
The Impact of Low Cardiac Output on Propofol Pharmacokinetics across Age Groups—An Investigation Using Physiologically Based Pharmacokinetic Modelling


Abstract
:1. Introduction
2. Materials and Methods
2.1. Hepatic and Renal Extraction Ratio Determination across Age Groups
2.2. Impact of CO Reduction on Systemic Propofol Clearance across Age Groups
2.3. Impact of Reduced Cardiac Output on Attainment of Target Propofol Concentrations
2.4. Dose Reduction Exploration to Achieve Target Concentrations in Reduced Cardiac Output Conditions
3. Results
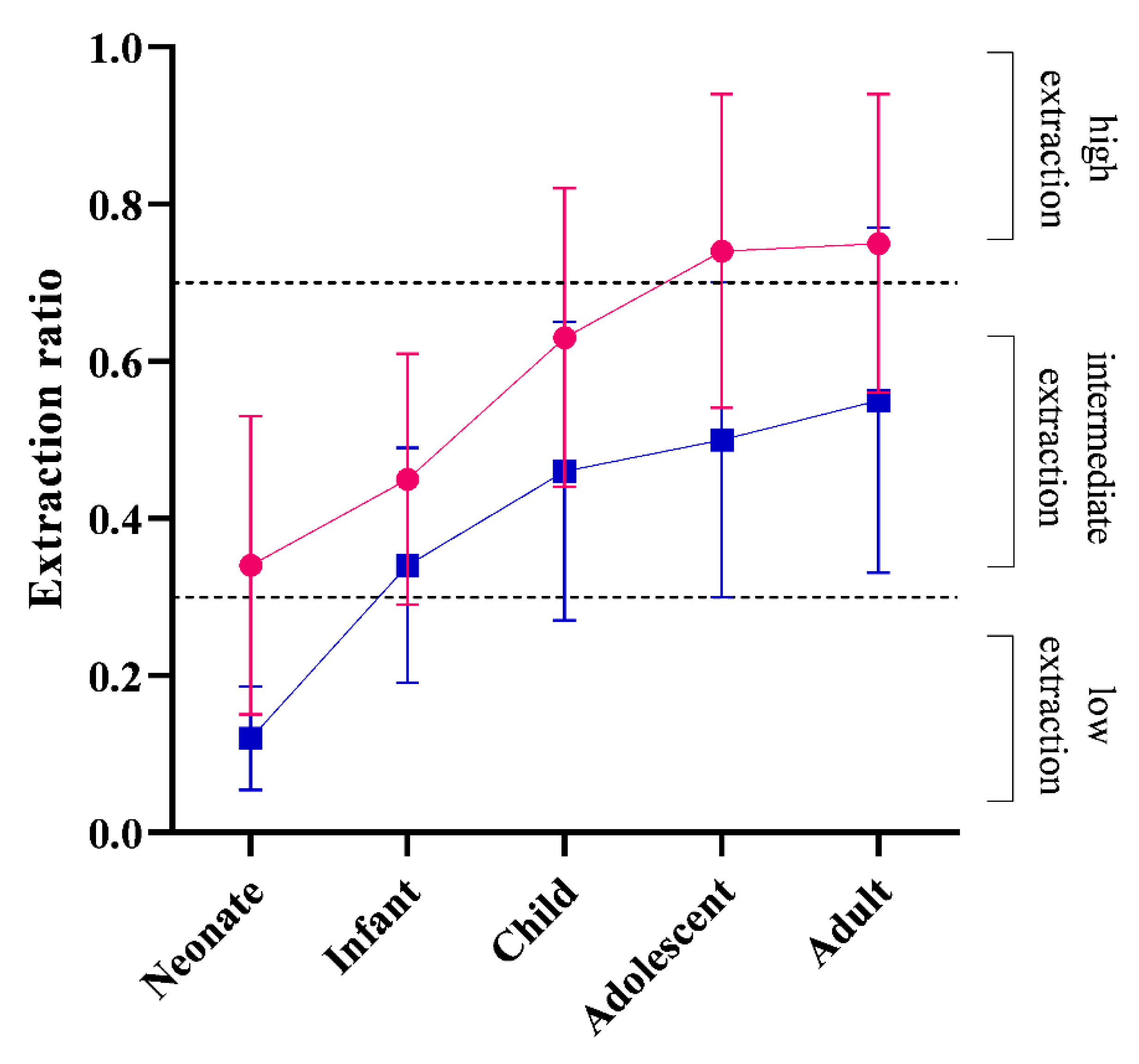
3.1. Hepatic and Renal Extraction Ratios across Age Groups
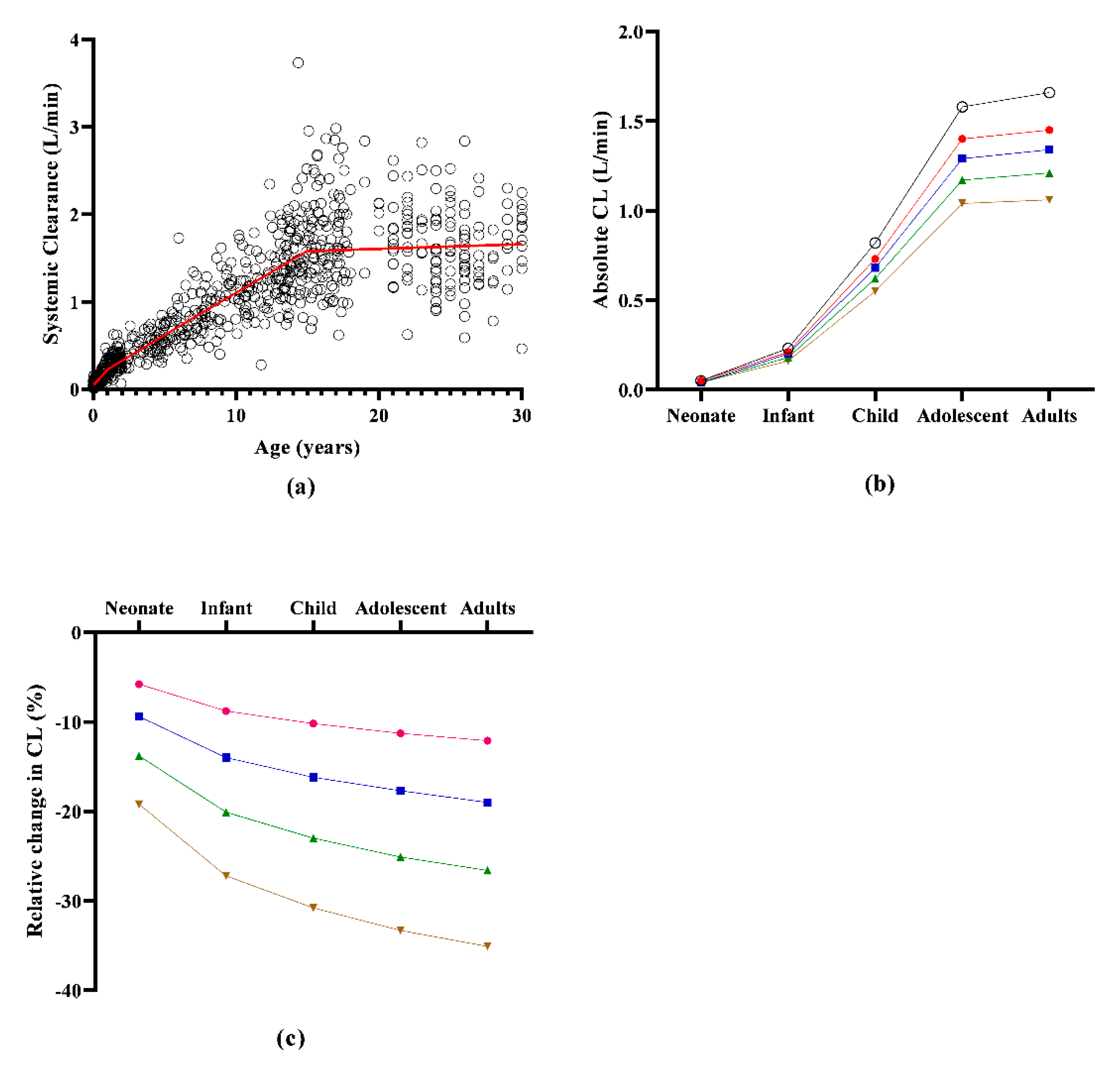
3.2. The Impact of Reduced Cardiac Output on Systemic Propofol Clearance across Age Groups
3.3. Impact of Reduced Cardiac Output on Attainment of Target Propofol Concentrations
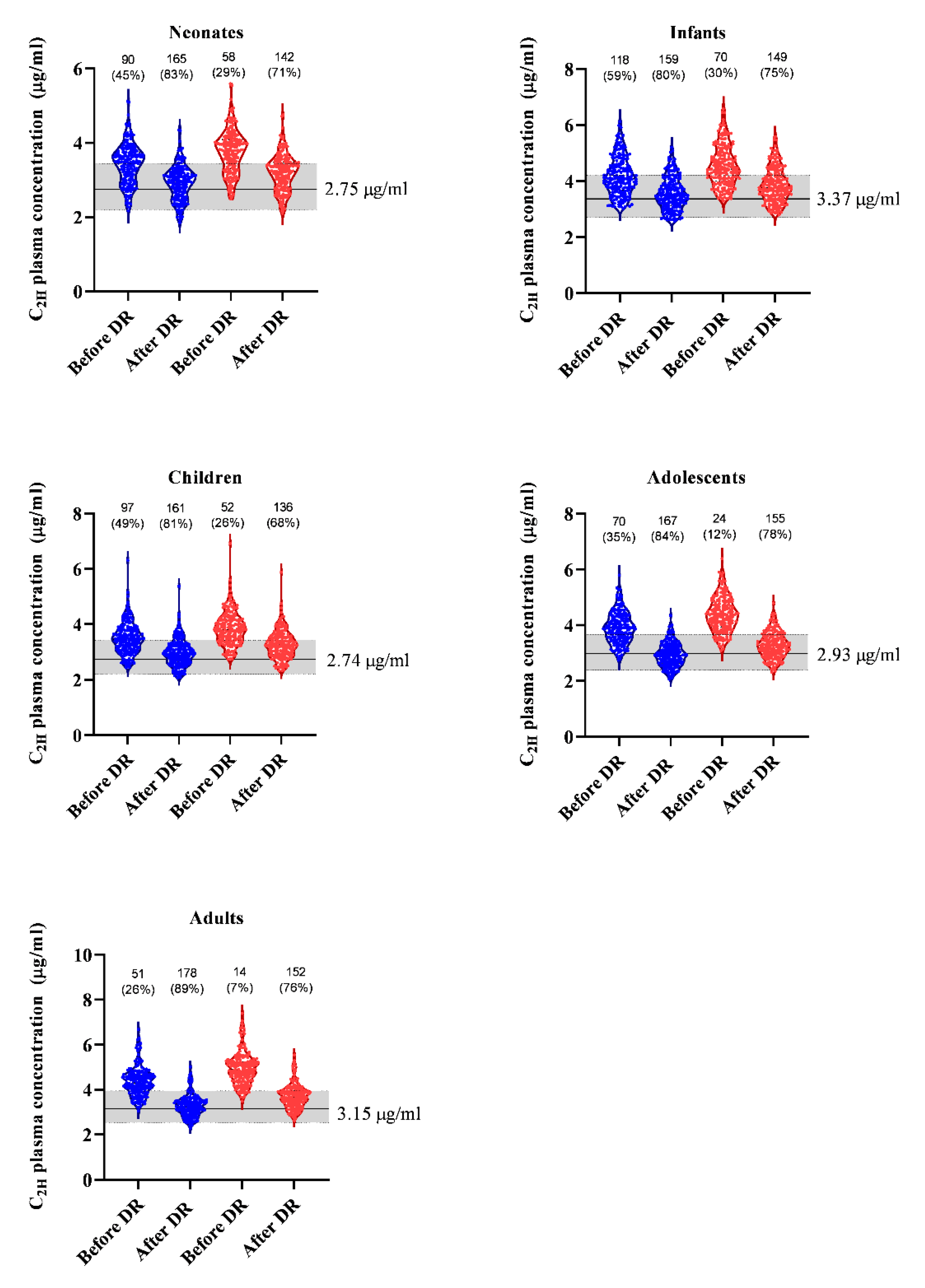
3.4. Dose Reduction Exploration to Achieve Target Concentrations in Reduced Cardiac Output Conditions
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Van den Anker, J.N.; Reed, M.D.; Allegaert, K.; Kearns, G.L. Developmental Changes in Pharmacokinetics and Pharmacodynamics. J. Clin. Pharmacol. 2018, 58, S10–S25. