
Ciprofloxacin in Patients Undergoing Extracorporeal Membrane Oxygenation (ECMO): A Population Pharmacokinetic Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting and Study Population
2.2. Extracorporeal Membrane Oxygenation Circuit
2.3. Dosing, Administration, and Data Collection
2.4. Sample Collection and Measurements
2.5. Population Pharmacokinetic Modeling
2.6. Probability of Target Attainment (PTA) Analysis
3. Results
3.1. Study Population and Pharmacokinetic Data
3.2. Population Pharmacokinetic Analysis
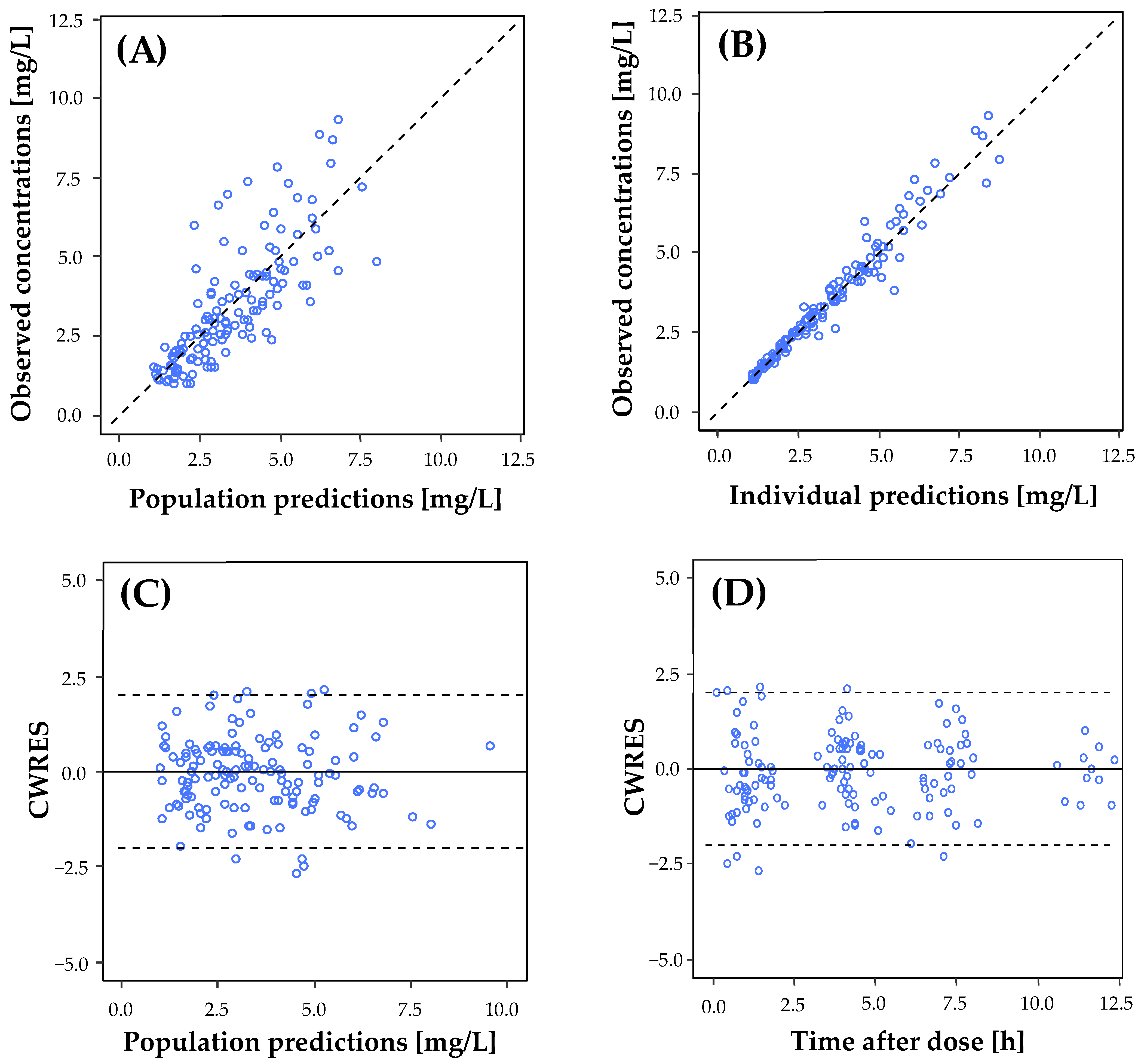
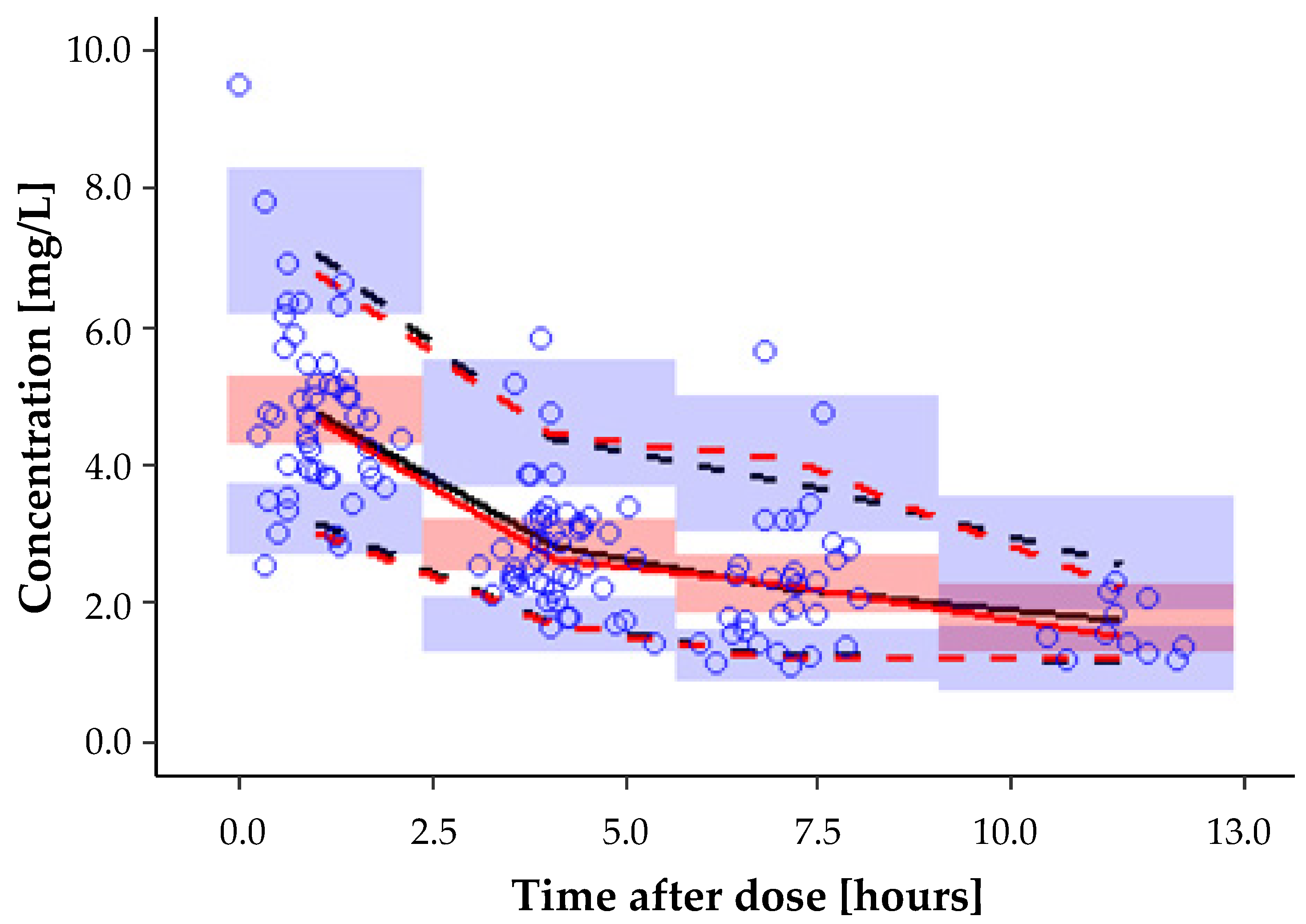
3.3. Model Evaluation
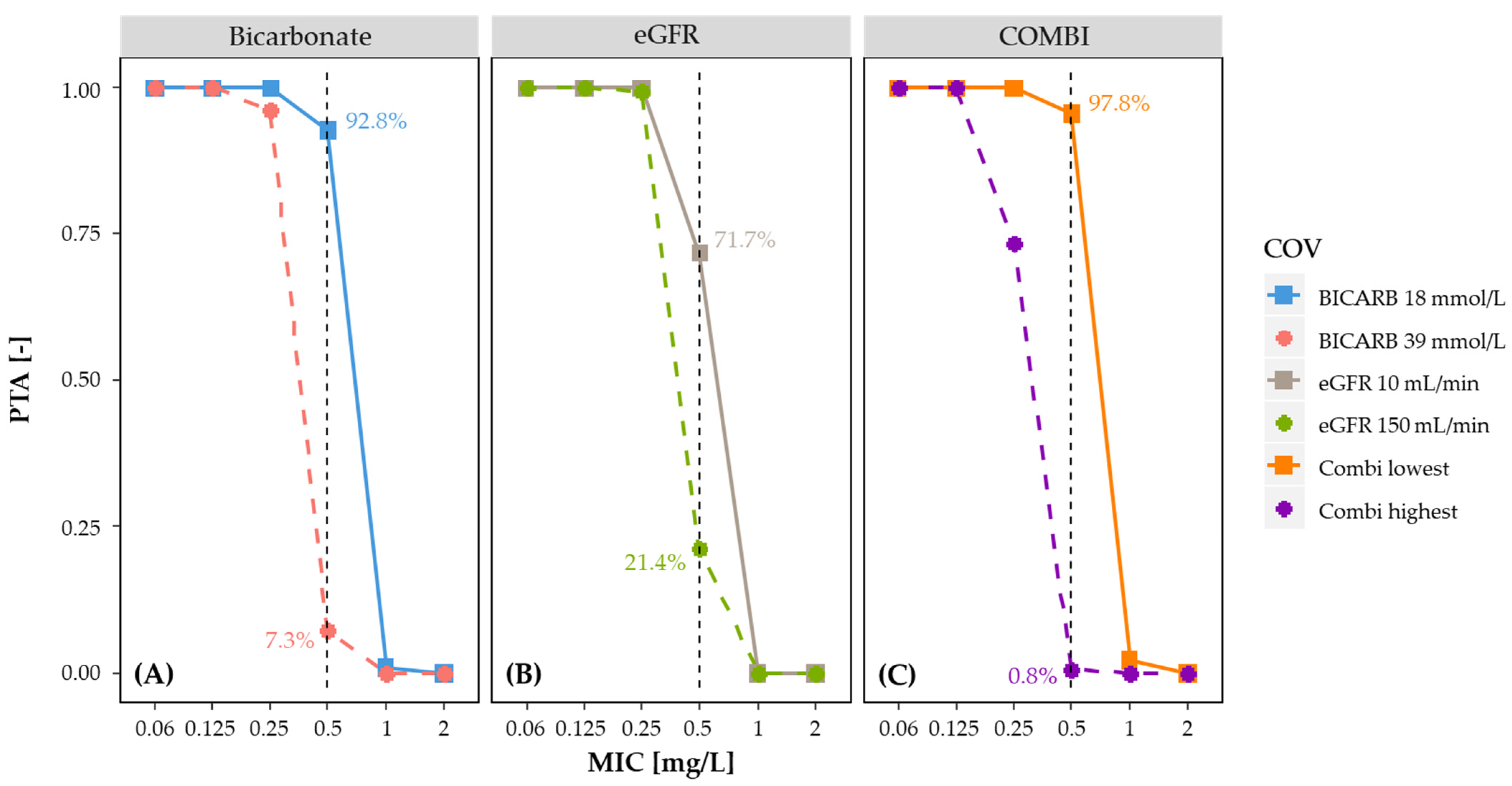
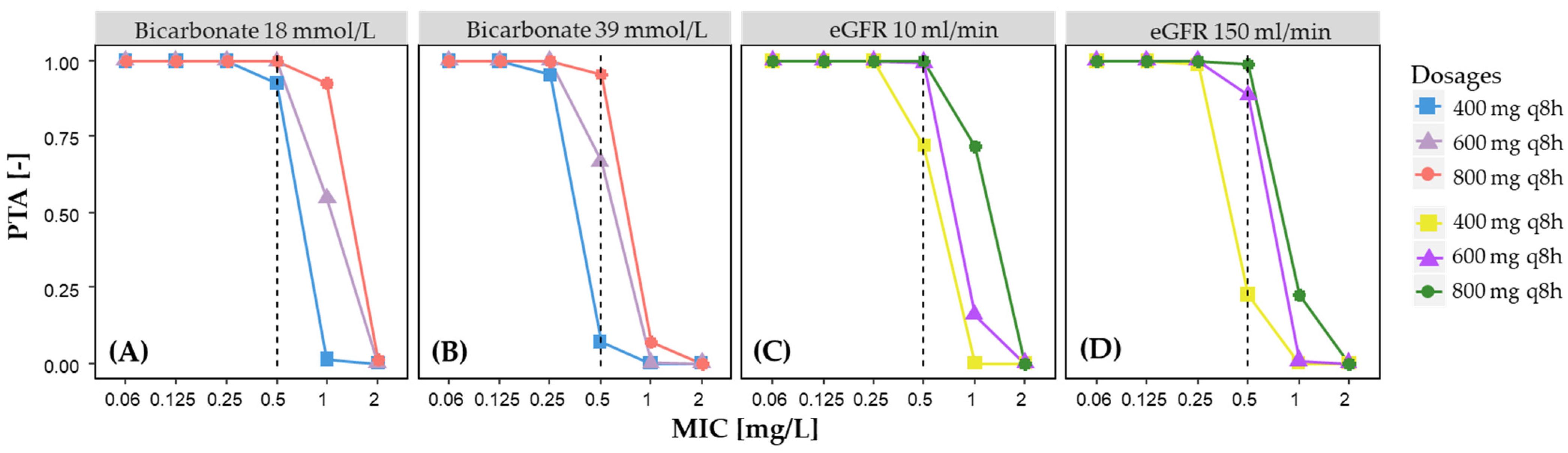
3.4. Probability of Target Attainment (PTA)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- Fraser, J.F.; Shekar, K.; Diab, S.; Dunster, K.; Foley, S.R.; McDonald, C.I.; Passmore, M.; Simonova, G.; Roberts, J.A.; Platts, D.G.; et al. ECMO-the Clinician’s View. ISBT Sci. Ser. 2012, 7, 82–88. [Google Scholar] [CrossRef]
- Kollef, M.H.; Sherman, G.; Ward, S.; Fraser, V.J. Inadequate Antimicrobial Treatment of Infections: A Risk Factor for Hospital Mortality among Critically III Patients. Chest 1999, 115, 462–474. [Google Scholar] [CrossRef]
- Biffi, S.; Di Bella, S.; Scaravilli, V.; Peri, A.M.; Grasselli, G.; Alagna, L.; Pesenti, A.; Gori, A. Infections during Extracorporeal Membrane Oxygenation: Epidemiology, Risk Factors, Pathogenesis and Prevention. Int. J. Antimicrob. Agents 2017, 50, 9–16. [Google Scholar] [CrossRef]
- Roberts, J.A.; Kruger, P.; Paterson, D.L.; Lipman, J. Antibiotic Resistance—What’s Dosing Got to Do with It? Crit. Care Med. 2008, 36, 2433–2440. [Google Scholar] [CrossRef]
- Roberts, J.A.; Lipman, J. Pharmacokinetic Issues for Antibiotics in the Critically Ill Patient. Crit. Care Med. 2009, 37, 840–851. [Google Scholar] [CrossRef] [Green Version]
