
Mucoadhesive Buccal Film of Estradiol for Hormonal Replacement Therapy: Development and In-Vivo Performance Prediction

 , ,
, , 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Methods
2.2.1. Solubility Enhancement
2.2.2. Preparation of Simulated Salivary Fluid (SSF)
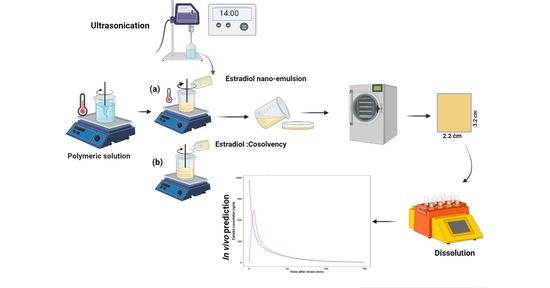
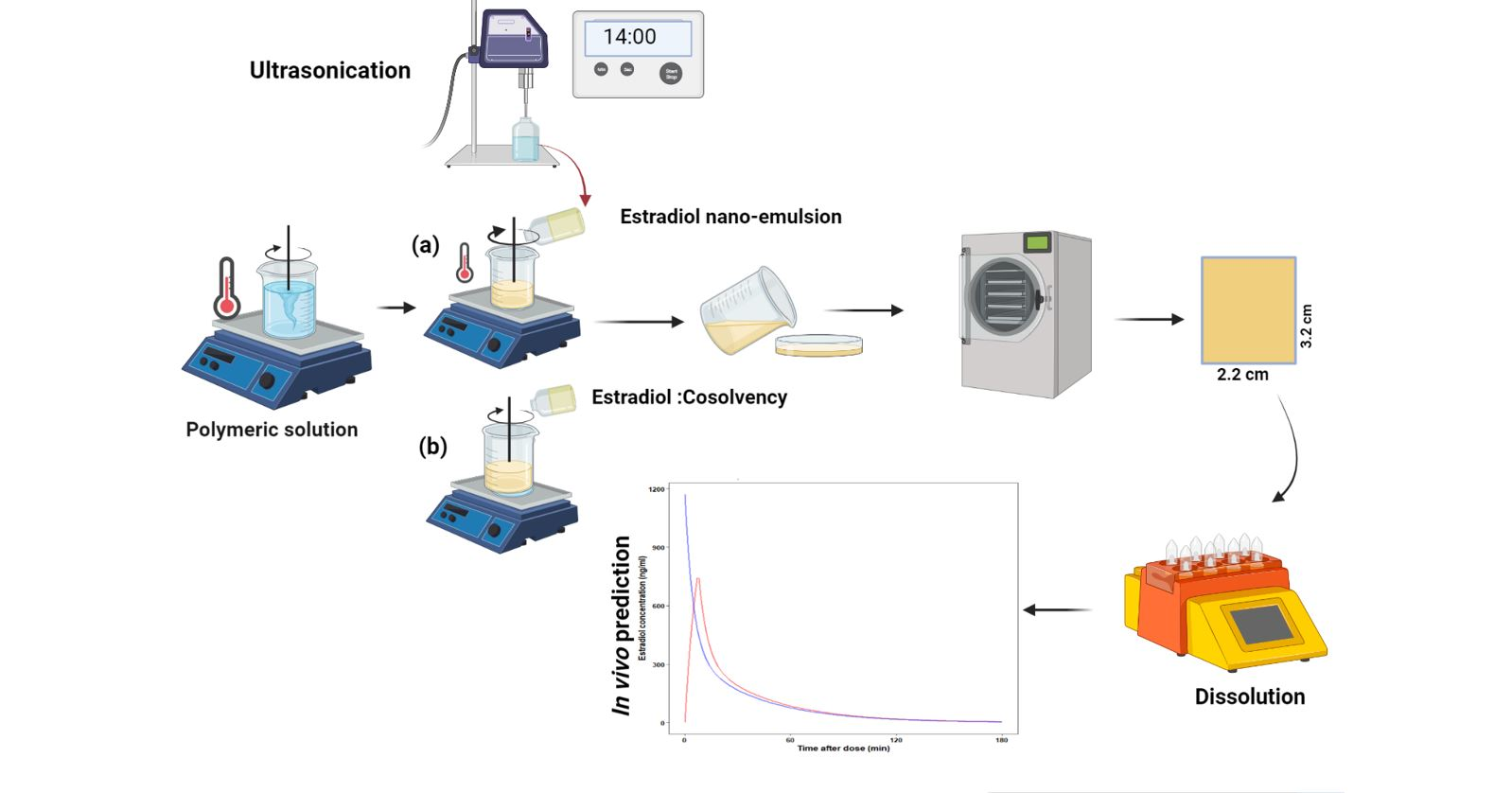
2.2.3. Formulation (Gel and Film) Development
2.2.4. Characterization of Estradiol Loaded Mucoadhesive Buccal Films
2.2.5. Tensile Strength (TS)
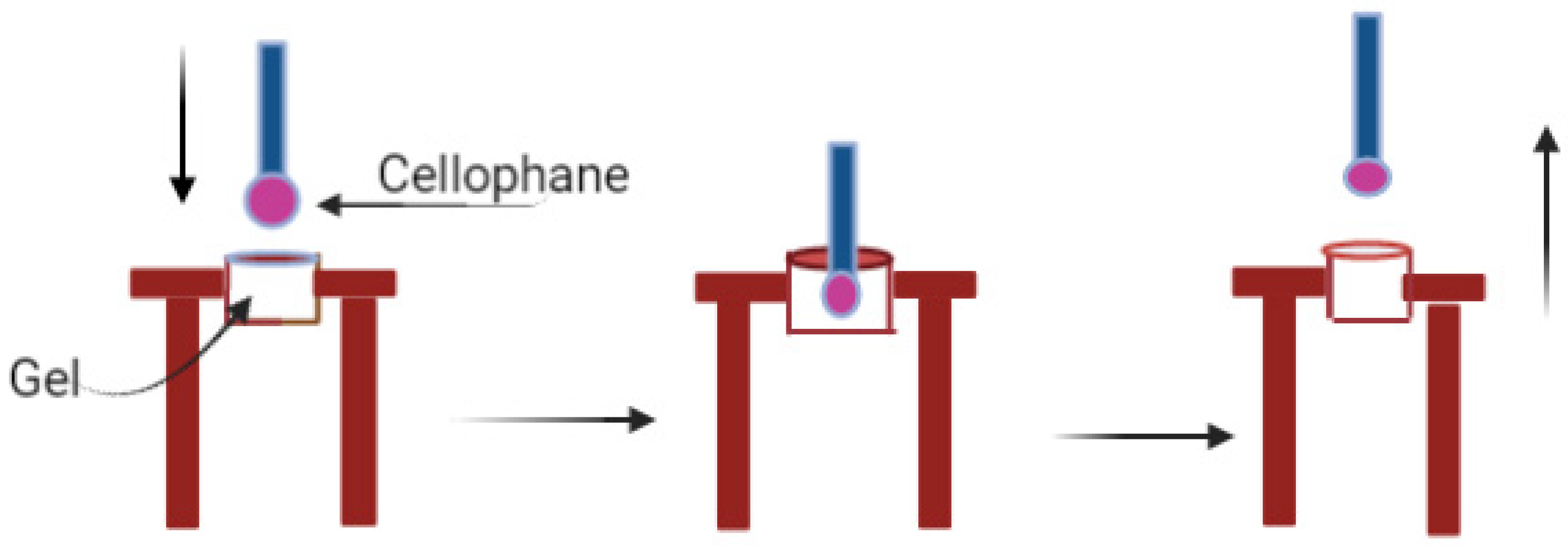
2.2.6. Muco-Adhesion
2.2.7. Thickness and Weight Uniformity
2.2.8. Content Uniformity
2.2.9. Folding Endurance
2.2.10. Surface pH
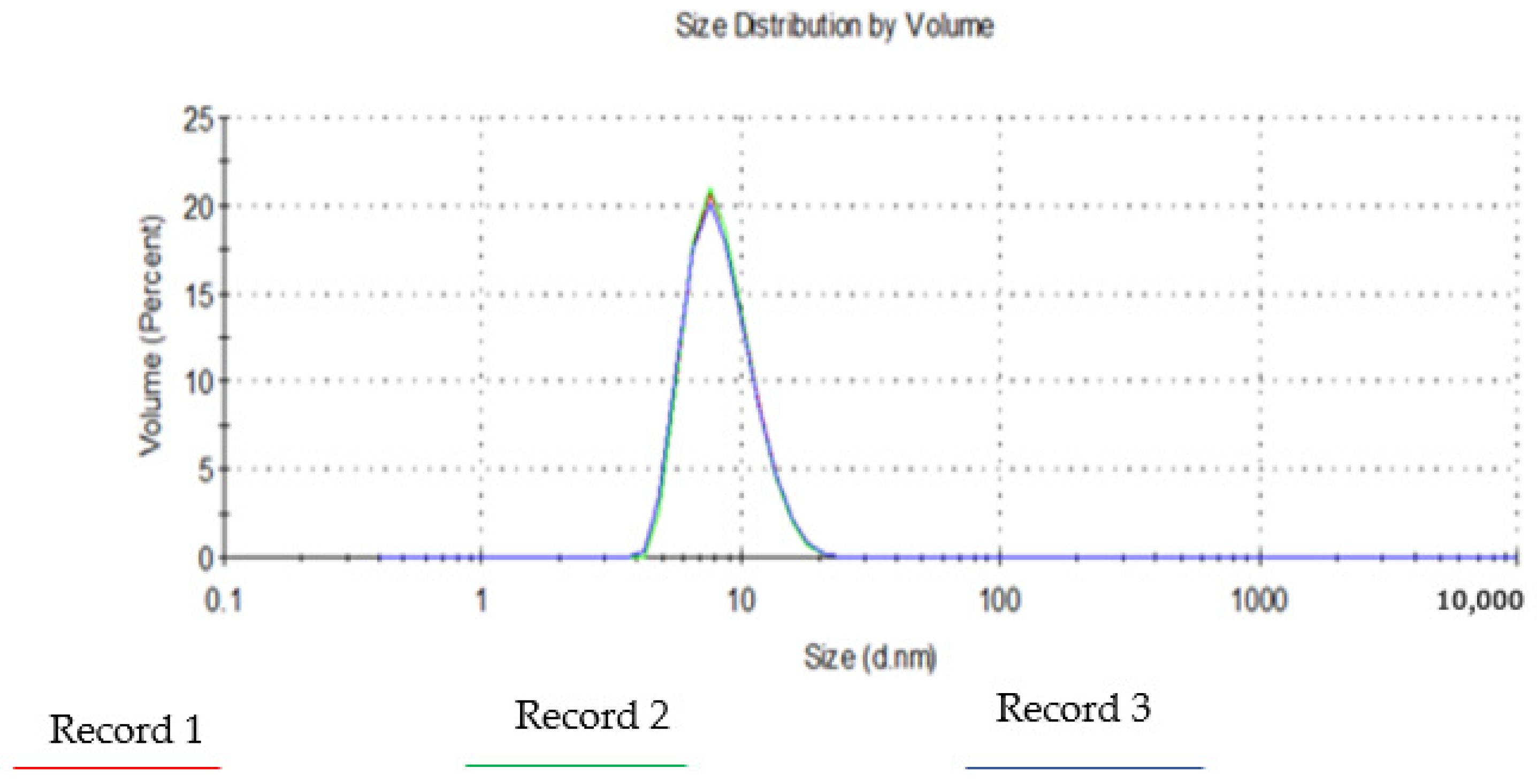
2.2.11. Droplet Size and Polydispersity Index
2.2.12. In Vitro Disintegration
2.2.13. In Vitro Dissolution Test
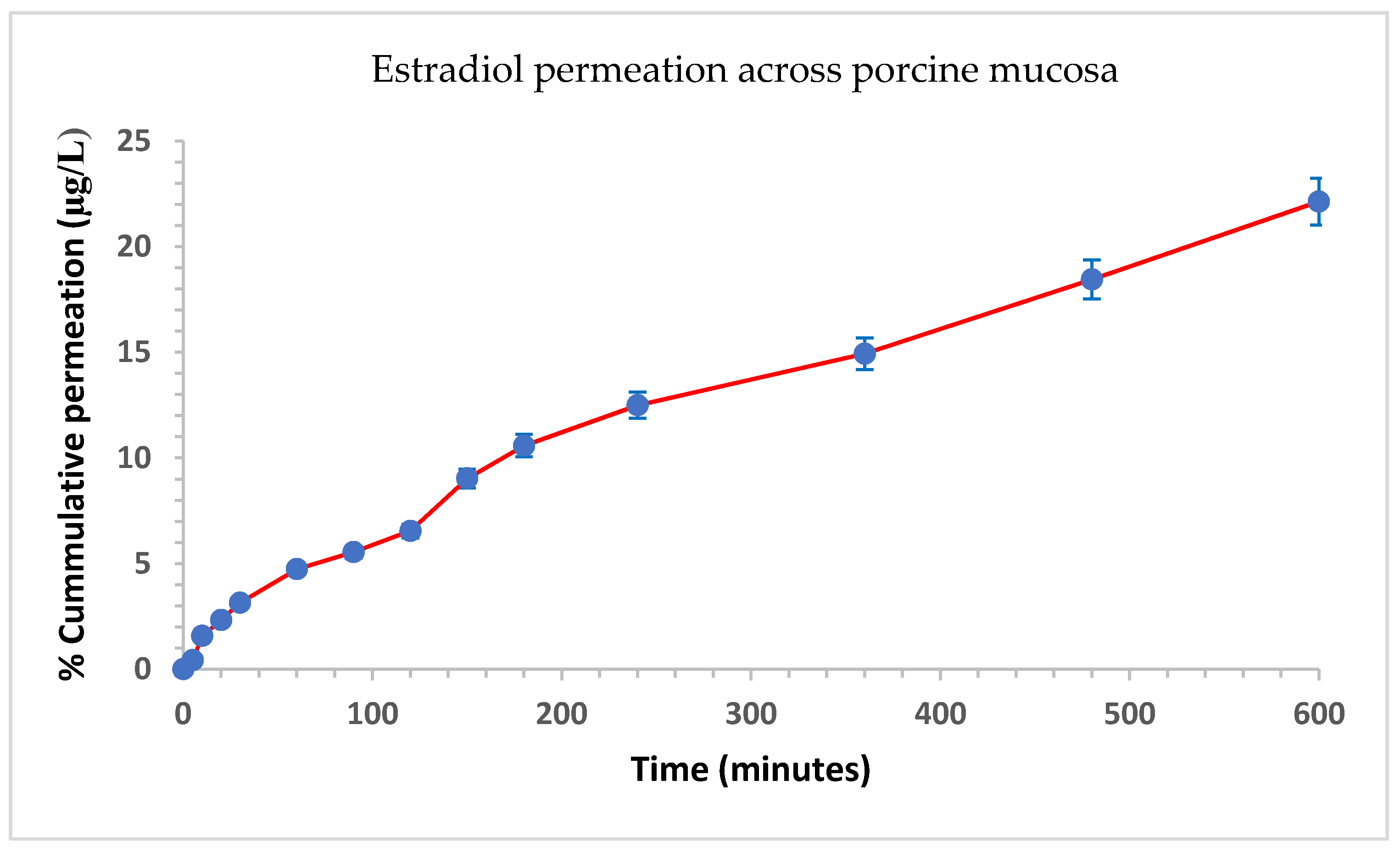
2.2.14. Permeation Studies
2.2.15. Fourier Transform Infrared Spectroscopy (FTIR)
2.2.16. Differential Scanning Calorimetry (DSC)
2.2.17. X-Ray Powder Diffraction (XRD)
2.2.18. Scanning Electron Microscopy (SEM)
2.2.19. Prediction of In Vivo Performance
3. Result and Discussion
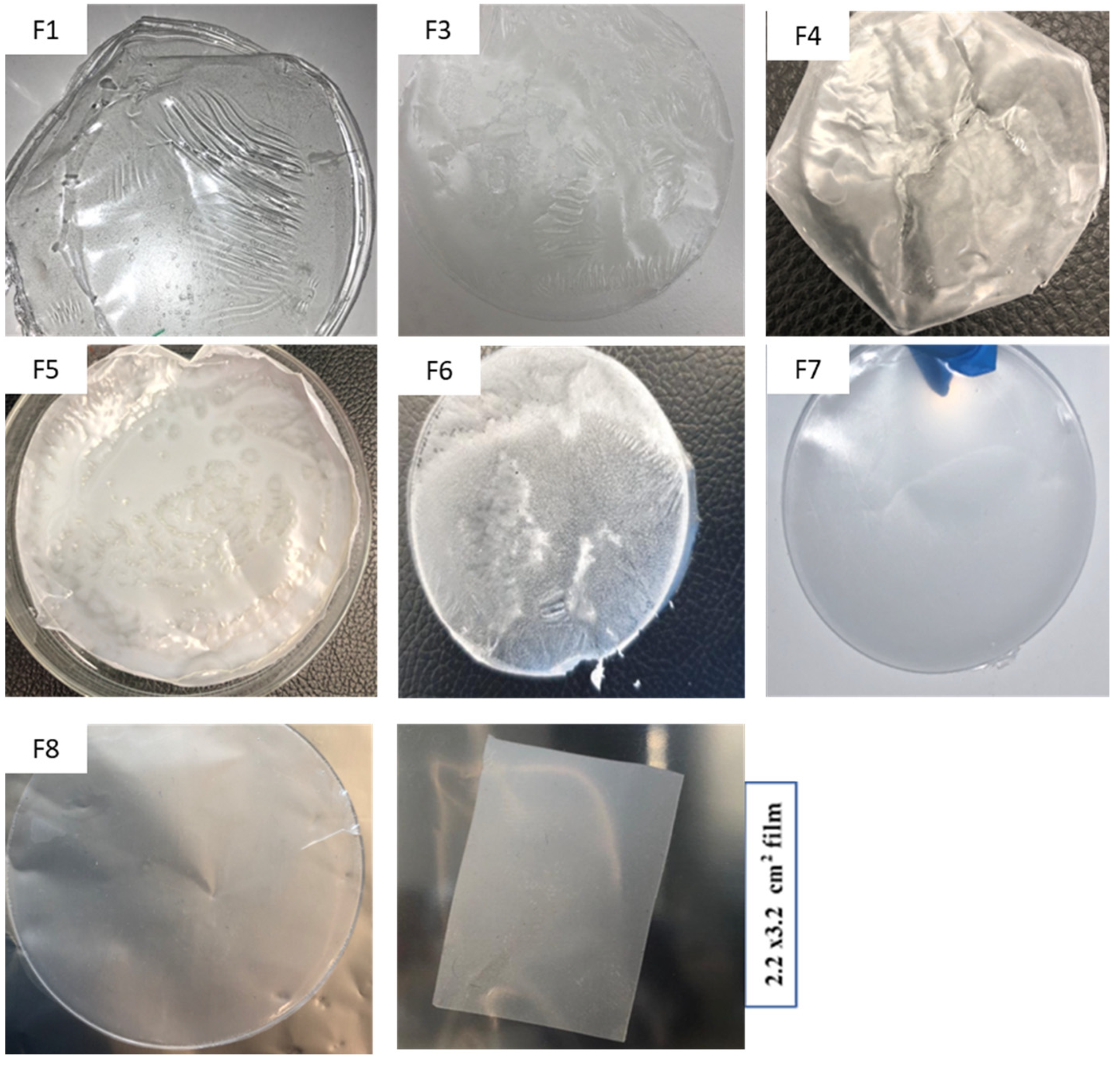
3.1. Physical Appearance of the Films
3.2. Tensile Strength (TS) and % Elongation (PE)
3.3. Thickness and Weight Uniformity
3.4. Surface pH
3.5. Droplet Size and Polydispersity Index (PDI)
3.6. Drug Content Uniformity
3.7. Muco-Adhesion Studies
3.8. In Vitro Disintegration
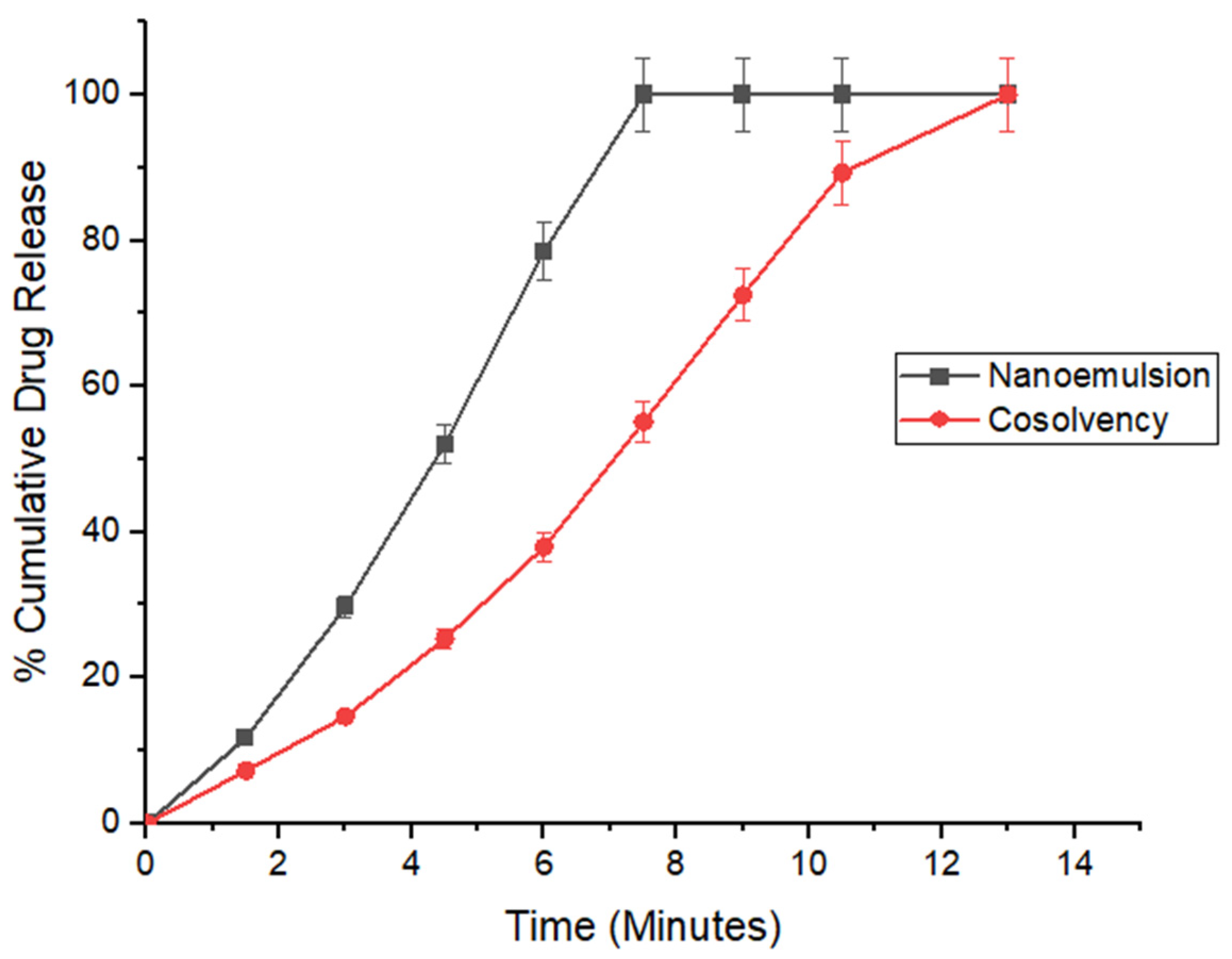
3.9. In Vitro Drug Release
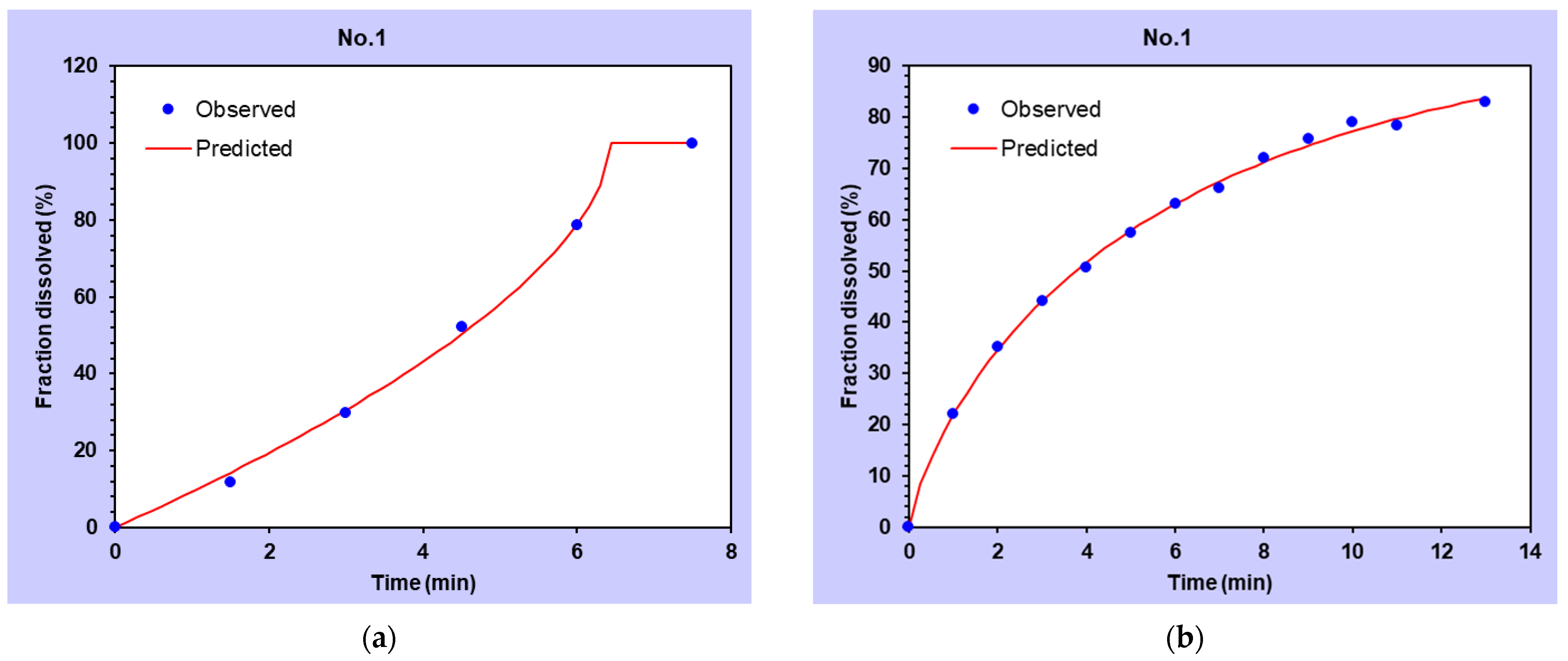
3.10. Mathematical Modeling of Drug Release Profiles
3.11. Permeation Studies
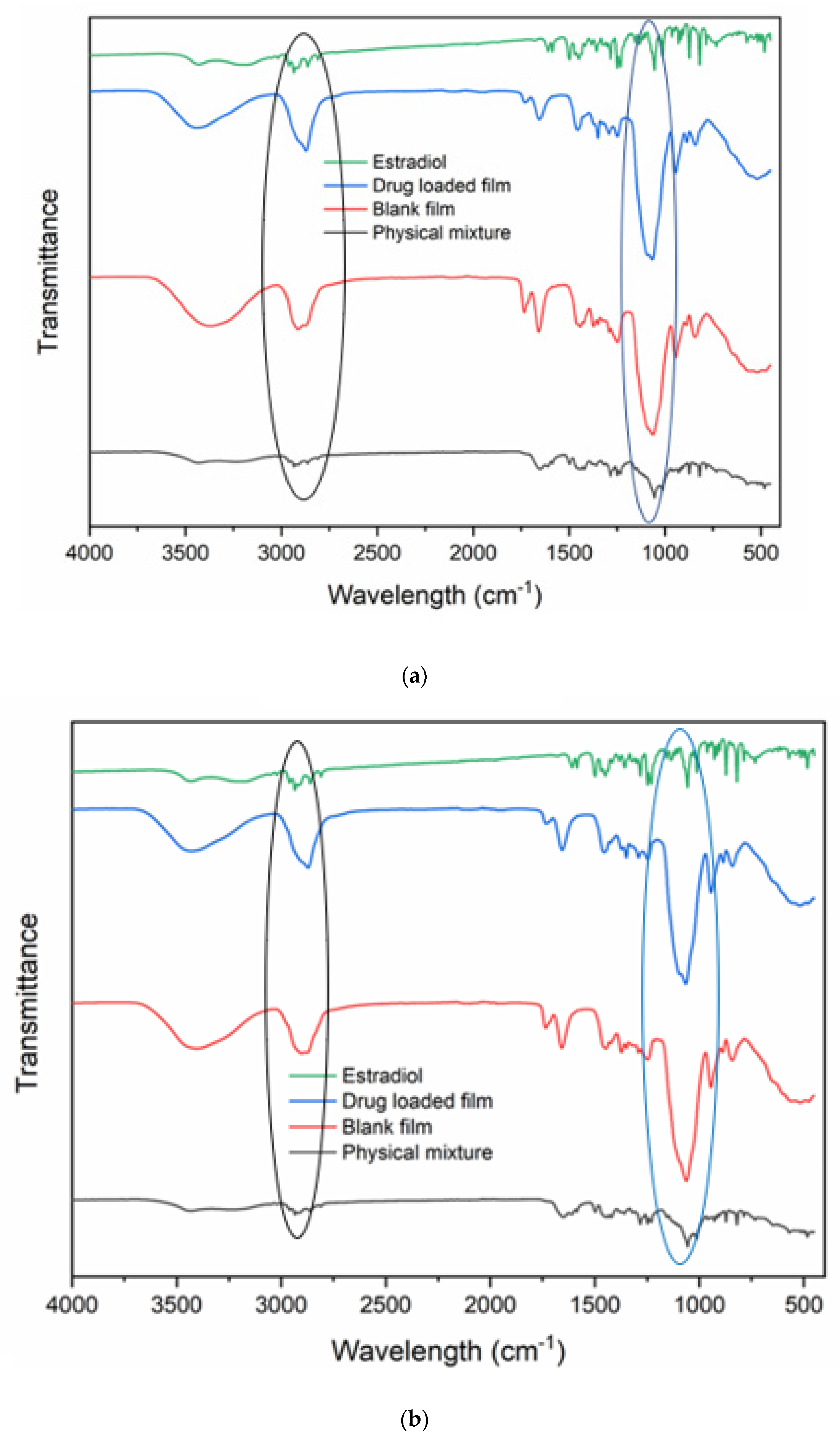
3.12. Fourier Transform Infrared (FTIR) Analysis
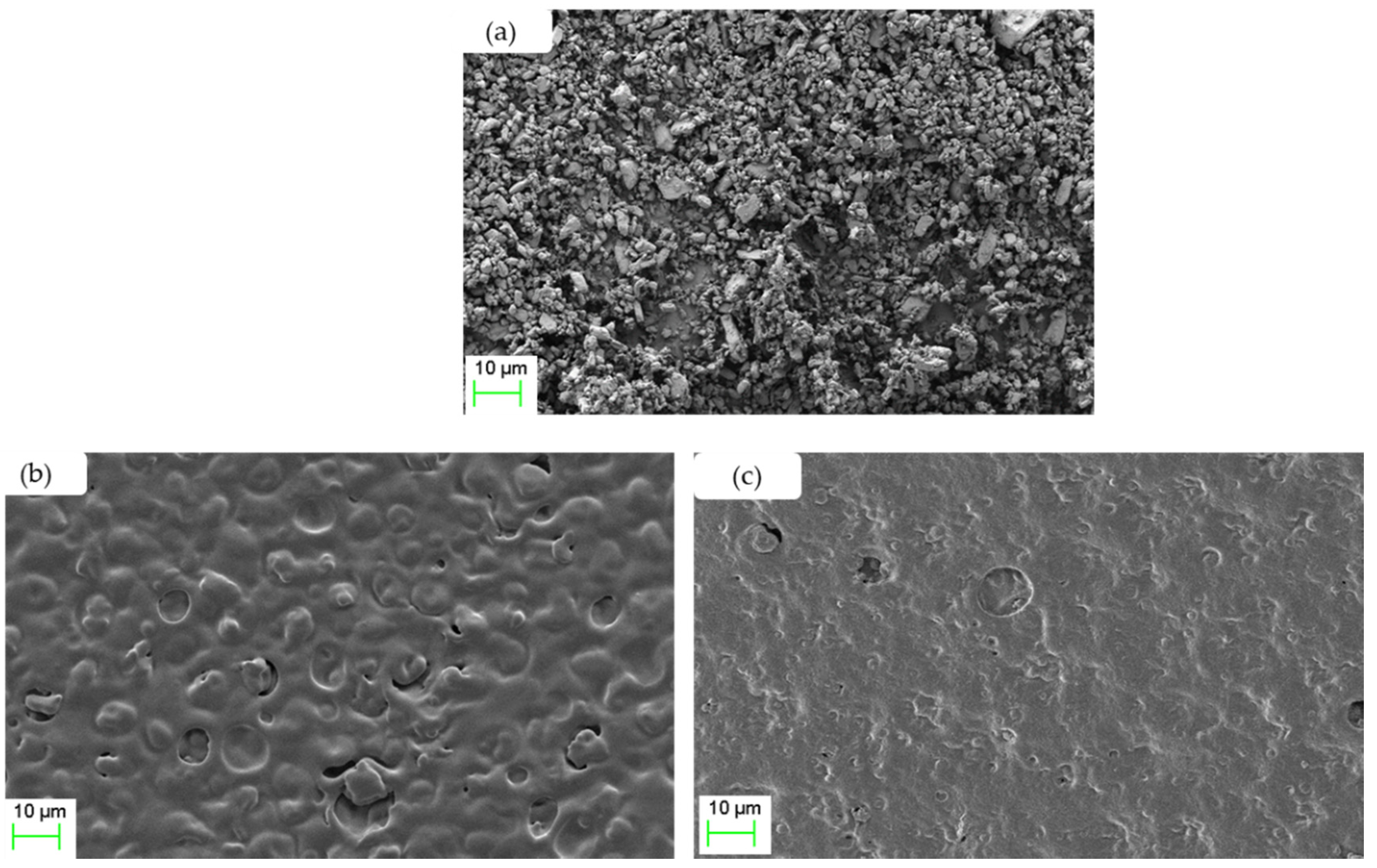
3.13. Scanning Electron Microscopy (SEM)
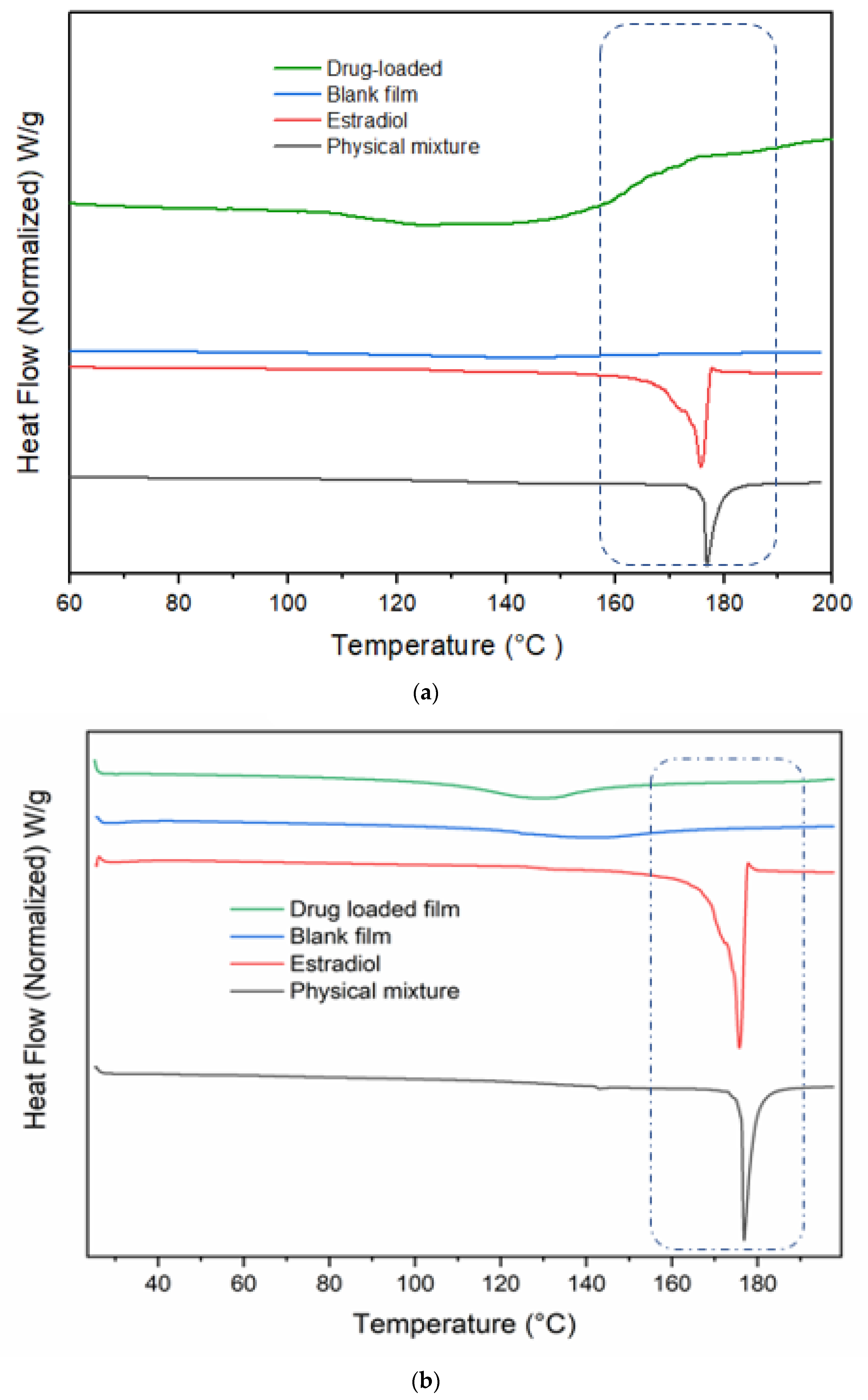
3.14. DSC Studies
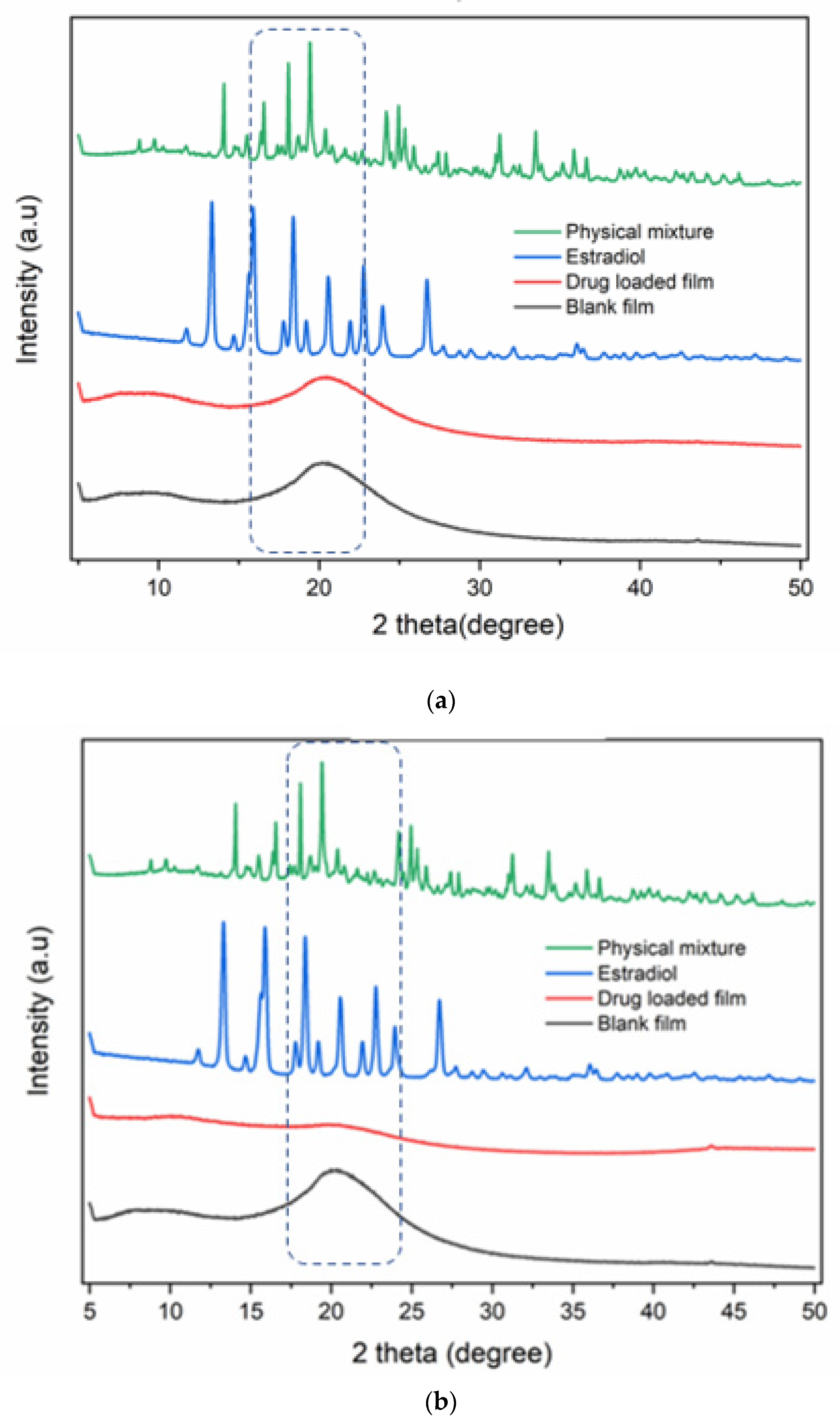
3.15. XRD Studies
3.16. Prediction of In Vivo Performance
4. Conclusions and Future Directions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Appendix A. R Script
