
Design of GSH-Responsive Curcumin Nanomicelles for Oesophageal Cancer Therapy

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Synthesis of ATRA-SS-HA
2.2. Preparation of Micelles
2.3. Calculation of Critical Micelle Concentration
2.4. Curcumin Chromatographic Analysis
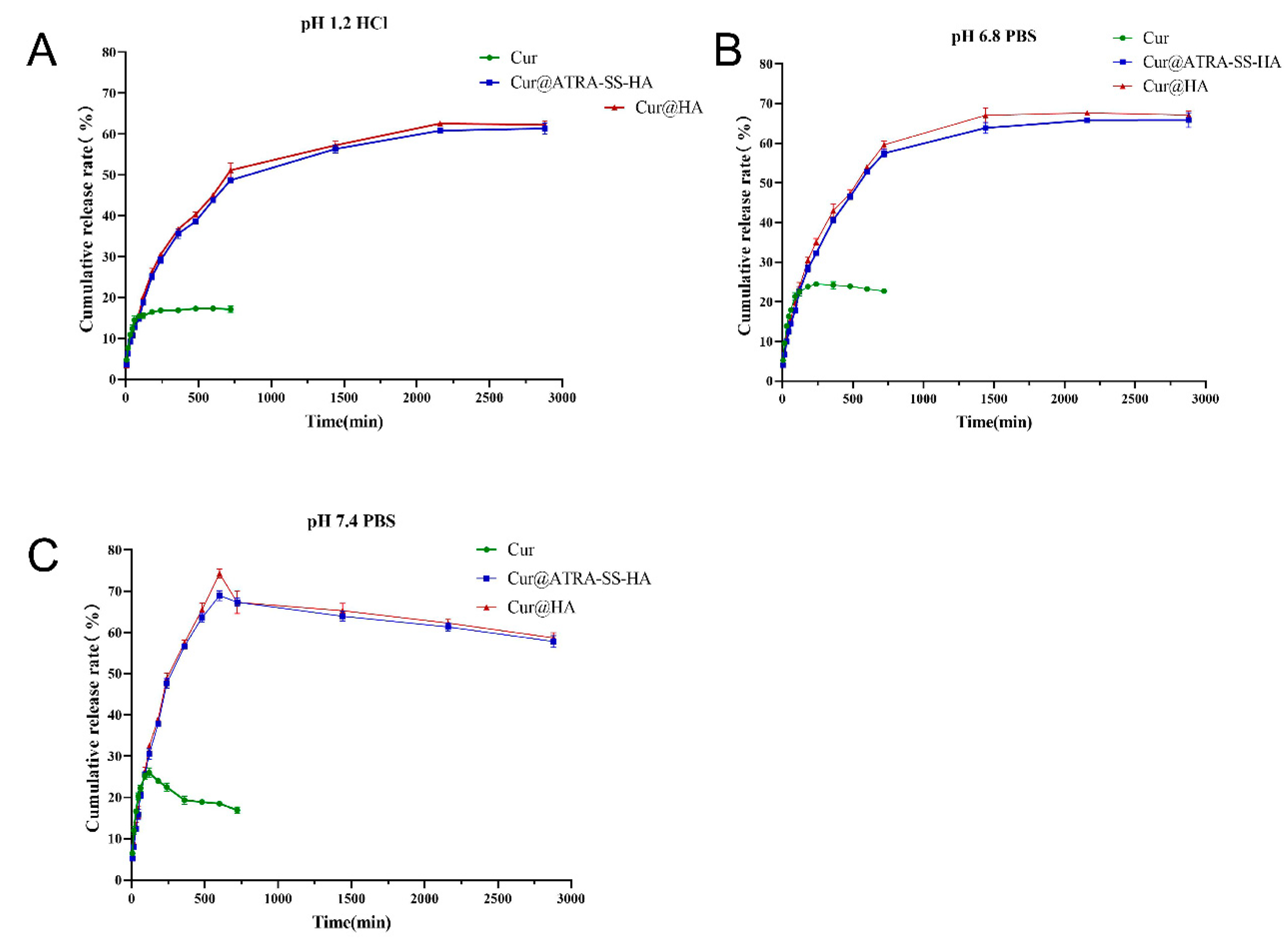
2.5. In Vitro Release of Cur@ATRA-SS-HA and Cur@HA Nano Micelles
2.6. GSH Sensitivity of Cur@HA and Cur@ATRA-SS-HA
2.7. Cell Culture
2.8. Cellular Targeting of Rho@HA and Rho@ATRA-SS-HA
2.9. In Vitro Biocompatibility and Antitumor Activity of Cur@ATRA-SS-HA
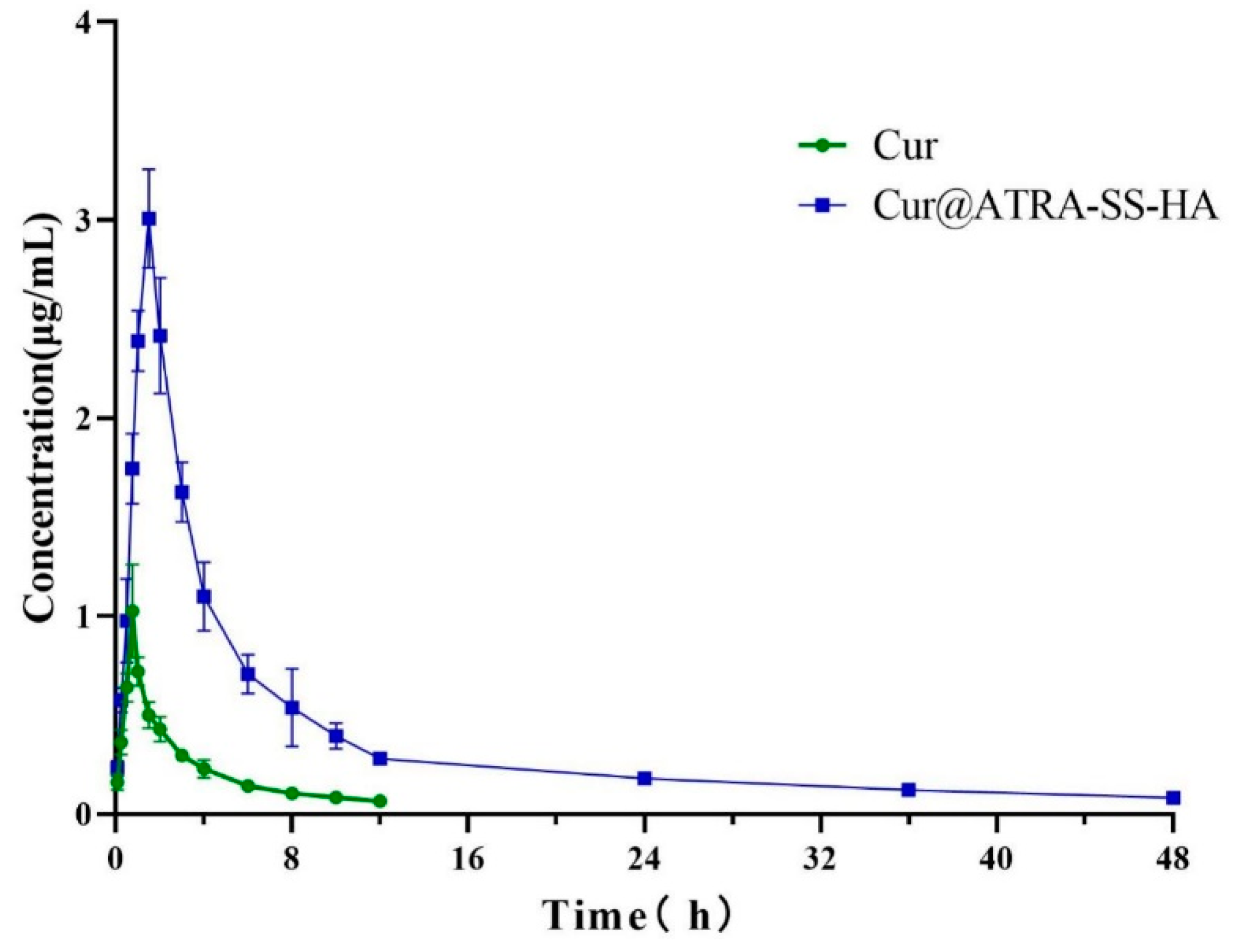
2.10. In Vivo Pharmacokinetic Testing
3. Results and Discussion
3.1. Synthesis of ATRA-SS-HA
3.2. Preparation and Characterization of Cur@ATRA-SS-HA Nanomicelles
3.3. In Vitro Release of Cur@ATRA-SS-HA and Cur@HA Nanomicelles
3.4. Cellular Targeting of Cur@ATRA-SS-HA
3.5. In Vitro Biocompatibility and Antitumor Activity of Cur@ATRA-SS-HA
3.6. In Vivo Pharmacokinetic Testing
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Lee, S.; Cohen, D.J. Pharmacotherapy for metastatic esophageal cancer: Where do we need to improve? Expert Opin. Pharm. 2019, 20, 357–366. [Google Scholar] [CrossRef]
- Raufi, A.G.; Klempner, S.J. Immunotherapy for advanced gastric and esophageal cancer: Preclinical rationale and ongoing clinical investigations. J. Gastrointest Oncol. 2015, 6, 561–569. [Google Scholar]
- Orazbayev, B.A.; Musulmanbekov, K.; Bukenov, A. Analysis of Treatment Results of the Thoracic Part of Oesophageal Cancer. Open Access Maced J. Med. Sci. 2019, 7, 82–87. [Google Scholar] [CrossRef]
- Jones, C.; Spencer, K.; Hitchen, C.; Pelly, T.; Wood, B.; Hatfield, P.; Crellin, A.; Sebag-Montefiore, D.; Goody, R.; Crosby, T.; et al. Hypofractionated Radiotherapy in Oesophageal Cancer for Patients Unfit for Systemic Therapy: A Retrospective Single-Centre Analysis. Clin. Oncol. 2019, 31, 356–364. [Google Scholar] [CrossRef]