- Ott, S.R.; Bodmann, K.-F.; Grabein, B.; Höffken, G.; Kolditz, M.; Lode, H.; Pletz, M.W.; Thalhammer, F. S2k Guidelines for Respiratory Infections. Excerpts from the S2k Guidelines for “Calculated Parenteral Initial Treatment of Bacterial Infections in Adults-Update 2018”. GMS Infect. Dis. 2020, 8, 90–115. [Google Scholar] [CrossRef]
- Cruciani, M.; Bassetti, D. The Fluoroquinolones as Treatment for Infections Caused by Gram-Positive Bacteria. J. Antimicrob. Chemother. 1994, 33, 403–417. [Google Scholar] [CrossRef]
- Ambrose, P.G.; Grasela, D.M.; Grasela, T.H.; Passarell, J.; Mayer, H.B.; Pierce, P.F. Pharmacodynamics of Fluoroquinolones against Streptococcus Pneumoniae in Patients with Community-Acquired Respiratory Tract Infections. Antimicrob. Agents Chemother. 2001, 45, 2793–2797. [Google Scholar] [CrossRef] [Green Version]
- Zelenitsky, S.A.; Ariano, R.E. Support for Higher Ciprofloxacin AUC24/MIC Targets in Treating Enterobacteriaceae Bloodstream Infection. J. Antimicrob. Chemother. 2010, 65, 1725–1732. [Google Scholar] [CrossRef] [Green Version]
- Forrest, A.; Nix, D.E.; Ballow, C.H.; Goss, T.F.; Birmingham, M.C.; Schentag, J.J. Pharmacodynamics of Intravenous Ciprofloxacin in Seriously Ill Patients. Antimicrob. Agents Chemother. 1993, 37, 1073–1081. [Google Scholar] [CrossRef] [Green Version]
- Sharma, P.C.; Jain, A.; Jain, S.; Pahwa, R.; Yar, M.S. Ciprofloxacin: Review on Developments in Synthetic, Analytical, and Medicinal Aspects. J. Enzym. Inhib. Med. Chem. 2010, 25, 577–589. [Google Scholar] [CrossRef] [Green Version]
- Vance-Bryan, K.; Guay, D.R.P.; Rotschafer, J.C. Clinical Pharmacokinetics of Ciprofloxacin. Clin. Pharmacokinet. 1990, 19, 434–461. [Google Scholar] [CrossRef]
