
Current Advances of Nanomedicines Delivering Arsenic Trioxide for Enhanced Tumor Therapy


Abstract
:1. Introduction
2. Pharmacological Properties of ATO
2.1. Physicochemical Properties
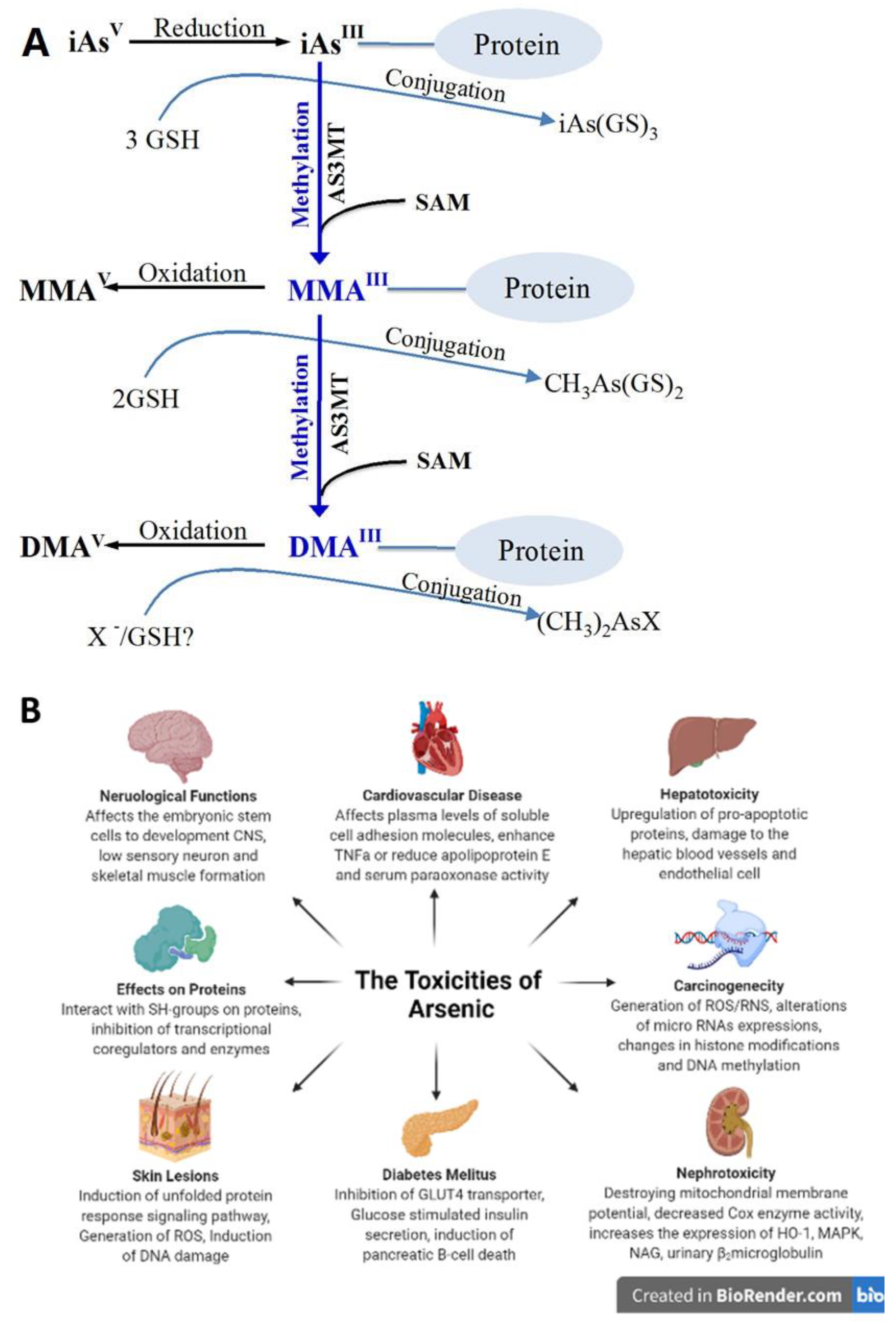
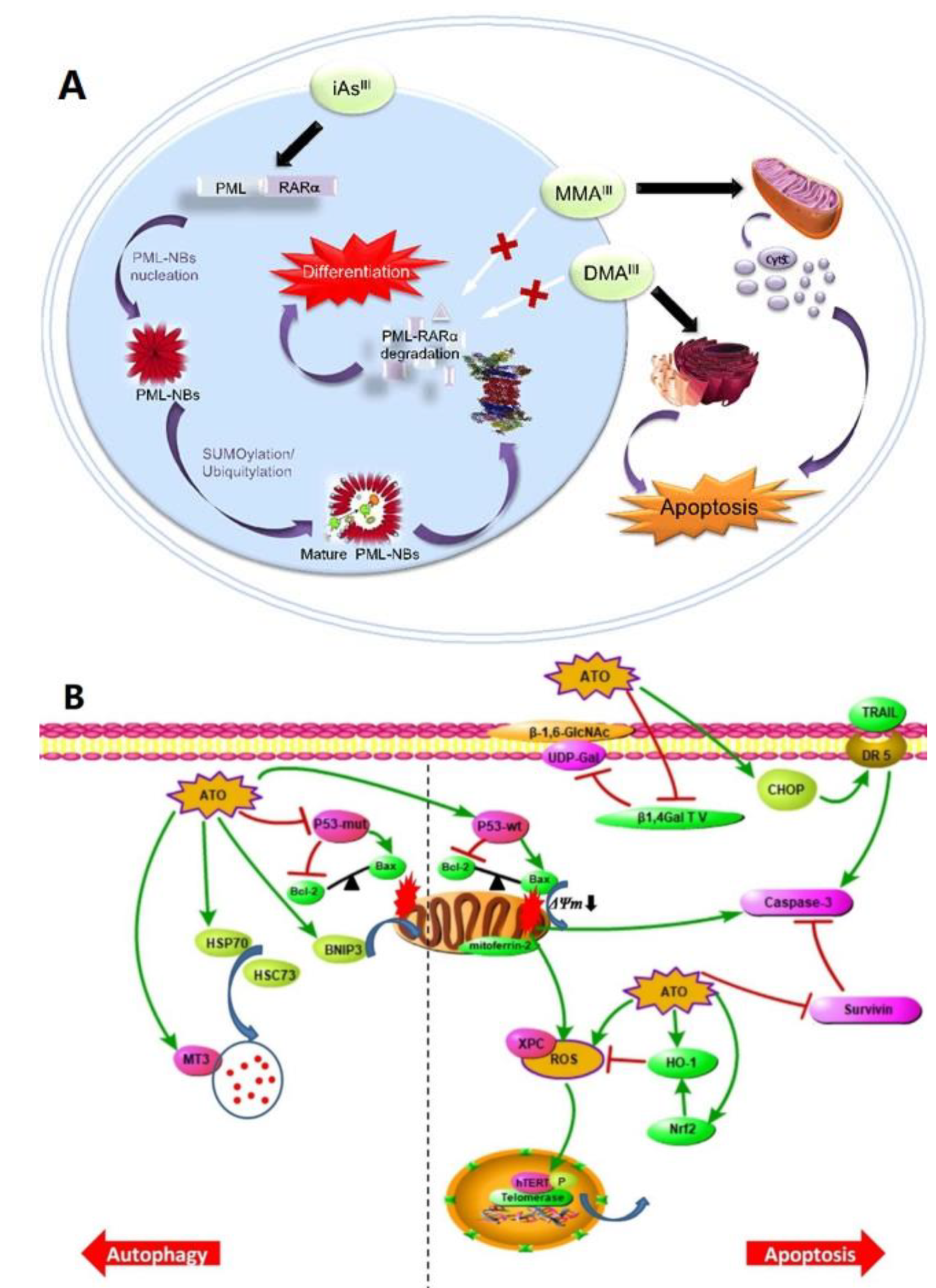
2.2. Anti-Cancer Mechanisms
3. Limitations of ATO for Clinical Applications
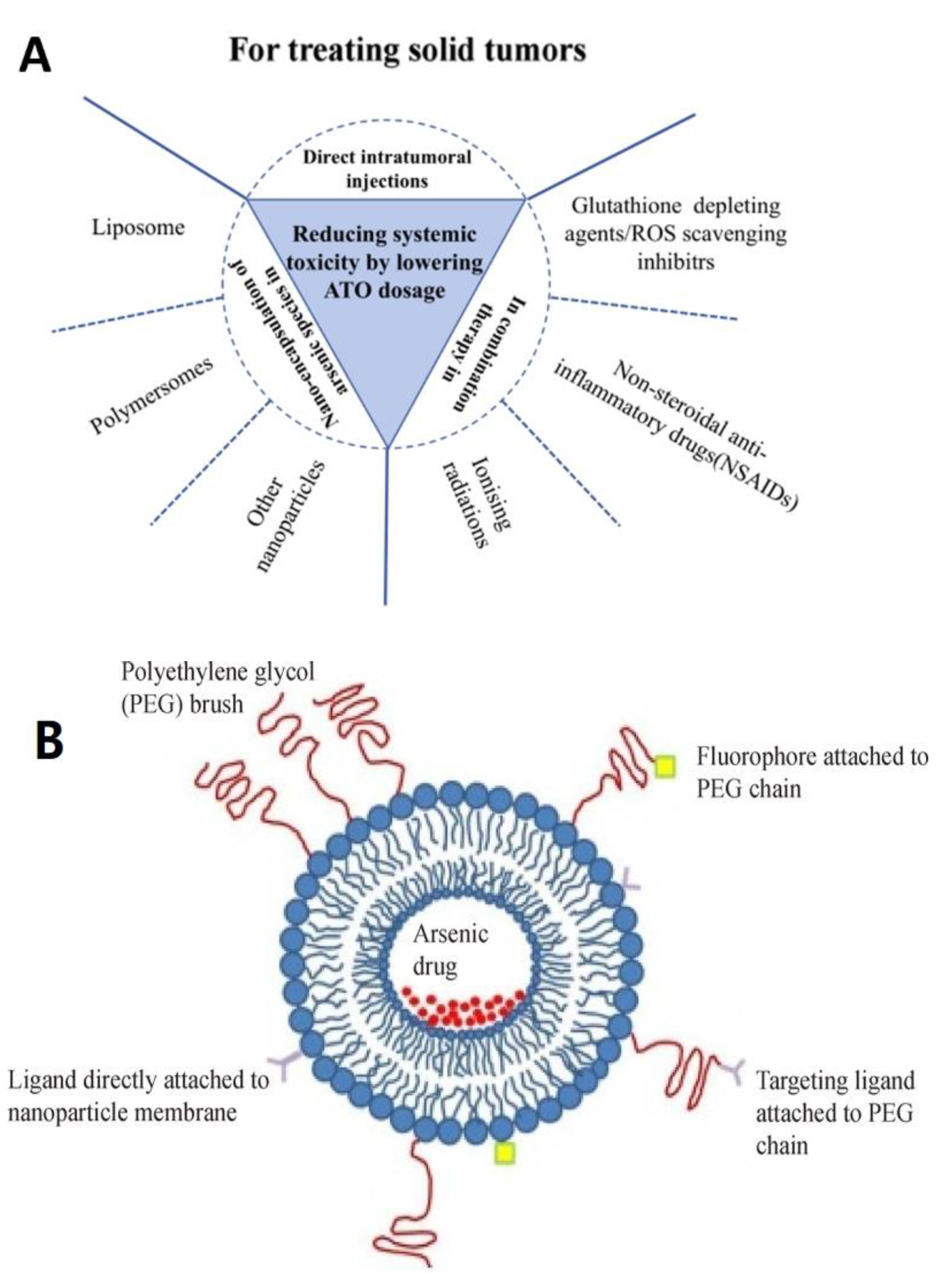
4. Strategies to Deliver ATO by Nanoparticles
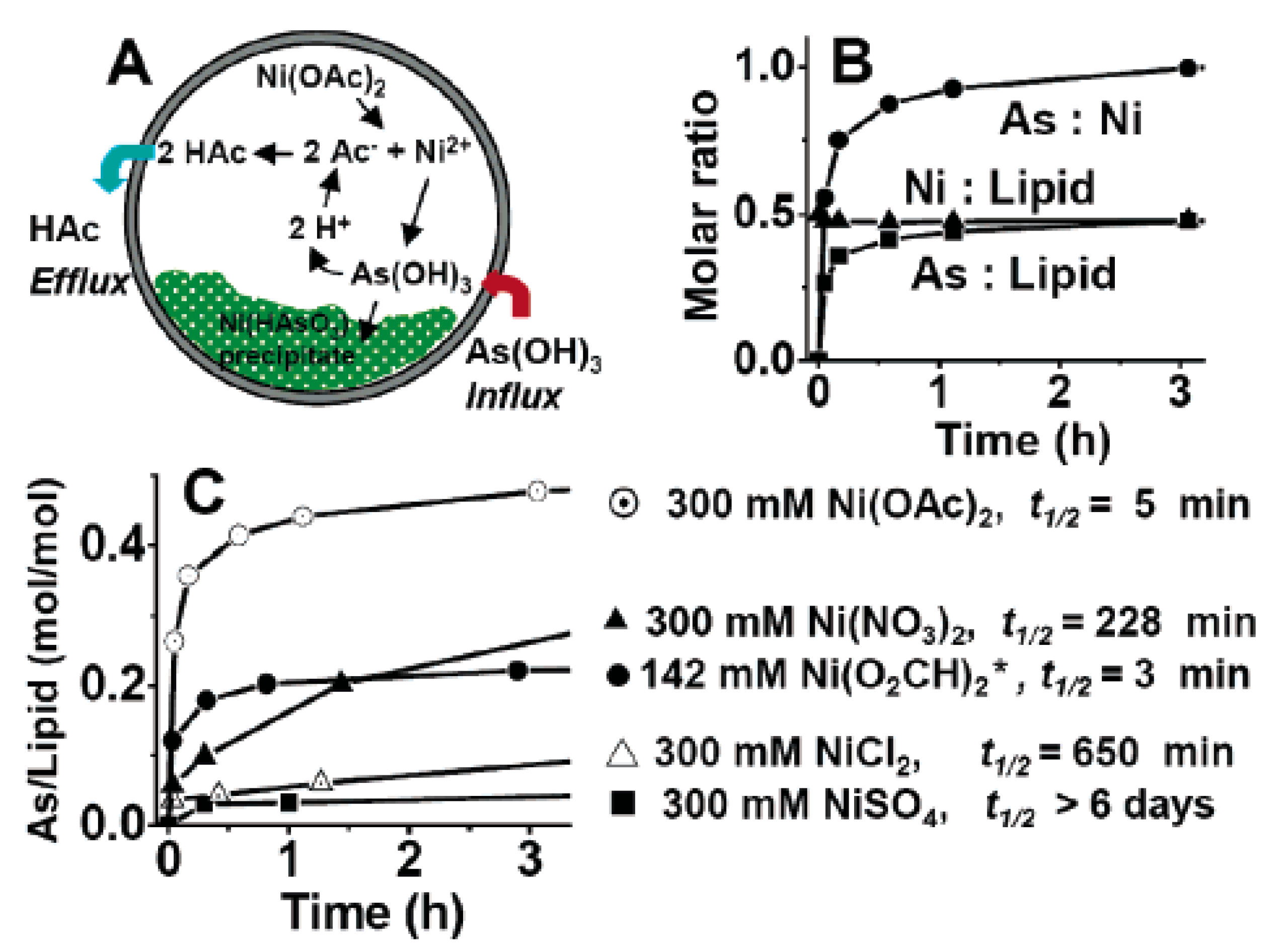
4.1. Liposome
4.2. Protein
4.3. Polymers
4.4. Coordination Polymer
4.5. Hollow Porous Silica Nanoparticles-Based Nanovehicles
5. Combinations of ATO That Enhanced the Efficacy of Chemo Agents
5.1. Combined with Molecular-Targeted Drug
5.2. Combined with Chemotherapy Drugs
5.3. Combined with Other Drugs
6. Conclusions and Future Perspective
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Li, R.; Li, Q.; Ji, Q. Molecular targeted study in tumors: From western medicine to active ingredients of traditional Chinese medicine. Biomed. Pharmacother. 2020, 121, 109624. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.C.; Sung, B.; Prasad, S.; Webb, L.J.; Aggarwal, B.B. Cancer drug discovery by repurposing: Teaching new tricks to old dogs. Trends Pharmacol. Sci. 2013, 34, 508–517. [Google Scholar] [CrossRef]
- Yang, X. Annual advances in traditional medicine for tumor therapy in 2019. Tradit. Med. Res. 2020, 5, 90. [Google Scholar] [CrossRef]
- Zeng, Y.; Xiang, Y.; Sheng, R.; Tomás, H.; Rodrigues, J.; Gu, Z.; Zhang, H.; Gong, Q.; Luo, K. Polysaccharide-based nanomedicines for cancer immunotherapy: A review. Bioact. Mater. 2021, 6, 3358–3382. [Google Scholar] [CrossRef] [PubMed]
- Fojo, T.; Parkinson, D.R. Biologically targeted cancer therapy and marginal benefits: Are we making too much of too little or are we achieving too little by giving too much? Clin. Cancer Res. 2010, 16, 5972–5980. [Google Scholar] [CrossRef] [Green Version]
- Desoize, B. Metals and metal compounds in cancer treatment. Anticancer Res. 2004, 24, 1529–1544. [Google Scholar] [PubMed]
- Akhtar, A.; Wang, S.X.; Ghali, L.; Bell, C.; Wen, X. Recent advances in arsenic trioxide encapsulated nanoparticles as drug delivery agents to solid cancers. J. Biomed. Res. 2017, 31, 177–188. [Google Scholar] [CrossRef] [Green Version]
- Cholujova, D.; Bujnakova, Z.; Dutkova, E.; Hideshima, T.; Groen, R.W.; Mitsiades, C.S.; Richardson, P.G.; Dorfman, D.M.; Balaz, P.; Anderson, K.C.; et al. Realgar nanoparticles versus ATO arsenic compounds induce In Vitro and In Vivo activity against multiple myeloma. Br. J. Haematol. 2017, 179, 756–771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Douer, D.; Tallman, M.S. Arsenic trioxide: New clinical experience with an old medication in hematologic malignancies. J. Clin. Oncol. 2005, 23, 2396–2410. [Google Scholar] [CrossRef] [PubMed]
- Sun, T.; Zhang, Y.S.; Pang, B.; Hyun, D.C.; Yang, M.; Xia, Y. Engineered Nanoparticles for Drug Delivery in Cancer Therapy. In Nanomaterials and Neoplasms; Jenny Stanford Publishing: Dubai, United Arab Emirates, 2021; pp. 31–142. [Google Scholar]
- Maeda, H. Toward a full understanding of the EPR effect in primary and metastatic tumors as well as issues related to its heterogeneity. Adv. Drug Deliv. Rev. 2015, 91, 3–6. [Google Scholar] [CrossRef]
- Noy, J.M.; Lu, H.; Hogg, P.J.; Yang, J.L.; Stenzel, M. Direct Polymerization of the Arsenic Drug PENAO to Obtain Nanoparticles with High Thiol-Reactivity and Anti-Cancer Efficiency. Bioconjug. Chem. 2018, 29, 546–558. [Google Scholar] [CrossRef]
- Palma-Lara, I.; Martinez-Castillo, M.; Quintana-Perez, J.C.; Arellano-Mendoza, M.G.; Tamay-Cach, F.; Valenzuela-Limon, O.L.; Garcia-Montalvo, E.A.; Hernandez-Zavala, A. Arsenic exposure: A public health problem leading to several cancers. Regul. Toxicol. Pharmacol. 2020, 110, 104539. [Google Scholar] [CrossRef] [PubMed]
- Pullella, K.; Kotsopoulos, J. Arsenic Exposure and Breast Cancer Risk: A Re-Evaluation of the Literature. Nutrients 2020, 12, 3305. [Google Scholar] [CrossRef] [PubMed]
- Khairul, I.; Wang, Q.Q.; Jiang, Y.H.; Wang, C.; Naranmandura, H. Metabolism, toxicity and anticancer activities of arsenic compounds. Oncotarget 2017, 8, 23905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Renu, K.; Saravanan, A.; Elangovan, A.; Ramesh, S.; Annamalai, S.; Namachivayam, A.; Abel, P.; Madhyastha, H.; Madhyastha, R.; Maruyama, M.; et al. An appraisal on molecular and biochemical signalling cascades during arsenic-induced hepatotoxicity. Life Sci. 2020, 260, 118438. [Google Scholar] [CrossRef] [PubMed]
