
Imaging the Effects of Whole-Body Vibration on the Progression of Hepatic Steatosis by Quantitative Ultrasound Based on Backscatter Envelope Statistics

 ,
,  and
and 
Abstract
:1. Introduction
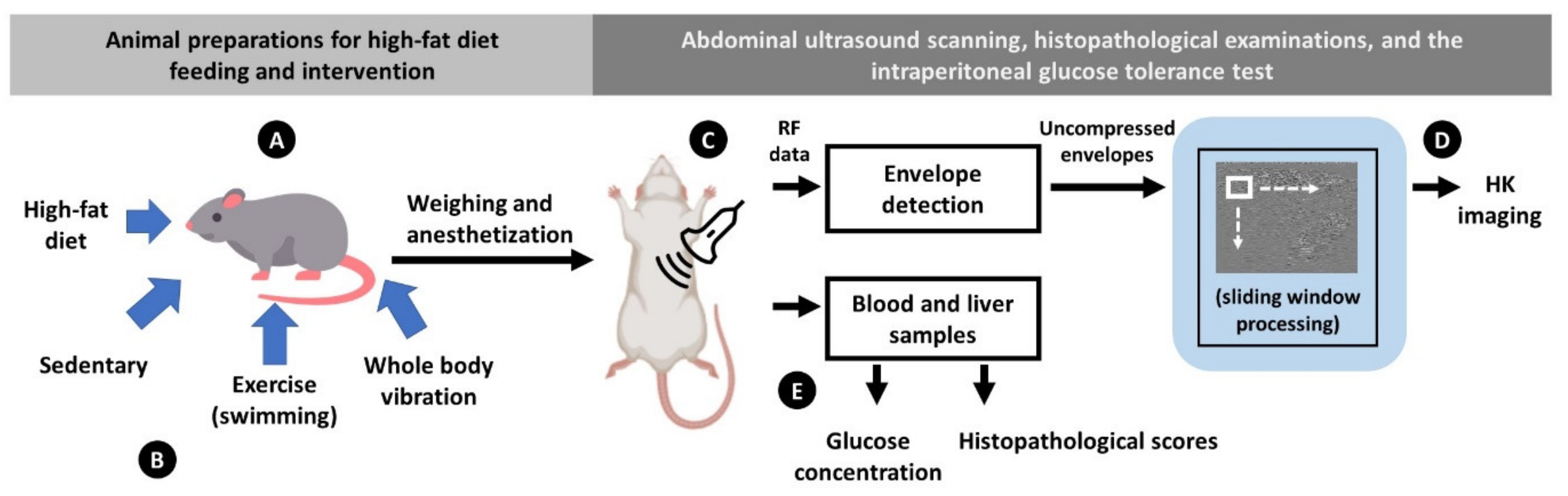
2. Materials and Methods
2.1. Animal Preparation
2.2. Interventions
2.3. Ultrasound Data Acquisition
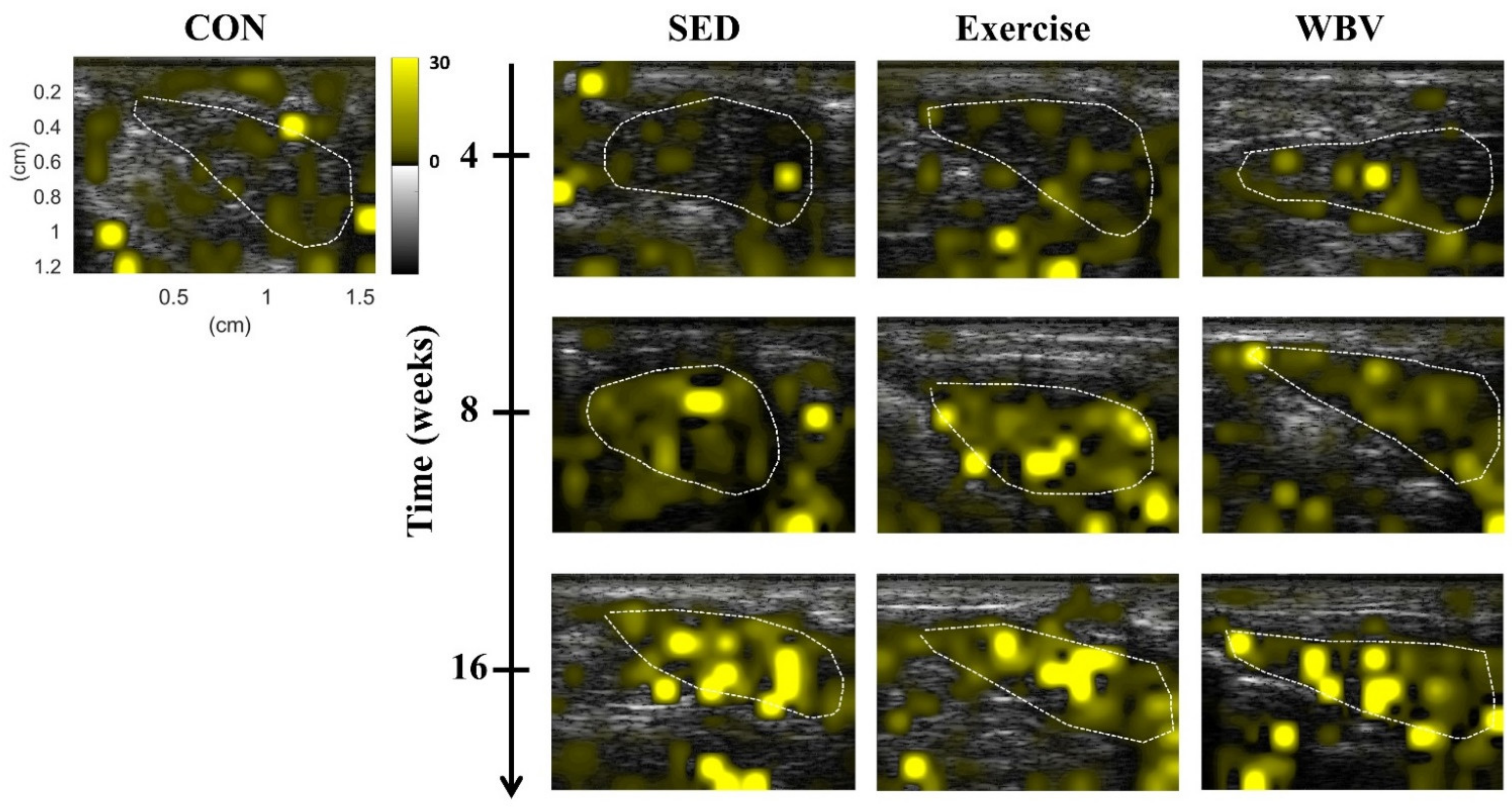
2.4. Ultrasound HK Parametric Imaging
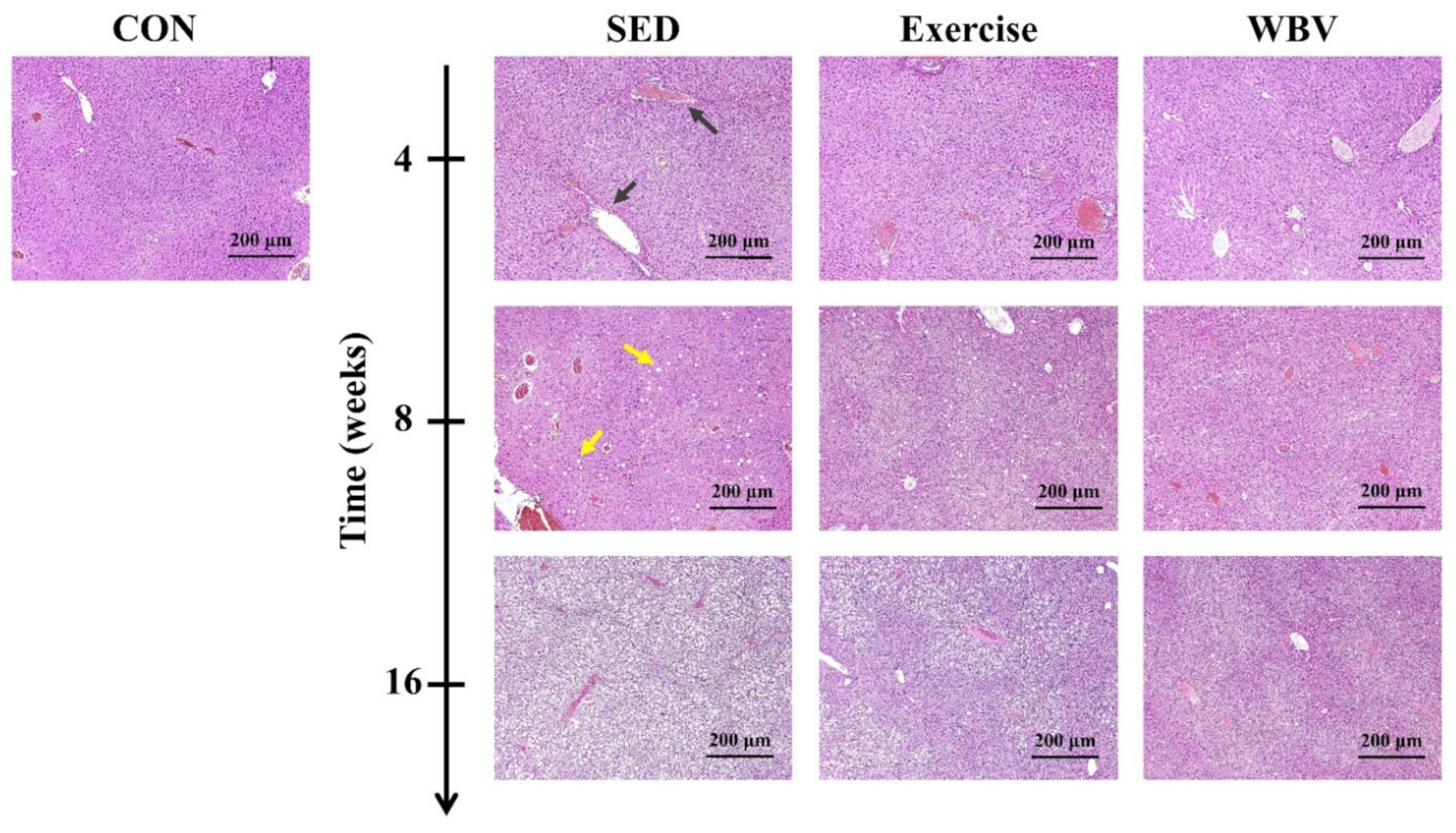
2.5. MetS Evaluations and Histopathological Examinations
2.6. Statistical Analysis
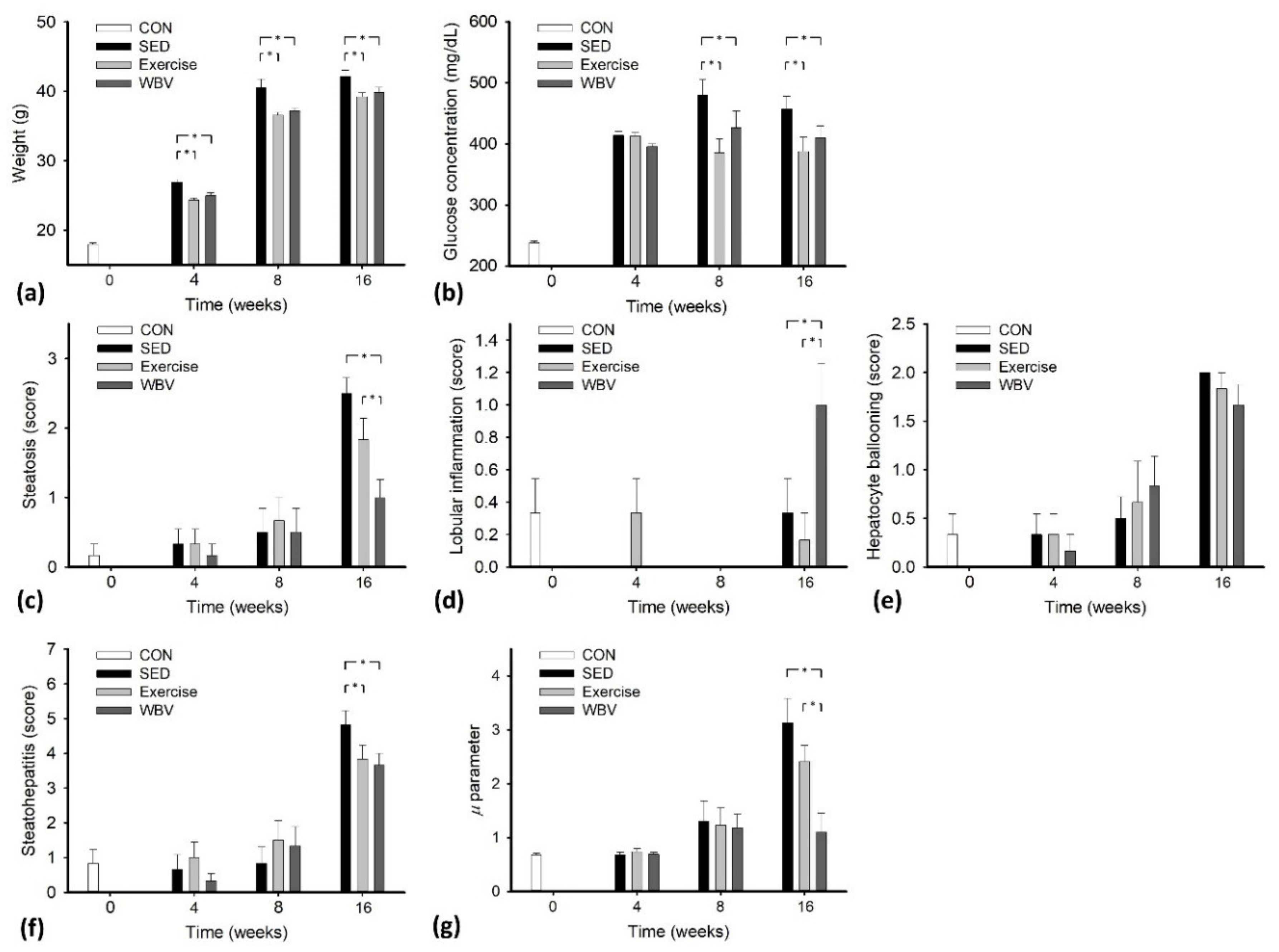
3. Results
4. Discussion
4.1. The Significance of This Study
4.2. Effects of WBV on Hepatic Steatosis
4.3. Changes in Acoustic Microstructures in a Fat-Infiltrated Liver
4.4. Usefulness of the HK Parameter in Characterizing Hepatic Steatosis
4.5. Limitations and Future Work
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Straub, B.K.; Schirmacher, P. Pathology and biopsy assessment of non–alcoholic fatty liver disease. Dig. Dis. 2010, 28, 197–202. [Google Scholar] [CrossRef]
- Targher, G.; Day, C.P.; Bonora, E. Risk of cardiovascular disease in patients with nonalcoholic fatty liver disease. N. Engl. J. Med. 2010, 363, 1341–1350. [Google Scholar] [CrossRef] [Green Version]
- Starley, B.Q.; Calcagno, C.J.; Harrison, S.A. Nonalcoholic fatty liver disease and hepatocellular carcinoma: A weighty connection. Hepatology 2010, 51, 1820–1832. [Google Scholar] [CrossRef]
- Lee, M.K.; Han, K.; Kim, M.K.; Koh, E.S.; Kim, E.S.; Nam, G.E.; Kwon, H.S. Changes in metabolic syndrome and its components and the risk of type 2 diabetes: A nationwide cohort study. Sci. Rep. 2020, 10, 2313. [Google Scholar] [CrossRef] [PubMed]
- Watt, M.J.; Miotto, P.M.; De Nardo, W.; Montgomery, M.K. The liver as an endocrine organ–linking NAFLD and insulin resistance. Endocr. Rev. 2019, 40, 1367–1393. [Google Scholar] [CrossRef] [PubMed]
- Gargiulo, P.; Marsico, F.; Renga, F.; Dell’Aversana, S.; Esposito, I.; Marciano, C.; Dellegrottaglie, S.; Perrone-Filardi, P.; Paolillo, S. The metabolic syndrome in heart failure: Insights to specific mechanisms. Heart Fail. Rev. 2020, 25, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Eslam, M.; Sanyal, A.J.; George, J.; International Consensus Panel. MAFLD: A consensus–driven proposed nomenclature for metabolic associated fatty liver disease. Gastroenterology 2020, 158, 1999–2014. [Google Scholar] [CrossRef] [PubMed]