- Shekar, K.; Roberts, J.A.; Mcdonald, C.I.; Fisquet, S.; Barnett, A.G.; Mullany, D.V.; Ghassabian, S.; Wallis, S.C.; Fung, Y.L.; Smith, M.T.; et al. Sequestration of Drugs in the Circuit May Lead to Therapeutic Failure during Extracorporeal Membrane Oxygenation. Crit. Care 2012, 16, R194. [Google Scholar] [CrossRef] [Green Version]
- Shekar, K.; Fraser, J.F.; Smith, M.T.; Roberts, J.A. Pharmacokinetic Changes in Patients Receiving Extracorporeal Membrane Oxygenation. J. Crit. Care 2012, 27, 741.e9–741.e18. [Google Scholar] [CrossRef]
- Shekar, K.; Roberts, J.A.; Mcdonald, C.I.; Ghassabian, S.; Anstey, C.; Wallis, S.C.; Mullany, D.V.; Fung, Y.L.; Fraser, J.F. Protein-Bound Drugs Are Prone to Sequestration in the Extracorporeal Membrane Oxygenation Circuit: Results from an Ex Vivo Study. Crit. Care 2015, 19, 164. [Google Scholar] [CrossRef] [Green Version]
- Sinnah, F.; Shekar, K.; Abdul-Aziz, M.; Buscher, H.; Diab, S.; Fisquet, S.; Fung, Y.L.; Mcdonald, C.; Reynolds, C.; Rudham, S.; et al. Incremental Research Approach to Describing the Pharmacokinetics of Ciprofloxacin during Extracorporeal Membrane Oxygenation. Crit. Care Resusc. 2017, 19, 8–14. [Google Scholar]
- Levey, A.; Bosch, J.; Lewis, J.; Greene, T.; Rogers, N.; Roth, D. A More Accurate Method to Estimate Glomerular Filtration Rate from Serum Creatinine: A New Prediction Equation. Modification of Diet in Renal Disease Study Group. Ann. Intern. Med. 1999, 130, 461–470. [Google Scholar] [CrossRef]
- Cockcroft, D.; Gault, M. Prediction of Creatinine Clearance from Serum Creatinine. Nephron 1976, 16, 31–41. [Google Scholar] [CrossRef]
- Levey, A.; Stevens, L.; Schmid, C.; Zhang, Y.; Castro, A.; Feldman, H.; Kusek, J.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A New Equation to Estimate Glomerular Filtration Rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Keizer, R.J.; Karlsson, M.O.; Hooker, A. Modeling and Simulation Workbench for NONMEM: Tutorial on Pirana, PsN, and Xpose. CPT Pharmacomet. Syst. Pharmacol. 2013, 2, 1–9. [Google Scholar] [CrossRef]