- Fang, Y.; Zhang, Z. Arsenic trioxide as a novel anti-glioma drug: A review. Cell. Mol. Biol. Lett. 2020, 25, 44. [Google Scholar] [CrossRef] [PubMed]
- Barbey, J.T. Cardiac toxicity of arsenic trioxide. Blood 2001, 98, 1632–1634. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X. Arsenic trioxide controls the fate of the PML-RAR alpha oncoprotein by directly binding PML. Science 2010, 328, 974. [Google Scholar] [CrossRef]
- Xu, W.; Li, X.; Quan, L.; Yao, J.; Mu, G.; Guo, J.; Wang, Y. Arsenic trioxide decreases the amount and inhibits the function of regulatory T cells, which may contribute to its efficacy in the treatment of acute promyelocytic leukemia. Leuk. Lymphoma 2018, 59, 650–659. [Google Scholar] [CrossRef] [PubMed]
- Cao, K.; Sheng, Y.; Zheng, S.; Yuan, S.; Huang, G.; Liu, Y. Arsenic trioxide preferentially binds to the ring finger protein PML: Understanding target selection of the drug. Metallomics 2018, 10, 1564–1569. [Google Scholar] [CrossRef]
- Abele, M.; Mueller, S.-L.; Schleicher, S.; Hartmann, U.; Doering, M.; Queudeville, M.; Lang, P.; Handgretinger, R.; Ebinger, M. Arsenic trioxide in pediatric cancer—A case series and review of literature. Pediatr. Hematol. Oncol. 2021, 38, 471–485. [Google Scholar] [CrossRef]
- Sun, Z.; Li, M.; Bai, L.; Fu, J.; Lu, J.; Wu, M.; Zhou, C.; Zhang, Y.; Wu, Y. Arsenic trioxide inhibits angiogenesis In Vitro and In Vivo by upregulating FoxO3a. Toxicol. Lett. 2019, 315, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.H.; Zhou, M.T.; Ye, A.F.; Li, Q.; Bai, Y.H.; Zhang, Q.Y. Research The conformation change of Bcl-2 is involved in arsenic trioxide-induced apoptosis and inhibition of proliferation in SGC7901 human gastric cancer cells. World J. Surg. Oncol. 2010, 8, 31. [Google Scholar] [CrossRef] [Green Version]
- Tian, W.; Wang, Z.; Tang, N.-N.; Li, J.-T.; Liu, Y.; Chu, W.-F.; Yang, B.-F. Ascorbic Acid Sensitizes Colorectal Carcinoma to the Cytotoxicity of Arsenic Trioxide via Promoting Reactive Oxygen Species-Dependent Apoptosis and Pyroptosis. Front. Pharmacol. 2020, 11, 123. [Google Scholar] [CrossRef] [PubMed]
- Beurel, E.; Jope, R.S. The paradoxical pro- and anti-apoptotic actions of GSK3 in the intrinsic and extrinsic apoptosis signaling pathways. Prog. Neurobiol. 2006, 79, 173–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, W.; Zeng, Y.C. A candidate for lung cancer treatment: Arsenic trioxide. Clin. Transl. Oncol. 2019, 21, 1115–1126. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.B.; Liu, J.H.; Hu, J.; Xue, K. Mechanism of As2O3 induces apoptosis of glioma U87 cells. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 4875–4881. [Google Scholar] [PubMed]
- Wang, L.Y.; Min, Z.H.; Wang, X.D.; Hu, M.S.; Song, D.L.; Ren, Z.G.; Cheng, Y.F.; Wang, Y.H. Arsenic trioxide and sorafenib combination therapy for human hepatocellular carcinoma functions via up-regulation of TNF-related apoptosis-inducing ligand. Oncol. Lett. 2018, 16, 3341–3350. [Google Scholar] [CrossRef] [Green Version]
- Jiang, X.; Chen, C.; Liu, Y.; Zhang, P.; Zhang, Z. Critical role of cellular glutathione homeostasis for trivalent inorganic arsenite-induced oxidative damage in human bronchial epithelial cells. Mutat. Res. Genet. Toxicol. Environ. Mutagen. 2014, 770, 35–45. [Google Scholar] [CrossRef]
- Sun, Y.; Wang, C.; Wang, L.; Dai, Z.; Yang, K. Arsenic trioxide induces apoptosis and the formation of reactive oxygen species in rat glioma cells. Cell. Mol. Biol. Lett. 2018, 23, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, M.; Li, Y.; Hu, Q.; Bai, X.-C.; Huang, W.; Yan, C.; Scheres, S.H.; Shi, Y. Atomic structure of the apoptosome: Mechanism of cytochrome c-and dATP-mediated activation of Apaf-1. Genes Dev. 2015, 29, 2349–2361. [Google Scholar] [CrossRef] [Green Version]
- Zheng, C.Y.; Lam, S.K.; Li, Y.Y.; Ho, J.C.M. Arsenic trioxide-induced cytotoxicity in small cell lung cancer via altered redox homeostasis and mitochondrial integrity. Int. J. Oncol. 2015, 46, 1067–1078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, G.Y.; Zhang, T.; Sun, W.; Wang, H.S.; Yin, F.; Wang, Z.Y.; Zuo, D.Q.; Sun, M.X.; Zhou, Z.F.; Lin, B.H.; et al. Arsenic sulfide induces apoptosis and autophagy through the activation of ROS/JNK and suppression of Akt/mTOR signaling pathways in osteosarcoma. Free Radic. Biol. Med. 2017, 106, 24–37. [Google Scholar] [CrossRef] [PubMed]