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Jiang, K.; Wei, X.; Li, Y.; Wang, T.; Song, Y. Physiologically Based Pharmacokinetic Models Are Effective Support for Pediatric Drug Development. AAPS PharmSciTech 2021, 22, 208. [Google Scholar] [CrossRef] [PubMed]
- Leslie, K.; Sessler, D.I.; Bjorksten, A.R.; Moayeri, A. Mild hypothermia alters propofol pharmacokinetics and increases the duration of action of atracurium. Anesth. Analg. 1995, 80, 1007–1014. [Google Scholar] [PubMed]
- Bjelland, T.W.; Klepstad, P.; Haugen, B.O.; Nilsen, T.; Dale, O. Effects of hypothermia on the disposition of morphine, midazolam, fentanyl, and propofol in intensive care unit patients. Drug Metab. Dispos. 2013, 41, 214–223. [Google Scholar] [CrossRef] [PubMed]
- Gebauer, C.M.; Knuepfer, M.; Robel-Tillig, E.; Pulzer, F.; Vogtmann, C. Hemodynamics among neonates with hypoxic-ischemic encephalopathy during whole-body hypothermia and passive rewarming. Pediatrics 2006, 117, 843–850. [Google Scholar] [CrossRef]
- Benowitz, N.L.; Meister, W. Pharmacokinetics in patients with cardiac failure. Clin. Pharmacokinet. 1976, 1, 389–405. [Google Scholar] [CrossRef]
- Rasool, M.F.; Khalil, F.; Läer, S. Predicting stereoselective disposition of carvedilol in adult and pediatric chronic heart failure patients by incorporating pathophysiological changes in organ blood flows—A physiologically based pharmacokinetic approach. Drug Metab. Dispos. 2016, 44, 1103–1115. [Google Scholar] [CrossRef]