- Sjoquist, K.M.; Burmeister, B.H.; Smithers, B.M.; Zalcberg, J.R.; Simes, R.J.; Barbour, A.; Gebski, V.; Australasian Gastro-Intestinal Trials Group. Survival after neoadjuvant chemotherapy or chemoradiotherapy for resectable oesophageal carcinoma: An updated meta-analysis. Lancet Oncol. 2011, 12, 681–692. [Google Scholar] [CrossRef]
- Yamazaki, K.; Hironaka, S.; Boku, N.; Yasui, H.; Fukutomi, A.; Yoshino, T.; Onozawa, Y.; Hasuike, N.; Inui, T.; Yamaguchi, Y.; et al. A retrospective study of second-line chemotherapy for unresectable or recurrent squamous cell carcinoma of the esophagus refractory to chemotherapy with 5-fluorouracil plus platinum. Int. J. Clin. Oncol. 2008, 13, 150–155. [Google Scholar] [CrossRef]
- Rice, T.W.; Vogelbaum, M.A.; Mason, D.P.; Blackstone, E.H. Brain metastases from esophageal cancer: A phenomenon of adjuvant therapy? Ann. Thorac. Surg. 2006, 82, 2042–2049.e1–2. [Google Scholar] [CrossRef]
- Wadhwa, R.; Taketa, T.; Correa, A.M.; Sudo, K.; Campagna, M.-C.; Blum, M.A.; Komaki, R.; Skinner, H.; Lee, J.H.; Bhutani, M.S.; et al. Incidence of brain metastases after trimodality therapy in patients with esophageal or gastroesophageal cancer: Implications for screening and surveillance. Oncology 2013, 85, 204–207. [Google Scholar] [CrossRef]
- Shiozaki, H.; Sudo, K.; Xiao, L.; Wadhwa, R.; Elimova, E.; Hofstetter, W.L.; Skinner, H.D.; Lee, J.H.; Weston, B.; Bhutani, M.S.; et al. Distribution and timing of distant metastasis after local therapy in a large cohort of patients with esophageal and esophagogastric junction cancer. Oncology 2014, 86, 336–339. [Google Scholar] [CrossRef]
- Kim, Y.-H.; Ha, K.-Y.; Kim, S.-I. Spinal Cord Injury and Related Clinical Trials. Clin. Orthop. Surg. 2017, 9, 1–9. [Google Scholar] [CrossRef]
- Giordano, A.; Tommonaro, G. Curcumin and Cancer. Nutrients 2019, 11, 2376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shao, Z.-M.; Shen, Z.-Z.; Liu, C.-H.; Sartippour, M.R.; Go, V.L.; Heber, D.; Nguyen, M. Curcumin exerts multiple suppressive effects on human breast carcinoma cells. Int. J. Cancer 2002, 98, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.-Y.; Shi, Y.-Q.; Chen, X.; Dai, J.; Jiang, Z.-F.; Li, N.; Zhang, Z.-B. Protective effect of curcumin against formaldehyde-induced genotoxicity in A549 Cell Lines. J. Appl. Toxicol. 2013, 33, 1468–1473. [Google Scholar] [PubMed]
