
Population Pharmacokinetics of Palbociclib and Its Correlation with Clinical Efficacy and Safety in Patients with Advanced Breast Cancer

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Population and Data
2.2. Analytical Methods
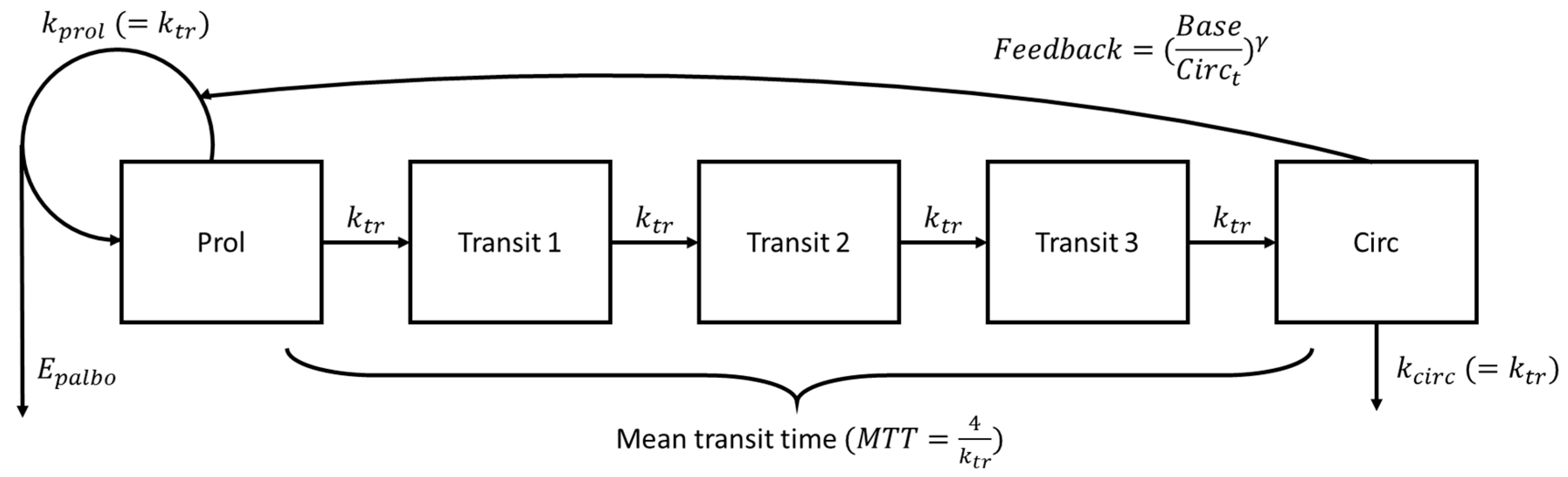
2.3. Pharmacokinetic Model and Exposure–Toxicity Relationship
2.3.1. Pharmacokinetic Model
2.3.2. Exposure–Toxicity Relationship
2.3.3. Covariate Analysis
2.3.4. Parameter Estimation and Model Selection
2.3.5. Model Evaluation
