
Swiss Medical Devices for Autologous Regenerative Medicine: From Innovation to Clinical Validation


Abstract
:1. Introduction
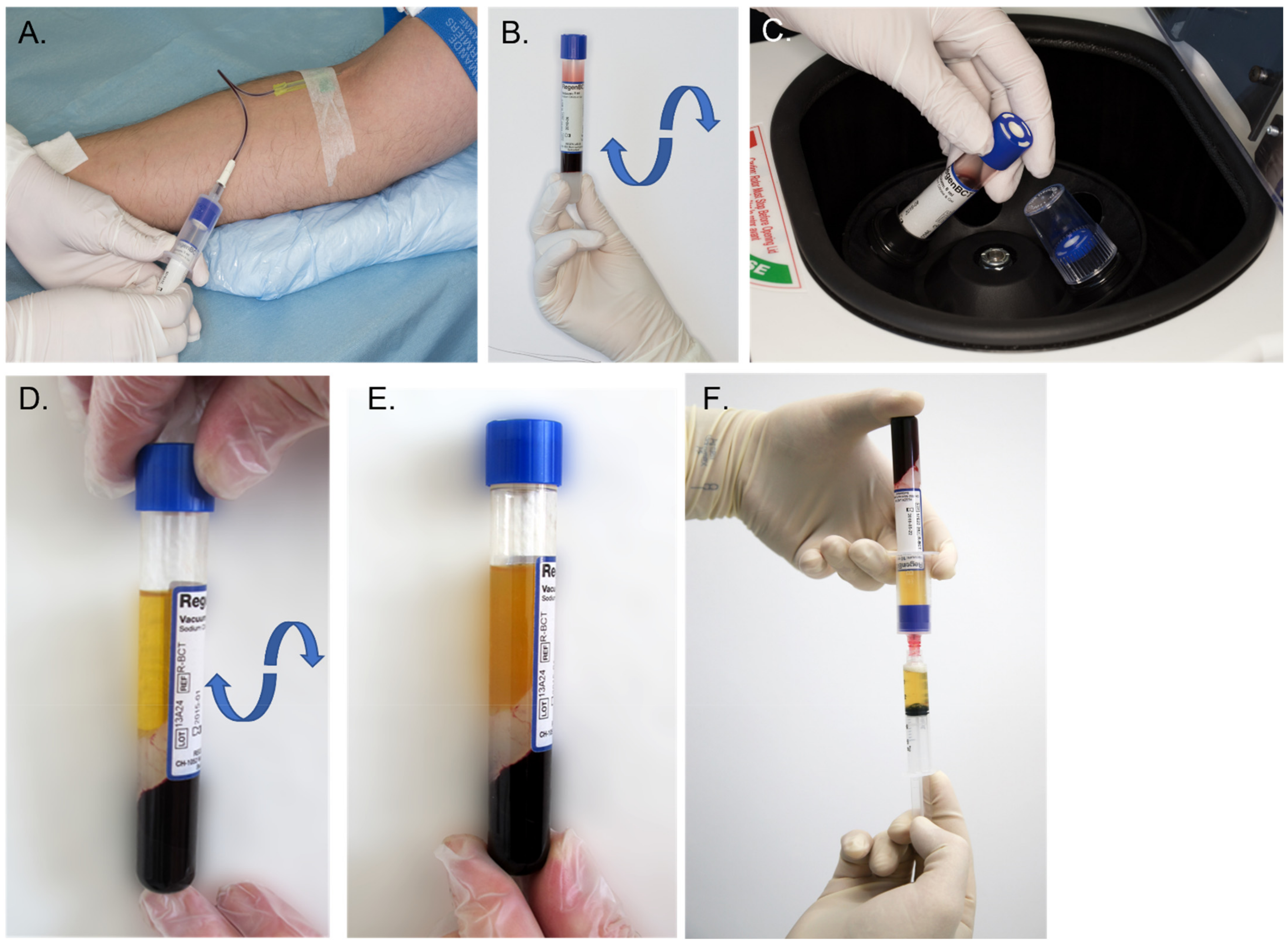
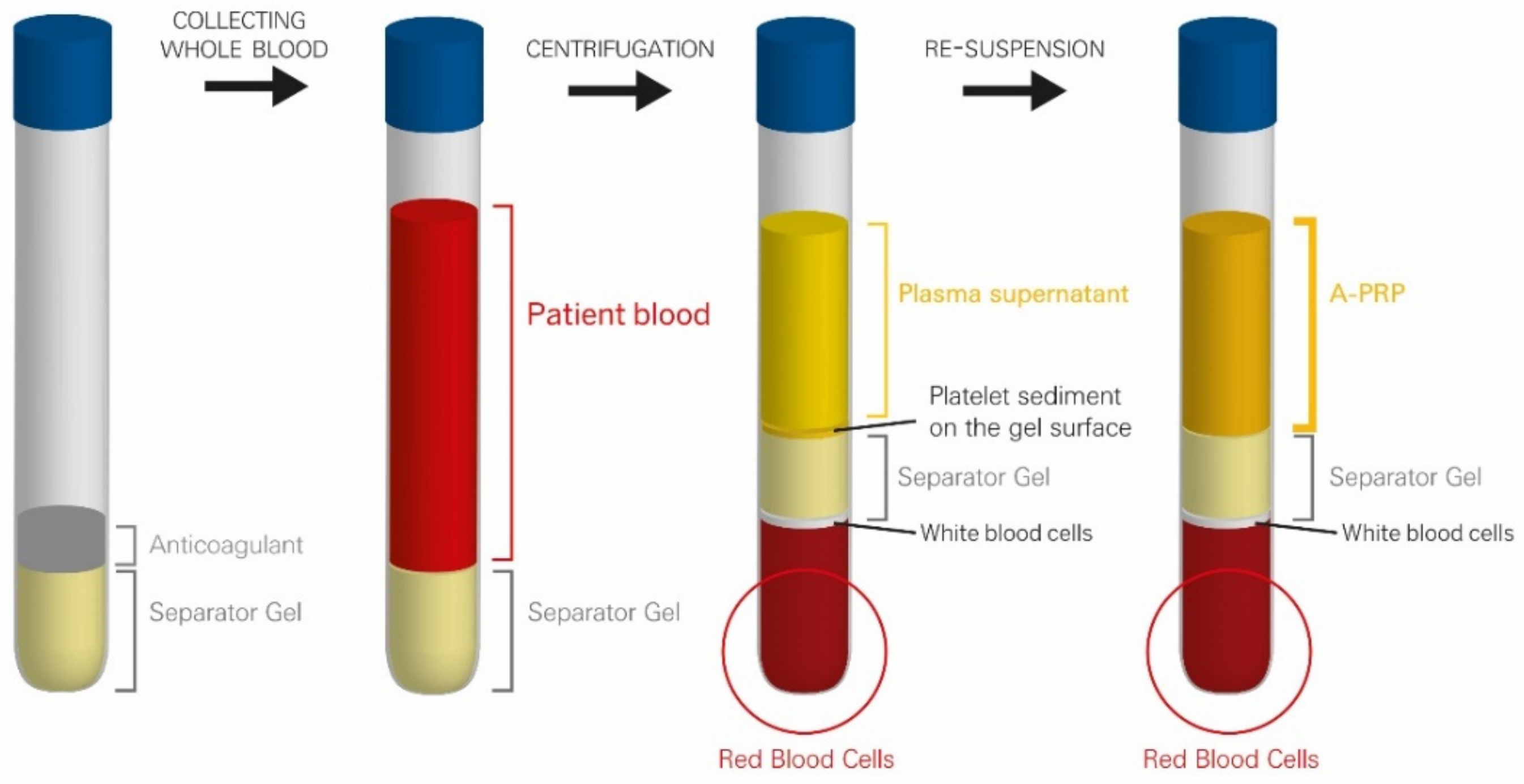
2. Standard PRP Isolation Processes
3. Manufacturing Innovative Devices for Standardized PRP Preparation
3.1. Design and Manufacturing of Medical Devices for Safe and Effective PRP Preparation
3.1.1. Essential Requirements for the Manufacturer
3.1.2. Design of Devices That Respond to User Needs for Preparation of Standardized PRP
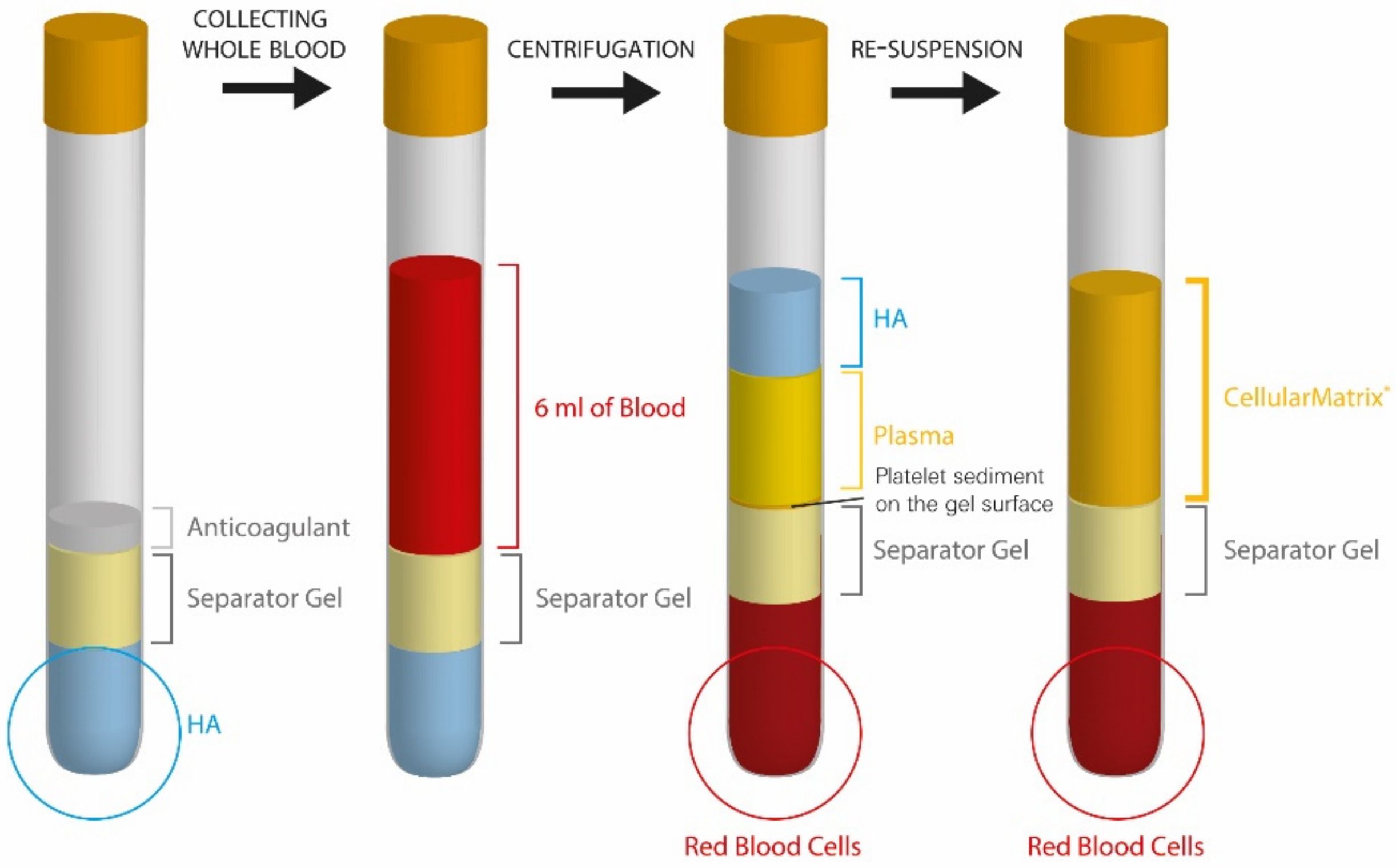
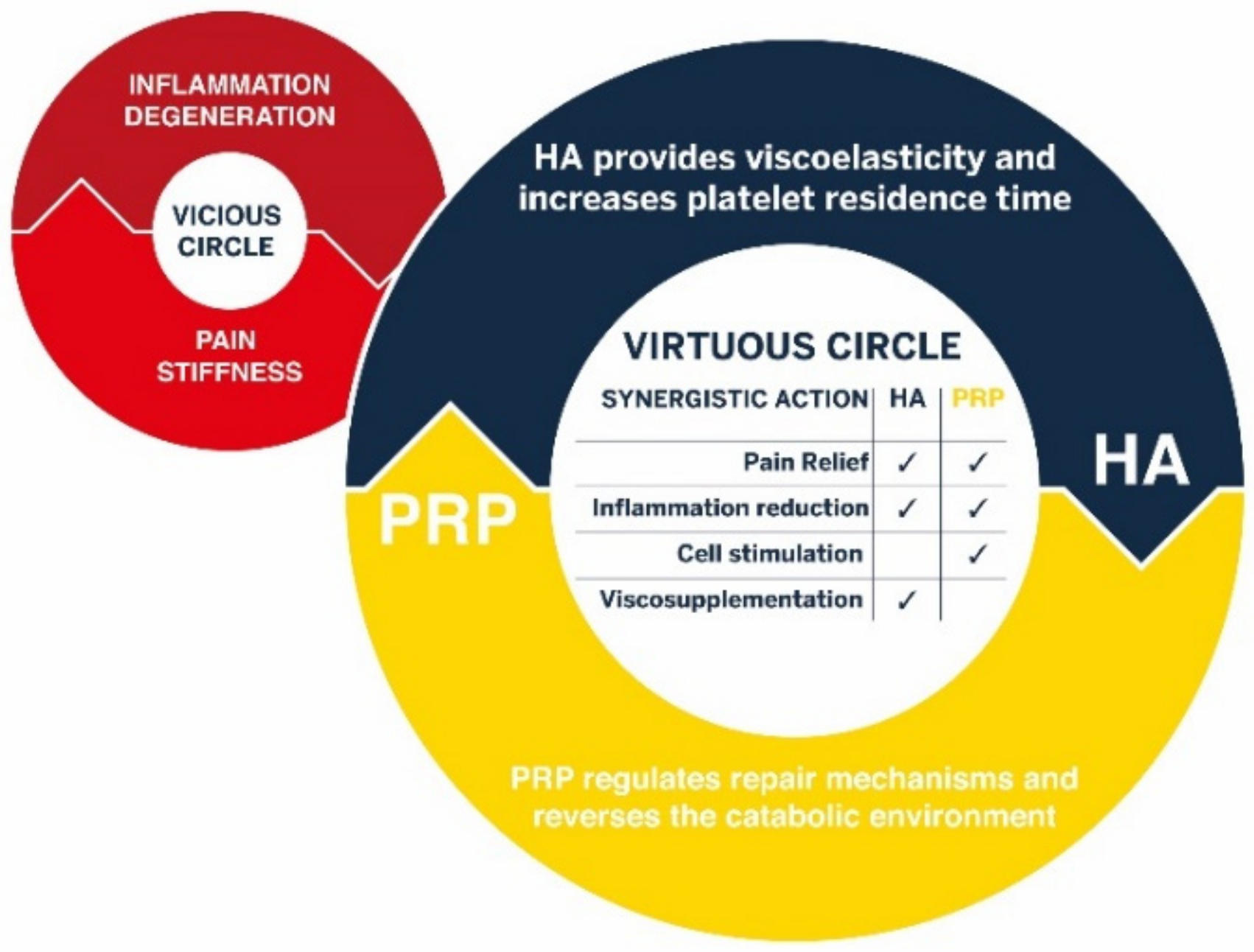
3.2. Innovative Biological Combinations with Hyaluronic Acid for a Synergistic Tissue Regeneration
4. Swiss Translational Research Projects for In Vitro Validation of Regen Lab Technology Platform for Tissue Engineering and Cell Therapy Research
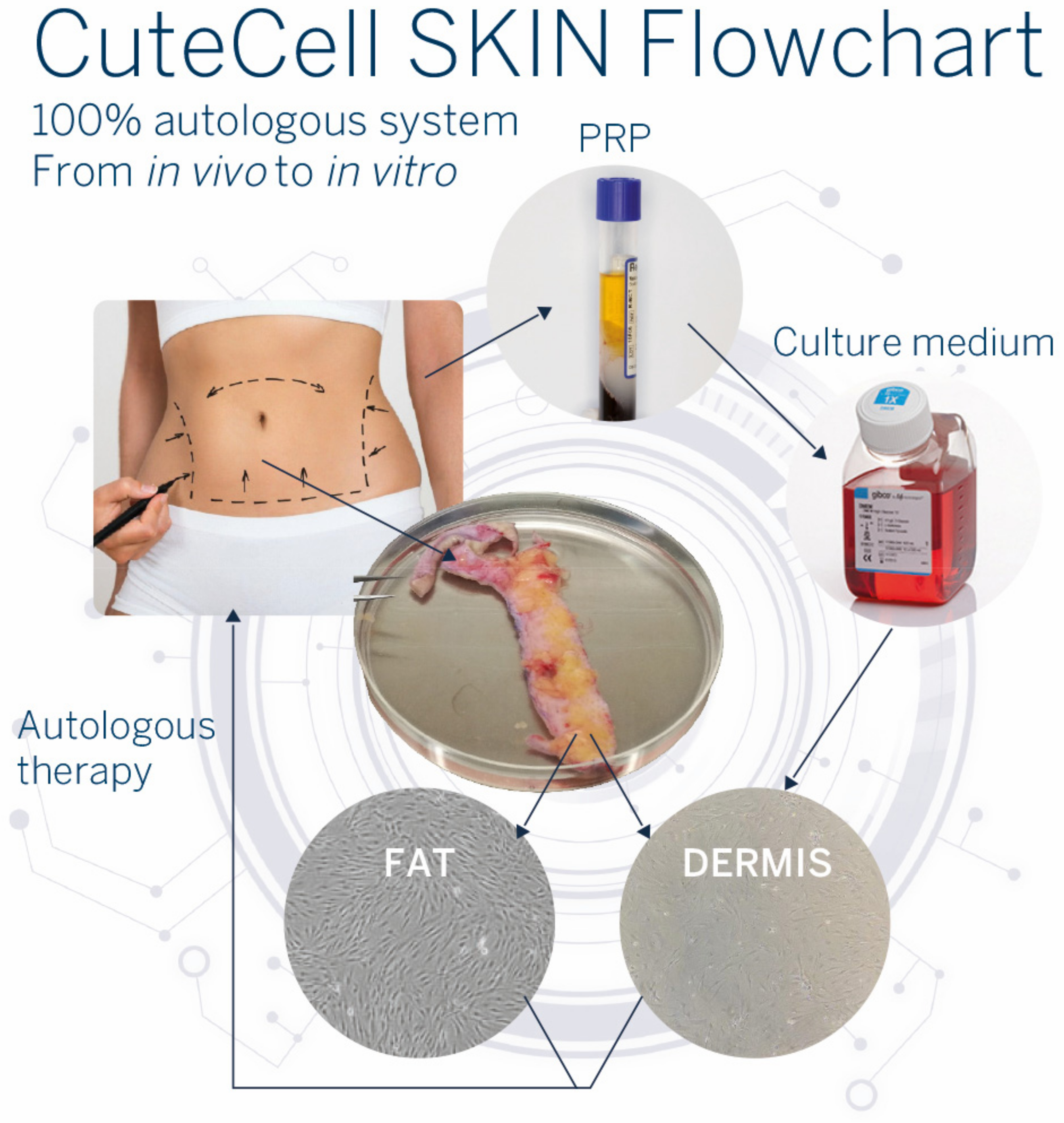
4.1. Cell Therapy Research: From In Vivo to In Vitro and Back to In Vivo
4.2. Safety and Efficacy Demonstration in Translational Research Projects: Establishment of 100% Autologous Cell Culture Models
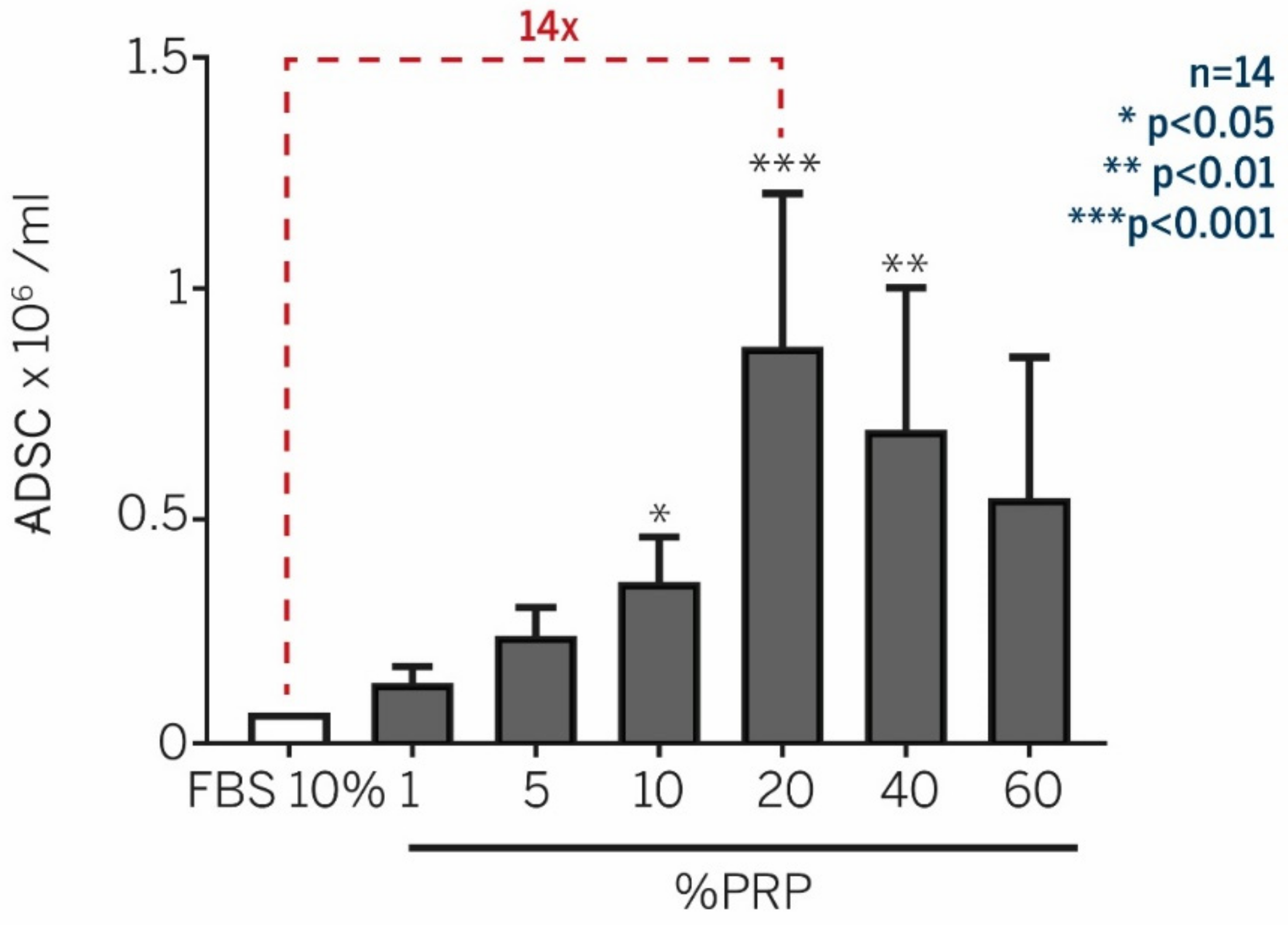
4.2.1. Adipose-Derived Mesenchymal Stem Cells (ADSCs)
- -
