
Pharmacokinetics of Bupivacaine Following Administration by an Ultrasound-Guided Transversus Abdominis Plane Block in Cats Undergoing Ovariohysterectomy

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Pharmacokinetic Study
2.1.1. Animals
2.1.2. Experimental Design and Treatment Groups
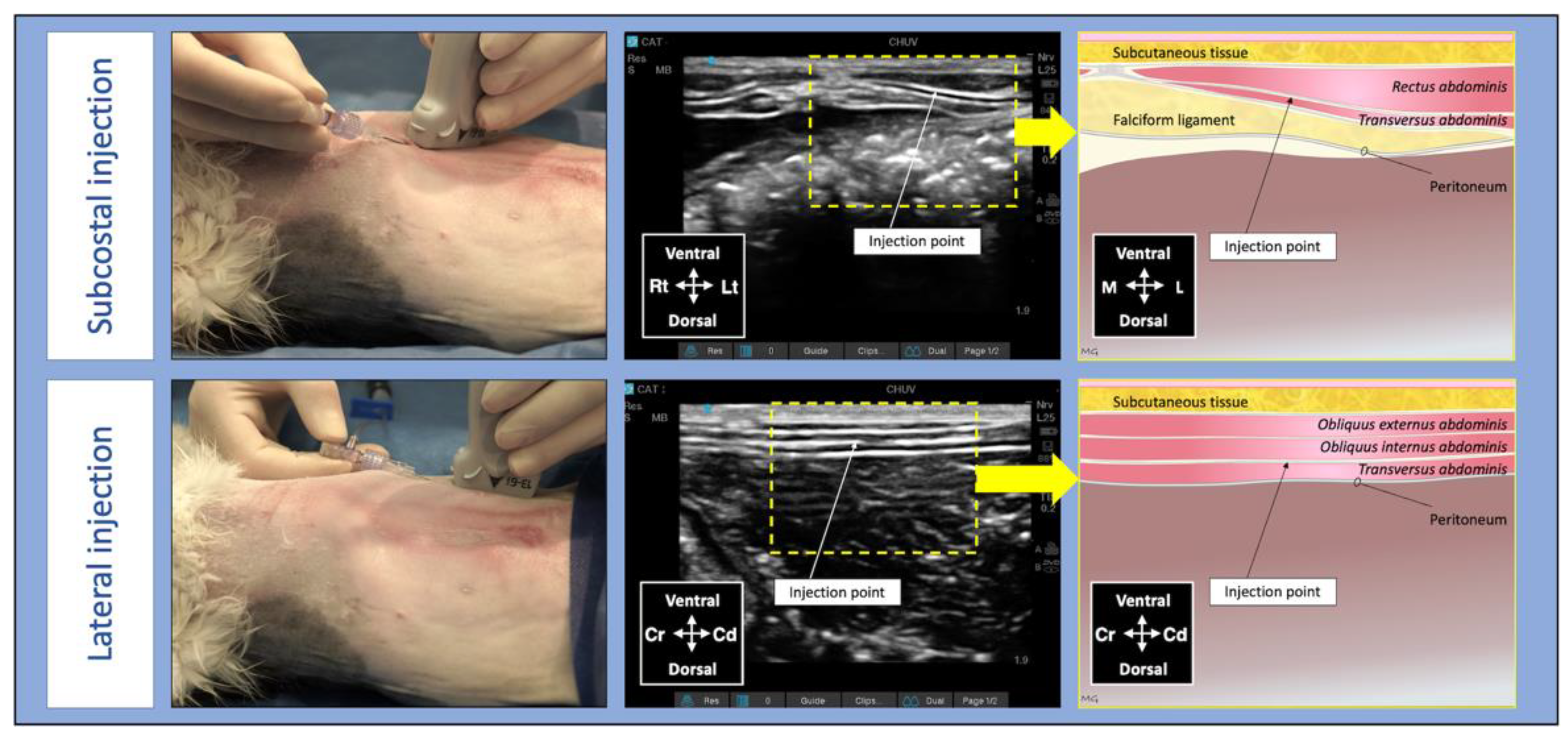
2.1.3. Anaesthesia and Surgery
2.2. Blood Sampling
2.3. Bupivacaine Analysis and Pharmacokinetics
2.4. Statistical Analysis
3. Results
3.1. Animals and Procedures
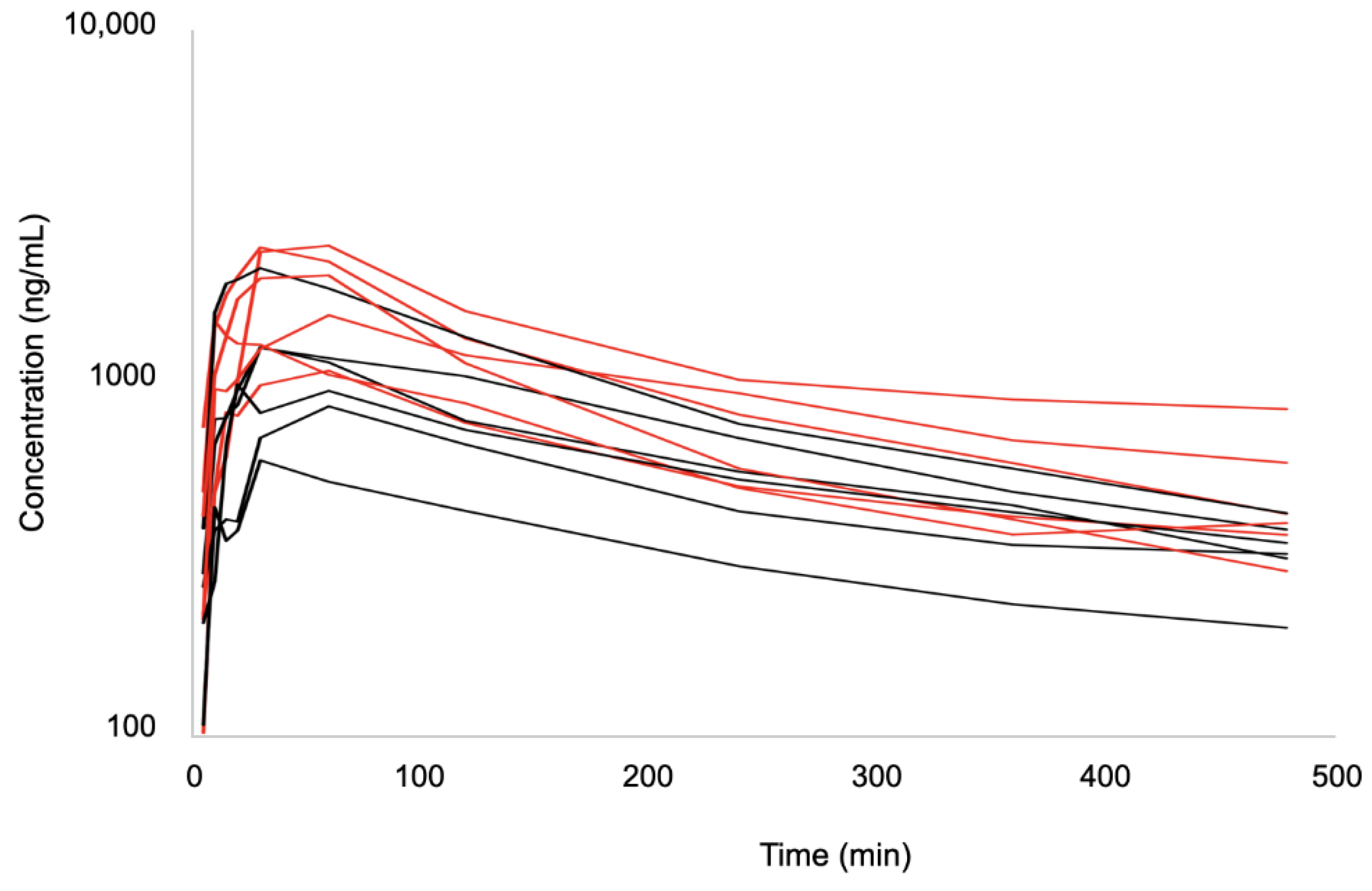
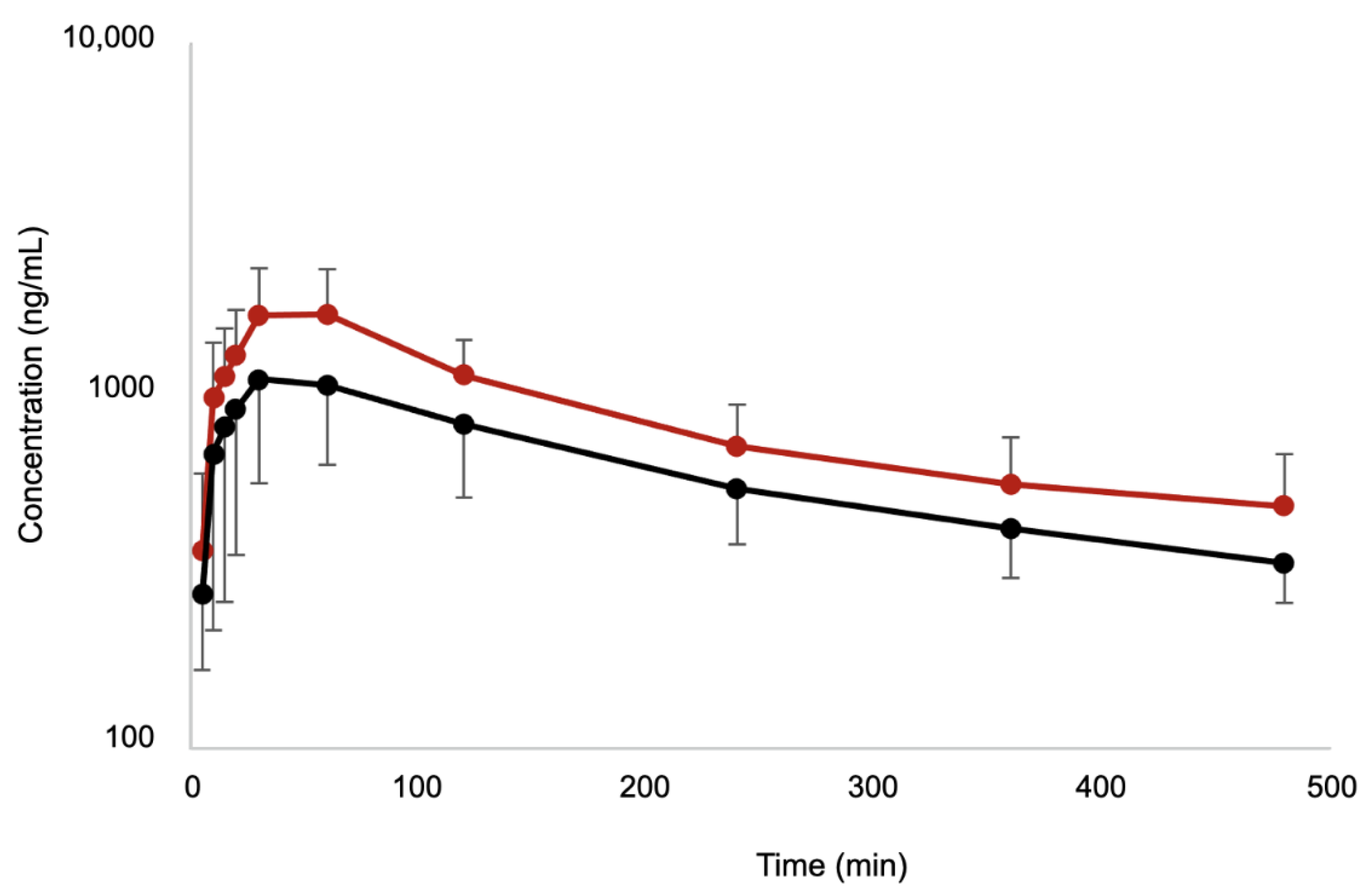
3.2. Pharmacokinetic Study
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Portela, D.A.; Romano, M.; Briganti, A. Retrospective clinical evaluation of ultrasound guided transverse abdominis plane block in dogs undergoing mastectomy. Vet. Anaesth. Analg. 2014, 41, 319–324. [Google Scholar] [CrossRef] [PubMed]
- Tsai, H.C.; Yoshida, T.; Chuang, T.Y.; Yang, S.F.; Chang, C.C.; Yao, H.Y.; Tai, Y.T.; Lin, J.A.; Chen, K.Y. Transversus Abdominis Plane Block: An Updated Review of Anatomy and Techniques. Biomed. Res. Int. 2017, 2017, 8284363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teixeira, L.G.; Pujol, D.M.; Pazzim, A.F.; Souza, R.P.; Fadel, L. Combination of Transversus abdominis plane block and Serratus plane block anesthesia in dogs submitted to masctetomy. Pesqui. Vet. Bras. 2018, 38, 315–319. [Google Scholar] [CrossRef] [Green Version]