- R Development Core Team. A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2018; Volume 2, ISBN 3900051070. [Google Scholar]
- Bonate, P.L. Pharmacokinetic-Pharmacodynamic Modeling and Simulation, 2nd ed.; Springer: New York, NY, USA, 2011; ISBN 9781441994844. [Google Scholar]
- Savic, R.M.; Karlsson, M.O. Importance of Shrinkage in Empirical Bayes Estimates for Diagnostics: Problems and Solutions. AAPS J. 2009, 11, 558–569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, B.J.; Holford, N.H.G. Mechanism-Based Concepts of Size and Maturity in Pharmacokinetics. Annu. Rev. Pharmacol. Toxicol. 2008, 48, 303–332. [Google Scholar] [CrossRef] [PubMed]
- Bergstrand, M.; Hooker, A.C.; Wallin, J.E.; Karlsson, M.O. Prediction-Corrected Visual Predictive Checks for Diagnosing Nonlinear Mixed-Effects Models. AAPS J. 2011, 13, 143–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Broeker, A.; Wicha, S.G. Assessing Parameter Uncertainty in Small-n Pharmacometric Analyses: Value of the Log-Likelihood Profiling-Based Sampling Importance Resampling (LLP-SIR) Technique. J. Pharmacokinet. Pharmacodyn. 2020, 47, 219–228. [Google Scholar] [CrossRef] [Green Version]
- EUCAST: Clinical Breakpoints and Dosing of Antibiotics. Available online: https://eucast.org/clinical_breakpoints/ (accessed on 11 January 2021).
- Lipman, J.; Scribante, J.; Gous, A.G.S.; Hon, H.; Tshukutsoane, S.; Pinder, M.; Piccolo, R.; Nel, E.; Verhoef, L.; Klugman, K.; et al. Pharmacokinetic Profiles of High-Dose Intravenous Ciprofloxacin in Severe Sepsis. Antimicrob. Agents Chemother. 1998, 42, 2235–2239. [Google Scholar] [CrossRef] [Green Version]
