
Novel Eye Drop Delivery Systems: Advance on Formulation Design Strategies Targeting Anterior and Posterior Segments of the Eye



Abstract
:1. Introduction
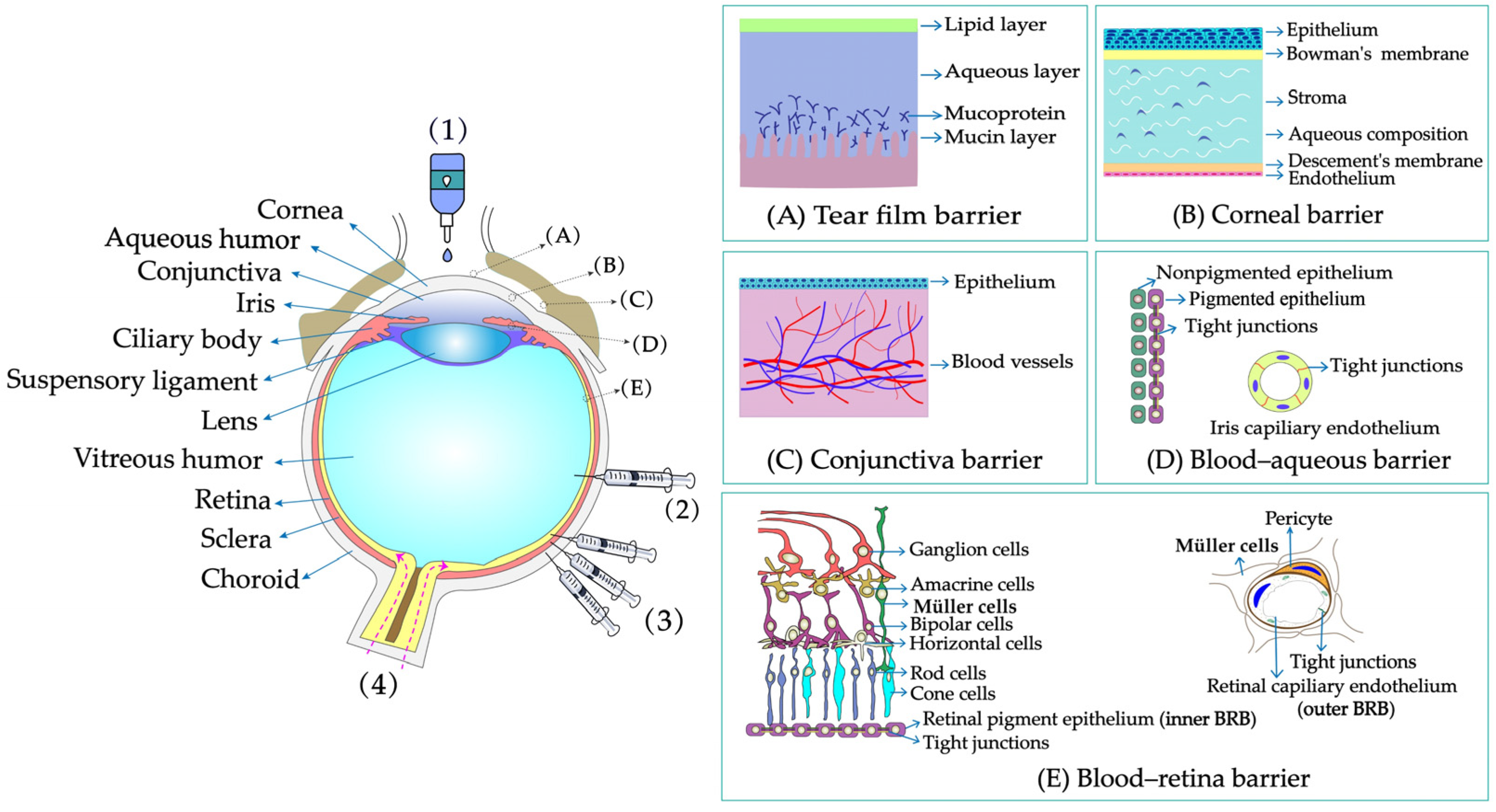
2. Physiological and Structural Barriers of the Eye
2.1. Tear Film Barrier
2.2. Corneal Barrier
2.3. Conjunctival Barrier
2.4. Blood–Aqueous Barrier
2.5. Blood–Retinal Barrier
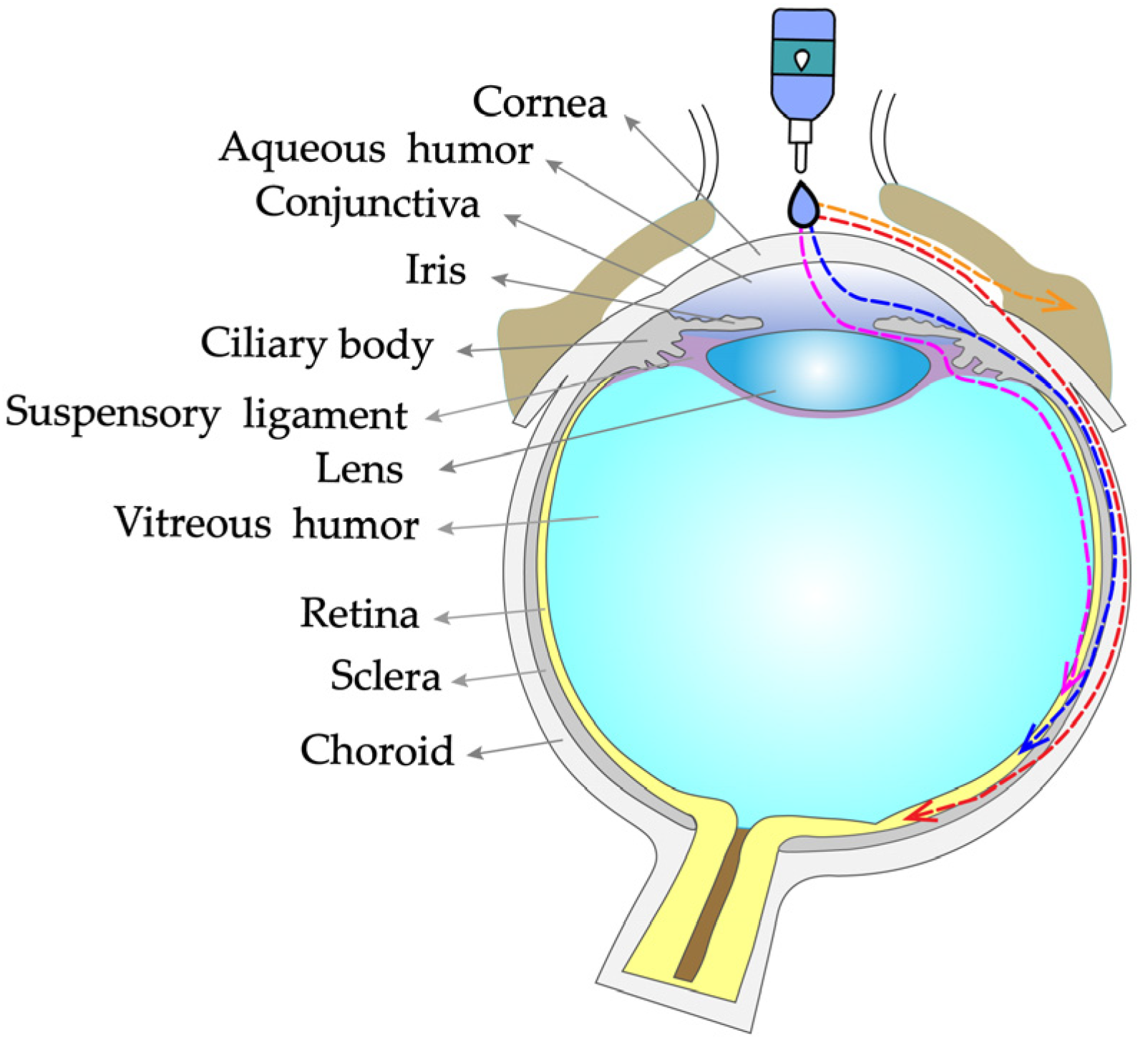
3. Drug Absorption Routes of Eye Drops
4. Novel Eye Drop Delivery Systems
4.1. Prodrug Eye Drop Delivery Systems
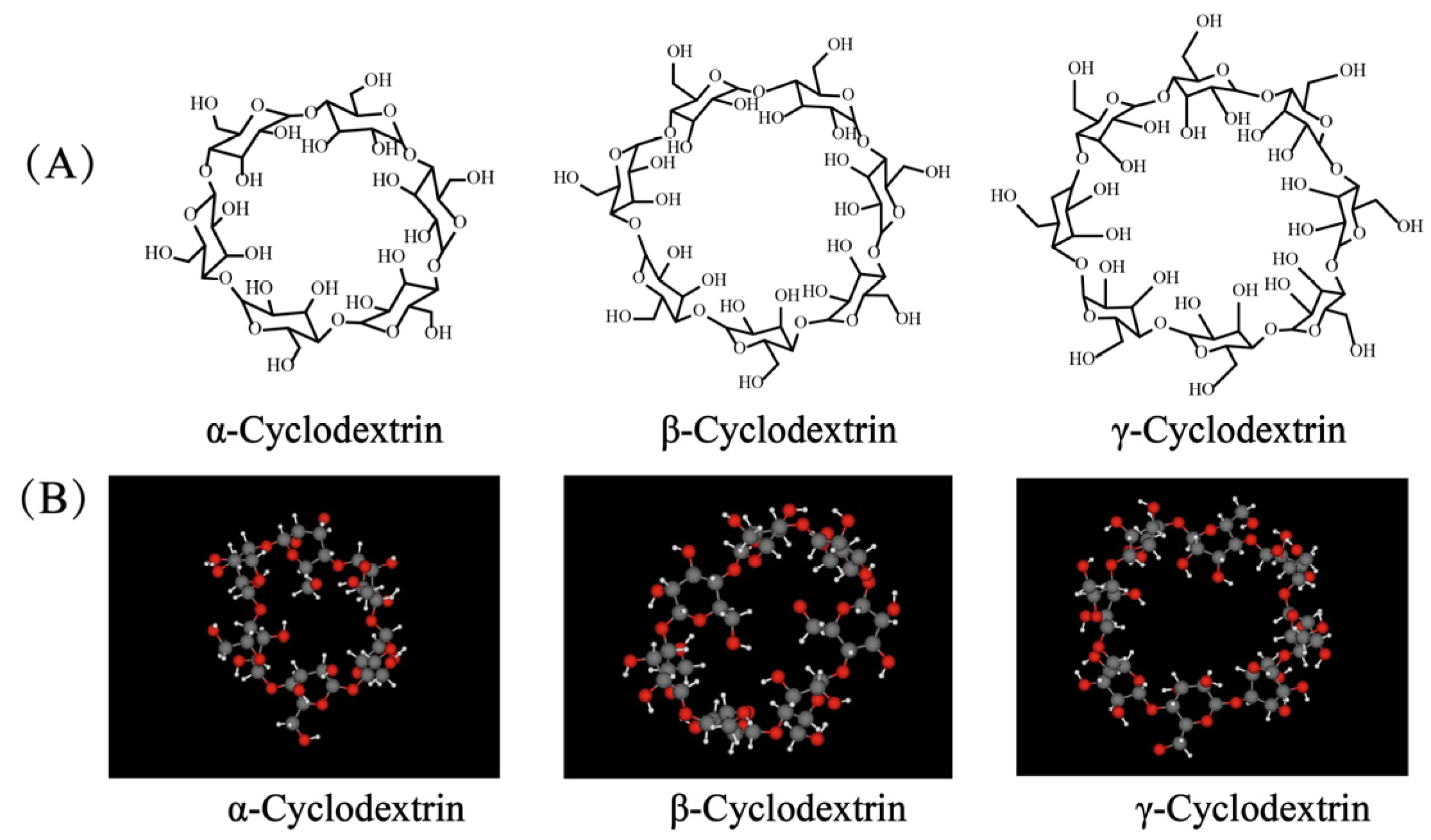
4.2. Cyclodextrin (CD) Eye Drop Delivery Systems
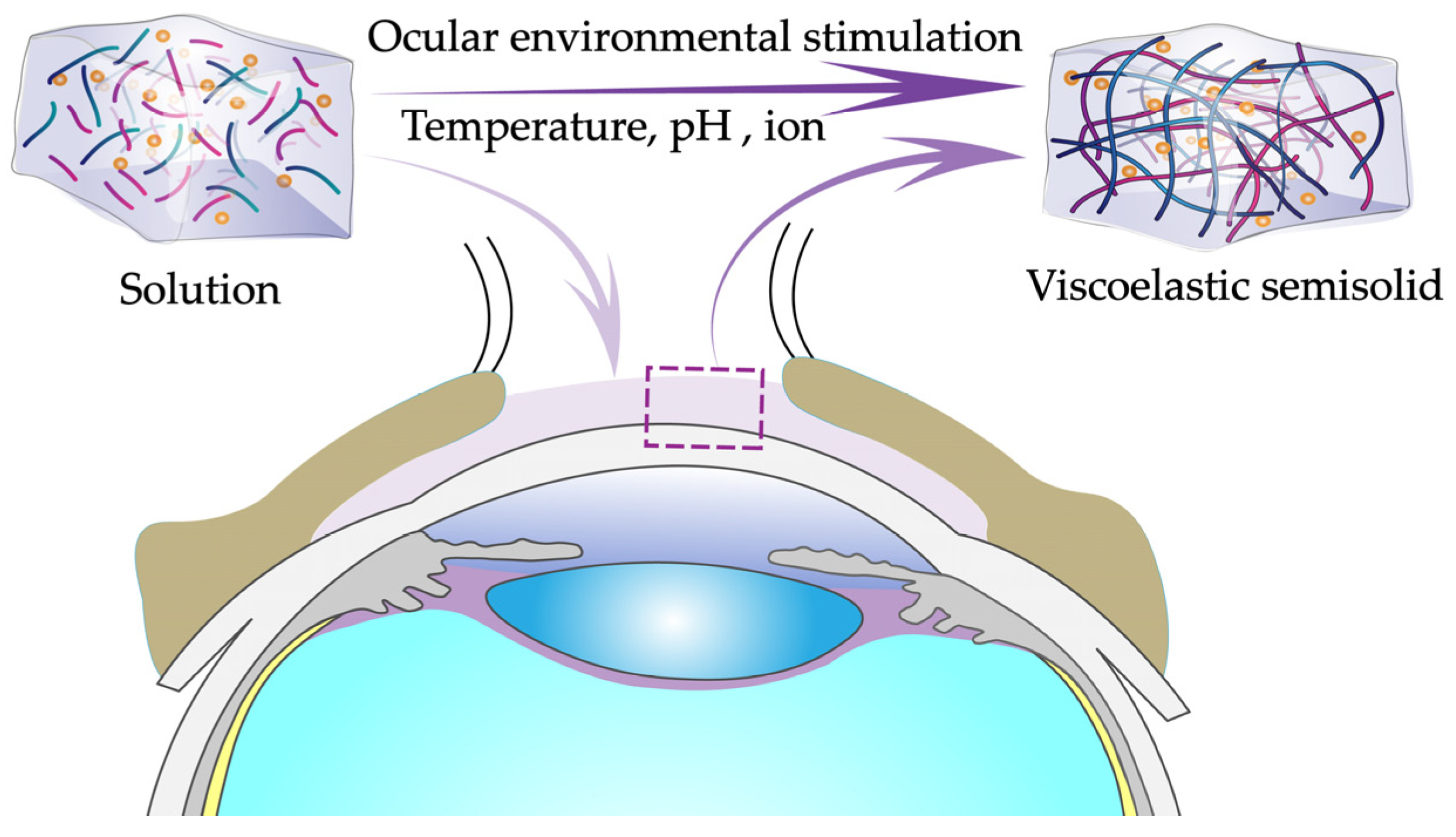
4.3. In Situ Gel Eye Drop Delivery Systems
4.3.1. Temperature-Sensitive In Situ Gel Eye Drop Delivery Systems
4.3.2. pH-Sensitive In Situ Gel Eye Drop Delivery Systems
4.3.3. Ion-Sensitive In Situ Gel Eye Drop Delivery Systems

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Model Drugs | Indications | Main Findings | Ref. |
|---|---|---|---|
| Anterior segment | |||
| Temperature-sensitive in situ gels | |||
| Brinzolamide | Glaucoma | The optimal formulation formed a gel at 33.2 ± 1.1 °C with a diffusion-controlled release time of 8 h. | [82] |
| Ketoconazole | Eye infections | The temperature of the gel was 33 °C, and the gel had a higher healing effect than commercial eye drops. | [83] |
| Tetrahydrozoline | Conjunctivitis | The best prescriptions were stable, nonirritating, and provided continuous drug release for up to 24 h. | [89] |
| Dorzolamide | Glaucoma | The retention time of the drug in front of the cornea was prolonged, and bioavailability was improved. | [90] |
| pH-sensitive in situ gels | |||
| Baicalin | Eye infections | In situ gel provided sustained release of the drug within 8 h. | [93] |
| Timolol maleate | Glaucoma | In situ gel eye drops rapidly transformed into a mucoadhesive gel at the pH of tears. | [94] |
| Gatifloxacin | Eye infections | Gel provided drug release over 8 h. | [95] |
| Ketorolac tromethamine | Eye infections | The retention time of the drug in front of the cornea was prolonged. | [96] |
| Natamycin | Eye inflammation | In vitro permeability was 3.3 times better than commercial formulations and 5.2 times better than suspensions. | [97] |
| Brimonidine tartrate | Glaucoma | The residence time of the drug in the cornea was significantly prolonged, and the intraocular pressure was significantly reduced. | [98] |
| Ion-sensitive in situ gels | |||
| Ketotifen | Seasonal allergic conjunctivitis | The retention time of the drug in front of the cornea was prolonged. | [101] |
| Terbinafine hydrochloride | Fungal keratitis | The optimized in situ gel prolonged the mean residence time of the drug and enhanced ocular bioavailability. | [102] |
| Pefloxacin mesylate | Conjunctivitis and corneal ulcers | The drug was released in vitro for up to 12 h, and the best prescription had good stability and a shelf life of 2 years. | [105] |
| Phenylephrine, tropicamide | Mydriasis | Compared with normal eye drops, the intensity and duration of pupil dilatation in rabbits were increased by 4 to 8 times. | [106] |
| Posterior segment | |||
| pH-sensitive in situ gels | |||
| Bear bile | Retinitis pigmentosa and age-related macular degeneration | The optimum prescription was biocompatible and nonirritating and prolonged the corneal retention time of the drug by approximately 3 times. | [99] |
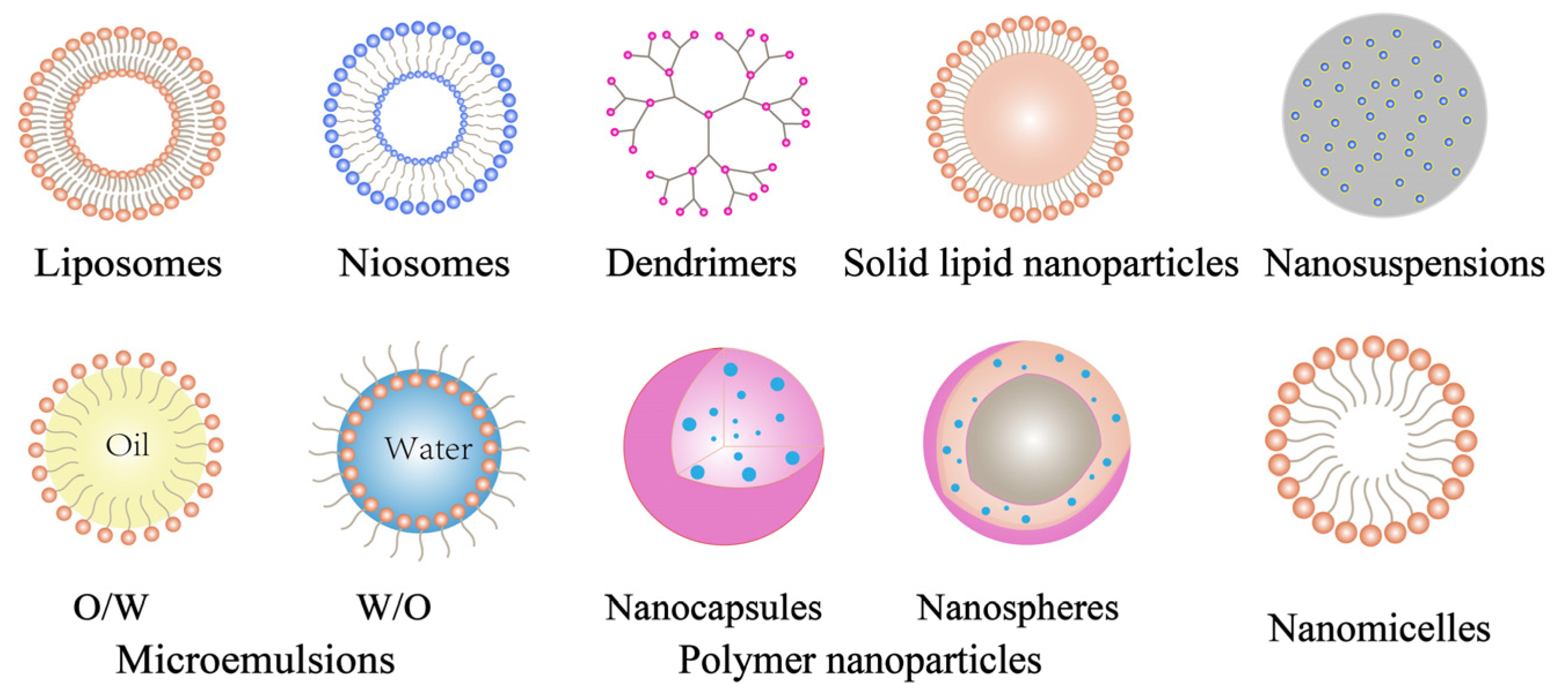
4.4. Nanoparticle Eye Drop Delivery Systems
4.4.1. Liposome Eye Drop Delivery Systems
4.4.2. Niosome Eye Drop Delivery Systems
4.4.3. Solid Lipid Nanoparticle Eye Drop Delivery Systems
4.4.4. Polymer Nanoparticle Eye Drop Delivery Systems
4.4.5. Micelle Eye Drop Delivery Systems
4.4.6. Nanosuspension Eye Drop Delivery Systems
4.4.7. Microemulsion Eye Drop Delivery Systems
4.4.8. Dendritic Polymer Eye Drop Delivery Systems
| Model Drugs | Indications | Main Findings | Ref. |
|---|---|---|---|
| Anterior segment | |||
| Liposomes | |||
| Ganciclovir | Eye infections | The AUC of the aqueous humor concentration–time profile of ganciclovir liposomes was found to be 1.7 times higher than that of ganciclovir solution. | [112] |
| Timolol maleate | Glaucoma | The Papp and Jss of timolol maleate liposomes were 1.50 times higher than that of the commercialized eye drops. | [125] |
| Azithromycin | Dry eye | Liposomes enhanced corneal permeation approximately twofold over that of azithromycin solution. | [126] |
| Niosomes | |||
| Gentamicin | Eye infections | Niosome had a slower release rate than gentamicin sulphate compositions. | [133] |
| Acetazolamide | Glaucoma | Niosome had higher ocular bioavailability than drug solution. | [134] |
| Tacrolimus | Corneal allograft rejection | The AUC of niosomes was 2.3 times greater than that of suspension. | [136] |
| Latanoprost | Glaucoma | The reduced IOP of niosomes was significantly longer than commercial eye drops. | [138] |
| Solid lipid nanoparticles | |||
| Ketoconazole | Ophthalmic mycoses | SLNs had higher ocular bioavailability than ketoconazole suspension. | [141] |
| Methazolamide | Glaucoma | SLNs had higher therapeutic efficacy, later occurrence of maximum action, and more prolonged effect than drug solutions and commercial products. | [150] |
| Methazolamide | Glaucoma | SLNs showed a significantly prolonged decreasing intraocular pressure effect compared with methazolamide solution. | [151] |
| Polymer nanoparticles | |||
| Dexibuprofen | Eye inflammations | NPs were confirmed to be more effective to treat and prevent ocular inflammation than dexibuprofen solution. | [161] |
| 5-fluorouracil | Squamous cell carcinoma | 5-FU level in the aqueous humor of the rabbit eye was significantly higher than that due to 5-FU solution. | [167] |
| Daptomycin | Bacterial endophthalmitis | The antimicrobial activity of daptomycin was preserved when the antibiotic was encapsulated into NPs. | [168] |
| Pranoprofen | Eye inflammations | The corneal permeation coefficient of NPs was four times higher than that of commercial eye drop formulations and freeform drug solutions groups. | [169] |
| Fluocinolone acetonide | Uveitis, posterior uveitis, and panuveitis | NP eye drops showed greatly prolonged residence time of the drug on the ocular surface. | [170] |
| Micelles | |||
| Cyclosporin A | Eye inflammations | The micelle formulation was well tolerated in the eye and represented a promising drug carrier for the treatment of eye diseases. | [175] |
| Nanosuspensions | |||
| Flurbiprofen | Cataract | Drug levels in the aqueous humor were higher after the application of the nanosuspensions. | [188] |
| Hydrocortisone | Inflammation disorders of the eye | The AUC was significantly higher than that of the hydrocortisone solution. | [190] |
| Microemulsions | |||
| Timolol maleate | Glaucoma | MEs had higher drug-loading and transport rates than control. | [195] |
| Gatifloxacin | Bacterial keratitis | MEs had good stability, greater corneal adherence, and permeability. | [196] |
| Dexamethasone | Uveitis | An improved therapeutic effect occurred for the treatment of uveitis. | [203] |
| Sirolimus | Immunosuppressants | Suitable for the immunomodulatory treatment of ocular surface disorders. | [204] |
| Dendritic polymers | |||
| Pilocarpine nitrate and tropicamide | Albino | The ocular residence time of dendrimer (generation 2) solutions was significantly longer even than that of carbomer or HPMC solutions. | [212] |
| Gatidloxacin | Eye inflammations | Enhanced corneal transport and increased antimicrobial activity. | [216] |
| Posterior segment | |||
| Liposomes | |||
| Diclofenac | Macular edema | Liposomes prolonged the retention time in the cornea and allowed higher bioavailability of diclofenac sodium. | [113] |
| Triamcinolone acetonide | Pseudophakic cystoid macular edema | The best corrected visual acuity and central eye socket thickness in the patient improved significantly. | [127] |
| Solid lipid nanoparticles | |||