- Hiraoka, H.; Yamamoto, K.; Miyoshi, S.; Morita, T.; Nakamura, K.; Kadoi, Y.; Kunimoto, F.; Horiuchi, R. Kidneys contribute to the extrahepatic clearance of propofol in humans, but not lungs and brain. Br. J. Clin. Pharmacol. 2005, 60, 176–482. [Google Scholar] [CrossRef]
- Xu, J.; Zhou, G.; Li, Y.; Li, N. Benefits of ultra-fast-track anesthesia for children with congenital heart disease undergoing cardiac surgery. BMC Pediatr. 2019, 19, 487. [Google Scholar] [CrossRef]
- Sahinovic, M.M.; Struys, M.; Absalom, A.R. Clinical Pharmacokinetics and Pharmacodynamics of Propofol. Clin. Pharmacokinet. 2018, 57, 1539–1558. [Google Scholar] [CrossRef] [Green Version]
- Simons, P.J.; Cockshott, I.D.; Douglas, E.J.; Gordon, E.A.; Hopkins, K.; Rowland, M. Disposition in male volunteers of a subanaesthetic intravenous dose of an oil in water emulsion of 14C-propofol. Xenobiotica 1988, 18, 429–440. [Google Scholar] [CrossRef] [PubMed]
- van Groen, B.D.; Nicolai, J.; Kuik, A.C.; Van Cruchten, S.; van Peer, E.; Smits, A.; Schmidt, S.; de Wildt, S.N.; Allegaert, K.; de Schaepdrijver, L.; et al. Ontogeny of Hepatic Transporters and Drug-Metabolizing Enzymes in Humans and in Nonclinical Species. Pharmacol. Rev. 2021, 73, 597–678. [Google Scholar] [CrossRef] [PubMed]