- Eslam, M.; Newsome, P.N.; Sarin, S.K.; Anstee, Q.M.; Targher, G.; Romero-Gomez, M.; Zelber-Sagi, S.; Wai-Sun Wong, V.; Dufour, J.F.; Schattenberg, J.M.; et al. A new definition for metabolic dysfunction–associated fatty liver disease: An international expert consensus statement. J. Hepatol. 2020, 73, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Gastaldelli, A. Fatty liver disease: The hepatic manifestation of metabolic syndrome. Hypertens. Res. 2010, 33, 546–547. [Google Scholar] [CrossRef]
- Romero–Gómez, M.; Zelber-Sagi, S.; Trenell, M. Treatment of NAFLD with diet, physical activity and exercise. J. Hepatol. 2017, 67, 829–846. [Google Scholar] [CrossRef] [Green Version]
- Redman, L.M.; Rood, J.; Anton, S.D.; Champagne, C.; Smith, S.R.; Ravussin, E.; Pennington Comprehensive Assessment of Long-Term Effects of Reducing Intake of Energy (CALERIE) Research Team. Calorie restriction and bone health in young, overweight individuals. Arch. Intern. Med. 2008, 168, 1859–1866. [Google Scholar] [CrossRef]
- Matarese, L.E.; Pories, W.J. Adult weight loss diets: Metabolic effects and outcomes. Nutr. Clin. Pract. 2014, 29, 759–767. [Google Scholar] [CrossRef]
- Dhurandhar, E.J.; Kaiser, K.A.; Dawson, J.A.; Alcorn, A.S.; Keating, K.D.; Allison, D.B. Predicting adult weight change in the real world: A systematic review and meta–analysis accounting for compensatory changes in energy intake or expenditure. Int. J. Obes. 2015, 39, 1181–1187. [Google Scholar] [CrossRef] [Green Version]
- Van der Windt, D.J.; Sud, V.; Zhang, H.; Tsung, A.; Huang, H. The effects of physical exercise on fatty liver disease. Gene Expr. 2018, 18, 89–101. [Google Scholar] [CrossRef] [Green Version]
- McArdle, W.D.; Katch, F.I.; Katch, V.L. Exercise Physiology: Nutrition, Energy, and Human Performance; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2010. [Google Scholar]
- Schultz, A.; Mendonca, L.S.; Aguila, M.B.; Mandarim-de-Lacerda, C.A. Swimming training beneficial effects in a mice model of nonalcoholic fatty liver disease. Exp. Toxicol. Pathol. 2012, 64, 273–282. [Google Scholar] [CrossRef]
- Fischer, M.; Vialleron, T.; Laffaye, G.; Fourcade, P.; Hussein, T.; Chèze, L.; Deleu, P.; Honeine, J.; Yiou, E.; Delafontaine, A. Long-term effects of whole-body vibration on human gait: A systematic review and meta-analysis. Front. Neurol. 2019, 10, 627. [Google Scholar] [CrossRef] [PubMed]
- Reijne, A.C.; Ciapaite, J.; van Dijk, T.H.; Havinga, R.; van der Zee, E.A.; Groen, A.K.; Reijngoud, D.; Bakker, B.M.; van Dijk, G. Whole-body vibration partially reverses aging-induced increases in visceral adiposity and hepatic lipid storage in mice. PLoS ONE 2016, 11, e0149419. [Google Scholar] [CrossRef] [Green Version]