| N-palmitoyleth anolamide | Retinal inflammation | NLCs significantly increased the levels of PEA in the vitreous and retina compared with a drug suspension. | [142] |
| Atorvastatin | Age-related macular degeneration | SLNs were 8 and 12 times more bioavailable in the aqueous and vitreous humor, respectively, than free atorvastatin. | [152] |
| Triamcinolone acetonide | Macular edema | NLCs could deliver lipophilic active substances to the posterior segment of the eye via both corneal and noncorneal pathways. | [153] |
| Micelles | |||
| Dexamethasone | Posterior uveitis | Micelles delivered the drug to the posterior part of the eye, probably by diffusion through the conjunctival–scleral pathway. | [179] |
| Dexamethasone | Diabetic macular edema | The AUC values showed 1.7- and 2.4-fold increases in bioavailability with Pluronic1 F127 and Pluronic1 F127/chitosan micelle systems, respectively, as compared with a standard dexamethasone suspension. | [180] |
5. Novel Eye Drop Products and Clinical Trials
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Janagam, D.R.; Wu, L.F.; Lowe, T.L. Nanoparticles for Drug Delivery to the Anterior Segment of the Eye. Adv. Drug Deliv. Rev. 2017, 122, 31–64. [Google Scholar] [CrossRef] [PubMed]
- Battaglia, L.; Serpe, L.; Foglietta, F.; Muntoni, E.; Gallarate, M.; Del Pozo Rodriguez, A.; Solinis, M.A. Application of Lipid Nanoparticles to Ocular Drug Delivery. Expert Opin. Drug Deliv. 2016, 13, 1743–1757. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Li, X.; Li, X.; Zeng, Z.; Strang, N.; Shu, X.; Tan, Z. Non-neglectable therapeutic options for age-related macular degeneration: A promising perspective from traditional Chinese medicine. J. Ethnopharmacol. 2020, 282, 114531. [Google Scholar] [CrossRef] [PubMed]
- Yasin, M.N.; Svirskis, D.; Seyfoddin, A.; Rupenthal, I.D. Implants for Drug Delivery to the Posterior Segment of the Eye: A Focus on Stimuli-responsive and Tunable Release Systems. J. Control. Release 2014, 196, 208–221. [Google Scholar] [CrossRef]
- Gaudana, R.; Jwala, J.; Boddu, S.H.; Mitra, A.K. Recent Perspectives in Ocular Drug Delivery. Pharm. Res. 2008, 26, 1197–1216. [Google Scholar] [CrossRef] [Green Version]
- Varela-Fernandez, R.; Diaz-Tome, V.; Luaces-Rodriguez, A.; Conde-Penedo, A.; Garcia-Otero, X.; Luzardo-Alvarez, A.; Fernandez-Ferreiro, A.; Otero-Espinar, F.J. Drug Delivery to the Posterior Segment of the Eye: Biopharmaceutic and Pharmacokinetic Considerations. Pharmaceutics 2020, 12, 269. [Google Scholar] [CrossRef] [Green Version]
- Kurz, D.; Ciulla, T.A. Novel Approaches for Retinal Drug Delivery. Ophthalmol. Clin. N. Am. 2002, 15, 405–410. [Google Scholar] [CrossRef]
- Del Amo, E.M.; Rimpelä, A.K.; Heikkinen, E.; Kari, O.K.; Ramsay, E.; Lajunen, T.; Schmitt, M.; Pelkonen, L.; Bhattacharya, M.; Richardson, D.; et al. Pharmacokinetic Aspects of Retinal Drug Delivery. Prog. Retin. Eye Res. 2017, 57, 134–185. [Google Scholar] [CrossRef]
- Ferroni, M.; De Gaetano, F.; Cereda, M.G.; Boschetti, F. A drug delivery analysis of large molecules in ocular vitreous chamber: Dependency on saccadic movements after intravitreal injection. Med. Eng. Phys. 2020, 82, 49–57. [Google Scholar] [CrossRef]
- Ranta, V.P.; Mannermaa, E.; Lummepuro, K.; Subrizi, A.; Laukkanen, A.; Antopolsky, M.; Murtomäki, L.; Hornof, M.; Urtti, A. Barrier Analysis of Periocular Drug Delivery to the Posterior Segment. J. Control. Release 2010, 148, 42–48. [Google Scholar] [CrossRef]
- Suri, R.; Beg, S.; Kohli, K. Target strategies for drug delivery bypassing ocular barriers. J. Drug Deliv. Sci. Technol. 2019, 55, 101389. [Google Scholar] [CrossRef]
- Bachu, R.D.; Chowdhury, P.; Al-Saedi, Z.H.; Karla, P.K.; Boddu, S.K. Ocular Drug Delivery Barriers-role of Nanocarriers in the Treatment of Anterior Segment Ocular Diseases. Pharmaceutics 2018, 10, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lakhani, P.; Patil, A.; Majumdar, S. Recent Advances in Topical Nano Drug-delivery Systems for the Anterior Ocular Segment. Ther. Deliv. 2018, 9, 137–153. [Google Scholar] [CrossRef]
- Loftsson, T.; Stefánsson, E. Aqueous eye drops containing drug/cyclodextrin nanoparticles deliver therapeutic drug concentrations to both anterior and posterior segment. Acta Ophthalmol. 2022, 100, 7–25. [Google Scholar] [CrossRef]
- Jumelle, C.; Gholizadeh, S.; Annabi, N.; Dana, R. Advances and limitations of drug delivery systems formulated as eye drops. J. Control. Release 2020, 321, 1–22. [Google Scholar] [CrossRef]
- Yellepeddi, V.K.; Palakurthi, S. Recent Advances in Topical Ocular Drug Delivery. J. Ocul. Pharmacol. Ther. 2016, 32, 67–82. [Google Scholar] [CrossRef]
- Alvarez-Trabado, J.; Diebold, Y.; Sanchez, A. Designing Lipid Nanoparticles for Topical Ocular Drug Delivery. Int. J. Pharm. 2017, 532, 204–217. [Google Scholar] [CrossRef]
- Cholkar, K.; Patel, S.P.; Vadlapudi, A.D.; Mitra, A.K. Novel strategies for anterior segment ocular drug delivery. J. Ocul. Pharmacol. Ther. 2013, 29, 106–123. [Google Scholar] [CrossRef] [Green Version]
- Madni, A.; Rahem, M.A.; Tahir, N.; Sarfraz, M.; Jabar, A.; Rehman, M.; Kashif, P.M.; Badshah, S.F.; Khan, K.U.; Santos, H.A. Non-invasive strategies for targeting the posterior segment of eye. Int. J. Pharm. 2017, 530, 326–345. [Google Scholar]
- Imperiale, J.C.; Acosta, G.B.; Sosnik, A. Polymer-based Carriers for Ophthalmic Drug Delivery. J. Control. Release 2018, 285, 106–141. [Google Scholar] [CrossRef]
- Wizert, A.; Iskander, D.R.; Cwiklik, L. Interaction of Lysozyme with A Tear Film Lipid Layer Model: A Molecular Dynamics Simulation Study. Biochim. Biophys. Acta Biomemb. 2017, 1859, 2289–2296. [Google Scholar] [CrossRef]
- Campos, P.M.; Petrilli, R.; Lopez, R.F.V. The Prominence of the Dosage Form Design to Treat Ocular Diseases. Int. J. Pharm. 2020, 586, 119577. [Google Scholar] [CrossRef] [PubMed]
- Gause, S.; Hsu, K.H.; Shafor, C.; Dixon, P.; Powell, K.C.; Chauhan, A. Mechanistic Modeling of Ophthalmic Drug Delivery to the Anterior Chamber by Eye Drops and Contact Lenses. Adv. Colloid. Interface Sci. 2016, 233, 139–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karla, P.K.; Earla, R.; Boddu, S.H.; Johnston, T.P.; Pal, D.; Mitra, A. Molecular Expression and Functional Evidence of a Drug Efflux Pump (BCRP) in Human Corneal Epithelial Cells. Curr. Eye Res. 2009, 34, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watsky, M.A.; Jablonski, M.M.; Edelhauser, H.F. Comparison of Conjunctival and Corneal Surface Areas in Rabbit and Human. Curr. Eye Res. 1988, 7, 483–486. [Google Scholar] [CrossRef]
- Huang, D.; Chen, Y.S.; Rupenthal, I.D. Overcoming Ocular Drug Delivery Barriers Through the Use of Physical Forces. Adv. Drug Deliv. Rev. 2018, 126, 96–112. [Google Scholar] [CrossRef]
- Hosoya, K.; Lee, V.H.; Kim, K.J. Roles of the Conjunctiva in Ocular Drug Delivery: A Review of Conjunctival Transport Mechanisms and Their Regulation. Eur. J. Pharm. Biopharm. 2005, 60, 227–240. [Google Scholar] [CrossRef]
- Ganapathy, M.E.; Ganapathy, V. Amino Acid Transporter ATB0,+ as a Delivery System for Drugs and Prodrugs. Curr. Drug Targets Immune Endocr. Metabol. Disord. 2005, 5, 357–364. [Google Scholar] [CrossRef]
- Yang, J.J.; Ann, D.K.; Kannan, R.; Lee, V.H. Multidrug Resistance Protein 1 (MRP1) in Rabbit Conjunctival Epithelial Cells: Its Effect on Drug Efflux and Its Regulation by Adenoviral Infection. Pharm. Res. 2007, 24, 1490–1500. [Google Scholar] [CrossRef]
- Coca-Prados, M. The Blood-aqueous Barrier in Health and Disease. J. Glaucoma 2014, 23, 36–38. [Google Scholar] [CrossRef]
- Barar, J.; Javadzadeh, A.R.; Omidi, Y. Ocular Novel Drug Delivery: Impacts of Membranes and Barriers. Expert Opin. Drug Deliv. 2008, 5, 567–581. [Google Scholar] [CrossRef] [PubMed]
- Hosoya, K.; Tachikawa, M. Inner Blood-retinal Barrier Transporters: Role of Retinal Drug Delivery. Pharm. Res. 2009, 26, 2055–2065. [Google Scholar] [CrossRef] [PubMed]