- Fu, D.X.; Yu, J.Y.; Yang, S.H.; Wu, M.Y.; Hammad, S.M.; Connell, A.R.; Du, M.; Chen, J.P.; Lyons, T.J. Survival or death: A dual role for autophagy in stress-induced pericyte loss in diabetic retinopathy. Diabetologia 2016, 59, 2251–2261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, B.W.; Tan, M.D.; Cai, W.L.; Wang, B.; He, P.H.; Zhang, X.P. Arsenic trioxide induces autophagic cell death in osteosarcoma cells via the ROS-TFEB signaling pathway. Biochem. Biophys. Res. Commun. 2018, 496, 167–175. [Google Scholar] [CrossRef]
- Yu, S.; Li, L.-H.; Lee, C.-H.; Jeyakannu, P.; Wang, J.-J.; Hong, C.-H. Arsenic leads to autophagy of keratinocytes by increasing aquaporin 3 expression. Sci. Rep. 2021, 11, 17523. [Google Scholar] [CrossRef]
- Cui, Z.F.; Zhang, Y.; Xia, K.; Yan, Q.L.; Kong, H.T.; Zhang, J.C.; Zuo, X.L.; Shi, J.Y.; Wang, L.H.; Zhu, Y.; et al. Nanodiamond autophagy inhibitor allosterically improves the arsenical-based therapy of solid tumors. Nat. Commun. 2018, 9, 4347. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zhang, Y.; Wang, W.; Zhang, Z. Potential molecular mechanisms underlying the effect of arsenic on angiogenesis. Arch. Pharmacal Res. 2019, 42, 962–976. [Google Scholar] [CrossRef]
- Beenken, A.; Mohammadi, M. The FGF family: Biology, pathophysiology and therapy. Nat. Rev. Drug Discov. 2009, 8, 235–253. [Google Scholar] [CrossRef] [Green Version]
- Ferrara, N. VEGF-A: A critical regulator of blood vessel growth. Eur. Cytokine Netw. 2009, 20, 158–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, L.; Liu, L.; Zhan, S.N.; Chen, L.L.; Wang, Y.Y.; Zhang, Y.J.; Du, J.; Wu, Y.P.; Gu, L. Arsenic Trioxide Suppressed Migration and Angiogenesis by Targeting FOXO3a in Gastric Cancer Cells. Int. J. Mol. Sci. 2018, 19, 3739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xin, J.; Zhang, K.; Huang, J.; Luo, X.; Gong, X.; Yang, Z.; Lin, H.; Shan, H.; Gao, J. Facile synthesis of aquo-cisplatin arsenite multidrug nanocomposites for overcoming drug resistance and efficient combination therapy. Biomater. Sci. 2018, 7, 262–271. [Google Scholar] [CrossRef]
- Song, P.; Hai, Y.; Wang, X.; Zhao, L.H.; Chen, B.Q.; Cui, P.; Xie, Q.J.; Yu, L.; Li, Y.; Wu, Z.R.; et al. Realgar transforming solution suppresses angiogenesis and tumor growth by inhibiting VEGF receptor 2 signaling in vein endothelial cells. Arch. Pharm. Res. 2018, 41, 467–480. [Google Scholar] [CrossRef] [PubMed]
- Leung, L.L.; Lam, S.K.; Li, Y.Y.; Ho, J.C.M. Tumour growth-suppressive effect of arsenic trioxide in squamous cell lung carcinoma. Oncol. Lett. 2017, 14, 3748–3754. [Google Scholar] [CrossRef] [PubMed]
- Laka, K.; Makgoo, L.; Mbita, Z. Survivin Splice Variants in Arsenic Trioxide (As₂O₃)-Induced Deactivation of PI3K and MAPK Cell Signalling Pathways in MCF-7 Cells. Genes 2019, 10, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moghaddaskho, F.; Eyvani, H.; Ghadami, M.; Tavakkoly-Bazzaz, J.; Alimoghaddam, K.; Ghavamzadeh, A.; Ghaffari, S.H. Demethylation and alterations in the expression level of the cell cycle-related genes as possible mechanisms in arsenic trioxide-induced cell cycle arrest in human breast cancer cells. Tumor Biol. 2017, 39, 1010428317692255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hassani, S.; Khaleghian, A.; Ahmadian, S.; Alizadeh, S.; Alimoghaddam, K.; Ghavamzadeh, A.; Ghaffari, S.H. Redistribution of cell cycle by arsenic trioxide is associated with demethylation and expression changes of cell cycle related genes in acute promyelocytic leukemia cell line (NB4). Ann. Hematol. 2018, 97, 83–93. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.F.; Ngai, P.; Ho, D.W.; Yu, W.C.; Ng, M.N.; Lau, C.K.; Li, M.L.; Tam, K.H.; Lam, C.T.; Poon, R.T. Identification of local and circulating cancer stem cells in human liver cancer. Hepatology 2008, 47, 919–928. [Google Scholar] [CrossRef] [PubMed]
- Ning, K.; Ning, W.L.; Ning, X.T.; Wang, X.Y.; Zhou, F. Effect of As2O3 on colorectal CSCs stained with ALDH1 in primary cell culture In Vitro. Oncol. Lett. 2018, 16, 4008–4012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, K.J.; Yang, M.H.; Zheng, J.C.; Li, B.; Nie, W. Arsenic trioxide inhibits cancer stem-like cells via down-regulation of Gli1 in lung cancer. Am. J. Transl. Res. 2016, 8, 1133–1143. [Google Scholar]