References
- Hill, K. The demography of menopause. Maturitas 1996, 23, 113–127. [Google Scholar] [CrossRef]
- NIH State-of-the-Science Panel. NIH State-of-the-Science Conference Statement on management of menopause-related symptoms. NIH Consens. State Sci. Statements 2005, 22, 1–38. [Google Scholar] [CrossRef]
- Pinkerton, J.V. Hormone Therapy for Postmenopausal Women. N. Engl. J. Med. 2020, 382, 446–455. [Google Scholar] [CrossRef]
- Fleat-Surgeou Corry, R.N.X.; Rooney, R. The Royal College of Physicians of Edinburgh. Available online: https://europepmc.org/backend/ptpmcrender.fcgi?accid=PMC2434947&blobtype=pdf (accessed on 20 January 2022).
- North American Menopause Society. The 2012 hormone therapy position statement of the North American Menopause Society. Menopause 2012, 19, 257. [Google Scholar] [CrossRef] [Green Version]
- Roberts, H.; Hickey, M. Managing the menopause: An update. Maturitas 2016, 86, 53–58. [Google Scholar] [CrossRef]
- American College of Obstetricians and Gynecologists. ACOG Practice Bulletin No. 141: Management of menopausal symptoms. Obstet. Gynecol. 2014, 123, 202–216. [Google Scholar] [CrossRef]
- Kaunitz, A.M.; Manson, J.E. Management of menopausal symptoms. Obstet. Gynecol. 2015, 126, 859. [Google Scholar] [CrossRef] [Green Version]
- Nelson, H.D. Commonly used types of postmenopausal estrogen for treatment of hot flashes: Scientific review. JAMA 2004, 291, 1610–1620. [Google Scholar] [CrossRef]
- MacLennan, A.H.; Broadbent, J.L.; Lester, S.; Moore, V. Oral oestrogen and combined oestrogen/progestogen therapy versus placebo for hot flushes. Cochrane Database Syst. Rev. 2004, 2004, CD002978. [Google Scholar] [CrossRef]
- Kuhl, H. Pharmacology of estrogens and progestogens: Influence of different routes of administration. Climacteric 2005, 8 (Suppl. 1), 3–63. [Google Scholar] [CrossRef]
- Bala, R.; Khanna, S.; Pawar, P.; Arora, S. Orally dissolving strips: A new approach to oral drug delivery system. Int. J. Pharm. Investig. 2013, 3, 67–76. [Google Scholar] [CrossRef] [Green Version]