- Khachman, D.; Conil, J.-M.; Georges, B.; Saivin, S.; Houin, G.; Toutain, P.-L.; Laffont, C.M. Optimizing Ciprofloxacin Dosing in Intensive Care Unit Patients through the Use of Population Pharmacokinetic-Pharmacodynamic Analysis and Monte Carlo Simulations. J. Antimicrob. Chemother. 2011, 66, 1798–1809. [Google Scholar] [CrossRef]
- Abdulla, A.; Rogouti, O.; Hunfeld, N.G.M.; Endeman, H.; Dijkstra, A.; van Gelder, T.; Muller, A.E.; de Winter, B.C.M.; Koch, B.C.P. Population Pharmacokinetics and Target Attainment of Ciprofloxacin in Critically Ill Patients. Eur. J. Clin. Pharmacol. 2020, 76, 957–967. [Google Scholar] [CrossRef]
- Conil, J.M.; Georges, B.; de Lussy, A.; Khachman, D.; Seguin, T.; Ruiz, S.; Cougot, P.; Fourcade, O.; Houin, G.; Saivin, S. Ciprofloxacin Use in Critically Ill Patients: Pharmacokinetic and Pharmacodynamic Approaches. Int. J. Antimicrob. Agents 2008, 32, 505–510. [Google Scholar] [CrossRef]
- Li, X.; Zoller, M.; Fuhr, U.; Huseyn-Zada, M.; Maier, B.; Vogeser, M.; Zander, J.; Taubert, M. Ciprofloxacin in Critically Ill Subjects: Considering Hepatic Function, Age and Sex to Choose the Optimal Dose. J. Antimicrob. Chemother. 2019, 74, 682–690. [Google Scholar] [CrossRef]
- Shah, A.; Lettieri, J.; Nix, D.; Wilton, J.; Heller, A.H. Pharmacokinetics of High-Dose Intravenous Ciprofloxacin in Young and Elderly and in Male and Female Subjects. Antimicrob. Agents Chemother. 1995, 39, 1003–1006. [Google Scholar] [CrossRef] [Green Version]
- Torniainen, K.; Tammilehto, S.; Ulvi, V. The Effect of PH, Buffer Type and Drug Concentration on the Photodegradation of Ciprofloxacin. Int. J. Pharm. 1996, 132, 53–61. [Google Scholar] [CrossRef]