- Enhancement of ADSC expansion with PRP supplementation
- -
- PRP does not alter ADSC phenotype, differentiation capacity, and chromosome status
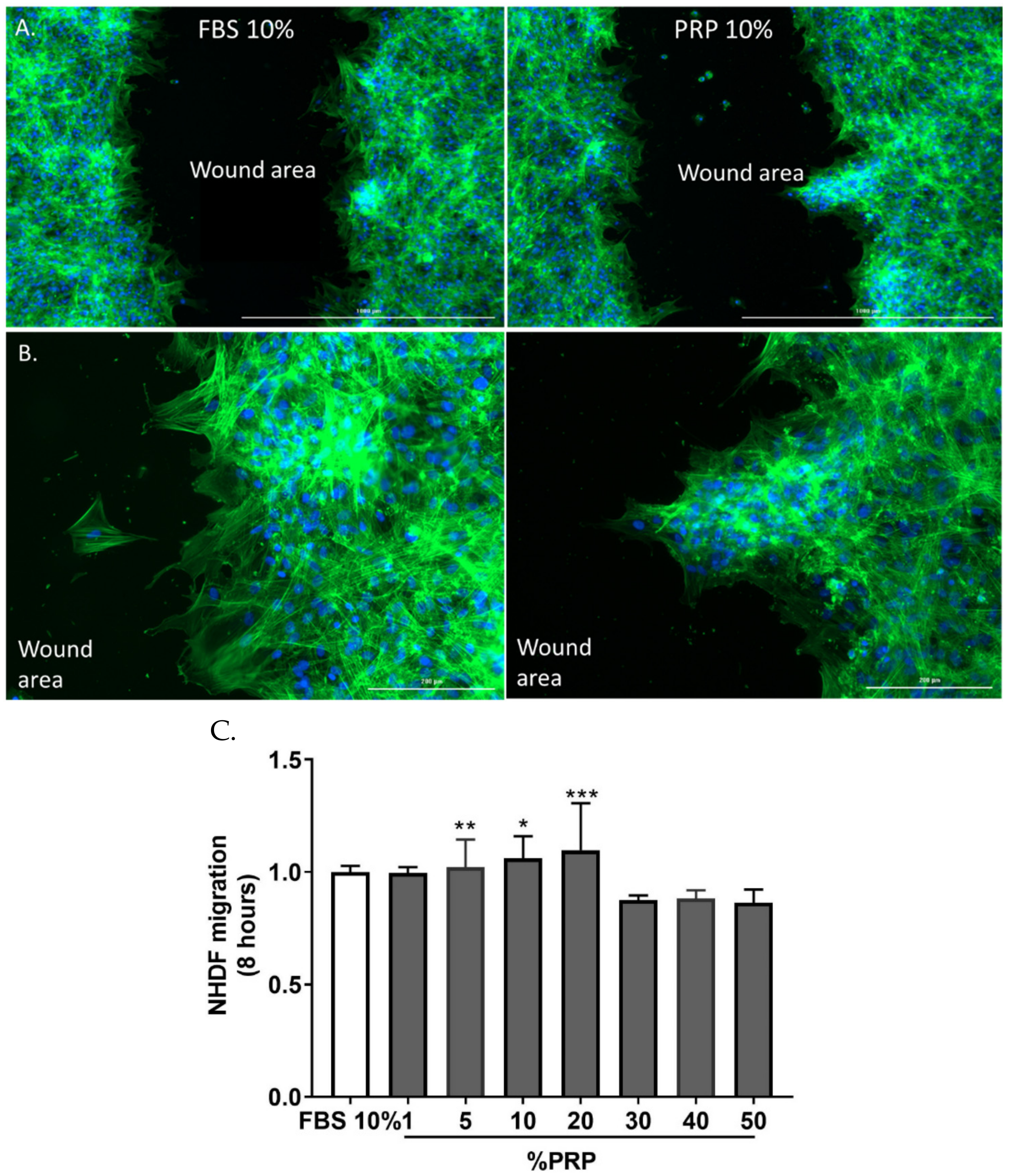
4.2.2. Human Dermal Fibroblasts (NHDF)
- -
- Enhancement of fibroblast expansion with autologous PRP treatment
- -
- Optimal PRP concentration is crucial for the maintenance of fibroblast phenotype
- -
- CuteCell PRP modulates metabolic activity, fibroblast adhesion, and favors migration
- -
- Whole genome analysis to demonstrate that CuteCell PRP is safe at the genomic level
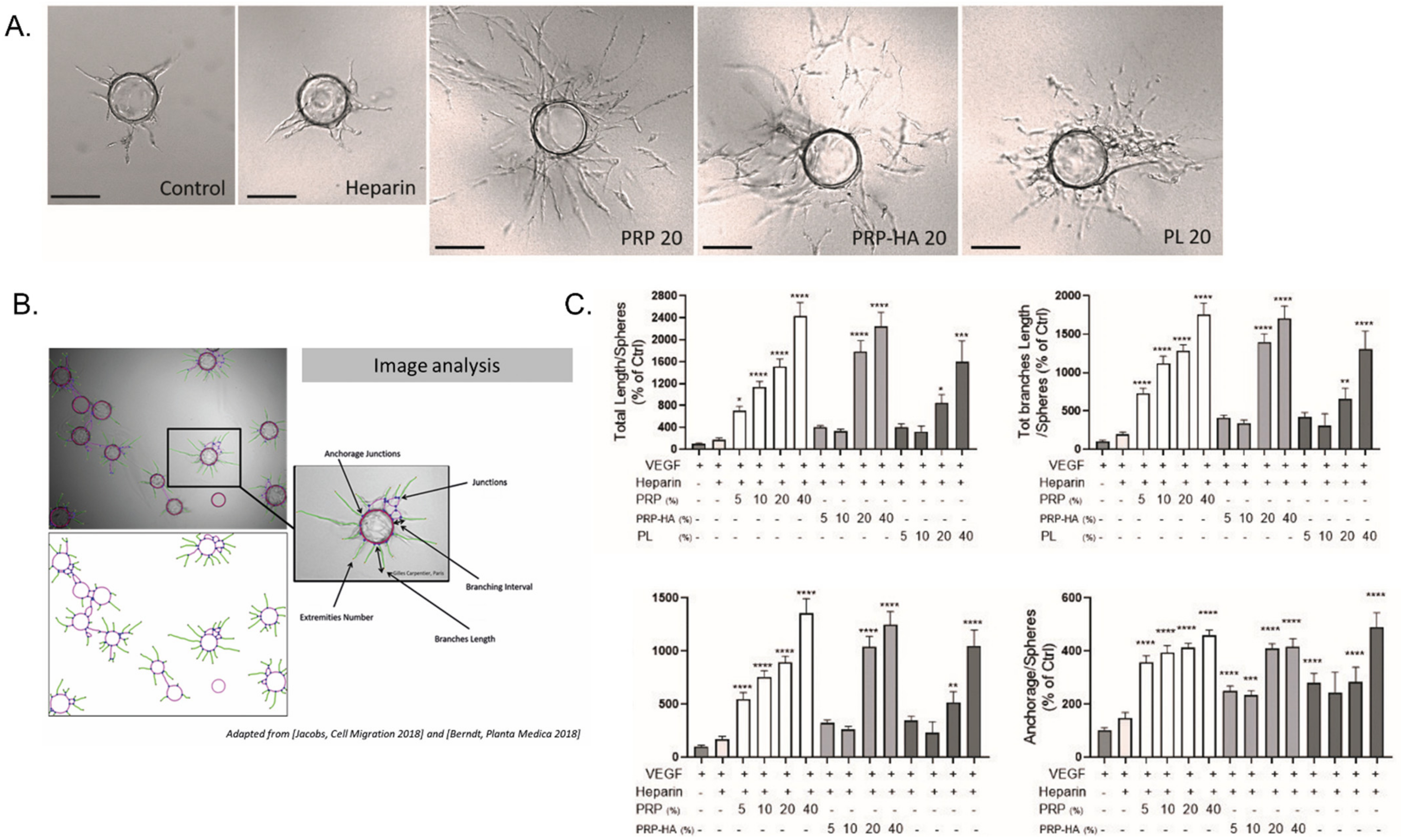
4.3. Angiogenesis Is Differentially Modulated by Platelet-Derived Preparations
- -
- PRP and PRP-HA modulate endothelial cells (HUVEC) angiogenic activities in 3D
- -
- Effect on HUVEC viability and senescence
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| 3D | three dimensional |
| ACDA | acid citrate dextrose solution |
| ADSC | Adipose-derived mesenchymal stem cells |
| Ang 1 | angiopoietin-1 |
| BCT | blood cell therapy |
| βIgH3 | factor-β-induced protein Ig-H3 |
| CE | European conformity |
| CEO | chief executive officer |
| EC | endothelial cells |
| FBA | fibrin bead assay |
| FBS | fetal bovine serum |