- Skouropoulou, D.; Lacitignola, L.; Centonze, P.; Simone, A.; Crovace, A.M.; Staffieri, F. Perioperative analgesic effects of an ultrasound-guided transversus abdominis plane block with a mixture of bupivacaine and lidocaine in cats undergoing ovariectomy. Vet. Anaesth. Analg. 2018, 45, 374–383. [Google Scholar] [CrossRef] [PubMed]
- Otero, P.E.; Romano, M.; Zaccagnini, A.S.; Fuensalida, S.E.; Verdier, N.; Sanchez, F.; Portela, D.A. Transversus abdominis plane block in cat cadavers: Anatomical description and comparison of injectate spread using two- and three-point approaches. Vet. Anaesth. Analg. 2021, 48, 432–441. [Google Scholar] [CrossRef] [PubMed]
- Uppal, V.; Sancheti, S.; Kalagara, H. Transversus Abdominis Plane (TAP) and Rectus Sheath Blocks: A Technical Description and Evidence Review. Curr. Anesthesiol. Rep. 2019, 9, 479–487. [Google Scholar] [CrossRef] [Green Version]
- Garbin, M.M.S.; Finck, C.; Steagall, P.V. Distribution of injectate spread using two approaches for an ultrasound-guided transversus abdominis plane block in cats: A cadaver and computed tomography study. In Proceedings of the AVA Spring Meeting 2022, Napflio, Greece, 20 May 2022. [Google Scholar]
- Griffiths, J.D.; Barron, F.A.; Grant, S.; Bjorksten, A.R.; Hebbard, P.; Royse, C.F. Plasma ropivacaine concentrations after ultrasound-guided transversus abdominis plane block. Br. J. Anaesth 2010, 105, 853–856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torup, H.; Mitchell, A.U.; Breindahl, T.; Hansen, E.G.; Rosenberg, J.; Moller, A.M. Potentially toxic concentrations in blood of total ropivacaine after bilateral transversus abdominis plane blocks; a pharmacokinetic study. Eur. J. Anaesthesiol. 2012, 29, 235–238. [Google Scholar] [CrossRef]