- Drusano, G.; Labro, M.-T.; Cars, O.; Mendes, P.; Shah, P.; Sörgel, F.; Weber, W. Pharmacokinetics and Pharmacodynamics of Fluoroquinolones. Clin. Microbiol. Infect. 1998, 4, 2S27–2S41. [Google Scholar] [CrossRef] [Green Version]
- Forrest, A.; Ballow, C.H.; Nix, D.E.; Birmingham, M.C.; Schentag, J.J. Development of a Population Pharmacokinetic Model and Optimal Sampling Strategies for Intravenous Ciprofloxacin. Antimicrob. Agents Chemother. 1993, 37, 1065–1072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cojutti, P.G.; Ramos-Martin, V.; Schiavon, I.; Rossi, P.; Baraldo, M.; Hope, W.; Pea, F. Population Pharmacokinetics and Pharmacodynamics of Levofloxacin in Acutely Hospitalized Older Patients with Various Degrees of Renal Function. Antimicrob. Agents Chemother. 2017, 61, e02134-16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heidelbaugh, J.J.; Holmstrom, H. The Perils of Prescribing Fluoroquinolones. J. Fam. Pract. 2013, 62, 191–197. [Google Scholar] [PubMed]
- Shekar, K.; Roberts, J.A.; Welch, S.; Buscher, H.; Rudham, S.; Burrows, F.; Ghassabian, S.; Wallis, S.C.; Levkovich, B.; Pellegrino, V.; et al. ASAP ECMO: Antibiotic, Sedative and Analgesic Pharmacokinetics during Extracorporeal Membrane Oxygenation: A Multi-Centre Study to Optimise Drug Therapy during ECMO. BMC Anesthesiol. 2012, 12, 29. [Google Scholar] [CrossRef]
- Alihodzic, D.; Broeker, A.; Baehr, M.; Kluge, S.; Langebrake, C.; Wicha, S.G. Impact of Inaccurate Documentation of Sampling and Infusion Time in Model-Informed Precision Dosing. Front. Pharmacol. 2020, 11, 172. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Median (IQR) | Range |
|---|---|---|
| Age (years) | 57 (51–63) | 25–73 |
| Weight (kg) | 90 (80–103) | 66–123 |
| Height (m) | 1.8 (1.75–1.82) | 1.60–1.97 |
| BMI (kg/m²) | 29.3 (26.1–30.9) | 20.4–36.7 |
| Scores | ||
| SOFA score | 13 (10–14) | 3.0–19 |
| SAPS II score | 48 (38–52) | 15–73 |