2.3.6. Model-Based Simulations
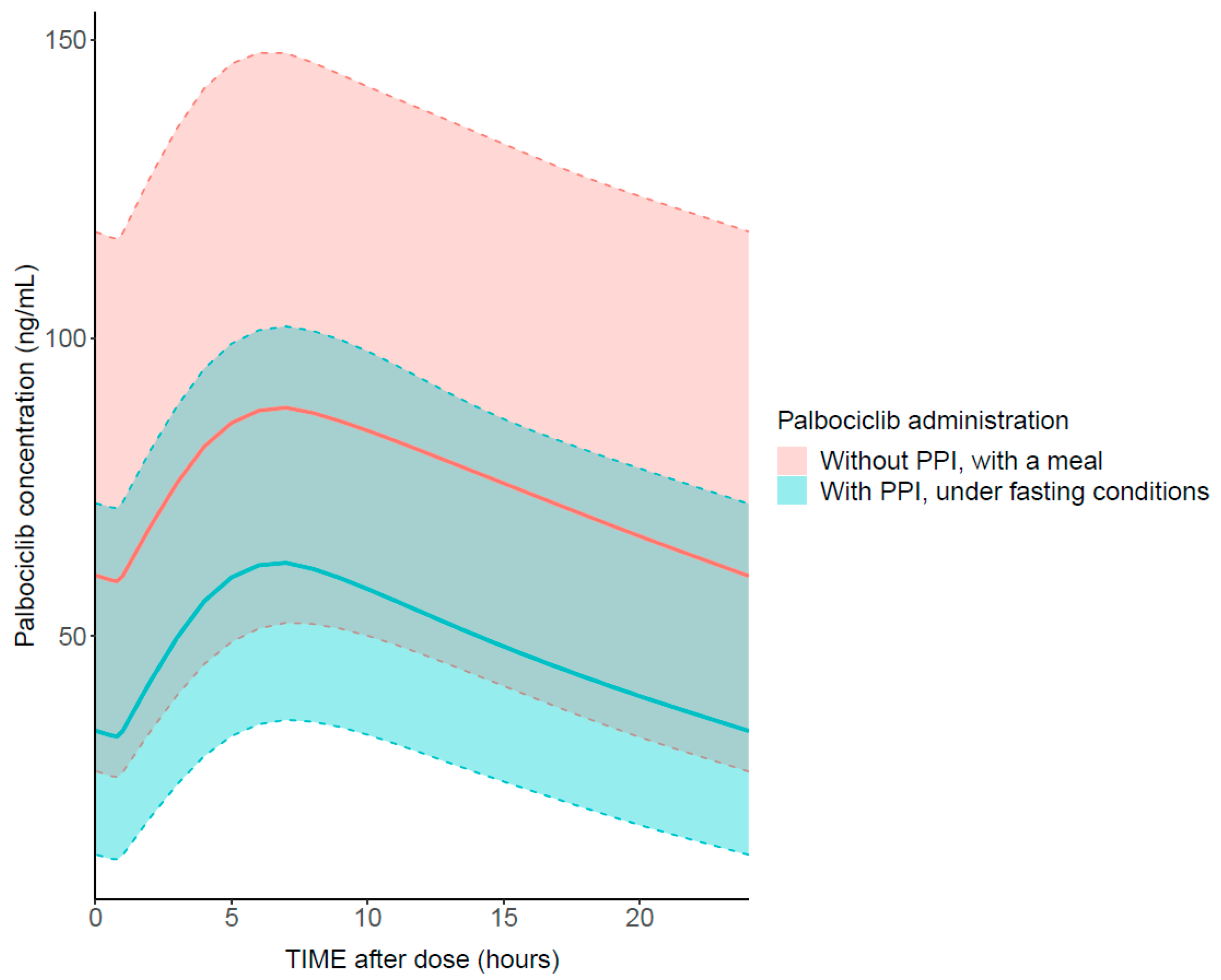
PPI Effect
Neutropenia Characteristics
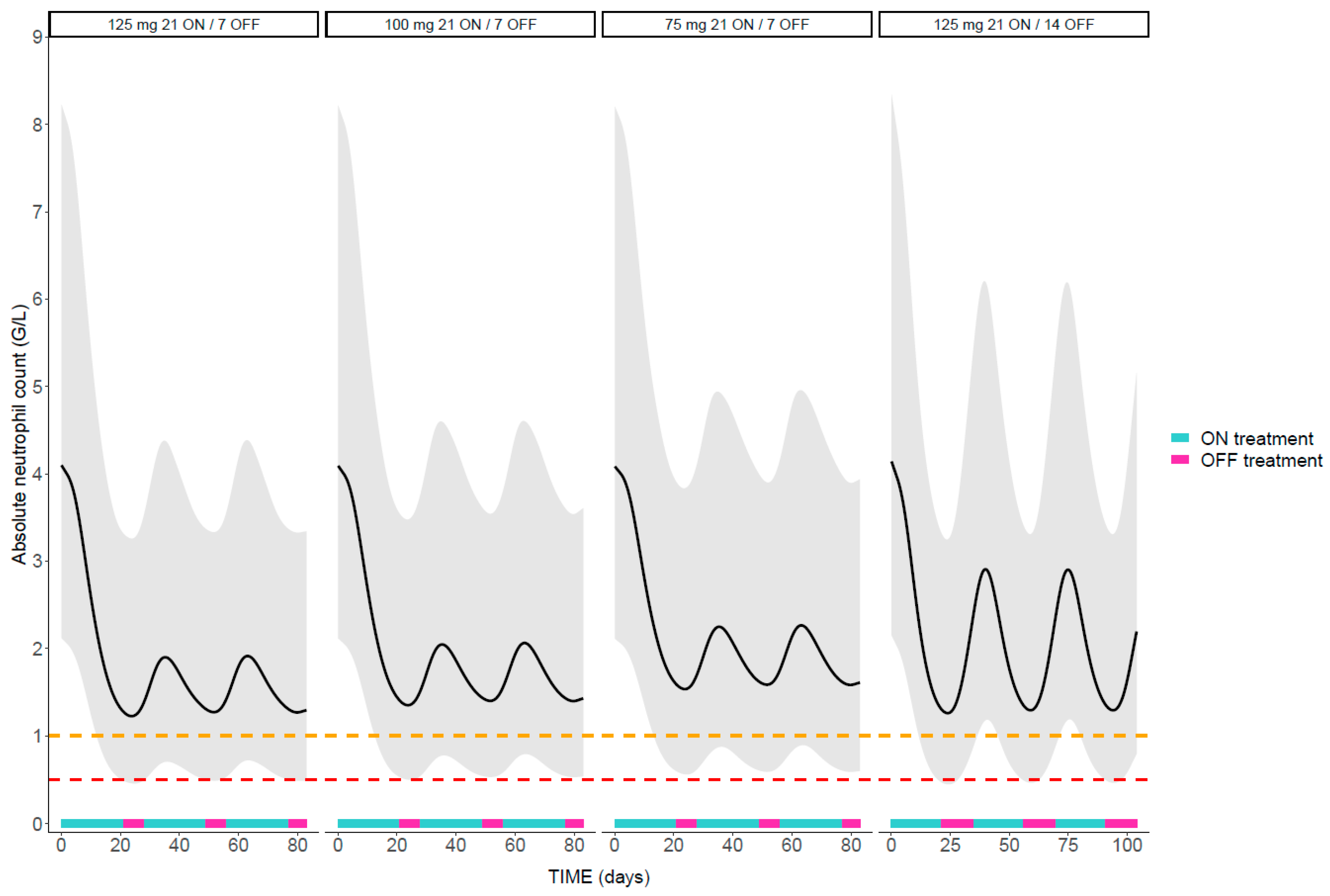
Influence of Palbociclib Dosage Regimen on Neutropenia
Exposure Threshold to Limit the Risk of Severe Neutropenia
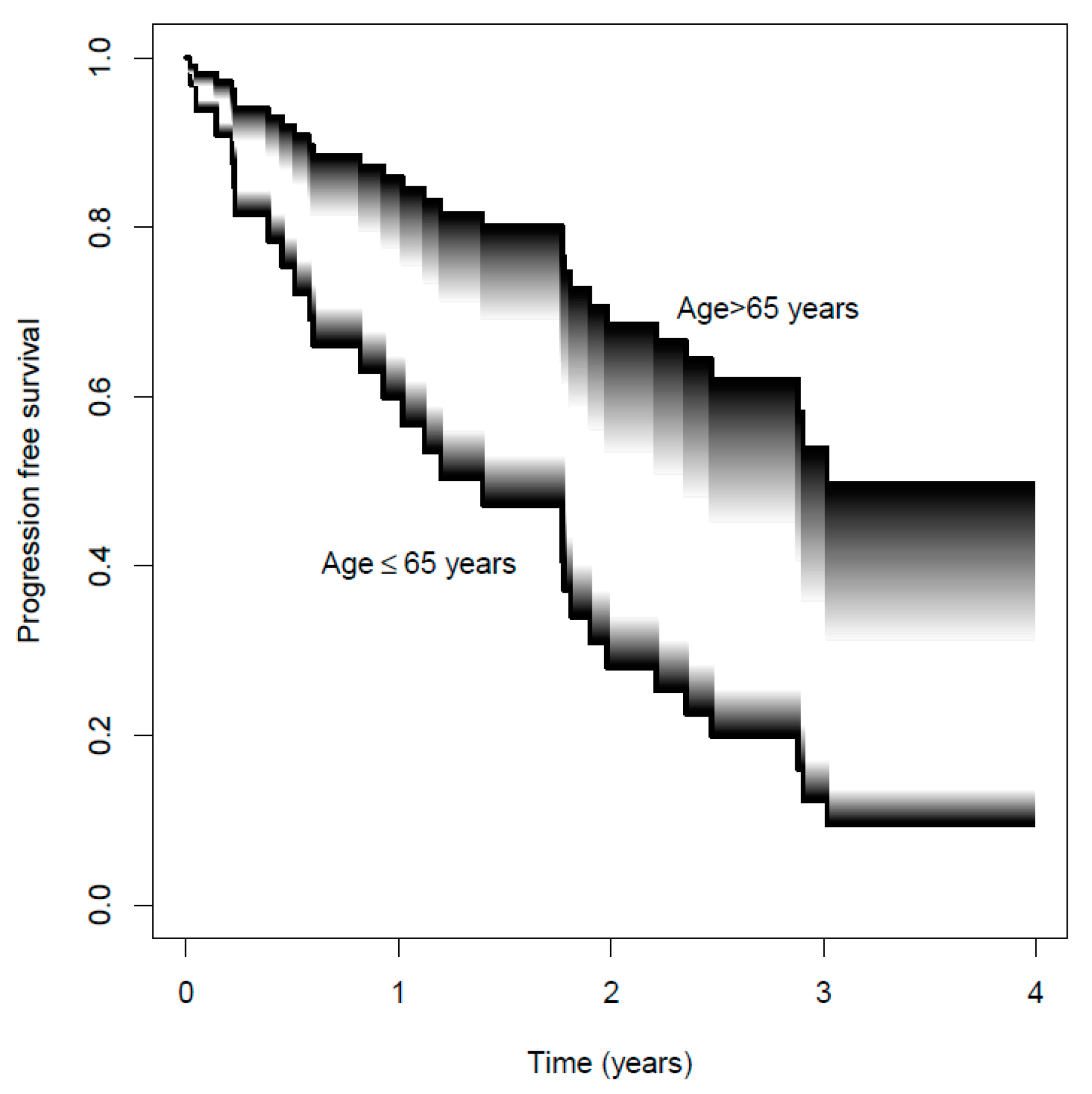
2.4. Exposure–Response Relationship
3. Results
3.1. Study Population and Data
3.2. Pharmacokinetic Model and Exposure–Toxicity Relationship
3.2.1. Pharmacokinetic Analysis
Base Model
Covariate Analysis
External Validation
3.2.2. Exposure–Toxicity Relationship
Base Model
Covariate Analysis
Validation of the Final Exposure–Toxicity Model
3.2.3. Model-Based Simulations
PPI Effect
Neutropenia Characteristics
Influence of Palbociclib Dosage Regimen on Neutropenia
Exposure Threshold to Limit the Risk of Severe Neutropenia
3.3. Exposure–Response Relationship
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Breast Cancer. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/breast-cancer (accessed on 8 February 2022).
- Higgins, M.J.; Baselga, J. Targeted therapies for breast cancer. J. Clin. Investig. 2011, 121, 3797–3803. [Google Scholar] [CrossRef]
- Masoud, V.; Pages, G. Targeted therapies in breast cancer: New challenges to fight against resistance. World J. Clin. Oncol. 2017, 8, 120–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Medicine Agency. Assessment Report, Ibrance. 2016. Available online: https://www.ema.europa.eu/en/documents/assessment-report/ibrance-epar-public-assessment-report_en.pdf (accessed on 8 February 2022).