- Lemke, K.A.; Dawson, S.D. Local and regional anesthesia. Vet. Clin. N. Am. Small Anim. Pract. 2000, 30, 839–857. [Google Scholar] [CrossRef]
- Chadwick, H.S. Toxicity and resuscitation in lidocaine- or bupivacaine-infused cats. Anesthesiology 1985, 63, 385–390. [Google Scholar] [CrossRef]
- Kasaba, T.; Shiraishi, S.; Taniguchi, M.; Takasaki, M. Bupivacaine-induced convulsion is suppressed by MK-801. Region. Anesth. Pain M 1998, 23, 71–76. [Google Scholar] [CrossRef]
- Romano, M.; Portela, D.A.; Thomson, A.; Otero, P.E. Comparison between two approaches for the transversus abdominis plane block in canine cadavers. Vet. Anaesth. Analg. 2021, 48, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.P.; Rekers, W.; Ellis, K.; Ellingsen, K.; Milovancev, M. Pedicle ties provide a rapid and safe method for feline ovariohysterectomy. J. Feline Med. Surg. 2016, 18, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Benito, J.; Monteiro, B.P.; Beaudry, F.; Lavoie, A.M.; Lascelles, B.D.; Steagall, P.V. Pharmacokinetics of bupivacaine after intraperitoneal administration to cats undergoing ovariohysterectomy. Am. J. Vet. Res. 2016, 77, 641–645. [Google Scholar] [CrossRef] [PubMed]
- Benito, J.; Monteiro, B.; Beaudry, F.; Steagall, P. Efficacy and pharmacokinetics of bupivacaine with epinephrine or dexmedetomidine after intraperitoneal administration in cats undergoing ovariohysterectomy. Can. J. Vet. Res. 2018, 82, 124–130. [Google Scholar] [PubMed]