| APACHE II score | 32 (21–33) | 14–46 |
| Blood chemistry, serum levels | ||
| Serum creatinine (mg/dL) | 1.3 (0.88–2.0) | 0.25–4.10 |
| GFR (CKD-EPI) (ml/min) | 46.8 (25.4–79.6) | 10.7–143 |
| Serum albumin concentration (g/L) | 21.3 (16.2–24.9) | 10.4–31.0 |
| Total bilirubin (mg/dL) | 1.0 (0.7–2.0) | 0.2–24.4 |
| AST level (U/L) | 56 (39.5–134) | 21–1568 |
| ALT level (U/L) | 56 (32–118.5) | 11–543 |
| C-reactive protein (mg/L) | 128 (73.5–202.3) | 8–475 |
| Bicarbonate (mmol/L) | 26.6 (24.3–29.7) | 18.0–39.0 |
| pH value | 7.43 (7.39–7.46) | 7.25–7.58 |
| ECMO parameter | ||
| Length of ECMO therapy (days) | 13 (9–16) | (4–28) |
| Blood flow (L/min) | 4.4 (3.9–5.2) | 2.2–6.73 |
| Gas flow (L/min) | 4.25 (3.5–5.1) | 0.9–10 |
| Revolutions per minutes (RPM) | 3460 (3185–3804) | 2270–5000 |
| PaO2/FiO2 | 102.5 (71.1–143.3) | 26.8–463 |
| Ciprofloxacin serum concentrations (mg/L) | ||
| Peak | 4.55 (3.69–5.9) | 2.38–12.14 |
| Mid-dose | 2.57 (1.97–3.45) | 1.06–9.3 |
| Through | 1.53 (1.11–2.57) | 0.77–6.88 |
| Number (%) | Range | |
| Sex | ||
| Male | 16 (94) | NA |
| Female | 1 (6) | NA |
| Indication for ECMO | ||
| ARDS | 6 (35) | NA |
| Global respiratory insufficiency | 1 (6) | NA |
| Pulmonary fibrosis | 1 (6) | NA |
| Cardiac decompensation | 1 (6) | NA |
| Bridge to transplant | 1 (6) | NA |
| Cardiogenic shock (STEMI/NSTEMI) | 7 (41) | NA |
| ECMO type | ||
| Veno-arterial (VA) | 8 (47) | NA |
| Veno-venous (VV) | 8 (47) | NA |
| Veno-veno-arterial (VVA) | 1 (6) | NA |
| Use of continuous hemodiafiltration | ||
| 8 (47) | NA | |
| Outcome | ||
| Survived | 5 (29) | NA |
| Deceased | 12 (71) | NA |
| Base Model | Final Model | LLP-SIR | |||
|---|---|---|---|---|---|
| Estimate | Shrinkage | Estimate | Shrinkage | 95% CI | |
| (% RSE) | (%) | (% RSE) | (%) | ||
| Fixed effects | |||||
