
Design, Development, and Testing of a Device for Gene Electrotransfer to Skin Cells In Vivo
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
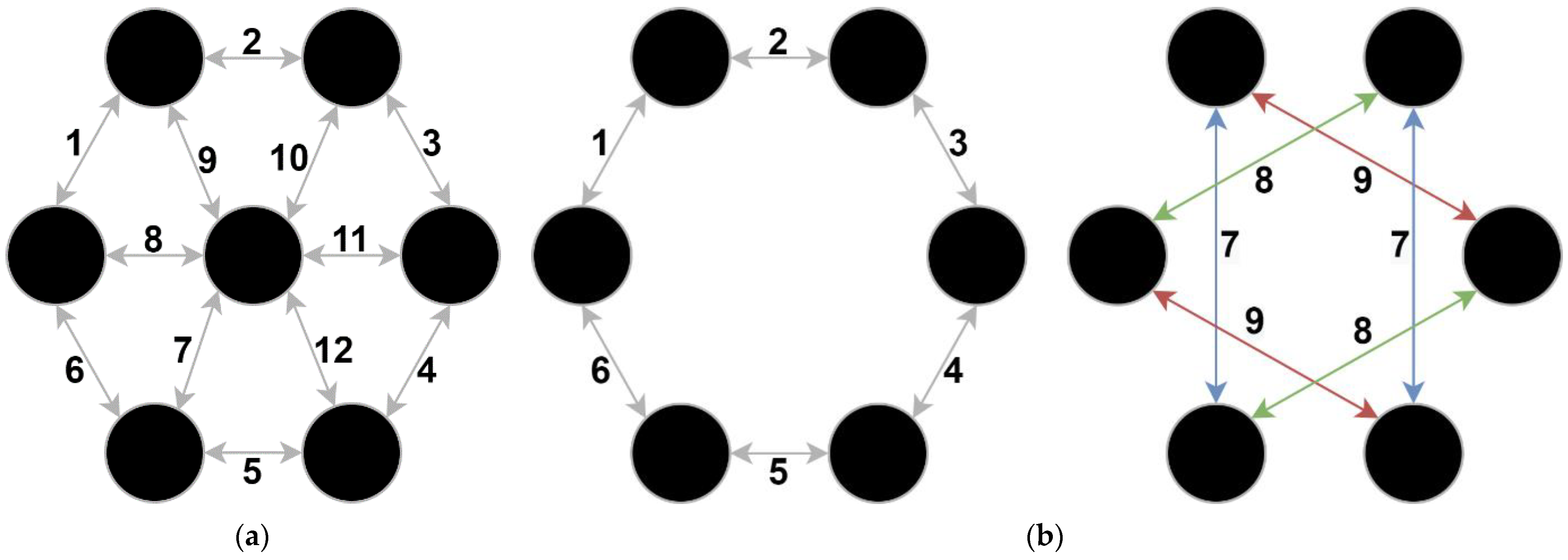
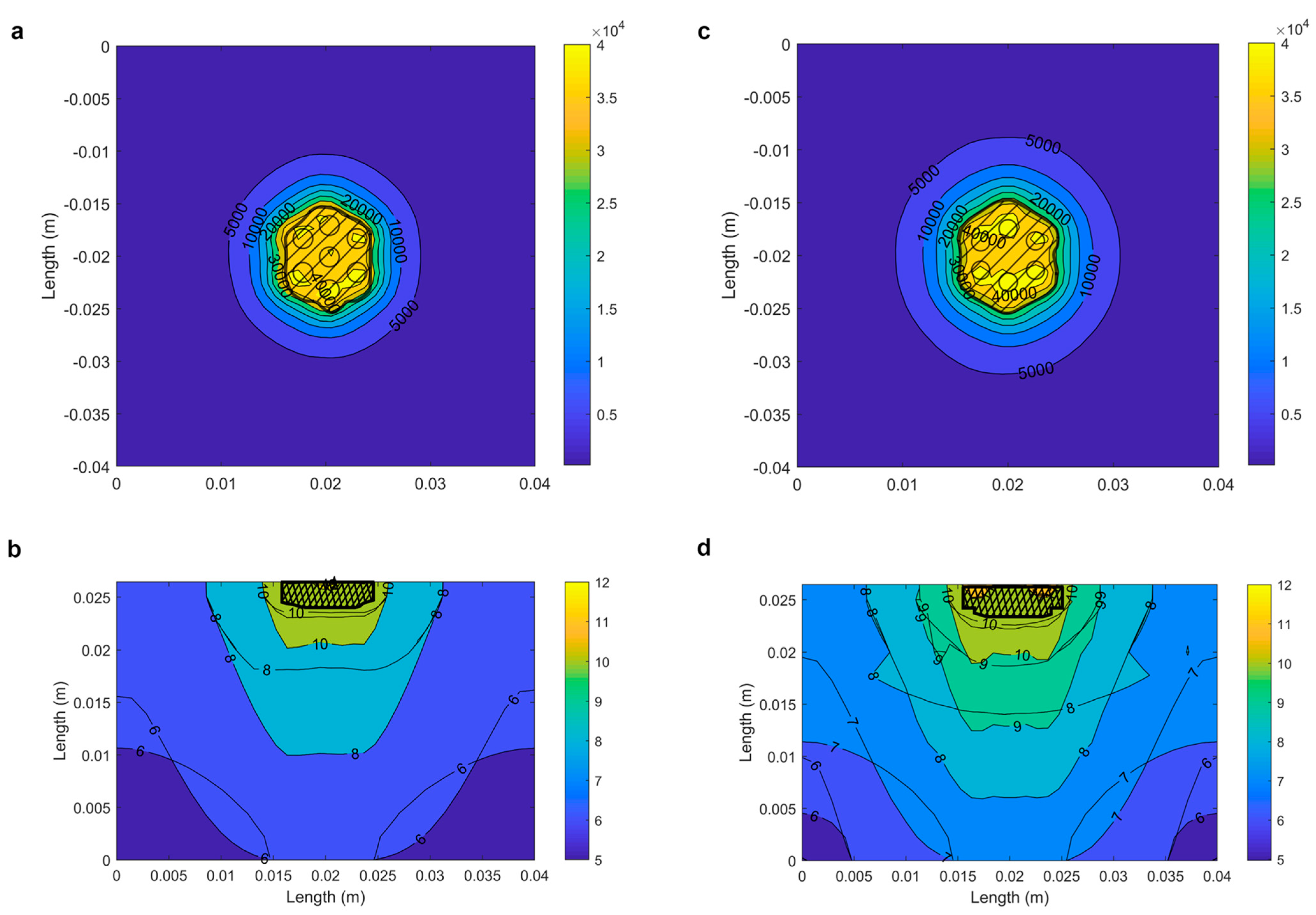
2.1. Numerical Determination of the Optimal Electrode Configuration
- Minimizing collateral damage by minimizing the volume of irreversible electroporation.
- Maximizing gene transfer efficiency by maximizing the reversibly electroporated volume.
2.2. Requirements and Recommendations to Be Considered When Designing a Clinical Electroporator for Gene Electrotransfer to Skin Cells
2.2.1. Medical Device Regulation and Standards
2.2.2. User and Technical Recommendations
2.2.3. Recommended Treatment Protocol for Safe and Efficient Gene Electrotransfer to Skin Cells
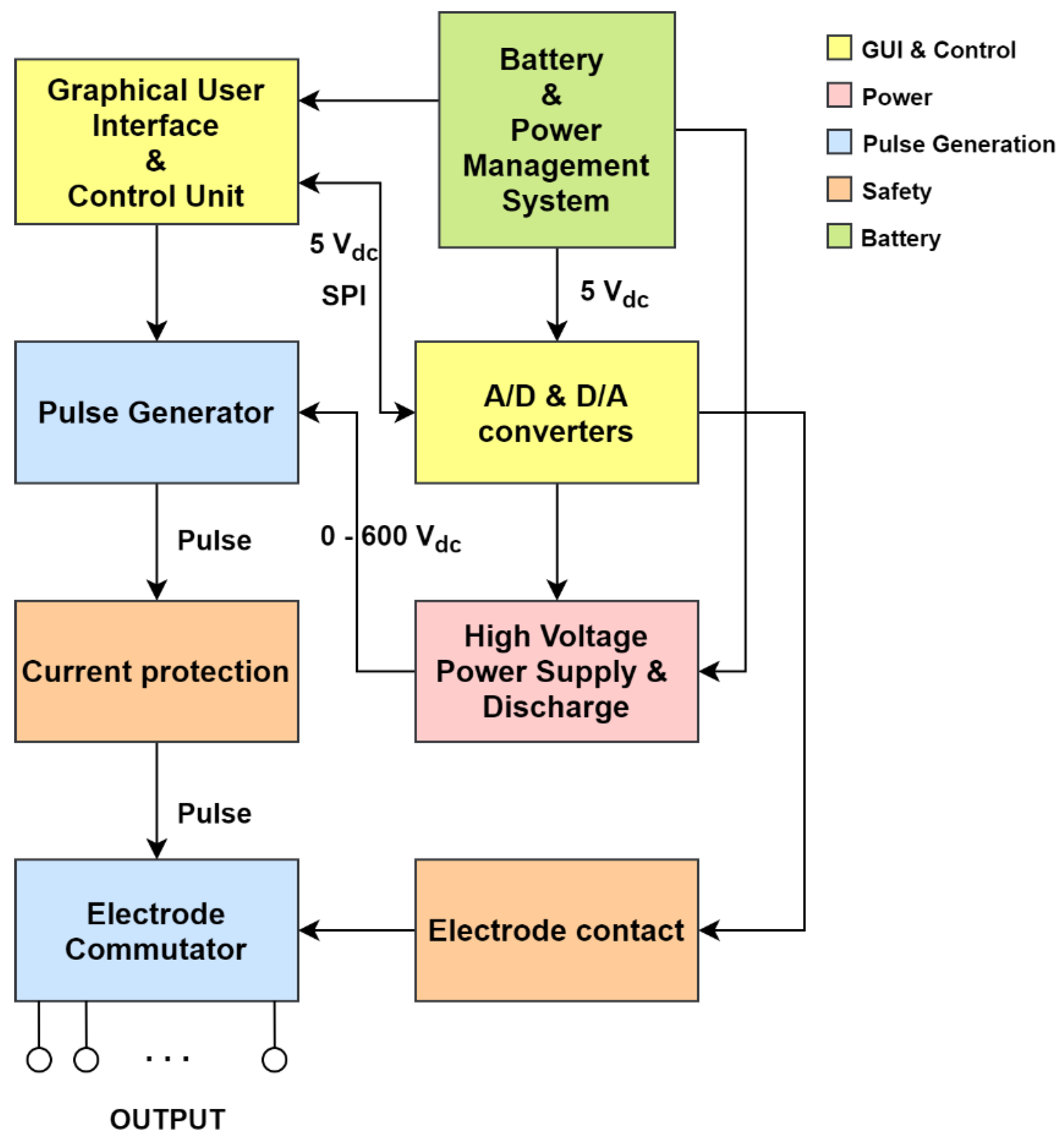
2.3. System Design
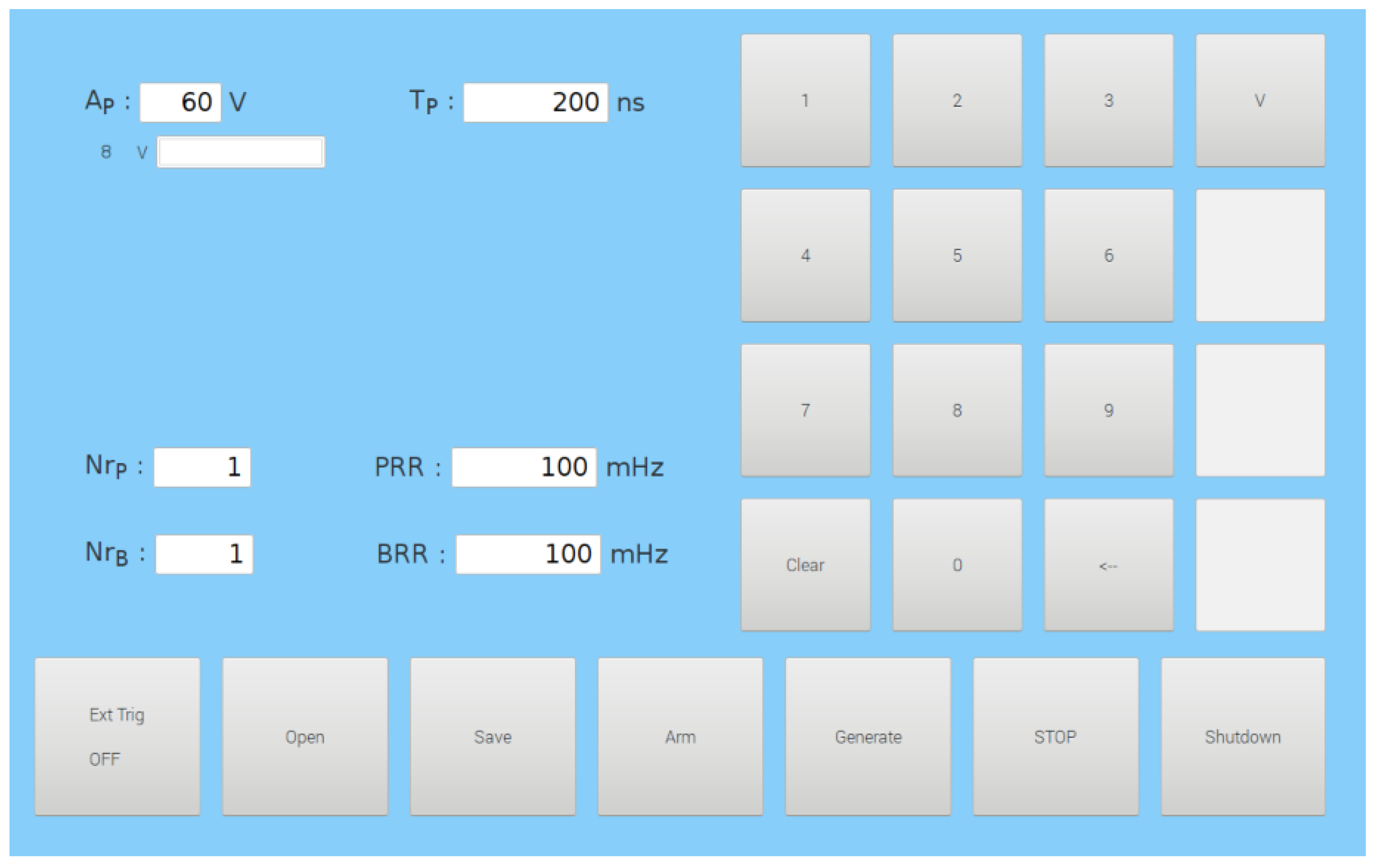
2.3.1. Graphical User Interface (GUI) and Control Unit
2.3.2. Power
2.3.3. Pulse Generation
2.3.4. Safety
2.3.5. Battery
2.4. In Vivo Experiments
2.4.1. Plasmid DNA
2.4.2. Mice
2.4.3. In Vivo Gene Electrotransfer
2.4.4. Image Acquisition and Analysis
3. Results
3.1. Numerical Determination of the Optimal Electrode Configuration
3.2. System Design