- Fonseca-Santos, B.; Chorilli, M. An overview of polymeric dosage forms in buccal drug delivery: State of art, design of formulations and their in vivo performance evaluation. Mater. Sci. Eng. C 2018, 86, 129–143. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, E.M.; Breitenbach, A.; Breitkreutz, J. Advances in orodispersible films for drug delivery. Expert Opin. Drug Deliv. 2011, 8, 299–316. [Google Scholar] [CrossRef]
- Pather, S.I.; Rathbone, M.J.; Şenel, S. Current status and the future of buccal drug delivery systems. Expert Opin. Drug Deliv. 2008, 5, 531–542. [Google Scholar] [CrossRef]
- Kuhnz, W.; Gansau, C.; Mahler, M. Pharmacokinetics of estradiol, free and total estrone, in young women following single intravenous and oral administration of 17 beta-estradiol. Arzneimittelforschung 1993, 43, 966–973. [Google Scholar]
- Wren, B.G.; Day, R.O.; McLachlan, A.J.; Williams, K.M. Pharmacokinetics of estradiol, progesterone, testosterone and dehydroepiandrosterone after transbuccal administration to postmenopausal women. Climacteric 2003, 6, 104–111. [Google Scholar] [CrossRef]
- Zhang, H.; Zhang, J.; Streisand, J.B. Oral mucosal drug delivery: Clinical pharmacokinetics and therapeutic applications. Clin. Pharmacokinet. 2002, 41, 661–680. [Google Scholar] [CrossRef]
- Han, S.K.; Kim, G.Y.; Park, Y.H. Solubilization of biphenyl dimethyl dicarboxylate by cosolvency. Drug Dev. Ind. Pharm. 1999, 25, 1193–1197. [Google Scholar] [CrossRef]
- Sareen, S.; Mathew, G.; Joseph, L. Improvement in solubility of poor water-soluble drugs by solid dispersion. Int. J. Pharm. Investig. 2012, 2, 12–17. [Google Scholar] [CrossRef] [Green Version]
- Loftsson, T.; Brewster, M.E. Pharmaceutical Applications of Cyclodextrins. 1. Drug Solubilization and Stabilization. J. Pharm. Sci. 1996, 85, 1017–1025. [Google Scholar] [CrossRef]
- Pattni, B.S.; Chupin, V.V.; Torchilin, V.P. New Developments in Liposomal Drug Delivery. Chem. Rev. 2015, 115, 10938–10966. [Google Scholar] [CrossRef]