- Dey, S.; Mitra, A.K. Transporters and Receptors in Ocular Drug Delivery: Opportunities and Challenges. Expert Opin. Drug Deliv. 2005, 2, 201–204. [Google Scholar] [CrossRef] [PubMed]
- Ranta, V.P.; Urtti, A. Transscleral Drug Delivery to the Posterior Eye: Prospects of Pharmacokinetic Modeling. Adv. Drug Deliv. Rev. 2006, 58, 1164–1181. [Google Scholar] [CrossRef]
- Urtti, A. Challenges and Obstacles of Ocular Pharmacokinetics and Drug Delivery. Adv. Drug Deliv. Rev. 2006, 58, 1131–1135. [Google Scholar] [CrossRef]
- Schoenwald, R.D.; Huang, H.S. Corneal Penetration Behavior of β-blocking Agents I: Physicochemical Factors. J. Pharm. Sci. 1983, 72, 1266–1272. [Google Scholar]
- Huang, H.S.; Schoenwald, R.D.; Lach, J.L. Corneal Penetration Behavior of β-blocking Agents II: Assessment of Barrier Contributions. J. Pharm. Sci. 1983, 72, 1272–1279. [Google Scholar] [CrossRef]
- Kuppermann, B.D.; Loewenstein, A. Drug Delivery to the Posterior Segment of the Eye. Dev. Ophthalmol. 2010, 47, 59–72. [Google Scholar]
- Ramsay, E.; Del Amo, E.M.; Toropainen, E.; Tengvall-Unadike, U.; Ranta, V.P.; Urtti, A.; Ruponen, M. Corneal and Conjunctival Drug Permeability: Systematic Comparison and Pharmacokinetic Impact in the Eye. Eur. J. Pharm. Sci. 2018, 119, 83–89. [Google Scholar] [CrossRef] [Green Version]
- Zambito, Y.; Zaino, C.; Di Colo, G. Effects of N-trimethylchitosan on Transcellular and Paracellular Transcorneal Drug Transport. Eur. J. Pharm. Biopharm. 2006, 64, 16–25. [Google Scholar] [CrossRef]
- Markovic, M.; Ben-Shabat, S.; Dahan, A. Prodrugs for Improved Drug Delivery: Lessons Learned from Recently Developed and Marketed Products. Pharmaceutics 2020, 12, 1031. [Google Scholar] [CrossRef] [PubMed]
- Taskar, P.; Tatke, A.; Majumdar, S. Advances in the Use of Prodrugs for Drug Delivery to the Eye. Expert Opin. Drug Deliv. 2016, 14, 49–63. [Google Scholar] [CrossRef]
- Hussain, A.; Truelove, J.E. Prodrug Approaches to Enhancement of Physicochemical Properties of Drugs IV: Novel Epinephrine Prodrug. J. Pharm. Sci. 1976, 65, 1510–1512. [Google Scholar] [CrossRef] [PubMed]
- Mandell, A.I.; Stentz, F.; Kitabchi, A.E. Dipivalyl epinephrine: A new prodrug in the treatment of glaucoma. Ophthalmology 1978, 85, 268–275. [Google Scholar] [CrossRef]
- Ikuta, Y.; Aoyagi, S.; Tanaka, Y.; Sato, K.; Inada, S.; Koseki, Y.; Onodera, T.; Oikawa, H.; Kasai, H. Creation of Nano Eye-drops and Effective Drug Delivery to the Interior of the Eye. Sci. Rep. 2017, 7, 44229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Babizhayev, M.A. Ocular Drug Metabolism of the Bioactivating Antioxidant N-acetylcarnosine for Vision in Ophthalmic Prodrug and Codrug Design and Delivery. Drug Dev. Ind. Pharm. 2008, 34, 1071–1089. [Google Scholar] [CrossRef]
- Cholkar, K.; Gilger, B.C.; Mitra, A.K. Topical delivery of aqueous micellar resolvin E1 analog (RX-10045). Int. J. Pharm. 2016, 498, 326–334. [Google Scholar] [CrossRef] [Green Version]
- Palanki, M.S.S.; Akiyama, H.; Campochiaro, P.; Cao, J.G.; Chow, C.P.; Dellamary, L.; Doukas, J.; Fine, R.; Gritzen, C.; Hood, J.D.; et al. Development of Prodrug 4-Chloro-3-(5-methyl-3-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}-1,2,4-benzotriazin-7-yl)phenyl Benzoate (TG100801): A Topically Administered Therapeutic Candidate in Clinical Trials for the Treatment of Age-Related Macular Degeneration. J. Med. Chem. 2008, 51, 1546–1559. [Google Scholar]
- Ye, T.; Yuan, K.; Zhang, W.; Song, S.; Chen, F.; Yang, X.; Wang, S.J.; Bi, J.W.; Pan, W. Prodrugs incorporated into nanotechnology-based drug delivery systems for possible improvement in bioavailability of ocular drugs delivery. Asian J. Pharm. Sci. 2013, 8, 207–217. [Google Scholar] [CrossRef] [Green Version]
- Hu, L.; Hu, Z.; Yu, Y.; Ding, X.; Li, K.; Gong, Q.; Lin, D.; Dai, M.; Lu, F.; Li, X. Preparation and characterization of a pterostilbene-peptide prodrug nanomedicine for the management of dry eye. Int. J. Pharm. 2020, 588, 119683. [Google Scholar] [CrossRef]
- Stella, B.; Arpicco, S.; Rocco, F.; Burgalassi, S.; Nicosia, N.; Tampucci, S.; Chetoni, P.; Cattel, L. Nonpolymeric nanoassemblies for ocular administration of acyclovir: Pharmacokinetic evaluation in rabbits. Eur. J. Pharm. Biopharm. 2012, 80, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Prokai-Tatrai, K.; Nguyen, V.; De La Cruz, D.L.; Guerra, R.; Zaman, K.; Rahlouni, F.; Prokai, L. Retina-targeted Delivery of 17β-Estradiol by the Topically Applied DHED Prodrug. Pharmaceutics 2020, 12, 456. [Google Scholar] [CrossRef] [PubMed]
- Vooturi, S.K.; Kadam, R.S.; Kompella, U.B. Transporter Targeted Gatifloxacin Prodrugs: Synthesis, Permeability, and Topical Ocular Delivery. Mol. Pharm. 2012, 9, 3136–3146. [Google Scholar] [CrossRef] [Green Version]
- Loftsson, T.; Stefánsson, E. Cyclodextrins and Topical Drug Delivery to the Anterior and Posterior Segments of the Eye. Int. J. Pharm. 2017, 531, 413–423. [Google Scholar] [CrossRef]
- Abd El-Gawad, A.E.H.; Soliman, O.A.; El-Dahan, M.S.; Al-Zuhairy, S.A.S. Improvement of the Ocular Bioavailability of Econazole Nitrate Upon Complexation with Cyclodextrins. AAPS PharmSciTech 2016, 18, 1795–1809. [Google Scholar] [CrossRef]
- Loftsson, T.; Hreinsdóttir, D.; Stefánsson, E. Cyclodextrin microparticles for drug delivery to the posterior segment of the eye: Aqueous dexamethasone eye drops. J. Pharm. Pharmacol. 2007, 59, 629–635. [Google Scholar] [CrossRef]
- Loftsson, T.; Sigurdsson, H.H.; Hreinsdóttir, D.; Konrádsdóttir, F.; Stefánsson, E. Dexamethasone delivery to posterior segment of the eye. J. Incl. Phenom. Macrocycl. Chem. 2007, 57, 585–589. [Google Scholar] [CrossRef]
- Rodriguez-Aller, M.; Guinchard, S.; Guillarme, D.; Pupier, M.; Jeannerat, D.; Rivara-Minten, E.; Veuthey, J.L.; Gurny, R. New prostaglandin analog formulation for glaucoma treatment containing cyclodextrins for improved stability, solubility and ocular tolerance. Eur. J. Pharm. Biopharm. 2015, 95, 203–214. [Google Scholar] [CrossRef]
- Jansook, P.; Stefánsson, E.; Thorsteinsdóttir, M.; Sigurdsson, B.B.; Kristjánsdóttir, S.S.; Bas, J.F.; Sigurdsson, H.H.; Loftsson, T. Cyclodextrin solubilization of carbonic anhydrase inhibitor drugs: Formulation of dorzolamide eye drop microparticle suspension. Eur. J. Pharm. Biopharm. 2010, 76, 208–214. [Google Scholar] [CrossRef]
- Senjoti, F.G.; Timmins, P.; Conway, B.R.; Smith, A.M. Optimizing ophthalmic delivery of a poorly water soluble drug from an aqueous in situ gelling system. Eur. J. Pharm. Biopharm. 2020, 154, 1–7. [Google Scholar] [CrossRef]
- Fernández-Ferreiro, A.; Fernández Bargiela, N.; Varela, M.S.; Martínez, M.G.; Pardo, M.; Piñeiro Ces, A.; Méndez, J.B.; Barcia, M.G.; Lamas, M.J.; Otero-Espinar, F. Cyclodextrin-polysaccharide-based, In Situ-gelled System for Ocular Antifungal Delivery. Beilstein J. Org. Chem. 2014, 10, 2903–2911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaudhari, P.; Naik, R.; Sruthi Mallela, L.; Roy, S.; Birangal, S.; Ghate, V.; Balladka Kunhanna, S.; Lewis, S.A. A supramo-lecular thermosensitive gel of ketoconazole for ocular applications: In silico, in vitro, and ex vivo studies. Int. J. Pharm. 2022, 613, 121409. [Google Scholar] [CrossRef]
- Zhou, X.; Li, X.; Xu, J.; Cheng, Y.; Cao, F. Latanoprost-loaded Cyclodextrin Microaggregate Suspension Eye Drops for Enhanced Bioavailability and Stability. Eur. J. Pharm. Sci. 2021, 160, 105758. [Google Scholar] [CrossRef] [PubMed]
- Mahmoudi, A.; Malaekeh-Nikouei, B.; Hanafi-Bojd, M.Y.; Toloei, M.; Hosseini, M.; Nikandish, M. Preliminary in Vivo Safety Evaluation of a Tacrolimus Eye Drop Formulation Using Hydroxypropyl Beta Cyclodextrin After Ocular Administration in NZW Rabbits. Clin. Ophthalmol. 2020, 14, 947–953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, S.; Tang, Y.; Zhang, X.; Dou, Y.; Shen, X. Preparation and characterization of diclofenac sodium β-cyclodextrin inclusion complex eye drops. J. Incl. Phenom. Macrocycl. Chem. 2019, 94, 85–94. [Google Scholar] [CrossRef]