3.2.1. Applicator—Electrode Development
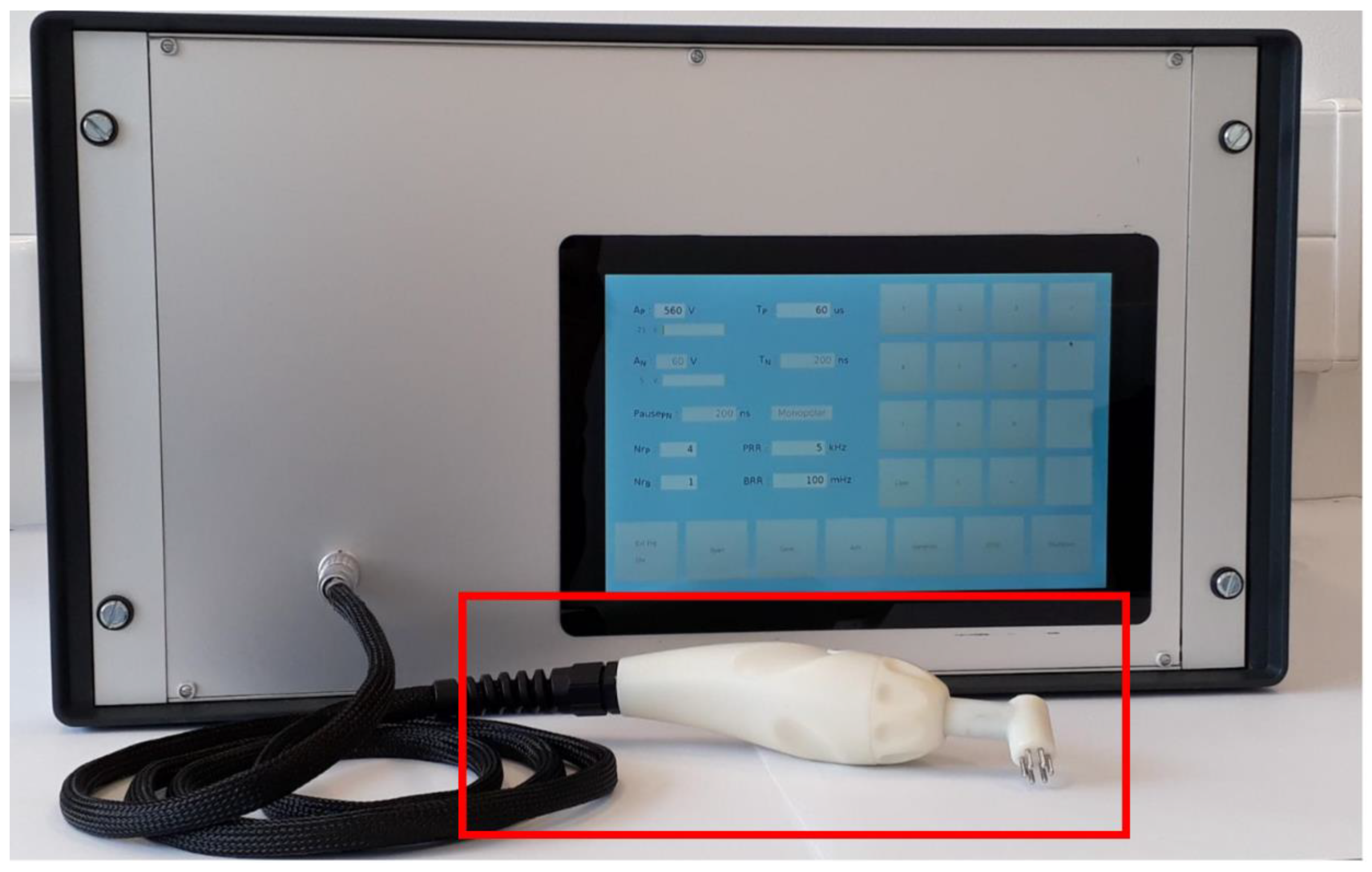
3.2.2. Device Development
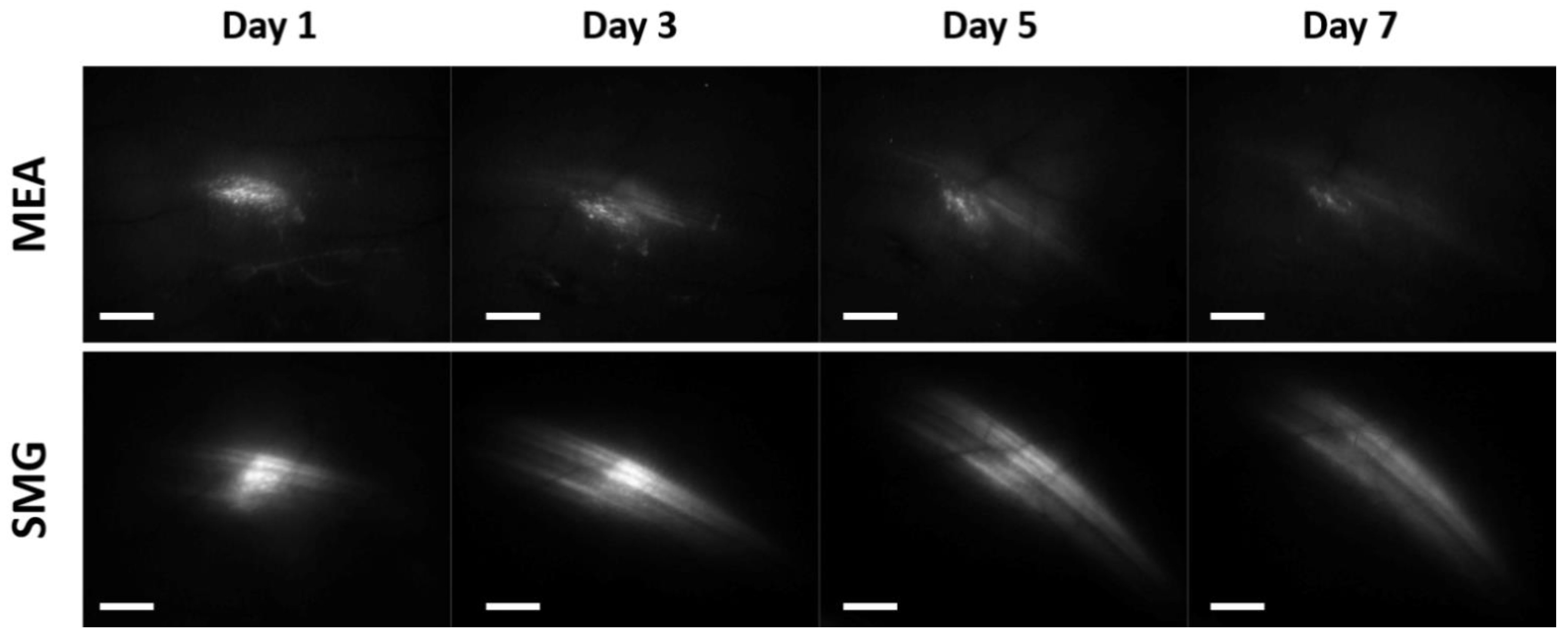
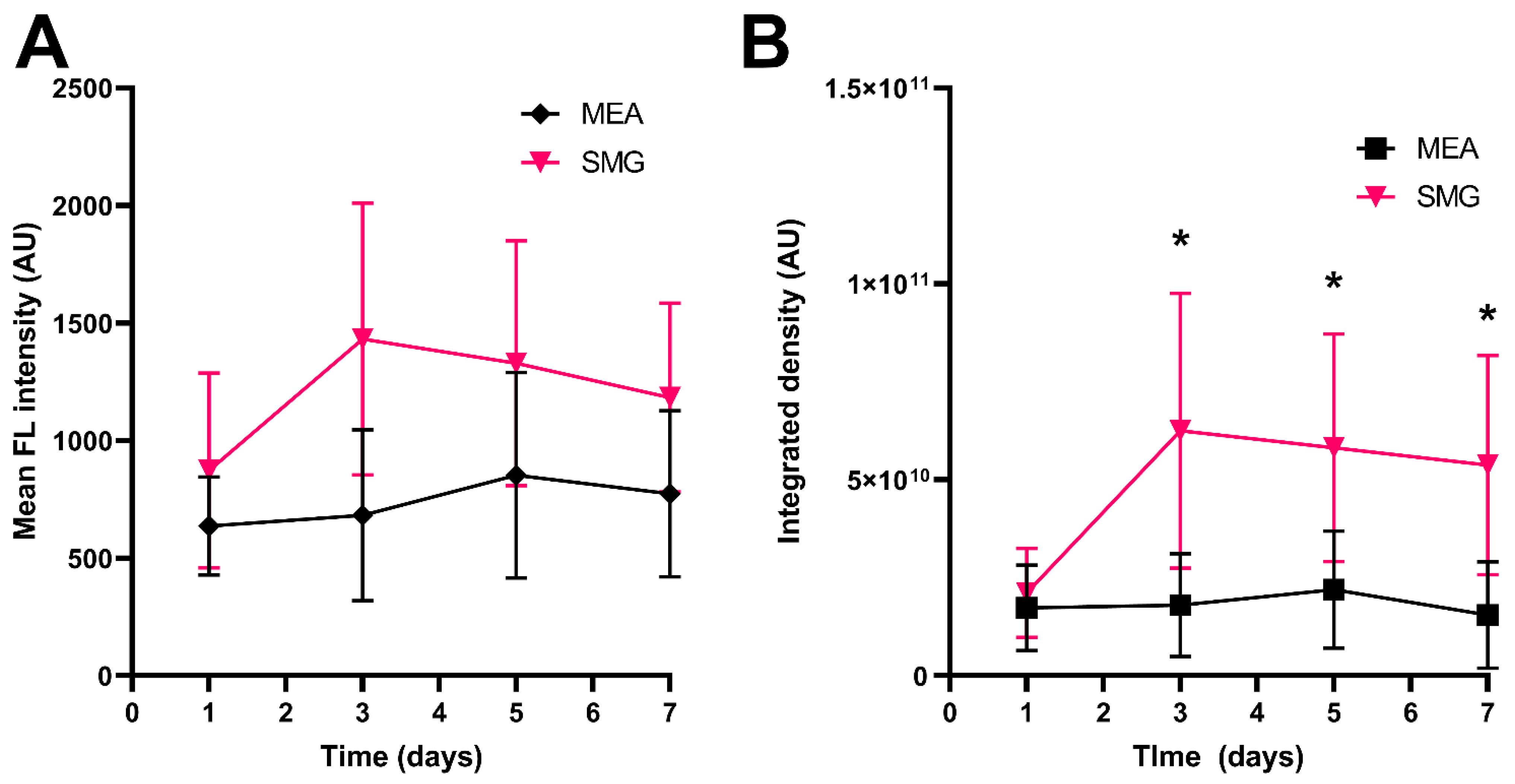
3.3. In Vivo Experiments
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kaestner, L.; Scholz, A.; Lipp, P. Bioorganic & Medicinal Chemistry Letters Conceptual and Technical Aspects of Transfection and Gene Delivery. Bioorg. Med. Chem. Lett. 2015, 25, 1171–1176. [Google Scholar] [CrossRef] [PubMed]
- Greco, O.; Scott, S.D.; Marples, B.; Dachs, G.U. Cancer Gene Therapy: ‘Delivery, Delivery, Delivery’. Front. Biosci. 2002, 7, d1516-24. [Google Scholar] [CrossRef] [PubMed]
- Bono, N.; Ponti, F.; Mantovani, D.; Candiani, G. Non-Viral in Vitro Gene Delivery: It Is Now Time to Set the Bar! Pharmaceutics 2020, 12, 183. [Google Scholar] [CrossRef]
- Sachdev, S.; Potočnik, T.; Rems, L.; Miklavčič, D. Revisiting the Role of Pulsed Electric Fields in Overcoming the Barriers to in Vivo Gene Electrotransfer. Bioelectrochemistry 2022, 144, 107994. [Google Scholar] [CrossRef]
- Kotnik, T.; Rems, L.; Tarek, M.; Miklavcic, D. Membrane Electroporation and Electropermeabilization: Mechanisms and Models. Annu. Rev. Biophys. 2019, 48, 63–91. [Google Scholar] [CrossRef]