- Li, Y.; Zheng, J.; Xiao, H.; McClements, D.J. Nanoemulsion-based delivery systems for poorly water-soluble bioactive compounds: Influence of formulation parameters on Polymethoxyflavone crystallization. Food Hydrocoll. 2012, 27, 517–528. [Google Scholar] [CrossRef] [Green Version]
- Singh, A.; Worku, Z.A.; Van den Mooter, G. Oral formulation strategies to improve solubility of poorly water-soluble drugs. Expert. Opin. Drug. Deliv. 2011, 8, 1361–1378. [Google Scholar] [CrossRef]
- Taneja, S.; Shilpi, S.; Khatri, K. Formulation and optimization of efavirenz nanosuspensions using the precipitation-ultrasonication technique for solubility enhancement. Artif. Cells Nanomed. Biotechnol. 2015, 44, 978–984. [Google Scholar] [CrossRef]
- Koland, M.; Charyulu, R.N.; Vijayanarayana, K. Prabhu In vitro and in vivo evaluation of chitosan buccal films of ondansetron hydrochloride. Int. J. Pharm. Investig. 2011, 1, 164–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, K.G.; Park, T.J.; Soo, S.Y.; Wang, K.W.; Kim, B., II; Park, J.H.; Lee, C.S.; Kim, D.H.; Lee, S.J. Synthesis and utilization of E. coli-encapsulated PEG-based microdroplet using a microfluidic chip for biological application. Biotechnol. Bioeng. 2010, 107, 747–751. [Google Scholar] [CrossRef] [PubMed]
- Sung, K.C.; Nixon, P.R.; Skoug, J.W.; Ju, T.R.; Gao, P.; Topp, E.M.; Patel, M.V. Effect of formulation variables on drug and polymer release from HPMC-based matrix tablets. Int. J. Pharm. 1996, 142, 53–60. [Google Scholar] [CrossRef]
- Kurakula, M.; Rao, G.S.N.K. Pharmaceutical assessment of polyvinylpyrrolidone (PVP): As excipient from conventional to controlled delivery systems with a spotlight on COVID-19 inhibition. J. Drug Deliv. Sci. Technol. 2020, 60, 102046. [Google Scholar] [CrossRef] [PubMed]
- Javadzadeh, Y.; Adibkia, K.; Hamishehkar, H. Transcutol® (Diethylene Glycol Monoethyl Ether): A Potential Penetration Enhancer; Springer: Berlin/Heidelberg, Germany, 2015; pp. 195–205. [Google Scholar]