- Chang, Q.; Bi, Z.; Fu, Y.; Rice, M.; Zhang, Q.; Wadgaonkar, P.; Almutairy, B.; Zhang, W.; Lu, Y.; Xu, L. Characterization of arsenic-induced cancer stem-like cells. In Stem Cell Transcriptional Networks; Springer: Berlin/Heidelberg, Germany, 2020; pp. 293–303. [Google Scholar]
- Linder, B.; Wehle, A.; Hehlgans, S.; Bonn, F.; Dikic, I.; Rodel, F.; Seifert, V.; Kogel, D. Arsenic Trioxide and (−)-Gossypol Synergistically Target Glioma Stem-Like Cells via Inhibition of Hedgehog and Notch Signaling. Cancers 2019, 11, 350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, H.Y.; Zhang, B.; Zhou, J.N.; Wang, D.X.; Xu, Y.C.; Zeng, Q.; Jia, Y.L.; Xi, J.F.; Nan, X.; He, L.J.; et al. Arsenic trioxide inhibits liver cancer stem cells and metastasis by targeting SRF/MCM7 complex. Cell Death Dis. 2019, 10, 453. [Google Scholar] [CrossRef] [Green Version]
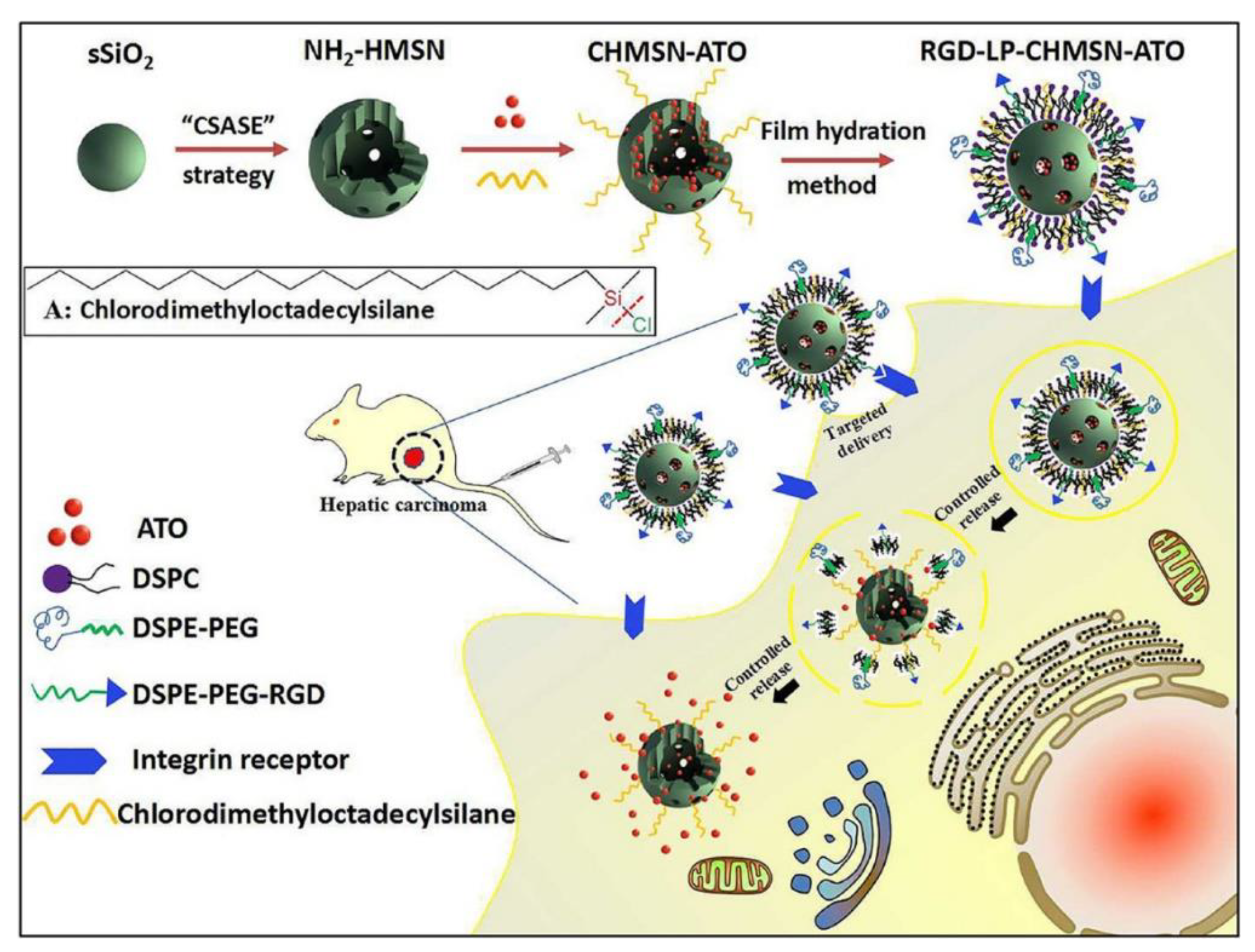
- Fei, W.; Zhang, Y.; Han, S.; Tao, J.; Zheng, H.; Wei, Y.; Zhu, J.; Li, F.; Wang, X. RGD conjugated liposome-hollow silica hybrid nanovehicles for targeted and controlled delivery of arsenic trioxide against hepatic carcinoma. Int. J. Pharm. 2017, 519, 250–262. [Google Scholar] [CrossRef] [Green Version]
- Kwong, Y.-L. Arsenic trioxide in the treatment of haematological malignancies. Expert Opin. Drug Safety 2004, 3, 589–597. [Google Scholar] [CrossRef] [PubMed]
- Costa, M. Review of arsenic toxicity, speciation and polyadenylation of canonical histones. Toxicol. Appl. Pharmacol. 2019, 375, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Tyler, C.R.; Allan, A.M. The effects of arsenic exposure on neurological and cognitive dysfunction in human and rodent studies: A review. Curr. Environ. Health Rep. 2014, 1, 132–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barajas-Olmos, F.M.; Ortiz-Sanchez, E.; Imaz-Rosshandler, I.; Cordova-Alarcon, E.J.; Martinez-Tovar, A.; Villanueva-Toledo, J.; Morales-Marin, M.E.; Cruz-Colin, J.L.; Rangel, C.; Orozco, L.; et al. Analysis of the dynamic aberrant landscape of DNA methylation and gene expression during arsenic-induced cell transformation. Gene 2019, 711, 143941. [Google Scholar] [CrossRef] [PubMed]
- Ngalame, N.N.O.; Luz, A.L.; Makia, N.; Tokar, E.J. Arsenic Alters Exosome Quantity and Cargo to Mediate Stem Cell Recruitment Into a Cancer Stem Cell-Like Phenotype. Toxicol. Sci. 2018, 165, 40–49. [Google Scholar] [CrossRef] [Green Version]
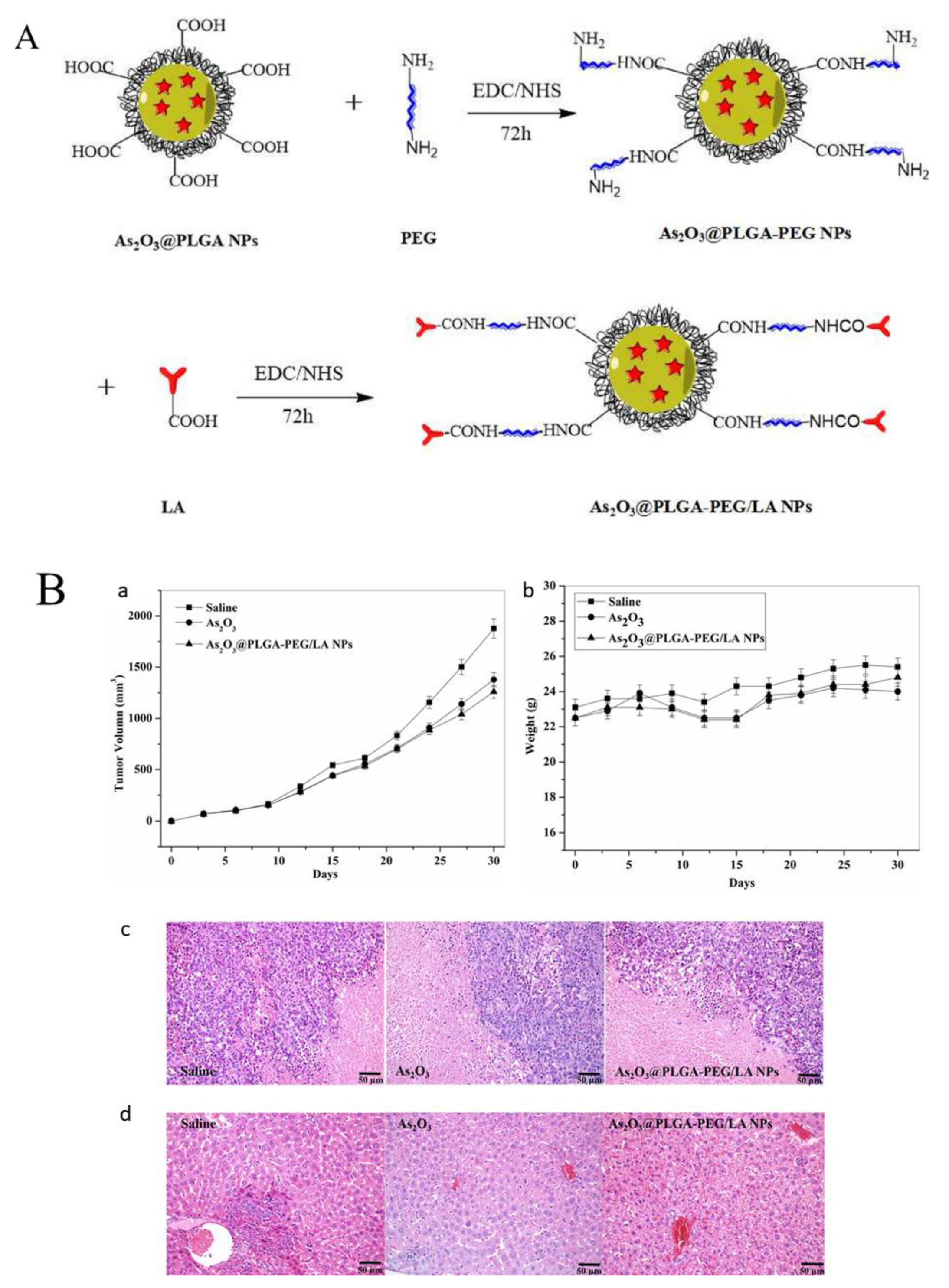
- Song, X.; You, J.; Shao, H.; Yan, C. Effects of surface modification of As2O3-loaded PLGA nanoparticles on its anti-liver cancer ability: An In Vitro and In Vivo study. Colloids Surf. B Biointerfaces 2018, 169, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Liu, C.; Wang, C.; Ma, J.; Xu, H.; Guo, J.; Deng, Y. Arsenic trioxide encapsulated liposomes prepared via copper acetate gradient loading method and its antitumor efficiency. Asian J. Pharm. Sci. 2020, 15, 365–373. [Google Scholar] [CrossRef] [PubMed]
- Eskandari, Z.; Bahadori, F.; Celik, B.; Onyuksel, H. Targeted Nanomedicines for Cancer Therapy, From Basics to Clinical Trials. J. Pharm. Pharm. Sci. 2020, 23, 132–157. [Google Scholar] [CrossRef] [PubMed]
- Wu, Q.; Chen, X.; Wang, P.; Wu, Q.; Qi, X.; Han, X.; Chen, L.; Meng, X.; Xu, K. Delivery of Arsenic Trioxide by Multifunction Nanoparticles to Improve the Treatment of Hepatocellular Carcinoma. ACS Appl. Mater. Interfaces 2020, 12, 8016–8029. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Ahn, R.; Van den Bossche, J.; Thompson, D.H.; O’Halloran, T.V. Folate-mediated intracellular drug delivery increases the anticancer efficacy of nanoparticulate formulation of arsenic trioxide. Mol. Cancer Ther. 2009, 8, 1955–1963. [Google Scholar] [CrossRef] [Green Version]
- Xu, H.; Li, C.; Wei, Y.; Zheng, H.; Zheng, H.; Wang, B.; Piao, J.G.; Li, F. Angiopep-2-modified calcium arsenite-loaded liposomes for targeted and pH-responsive delivery for anti-glioma therapy. Biochem. Biophys. Res. Commun. 2021, 551, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Das, B.; Rahaman, H.; Ghosh, S.K.; Sengupta, M. Synthesis and Characterization of Arsenic(III) Oxide Nanoparticles as Potent Inhibitors of MCF 7 Cell Proliferation through Proapoptotic Mechanism. BioNanoScience 2020, 10, 420–429. [Google Scholar] [CrossRef]