- Yarmush, M.L.; Golberg, A.; Serša, G.; Kotnik, T.; Miklavčič, D. Electroporation-Based Technologies for Medicine: Principles, Applications, and Challenges. Annu. Rev. Biomed. Eng. 2014, 16, 295–320. [Google Scholar] [CrossRef]
- Rosazza, C.; Haberl Meglic, S.; Zumbusch, A.; Rols, M.-P.; Miklavcic, D. Gene Electrotransfer: A Mechanistic Perspective. Curr. Gene Ther. 2016, 16, 98–129. [Google Scholar] [CrossRef]
- Young, J.L.; Dean, D.A. Electroporation-Mediated Gene Delivery. In Advances in Genetics; Elsevier: Amsterdam, The Netherlands, 2015; Volume 89, pp. 49–88. [Google Scholar]
- Rebersek, M.; Miklavcic, D. Concepts of Electroporation Pulse Generation and Overview of Electric Pulse Generators for Cell and Tissue Electroporation. In Advanced Electroporation Techniques in Biology and Medicine; Pakhomov, A.G., Miklavcic, D., Markov, M.S., Eds.; CRC: Boca Raton, FL, USA, 2010; pp. 323–339. [Google Scholar]
- Reberšek, M. Beyond Electroporation Pulse Parameters: From Application to Evaluation. In Handbook of Electroporation; Miklavcic, D., Ed.; Springer International Publishing: Cham, Switzerland, 2017; pp. 1–21. ISBN 978-3-319-26779-1. [Google Scholar]