| GMP | good manufacturing practices |
| HA | hyaluronic acid |
| HGF | hepatocyte growth factor |
| HUVEC | human umbilical vein endothelial cells |
| IGFBP7 | insulin-like growth factor binding protein 7 |
| LP-PRP | leukocyte poor PRP |
| LR-PRP | leukocyte rich PRP |
| NHDF | normal human dermal fibroblasts |
| MDD | medical device directive |
| MDR | medical device regulation |
| MDSAP | medical device single audit program |
| MNC | mononuclear cells |
| MTT | 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyl-2H-tetrazolium bromide |
| OA | osteoarthritis |
| Ph. Eur | European pharmacopeia |
| PPP | platelet poor plasma |
| PRP | platelet-rich plasma |
| PRP-HA | platelet-rich plasma combined with hyaluronic acid |
| PL | platelet lysates |
| SMA | smooth muscle actin |
| SPARC | secreted protein acidic and cysteine-rich |
| TGF-α | transforming growth factor alpha |
| USP | US pharmacopeia |
References
- Wu, P.I.; Diaz, R.; Borg-Stein, J. Platelet-Rich Plasma. Phys. Med. Rehabil. Clin. N. Am. 2016, 27, 825–853. [Google Scholar] [CrossRef] [PubMed]
- Knighton, D.R.; Hunt, T.K.; Thakral, K.K.; Goodson, W.H., 3rd. Role of platelets and fibrin in the healing sequence: An in vivo study of angiogenesis and collagen synthesis. Ann. Surg 1982, 196, 379–388. [Google Scholar] [CrossRef] [PubMed]