- Tanito, M.; Hara, K.; Takai, Y.; Matsuoka, Y.; Nishimura, N.; Jansook, P.; Loftsson, T.; Stefánsson, E.; Ohira, A. Topical Dexamethasone-cyclodextrin Microparticle Eye Drops for Diabetic Macular Edema. Investig. Opthalmol. Vis. Sci. 2011, 52, 7944. [Google Scholar] [CrossRef]
- Jansook, P.; Kulsirachote, P.; Asasutjarit, R.; Loftsson, T. Development of Celecoxib Eye Drop Solution and Microsuspension: A Comparative Investigation of Binary and Ternary Cyclodextrin Complexes. Carbohydr. Polym. 2019, 225, 115209. [Google Scholar] [CrossRef]
- Khan, N.; Aqil, M.; Imam, S.S.; Ali, A. Development and Evaluation of a Novel in Situ Gel of Sparfloxacin for Sustained Ocular Drug Delivery: In Vitro and ex Vivo Characterization. Pharm. Dev. Technol. 2015, 20, 662–669. [Google Scholar] [CrossRef]
- Agrawal, A.K.; Das, M.; Jain, S. In Situ Gel Systems as ‘smart’ Carriers for Sustained Ocular Drug Delivery. Expert Opin. Drug Deliv. 2012, 9, 383–402. [Google Scholar] [CrossRef]
- Mandal, S.; Thimmasetty, M.K.; Prabhushankar, G.; Geetha, M. Formulation and Evaluation of an in situ Gel-forming Ophthalmic Formulation of Moxifloxacin Hydrochloride. Int. J. Pharm. Investig. 2012, 2, 78–82. [Google Scholar] [CrossRef] [Green Version]
- Kushwaha, S.K.; Saxena, P.; Rai, A. Stimuli Sensitive Hydrogels for Ophthalmic Drug Delivery: A Review. Int. J. Pharm. Investig. 2012, 2, 54–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alvarez-Lorenzo, C.; Bromberg, L.; Concheiro, A. Light-sensitive Intelligent Drug Delivery Systems. Photochem. Photobiol. 2009, 85, 848–860. [Google Scholar] [CrossRef] [PubMed]
- Mitragotri, S. Healing Sound: The Use of Ultrasound in Drug Delivery and Other Therapeutic Applications. Nat. Rev. Drug Discov. 2005, 4, 255–260. [Google Scholar] [CrossRef]
- Murdan, S. Electro-responsive Drug Delivery from Hydrogels. J. Control. Release 2003, 92, 1–17. [Google Scholar] [CrossRef]
- Packhaeuser, C.B.; Schnieders, J.; Oster, C.G.; Kissel, T. In Situ Forming Parenteral Drug Delivery Systems: An Overview. Eur. J. Pharm. Biopharm. 2004, 58, 445–455. [Google Scholar] [CrossRef]
- Almeida, H.; Amaral, M.H.; Lobão, P.; Lobo, J.M.S. In Situ Gelling Systems: A Strategy to Improve the Bioavailability of Ophthalmic Pharmaceutical Formulations. Drug Discov. Today 2014, 19, 400–412. [Google Scholar] [CrossRef]
- He, S.; Tourkakis, G.; Berezin, O.; Gerasimchuk, N.; Zhang, H.R.; Zhou, H.Y.; Izraely, A.; Akers, W.J.; Berezin, M.Y. Temperature-dependent Shape-Responsive Fluorescent Nanospheres for Image-guided Drug Delivery. J. Mater. Chem. C 2016, 4, 3028–3035. [Google Scholar] [CrossRef] [Green Version]
- Qiu, Y.; Park, K. Environment-sensitive Hydrogels for Drug Delivery. Adv. Drug Deliv. Rev. 2012, 64, 49–60. [Google Scholar] [CrossRef]
- Belal, K.; Stoffelbach, F.; Lyskawa, J.; Fumagalli, M.; Hourdet, D.; Marcellan, A.; De Smet, L.; de la Rosa, V.R.; Cooke, G.; Hoogenboom, R.; et al. Recognition-mediated Hydrogel Swelling Controlled by Interaction with A Negative Thermoresponsive LCST Polymer. Angew. Chem. Int. Ed. Engl. 2016, 55, 13974–13978. [Google Scholar] [CrossRef] [Green Version]
- Wei, G.; Xu, H.; Ding, P.T.; Li, S.M.; Zheng, J.M. Thermosetting Gels with Modulated Gelation Temperature for Ophthalmic Use: The Rheological and Gamma Scintigraphic Studies. J. Control. Release 2002, 83, 65–74. [Google Scholar] [CrossRef]
- Tuthill, J.C.; Borghuis, B.G. Four to Foxtrot: How Visual Motion is Computed in the Fly Brain. Neuron 2016, 89, 677–680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.; Liu, H.; Liu, L.L.; Cai, C.N.; Xin, H.X.; Liu, W. Design and Evaluation of a Brinzolamide Drug-resin in Situ Thermosensitive Gelling System for Sustained Ophthalmic Drug Delivery. Chem. Pharm. Bull. 2014, 62, 1000–1008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, M.Q.; Wang, J.; Li, N. A Novel Thermo-sensitive Hydrogel-based on Poly(N-isopropylacrylamide)/hyaluronic Acid of Ketoconazole for Ophthalmic Delivery. Artif. Cells Nanomed. Biotechnol. 2018, 46, 1282–1287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vodithala, S.; Khatry, S.; Shastri, N.; Sadanandam, M. Development and evaluation of thermoreversible ocular gels of ketorolac tromethamine. Int. J. Biopharm. 2010, 1, 39–45. [Google Scholar]
- Gratieri, T.; Gelfuso, G.M.; Rocha, E.M.; Sarmento, V.H.; de-Freitas, O.; Lopez, R.F.V. A Poloxamer/chitosan in Situ Forming Gel with Prolonged Retention Time for Ocular Delivery. Eur. J. Pharm. Biopharm. 2010, 75, 186–193. [Google Scholar] [CrossRef]
- Morsi, N.; Ghorab, D.; Refai, H.; Teba, H. Ketoroloac tromethamine loaded nanodispersion incorporated into thermosensitive in situ gel for prolonged ocular delivery. Int. J. Pharm. 2016, 506, 57–67. [Google Scholar] [CrossRef]
- Bhowmik, M.; Bain, M.K.; Ghosh, L.K.; Chattopadhyay, D. Effect of salts on gelation and drug release profiles of methylcellulose-based ophthalmic thermo-reversible in situ gels. Pharm. Dev. Technol. 2011, 16, 385–391. [Google Scholar] [CrossRef]
- Bhowmick, B.; Sarkar, G.; Roy, I.; Saha, N.R.; Ghosh, S.; Rana, D.; Chattopadhyay, D. Effect of carrageenan and potassiumchloride on in-situ gelling ophthalmic drug delivery system based on methylcellulose. RSC Adv. 2015, 5, 60386–60391. [Google Scholar] [CrossRef]
- Okur, N.Ü.; Yozgatli, V.; Okur, M.E. In Vitro-in Vivo Evaluation of Tetrahydrozoline-loaded Ocular in Situ Gels on Rabbits for Allergic Conjunctivitis Management. Drug Dev. Res. 2020, 81, 716–727. [Google Scholar] [CrossRef]
- Ammar, H.O.; Salama, H.A.; Ghorab, M.; Mahmoud, A.A. Development of Dorzolamide Hydrochloride in Situ Gel Nanoemulsion for Ocular Delivery. Drug Dev. Ind. Pharm. 2010, 36, 1330–1339. [Google Scholar] [CrossRef]
- Schmaljohann, D. Thermo-and PH-responsive Polymers in Drug Delivery. Adv. Drug Deliv. Rev. 2006, 58, 1655–1670. [Google Scholar] [CrossRef] [PubMed]
- Srividya, B.; Cardoza, R.M.; Amin, P.D. Sustained Ophthalmic Delivery of Ofloxacin from a PH Triggered in Situ Gelling System. J. Control. Release 2001, 73, 205–211. [Google Scholar] [CrossRef]
- Wu, H.Y.; Liu, Z.D.; Peng, J.J.; Li, L.; Li, N.; Li, J.W.; Pan, H. Design and Evaluation of Baicalin-containing in Situ PH-Triggered Gelling System for Sustained Ophthalmic Drug Delivery. Int. J. Pharm. 2011, 410, 31–40. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Vyas, S.P. Carbopol/chitosan Based PH Triggered in Situ Gelling System for Ocular Delivery of Timolol Maleate. Sci. Pharm. 2010, 78, 959–976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanoujia, J.; Sonker, K.; Pandey, M.; Kymonil, K.M.; Saraf, S.A. Formulation and characterization of a novel ph-triggered in-situ gelling ocular system containing gatifloxacin. Int. Curr. Pharm. J. 2012, 1, 43–49. [Google Scholar] [CrossRef] [Green Version]
- Manjappa, A.S.; Nanjwade, B.K.; Manvi, F.V.; Murthy, R.S. Sustained ophthalmic in situ gel of ketorolac tromethamine: Rheology and in vivo studies. Drug Dev. Res. 2009, 70, 417–424. [Google Scholar] [CrossRef]
- Hosny, K.M.; Rizg, W.Y.; Alkhalidi, H.M.; Abualsunun, W.A.; Bakhaidar, R.B.; Almehmady, A.M.; Alghaith, A.F.; Alshehri, S.; El Sisi, A.M. Nanocubosomal Based in Situ Gel Loaded with Natamycin for Ocular Fungal Diseases: Development, Optimization, In-vitro, and in-vivo Assessment. Drug Deliv. 2021, 28, 1836–1848. [Google Scholar] [CrossRef]
- Barse, R.K.; Tagalpallewar, A.A.; Kokare, C.R.; Sharma, J.P.; Sharma, P.K. Formulation and ex Vivo-in vivo Evaluation of PH-triggered Brimonidine Tartrate in Situ Gel for the Glaucoma Treatment Using Application of 32 Factorial Design. Drug Dev. Ind. Pharm. 2017, 44, 800–807. [Google Scholar] [CrossRef]
- Ni, X.M.; Guo, Q.; Zou, Y.; Xuan, Y.; Mohammad, I.S.; Ding, Q.; Hu, H. Preparation and Characterization of Bear Bile-loaded PH Sensitive in-situ Gel Eye Drops for Ocular Drug Delivery. Iran. J. Basic Med. Sci. 2020, 23, 922–929. [Google Scholar]
- Kalam, M.A.; Sultana, Y.; Samad, A.; Ali, A.; Aqil, M.; Sharma, M.; Mishta, A.K. Gelrite-based in vitro gelation ophthalmic drug delivery system of gatifloxacin. J. Dispers. Sci. Technol. 2008, 29, 89–96. [Google Scholar] [CrossRef]