- Heller, R.; Schultz, J.; Lucas, M.L.; Jaroszeski, M.J.; Heller, L.C.; Gilbert, R.A.; Moelling, K.; Nicolau, C. Intradermal Delivery of Interleukin-12 Plasmid DNA by in Vivo Electroporation. DNA Cell Biol. 2001, 20, 21–26. [Google Scholar] [CrossRef]
- Lambricht, L.; Lopes, A.; Kos, S.; Sersa, G.; Préat, V.; Vandermeulen, G. Clinical Potential of Electroporation for Gene Therapy and DNA Vaccine Delivery. Expert Opin. Drug Deliv. 2016, 13, 295–310. [Google Scholar] [CrossRef]
- Schoellhammer, C.M.; Blankschtein, D.; Langer, R. Skin Permeabilization for Transdermal Drug Delivery: Recent Advances and Future Prospects. Expert Opin. Drug Deliv. 2014, 11, 393–407. [Google Scholar] [CrossRef] [Green Version]
- Gothelf, A.; Gehl, J. Gene Electrotransfer to Skin; Review of Existing Literature and Clinical Perspectives. Curr. Gene Ther. 2010, 10, 287–299. [Google Scholar] [CrossRef] [PubMed]
- Dermol-Černe, J.; Pirc, E.; Miklavčič, D. Mechanistic View of Skin Electroporation—Models and Dosimetry for Successful Applications: An Expert Review. Expert Opin. Drug Deliv. 2020, 17, 689–704. [Google Scholar] [CrossRef] [PubMed]
- Pirc, E.; Reberšek, M.; Miklavčič, D. Dosimetry in Electroporation-Based Technologies and Treatments. In Dosimetry in Bioelectromagnetics; Markov, M., Ed.; CRC Press: Boca Raton, FL, USA, 2017; pp. 233–268. ISBN 978-1-315-15457-2. [Google Scholar]