- Knighton, D.R.; Ciresi, K.F.; Fiegel, V.D.; Austin, L.L.; Butler, E.L. Classification and treatment of chronic nonhealing wounds. Successful treatment with autologous platelet-derived wound healing factors (PDWHF). Ann. Surg. 1986, 204, 322–330. [Google Scholar] [CrossRef]
- Labusca, L.S.; Cionca, D. Clinical review about the role of platelet rich plasma for the treatment of traumatic and degenerative musculoskeletal disorders. Orthop. Rheumatol. Open Access J. 2016, 2, 70–82. [Google Scholar] [CrossRef]
- Cohn, C.S.; Lockhart, E. Autologous platelet-rich plasma: Evidence for clinical use. Curr. Opin. Hematol. 2015, 22, 527–532. [Google Scholar] [CrossRef] [PubMed]
- Engebretsen, L.; Steffen, K.; Alsousou, J.; Anitua, E.; Bachl, N.; Devilee, R.; Everts, P.; Hamilton, B.; Huard, J.; Jenoure, P.; et al. IOC consensus paper on the use of platelet-rich plasma in sports medicine. Br. J. Sports Med. 2010, 44, 1072–1081. [Google Scholar] [CrossRef]
- Department of Health and Human Services. Federal Food, Drug, and Cosmetic Act (FD&C Act); FDA: Silver Spring, ML, USA, 2022; pp. 103–117.