- Tateishi, T.; Nakura, H.; Asoh, M.; Watanabe, M.; Tanaka, M.; Kumai, T.; Takashima, S.; Imaoka, S.; Funae, Y.; Yabusaki, Y.; et al. A comparison of hepatic cytochrome P450 protein expression between infancy and postinfancy. Life Sci. 1997, 61, 2567–2574. [Google Scholar] [CrossRef]
- Bhatt, D.K.; Mehrotra, A.; Gaedigk, A.; Chapa, R.; Basit, A.; Zhang, H.; Choudhari, P.; Boberg, M.; Pearce, R.E.; Gaedigk, R.; et al. Age- and Genotype-Dependent Variability in the Protein Abundance and Activity of Six Major Uridine Diphosphate-Glucuronosyltransferases in Human Liver. Clin. Pharmacol. Ther. 2019, 105, 131–141. [Google Scholar] [CrossRef] [PubMed]
- Edginton, A.N.; Schmitt, W.; Willmann, S. Development and evaluation of a generic physiologically based pharmacokinetic model for children. Clin. Pharmacokinet. 2006, 45, 1013–1034. [Google Scholar] [CrossRef]
- Verscheijden, L.F.M.; Koenderink, J.B.; Johnson, T.N.; de Wildt, S.N.; Russel, F.G.M. Physiologically-based pharmacokinetic models for children: Starting to reach maturation? Pharmacol. Ther. 2020, 211, 107541. [Google Scholar] [CrossRef]