- Kong, D.; Jiang, T.; Liu, J.; Jiang, X.; Liu, B.; Lou, C.; Zhao, B.; Carroll, S.L.; Feng, G. Chemoembolizing hepatocellular carcinoma with microsphere cored with arsenic trioxide microcrystal. Drug Deliv. 2020, 27, 1729–1740. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Sun, S.; Feng, Q.; Wu, G.; Wu, Y.; Kong, N.; Yu, Z.; Yao, J.; Zhang, X.; Chen, W.; et al. Arsenene Nanodots with Selective Killing Effects and their Low-Dose Combination with ss-Elemene for Cancer Therapy. Adv. Mater. 2021, 33, e2102054. [Google Scholar] [CrossRef]
- Chen, X.; Huang, Y.; Chen, H.; Chen, Z.; Chen, J.; Wang, H.; Li, D.; Su, Z. Augmented EPR effect post IRFA to enhance the therapeutic efficacy of arsenic loaded ZIF-8 nanoparticles on residual HCC progression. J. Nanobiotechnol. 2022, 20, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Chi, X.; Yin, Z.; Jin, J.; Li, H.; Zhou, J.; Zhao, Z.; Zhang, S.; Zhao, W.; Xie, C.; Li, J.; et al. Arsenite-loaded nanoparticles inhibit the invasion and metastasis of a hepatocellular carcinoma: In Vitro and In Vivo study. Nanotechnology 2017, 28, 445101. [Google Scholar] [CrossRef] [PubMed]
- Akhtar, A.; Ghali, L.; Wang, S.X.; Bell, C.; Li, D.; Wen, X. Optimisation of Folate-Mediated Liposomal Encapsulated Arsenic Trioxide for Treating HPV-Positive Cervical Cancer Cells In Vitro. Int. J. Mol. Sci. 2019, 20, 2156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahn, R.W.; Chen, F.; Chen, H.; Stern, S.T.; Clogston, J.D.; Patri, A.K.; Raja, M.R.; Swindell, E.P.; Parimi, V.; Cryns, V.L. A novel nanoparticulate formulation of arsenic trioxide with enhanced therapeutic efficacy in a murine model of breast cancer. Clin. Cancer Res. 2010, 16, 3607–3617. [Google Scholar] [CrossRef] [Green Version]
- Zhao, S.; Zhang, X.; Zhang, J.; Zhang, J.; Zou, H.; Liu, Y.; Dong, X.; Sun, X. Intravenous administration of arsenic trioxide encapsulated in liposomes inhibits the growth of C6 gliomas in rat brains. J. Chemother. 2008, 20, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Jin, Z.; Yi, X.; Yang, J.; Zhou, M.; Wu, P.; Yan, G. Liposome-Coated Arsenic-Manganese Complex for Magnetic Resonance Imaging-Guided Synergistic Therapy against Carcinoma. Int. J. Nanomed. 2021, 16, 3775–3788. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; MacDonald, R.C.; Li, S.; Krett, N.L.; Rosen, S.T.; O’Halloran, T.V. Lipid encapsulation of arsenic trioxide attenuates cytotoxicity and allows for controlled anticancer drug release. J. Am. Chem. Soc. 2006, 128, 13348–13349. [Google Scholar] [CrossRef]
- Hoonjan, M.; Sachdeva, G.; Chandra, S.; Kharkar, P.S.; Sahu, N.; Bhatt, P. Investigation of HSA as a biocompatible coating material for arsenic trioxide nanoparticles. Nanoscale 2018, 10, 8031–8041. [Google Scholar] [CrossRef] [PubMed]
- Larsen, M.T.; Kuhlmann, M.; Hvam, M.L.; Howard, K.A. Albumin-based drug delivery: Harnessing nature to cure disease. Mol. Cell. Ther. 2016, 4, 3. [Google Scholar] [CrossRef] [Green Version]
- Manoochehri, S.; Darvishi, B.; Kamalinia, G.; Amini, M.; Fallah, M.; Ostad, S.N.; Atyabi, F.; Dinarvand, R. Surface modification of PLGA nanoparticles via human serum albumin conjugation for controlled delivery of docetaxel. DARU J. Pharm. Sci. 2013, 21, 58. [Google Scholar] [CrossRef] [Green Version]
- Kalidasan, V.; Liu, X.L.; Herng, T.S.; Yang, Y.; Ding, J. Bovine Serum Albumin-Conjugated Ferrimagnetic Iron Oxide Nanoparticles to Enhance the Biocompatibility and Magnetic Hyperthermia Performance. Nanomicro Lett. 2016, 8, 80–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Z.; Yang, M.; Peng, J. Evaluation of arsenic trioxide-loaded albumin nanoparticles as carriers: Preparation and antitumor efficacy. Drug Dev. Ind. Pharm. 2008, 34, 834–839. [Google Scholar] [CrossRef]
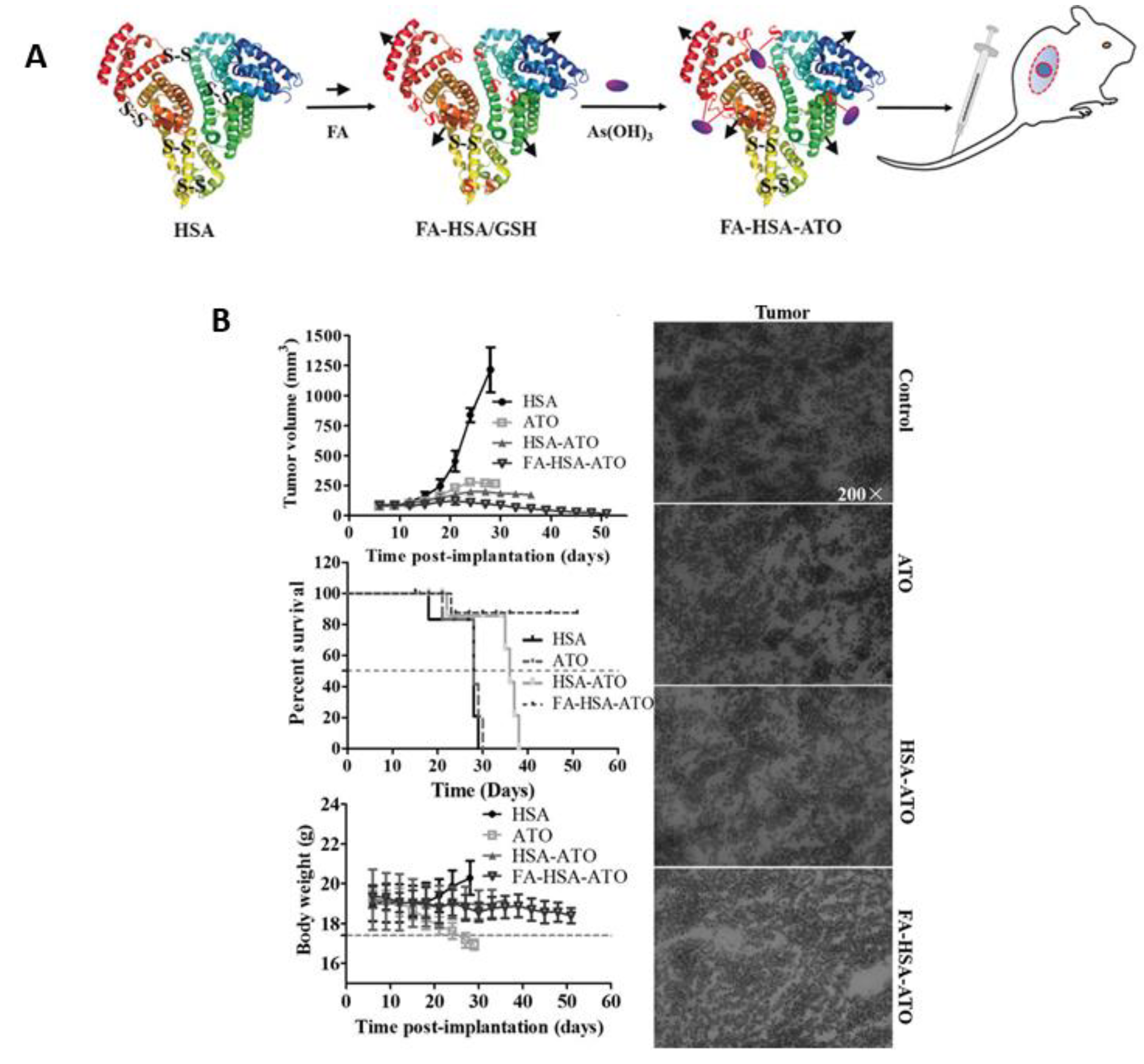
- Peng, Y.; Zhao, Z.; Liu, T.; Li, X.; Hu, X.; Wei, X.; Zhang, X.; Tan, W. Smart human-serum-albumin–As2O3 nanodrug with self-amplified folate receptor-targeting ability for chronic myeloid leukemia treatment. Angew. Chem. Int. Ed. 2017, 56, 10845–10849. [Google Scholar] [CrossRef]
- Ortega-Oller, I.; Padial-Molina, M.; Galindo-Moreno, P.; O’Valle, F.; Jódar-Reyes, A.B.; Peula-García, J.M. Bone regeneration from PLGA micro-nanoparticles. BioMed Res. Int. 2015, 2015, 415289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, C.; Liu, D.; Lin, W. Nanomedicine applications of hybrid nanomaterials built from metal–ligand coordination bonds: Nanoscale metal–organic frameworks and nanoscale coordination polymers. Chem. Rev. 2015, 115, 11079–11108. [Google Scholar] [CrossRef] [PubMed]
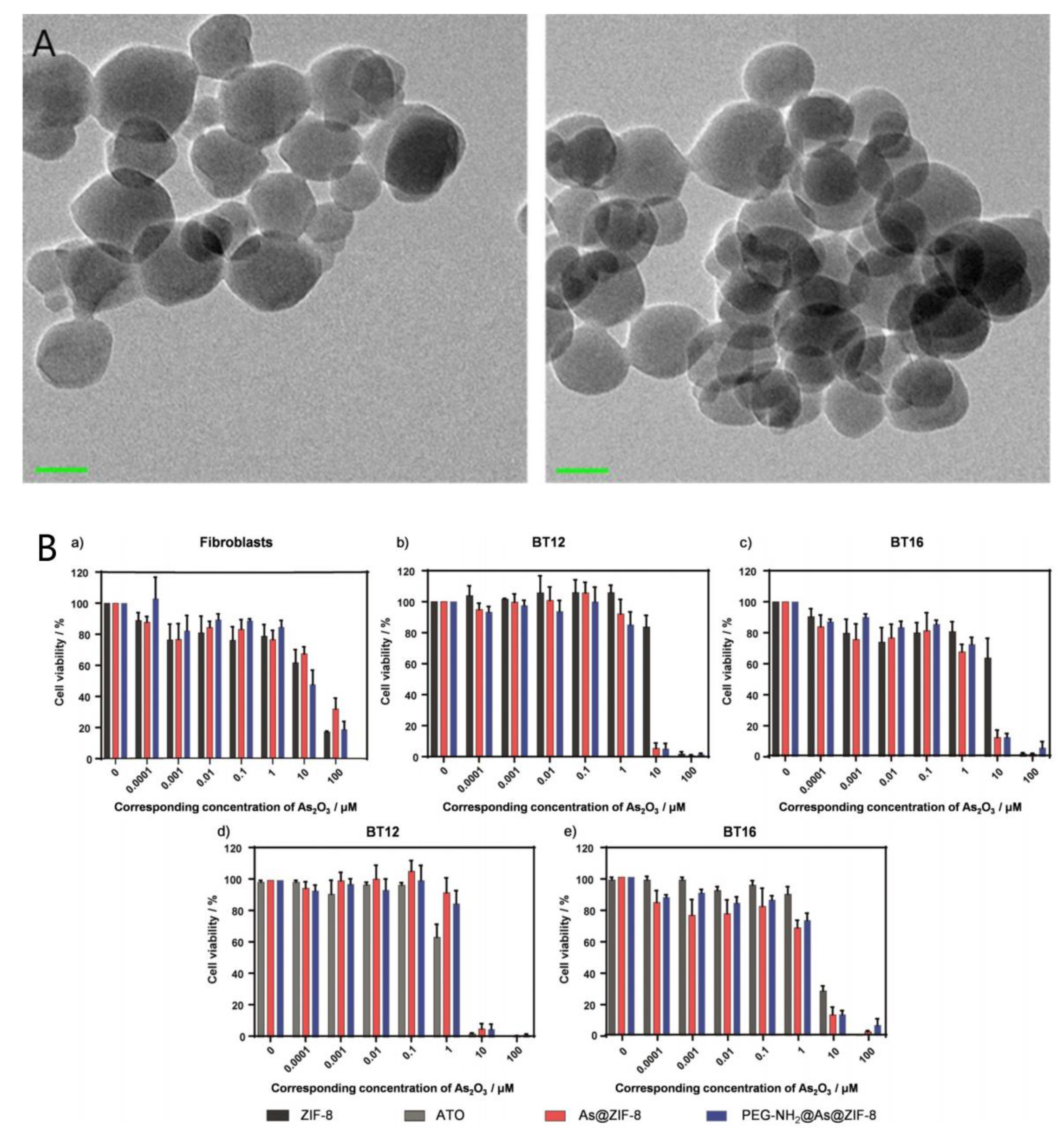
