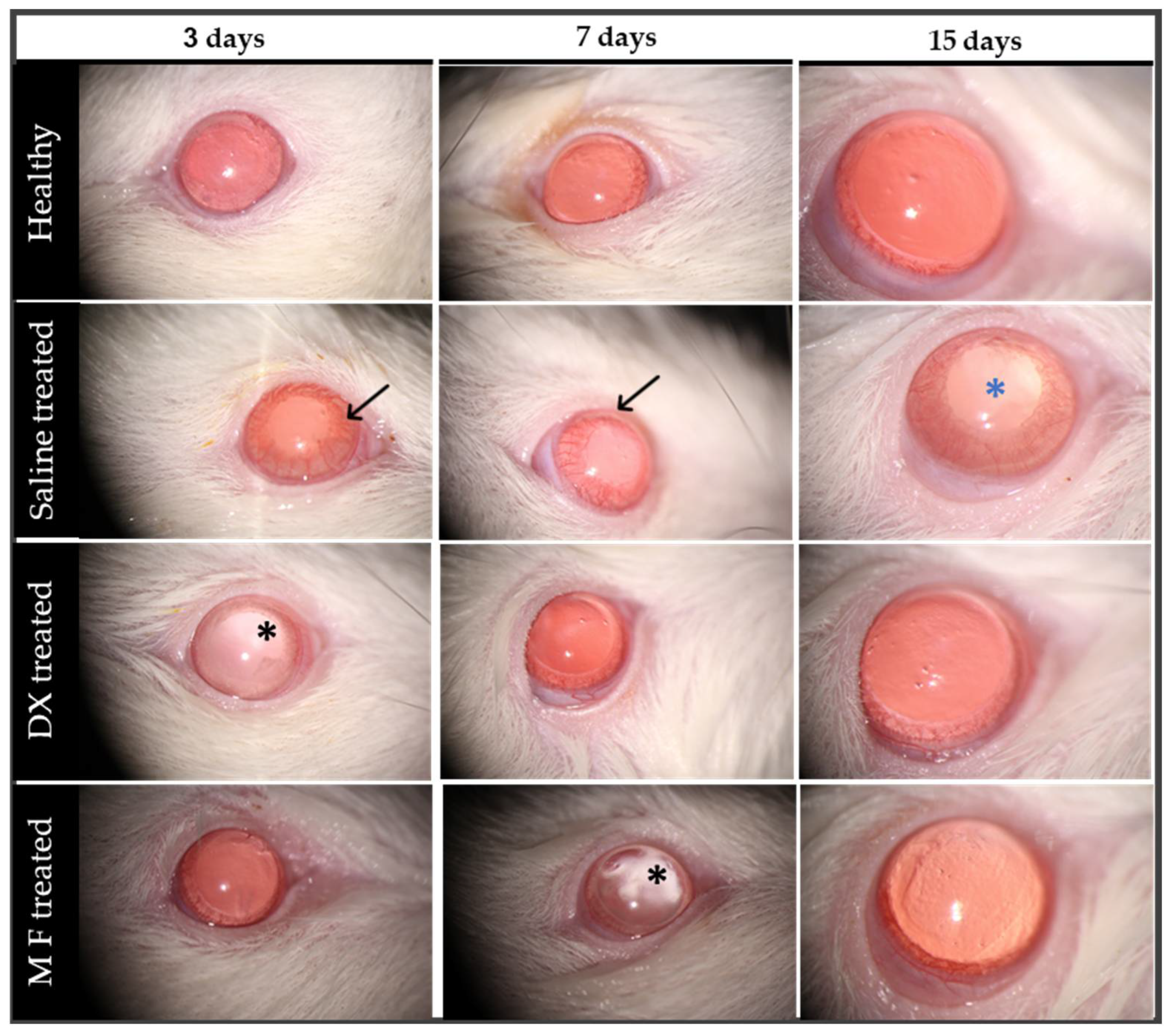
3.2. Treatment of BCG-Induced Uveitis with Intravitreal Mometasone
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tsirouki, T.; Dastiridou, A.; Symeonidis, C.; Tounakaki, O.; Brazitikou, I.; Kalogeropoulos, C.; Androudi, S. A Focus on the Epidemiology of Uveitis. Ocul. Immunol. Inflamm. 2018, 26, 2–16. [Google Scholar] [CrossRef]
- Da Silva, L.M.P.; Muccioli, C.; de Oliveira, F.; Arantes, T.E.; Gonzaga, L.R.; Nakanami, C. Visual Impairment from Uveitis in a Reference Hospital of Southeast Brazil: A Retrospective Review over a Twenty Years Period. Arq. Bras. Oftalmol. 2013, 76, 366–369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gamalero, L.; Simonini, G.; Ferrara, G.; Polizzi, S.; Giani, T.; Cimaz, R. Evidence-Based Treatment for Uveitis. Isr. Med. Assoc. J. 2019, 21, 475–479. [Google Scholar] [PubMed]
- Valdes, L.M.; Sobrin, L. Uveitis Therapy: The Corticosteroid Options. Drugs 2020, 80, 765–773. [Google Scholar] [CrossRef]
- Burkholder, B.M.; Jabs, D.A. Uveitis for the Non-Ophthalmologist. BMJ 2021, 372, m4979. [Google Scholar] [CrossRef]
- Conrady, C.D.; Yeh, S. A Review of Ocular Drug Delivery Platforms and Drugs for Infectious and Noninfectious Uveitis: The Past, Present, and Future. Pharmaceutics 2021, 13, 1224. [Google Scholar] [CrossRef] [PubMed]
- Onrust, S.V.; Lamb, H.M. A Review of Its Intranasal Use in Allergic Rhinitis. Adis Drug Eval. 1998, 56, 725–745. [Google Scholar]
- Baldwin, C.M.; Scott, L.J. Mometasone Furoate: A Review of Its Intranasal Use in Allergic Rhinitis. Drugs 2008, 68, 18. [Google Scholar] [CrossRef]
- Mcculloch, D.L.; Marmor, M.F.; Brigell, M.G.; Hamilton, R.; Holder, G.E.; Tzekov, R.; Bach, M.; Marmor, M.F.; Brigell, M.G.; Hamilton, R.; et al. ISCEV Standard for Full-Field Clinical Electroretinography (2015 Update). Doc. Ophthalmol. 2015, 130, 1–12. [Google Scholar] [CrossRef] [Green Version]
- De Paiva, M.R.B.; de Vasconcelos-Santos, D.V.; Coelho, M.M.; Machado, R.R.; Lopes, N.P.; Silva-Cunha, A.; Fialho, S.L. Licarin A as a Novel Drug for Inflammatory Eye Diseases. J. Ocul. Pharmacol. Ther. 2021, 37, 290–300. [Google Scholar] [CrossRef]
- Castro, B.F.M.; Vieira, L.C.; Vasconcelos-Santos, D.V.; Cenachi, S.P.d.F.; Cotta, O.A.L.; Guerra, M.C.A.; Paiva, M.R.B.; Silva, L.M.; Silva-Cunha, A.; Fialho, S.L. Intravitreal Thalidomide Ameliorates Inflammation in a Model of Experimental Uveitis Induced by BCG. Int. Immunopharmacol. 2020, 81, 106129. [Google Scholar] [CrossRef]