- Regulation (EU) 2017/745 of the European Parliament and of the Council of 5 April 2017 on Medical Devices, Amending Directive 2001/83/EC, Regulation (EC) No 178/2002 and Regulation (EC) No 1223/2009 and Repealing Council Directives 90/385/EEC and 93/42/EEC. Available online: https://eur-lex.europa.eu (accessed on 5 April 2017).
- Harmon, K.; Hanson, R.; Bowen, J.; Greenberg, S.; Magaziner, E.; Vandenbosch, J.; Harshfield, D.; Shiple, B.; Audley, D. Guidelines for the Use of Platelet Rich Plasma. Int. Cell. Med. Soc. 2011. Available online: http://www.cellmedicinesociety.org (accessed on 5 April 2017).
- DeLong, J.M.; Russell, R.P.; Mazzocca, A.D. Platelet-rich plasma: The PAW classification system. Arthrosc. J. Arthrosc. Relat. Surg. 2012, 28, 998–1009. [Google Scholar] [CrossRef] [PubMed]
- Maisel-Campbell, A.L.; Ismail, A.; Reynolds, K.A.; Poon, E.; Serrano, L.; Grushchak, S.; Farid, C.; West, D.P.; Alam, M. A systematic review of the safety and effectiveness of platelet-rich plasma (PRP) for skin aging. Arch. Derm. Res. 2020, 312, 301–315. [Google Scholar] [CrossRef]
- Corash, L.; Tan, H.; Gralnick, H.R. Heterogeneity of human whole blood platelet subpopulations. I. Relationship between buoyant density, cell volume, and ultrastructure. Blood 1977, 49, 71–87. [Google Scholar] [CrossRef]
- Oh, J.H.; Kim, W.; Park, K.U.; Roh, Y.H. Comparison of the Cellular Composition and Cytokine-Release Kinetics of Various Platelet-Rich Plasma Preparations. Am. J. Sports Med. 2015, 43, 3062–3070. [Google Scholar] [CrossRef]
- Degen, R.M.; Bernard, J.A.; Oliver, K.S.; Dines, J.S. Commercial Separation Systems Designed for Preparation of Platelet-Rich Plasma Yield Differences in Cellular Composition. HSS J. Musculoskelet. J. Hosp. Spec. Surg. 2017, 13, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Gorgu, M.; Gokkaya, A.; Dogan, A. Comparison of Two Anticoagulants for Pain Associated with Platelet-Rich Plasma Injections. Aesthetic Plast. Surg. 2020, 44, 955–961. [Google Scholar] [CrossRef] [PubMed]
- Bowen, R.A.; Remaley, A.T. Interferences from blood collection tube components on clinical chemistry assays. Biochem. Med. 2014, 24, 31–44. [Google Scholar] [CrossRef]
- Larsen, R.; Gouveia, Z.; Soares, M.P.; Gozzelino, R. Heme cytotoxicity and the pathogenesis of immune-mediated inflammatory diseases. Front. Pharm. 2012, 3, 77. [Google Scholar] [CrossRef]
- Boswell, S.G.; Cole, B.J.; Sundman, E.A.; Karas, V.; Fortier, L.A. Platelet-rich plasma: A milieu of bioactive factors. Arthroscopy 2012, 28, 429–439. [Google Scholar] [CrossRef] [PubMed]
- Brancato, S.K.; Albina, J.E. Wound macrophages as key regulators of repair: Origin, phenotype, and function. Am. J. Pathol 2011, 178, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Nishio, H.; Saita, Y.; Kobayashi, Y.; Takaku, T.; Fukusato, S.; Uchino, S.; Wakayama, T.; Ikeda, H.; Kaneko, K. Platelet-rich plasma promotes recruitment of macrophages in the process of tendon healing. Regen. Ther. 2020, 14, 262–270. [Google Scholar] [CrossRef]
- Yoshida, R.; Murray, M.M. Peripheral blood mononuclear cells enhance the anabolic effects of platelet-rich plasma on anterior cruciate ligament fibroblasts. J. Orthop. Res. Off. Publ. Orthop. Res. Soc. 2013, 31, 29–34. [Google Scholar] [CrossRef]
- Naldini, A.; Morena, E.; Fimiani, M.; Campoccia, G.; Fossombroni, V.; Carraro, F. The effects of autologous platelet gel on inflammatory cytokine response in human peripheral blood mononuclear cells. Platelets 2008, 19, 268–274. [Google Scholar] [CrossRef]
- Zhou, Y.; Zhang, J.; Wu, H.; Hogan, M.V.; Wang, J.H. The differential effects of leukocyte-containing and pure platelet-rich plasma (PRP) on tendon stem/progenitor cells—implications of PRP application for the clinical treatment of tendon injuries. Stem Cell Res. Ther. 2015, 6, 173. [Google Scholar] [CrossRef]
- Kim, J.H.; Park, Y.B.; Ha, C.W.; Roh, Y.J.; Park, J.G. Adverse Reactions and Clinical Outcomes for Leukocyte-Poor Versus Leukocyte-Rich Platelet-Rich Plasma in Knee Osteoarthritis: A Systematic Review and Meta-analysis. Orthop. J. Sports Med. 2021, 9, 23259671211011948. [Google Scholar] [CrossRef] [PubMed]
- Cavallo, C.; Filardo, G.; Mariani, E.; Kon, E.; Marcacci, M.; Pereira Ruiz, M.T.; Facchini, A.; Grigolo, B. Comparison of platelet-rich plasma formulations for cartilage healing: An in vitro study. J. Bone Jt. Surgery. Am. Vol. 2014, 96, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, J.; Bulsara, M.; Zheng, M.H. The Effectiveness of Platelet-Rich Plasma in the Treatment of Tendinopathy: A Meta-analysis of Randomized Controlled Clinical Trials. Am. J. Sports Med. 2017, 45, 226–233. [Google Scholar] [CrossRef]
- Dovi, J.V.; Szpaderska, A.M.; DiPietro, L.A. Neutrophil function in the healing wound: Adding insult to injury? Thromb Haemost 2004, 92, 275–280. [Google Scholar] [CrossRef] [PubMed]
- Graziani, F.; Ivanovski, S.; Cei, S.; Ducci, F.; Tonetti, M.; Gabriele, M. The in vitro effect of different PRP concentrations on osteoblasts and fibroblasts. Clin. Oral Implant. Res. 2006, 17, 212–219. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, R.; Cheng, M.; Murray, M.M. Increasing platelet concentration in platelet-rich plasma inhibits anterior cruciate ligament cell function in three-dimensional culture. J. Orthop. Res. Off. Publ. Orthop. Res. Soc. 2014, 32, 291–295. [Google Scholar] [CrossRef]
- Fleming, B.C.; Proffen, B.L.; Vavken, P.; Shalvoy, M.R.; Machan, J.T.; Murray, M.M. Increased platelet concentration does not improve functional graft healing in bio-enhanced ACL reconstruction. Knee Surg. Sports Traumatol. Arthrosc. Off. J. ESSKA 2015, 23, 1161–1170. [Google Scholar] [CrossRef]
- Filardo, G.; Kon, E.; Pereira Ruiz, M.T.; Vaccaro, F.; Guitaldi, R.; Di Martino, A.; Cenacchi, A.; Fornasari, P.M.; Marcacci, M. Platelet-rich plasma intra-articular injections for cartilage degeneration and osteoarthritis: Single- versus double-spinning approach. Knee Surg. Sports Traumatol. Arthrosc. Off. J. ESSKA 2012, 20, 2082–2091. [Google Scholar] [CrossRef]
- Rappl, L.M. Effect of platelet rich plasma gel in a physiologically relevant platelet concentration on wounds in persons with spinal cord injury. Int. Wound J. 2011, 8, 187–195. [Google Scholar] [CrossRef]