- Cristofanilli, M.; Turner, N.C.; Bondarenko, I.; Ro, J.; Im, S.-A.; Masuda, N.; Colleoni, M.; DeMichele, A.; Loi, S.; Verma, S.; et al. Fulvestrant plus palbociclib versus fulvestrant plus placebo for treatment of hormone-receptor-positive, HER2-negative metastatic breast cancer that progressed on previous endocrine therapy (PALOMA-3): Final analysis of the multicentre, double-blind, phase 3 randomised controlled trial. Lancet Oncol. 2016, 17, 425–439. [Google Scholar]
- Finn, R.S.; Martin, M.; Rugo, H.S.; Jones, S.; Im, S.-A.; Gelmon, K.; Harbeck, N.; Lipatov, O.N.; Walshe, J.M.; Moulder, S.; et al. Palbociclib and Letrozole in Advanced Breast Cancer. N. Engl. J. Med. 2016, 375, 1925–1936. [Google Scholar] [CrossRef]
- Royer, B.; Kaderbhaï, C.; Fumet, J.-D.; Hennequin, A.; Desmoulins, I.; Ladoire, S.; Ayati, S.; Mayeur, D.; Ilie, S.; Schmitt, A. Population Pharmacokinetics of Palbociclib in a Real-World Situation. Pharmaceuticals 2021, 14, 181. [Google Scholar] [CrossRef]
- Sun, W.; Klamerus, K.J.; Yuhas, L.M.; Pawlak, S.; Plotka, A.; O’Gorman, M.; Kirkovsky, L.; Kosa, M.; Wang, D. Impact of Acid-Reducing Agents on the Pharmacokinetics of Palbociclib, a Weak Base With pH-Dependent Solubility, With Different Food Intake Conditions. Clin Pharmacol. Drug Dev. 2017, 6, 614–626. [Google Scholar] [CrossRef] [PubMed]
- Verheijen, R.B.; Yu, H.; Schellens, J.H.; Beijnen, J.H.; Steeghs, N.; Huitema, A.D.R. Practical Recommendations for Therapeutic Drug Monitoring of Kinase Inhibitors in Oncology. Clin. Pharmacol. Ther. 2017, 102, 765–776. [Google Scholar] [CrossRef]
- Demetri, G.D.; Wang, Y.; Wehrle, E.; Racine, A.; Nikolova, Z.; Blanke, C.D.; Joensuu, H.; von Mehren, M. Imatinib plasma levels are correlated with clinical benefit in patients with unresectable/metastatic gastrointestinal stromal tumors. J. Clin. Oncol. 2009, 27, 3141–3147. [Google Scholar] [CrossRef] [PubMed]
- Wilkie, J.; Schickli, M.A.; Berger, M.J.; Lustberg, M.; Reinbolt, R.; Noonan, A.; Ramaswamy, B.; Sardesai, S.; VanDeusen, J.; Wesolowski, R.; et al. Progression-Free Survival for Real-World Use of Palbociclib in Hormone Receptor-Positive Metastatic Breast Cancer. Clin. Breast Cancer 2020, 20, 33–40. [Google Scholar] [CrossRef]
- Costa, R.; Costa, R.B.; Talamantes, S.M.; Helenowski, I.; Peterson, J.; Kaplan, J.; Carneiro, B.A.; Giles, F.J.; Gradishar, W.J. Meta-analysis of selected toxicity endpoints of CDK4/6 inhibitors: Palbociclib and ribociclib. Breast 2017, 35, 1–7. [Google Scholar] [CrossRef]
- Le Marouille, A.; Petit, E.; Kaderbhai, C.; Desmoulins, I.; Hennequin, A.; Mayeur, D.; Fumet, J.-D.; Ladoire, S.; Tharin, Z.; Ayati, S.; et al. Pharmacokinetic/Pharmacodynamic Model of Neutropenia in Real-Life Palbociclib-Treated Patients. Pharmaceutics 2021, 13, 1708. [Google Scholar] [CrossRef] [PubMed]