- Gaudette, F.; Benito, J.; Steagall, P.; Beaudry, F. Assessment of tandem mass spectrometry and high-resolution mass spectrometry for the analysis of bupivacaine in plasma. Biomed. Chromatogr. 2015, 29, 1724–1730. [Google Scholar] [CrossRef] [Green Version]
- Grubb, T.; Sager, J.; Gaynor, J.S.; Montgomery, E.; Parker, J.A.; Shafford, H.; Tearney, C. 2020 AAHA Anesthesia and Monitoring Guidelines for Dogs and Cats. J. Am. Anim Hosp. Assoc. 2020, 56, 59–82. [Google Scholar] [CrossRef]
- de Jong, R.H.; Ronfeld, R.A.; DeRosa, R.A. Cardiovascular effects of convulsant and supraconvulsant doses of amide local anesthetics. Anesth. Analg. 1982, 61, 3–9. [Google Scholar] [CrossRef]
- Mathews, K.; Kronen, P.W.; Lascelles, D.; Nolan, A.; Robertson, S.; Steagall, P.V.; Wright, B.; Yamashita, K. Guidelines for recognition, assessment and treatment of pain: WSAVA Global Pain Council members and co-authors of this document. J. Small Anim. Pract. 2014, 55, E10–E68. [Google Scholar] [CrossRef]
- Cassuto, J.; Sinclair, R.; Bonderovic, M. Anti-inflammatory properties of local anesthetics and their present and potential clinical implications. Acta Anaesthesiol. Scand. 2006, 50, 265–282. [Google Scholar] [CrossRef]
- Hollmann, M.W.; Durieux, M.E. Local anesthetics and the inflammatory response: A new therapeutic indication? Anesthesiology 2000, 93, 858–875. [Google Scholar] [CrossRef] [PubMed]
- Suresh, S.; Taylor, L.J.; De Oliveira, G.S., Jr. Dose effect of local anesthetics on analgesic outcomes for the transversus abdominis plane (TAP) block in children: A randomized, double-blinded, clinical trial. Paediatr. Anaesth. 2015, 25, 506–510. [Google Scholar] [CrossRef]