- Allegaert, K.; Abbasi, M.Y.; Annaert, P.; Olafuyi, O. Current and future physiologically based pharmacokinetic (PBPK) modeling approaches to optimize pharmacotherapy in preterm neonates. Expert Opin. Drug Metab. Toxicol. 2022, 18, 301–312. [Google Scholar] [CrossRef]
- Zakaria, Z.; Badhan, R.K.S. The impact of CYP2B6 polymorphisms on the interactions of efavirenz with lumefantrine: Implications for paediatric antimalarial therapy. Eur. J. Pharm. Sci. 2018, 119, 90–101. [Google Scholar] [CrossRef]
- Olafuyi, O.; Abbasi, M.Y.; Allegaert, K. Physiologically based pharmacokinetic modelling of acetaminophen in preterm neonates-The impact of metabolising enzyme ontogeny and reduced cardiac output. Biopharm. Drug Dispos. 2021, 42, 401–417. [Google Scholar] [CrossRef]
- Bienert, A.; Sobczynski, P.; Mlodawska, K.; Hartmann-Sobczynska, R.; Grzeskowiak, E.; Wiczling, P. The influence of cardiac output on propofol and fentanyl pharmacokinetics and pharmacodynamics in patients undergoing abdominal aortic surgery. J. Pharmacokinet. Pharmacodyn. 2020, 47, 583–596. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention, National Center for Health Statistics. National Health and Nutrition Examination Survey, National Center for Health Statistics. Available online: https://www.cdc.gov/nchs/nhanes/ (accessed on 4 August 2022).