- Dermol-Černe, J.; Miklavčič, D. From Cell to Tissue Properties-Modeling Skin Electroporation With Pore and Local Transport Region Formation. IEEE Trans. Biomed. Eng. 2018, 65, 458–468. [Google Scholar] [CrossRef]
- Huclova, S.; Fröhlich, J.; Falco, L.; Dewarrat, F.; Talary, M.S.; Vahldieck, R. Validation of Human Skin Models in the MHz Region. In Proceedings of the 2009 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Minneapolis, MN, USA, 3–6 September 2009; pp. 4461–4464. [Google Scholar]
- Corovic, S.; Lackovic, I.; Sustaric, P.; Sustar, T.; Rodic, T.; Miklavcic, D. Modeling of Electric Field Distribution in Tissues during Electroporation. Biomed. Eng. Online 2013, 12, 16. [Google Scholar] [CrossRef] [PubMed]
- Pavšelj, N.; Bregar, Z.; Cukjati, D.; Batiuskaite, D.; Mir, L.M.; Miklavčič, D. The Course of Tissue Permeabilization Studied on a Mathematical Model of a Subcutaneous Tumor in Small Animals. IEEE Trans. Biomed. Eng. 2005, 52, 1373–1381. [Google Scholar] [CrossRef]
- Kos, S.; Vanvarenberg, K.; Dolinsek, T.; Cemazar, M.; Jelenc, J.; Préat, V.; Sersa, G.; Vandermeulen, G. Gene Electrotransfer into Skin Using Noninvasive Multi-Electrode Array for Vaccination and Wound Healing. Bioelectrochemistry 2017, 114, 33–41. [Google Scholar] [CrossRef]