- Becker, D.E.; Reed, K.L. Essentials of local anesthetic pharmacology. Anesth. Prog. 2006, 53, 98–108; quiz 109–110. [Google Scholar] [CrossRef]
- Wildsmith, J.A.; Tucker, G.T.; Cooper, S.; Scott, D.B.; Covino, B.G. Plasma concentrations of local anaesthetics after interscalene brachial plexus block. Br. J. Anaesth 1977, 49, 461–466. [Google Scholar] [CrossRef] [Green Version]
- Shilo-Benjamini, Y.; Pypendop, B.H.; Newbold, G.; Pascoe, P.J. Plasma bupivacaine concentrations following orbital injections in cats. Vet. Anaesth. Analg. 2017, 44, 178–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variables | Population n = 12 | BUPI-2 n = 6 | BUPI-2.5 n = 6 | p-Value |
|---|---|---|---|---|
| Body weight (kg) | 3.68 ± 0.68 | 3.61 ± 0.69 | 3.75 ± 0.72 | p = 0.74 |
| BCS (1 to 9) | 4 ± 1 | 4 ± 1 | 4 ± 1 | p = 1.00 |
| Haematocrit before (%) * | 42.9 ± 4.7 | 43.0 ± 4.9 | 42.8 ± 4.9 | p = 0.95 |
| Haematocrit after (%) * | 35.9 ± 4.4 | 34.7 ± 5.5 | 37.1 ± 3.1 | p = 0.36 |
| Total protein before (g/L) * | 65.3 ± 6.00 | 62.3 ± 5.3 | 68.3 ± 5.3 | p = 0.08 |
| Total protein after (g/L) * | 58.3 ± 6.1 | 57.5 ± 8.1 | 58.2 ± 3.8 | p = 0.86 |
| Dose of propofol (mg/kg) | 4.9 ± 0.7 | 4.8 ± 0.7 | 4.9 ± 0.8 | p = 0.79 |
| Duration of anaesthesia (min) | 38.9 ± 8.1 | 39.0 ± 9.5 | 38.8 ± 7.3 | p = 0.97 |
| Duration of surgery (min) | 17.6 ± 5.4 | 17.8 ± 7.5 | 17.3 ± 3.0 | p = 0.89 |
| Time to extubation (min) | 3.25 ± 1.86 | 2.50 ± 1.05 | 4.00 ± 2.28 | p = 0.19 |
| Parameters | Units |
BUPI-2 n = 6 |