- Luu, Y.K.; Ozcivici, E.; Capilla, E.; Adler, B.; Chan, E.; Shroyer, K.; Rubin, J.; Judex, S.; Pessin, J.E.; Rubin, C.T. Development of diet-induced fatty liver disease in the aging mouse is suppressed by brief daily exposure to low-magnitude mechanical signal. Int. J. Obes. 2010, 34, 401–405. [Google Scholar] [CrossRef] [Green Version]
- Ren, Z.; Lan, Q.; Chen, Y.; Chan, Y.W.J.; Mahady, G.B.; Lee, S.M. Low-magnitude high-frequency vibration decreases body weight gain and increases muscle strength by enhancing the p38 and AMPK pathways in db/db mice. Diabetes Metab. Syndr. Obes. 2020, 13, 979–989. [Google Scholar] [CrossRef] [Green Version]
- Oh, A.; Oshida, N.; Someya, N.; Maruyama, T.; Isobe, T.; Okamoto, Y.; Kim, T.; Kim, B.; Shoda, J. Whole-body vibration for patients with nonalcoholic fatty liver disease: A 6-month prospective study. Physiol. Rep. 2019, 7, e14062. [Google Scholar] [CrossRef]
- Shung, K.K.; Thieme, G.A. Ultrasonic Scattering in Biological Tissues; CRC Press: Boca Raton, FL, USA, 1993. [Google Scholar]
- Mamou, J.; Oelze, M.L. Review of Envelope Statistics Models for Quantitative Ultrasound Imaging and Tissue Characterization. In Quantitative Ultrasound in Soft Tissues; Springer: New York, NY, USA, 2013; Chapter 10. [Google Scholar]
- Huang, Y.; Wang, Z.; Liao, B.; Liang, J.; Zhou, L.; Wang, F.; Li, W.; Liu, J.Y.; Xie, X.Y.; Lu, M.; et al. Assessment of liver fibrosis in chronic hepatitis B using acoustic structure quantification: Quantitative morphological ultrasound. Eur. Radiol. 2016, 26, 2344–2451. [Google Scholar] [CrossRef] [PubMed]
- Dutt, V.; Greenleaf, J.F. Ultrasound echo envelope analysis using a homodyned K distribution signal model. Ultrason. Imaging 1994, 16, 265–287. [Google Scholar] [CrossRef] [PubMed]
- Oelze, M.L.; Mamou, J. Review of quantitative ultrasound: Envelope statistics and backscatter coefficient imaging and contributions to diagnostic ultrasound. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2016, 63, 336–351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Z.; Fang, J.; Cristea, A.; Lin, Y.; Tsai, Y.; Wan, Y.; Yeow, K.; Ho, M.; Tsui, P. Value of homodyned K distribution in ultrasound parametric imaging of hepatic steatosis: An animal study. Ultrasonics 2020, 101, 106001. [Google Scholar] [CrossRef]
- Tsai, Y.W.; Zhou, Z.; Gong, C.A.; Tai, D.; Cristea, A.; Lin, Y.; Tang, Y.; Tsui, P. Ultrasound detection of liver fibrosis in individuals with hepatic steatosis using the homodyned K distribution. Ultrasound Med. Biol. 2021, 47, 84–94. [Google Scholar] [CrossRef]