- Xue, X.; Yu, J.-L.; Sun, D.-Q.; Kong, F.; Qu, X.-J.; Zou, W.; Wu, J.; Wang, R.-M. Curcumin induces apoptosis in SGC-7901 gastric adenocarcinoma cells via regulation of mitochondrial signaling pathways. Asian Pac. J. Cancer Prev. 2014, 15, 3987–3992. [Google Scholar] [CrossRef]
- Kunati, S.R.; Yang, S.; William, B.M.; Xu, Y. An LC-MS/MS method for simultaneous determination of curcumin, curcumin glucuronide and curcumin sulfate in a phase II clinical trial. J. Pharm. Biomed. Anal. 2018, 156, 189–198. [Google Scholar] [CrossRef]
- Dosio, F.; Arpicco, S.; Stella, B.; Fattal, E. Hyaluronic acid for anticancer drug and nucleic acid delivery. Adv. Drug. Deliv. Rev. 2016, 97, 204–236. [Google Scholar]
- Bhattacharya, D.S.; Svechkarev, D.; Souchek, J.J.; Hill, T.K.; Taylor, M.A.; Natarajan, A.; Mohs, A.M. Impact of structurally modifying hyaluronic acid on CD44 interaction. J. Mater Chem. B 2017, 5, 8183–8192. [Google Scholar]
- Cadete, A.; Alonso, M.J. Targeting cancer with hyaluronic acid-based nanocarriers: Recent advances and translational perspectives. Nanomedicine 2016, 11, 2341–2357. [Google Scholar] [CrossRef]
- Ying, M.; Zhou, X.; Lin, N.; Jing, H.; Yang, X.; Yang, B. Bortezomib sensitizes human acute myeloid leukemia cells to all-trans-retinoic acid-induced differentiation by modifying the RARalpha/STAT1 axis. Mol. Cancer Ther. 2013, 12, 195–206. [Google Scholar] [CrossRef]
- Bobal, P.; Lastovickova, M.; Bobalova, J. The Role of ATRA, Natural Ligand of Retinoic Acid Receptors, on EMT-Related Proteins in Breast Cancer: Minireview. Int. J. Mol. Sci. 2021, 22, 13345. [Google Scholar] [CrossRef]
- Ling, X.; Tu, J.; Wang, J.; Shajii, A.; Kong, N.; Feng, C.; Zhang, Y.; Yu, M.; Xie, T.; Bharwani, Z.; et al. Glutathione-Responsive Prodrug Nanoparticles for Effective Drug Delivery and Cancer Therapy. ACS Nano 2019, 13, 357–370. [Google Scholar] [PubMed]
- Giorgio, M.; Trinei, M.; Migliacco, E.; Pelicci, P.G. Hydrogen peroxide: A metabolic by-product or a common mediator of ageing signals? Nat. Rev. Mol. Cell Biol. 2007, 8, 722–728. [Google Scholar] [PubMed]