- Gilbert, R.A.; Jaroszeski, M.J.; Heller, R. Novel Electrode Designs for Electrochemotherapy. Biochim. Biophys. Acta-Gen. Subj. 1997, 1334, 9–14. [Google Scholar]
- Zhang, L.; Finnefrock, A.C.; Casimiro, D.R.; Rabussay, D. DNA Vaccination Using the Medpulser DNA Delivery System in Rhesus Macaques: Development of Clinical Electroporation Parameters. Mol. Ther. 2008, 16, S149–S150. [Google Scholar] [CrossRef]
- Cvetkoska, A.; Piro, E.; Reberšek, M.; Magjarević, R.; Miklavčič, D. Towards Standardization of Electroporation Devices and Protocols. IEEE Instrum. Meas. Mag. 2020, 23, 74–81. [Google Scholar] [CrossRef]
- Gehl, J. Electroporation for Drug and Gene Delivery in the Clinic: Doctors Go Electric. In Methods in Molecular Biology (Clifton, N.J.); Li, S., Ed.; Humana Press: Totowa, NJ, USA, 2008; Volume 423, pp. 351–359. ISBN 978-1-58829-877-5/978-1-59745-194-9. [Google Scholar]
- Kos, S.; Blagus, T.; Cemazar, M.; Lampreht Tratar, U.; Stimac, M.; Prosen, L.; Dolinsek, T.; Kamensek, U.; Kranjc, S.; Steinstraesser, L.; et al. Electrotransfer Parameters as a Tool for Controlled and Targeted Gene Expression in Skin. Mol. Ther. Nucleic Acids 2016, 5, e356. [Google Scholar] [CrossRef]