- Marx, R.E. Platelet-rich plasma (PRP): What is PRP and what is not PRP? Implant. Dent. 2001, 10, 225–228. [Google Scholar] [CrossRef]
- Ross, R.; Glomset, J.; Kariya, B.; Harker, L. A platelet-dependent serum factor that stimulates the proliferation of arterial smooth muscle cells in vitro. Proc. Natl. Acad. Sci. USA 1974, 71, 1207–1210. [Google Scholar] [CrossRef]
- Hersant, B.; SidAhmed-Mezi, M.; La Padula, S.; Niddam, J.; Bouhassira, J.; Meningaud, J.P. Efficacy of Autologous Platelet-rich Plasma Glue in Weight Loss Sequelae Surgery and Breast Reduction: A Prospective Study. Plast. Reconstr. Surg. Glob. Open 2016, 4, e871. [Google Scholar] [CrossRef] [PubMed]
- Gumina, S.; Campagna, V.; Ferrazza, G.; Giannicola, G.; Fratalocchi, F.; Milani, A.; Postacchini, F. Use of platelet-leukocyte membrane in arthroscopic repair of large rotator cuff tears: A prospective randomized study. J. Bone Jt. Surg. Am. 2012, 94, 1345–1352. [Google Scholar] [CrossRef] [PubMed]
- Hu, Z.; Qu, S.; Zhang, J.; Cao, X.; Wang, P.; Huang, S.; Shi, F.; Dong, Y.; Wu, J.; Tang, B.; et al. Efficacy and Safety of Platelet-Rich Plasma for Patients with Diabetic Ulcers: A Systematic Review and Meta-analysis. Adv. Wound Care 2019, 8, 298–308. [Google Scholar] [CrossRef] [PubMed]
- Neuman, M.G.; Nanau, R.M.; Oruna-Sanchez, L.; Coto, G. Hyaluronic acid and wound healing. J. Pharm. Pharm. Sci. A Publ. Can. Soc. Pharm. Sci. Soc. Can. Des Sci. Pharm. 2015, 18, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Abatangelo, G.; Vindigni, V.; Avruscio, G.; Pandis, L.; Brun, P. Hyaluronic Acid: Redefining Its Role. Cells 2020, 9, 1743. [Google Scholar] [CrossRef] [PubMed]
- Litwiniuk, M.; Krejner, A.; Speyrer, M.S.; Gauto, A.R.; Grzela, T. Hyaluronic Acid in Inflammation and Tissue Regeneration. Wounds A Compend. Clin. Res. Pract. 2016, 28, 78–88. [Google Scholar]
- Lierova, A.; Kasparova, J.; Filipova, A.; Cizkova, J.; Pekarova, L.; Korecka, L.; Mannova, N.; Bilkova, Z.; Sinkorova, Z. Hyaluronic Acid: Known for Almost a Century, but Still in Vogue. Pharmaceutics 2022, 14, 838. [Google Scholar] [CrossRef] [PubMed]
- Ding, Y.W.; Wang, Z.Y.; Ren, Z.W.; Zhang, X.W.; Wei, D.X. Advances in modified hyaluronic acid-based hydrogels for skin wound healing. Biomater. Sci. 2022, 10, 3393–3409. [Google Scholar] [CrossRef]
- Juncan, A.M.; Moisa, D.G.; Santini, A.; Morgovan, C.; Rus, L.L.; Vonica-Tincu, A.L.; Loghin, F. Advantages of Hyaluronic Acid and Its Combination with Other Bioactive Ingredients in Cosmeceuticals. Molecules 2021, 26, 4429. [Google Scholar] [CrossRef] [PubMed]
- Dovedytis, M.L.; Liu, Z.J.; Bartlett, S. Hyaluronic acid and its biomedical applications: A review. Eng. Regen. 2020, 1, 102–113. [Google Scholar] [CrossRef]
- Vilchez-Cavazos, F.; Blazquez-Saldana, J.; Gamboa-Alonso, A.A.; Pena-Martinez, V.M.; Acosta-Olivo, C.A.; Sanchez-Garcia, A.; Simental-Mendia, M. The use of platelet-rich plasma in studies with early knee osteoarthritis versus advanced stages of the disease: A systematic review and meta-analysis of 31 randomized clinical trials. Arch. Orthop. Trauma. Surg. 2022, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Abbas, A.; Du, J.T.; Dhotar, H.S. The Effect of Leukocyte Concentration on Platelet-Rich Plasma Injections for Knee Osteoarthritis: A Network Meta-Analysis. J. Bone Jt. Surg. 2021, 104, 559–570. [Google Scholar] [CrossRef] [PubMed]
- Hong, M.; Cheng, C.; Sun, X.; Yan, Y.; Zhang, Q.; Wang, W.; Guo, W. Efficacy and Safety of Intra-Articular Platelet-Rich Plasma in Osteoarthritis Knee: A Systematic Review and Meta-Analysis. BioMed Res. Int. 2021, 2021, 2191926. [Google Scholar] [CrossRef] [PubMed]
- Abate, M.; Verna, S.; Schiavone, C.; Di Gregorio, P.; Salini, V. Efficacy and safety profile of a compound composed of platelet-rich plasma and hyaluronic acid in the treatment for knee osteoarthritis (preliminary results). Eur. J. Orthop. Surg. Traumatol. Orthop. Traumatol. 2015, 25, 1321–1326. [Google Scholar] [CrossRef]
- Abbassy, A.A.; Trebinjac, S.; Kotb, N. The use of cellular matrix in symptomatic knee osteoarthritis. Bosn. J. Basic Med. Sci. 2020, 20, 271–274. [Google Scholar] [CrossRef]
- Adam, P.; Renevier, J.L.; Marc, J.F. A novel treatment of knee degenerative disorders all-in-one intra-articular injection of platelet-rich plasma combined with hyaluronic acid. Int. J. Clin. Rheumatol. 2018, 13, 280–288. [Google Scholar] [CrossRef]
- Barac, B.; Damjanov, N.; Zekovic, A. The new treatment approach in knee osteoarthritis: Efficacy of cellular matrix combination of platelet rich plasma with hyaluronic acid versus two different types of hyaluronic acid (HA). Int. J. Clin. Rheumatol. 2018, 13, 289–295. [Google Scholar] [CrossRef]
- Dallo, I.; Szwedowski, D.; Mobasheri, A.; Irlandini, E.; Gobbi, A. A Prospective Study Comparing Leukocyte-Poor Platelet-Rich Plasma Combined with Hyaluronic Acid and Autologous Microfragmented Adipose Tissue in Patients with Early Knee Osteoarthritis. Stem Cells Dev. 2021, 30, 651–659. [Google Scholar] [CrossRef]
- Landro, M.E.; Daffunchio, C.; Cambiaggi, G.; Galatro, G.; Caviglia, H. Platelet-rich plasma vs platelet-rich plasma plus hyaluronic acid for haemophilic knee arthropathy treatment. Acta Orthop. Belg. 2021, 87, 705–712. [Google Scholar] [CrossRef]
- Łęgosz, P.; Sarzyńska, S.; Stępiński, P.; Pulik, Ł.; Niewczas, P.; Kotela, A.; Gołębiewski, M.; Małdyk, P. Early term results of usage combined hyaluronic acid and platelet rich plasma in knee osteoarthritis. Chir. Narz. Ruchu Ortop. Pol. 2017, 82, 151–159. [Google Scholar]
- Palco, M.; Fenga, D.; Basile, G.C.; Rizzo, P.; Cavalieri, B.; Leonetti, D.; Alito, A.; Bruschetta, A.; Traina, F. Platelet-Rich Plasma Combined with Hyaluronic Acid versus Leucocyte and Platelet-Rich Plasma in the Conservative Treatment of Knee Osteoarthritis. A Retrospective Study. Medicina 2021, 57, 232. [Google Scholar] [CrossRef] [PubMed]