- Ettlinger, R.; Moreno, N.; Volkmer, D.; Kerl, K.; Bunzen, H. Zeolitic Imidazolate Framework-8 as pH-Sensitive Nanocarrier for “Arsenic Trioxide” Drug Delivery. Chemistry 2019, 25, 13189–13196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, Z.; Zhang, H.; Chi, X.; Li, H.; Yin, Z.; Huang, D.; Wang, X.; Gao, J. Silica nanovehicles endow arsenic trioxide with an ability to effectively treat cancer cells and solid tumors. J. Mater. Chem. B 2014, 2, 6313–6323. [Google Scholar] [CrossRef]
- Quan, G.; Pan, X.; Wang, Z.; Wu, Q.; Li, G.; Dian, L.; Chen, B.; Wu, C. Lactosaminated mesoporous silica nanoparticles for asialoglycoprotein receptor targeted anticancer drug delivery. J. Nanobiotechnol. 2015, 13, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fei, W.; Li, C.; Tao, J.; Cai, X.; Yao, W.; Ye, Y.; Zhang, Y.; Yao, Y.; Song, Q.; Li, F.; et al. Construction of arsenic-metal complexes loaded nanodrugs for solid tumor therapy: A mini review. Int. J. Pharm. 2020, 583, 119385. [Google Scholar] [CrossRef] [PubMed]
- Cicconi, L.; Lo-Coco, F. Current management of newly diagnosed acute promyelocytic leukemia. Ann. Oncol. 2016, 27, 1474–1481. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Xie, Y. Nanodrug delivery systems for targeting the endogenous tumor microenvironment and simultaneously overcoming multidrug resistance properties. J. Control. Release 2017, 251, 49–67. [Google Scholar] [CrossRef]
- Li, Y.; Xia, Y.-Z.; Hu, S.-M.; Kong, L.-Y.; Yang, L. Tooniliatone A sensitizes multidrug resistant cancer cells by decreasing Bcl-xL via activation of JNK MAPK signaling. Phytomedicine 2019, 62, 152947. [Google Scholar] [CrossRef]
- Yu, Q.; Chen, B.; Zhang, X.; Qian, W.; Ye, B.; Zhou, Y. Arsenic trioxide-enhanced, matrine-induced apoptosis in multiple myeloma cell lines. Planta Med. 2013, 79, 775–781. [Google Scholar] [CrossRef] [Green Version]
- Mesbahi, Y.; Zekri, A.; Ahmadian, S.; Alimoghaddam, K.; Ghavamzadeh, A.; Ghaffari, S.H. Targeting of EGFR increase anti-cancer effects of arsenic trioxide: Promising treatment for glioblastoma multiform. Eur. J. Pharmacol. 2018, 820, 274–285. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.M.; Liu, X.J.; Wang, S.F.; Ouyang, L.Q.; Li, H.; Ding, J.S.; Deng, G.M.; Zhou, W.H. Imatinib co-loaded targeted realgar nanocrystal for synergistic therapy of chronic myeloid leukemia. J. Control. Release 2021, 338, 190–200. [Google Scholar] [CrossRef] [PubMed]
- Byun, J.M.; Lee, D.S.; Landen, C.N.; Kim, D.H.; Kim, Y.N.; Lee, K.B.; Sung, M.S.; Park, S.G.; Jeong, D.H. Arsenic trioxide and tetraarsenic oxide induce cytotoxicity and have a synergistic effect with cisplatin in paclitaxel-resistant ovarian cancer cells. Acta Oncologica 2019, 58, 1594–1602. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Cheng, C.; Peng, L.; Gao, M.; Xi, M.; Rousseaux, S.; Khochbin, S.; Wang, J.; Mi, J. Combination of arsenic trioxide and Dasatinib: A new strategy to treat Philadelphia chromosome-positive acute lymphoblastic leukaemia. J. Cell. Mol. Med. 2018, 22, 1614–1626. [Google Scholar] [CrossRef] [Green Version]
- Hu, J.; Sun, Q.; Fang, W.; Wang, Q. Effect of combination of all-trans retinoic acid and arsenic trioxide on apoptosis of acute promyelocytic leukemia cells. Cell. Mol. Biol. 2019, 65, 97–100. [Google Scholar] [CrossRef]
- Miodragovic, D.U.; Quentzel, J.A.; Kurutz, J.W.; Stern, C.L.; Ahn, R.W.; Kandela, I.; Mazar, A.; O’Halloran, T.V. Robust Structure and Reactivity of Aqueous Arsenous Acid-Platinum(II) Anticancer Complexes. Angew. Chem. Int. Ed. 2013, 52, 10749–10752. [Google Scholar] [CrossRef] [Green Version]
- Bureta, C.; Saitoh, Y.; Tokumoto, H.; Sasaki, H.; Maeda, S.; Nagano, S.; Komiya, S.; Taniguchi, N.; Setoguchi, T. Synergistic effect of arsenic trioxide, vismodegib and temozolomide on glioblastoma. Oncol. Rep. 2019, 41, 3404–3412. [Google Scholar] [CrossRef] [PubMed]
- Dizaji, M.Z.; Malehmir, M.; Ghavamzadeh, A.; Alimoghaddam, K.; Ghaffari, S.H. Synergistic effects of arsenic trioxide and silibinin on apoptosis and invasion in human glioblastoma U87MG cell line. Neurochem. Res. 2012, 37, 370–380. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.-B.; Chen, X.-J.; Fan, X.-D.; Zhu, J.-J.; Wei, Y.-H.; Zheng, H.-S.; Zheng, H.-Y.; Wang, B.-H.; Piao, J.-G.; Li, F.-Z. Lipid/PAA-coated mesoporous silica nanoparticles for dual-pH-responsive codelivery of arsenic trioxide/paclitaxel against breast cancer cells. Acta Pharmacol. Sin. 2021, 42, 832–842. [Google Scholar] [CrossRef] [PubMed]