BUPI-2.5 n = 6 | p-Value |
|---|---|---|---|---|
| Cmax | ng/mL | 1166 ± 511 | 1810 ± 536 | p = 0.06 |
| Tmax | min | 33 ± 14 | 47 ± 22 | p = 0.22 |
| CL/F | mL/min/kg | 5.3 ± 1.8 | 4.9 ± 1.5 | p = 0.68 |
| T1/2 | min | 253 ± 55 | 217 ± 52 | p = 0.27 |
| AUC0-last | Min·µg/mL | 297 ± 104 | 418 ± 115 | p = 0.09 |
| AUMC0-last | min·min·µg/mL | 56,214 ± 16,681 | 77,141 ± 24,478 | p = 0.12 |
| MRT0-last | min | 192 ± 11 | 184 ± 18 | p = 0.38 |
| C480 | ng/mL | 335 ± 76 | 485 ± 198 | p = 0.13 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garbin, M.; Benito, J.; Ruel, H.L.M.; Watanabe, R.; Monteiro, B.P.; Cagnardi, P.; Steagall, P.V. Pharmacokinetics of Bupivacaine Following Administration by an Ultrasound-Guided Transversus Abdominis Plane Block in Cats Undergoing Ovariohysterectomy. Pharmaceutics 2022, 14, 1548. https://doi.org/10.3390/pharmaceutics14081548
Garbin M, Benito J, Ruel HLM, Watanabe R, Monteiro BP, Cagnardi P, Steagall PV. Pharmacokinetics of Bupivacaine Following Administration by an Ultrasound-Guided Transversus Abdominis Plane Block in Cats Undergoing Ovariohysterectomy. Pharmaceutics. 2022; 14(8):1548. https://doi.org/10.3390/pharmaceutics14081548
Chicago/Turabian StyleGarbin, Marta, Javier Benito, Hélène L. M. Ruel, Ryota Watanabe, Beatriz P. Monteiro, Petra Cagnardi, and Paulo V. Steagall. 2022. "Pharmacokinetics of Bupivacaine Following Administration by an Ultrasound-Guided Transversus Abdominis Plane Block in Cats Undergoing Ovariohysterectomy" Pharmaceutics 14, no. 8: 1548. https://doi.org/10.3390/pharmaceutics14081548