- Remic, T.; Sersa, G.; Ursic, K.; Cemazar, M.; Kamensek, U. Development of Tumor Cell-Based Vaccine with IL-12 Gene Electrotransfer as Adjuvant. Vaccines 2020, 8, 111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schindelin, J.; Arganda-Carreras, I.; Frise, E.; Kaynig, V.; Longair, M.; Pietzsch, T.; Preibisch, S.; Rueden, C.; Saalfeld, S.; Schmid, B.; et al. Fiji: An Open-Source Platform for Biological-Image Analysis. Nat. Methods 2012, 9, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Heller, R.; Cruz, Y.; Heller, L.C.; Gilbert, R.A.; Jaroszeski, M.J. Electrically Mediated Delivery of Plasmid DNA to the Skin, Using a Multielectrode Array. Hum. Gene Ther. 2010, 21, 357–362. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Skin Layer | Layer Thickness | σx (S/m) | σy (S/m) | σz (S/m) | RE Threshold (V/cm) | IRE Threshold (V/cm) | Maximal σ Increase |
|---|---|---|---|---|---|---|---|
| Stratum corneum | 20 µm | 1.10 × 10−2 | 1.10 × 10−2 | 2.23 × 10−4 | 400 | 1200 | 100× |
| Epidermis | 0.1 mm | 5.82 × 10−2 | 5.82 × 10−2 | 6.36 × 10−2 | 400 | 1200 | 3.5× |
| Papillary dermis * | 0.15 mm | 7.19 × 10−2 | 7.19 × 10−2 | 7.19 × 10−2 | 300 | 1200 | 3.5× |
| Upper vessel plexus | 80 µm | 4.22 × 10−1 | 3.86 × 10−1 | 3.86 × 10−1 | 300 | 1200 | 3.5× |