- Bandiera, C.; Cardoso, E.; Locatelli, I.; Digklia, A.; Zaman, K.; Diciolla, A.; Cristina, V.; Stravodimou, A.; Veronica, A.L.; Dolcan, A.; et al. Optimizing Oral Targeted Anticancer Therapies Study for Patients With Solid Cancer: Protocol for a Randomized Controlled Medication Adherence Program Along With Systematic Collection and Modeling of Pharmacokinetic and Pharmacodynamic Data. JMIR Res. Protoc. 2021, 10, e30090. [Google Scholar] [CrossRef]
- Lelubre, M.; Kamal, S.; Genre, N.; Celio, J.; Gorgerat, S.; Hampai, D.H.; Bourdin, A.; Berger, J.; Bugnon, O.; Schneider, M. Interdisciplinary Medication Adherence Program: The Example of a University Community Pharmacy in Switzerland. Biomed Res. Int. 2015, 2015, 103546. [Google Scholar] [CrossRef]
- Keizer, R.J.; van Benten, M.; Beijnen, J.H.; Schellens, J.H.; Huitema, A.D. Pirana and PCluster: A modeling environment and cluster infrastructure for NONMEM. Comput. Methods Programs Biomed. 2011, 101, 72–79. [Google Scholar] [CrossRef]
- Lindbom, L.; Pihlgren, P.; Jonsson, E.N. PsN-Toolkit--a collection of computer intensive statistical methods for non-linear mixed effect modeling using NONMEM. Comput. Methods Programs Biomed. 2005, 79, 241–257. [Google Scholar] [CrossRef]
- Friberg, L.E.; Henningsson, A.; Maas, H.; Nguyen, L.; Karlsson, M.O. Model of chemotherapy-induced myelosuppression with parameter consistency across drugs. J. Clin. Oncol. 2002, 20, 4713–4721. [Google Scholar] [CrossRef]
- Sun, W.; O'Dwyer, P.J.; Finn, R.S.; Ruiz-Garcia, A.; Shapiro, G.I.; Schwartz, G.K.; DeMichele, A.; Wang, D. Characterization of Neutropenia in Advanced Cancer Patients Following Palbociclib Treatment Using a Population Pharmacokinetic-Pharmacodynamic Modeling and Simulation Approach. J. Clin. Pharmacol. 2017, 57, 1159–1173. [Google Scholar] [CrossRef]
- European Medicines Agency. Assessment Report, Faslodex. 2017. Available online: https://www.ema.europa.eu/en/documents/variation-report/faslodex-h-c-540-ii-0059-epar-assessment-report-variation_en.pdf (accessed on 12 April 2022).
- Overgaard, R.; Ingwersen, S.; Tornøe, C. Establishing Good Practices for Exposure-Response Analysis of Clinical Endpoints in Drug Development. CPT: Pharmacomet. Syst. Pharmacol. 2015, 4, 565–575. [Google Scholar] [CrossRef]
- Mould, D.R.; Upton, R.N. Basic concepts in population modeling, simulation, and model-based drug development-part 2: Introduction to pharmacokinetic modeling methods. CPT: Pharmacomet. Syst. Pharmacol. 2013, 2, e38. [Google Scholar] [CrossRef]
- Sheiner, L.B.; Beal, S.L. Some suggestions for measuring predictive performance. J. Pharmacokinet. Biopharm. 1981, 9, 503–512. [Google Scholar] [CrossRef] [PubMed]
- Bergstrand, M.; Hooker, A.; Wallin, J.E.; Karlsson, M.O. Prediction-corrected visual predictive checks for diagnosing nonlinear mixed-effects models. AAPS J. 2011, 13, 143–151. [Google Scholar] [CrossRef] [Green Version]
- U.S. Department of Health and Human Services. Common Terminology Criteria for Adverse Events (CTCAE). 2017. Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/CTCAE_v5_Quick_Reference_8.5x11.pdf (accessed on 12 April 2022).