- Seo, D.Y.; Lee, S.R.; Kim, N.; Ko, K.S.; Rhee, B.D.; Han, J. Humanized animal exercise model for clinical implication. Pflug. Arch. 2014, 466, 1673–1687. [Google Scholar] [CrossRef]
- Arida, R.M.; Scorza, F.A.; da Silva, S.G.; Cysneiros, R.M.; Cavalheiro, E.A. Exercise paradigms to study brain injury recovery in rodents. Am. J. Phys. Med. Rehabil. 2011, 90, 452–465. [Google Scholar] [CrossRef]
- Cardoso, A.M.; Abdalla, F.H.; Bagatini, M.D.; Martins, C.C.; Fiorin, F.D.; Baldissarelli, J.; Costa, P.; de Mello, F.F.; Fiorenza, A.M.; da Silva Serres, J.D.; et al. Swimming training prevents alterations in acetylcholinesterase and butyrylcholinesterase activities in hypertensive rats. Am. J. Hypertens. 2014, 27, 522–529. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.C.; Tseng, T.L.; Huang, W.C.; Chung, Y.H.; Chuang, H.L.; Wu, J.H. Whole–body vibration training effect on physical performance and obesity in mice. Int. J. Med. Sci. 2014, 11, 1218–1227. [Google Scholar] [CrossRef] [Green Version]
- Bahga, S.S. Experimental Uncertainty Analysis: A Textbook for Science and Engineering Students, 1st ed.; White Falcon Publishing: Chandigarh, India, 2021; pp. 80–101. [Google Scholar]
- Destrempes, F.; Porée, J.; Cloutier, G. Estimation method of the homodyned K-distribution based on the mean intensity and two log-moments. SIAM J. Imaging Sci. 2013, 6, 1499–1530. [Google Scholar] [CrossRef]
- Fernández, A.; Ibáñez, A.; Parrilla, M.; Elvira, L.; Bassat, Q.; Jiménez, J. Estimation of the concentration of particles in suspension based on envelope statistics of ultrasound backscattering. Ultrasonics 2021, 116, 106501. [Google Scholar] [CrossRef]
- Han, A.; Zhang, Y.N.; Boehringer, A.S.; Montes, V.; Andre, M.P.; Erdman, J.W.; Loomba, R.; Valasek, M.A.; Sirlin, C.B.; O’Brien, W.D. Assessment of hepatic steatosis in nonalcoholic fatty liver disease by using quantitative US. Radiology 2020, 295, 106–113. [Google Scholar] [CrossRef]
- Jørgensen, M.S.; Tornqvist, K.S.; Hvid, H. Calculation of glucose dose for intraperitoneal glucose tolerance tests in lean and obese mice. J. Am. Assoc. Lab. Anim. Sci. 2017, 56, 95–97. [Google Scholar]
- Kleiner, D.E.; Brunt, E.M.; Natta, M.V.; Behling, C.; Contos, M.J.; Cummings, O.W.; Ferrell, L.D.; Liu, Y.C.; Torbenson, M.S.; Unalp-Arida, A.; et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology 2005, 41, 1313–1321. [Google Scholar] [CrossRef]
- Hauke, J.; Kossowski, T. Comparison of values of Pearson’s and Spearman’s correlation coefficients on the same sets of data. Quaest. Geogr. 2011, 30, 87–93. [Google Scholar] [CrossRef] [Green Version]