- Cilurzo, F.; Cupone, I.E.; Minghetti, P.; Selmin, F.; Montanari, L. Fast dissolving films made of maltodextrins. Eur. J. Pharm. Biopharm. 2008, 70, 895–900. [Google Scholar] [CrossRef]
- Kumar, A.; Ahuja, M. Carboxymethyl gum kondagogu: Synthesis, characterization and evaluation as mucoadhesive polymer. Carbohydr. Polym. 2012, 90, 637–643. [Google Scholar] [CrossRef]
- White, C.M.; Ferraro-Borgida, M.J.; Fossati, A.T.; McGill, C.C.; Ahlberg, A.W.; Feng, Y.J.; Heller, G.V.; Chow, M.S. The pharmacokinetics of intravenous estradiol—a preliminary study. Pharmacother. J. Hum. Pharmacol. Drug Ther. 1998, 18, 1343–1346. [Google Scholar]
- Jovanović, M.; Petrović, M.; Cvijić, S.; Tomić, N.; Stojanović, D.; Ibrić, S.; Uskoković, P. 3D Printed Buccal Films for Prolonged-Release of Propranolol Hydrochloride: Development, Characterization and Bioavailability Prediction. Pharmaceutics 2021, 13, 2143. [Google Scholar] [CrossRef]
- Wong, C.; Yuen, K.; Peh, K. Formulation and evaluation of controlled release Eudragit buccal patches. Int. J. Pharm. 1999, 178, 11–22. [Google Scholar] [CrossRef]
- Shinkar, D.M.; Dhake, A.S.; Setty, C.M. Drug Delivery from the Oral Cavity: A Focus on Mucoadhesive Buccal Drug Delivery Systems. PDA J. Pharm. Sci. Technol. 2012, 66, 466–500. [Google Scholar] [CrossRef]
- Constantinides, P.P.; Scalart, J. Formulation and physical characterization of water-in-oil microemulsions containing long-versus medium-chain glycerides. Int. J. Pharm. 1997, 158, 57–68. [Google Scholar] [CrossRef]
- Cook, S.L.; Bull, S.P.; Methven, L.; Parker, J.K.; Khutoryanskiy, V.V. Mucoadhesion: A food perspective. Food Hydrocoll. 2017, 72, 281–296. [Google Scholar] [CrossRef]
- Kumar, G.P.; Phani, A.; Prasad, R.; Sanganal, J.S.; Manali, N.; Gupta, R.; Rashmi, N.; Prabhakara, G.; Salins, C.P.; Sandeep, K.; et al. Polyvinylpyrrolidone oral films of enrofloxacin: Film characterization and drug release. Int. J. Pharm. 2014, 471, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Sharma, D.; Garg, R.; Sharma, A. Design, Development and in vitro/Ex vivo Evaluation of Mucoadhesive Buccal Film of Benzydamine Hydrochloride for the Effective Treatment of Aphthous Stomatitis. Recent Patents Drug Deliv. Formul. 2018, 12, 277–294. [Google Scholar] [CrossRef]