- Michelet, R.; Van Bocxlaer, J.; Allegaert, K.; Vermeulen, A. The use of PBPK modeling across the pediatric age range using propofol as a case. J. Pharmacokinet. Pharmacodyn. 2018, 45, 765–785. [Google Scholar] [CrossRef]
- Rohatgi, A.; Stanojevic, Z. WebPlotDigitizer: Version 3.10 of WebPlotDigitizer. Available online: https://apps.automeris.io/wpd/ (accessed on 4 August 2022).
- Ginsberg, G.; Hattis, D.; Russ, A.; Sonawane, B. Physiologically based pharmacokinetic (PBPK) modeling of caffeine and theophylline in neonates and adults: Implications for assessing children’s risks from environmental agents. J. Toxicol. Environ. Health A 2004, 67, 297–329. [Google Scholar] [CrossRef] [PubMed]
- Parrott, N.; Davies, B.; Hoffmann, G.; Koerner, A.; Lave, T.; Prinssen, E.; Theogaraj, E.; Singer, T. Development of a Physiologically Based Model for Oseltamivir and Simulation of Pharmacokinetics in Neonates and Infants. Clin. Pharmacokinet. 2011, 50, 613–623. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services. Administration UFaD. 2012 Meeting Materials, Pharmaceutical Science and Clinical Pharmacology Advisory Committee. Available online: https://wayback.archive-it.org/7993/20170403224110/https://www.fda.gov/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/AdvisoryCommitteeforPharmaceuticalScienceandClinicalPharmacology/ucm286697.htm (accessed on 4 August 2022).
- Struys, M.M.; Coppens, M.J.; De Neve, N.; Mortier, E.P.; Doufas, A.G.; Van Bocxlaer, J.F.; Shafer, S.L. Influence of administration rate on propofol plasma-effect site equilibration. Anesthesiology 2007, 107, 386–396. [Google Scholar] [CrossRef] [PubMed]
- Schnider, T.W.; Minto, C.F.; Gambus, P.L.; Andresen, C.; Goodale, D.B.; Shafer, S.L.; Youngs, E.J. The influence of method of administration and covariates on the pharmacokinetics of propofol in adult volunteers. Anesthesiology 1998, 88, 1170–1182. [Google Scholar] [CrossRef] [PubMed]
- Levitt, D.G.; Schnider, T.W. Human physiologically based pharmacokinetic model for propofol. BMC Anesthesiol. 2005, 5, 4. [Google Scholar] [CrossRef] [PubMed]
- Gepts, E.; Camu, F.; Cockshott, I.D.; Douglas, E.J. Disposition of propofol administered as constant rate intravenous infusions in humans. Anesth. Analg. 1987, 66, 1256–1263. [Google Scholar] [CrossRef]
- Doufas, A.G.; Orhan-Sungur, M.; Komatsu, R.; Lauber, R.; Akca, O.; Shafer, S.L.; Sessler, D.I. Bispectral index dynamics during propofol hypnosis is similar in red-haired and dark-haired subjects. Anesth. Analg. 2013, 116, 319–326. [Google Scholar] [CrossRef]
- Jones, R.D.; Chan, K.; Andrew, L.J. Pharmacokinetics of propofol in children. Br. J. Anaesth. 1990, 65, 661–667. [Google Scholar] [CrossRef]
- Murat, I.; Billard, V.; Vernois, J.; Zaouter, M.; Marsol, P.; Souron, R.; Farinotti, R. Pharmacokinetics of propofol after a single dose in children aged 1-3 years with minor burns. Comparison of three data analysis approaches. Anesthesiology 1996, 84, 526–532. [Google Scholar] [CrossRef]