- De Winter, J.C.F.; Gosling, S.D.; Potter, J. Comparing the Pearson and Spearman correlation coefficients across distributions and sample sizes: A tutorial using simulations and empirical data. Psychol. Methods 2016, 21, 273–290. [Google Scholar] [CrossRef]
- Zaidell, L.N.; Mileva, K.N.; Sumners, D.P.; Bowtell, J.L. Experimental evidence of the tonic vibration reflex during whole–body vibration of the loaded and unloaded leg. PLoS ONE 2013, 8, e85247. [Google Scholar] [CrossRef] [Green Version]
- Sá-Caputo, D.; Paineiras-Domingos, L.L.; Francisca-Santos, A.; Dos Anjos, E.M.; Reis, A.S.; Neves, M.F.T.; Oigman, W.; Oliveira, R.; Brandão, A.; Machado, C.B.; et al. Whole-body vibration improves the functional parameters of individuals with metabolic syndrome: An exploratory study. BMC Endocr. Disord. 2019, 19, 6. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Zhai, M.; Guo, F.; Shi, T.; Liu, J.; Wang, X.; Zhang, X.; Jing, D.; Hai, C. Whole body vibration improves insulin resistance in db/db mice: Amelioration of lipid accumulation and oxidative stress. Appl. Biochem. Biotechnol. 2015, 179, 819–829. [Google Scholar] [CrossRef]
- Ribeiro, V.G.C.; Mendonça, V.A.; Souza, A.L.C.; Fonseca, S.F.; Camargos, A.C.R.; Lage, V.K.S.; Neves, C.D.C.; Santos, J.M.; Teixeira, L.A.C.; Vieira, E.L.M.; et al. Inflammatory biomarkers responses after acute whole body vibration in fibromyalgia. Braz. J. Med. Biol. Res. 2018, 51, e6775. [Google Scholar] [CrossRef]
- Alex, S.; Boss, A.; Heerschap, A.; Kersten, S. Exercise training improves liver steatosis in mice. Nutr. Metab. 2015, 12, 29. [Google Scholar] [CrossRef] [Green Version]
- Vissers, D.; Verrijken, A.; Mertens, I.; Gils, C.V.; de Sompel, A.V.; Truijen, S.; Gaal, L.V. Effect of long–term whole body vibration training on visceral adipose tissue: A preliminary report. Obes. Facts 2010, 3, 93–100. [Google Scholar] [CrossRef]
- Oh, S.; Shida, T.; Sawai, A.; Maruyama, T.; Eguchi, K.; Isobe, T.; Okamoto, Y.; Someya, N.; Tanaka, K.; Arai, E.; et al. Acceleration training for managing nonalcoholic fatty liver disease: A pilot study. Ther. Clin. Risk Manag. 2014, 10, 925–936. [Google Scholar] [CrossRef] [Green Version]
- Belloa, A.; Sallì, M.; Lombardo, M.; D’Adamo, M.; Guglielmi, V.; Tirabasso, C.; Giordani, L.; Federici, M.; Lauro, D.; Foti, C.; et al. Effects of whole body vibration plus diet on insulin-resistance in middle-aged obese subjects. Int. J. Sports Med. 2014, 35, 511–516. [Google Scholar] [CrossRef]
- Tsui, P.H.; Zhou, Z.; Lin, Y.H.; Humg, C.M.; Chung, S.J.; Wan, Y.L. Effect of ultrasound frequency on the Nakagami statistics of human liver tissues. PLoS ONE 2017, 12, e0181789. [Google Scholar] [CrossRef] [Green Version]