- Meister, M.T.; Boedicker, C.; Graab, U.; Hugle, M.; Hahn, H.; Klingebiel, T.; Fulda, S. Arsenic trioxide induces Noxa-dependent apoptosis in rhabdomyosarcoma cells and synergizes with antimicrotubule drugs. Cancer Lett. 2016, 381, 287–295. [Google Scholar] [CrossRef]
- Klauser, E.; Gulden, M.; Maser, E.; Seibert, S.; Seibert, H. Additivity, antagonism, and synergy in arsenic trioxide-induced growth inhibition of C6 glioma cells: Effects of genistein, quercetin and buthionine-sulfoximine. Food Chem. Toxicol. 2014, 67, 212–221. [Google Scholar] [CrossRef]
- Kim, H.R.; Kim, E.J.; Yang, S.H.; Jeong, E.T.; Park, C.; Kim, S.J.; Youn, M.J.; So, H.S.; Park, R. Combination treatment with arsenic trioxide and sulindac augments their apoptotic potential in lung cancer cells through activation of caspase cascade and mitochondrial dysfunction. Int. J. Oncol. 2006, 28, 1401–1408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mandegary, A.; Torshabi, M.; Seyedabadi, M.; Amirheidari, B.; Sharif, E.; Ghahremani, M.H. Indomethacin-enhanced anticancer effect of arsenic trioxide in A549 cell line: Involvement of apoptosis and phospho-ERK and p38 MAPK pathways. BioMed Res. Int. 2013, 2013, 237543. [Google Scholar] [CrossRef] [PubMed]
- Zeng, L.J.; Li, J.G.; Wang, Y.; Qian, C.C.; Chen, Y.T.; Zhang, Q.B.; Wu, W.; Lin, Z.; Liang, J.Z.; Shuai, X.T.; et al. Combination of siRNA-directed Kras oncogene silencing and arsenic-induced apoptosis using a nanomedicine strategy for the effective treatment of pancreatic cancer. Nanomed. Nanotechnol. Biol. Med. 2014, 10, 463–472. [Google Scholar] [CrossRef]
- Feng, C.; Gong, R.; Zheng, Q.; Yang, G.; He, M.; Lei, H.; Li, X.; Zhang, L.; Xu, Z.; Liu, S.; et al. Synergistic anti-tumor effects of arsenic trioxide and blue LED irradiation on human osteosarcoma. Int. J. Biol. Sci. 2019, 15, 386–394. [Google Scholar] [CrossRef] [Green Version]
- Walasek, A. The new perspectives of targeted therapy in acute myeloid leukemia. Adv. Clin. Exp. Med. 2019, 28, 271–276. [Google Scholar] [CrossRef]
- Qi, K.; Li, Y.; Huang, K.; Xiong, X.; Chuchu, F.; Zhang, C.; Weng, W. Pre-application of arsenic trioxide may potentiate cytotoxic effects of vinorelbine/docetaxel on neuroblastoma SK-N-SH cells. Biomed. Pharmacother. 2019, 113, 108665. [Google Scholar] [CrossRef]
- Gartenhaus, R.B.; Prachand, S.N.; Paniaqua, M.; Li, Y.Y.; Gordon, L.I. Arsenic trioxide cytotoxicity in steroid and chemotherapy-resistant myeloma cell lines: Enhancement of apoptosis by manipulation of cellular redox state. Clin. Cancer Res. 2002, 8, 566–572. [Google Scholar]
- Kallinteri, P.; Fatouros, D.; Klepetsanis, P.; Antimisiaris, S.G. Arsenic trioxide liposomes: Encapsulation efficiency and In Vitro stability. J. Liposome Res. 2004, 14, 27–38. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nanoparticle Formulation | Experimental Models | Drug Delivery Targets | Outcome of Treatment | References |
|---|---|---|---|---|
| Liposome | In vitro | Via folate receptor (FR) mediated endocytosis | Significantly increased both the potency and specificity of ATO to the relatively insensitive solid tumor-derived cells | [66] |
| In vitro and in vivo | Mediated by the lipoprotein receptor-related (LRP) receptor | Promoted the anti-glioma effect of ATO | [67] | |
| Protein | In vitro | Serum albumin interacts with cell surface glycoprotein 60 receptor (albondin) and/or SPARC, leading to transcytosis | Increased cellular uptake and had better cytotoxicity | [68] |
| Polymers | In vitro and in vivo | Chemoembolization of tumor vessels was performed by drug elution | Inhibited tumor growth on HCC cells | [69] |
| In vitro and in vivo | Via the modified with DSPE-mPEG to prolong the in vivo systemic circulation of the nanodots | Effectively reduced the viability of different cancer cells but showed less toxicity in normal cells, inhibited the growth of solid tumors | [70] | |
| Coordination polymer | In vitro | Drug release triggered by a pH change in the vicinity of the tumour | Triggered specific cytotoxicity at low concentrations and drastically reduced the possible toxicity on healthy tissues. | [71] |
| Hollow porous silica nanoparticles-based nanovehicles | In vitro and in vivo | By passive targeting of the HSN through an enhanced permeability and retention effect | Significantly improves the efficacy of ATO for tumor treatment and increases the cellular uptake of arsenite. | [72] |