- Sun, H.; Meng, F.; Cheng, R.; Deng, C.; Zhong, Z. Reduction-responsive polymeric micelles and vesicles for triggered intracellular drug release. Antioxid Redox Signal. 2014, 21, 755–767. [Google Scholar] [PubMed] [Green Version]
- Guo, Y.; Gao, T.; Fang, F.; Sun, S.; Yang, D.; Li, Y.; Lv, S. A novel polymer micelle as a targeted drug delivery system for 10-hydroxycamptothecin with high drug-loading properties and anti-tumor efficacy. Biophys. Chem. 2021, 279, 106679. [Google Scholar]
- Oyarzun-Ampuero, F.A.; Goycoolea, F.M.; Torres, D.; Alonso, M.J. A new drug nanocarrier consisting of polyarginine and hyaluronic acid. Eur. J. Pharm. Biopharm. 2011, 79, 54–57. [Google Scholar]
- Subongkot, T.; Ngawhirunpat, T. Development of a novel microemulsion for oral absorption enhancement of all-trans retinoic acid. Int. J. Nanomed. 2017, 12, 5585. [Google Scholar]
- Le-Vinh, B.; Le, N.-M.N.; Nazir, I.; Matuszczak, B.; Bernkop-Schnürch, A. Chitosan based micelle with zeta potential changing property for effective mucosal drug delivery. Int. J. Biol. Macromol. 2019, 133, 647–655. [Google Scholar]
- Zhang, S.-F.; Hu, W.; Yan, X.; Wang, D.; Yang, W.; Zhang, J.; Liu, Z. Chondroitin sulfate-curcumin micelle with good stability and reduction sensitivity for anti-cancer drug carrier. Mater. Lett. 2021, 304, 130667. [Google Scholar]
- Lin, D.; Xiao, L.; Qin, W.; Loy, D.A.; Wu, Z.; Chen, H.; Zhang, Q. Preparation, characterization and antioxidant properties of curcumin encapsulated chitosan/lignosulfonate micelles. Carbohydr. Polym. 2022, 281, 119080. [Google Scholar]
- Sahu, A.; Kasoju, N.; Goswami, P.; Bora, U. Encapsulation of curcumin in Pluronic block copolymer micelles for drug delivery applications. J. Biomater. Appl. 2011, 25, 619–639. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample | Particle Size (nm) | PDI | Zeta Potential (mV) |
|---|---|---|---|
| Cur@ATRA-SS-HA | 149.87 ± 2.34 | 0.198 ± 0.012 | −27.52 ± 0.46 |
| Cur@HA | 147.87 ± 2.71 | 0.201 ± 0.011 | −25.91 ± 0.39 |