- Shankar, P.M.; Dumane, V.A.; Piccoli, C.W.; Reid, J.M.; Forsberg, F.; Goldberg, B.B. Classification of breast masses in ultrasonic B-mode images using a compounding technique in the Nakagami distribution domain. Ultrasound Med. Biol. 2002, 28, 1295–1300. [Google Scholar] [CrossRef]
- Son, J.Y.; Lee, J.Y.; Yi, N.J.; Lee, K.W.; Suh, K.S.; Kim, K.G.; Lee, J.M.; Han, J.K.; Choi, B.I. Hepatic steatosis: Assessment with acoustic structure quantification of US imaging. Radiology 2016, 278, 257–264. [Google Scholar] [CrossRef] [Green Version]
- Shankar, P.M. A general statistical model for ultrasonic backscattering from tissues. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2000, 47, 727–736. [Google Scholar] [CrossRef]
- Wang, L.; Yu, S.; Chan, A.W.H. Pathology of non-alcoholic fatty liver disease. Int. J. Dig. Dis. 2016, 2, 1. [Google Scholar] [CrossRef]
- Masterton, G.; Ngoh, L.Y.C.; Lockman, A.; Hayes, P.C.; Plevris, J. The significance of fat droplet size and the prognostic value of hyaluronic acid in non-alcoholic fatty liver disease (NAFLD): A biopsy based analysis. Gut 2011, 60, A239–A240. [Google Scholar] [CrossRef] [Green Version]
- Trop, I.; Destrempes, F.; El Khoury, M.; Robidoux, A.; Gaboury, L.; Allard, L.; Chayer, B.; Cloutier, G. The added value of statistical modeling of backscatter properties in the management of breast lesions at US. Radiology 2015, 275, 666–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wuestefel, A.; Fuermaier, A.B.M.; Bernardo-Filho, M.; de Sá-Caputo, D.; Rittweger, J.; Schoenau, E.; Stark, C.; Marin, P.J.; Seixas, A.; Judex, S.; et al. Towards reporting guidelines of research using whole-body vibration as training or treatment regimen in human subjects–A Delphi consensus study. PLoS ONE 2020, 15, e0235905. [Google Scholar] [CrossRef]
- Zhou, Z.; Zhang, Q.; Wu, W.; Lin, Y.H.; Tai, D.I.; Tseng, J.H.; Lin, Y.R.; Wu, S.; Tsui, P.H. Hepatic steatosis assessment using ultrasound homodyned-K parametric imaging: The effects of estimators. Quant. Imaging Med. Surg. 2019, 9, 1932–1947. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.; Gao, A.; Wu, W.; Tai, S.; Tseng, J.H.; Wu, S.; Tsui, P.H. Parameter estimation of the homodyned K distribution based on an artificial neural network for ultrasound tissue characterization. Ultrasonics 2021, 111, 106308. [Google Scholar] [CrossRef]