- Zhu, L.N.; Ao, J.P.; Li, P.L. A Novel in Situ Gel Base of Deacetylase Gellan Gum for Sustained Ophthalmic Drug Delivery of Ketotifen: In Vitro and in Vivo Evaluation. Drug Des. Devel. Ther. 2015, 9, 3943–3949. [Google Scholar] [PubMed] [Green Version]
- Tayel, S.A.; El-Nabarawi, M.A.; Tadros, M.I.; Abd-Elsalam, W.H. Promising Ion-sensitive in Situ Ocular Nanoemulsion Gels of Terbinafine Hydrochloride: Design, In Vitro Characterization and in Vivo Estimation of the Ocular Irritation and Drug Pharmacokinetics in the Aqueous Humor of Rabbits. Int. J. Pharm. 2013, 443, 293–305. [Google Scholar] [CrossRef] [PubMed]
- Rupenthal, I.D.; Green, C.R.; Alany, R.G. Comparison of Ion-activated in Situ Gelling Systems for Ocular Drug Delivery Part 2: Precorneal Retention and in Vivo Pharmacodynamic Study. Int. J. Pharm. 2011, 411, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Li, P.F.; Wang, S.; Chen, H.Y.; Zhang, S.M.; Yu, S.H.; Li, Y.N.; Cui, M.S.; Pan, W.S.; Yang, X.G. A Novel Ion-activated in Situ Gelling Ophthalmic Delivery System Based on Kappa-carrageenan for Acyclovir. Drug Dev. Ind. Pharm. 2018, 44, 829–836. [Google Scholar] [CrossRef]
- Sultana, Y.; Aqil, M.; Ali, A. Ion-activated, Gelrite®-based in Situ Ophthalmic Gels of Pefloxacin Mesylate: Comparison with Conventional Eye Drops. Drug Deliv. 2006, 13, 215–219. [Google Scholar] [CrossRef] [Green Version]
- Destruel, P.L.; Zeng, N.; Brignole-Baudouin, F.; Douat, S.; Seguin, J.; Olivier, E.; Dutot, M.; Rat, P.; Dufaÿ, S.; Dufaÿ-Wojcicki, A.; et al. In Situ Gelling Ophthalmic Drug Delivery System for the Optimization of Diagnostic and Preoperative Mydriasis: In Vitro Drug Release, Cytotoxicity and Mydriasis Pharmacodynamics. Pharmaceutics 2020, 12, 360. [Google Scholar] [CrossRef] [Green Version]
- Kompella, U.B.; Amrite, A.C.; Ravi, R.P.; Durazo, S.A. Nanomedicines for Back of the Eye Drug Delivery, Gene Delivery, and Imaging. Prog. Retin. Eye Res. 2001, 36, 172–198. [Google Scholar] [CrossRef] [Green Version]
- Andrei, G.; Peptu, C.A.; Popa, M.; Desbrieres, J.; Peptu, C.; Gardikiotis, F.; Costuleanu, M.; Costin, D.; Dupin, J.C.; Uhart, A. Formulation and Evaluation of Cefuroxim Loaded Submicron Particles for Ophthalmic Delivery. Int. J. Pharm. 2015, 493, 16–29. [Google Scholar] [CrossRef]
- Akbarzadeh, A.; Rezaei-Sadabady, R.; Davaran, S.; Joo, S.W.; Zarghami, N.; Hanifehpour, Y.; Samiei, M.; Kouhi, M.; Nejati-Koshki, K. Liposome: Classification, Preparation, and Applications. Nanoscale Res. Lett. 2013, 8, 102. [Google Scholar] [CrossRef] [Green Version]
- Feghhi, M.; Makhmalzadeh, B.S.; Farrahi, F.; Akmali, M.; Hasanvand, N. Anti-microbial Effect and in Vivo Ocular Delivery of Ciprofloxacin-loaded Liposome Through Rabbit’s Eye. Curr. Eye Res. 2020, 45, 1245–1251. [Google Scholar] [CrossRef]
- Natarajan, J.V.; Ang, M.; Darwitan, A.; Chattopadhyay, S.; Wong, T.T.; Venkatraman, S.S. Nanomedicine for Glaucoma: Liposomes Provide Sustained Release of Latanoprost in the Eye. Int. J. Nanomed. 2012, 7, 123–131. [Google Scholar]
- Shen, Y.; Tu, J.S. Preparation and Ocular Pharmacokinetics of Ganciclovir Liposomes. AAPS PharmSciTech 2007, 9, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujisawa, T.; Miyai, H.; Hironaka, K.; Tsukamoto, T.; Tahara, K.; Tozuka, Y.; Ito, M.; Takeuchi, H. Liposomal Diclofenac Eye Drop Formulations Targeting the Retina: Formulation Stability Improvement Using Surface Modification of Liposomes. Int. J. Pharm. 2012, 436, 564–567. [Google Scholar] [CrossRef] [PubMed]
- Hironaka, K.; Inokuchi, Y.; Tozuka, Y.; Shimazawa, M.; Hara, H.; Takeuchi, H. Design and evaluation of a liposomal delivery system targeting the posterior segment of the eye. J. Control. Release 2009, 136, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Elbialy, N.S.; Abdol-Azim, B.M.; Shafaa, M.W.; El Shazly, L.H.; El Shazly, A.H.; Khalil, W.A. Enhancement of the Ocular Therapeutic Effect of Prednisolone Acetate by Liposomal Entrapment. J. Biomed. Nanotechnol. 2013, 9, 2105–2116. [Google Scholar] [CrossRef] [PubMed]
- Law, S.L.; Huang, K.J.; Chiang, C.H. Acyclovir-containing Liposomes for Potential Ocular Delivery: Corneal Penetration and Absorption. J. Control. Release 2000, 63, 135–140. [Google Scholar] [CrossRef]
- Gai, X.M.; Cheng, L.Z.; Li, T.; Liu, D.D.; Wang, Y.Y.; Wang, T.J.; Pan, W.S.; Yang, X.G. In Vitro and in Vivo Studies on a Novel Bioadhesive Colloidal System: Cationic Liposomes of Ibuprofen. AAPS PharmSciTech 2018, 19, 700–709. [Google Scholar] [CrossRef]
- Khallaf, A.M.; El-Moslemany, R.M.; Ahmed, M.F.; Morsi, M.H.; Khalafallah, N.M. Exploring a Novel Fasudil-Phospholipid Complex Formulated as Liposomal Thermosensitive in situ Gel for Glaucoma. Int. J. Nanomed. 2022, 17, 163–181. [Google Scholar] [CrossRef]
- Kari, O.K.; Tavakoli, S.; Parkkila, P.; Baan, S.; Savolainen, R.; Ruoslahti, T.; Johansson, N.G.; Ndika, J.; Alenius, H.; Viitala, T.; et al. Light-Activated Liposomes Coated with Hyaluronic Acid as a Potential Drug Delivery System. Pharmaceutics 2020, 12, 763. [Google Scholar] [CrossRef]
- Lin, J.; Wu, H.J.; Wang, Y.J.; Lin, J.H.; Chen, Q.; Zhu, X. Preparation and Ocular Pharmacokinetics of Hyaluronan Acid-modified Mucoadhesive Liposomes. Drug Deliv. 2016, 23, 1144–1151. [Google Scholar] [CrossRef]
- Tan, G.; Yu, S.; Pan, H.; Li, J.; Liu, D.; Yuan, K.; Yang, X.; Pan, W. Bioadhesive Chitosan-loaded Liposomes: A More Efficient and Higher Permeable Ocular Delivery Platform for Timolol Maleate. Int. J. Biol. Macromol. 2017, 94, 355–363. [Google Scholar] [CrossRef] [PubMed]
- Londhe, V.Y.; Sharma, S. Formulation, characterization, optimization and in-vivo evaluation of methazolamide liposomal in-situ gel for treating glaucoma. J. Drug Deliv. Sci. Technol. 2022, 67, 102951. [Google Scholar] [CrossRef]
- Teesalu, T.; Sugahara, K.N.; Kotamraju, V.R.; Ruoslahti, E. C-end Rule Peptides Mediate Neuropilin-1-dependent Cell, Vascular, and Tissue Penetration. Proc. Natl. Acad. Sci. USA 2009, 106, 16157–16162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, H.; Yang, X.R.; Li, H.L.; Lu, H.S.; Oswald, J.; Liu, Y.M.; Zeng, J.; Jin, C.H.; Peng, X.C.; Liu, J.Y.; et al. iRGD decorated liposomes: A novel actively penetrating topical ocular drug delivery strategy. Nano Res. 2020, 13, 3105–3109. [Google Scholar] [CrossRef]
- Zhang, H.H.; Luo, Q.H.; Yang, Z.J.; Pan, W.S.; Nie, S.F. Novel Ophthalmic Timolol Meleate Liposomal-hydrogel and Its Improved Local Glaucomatous Therapeutic Effect in Vivo. Drug Deliv. 2011, 18, 502–510. [Google Scholar] [PubMed] [Green Version]
- Ren, T.; Lin, X.; Zhang, Q.; You, D.; Liu, X.; Tao, X.; Gou, J.; Zhang, Y.; Yin, T.; He, H.; et al. Encapsulation of Azithromycin Ion Pair in Liposome for Enhancing Ocular Delivery and Therapeutic Efficacy on Dry Eye. Mol. Pharm. 2018, 15, 4862–4871. [Google Scholar] [CrossRef] [PubMed]
- Cheng, T.; Li, J.; Cheng, Y.; Zhang, X.; Qu, Y. Triamcinolone Acetonide-chitosan Coated Liposomes Efficiently Treated Retinal Edema as Eye Drops. Exp. Eye Res. 2019, 188, 107805. [Google Scholar] [CrossRef]
- Durak, S.; Esmaeili Rad, M.; Alp Yetisgin, A.; Eda Sutova, H.; Kutlu, O.; Cetinel, S.; Zarrabi, A. Niosomal Drug Delivery Systems for Ocular Disease-recent Advances and Future Prospects. Nanomaterials 2020, 10, 1191. [Google Scholar] [CrossRef]
- Kaur, I.P.; Rana, C.; Singh, H. Development of Effective Ocular Preparations of Antifungal Agents. J. Ocul. Pharmacol. Ther. 2008, 24, 481–494. [Google Scholar] [CrossRef]
- Kaur, I.P.; Garg, A.; Singla, A.K.; Aggarwal, D. Vesicular Systems in Ocular Drug Delivery: An Overview. Int. J. Pharm. 2004, 269, 1–14. [Google Scholar] [CrossRef]
- Ameeduzzafar; Alruwaili, N.K.; Imam, S.S.; Alotaibi, N.H.; Alhakamy, N.A.; Alharbi, K.S.; Afzal, M.; Alenezi, S.K.; Bukhari, S.N.A. Formulation of Chitosan Polymeric Vesicles of Ciprofloxacin for Ocular Delivery: Box-behnken Optimization, in Vitro Characterization, HET-CAM Irritation, and Antimicrobial Assessment. AAPS PharmSciTech 2020, 21, 167. [Google Scholar] [CrossRef] [PubMed]