- Pinto, S.; Pintado, M.E.; Sarmento, B. In vivo, ex vivo and in vitro assessment of buccal permeation of drugs from delivery systems. Expert Opin. Drug Deliv. 2020, 17, 33–48. [Google Scholar] [CrossRef] [PubMed]
- Kraisit, P.; Limmatvapirat, S.; Luangtana-Anan, M. Sriamornsak Buccal administration of mucoadhesive blend films saturated with propranolol loaded nanoparticles. Asian J. Pharm. Sci. 2018, 13, 34–43. [Google Scholar] [CrossRef]
- Minaeva, V.; Minaev, B.F.; Hovorun, D. Vibrational spectra of the steroid hormones, estradiol and estriol, calculated by density functional theory. The role of low-frequency vibrations. Ukr. Biokhim. Zh. 2008, 80, 82–95. [Google Scholar]
- Ranjbar, M.; Pardakhty, A.; Amanatfard, A.; Asadipour, A. Efficient drug delivery of β-estradiol encapsulated in Zn-metal–organic framework nanostructures by microwave-assisted coprecipitation method. Drug Des. Dev. Ther. 2018, ume 12, 2635–2643. [Google Scholar] [CrossRef] [Green Version]
- De Paula, D.; Oliveira, D.C.R.; Tedesco, A.C.; Bentley, M.V.L.B. Enhancing effect of modified beta-cyclodextrins on in vitro skin permeation of estradiol. Rev. Bras. De Ciências Farm. 2007, 43, 111–120. [Google Scholar] [CrossRef]
- Tappa, K.; Jammalamadaka, U.; Ballard, D.H.; Bruno, T.; Israel, M.R.; Vemula, H.; Meacham, J.; Mills, D.K.; Woodard, P.K.; Weisman, J.A. Medication eluting devices for the field of OBGYN (MEDOBGYN): 3D printed biodegradable hormone eluting constructs, a proof of concept study. PLoS ONE 2017, 12, e0182929. [Google Scholar] [CrossRef] [PubMed]
- Akhtar, M.; Ahmad, M.; Khan, S.A.; Murtaza, G. Novel modified release tableted microspheres of ibuprofen and misoprostol in a combined formulation: Use of software DDSolver. Afr. J. Pharm. Pharmacol. 2012, 6, 2613–2620. [Google Scholar] [CrossRef] [Green Version]