- Destrempes, F.; Cloutier, G. Interpretation based on stochastic geometry of homodyned-K distribution scatterer clustering parameter for quantitative ultrasound imaging. In Proceedings of the IEEE International Ultrasonics Symposium (IUS), Las Vegas, NV, USA, 7–11 September 2020; pp. 1–4. [Google Scholar] [CrossRef]
- Destrempes, F.; Cloutier, G. Statistical modeling of ultrasound signals related to the packing factor of wave scattering phenomena for structural characterization. J. Acoust. Soc. Am. 2021, 150, 3544–3556. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Control Group | SED for 4 Weeks | SED for 8 Weeks | SED for 16 Weeks | p Value |
|---|---|---|---|---|---|
| μ parameter | 0.64, 0.75, 0.67 0.64, 0.65, 0.70 | 0.74, 0.56, 0.76 0.46, 0.85, 0.64 | 0.69, 1.11, 0.74 1.22, 2.74, 1.30 | 2.08, 4.15, 3.94 3.70, 1.42, 3.44 | 7.26 × 10−6 |
| Weight (g) | 17.43, 18.55, 18.22 17.44, 17.77, 18.54 | 27.06, 26.63, 26.76 25.96, 28.91, 25.98 | 37.21, 38.69, 39.52 41.18, 46.17, 40.21 | 42.76, 43.17, 42.3 43.25, 37.78, 43.58 | 4.76 × 10−15 |
| Peak of glucose concentration (mg/dL) | 231, 249, 237 232, 236, 244 | 413, 402, 429 394, 434, 413 | 361, 509, 481 493, 525, 514 | 447, 493, 463 482, 364, 497 | 4.35 × 10−9 |
| Steatosis (score, 0–3) | 0,0, 0, 1, 0, 0 | 1, 1, 0, 0, 0, 0 | 0, 0, 0, 2, 1, 0 | 2, 3, 3, 2, 2, 3 | 3.14 × 10−6 |
| Lobular inflammation (score, 0–3) | 1, 1, 0, 0, 0, 0 | 0, 0, 0, 0, 0, 0 | 0, 0, 0, 0, 0, 0 | 0, 0, 1, 0, 0, 1 | 0.26 |
| Hepatocyte ballooning (score, 0–2) | 1, 1, 0, 0, 0, 0 | 1, 1, 0, 0, 0, 0 | 0, 1, 0, 1, 1, 0 | 2, 2, 2, 2, 2, 2 | 4.75 × 10−6 |
| Steatohepatitis (score, 0–8) | 2, 2, 0, 1, 0, 0 | 2, 2, 0, 0, 0, 0 | 0, 1, 0, 3, 1, 0 | 4, 5, 6, 4, 4, 6 | 1.22 × 10−6 |
| Fibrosis (stage, 0–4) | 0, 0, 0, 0, 0, 0 | 0, 0, 0, 0, 0, 0 | 0, 0, 0, 0, 0, 0 | 0, 0, 0, 0, 0, 0 | 1 |
| Parameter | Control Group | Exercise for 4 Weeks | Exercise for 8 Weeks | Exercise for 16 Weeks | p Value |
|---|---|---|---|---|---|
| μ parameter | 0.64, 0.75, 0.67 0.64, 0.65, 0.70 | 0.82, 0.52, 0.85 0.57, 0.77, 0.85 | 2.32, 0.72, 0.59 1.62, 0.86, 1.26 | 2.10, 3.18, 2.45 3.28, 2.15, 1.31 | 1.78 × 10−5 |
| Weight (g) | 17.43, 18.55, 18.22 17.44, 17.77, 18.54 | 24.23, 23.46, 25.67 23.89, 24.06, 24.63 | 37.96, 36.11, 35.14 37.08, 36.14, 37.07 | 38.51, 39.87, 39.82 40.96, 39.23, 37.01 | 3.48 × 10−20 |
| Peak of glucose concentration (mg/dL) | 231, 249, 237 232, 236, 244 | 409, 396, 422 401, 413, 436 | 462, 335, 348, 457, 354, 355 | 382, 447, 399, 429, 388, 281 | 1.66 × 10−6 |
| Steatosis (score, 0–3) | 0,0, 0, 1, 0, 0 | 1, 0, 1, 0, 0, 0 | 2, 1, 0, 1, 0, 1 | 1, 2, 2, 3, 2, 1 | 0.0007 |
| Lobular inflammation (score, 0–3) | 1, 1, 0, 0, 0, 0 | 0, 1, 1, 0, 0, 0 | 0, 0, 0, 0, 0, 0 | 1, 0, 0, 0, 0, 0 | 0.42 |