- Henrich, A.; Joerger, M.; Kraff, S.; Jaehde, U.; Huisinga, W.; Kloft, C.; Guillen, Z.P.P. Semimechanistic Bone Marrow Exhaustion Pharmacokinetic/Pharmacodynamic Model for Chemotherapy-Induced Cumulative Neutropenia. J. Pharmacol. Exp. Ther. 2017, 362, 347–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, W.; Wang, D. A population pharmacokinetic (PK) analysis of palbociclib (PD-0332991) in patients (PTS) with advances solid tumors. Ann. Oncol. 2014, 25, 154. [Google Scholar] [CrossRef]
- Hu, W.; Sung, T.; Jessen, B.A.; Thibault, S.; Finkelstein, M.B.; Khan, N.K.; Sacaan, A.I. Mechanistic Investigation of Bone Marrow Suppression Associated with Palbociclib and its Differentiation from Cytotoxic Chemotherapies. Clin. Cancer Res. 2016, 22, 2000–2008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verma, S.; Bartlett, C.H.; Schnell, P.; DeMichele, A.M.; Loi, S.; Ro, J.; Colleoni, M.; Iwata, H.; Harbeck, N.; Cristofanilli, M.; et al. Palbociclib in Combination With Fulvestrant in Women With Hormone Receptor-Positive/HER2-Negative Advanced Metastatic Breast Cancer: Detailed Safety Analysis From a Multicenter, Randomized, Placebo-Controlled, Phase III Study (PALOMA-3). Oncologist 2016, 21, 1165–1175. [Google Scholar] [CrossRef] [Green Version]
- Finn, R.S.; Crown, J.P.; Lang, I.; Boer, K.; Bondarenko, I.M.; Kulyk, S.O.; Ettl, J.; Patel, R.; Pinter, T.; Schmidt, M.; et al. The cyclin-dependent kinase 4/6 inhibitor palbociclib in combination with letrozole versus letrozole alone as first-line treatment of oestrogen receptor-positive, HER2-negative, advanced breast cancer (PALOMA-1/TRIO-18): A randomised phase 2 study. Lancet Oncol. 2015, 16, 25–35. [Google Scholar] [CrossRef]
- Spring, L.M.; Zangardi, M.L.; Moy, B.; Bardia, A. Clinical Management of Potential Toxicities and Drug Interactions Related to Cyclin-Dependent Kinase 4/6 Inhibitors in Breast Cancer: Practical Considerations and Recommendations. Oncologist 2017, 22, 1039–1048. [Google Scholar] [CrossRef] [Green Version]
- Buclin, T.; Thoma, Y.; Widmer, N.; André, P.; Guidi, M.; Csajka, C.; Decosterd, L. The Steps to Therapeutic Drug Monitoring: A Structured Approach Illustrated With Imatinib. Front. Pharm. 2020, 11, 177. [Google Scholar] [CrossRef]
- Mueller-Schoell, A.; Groenland, S.L.; Scherf-Clavel, O.; van Dyk, M.; Huisinga, W.; Michelet, R.; Jaehde, U.; Steeghs, N.; Huitema, A.D.; Kloft, C. Therapeutic drug monitoring of oral targeted antineoplastic drugs. Eur. J. Clin. Pharmacol. 2021, 77, 441–464. [Google Scholar] [CrossRef]
- Cardoso, E.; Csajka, C.; Schneider, M.P.; Widmer, N. Effect of Adherence on Pharmacokinetic/Pharmacodynamic Relationships of Oral Targeted Anticancer Drugs. Clin. Pharmacokinet. 2018, 57, 1–6. [Google Scholar] [CrossRef]
- Dubovitskaya, A.; Buclin, T.; Schumacher, M.; Aberer, K.; Thoma, Y. TUCUXI–An Intelligent System for Personalized Medicine: From Individualization of Treatments to Research Databases and Back. In Proceedings of the 8th ACM International Conference on Bioinformatics, Computational Biology, and Health Informatics, Boston, MA, USA, 20–23 August 2017. [Google Scholar]