- Macedo, A.; Castro, P.M.; Roque, L.; Thomé, N.G.; Reis, C.; Pintado, M.M.; Fonte, P. Novel and revisited approaches in nanoparticle systems for buccal drug delivery. J. Control. Release 2020, 320, 125–141. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Lee, V.J.; Yoon, M.K.; Choi, Y.W. Ex Vivo Permeability Characteristics of Porcine Buccal Mucosa to Drugs with Various Polarity. J. Kor. Pharm. Sci. 2005, 35, 71–74. [Google Scholar]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ingredients | F1 | F2 | F3 | F4 | F5 | F6 | F7 | F8 |
|---|---|---|---|---|---|---|---|---|
| Estradiol (g) | 0.08 | 0.08 | 0.08 | |||||
| PVA (g) | 0.5 | 0.5 | 0.75 | 0.75 | 1 | 1 | ||
| HPMC (g) | 1 | 1 | 1 | 1.5 | 1.5 | |||
| PVP (g) | 0.4 | 0.4 | ||||||
| Kollicoat(g) | 4 | 4 | ||||||
| Xanthan (g) | 0.015 | 0.015 | ||||||
| Glycerin (mL) | 0.2 | |||||||
| PEG (mL) | 1 | 1.5 | 0.5 | 1.5 | 2.5 | 2.5 | ||
| Tween 80 (mL) | 0.5 | 0.5 | ||||||
| Transcutol (mL) | 1 | |||||||
| Ethanol (mL) | 12 | |||||||
| Citric acid (g) | 0.125 | 0.125 | ||||||
| Sucralose (g) | 0.25 | 0.25 | ||||||
| Water (QS) (mL) | 50 | 50 | 50 | 50 | 50 | 50 | 50 | 50 |
| Co-Solvency | Nano-Emulsion | p-Value | |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| Tensile strength (MPa) | 0.51 ± 0.06 | 0.51 ± 0.01 | 0.811 |
| Percent elongation | 11.05 ± 0.52 | 12.3 ± 2.46 | 0.43 |
| Film Preparation Approach | Weight (mg) | Thickness (mm) | ||
|---|---|---|---|---|
| Mean ± SD | p-Value | Mean ± SD | p-Value | |
| Co-solvency | 0.102 ± 0.004 | <0.001 | 0.14 ± 0.01 | 0.492 |
| Nano-emulsion | 0.133 ± 0.00 | 0.15 ± 0.01 | ||
| Z-Average (d.nm) | 14.92 |
|---|---|
| PdI | 0.487 |
| Result Quality | Good |
| Film Preparation Approach | Mean ± SD | % Drug Recovery | p-Value |
|---|---|---|---|
| Co-solvency | 1.47 ± 0.11 | 98.25% | 0.971 |
| Nano-emulsion | 1.46 ± 0.27 | 97.50% |
| Model Name | Equation | Goodness of Fit Parameter | Cosolvency Film | Nanoemulision Film |
|---|---|---|---|---|
| R2 adjusted | 0.9689 | 0.9768 | ||