- Saint-Maurice, C.; Cockshott, I.D.; Douglas, E.J.; Richard, M.O.; Harmey, J.L. Pharmacokinetics of propofol in young children after a single dose. Br. J. Anaesth. 1989, 63, 667–670. [Google Scholar] [CrossRef] [PubMed]
- Sepulveda, P.; Cortinez, L.I.; Saez, C.; Penna, A.; Solari, S.; Guerra, I.; Absalom, G.A.R. Performance evaluation of paediatric propofol pharmacokinetic models in healthy young children. Br. J. Anaesth. 2011, 107, 593–600. [Google Scholar] [CrossRef] [PubMed]
- Raoof, A.A.; van Obbergh, L.J.; Verbeeck, R.K. Propofol pharmacokinetics in children with biliary atresia. Br. J. Anaesth. 1995, 74, 46–49. [Google Scholar] [CrossRef]
- Allegaert, K.; de Hoon, J.; Verbesselt, R.; Naulaers, G.; Murat, I. Maturational pharmacokinetics of single intravenous bolus of propofol. Paediatr. Anaesth. 2007, 17, 1028–1034. [Google Scholar] [CrossRef] [PubMed]
- Allegaert, K.; Peeters, M.Y.; Verbesselt, R.; Tibboel, D.; Naulaers, G.; de Hoon, J.N.; Knibbe, C.A. Inter-individual variability in propofol pharmacokinetics in preterm and term neonates. Br. J. Anaesth. 2007, 99, 864–870. [Google Scholar] [CrossRef] [PubMed]
- Morse, J.; Hannam, J.A.; Cortinez, L.I.; Allegaert, K.; Anderson, B.J. A manual propofol infusion regimen for neonates and infants. Paediatr. Anaesth. 2019, 29, 907–914. [Google Scholar] [CrossRef]
- Roberts, F.L.; Dixon, J.; Lewis, G.T.; Tackley, R.M.; Prys-Roberts, C. Induction and maintenance of propofol anaesthesia. A manual infusion scheme. Anaesthesia 1988, 43, 14–17. [Google Scholar] [CrossRef]
- Wiczling, P.; Bieda, K.; Przybylowski, K.; Hartmann-Sobczynska, R.; Borsuk, A.; Matysiak, J.; Kokot, Z.J.; Sobczynski, P.; Greskowiak, E.; Biener, A. Pharmacokinetics and pharmacodynamics of propofol and fentanyl in patients undergoing abdominal aortic surgery—A study of pharmacodynamic drug-drug interactions. Biopharm. Drug Dispos. 2016, 37, 252–263. [Google Scholar] [CrossRef]
- Wiczling, P.; Bienert, A.; Sobczynski, P.; Hartmann-Sobczynska, R.; Bieda, K.; Marcinkowska, A.; Malatynska, M.; Kaliszan, R.; Grzeskowiak, E. Pharmacokinetics and pharmacodynamics of propofol in patients undergoing abdominal aortic surgery. Pharmacol. Rep. 2012, 64, 113–122. [Google Scholar] [CrossRef]
- Eipel, C.; Abshagen, K.; Vollmar, B. Regulation of hepatic blood flow: The hepatic arterial buffer response revisited. World J. Gastroenterol. 2010, 16, 6046–6057. [Google Scholar] [CrossRef]
- Salem, F.; Abduljalil, K.; Kamiyama, Y.; Rostami-Hodjegan, A. Considering Age Variation When Coining Drugs as High versus Low Hepatic Extraction Ratio. Drug Metab. Dispos. 2016, 44, 1099–1102. [Google Scholar] [CrossRef] [PubMed]
- Takizawa, D.; Sato, E.; Ito, N.; Ogino, Y.; Hiraoka, H.; Goto, F.; Cavaliere, F.; Conti, G.; Moscato, U.; Meo, F.; et al. Hypoalbuminaemia and propofol pharmacokinetics. Br. J. Anaesth. 2005, 95, 559. [Google Scholar] [CrossRef] [PubMed]