- Palco, M.; Rizzo, P.; Basile, G.C.; Alito, A.; Bruschetta, D.; Accorinti, M.; Restuccia, R.; Leonetti, D. Short- and Midterm Comparison of Platelet-Rich Plasma with Hyaluronic Acid versus Leucocyte and Platelet-Rich Plasma on Pain and Function to Treat Hip Osteoarthritis. A Retrospective Study. Gels 2021, 7, 222. [Google Scholar] [CrossRef] [PubMed]
- Renevier, J.L.; Marc, J.F.; Adam, P.; Sans, N.; Le Coz, J.; Prothoy, I. “Cellular matrix™ PRP-HA”: A new treatment option with platelet-rich plasma and hyaluronic acid for patients with osteoarthritis having had an unsatisfactory clinical response to hyaluronic acid alone: Results of a pilot, multicenter French study with long-term follow-up. Int. J. Clin. Rheumatol. 2018, 13, 230–238. [Google Scholar]
- Rizzo, L. Platelet-Rich Plasma (PRP) in the Treatment of Knee Osteoarthritis. J. Regen. Med. 2019, 8. [Google Scholar] [CrossRef]
- Seleem, N.A.; Elshereef, E.; Elhosary, A.A.; Salama, N.M. Intra-Articular Injections of Platelet-Rich Plasma Combined with Hyaluronic Acid Versus Hyaluronic Acid Alone in Treatment of Knee Osteoarthritis. EJPMR 2017, 4, 608–615. [Google Scholar]
- Van Tiel, J.; Reijman, M.; Bos, P.K.; Hermans, J.; van Buul, G.M.; Bron, E.E.; Klein, S.; Verhaar, J.A.; Krestin, G.P.; Bierma-Zeinstra, S.M.; et al. Delayed gadolinium-enhanced MRI of cartilage (dGEMRIC) shows no change in cartilage structural composition after viscosupplementation in patients with early-stage knee osteoarthritis. PLoS ONE 2013, 8, e79785. [Google Scholar] [CrossRef]
- Ahmad, H.S.; Farrag, S.E.; Okasha, A.E.; Kadry, A.O.; Ata, T.B.; Monir, A.A.; Shady, I. Clinical outcomes are associated with changes in ultrasonographic structural appearance after platelet-rich plasma treatment for knee osteoarthritis. Int. J. Rheum. Dis. 2018, 21, 960–966. [Google Scholar] [CrossRef]
- Buendia-Lopez, D.; Medina-Quiros, M.; Fernandez-Villacanas Marin, M.A. Clinical and radiographic comparison of a single LP-PRP injection, a single hyaluronic acid injection and daily NSAID administration with a 52-week follow-up: A randomized controlled trial. J. Orthop. Traumatol. 2018, 19, 3. [Google Scholar] [CrossRef] [PubMed]
- Halpern, B.; Chaudhury, S.; Rodeo, S.A.; Hayter, C.; Bogner, E.; Potter, H.G.; Nguyen, J. Clinical and MRI outcomes after platelet-rich plasma treatment for knee osteoarthritis. Clin. J. Sport Med. Off. J. Can. Acad. Sport Med. 2013, 23, 238–239. [Google Scholar] [CrossRef]
- Hart, R.; Safi, A.; Komzak, M.; Jajtner, P.; Puskeiler, M.; Hartova, P. Platelet-rich plasma in patients with tibiofemoral cartilage degeneration. Arch. Orthop. Trauma Surg. 2013, 133, 1295–1301. [Google Scholar] [CrossRef]
- Raeissadat, S.A.; Ghorbani, E.; Sanei Taheri, M.; Soleimani, R.; Rayegani, S.M.; Babaee, M.; Payami, S. MRI changes after platelet rich plasma injection in knee osteoarthritis (randomized clinical trial). J. Pain Res. 2020, 13, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Raeissadat, S.A.; Karimzadeh, A.; Hashemi, M.; Bagherzadeh, L. Safety and efficacy of platelet-rich plasma in treatment of carpal tunnel syndrome; a randomized controlled trial. BMC Musculoskelet. Disord. 2018, 19, 49. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Hall, S.; Hanna, F.; Wluka, A.E.; Grant, G.; Marks, P.; Feletar, M.; Cicuttini, F.M. Effects of Hylan G-F 20 supplementation on cartilage preservation detected by magnetic resonance imaging in osteoarthritis of the knee: A two-year single-blind clinical trial. BMC Musculoskelet. Disord. 2011, 12, 195. [Google Scholar] [CrossRef]
- Chen, W.H.; Lo, W.C.; Hsu, W.C.; Wei, H.J.; Liu, H.Y.; Lee, C.H.; Tina Chen, S.Y.; Shieh, Y.H.; Williams, D.F.; Deng, W.P. Synergistic anabolic actions of hyaluronic acid and platelet-rich plasma on cartilage regeneration in osteoarthritis therapy. Biomaterials 2014, 35, 9599–9607. [Google Scholar] [CrossRef]
- Sun, S.F.; Lin, G.C.; Hsu, C.W.; Lin, H.S.; Liou, I.S.; Wu, S.Y. Comparing efficacy of intraarticular single crosslinked Hyaluronan (HYAJOINT Plus) and platelet-rich plasma (PRP) versus PRP alone for treating knee osteoarthritis. Sci. Rep. 2021, 11, 140. [Google Scholar] [CrossRef]
- Karasavvidis, T.; Totlis, T.; Gilat, R.; Cole, B.J. Platelet-Rich Plasma Combined With Hyaluronic Acid Improves Pain and Function Compared With Hyaluronic Acid Alone in Knee Osteoarthritis: A Systematic Review and Meta-analysis. Arthrosc. J. Arthrosc. Relat. Surg. Off. Publ. Arthrosc. Assoc. N. Am. Int. Arthrosc. Assoc. 2021, 37, 1277–1287.e1. [Google Scholar] [CrossRef] [PubMed]
- Hersant, B.; SidAhmed-Mezi, M.; Niddam, J.; La Padula, S.; Noel, W.; Ezzedine, K.; Rodriguez, A.M.; Meningaud, J.P. Efficacy of autologous platelet-rich plasma combined with hyaluronic acid on skin facial rejuvenation: A prospective study. J. Am. Acad. Dermatol. 2017, 77, 584–586. [Google Scholar] [CrossRef] [PubMed]
- Pirrello, R.; Verro, B.; Grasso, G.; Ruscitti, P.; Cordova, A.; Giacomelli, R.; Ciccia, F.; Guggino, G. Hyaluronic acid and platelet-rich plasma, a new therapeutic alternative for scleroderma patients: A prospective open-label study. Arthritis Res. Ther. 2019, 21, 286. [Google Scholar] [CrossRef]
- Hersant, B.; SidAhmed-Mezi, M.; Aboud, C.; Niddam, J.; Levy, S.; Mernier, T.; La Padula, S.; Meningaud, J.P. Synergistic Effects of Autologous Platelet-Rich Plasma and Hyaluronic Acid Injections on Facial Skin Rejuvenation. Aesthet. Surg. J. 2021, 41, NP854–NP865. [Google Scholar] [CrossRef]
- Edwards, P.C.; Fantasia, J.E. Review of long-term adverse effects associated with the use of chemically-modified animal and nonanimal source hyaluronic acid dermal fillers. Clin. Interv. Aging 2007, 2, 509–519. [Google Scholar] [CrossRef]
- Anitua, E.; Sanchez, M.; Nurden, A.T.; Zalduendo, M.M.; de la Fuente, M.; Azofra, J.; Andia, I. Platelet-released growth factors enhance the secretion of hyaluronic acid and induce hepatocyte growth factor production by synovial fibroblasts from arthritic patients. Rheumatology 2007, 46, 1769–1772. [Google Scholar] [CrossRef] [PubMed]
- Cervelli, V.; De Angelis, B.; Lucarini, L.; Spallone, D.; Balzani, A.; Palla, L.; Gentile, P.; Cerulli, P. Tissue regeneration in loss of substance on the lower limbs through use of platelet-rich plasma, stem cells from adipose tissue, and hyaluronic acid. Adv. Ski. Wound Care 2010, 23, 262–272. [Google Scholar] [CrossRef]