| In vitro and in vivo | A TPP mitochondrial targeting marker was loaded to enhance mitochondrial targeting by the nanoparticles | Improves the activity of chemotherapeutics and the efficiency of hyperthermia therapy | [65] |
| ATO in Combination with Chemo Agents | Experimental Models | Identified Molecular Targets and Signaling Pathways | Outcome of Combinatorial Treatment | References |
|---|---|---|---|---|
| Dasatinib | In vitro | Activated the UPR apoptotic IRE1/JNK/PUMA axis, neutralized the UPR ATF4-dependent anti-apoptotic axis | Increased apoptosis in both TKI-sensitive and resistant Ph+ ALL cell lines | [97] |
| Erlotinib | In vitro | Triggered ATO-induced apoptosis in GBM cell lines and increased reactive oxygen species generation | Synergistically reduced metabolic activity, proliferation and colony forming potential in treated GBM cell lines | [94] |
| All-trans retinoic acid (ATRA) | In vitro and In vivo | ↑ Apoptosis of NB4 cells and ↓ serum IL-6 and TNF-α levels in patients with APL | Significantly inhibits the proliferation of NB4 cells and promotes their apoptosis, and reduces inflammatory responses in patients with APL | [98] |
| Cisplatin | In vitro | Induced apoptotic cell death | Displayed significant anti-cancer activity in a panel of human cancer cell lines and overcame the tumor-based drug resistance | [99] |
| Temozolomide (TMZ) and Vismodegib (VIS) | In vitro and In vivo | Damaged the DNA repair enzyme encoded in the human as O6-methylguanine-DNA methyltransferase (MGMT) and inhibited The Hedgehog (Hh) signalling pathway | Synergistically inhibited the proliferation of glioblastoma and decreased tumor growth in mice | [100] |
| Silibin | In vitro | Decreased the mRNA levels of cathepsin B, urokinase-type plasminogen activator, Bcl-2 and upregulated caspase-3 | Synergistically inhibits glioma cell proliferation and induced apoptosis | [101] |
| Paclitaxel | In vitro and In vivo | Inhibited the expression of Bcl-2, caspase-7, caspase-9, cyclin B-1, and cyclin D-1; induced apoptosis | Significantly affected cell-cycle and induced apoptosis | [102] |
| Vincristine | In vitro | Triggered caspase-dependent apoptosis via the mitochondrial pathway | Synergistically induced apoptosis | [103] |
| Butylthionine sulfoxide | In vitro | Depleted intracellular GSH | Enhanced the ATO-toxicity in C6 cells | [104] |
| Ascorbic acid | In vitro | Activated caspase-3 to trigger apoptosis, upregulated the expression of caspase-1 and promoted formation of inflammasomes | Enhanced the proapoptotic effects of arsenic, synergistically inhibited the viability of human CRC cells | [26] |
| Itraconazole | In vivo | Modulating Hedgehog (Hh) pathway | Effectively reduced tumor growth of medulloblastoma cells | [23] |
| Sulindac | In vitro | Increased the catalytic activity of caspase-3, -8, and -9 along with induction of Fas/FasL expression and cytosolic release of cytochrome c | Synergistically enhanced cytotoxicity to NCI-H157 lung cancer cells | [105] |
| Indomethacin | In vitro | Activation of ERK and p38 pathways, considerably high Caspase-3 activity | Exerted a very potent in vitro cytotoxic effect against A549 lung cancer cells | [106] |
| SiRNA-directed Kras oncogene silencing | In vitro and In vivo | Down-regulation of the mutant Kras gene by siRNA and tumor growth inhibition of arsenic | Inhibited proliferative, migratory and invasive pancreatic cancer cells, and substantially improved the apoptotic effect | [107] |
| Blue LED irradiation | In vitro | Increased ROS accumulation, DNA damaged mediated p53 activation | Significantly decreased the percentages of proliferative cells, and increased apoptotic rate on human osteosarcoma | [108] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, M.; Zhang, Y.; Fang, M.; Jehan, S.; Zhou, W. Current Advances of Nanomedicines Delivering Arsenic Trioxide for Enhanced Tumor Therapy. Pharmaceutics 2022, 14, 743. https://doi.org/10.3390/pharmaceutics14040743
Yu M, Zhang Y, Fang M, Jehan S, Zhou W. Current Advances of Nanomedicines Delivering Arsenic Trioxide for Enhanced Tumor Therapy. Pharmaceutics. 2022; 14(4):743. https://doi.org/10.3390/pharmaceutics14040743
Chicago/Turabian StyleYu, Mengzhen, Yanwen Zhang, Meirong Fang, Shah Jehan, and Wenhu Zhou. 2022. "Current Advances of Nanomedicines Delivering Arsenic Trioxide for Enhanced Tumor Therapy" Pharmaceutics 14, no. 4: 743. https://doi.org/10.3390/pharmaceutics14040743