| Sample Time | Drug Loading (%) | Encapsulation Rate (%) | Particle Size (nm) | ||||
|---|---|---|---|---|---|---|---|
| Cur@ATRA-SS-HA | 4 °C | 25 °C | 4 °C | 25 °C | 4 °C | 25 °C | |
| 0 day | 25.72 ± 1.12 | 25.59 ± 0.98 | 90.76 ± 0.46 | 90.54 ± 0.68 | 147.26 ± 2.87 | 147.39 ± 1.78 | |
| 15 days | 24.12 ± 1.47 | 23.82 ± 2.11 | 88.12 ± 1.52 | 87.10 ± 1.77 | 150.32 ± 2.98 | 156.14 ± 2.68 | |
| 30 days | 23.65 ± 1.86 | 22.65 ± 2.01 | 87.23 ± 1.89 | 85.12 ± 2.53 | 156.46 ± 3.35 | 164.58 ± 3.78 | |
| Cur@HA | 4 °C | 25 °C | 4 °C | 25 °C | 4 °C | 25 °C | |
| 0 day | 25.51 ± 1.82 | 25.35 ± 0.67 | 91.16 ± 0.67 | 91.27 ± 0.56 | 149.89 ± 2.41 | 148.17 ± 1.37 | |
| 15 days | 23.87 ± 1.89 | 22.19 ± 2.44 | 88.82 ± 1.64 | 87.34 ± 1.58 | 152.17 ± 3.49 | 155.63 ± 2.56 | |
| 30 days | 21.92 ± 1.71 | 21.28 ± 2.58 | 86.53 ± 1.99 | 84.48 ± 2.78 | 157.39 ± 3.88 | 165.49 ± 3.87 | |
| Sample | Particle Size (nm) |
|---|---|
| 10 Μm GSH + Cur@ATRA-SS-HA | 146.23 ± 3.18 |
| 100 μM GSH + Cur@ATRA-SS-HA | 148.62 ± 3.52 |
| 1 mM GSH + Cur@ATRA-SS-HA | 183.43 ± 4.98 |
| 10 mM GSH + Cur@ATRA-SS-HA | 263.81 ± 6.84 |
| Cur@ATRA-SS-HA | 149.11 ± 2.59 |
| 10 mM GSH + Cur@HA | 152.73 ± 2.39 |
| Sample | 5-FU | Cur | Cur@ATRA-SS-HA |
|---|---|---|---|
| IC50 (μg/mL) | 1.625 | 2.588 | 1.136 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ma, Z.; Gao, X.; Raza, F.; Zafar, H.; Huang, G.; Yang, Y.; Shi, F.; Wang, D.; He, X. Design of GSH-Responsive Curcumin Nanomicelles for Oesophageal Cancer Therapy. Pharmaceutics 2022, 14, 1802. https://doi.org/10.3390/pharmaceutics14091802
Ma Z, Gao X, Raza F, Zafar H, Huang G, Yang Y, Shi F, Wang D, He X. Design of GSH-Responsive Curcumin Nanomicelles for Oesophageal Cancer Therapy. Pharmaceutics. 2022; 14(9):1802. https://doi.org/10.3390/pharmaceutics14091802
Chicago/Turabian StyleMa, Zhaoming, Xuzhu Gao, Faisal Raza, Hajra Zafar, Guanhong Huang, Yunyun Yang, Feng Shi, Deqiang Wang, and Xia He. 2022. "Design of GSH-Responsive Curcumin Nanomicelles for Oesophageal Cancer Therapy" Pharmaceutics 14, no. 9: 1802. https://doi.org/10.3390/pharmaceutics14091802