- Iio, K.; Furukawa, K.I.; Tsuda, E.; Yamamoto, Y.; Maeda, S.; Naraoka, T.; Kimura, Y.; Ishibashi, Y. Hyaluronic acid induces the release of growth factors from platelet-rich plasma. Asia-Pac. J. Sports Med. Arthrosc. Rehabil. Technol. 2016, 4, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.D.; Melhem, M.E.; Magge, K.T.; Waggoner, A.S.; Campbell, P.G. Improved growth factor directed vascularization into fibrin constructs through inclusion of additional extracellular molecules. Microvasc. Res. 2007, 73, 84–94. [Google Scholar] [CrossRef] [PubMed]
- Atashi, F.; Jaconi, M.E.; Pittet-Cuenod, B.; Modarressi, A. Autologous platelet-rich plasma: A biological supplement to enhance adipose-derived mesenchymal stem cell expansion. Tissue Eng. Part C Methods 2015, 21, 253–262. [Google Scholar] [CrossRef]
- Berndt, S.; Turzi, A.; Modarressi, A. Production of Autologous Platelet-Rich Plasma for Boosting In Vitro Human Fibroblast Expansion. J. Vis. Exp. JoVE 2021, e60816. [Google Scholar] [CrossRef] [PubMed]
- Berndt, S.; Turzi, A.; Pittet-Cuenod, B.; Modarressi, A. Autologous Platelet-Rich Plasma (CuteCell PRP) Safely Boosts In Vitro Human Fibroblast Expansion. Tissue Eng. Part A 2019, 25, 1550–1563. [Google Scholar] [CrossRef] [PubMed]
- Anitua, E.; Zalduendo, M.; Troya, M.; Alkhraisat, M.H.; Blanco-Antona, L.A. Platelet-Rich Plasma as an Alternative to Xenogeneic Sera in Cell-Based Therapies: A Need for Standardization. Int. J. Mol. Sci. 2022, 23, 6552. [Google Scholar] [CrossRef] [PubMed]
- Luzo, A.C.M.; Favaro, W.J.; Seabra, A.B.; Duran, N. What is the potential use of platelet-rich-plasma (PRP) in cancer treatment? A mini review. Heliyon 2020, 6, e03660. [Google Scholar] [CrossRef]
- Berndt, S.; Carpentier, G.; Turzi, A.; Borlat, F.; Cuendet, M.; Modarressi, A. Angiogenesis Is Differentially Modulated by Platelet-Derived Products. Biomedicines 2021, 9, 251. [Google Scholar] [CrossRef]
- Nowak-Sliwinska, P.; Alitalo, K.; Allen, E.; Anisimov, A.; Aplin, A.C.; Auerbach, R.; Augustin, H.G.; Bates, D.O.; van Beijnum, J.R.; Bender, R.H.F.; et al. Consensus guidelines for the use and interpretation of angiogenesis assays. Angiogenesis 2018, 21, 425–532. [Google Scholar] [CrossRef] [PubMed]
- Carpentier, G.; Berndt, S.; Ferratge, S.; Rasband, W.; Cuendet, M.; Uzan, G.; Albanese, P. Angiogenesis Analyzer for ImageJ—A comparative morphometric analysis of “Endothelial Tube Formation Assay” and “Fibrin Bead Assay”. Sci. Rep. 2020, 10, 11568. [Google Scholar] [CrossRef] [PubMed]
- Schneider, C.A.; Rasband, W.S.; Eliceiri, K.W. NIH Image to ImageJ: 25 years of image analysis. Nat. Methods 2012, 9, 671–675. [Google Scholar] [CrossRef] [PubMed]
- Heng, B.C.; Bezerra, P.P.; Preiser, P.R.; Law, S.K.; Xia, Y.; Boey, F.; Venkatraman, S.S. Effect of cell-seeding density on the proliferation and gene expression profile of human umbilical vein endothelial cells within ex vivo culture. Cytotherapy 2011, 13, 606–617. [Google Scholar] [CrossRef] [PubMed]
- Dimri, G.P.; Lee, X.; Basile, G.; Acosta, M.; Scott, G.; Roskelley, C.; Medrano, E.E.; Linskens, M.; Rubelj, I.; Pereira-Smith, O.; et al. A biomarker that identifies senescent human cells in culture and in aging skin in vivo. Proc. Natl. Acad. Sci. USA 1995, 92, 9363–9367. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Technology | Examples of Devices | Blood Vol. | PRP Vol. | Platelet Conc. Factor | Biological Product | Remarks |
|---|---|---|---|---|---|---|
| Low force centrifugation in tubes or syringes | BTI PRGF Endoret | 8 mL | 1–2 mL | 2–3× | Plasma PRP (LP-PRP) | Devices with no physical separation of platelet rich plasma from red and white blood cells. Operator dependent results |
| Arthrex ACP double syringe | 15 mL | 4–6 mL | 1.6–2× | |||
| High force centrifugation in hourglass shaped devices | Tozai Holdings Prosys | 25 mL | 2 mL | 6–8× | Buffy coat PRP (LR-PRP) | |
| High force centrifugation in devices with floating buoy or shelf | Biomet GPS III | 27–54 mL | 3–6 mL | 6–9× | Buffy coat PRP (LR-PRP) | Devices with physical separation of platelet rich plasma from red and white blood cells. Device dependent results |
| Harvest SmartPrep2 | 27–54 mL | 3–7 mL | 3–8× | |||
| Variable force centrifugation in computer aided systems | Arthrex Angel | 40–180 mL | variable | 1–18× | Setting dependent product | |
| Arteriocyte Magellan | 26–52 mL | 6 mL | 3–7× | |||
| High force centrifugation in tubes with separating gel | RegenTubes | 10 mL | 5–6 mL Can be reduced to 1.5 mL | 1.6–1.7× Up to 4× by PPP removal | Plasma PRP (LP-PRP) |
| Herapeutical Domain | Pathologies | Studies | Treated Patients |
|---|---|---|---|
| Sports medicine | Osteoarthritis and other cartilage pathologies | 37 | 2053 |
| Tendinopathies | 15 | 596 | |
| Muscle | 3 | 18 | |
| Carpal tunnel | 6 | 215 | |
| Orthopedic surgery | Bone reconstruction, cartilage and tendon surgery | 16 | 649 |
| Spine surgery | 3 | 46 | |
| Dermatology | Skin care | 14 | 353 |
| Alopecia | 10 | 240 | |
| Chronic wounds | 12 | 238 | |
| Plastic and reconstructive surgery | 7 | 178 | |
| Cardiovascular surgery wounds | 3 | 425 | |
| Urology | 4 | 122 | |
| Gynecology | 8 | 105 | |
| Penile disfunction | 3 | 151 | |
| Fertility | 3 | 67 | |
| Ophthalmology | 10 | 170 | |
| Otorhinolaryngology | 7 | 103 | |
| Dental/maxillofacial surgery | 7 | 200 | |
| Total | 168 | 5929 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gomri, F.; Vischer, S.; Turzi, A.; Berndt, S. Swiss Medical Devices for Autologous Regenerative Medicine: From Innovation to Clinical Validation. Pharmaceutics 2022, 14, 1617. https://doi.org/10.3390/pharmaceutics14081617
Gomri F, Vischer S, Turzi A, Berndt S. Swiss Medical Devices for Autologous Regenerative Medicine: From Innovation to Clinical Validation. Pharmaceutics. 2022; 14(8):1617. https://doi.org/10.3390/pharmaceutics14081617
Chicago/Turabian StyleGomri, Farid, Solange Vischer, Antoine Turzi, and Sarah Berndt. 2022. "Swiss Medical Devices for Autologous Regenerative Medicine: From Innovation to Clinical Validation" Pharmaceutics 14, no. 8: 1617. https://doi.org/10.3390/pharmaceutics14081617