- Allam, A.; Elsabahy, M.; El Badry, M.; Eleraky, N.E. Betaxolol-loaded Niosomes Integrated within PH-sensitive in Situ Forming Gel for Management of Glaucoma. Int. J. Pharm. 2021, 598, 120380. [Google Scholar] [CrossRef] [PubMed]
- Abdelbary, G.; El-Gendy, N. Niosome-encapsulated Gentamicin for Ophthalmic Controlled Delivery. AAPS PharmSciTech 2008, 9, 740–747. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, D.; Pal, D.; Mitra, A.K.; Kaur, I.P. Study of the Extent of Ocular Absorption of Acetazolamide from a Developed Niosomal Formulation, by Microdialysis Sampling of Aqueous Humor. Int. J. Pharm. 2007, 338, 21–26. [Google Scholar] [CrossRef]
- Elmotasem, H.; Awad, G.E.A. A stepwise optimization strategy to formulate in situ gelling formulations comprising flucona-zole-hydroxypropyl-beta-cyclodextrin complex loaded niosomal vesicles and Eudragit nanoparticles for enhanced antifungal activity and prolonged ocular delivery. Asian J. Pharm. Sci. 2020, 15, 617–636. [Google Scholar] [CrossRef]
- Zeng, W.; Li, Q.; Wan, T.; Liu, C.; Pan, W.; Wu, Z.; Xu, Y. Hyaluronic Acid-coated Niosomes Facilitate Tacrolimus Ocular Delivery: Mucoadhesion, Precorneal Retention, Aqueous Humor Pharmacokinetics, and Transcorneal Permeability. Colloids Surf. B Biointerfaces 2016, 141, 28–35. [Google Scholar] [CrossRef]
- Gupta, P.; Yadav, K.S. Formulation and evaluation of brinzolamide encapsulated niosomal in-situ gel for sustained reduction of IOP in rabbits. J. Drug Deliv. Sci. Technol. 2022, 67, 103004. [Google Scholar] [CrossRef]
- Fathalla, D.; Fouad, E.A.; Soliman, G.M. Latanoprost Niosomes as a Sustained Release Ocular Delivery System for the Management of Glaucoma. Drug Dev. Ind. Pharm. 2020, 46, 806–813. [Google Scholar] [CrossRef]
- Sawant, K.K.; Dodiya, S.S. Recent advances and patents on solid lipid nanoparticles. Recent Pat. Drug Deliv. Formul. 2008, 2, 120–135. [Google Scholar] [CrossRef]
- Müller, R.H.; Radtke, M.; Wissing, S.A. Nanostructured lipid matrices for improved microencapsulation of drugs. Int. J. Pharm. 2002, 242, 121–128. [Google Scholar] [CrossRef]
- El-Salamouni, N.S.; Farid, R.M.; El-Kamel, A.H.; El-Gamal, S.S. Nanostructured lipid carriers for intraocular brimonidine localization; development, in-vitro and in-vivo evaluation. J. Microencapsul. 2018, 35, 102–113. [Google Scholar] [CrossRef] [PubMed]
- Kakkar, S.; Karuppayil, S.M.; Raut, J.S.; Giansanti, F.; Papucci, L.; Schiavone, N.; Kaur, I.P. Lipid-polyethylene Glycol Based Nano-ocular Formulation of Ketoconazole. Int. J. Pharm. 2015, 495, 276–289. [Google Scholar] [CrossRef] [PubMed]
- Puglia, C.; Blasi, P.; Ostacolo, C.; Sommella, E.; Bucolo, C.; Platania, C.B.M.; Romano, G.L.; Geraci, F.; Drago, F.; Santonocito, D.; et al. Innovative Nanoparticles Enhance N-palmitoyleth Anolamide Intraocular Delivery. Front. Pharmacol. 2018, 9, 285. [Google Scholar] [CrossRef] [PubMed]
- Kalam, M.A.; Sultana, Y.; Ali, A.; Aqil, M.; Mishra, A.K.; Chuttani, K. Preparation, characterization, and evaluation of gatifloxacin loaded solid lipid nanoparticles as colloidal ocular drug delivery system. J. Drug. Target. 2010, 18, 191–204. [Google Scholar] [CrossRef]
- Tamilvanan, S.; Kumar, B.A. Influence of acetazolamide loading on the (in vitro) performances of non-phospholipid-based cationic nanosized emulsion in comparison with phospholipid-based anionic and neutral-charged nanosized emulsions. Drug Dev. Ind. Pharm. 2011, 37, 1003–1015. [Google Scholar] [CrossRef]
- Almeida, H.; Lobão, P.; Frigerio, C.; Fonseca, J.; Silva, R.; Sousa Lobo, J.M.; Amaral, M.H. Preparation, Characterization and Biocompatibility Studies of Thermoresponsive Eyedrops Based on the Combination of Nanostructured Lipid Carriers (NLC) and the Polymer Pluronic F-127 for Controlled Delivery of Ibuprofen. Pharm. Dev. Technol. 2017, 22, 336–349. [Google Scholar] [CrossRef]
- Liu, D.; Li, J.; Cheng, B.; Wu, Q.Y.; Pan, H. Ex Vivo and in Vivo Evaluation of the Effect of Coating a Coumarin-6-labeled Nanostructured Lipid Carrier with Chitosan-N-acetylcysteine on Rabbit Ocular Distribution. Mol. Pharm. 2017, 14, 2639–2648. [Google Scholar] [CrossRef]
- Battaglia, L.; D’Addino, I.; Peira, E.; Trotta, M.; Gallarate, M. Solid lipid nanoparticles prepared by coacervation method as vehicles for ocular cyclosporine. J. Drug Deliv. Sci. Technol. 2012, 22, 125–130. [Google Scholar] [CrossRef]
- Delgado, D.; del Pozo-Rodríguez, A.; Solinís, M.Á.; Avilés-Triqueros, M.; Weber, B.H.; Fernández, E.; Gascón, A.R. Dextran and protamine-based solid lipid nanoparticles as potential vectors for the treatment of X-linked juvenile retinoschisis. Hum. Gene Ther. 2012, 23, 345–355. [Google Scholar] [CrossRef]
- Wang, F.; Chen, L.; Jiang, S.; He, J.; Zhang, X.; Peng, J.; Xu, Q.; Li, R. Optimization of Methazolamide-loaded Solid Lipid Nanoparticles for Ophthalmic Delivery Using Box-behnken Design. J. Liposome Res. 2014, 24, 171–181. [Google Scholar] [CrossRef]
- Li, R.; Jiang, S.; Liu, D.; Bi, X.; Wang, F.; Zhang, Q.; Xu, Q. A Potential New Therapeutic System for Glaucoma: Solid Lipid Nanoparticles Containing Methazolamide. J. Microencapsul. 2010, 28, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Yadav, M.; Schiavone, N.; Guzman-Aranguez, A.I.G.; Giansanti, F.; Papucci, L.; Perez de Lara, M.J.; Kaur, I.P. Atorvastatin-loaded Solid Lipid Nanoparticles as Eye Drops: Proposed Treatment Option for Age-related Macular Degeneration (AMD). Drug Deliv. Transl. Res. 2020, 10, 919–944. [Google Scholar] [CrossRef] [PubMed]
- Araújo, J.; Nikolic, S.; Egea, M.A.; Souto, E.B.; Garcia, M.L. Nanostructured Lipid Carriers for Triamcinolone Acetonide Delivery to the Posterior Segment of the Eye. Colloids Surf. B Biointerfaces 2011, 88, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Swetledge, S.; Jung, J.P.; Carter, R.; Sabliov, C. Distribution of Polymeric Nanoparticles in the Eye: Implications in Ocular Disease Therapy. J. Nanobiotechnology 2021, 19, 10. [Google Scholar] [CrossRef] [PubMed]
- Asasutjarit, R.; Theerachayanan, T.; Kewsuwan, P.; Veeranondha, S.; Fuongfuchat, A.; Ritthidej, G.C. Gamma Sterilization of Diclofenac Sodium Loaded-N-trimethyl Chitosan Nanoparticles for Ophthalmic Use. Carbohydr. Polym. 2017, 157, 603–612. [Google Scholar] [CrossRef]
- Ogunjimi, A.T.; Melo, S.M.G.; Vargas-Rechia, C.G.; Emery, F.S.; Lopez, R.F.V. Hydrophilic Polymeric Nanoparticles Prepared from Delonix Galactomannan with Low Cytotoxicity for Ocular Drug Delivery. Carbohydr. Polym. 2017, 157, 1065–1075. [Google Scholar] [CrossRef]
- Kalam, M.A. Development of Chitosan Nanoparticles Coated with Hyaluronic Acid for Topical Ocular Delivery of Dexamethasone. Int. J. Biol. Macromol. 2016, 89, 127–136. [Google Scholar] [CrossRef]
- Canfarotta, F.; Whitcombe, M.J.; Piletsky, S.A. Polymeric Nanoparticles for Optical Sensing. Biotechnol. Adv. 2013, 31, 1585–1599. [Google Scholar] [CrossRef] [Green Version]
- Zamboulis, A.; Nanaki, S.; Michailidou, G.; Koumentakou, I.; Lazaridou, M.; Ainali, N.M.; Xanthopoulou, E.; Bikiaris, D.N. Chitosan and its Derivatives for Ocular Delivery Formulations: Recent Advances and Developments. Polymers 2020, 12, 1519. [Google Scholar] [CrossRef]
- Ameeduzzafar; Ali, J.; Bhatnagar, A.; Kumar, N.; Ali, A. Chitosan nanoparticles amplify the ocular hypotensive effect of cateolol in rabbits. Int. J. Biol. Macromol. 2014, 65, 479–491. [Google Scholar] [CrossRef]
- Karava, A.; Lazaridou, M.; Nanaki, S.; Michailidou, G.; Christodoulou, E.; Kostoglou, M.; Iatrou, H.; Bikiaris, D.N. Chitosan Derivatives with Mucoadhesive and Antimicrobial Properties for Simultaneous Nanoencapsulation and Extended Ocular Release Formulations of Dexamethasone and Chloramphenicol Drugs. Pharmaceutics 2020, 12, 594. [Google Scholar] [CrossRef] [PubMed]