- Estape, T. Cancer in the Elderly: Challenges and Barriers. Asia Pac. J. Oncol. Nurs. 2018, 5, 40–42. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.; Yu, Y.; Durairaj, C.; Diéras, V.; Finn, R.S.; Wang, D.D. Impact of Dose Reduction on Efficacy: Implications of Exposure-Response Analysis of Palbociclib. Target. Oncol. 2021, 16, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Watson, G.A.; Deac, O.; Aslam, R.; O'Dwyer, R.; Tierney, A.; Sukor, S.; Kennedy, J. Real-World Experience of Palbociclib-Induced Adverse Events and Compliance With Complete Blood Count Monitoring in Women With Hormone Receptor-Positive/HER2-Negative Metastatic Breast Cancer. Clin. Breast Cancer 2019, 19, e186–e194. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients’ Characteristics | Median [IQR] or n (%) | Missing Data (%) |
|---|---|---|
| Age (years) 1 | 65 [55–75] | |
| Body weight (kg) 1 | 67 [61–80] | |
| AST (UI·L−1) 1 | 23 [19–28] | 8 |
| ALT (UI·L−1) 1 | 20 [15–27] | 9 |
| BILT (µmol·L−1) 1 | 5 [4–7] | 13 |
| Albumin (g·L−1) 1 | 43 [41–45] | 26 |
| ALK (UI·L−1) 1 | 61 [49–81] | 9 |
| GGT (UI·L−1) 1 | 29 [18–51] | 20 |
| CRT (µmol·L−1) 1 | 71 [63–85] | 9 |
| eGFR (mL·min−1·1.73 m−2) 1 | 71 [54–98] | 9 |
| Number of cycles per patient | 33 [22–38] | |
| Administration under fasting conditions 2 | 54 (21) | |
| Co-administration of weak and moderate CYP3A4 inhibitor 2 | 44 (17) | |
| Co-administration of weak and moderate CYP3A4 inducer 2 | 13 (5) | |
| Co-administration of PPI 2 | 78 (31) | |
| Co-administration with fulvestrant 3 | 822 (70) | |
| Chemotherapy in the previous treatment line 3,* | 256 (22) | |
| POCT measurement 3 | 295 (25) |
| Parameter | Final Model | Bootstrap (n = 502 Samples) | ||
|---|---|---|---|---|
| Estimate | RSE (%) | Median | CI95% | |
| Pharmacokinetics | ||||
| ka (h−1) | 0.8 | 30 | 1.0 | 0.5–3.0 |
| ωka (CV%) | 125 | 26 | 120 | 5–368 |
| ALAG (h) | 2.0 | 8 | 2.0 | 1.8–2.5 |
| CL/F (L·h−1) | 67 | 5 | 68 | 62–74 |
| ωCL (CV%) | 29 | 12 | 28 | 20–35 |
| CL/FPPI,no food (L·h−1) | 131 | 4 | 132 | 114–151 |
| Vc /F(L) | 2800 | 7 | 2778 | 2295–3256 |
| ωVc (CV%) | 32 | 16 | 28 | 5–41 |
| Q (L·h−1) | 7 | 31 | 7 | 4–25 |
| Vp/F (L) | 704 | 9 | 738 | 629–1376 |
| Proportional residual error (%) | 18 | 9 | 18 | 15–21 |
| Pharmacodynamics | ||||
| Base (G·L−1) | 4.1 | 7 | 4.1 | 3.6–4.7 |
| ωbase (CV%) | 35 | 14 | 35 | 25–44 |
| MTT (h) | 122 | 5 | 121 | 109–133 |
| ωMTT (CV%) | 12 | 28 | 12 | 2–19 |
| Emax | 0.22 | 7 | 0.22 | 0.19–0.25 |
| ωEmax (CV%) | 15 | 31 | 16 | 1–25 |
| EC50 (ng·mL−1) | 40.1 | FIX | ||
| ωEC50 (CV%) | 93 | 47 | 91 | 1–529 |
| γ | 0.13 | 9 | 0.13 | 0.11–0.17 |
| Additive residual error a | 0.31 | 9 | 0.30 | 0.26–0.35 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Courlet, P.; Cardoso, E.; Bandiera, C.; Stravodimou, A.; Zurcher, J.-P.; Chtioui, H.; Locatelli, I.; Decosterd, L.A.; Darnaud, L.; Blanchet, B.; et al. Population Pharmacokinetics of Palbociclib and Its Correlation with Clinical Efficacy and Safety in Patients with Advanced Breast Cancer. Pharmaceutics 2022, 14, 1317. https://doi.org/10.3390/pharmaceutics14071317
Courlet P, Cardoso E, Bandiera C, Stravodimou A, Zurcher J-P, Chtioui H, Locatelli I, Decosterd LA, Darnaud L, Blanchet B, et al. Population Pharmacokinetics of Palbociclib and Its Correlation with Clinical Efficacy and Safety in Patients with Advanced Breast Cancer. Pharmaceutics. 2022; 14(7):1317. https://doi.org/10.3390/pharmaceutics14071317
Chicago/Turabian StyleCourlet, Perrine, Evelina Cardoso, Carole Bandiera, Athina Stravodimou, Jean-Philippe Zurcher, Haithem Chtioui, Isabella Locatelli, Laurent Arthur Decosterd, Léa Darnaud, Benoit Blanchet, and et al. 2022. "Population Pharmacokinetics of Palbociclib and Its Correlation with Clinical Efficacy and Safety in Patients with Advanced Breast Cancer" Pharmaceutics 14, no. 7: 1317. https://doi.org/10.3390/pharmaceutics14071317