| Zero order | F = k0 × t | RMSE | 6.4343 | 5.926 |
| AIC | 54.2245 | 33.0089 | ||
| R2 adjusted | 0.8511 | 0.8596 | ||
| First order | F = 100 × [1 − Exp(−k1 × t)] | RMSE | 14.0805 | 14.5686 |
| AIC | 68.3212 | 43.803 | ||
| R2 adjusted | 0.7687 | 0.7953 | ||
| Higuchi | F = kH × t0.5 | RMSE | 17.5484 | 17.5899 |
| AIC | 72.2843 | 46.0645 | ||
| R2 adjusted | 0.9837 | 0.9982 | ||
| Korsmeyer-Peppasb | F = kkP × tn | RMSE | 4.6546 | 1.6313 |
| AIC | 49.1944 | 18.1902 | ||
| R2 adjusted | 0.8924 | 0.8993 | ||
| Hixson-Crowell | F = 100 × [1 − (1 − kHC × t)3] | RMSE | 11.9675 | 12.3362 |
| AIC | 65.3945 | 41.8071 | ||
| R2 adjusted | 0.9933 | 0.9983 | ||
| Hopfenberg | F = 100 × [1 − (1 − kHB × t)n] | RMSE | 2.9814 | 1.6108 |
| AIC | 41.1765 | 18.0388 | ||
| R2 adjusted | 0.7007 | 0.7312 | ||
| Baker-Lonsdale | 3/2 × [1 − (1 − F/100)2/3] − F/100 = kBL × t | RMSE | 19.9617 | 20.1554 |
| AIC | 74.6036 | 47.6983 | ||
| R2 adjusted | 0.9841 | 0.9983 | ||
| Peppas-Sahlinc | F = k1 × tm + k2 × t2m | RMSE | 4.6033 | 1.604 |
| AIC | 49.6076 | 18.2614 | ||
| R2 adjusted | 0.9972 | 0.9912 | ||
| Weibull | F = 100 × {1 − Exp[− ((t − Ti)β)/α]} | RMSE | 1.9443 | 3.6431 |
| AIC | 34.0936 | 28.1058 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdella, S.; Afinjuomo, F.; Song, Y.; Upton, R.; Garg, S. Mucoadhesive Buccal Film of Estradiol for Hormonal Replacement Therapy: Development and In-Vivo Performance Prediction. Pharmaceutics 2022, 14, 542. https://doi.org/10.3390/pharmaceutics14030542
Abdella S, Afinjuomo F, Song Y, Upton R, Garg S. Mucoadhesive Buccal Film of Estradiol for Hormonal Replacement Therapy: Development and In-Vivo Performance Prediction. Pharmaceutics. 2022; 14(3):542. https://doi.org/10.3390/pharmaceutics14030542
Chicago/Turabian StyleAbdella, Sadikalmahdi, Franklin Afinjuomo, Yunmei Song, Richard Upton, and Sanjay Garg. 2022. "Mucoadhesive Buccal Film of Estradiol for Hormonal Replacement Therapy: Development and In-Vivo Performance Prediction" Pharmaceutics 14, no. 3: 542. https://doi.org/10.3390/pharmaceutics14030542