- Yuan, X.B.; Yuan, Y.B.; Jiang, W.; Liu, J.; Tian, E.J.; Shun, H.M.; Huang, D.H.; Yuan, X.Y.; Li, H.; Sheng, J. Preparation of rapamycin-loaded chitosan/PLA nanoparticles for immunosuppression in corneal transplantation. Int. J. Pharm. 2008, 349, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Tahara, K.; Karasawa, K.; Onodera, R.; Takeuchi, H. Feasibility of drug delivery to the eye’s posterior segment by topical instillation of PLGA nanoparticles. Asian J. Pharm. Sci. 2017, 12, 394–399. [Google Scholar] [CrossRef] [PubMed]
- Musumeci, T.; Bucolo, C.; Carbone, C.; Pignatello, R.; Drago, F.; Puglisi, G. Polymeric Nanoparticles Augment the Ocular Hypotensive Effect of Melatonin in Rabbits. Int. J. Pharm. 2013, 440, 135–140. [Google Scholar] [CrossRef]
- Kompella, U.B.; Sundaram, S.; Raghava, S.; Escobar, E.R. Luteinizing Hormone-releasing Hormone Agonist and Transferrin Functionalizations Enhance Nanoparticle Delivery in a Novel Bovine ex Vivo Eye Model. Mol. Vis. 2006, 12, 1185–1198. [Google Scholar]
- Sharma, A.; Tandon, A.; Tovey, J.C.; Gupta, R.; Robertson, J.D.; Fortune, J.A.; Klibanov, A.M.; Cowden, J.W.; Rieger, F.G.; Mohan, R.R. Polyethylenimine-conjugated Gold Nanoparticles: Gene Transfer Potential and Low Toxicity in the Cornea. Nanomedicine 2011, 7, 505–513. [Google Scholar] [CrossRef] [Green Version]
- Nagarwal, R.C.; Singh, P.N.; Kant, S.; Maiti, P.; Pandit, J.K. Chitosan Nanoparticles of 5-fluorouracil for Ophthalmic Delivery: Characterization, in-vitro and in-vivo Study. Pharm. Bull. 2011, 59, 272–278. [Google Scholar] [CrossRef] [Green Version]
- Silva, N.C.; Silva, S.; Sarmento, B.; Pintado, M. Chitosan Nanoparticles for Daptomycin Delivery in Ocular Treatment of Bacterial Endophthalmitis. Drug Deliv. 2015, 22, 885–893. [Google Scholar] [CrossRef] [Green Version]
- Cañadas, C.; Alvarado, H.; Calpena, A.C.; Silva, A.M.; Souto, E.B.; García, M.L.; Abrego, G. In Vitro, ex Vivo and in Vivo Characterization of PLGA Nanoparticles Loading Pranoprofen for Ocular Administration. Int. J. Pharm. 2016, 511, 719–727. [Google Scholar] [CrossRef]
- Ammar, H.O.; El-Nahhas, S.; Ghorab, M.; Salama, A. Chitosan/cyclodextrin Nanoparticles as Drug Delivery System. J. Incl. Phenom. Macrocycl. Chem. 2012, 72, 127–136. [Google Scholar] [CrossRef]
- DiPrima, G.; Saladino, S.; Bongiovi, F.; Adamo, G.; Ghersi, G.; Pitarresi, G.; Giammona, G. Novel Inulin-based Mucoadhesive Micelles Loaded with Corticosteroids as Potential Transcorneal Permeation Enhancers. Eur. J. Pharm. Biopharm. 2017, 117, 385–399. [Google Scholar] [CrossRef] [PubMed]
- Durgun, M.E.; Gungor, S.; Ozsoy, Y. Micelles: Promising Ocular Drug Carriers for Anterior and Posterior Segment Diseases. J. Ocul. Pharmacol. Ther. 2020, 36, 323–341. [Google Scholar] [CrossRef] [PubMed]
- Mandal, A.; Bisht, R.; Rupenthal, I.D.; Mitra, A.K. Polymeric Micelles for Ocular Drug Delivery: From Structural Frameworks to Recent Preclinical Studies. J. Control. Release 2017, 28, 96–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.Y.; Xu, X.Y.; Gu, Y.; Cheng, Y.J.; Cao, F. Recent Advance of Nanoparticle-based Topical Drug Delivery to the Posterior Segment of the Eye. Expert Opin. Drug Deliv. 2018, 15, 687–701. [Google Scholar] [CrossRef]
- Di Tommaso, C.; Torriglia, A.; Furrer, P.; Behar-Cohen, F.; Gurny, R.; Moller, M. Ocular Biocompatibility of Novel Cyclosporin A Formulations Based on Methoxy Poly(ethylene glycol)-hexylsubstituted Poly(lactide) Micelle Carriers. Int. J. Pharm. 2011, 416, 515–524. [Google Scholar] [CrossRef]
- Zhang, F.; Chen, H.; Lan, J.; Song, K.; Wu, X. Preparation and in vitro/in vivo evaluations of novel ocular micelle formulations of hesperetin with glycyrrhizin as a nanocarrier. Exp. Eye Res. 2021, 202, 108313. [Google Scholar] [CrossRef]
- Earla, R.; Boddu, S.H.; Cholkar, K.; Hariharan, S.; Jwala, J.; Mitra, A.K. Development and Validation of a Fast and Sensitive Bioanalytical Method for the Quantitative Determination of Glucocorticoids Quantitative Measurement of Dexamethasone in Rabbit Ocular Matrices by Liquid Chromatography Tandem Mass Spectrometry. J. Pharm. Biomed. Anal. 2010, 52, 525–533. [Google Scholar] [CrossRef] [Green Version]
- Cholkar, K.; Gunda, S.; Earla, R.; Pal, D.; Mitra, A.K. Nanomicellar Topical Aqueous Drop Formulation of Rapamycin for Back-of-the-eye Delivery. AAPS PharmSciTech 2015, 16, 610–622. [Google Scholar] [CrossRef] [Green Version]
- Patel, S.; Garapati, C.; Chowdhury, P.; Gupta, H.; Nesamony, J.; Nauli, S.; Boddu, S.H.S. Development and Evaluation of Dexamethasone Nanomicelles with Potential for Treating Posterior Uveitis after Topical Application. J. Ocul. Pharmacol. Ther. 2015, 31, 215–227. [Google Scholar] [CrossRef]
- Pepić, I.; Hafner, A.; Lovric, J.; Pirkic, B.; Filipovic-Grcic, J. A Nonionic Surfactant/chitosan Micelle System in an Innovative Eye Drop Formulation. J. Pharm. Sci. 2010, 99, 4317–4325. [Google Scholar] [CrossRef]
- Mandal, A.; Cholkar, K.; Khurana, V.; Shah, A.; Agrahari, V.; Bisht, R.; Pal, D.; Mitra, A.K. Topical Formulation of Self-assembled Antiviral Prodrug Nanomicelles for Targeted Retinal Delivery. Mol. Pharm. 2017, 14, 2056–2069. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zheng, Y.; Zhang, L.; Wang, Q.; Zhang, D. Stability of Nanosuspensions in Drug Delivery. J. Control. Release 2013, 172, 1126–1141. [Google Scholar] [CrossRef] [PubMed]
- Yue, P.F.; Li, G.; Dan, J.X.; Wu, Z.F.; Wang, C.H.; Zhu, W.F.; Yang, M. Study on Formability of Solid Nanosuspensions During Solidification: II Novel Roles of Freezing Stress and Cryoprotectant Property. Int. J. Pharm. 2014, 475, 35–48. [Google Scholar] [CrossRef] [PubMed]
- Yue, P.F.; Wan, J.; Wang, Y.; Li, Y.; Ma, Y.Q.; Yang, M.; Hu, P.Y.; Yuan, H.L.; Wang, C.H. D-alpha-tocopherol Acid Polyethylene Glycol 1000 Succinate, An Effective Stabilizer During Solidification Transformation of Baicalin Nanosuspensions. Int. J. Pharm. 2013, 443, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Pignatello, R.; Bucolo, C.; Puglisi, G. Ocular Tolerability of Eudragit RS100® and RL100® Nanosuspensions as Carriers for Ophthalmic Controlled Drug Delivery. J. Pharm. Sci. 2002, 91, 2636–2641. [Google Scholar] [CrossRef]
- Kassem, M.A.; Abdel Rahman, A.A.; Ghorab, M.M.; Ahmed, M.B.; Khalil, R.M. Nanosuspension as an ophthalmic delivery system for certain glucocorticoid drugs. Int. J. Pharm. 2007, 340, 126–133. [Google Scholar] [CrossRef]
- Romero, G.B.; Keck, C.M.; Müller, R.H.; Bou-Chacra, N.A. Development of cationic nanocrystals for ocular delivery. Eur. J. Pharm. Biopharm. 2016, 107, 215–222. [Google Scholar] [CrossRef]
- Pignatello, R.; Bucolo, C.; Spedalieri, G.; Maltese, A.; Puglisi, G. Flurbiprofen-loaded Acrylate Polymer Nanosuspensions for Ophthalmic Application. Biomaterials 2002, 23, 3247–3255. [Google Scholar] [CrossRef]
- Shi, S.; Zhang, Z.L.; Luo, Z.C.; Yu, J.; Liang, R.L.; Li, X.Y.; Chen, H. Chitosan Grafted Methoxy Poly(ethylene glycol)-poly(epsilon-caprolactone) Nanosuspension for Ocular Delivery of Hydrophobic Diclofenac. Sci. Rep. 2015, 5, 113–137. [Google Scholar]
- Ali, H.S.M.; York, P.; Ali, A.M.A.; Blagden, N. Hydrocortisone Nanosuspensions for Ophthalmic Delivery: A Comparative Study between Microfluidic Nanoprecipitation and Wet Milling. J. Control. Release 2011, 149, 175–181. [Google Scholar] [CrossRef]
- Kumar, R.; Sinha, V.R. Preparation and Optimization of Voriconazole Microemulsion for Ocular Delivery. Colloids Surf. B Biointerfaces 2014, 117, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Gore, A.; Attar, M.; Pujara, C.; Neervannan, S. Comment on “quality by design approach for understanding the critical quality attributes of cyclosporine ophthalmic emulsion”. Mol. Pharm. 2014, 11, 2490–2492. [Google Scholar] [CrossRef] [PubMed]
- Bachu, R.D.; Stepanski, M.; Alzhrani, R.M.; Jung, R.; Boddu, S.H.S. Development and Evaluation of a Novel Microemulsion of Dexamethasone and Tobramycin for Topical Ocular Administration. J. Ocul. Pharmacol. Ther. 2018, 34, 312–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yin, J.; Xiang, C.; Lu, G. Cationic Lipid Emulsions as Potential Bioadhesive Carriers for Ophthalmic Delivery of Palmatine. J. Microencapsul. 2016, 33, 718–724. [Google Scholar] [CrossRef]