| CL (L/h) | 13.6 (12) | - | 12.9 (7.6) | - | 11.2–14.7 |
| V1 (L) | 73.2 (16) | - | 73.4 (15) | - | 53.3–95.5 |
| Q (L/h) | 39.4 (33) | - | 38.8 (30) | - | 25.7–57.7 |
| V2 (L) | 88.3 (17) | - | 87.6 (16) | - | 66.1–115.1 |
| COV_CL_BICARB (L/mmol) | - | - | 0.0571 (12) | - | 0.0334–0.0770 |
| COV_CL_eGFR (min/mL) | - | - | 0.0038 (29) | - | 0.0003–0.0074 |
| First level of random effects | |||||
| IIV CL (CV%) | 46.4 (20) | 0 | 25.8 (19) | 4 | 18.7–36.0 |
| IIV V1 (CV%) | 48.1 (18) | 14 | 53.9 (17) | 12 | 33.1–76.1 |
| IIV Q (CV%) | 38.7 (64) | 47 | 34.1 (76) | 52 | 4.2–69.6 |
| IIV V2 (CV%) | 3.2 FIX | 94 | - | - | - |
| IOV CL (CV%) | 18.5 (17) | - | 17.2 (21) | - | 11.3–23.3 |
| Second level of random effects | |||||
| Prop. σ (CV%) | 12.2 (17.3) | 29 | 12.1 (21.9) | 28 | 10.2–15.2 |
| OFV | 29.054 | - | 2.082 | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alihodzic, D.; Wicha, S.G.; Frey, O.R.; König, C.; Baehr, M.; Jarczak, D.; Kluge, S.; Langebrake, C. Ciprofloxacin in Patients Undergoing Extracorporeal Membrane Oxygenation (ECMO): A Population Pharmacokinetic Study. Pharmaceutics 2022, 14, 965. https://doi.org/10.3390/pharmaceutics14050965
Alihodzic D, Wicha SG, Frey OR, König C, Baehr M, Jarczak D, Kluge S, Langebrake C. Ciprofloxacin in Patients Undergoing Extracorporeal Membrane Oxygenation (ECMO): A Population Pharmacokinetic Study. Pharmaceutics. 2022; 14(5):965. https://doi.org/10.3390/pharmaceutics14050965
Chicago/Turabian StyleAlihodzic, Dzenefa, Sebastian G. Wicha, Otto R. Frey, Christina König, Michael Baehr, Dominik Jarczak, Stefan Kluge, and Claudia Langebrake. 2022. "Ciprofloxacin in Patients Undergoing Extracorporeal Membrane Oxygenation (ECMO): A Population Pharmacokinetic Study" Pharmaceutics 14, no. 5: 965. https://doi.org/10.3390/pharmaceutics14050965