| Supply layer | 1 mm | 3.12 × 10−1 | 3.12 × 10−1 | 3.19 × 10−1 | 300 | 1200 | 3.5× |
| Deeper vessel plexus | 0.1 cm | 3.42 × 10−1 | 3.28 × 10−1 | 3.28 × 10−1 | 300 | 1200 | 3.5× |
| Hypodermis * | 0.5 cm | 6.35 × 10−2 | 6.35 × 10−2 | 6.35 × 10−2 | 300 | 1200 | 3.5× |
| Muscles | 2 cm | 1.57 × 10−2 | 6.86 × 10−2 | 1.57 × 10−2 | 200 ** 80 ** | 800 | 2.5× |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cvetkoska, A.; Dermol-Černe, J.; Miklavčič, D.; Kranjc Brezar, S.; Markelc, B.; Serša, G.; Reberšek, M. Design, Development, and Testing of a Device for Gene Electrotransfer to Skin Cells In Vivo. Pharmaceutics 2022, 14, 1826. https://doi.org/10.3390/pharmaceutics14091826
Cvetkoska A, Dermol-Černe J, Miklavčič D, Kranjc Brezar S, Markelc B, Serša G, Reberšek M. Design, Development, and Testing of a Device for Gene Electrotransfer to Skin Cells In Vivo. Pharmaceutics. 2022; 14(9):1826. https://doi.org/10.3390/pharmaceutics14091826
Chicago/Turabian StyleCvetkoska, Aleksandra, Janja Dermol-Černe, Damijan Miklavčič, Simona Kranjc Brezar, Boštjan Markelc, Gregor Serša, and Matej Reberšek. 2022. "Design, Development, and Testing of a Device for Gene Electrotransfer to Skin Cells In Vivo" Pharmaceutics 14, no. 9: 1826. https://doi.org/10.3390/pharmaceutics14091826