- Eleveld, D.J.; Colin, P.; Absalom, A.R.; Struys, M. Pharmacokinetic-pharmacodynamic model for propofol for broad application in anaesthesia and sedation. Br. J. Anaesth. 2018, 120, 942–959. [Google Scholar] [CrossRef]
- McFarlan, C.S.; Anderson, B.J.; Short, T.G. The use of propofol infusions in paediatric anaesthesia: A practical guide. Paediatr. Anaesth. 1999, 9, 209–216. [Google Scholar] [CrossRef]
- Sehgal, A.; Wong, F.; Mehta, S. Reduced cardiac output and its correlation with coronary blood flow and troponin in asphyxiated infants treated with therapeutic hypothermia. Eur. J. Pediatr. 2012, 171, 1511–1577. [Google Scholar] [CrossRef]
- Peeters, M.Y.; Allegaert, K.; Blusse van Oud-Alblas, H.J.; Cella, M.; Tibboel, D.; Danhof, M.; Knibbe, C.A.J. Prediction of propofol clearance in children from an allometric model developed in rats, children and adults versus a 0.75 fixed-exponent allometric model. Clin. Pharmacokinet. 2010, 49, 269–275. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cardiac Output | Neonates | Infants | Children | Adolescents | Adults | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Absolute (L/min) | Relative (%) | Absolute (L/min) | Relative (%) | Absolute (L/min) | Relative (%) | Absolute (L/min) | Relative (%) | Absolute (L/min) | Relative (%) | |
| Normal CO | 0.05 (0.02) | 0.23 (0.11) | 0.82 (0.35) | 1.58 (0.50) | 1.66 (0.45) | |||||
| 20% ↓CO | 0.05 (0.02) | −5.8 (2.3) | 0.21 (0.10) | −8.8 (2.4) | 0.73 (0.30) | −10.2 (2.2) | 1.40 (0.41) | −11.3 (2.2) | 1.45 (0.36) | −12.1 (2.3) |
| 30% ↓CO | 0.04 (0.018) | −9.4 (3.6) | 0.20 (0.09) | −14.0 (3.7) | 0.68 (0.27) | −16.2 (3.3) | 1.29 (0.37) | −17.7 (3.3) | 1.34 (0.32) | −19.0 (3.3) |
| 40% ↓CO | 0.04 (0.016) | −13.8 (5.0) | 0.18 (0.18) | −20.1 (4.9) | 0.62 (0.24) | −23.0 (4.3) | 1.17 (0.32) | −25.1 (4.2) | 1.21 (0.28) | −26.6 (4.3) |
| 50% ↓CO | 0.04 (0.014) | −19.2 (6.4) | 0.16 (0.07) | −27.2 (6.1) | 0.55 (0.21) | −30.8 (5.3) | 1.04 (0.27) | −33.3 (5.0) | 1.061 (0.23) | −35.1 (5.1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Allegaert, K.; Abbasi, M.Y.; Michelet, R.; Olafuyi, O. The Impact of Low Cardiac Output on Propofol Pharmacokinetics across Age Groups—An Investigation Using Physiologically Based Pharmacokinetic Modelling. Pharmaceutics 2022, 14, 1957. https://doi.org/10.3390/pharmaceutics14091957
Allegaert K, Abbasi MY, Michelet R, Olafuyi O. The Impact of Low Cardiac Output on Propofol Pharmacokinetics across Age Groups—An Investigation Using Physiologically Based Pharmacokinetic Modelling. Pharmaceutics. 2022; 14(9):1957. https://doi.org/10.3390/pharmaceutics14091957
Chicago/Turabian StyleAllegaert, Karel, Mohammad Yaseen Abbasi, Robin Michelet, and Olusola Olafuyi. 2022. "The Impact of Low Cardiac Output on Propofol Pharmacokinetics across Age Groups—An Investigation Using Physiologically Based Pharmacokinetic Modelling" Pharmaceutics 14, no. 9: 1957. https://doi.org/10.3390/pharmaceutics14091957