- Toledo, C.R.; Paiva, M.R.B.; Castro, B.F.M.; Pereira, V.V.; Cenachi, S.P.d.F.; Vasconcelos-Santos, D.V.; Fialho, S.L.; Silva-Cunha, A. Intravitreal Lupeol: A New Potential Therapeutic Strategy for Noninfectious Uveitis. Biomed. Pharmacother. 2021, 143, 112145. [Google Scholar] [CrossRef]
- Saliba, S.B.; Vieira, L.C.; Fernandes-Cunha, G.M.; Rodrigues, S.G.; Fialho, S.L.; Silva-Cunha, A.; Bousquet, E.; Naud, M.C.; Ayres, E.; Oréfice, R.L.; et al. Anti-Inflammatory Effect of Dexamethasone Controlled Released From Anterior Suprachoroidal Polyurethane Implants on Endotoxin-Induced Uveitis in Rats. Investig. Opthalmol. Vis. Sci. 2016, 57, 1671–1679. [Google Scholar] [CrossRef] [Green Version]
- Perlman, I. Testing Retinal Toxicity of Drugs in Animal Models Using Electrophysiological and Morphological Techniques. Doc. Ophthalmol. 2009, 118, 3–28. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.; Collette, W.; Twamley, M.; Aguirre, S.A.; Sacaan, A. Application of Electroretinography (ERG) in Early Drug Development for Assessing Retinal Toxicity in Rats. Toxicol. Appl. Pharmacol. 2015, 289, 525–533. [Google Scholar] [CrossRef] [PubMed]
- Paiva, M.R.B.; Arribada, R.G.; da Silva, C.N.; Ribeiro, M.C.S.; Jorge, R.; Fialho, S.L.; Silva-Cunha, A. Assessment of the Safety of Intravitreal Injection of Metoprolol Tartrate in Rabbits. Doc. Ophthalmol. 2020, 142, 75–85. [Google Scholar] [CrossRef] [PubMed]
- Paiva, M.R.B.; Vasconcelos-Santos, D.V.; Vieira, L.C.; Fialho, S.L.; Silva-Cunha, A. Sirolimus-Loaded Intravitreal Implant for Effective Treatment of Experimental Uveitis. AAPS PharmSciTech 2021, 22, 1–10. [Google Scholar] [CrossRef]
- Moreira Castro, B.F.; da Silva, C.N.; Barbosa Cordeiro, L.P.; Pereira de Freitas Cenachi, S.; Vasconcelos-Santos, D.V.; Machado, R.R.; Dias Heneine, L.G.; Silva, L.M.; Silva-Cunha, A.; Fialho, S.L. Low-Dose Melittin Is Safe for Intravitreal Administration and Ameliorates Inflammation in an Experimental Model of Uveitis. Curr. Res. Pharmacol. Drug Discov. 2022, 3, 100107. [Google Scholar] [CrossRef]
- Graff, G.; Gamache, D.A.; Brady, M.T.; Spellman, J.M.; Yanni, J.M. Improved Myeloperoxidase Assay for Quantitation of Neutrophil Influx in a Rat Model of Endotoxin-Induced Uveitis. J. Pharmacol. Toxicol. Methods 1998, 39, 169–178. [Google Scholar] [CrossRef]