- Li, C.C.; Abrahamson, M.; Kapoor, Y.; Chauhan, A. Timolol Transport from Microemulsions Trapped in HEMA Gels. J. Colloid Interface Sci. 2007, 315, 297–306. [Google Scholar] [CrossRef]
- Kalam, M.A.; Alshamsan, A.; Aljuffali, I.A.; Mishra, A.K.; Sultana, Y. Delivery of Gatifloxacin Using Microemulsion as Vehicle: Formulation, Evaluation, Transcorneal Permeation and Aqueous Humor Drug Determination. Drug Deliv. 2016, 23, 896–907. [Google Scholar] [CrossRef]
- Fialho, S.L.; Silva-Cunha, A. New Vehicle Based on a Microemulsion for Topical Ocular Administration of Dexamethasone. Clin. Exp. Ophthalmol. 2004, 32, 626–632. [Google Scholar] [CrossRef]
- Badawi, A.A.; El-Laithy, H.M.; El Qidra, R.K.; El Mofty, H.; El Dally, M. Chitosan based nanocarriers for indomethacin ocular delivery. Arch. Pharm Res. 2008, 3, 1040–1049. [Google Scholar] [CrossRef]
- Ying, L.; Tahara, K.; Takeuchi, H. Drug Delivery to the Ocular Posterior Segment Using Lipid Emulsion via Eye Drop Administration: Effect of Emulsion Formulations and Surface Modification. Int. J. Pharm. 2013, 453, 329–335. [Google Scholar] [CrossRef]
- Dhaval, M.; Devani, J.; Parmar, R.; Soniwala, M.M.; Chavda, J. Formulation, and optimization of microemulsion based sparfloxacin in-situ gel for ocular delivery: In vitro and ex vivo characterization. J. Drug Deliv. Sci. Technol. 2020, 55, 101373. [Google Scholar] [CrossRef]
- Gan, L.; Gan, Y.; Zhu, C.; Zhang, X.; Zhu, J. Novel Microemulsion in Situ Electrolyte-triggered Gelling System for Ophthalmic Delivery of Lipophilic Cyclosporine A: In Vitro and in Vivo Results. Int. J. Pharm. 2009, 365, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Tajika, T.; Isowaki, A.; Sakaki, H. Ocular Distribution of Difluprednate Ophthalmic Emulsion 0.05% in Rabbits. J. Ocul. Pharmacol. Ther. 2011, 27, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Kesavan, K.; Kant, S.; Singh, P.N.; Pandit, J.K. Mucoadhesive Chitosancoated Cationic Microemulsion of Dexamethasone for Ocular Delivery: In Vitro and in Vivo Evaluation. Curr. Eye Res. 2013, 38, 342–352. [Google Scholar] [CrossRef] [PubMed]
- Buech, G.; Bertelmann, E.; Pleyer, U.; Siebenbrodt, I.; Borchert, H.H. Formulation of Sirolimus Eye Drops and Corneal Permeation Studies. J. Ocul. Pharmacol. Ther. 2007, 23, 292–303. [Google Scholar] [CrossRef]
- Rodríguez Villanueva, J.; Navarro, M.G.; Rodríguez Villanueva, L. Dendrimers as a Promising Tool in Ocular Therapeutics: Latest Advances and Perspectives. Int. J. Pharm. 2016, 511, 359–366. [Google Scholar] [CrossRef]
- Alhalafi, A.M. Applications of Polymers in Intraocular Drug Delivery Systems. Oman J. Ophthalmol. 2017, 10, 3–8. [Google Scholar] [CrossRef]
- Chaplot, S.P.; Rupenthal, I.D. Dendrimers for Gene Delivery-a Potential Approach for Ocular Therapy? J. Pharm. Pharmacol. 2014, 66, 542–556. [Google Scholar] [CrossRef]
- Bravo-Osuna, I.; Vicario-de-la-Torre, M.; Andres-Guerrero, V.; Sanchez-Nieves, J.; Guzman-Navarro, M.; de la Mata, F.J.; Gomez, R.; de las Heras, B.; Argueso, P.; Ponchel, G.; et al. Novel Water-soluble Mucoadhesive Carbosilane Dendrimers for Ocular Administration. Mol. Pharm. 2016, 13, 2966–2976. [Google Scholar] [CrossRef]
- Jevprasesphant, R.; Penny, J.; Jalal, R.; Attwood, D.; McKeown, N.B.; D’Emanuele, A. The Influence of Surface Modification on the Cytotoxicity of PAMAM Dendrimers. Int. J. Pharm. 2003, 252, 263–266. [Google Scholar] [CrossRef]
- Froehlich, E.; Mandeville, J.S.; Jennings, C.J.; Sedaghat-Herati, R.; Tajmir-Riahi, H.A. Dendrimers Bind Human Serum Albumin. J. Phys. Chem. 2009, 113, 6986–6993. [Google Scholar] [CrossRef]
- Iezzi, R.; Guru, B.R.; Glybina, I.V.; Mishra, M.K.; Kennedy, A.; Kannan, R.M. Dendrimer-based Targeted Intravitreal Therapy for Sustained Attenuation of Neuroinflammation in Retinal Degeneration. Biomaterials 2012, 33, 979–988. [Google Scholar] [CrossRef] [PubMed]
- Vandamme, T.F.; Brobeck, L. Poly(amidoamine) Dendrimers as Ophthalmic Vehicles for Ocular Delivery of Pilocarpine Nitrate and Tropicamide. J. Control. Release 2005, 102, 23–38. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.Y.; Yao, C.; Shao, Y.F.; Mu, H.J.; Sun, K.X. Determination of Puerarin in Rabbit Aqueous Humor by Liquid Chromatography Tandem Mass Spectrometry Using Microdialysis Sampling after Topical Administration of Puerarin PAMAM Dendrimer Complex. J. Pharm. Biomed. Anal. 2011, 56, 825–829. [Google Scholar] [CrossRef] [PubMed]
- Yavuz, B.; Pehlivan, S.B.; Vural, I.; Unlu, N. In Vitro/in Vivo Evaluation of Dexamethasone-PAMAM Dendrimer Complexes for Retinal Drug Delivery. J. Pharm. Sci. 2015, 104, 3814–3823. [Google Scholar] [CrossRef]
- Liu, C.; Jiang, K.; Tai, L.; Liu, Y.; Wei, G.; Lu, W.Y.; Pan, W.S. Facile Noninvasive Retinal Gene Delivery Enabled by Penetratin. ACS Appl. Mate. Interfaces 2016, 8, 19256–19267. [Google Scholar] [CrossRef]
- Durairaj, C.; Kadam, R.S.; Chandler, J.W.; Hutcherson, S.L.; Kompella, U.B. Nanosized Dendritic Polyguanidilyated Translocators for Enhanced Solubility, Permeability and Delivery of Gatifloxacin. Investig. Ophthalmol. Vis. Sci. 2010, 51, 5804–5816. [Google Scholar] [CrossRef] [Green Version]





| Model Drugs | Prodrugs | Indications | Main Findings | Ref. |
|---|---|---|---|---|
| Anterior segment | ||||
 Brinzolamide |  TML prodrug | Glaucoma | Prodrug penetrated corneal tissue more easily and was approximately five times more effective in reducing IOP than commercial eye drops. | [45] |
 L-carnosine |  NAC | Cataracts | The intraocular retention time was prolonged, corneal permeability was increased, and bioavailability was significantly improved. | [46] |
| Posterior segment | ||||
 E2 |  DHED | Retinal neuroprotection | Prodrug protected the retina more effectively and safely. | [52] |
 GFX |  DMAP-GFX  CP-GFX  APM-GFX | Eye inflammation caused by the vitreous humor | The solubility and LogD of the drug were increased. Of the three prodrugs, DMAP-GFX could deliver the drug to the posterior part of the eye via OCT-mediated transport. | [53] |
| Model Drugs | Indications | Main Findings | Ref. |
|---|---|---|---|
| Anterior segment | |||
| Econazole nitrate | Eye infections | β-CD and HP-β-CD increased the solubility of EC by approximately threefold and fourfold, respectively. | [55] |
| Fluconazole | Eye infections | The retention time in front of the cornea was prolonged. | [56] |
| Latanoprost | Glaucoma | Stability and ocular bioavailability were higher than those of commercial eye drops. | [63] |
| Tacrolimus | Dry eye | Solubility was increased by approximately 42-fold. | [64] |
| Diclofenac sodium | Eye inflammations | Solubility was increased by approximately 20-fold. | [65] |
| Posterior segment | |||
| Dexamethasone | Macular edema and branch retinal vein occlusion | More drugs were delivered to the retinal tissue. | [57] |
| Dexamethasone | Diabetic macular edema | The patient tolerated it well, with a reduction in central macular thickness and improved vision. | [66] |
| Celecoxib | Age-related macular degeneration and diabetic retinopathy | The amount of drug passing through semipermeable membranes, simulated vitreous, and sclera was increased. | [67] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.; Wang, C. Novel Eye Drop Delivery Systems: Advance on Formulation Design Strategies Targeting Anterior and Posterior Segments of the Eye. Pharmaceutics 2022, 14, 1150. https://doi.org/10.3390/pharmaceutics14061150
Wang Y, Wang C. Novel Eye Drop Delivery Systems: Advance on Formulation Design Strategies Targeting Anterior and Posterior Segments of the Eye. Pharmaceutics. 2022; 14(6):1150. https://doi.org/10.3390/pharmaceutics14061150
Chicago/Turabian StyleWang, Yaru, and Changhong Wang. 2022. "Novel Eye Drop Delivery Systems: Advance on Formulation Design Strategies Targeting Anterior and Posterior Segments of the Eye" Pharmaceutics 14, no. 6: 1150. https://doi.org/10.3390/pharmaceutics14061150