| Hepatocyte ballooning (score, 0–2) | 1, 1, 0, 0, 0, 0 | 1, 1, 0, 0, 0, 0 | 2, 0, 2, 0, 0, 0 | 2, 2, 2, 2, 2, 1 | 0.0023 |
| Steatohepatitis (score, 0–8) | 2, 2, 0, 1, 0, 0 | 2, 2, 2, 0, 0, 0 | 4, 1, 2, 1, 0, 1 | 4, 4, 4, 5, 4, 2 | 0.0005 |
| Fibrosis (stage, 0–4) | 0, 0, 0, 0, 0, 0 | 0, 0, 0, 0, 0, 0 | 0, 0, 0, 0, 0, 0 | 0, 0, 0, 0, 0, 0 | 1 |
| Parameter | Control Group | WBV for 4 Weeks | WBV for 8 Weeks | WBV for 16 Weeks | p Value |
|---|---|---|---|---|---|
| μ parameter | 0.64, 0.75, 0.67 0.64, 0.65, 0.70 | 0.74, 0.61, 0.72 0.69, 0.54, 0.81 | 1.13, 2.37, 1.18 1.09, 0.56, 0.74 | 0.75, 0.72, 1.05 2.82, 0.65, 0.59 | 0.25 |
| Weight (g) | 17.43, 18.55, 18.22 17.44, 17.77, 18.54 | 26.01, 25.49, 24.45 24.63, 23.16, 26.13 | 31.29, 38.12, 36.21 30.37, 28.59, 31.22 | 40.38, 40.76, 41.19 41.32, 36.96, 38.62 | 6.69 × 10−13 |
| Peak of glucose concentration (mg/dL) | 231, 249, 237 232, 236, 244 | 401, 392, 397 389, 383, 413 | 486, 495, 471, 398, 327, 382 | 420, 431, 444, 463, 349, 352 | 4.38 × 10−7 |
| Steatosis (score, 0–3) | 0,0, 0, 1, 0, 0 | 0, 1, 0, 0, 0, 0 | 1, 2, 0, 0, 0,0 | 1, 1, 1, 2, 1, 0 | 0.0808 |
| Lobular inflammation (score, 0–3) | 1, 1, 0, 0, 0, 0 | 0, 0, 0, 0, 0, 0 | 0, 0, 0, 0, 0, 0 | 1, 1, 1, 1, 0, 2 | 0.0011 |
| Hepatocyte ballooning (score, 0–2) | 1, 1, 0, 0, 0, 0 | 0, 0, 1, 0, 0, 0 | 2, 1, 1, 1, 0, 0 | 1, 2, 2, 2, 2, 1 | 0.0007 |
| Steatohepatitis (score, 0–8) | 2, 2, 0, 1, 0, 0 | 0, 1, 0, 1, 0, 0 | 3, 3, 1, 1, 0, 0 | 3, 4, 4, 5, 3, 3 | 4.07 × 10−5 |
| Fibrosis (stage, 0–4) | 0, 0, 0, 0, 0, 0 | 0, 0, 0, 0, 0, 0 | 0, 0, 0, 0, 0, 0 | 0, 0, 0, 0, 0, 0 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fang, J.; Lai, M.-W.; Cheng, H.-T.; Cristea, A.; Zhou, Z.; Tsui, P.-H. Imaging the Effects of Whole-Body Vibration on the Progression of Hepatic Steatosis by Quantitative Ultrasound Based on Backscatter Envelope Statistics. Pharmaceutics 2022, 14, 741. https://doi.org/10.3390/pharmaceutics14040741
Fang J, Lai M-W, Cheng H-T, Cristea A, Zhou Z, Tsui P-H. Imaging the Effects of Whole-Body Vibration on the Progression of Hepatic Steatosis by Quantitative Ultrasound Based on Backscatter Envelope Statistics. Pharmaceutics. 2022; 14(4):741. https://doi.org/10.3390/pharmaceutics14040741
Chicago/Turabian StyleFang, Jui, Ming-Wei Lai, Hao-Tsai Cheng, Anca Cristea, Zhuhuang Zhou, and Po-Hsiang Tsui. 2022. "Imaging the Effects of Whole-Body Vibration on the Progression of Hepatic Steatosis by Quantitative Ultrasound Based on Backscatter Envelope Statistics" Pharmaceutics 14, no. 4: 741. https://doi.org/10.3390/pharmaceutics14040741