- Mo, J.S.; Matsukawa, A.; Ohkawara, S.; Yoshinaga, M. Involvement of TNF α, IL-1β and IL-1 Receptor Antagonist in LPS-Induced Rabbit Uveitis. Exp. Eye Res. 1998, 66, 547–557. [Google Scholar] [CrossRef]
- Mérida, S.; Palacios, E.; Navea, A.; Bosch-Morell, F. New Immunosuppressive Therapies in Uveitis Treatment. Int. J. Mol. Sci. 2015, 16, 18778–18795. [Google Scholar] [CrossRef]
- Moschos, M.M.; Gouliopoulos, N.S.; Kalogeropoulos, C. Electrophysiological Examination in Uveitis: A Review of the Literature. Clin. Ophthalmol. 2014, 8, 199–214. [Google Scholar] [CrossRef] [Green Version]
- Noma, H.; Mimura, T.; Kuse, M.; Shimada, K. Association of Electroretinogram and Morphological Findings in Central Retinal Vein Occlusion with Macular Edema. Clin. Ophthalmol. 2014, 8, 191–197. [Google Scholar] [CrossRef] [Green Version]
- Brouwer, A.H.; van Genderen, M.M.; de Wit, G.C.; de Boer, J.H. Electroretinogram Abnormalities in Nonanterior Childhood Uveitis. Acta Ophthalmol. 2019, 97, 372–377. [Google Scholar] [CrossRef] [PubMed]
- Robson, A.G.; Nilsson, J.; Li, S.; Jalali Srimati Kanuri, S.; Fulton, A.B.; Tormene, A.P.; Holder, G.E.; Brodie, S.E. ISCEV Guide to Visual Electrodiagnostic Procedures. Doc. Ophthalmol. 2018, 136, 1–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brouwer, A.H.; de Wit, G.C.; ten Dam, N.H.; Wijnhoven, R.; van Genderen, M.M.; de Boer, J.H. Prolonged Cone B-Wave on Electroretinography Is Associated with Severity of Inflammation in Noninfectious Uveitis. Am. J. Ophthalmol. 2019, 207, 121–129. [Google Scholar] [CrossRef] [PubMed]







Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lage, N.A.; de Paiva, M.R.B.; Vasconcelos-Santos, D.V.; Machado, R.R.; Fialho, S.L.; Silva-Cunha, A. Efficacy and Safety Evaluation of Mometasone Furoate in Treating Ocular Inflammation. Pharmaceutics 2023, 15, 193. https://doi.org/10.3390/pharmaceutics15010193
Lage NA, de Paiva MRB, Vasconcelos-Santos DV, Machado RR, Fialho SL, Silva-Cunha A. Efficacy and Safety Evaluation of Mometasone Furoate in Treating Ocular Inflammation. Pharmaceutics. 2023; 15(1):193. https://doi.org/10.3390/pharmaceutics15010193
Chicago/Turabian StyleLage, Nayara Almeida, Mayara Rodrigues Brandão de Paiva, Daniel Vitor Vasconcelos-Santos, Renes Resende Machado, Sílvia Ligório Fialho, and Armando Silva-Cunha. 2023. "Efficacy and Safety Evaluation of Mometasone Furoate in Treating Ocular Inflammation" Pharmaceutics 15, no. 1: 193. https://doi.org/10.3390/pharmaceutics15010193