
A Randomized Placebo-Controlled Phase 2 Study of Gemcitabine and Capecitabine with or without T-ChOS as Adjuvant Therapy in Patients with Resected Pancreatic Cancer (CHIPAC)

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Design and Objectives
2.3. Study Treatment
2.4. Study Assessments and Procedures
2.5. Translational Research
2.6. QoL
2.7. Statistical Methods
3. Results
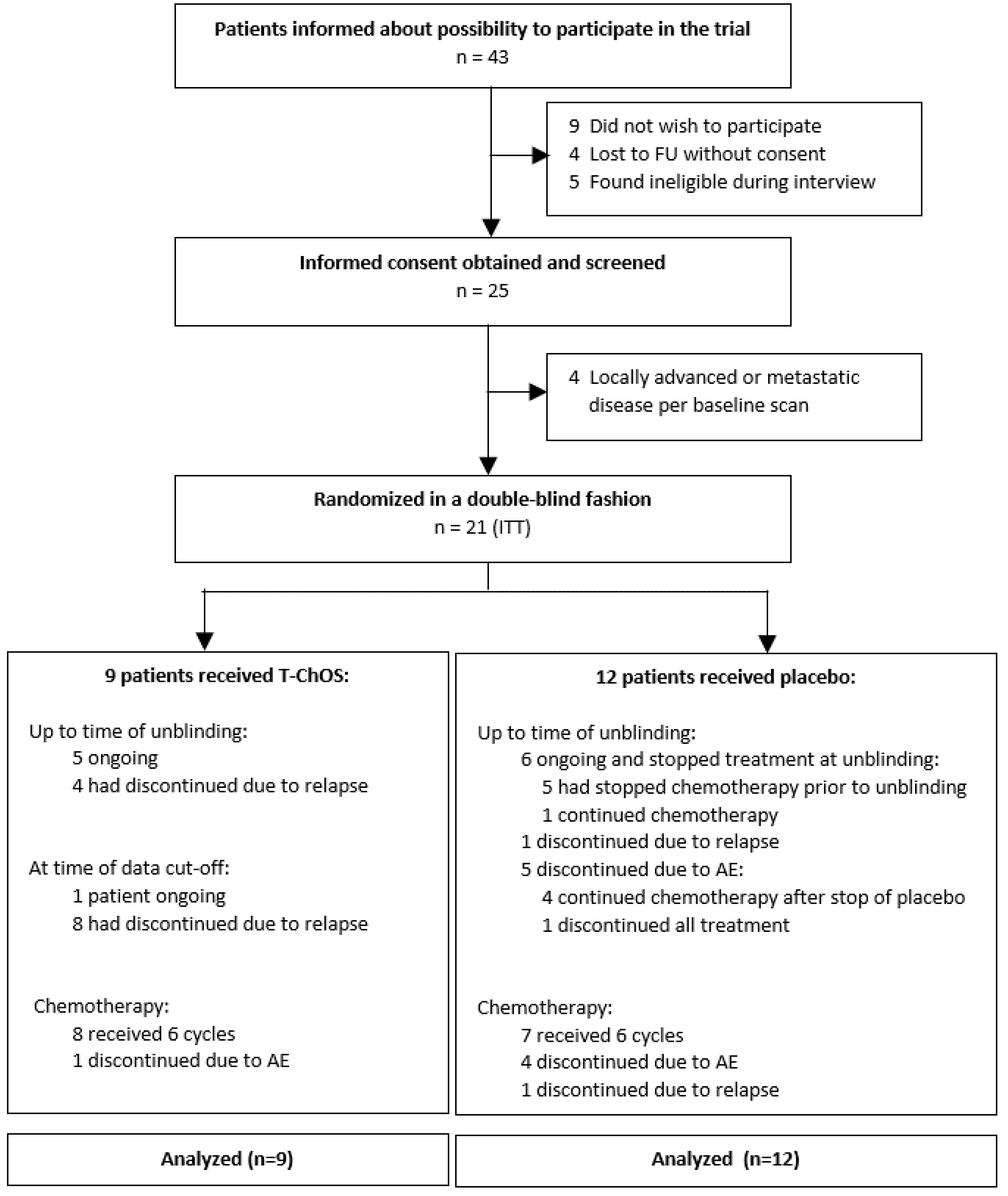
3.1. Patient Inclusion
3.2. Treatment
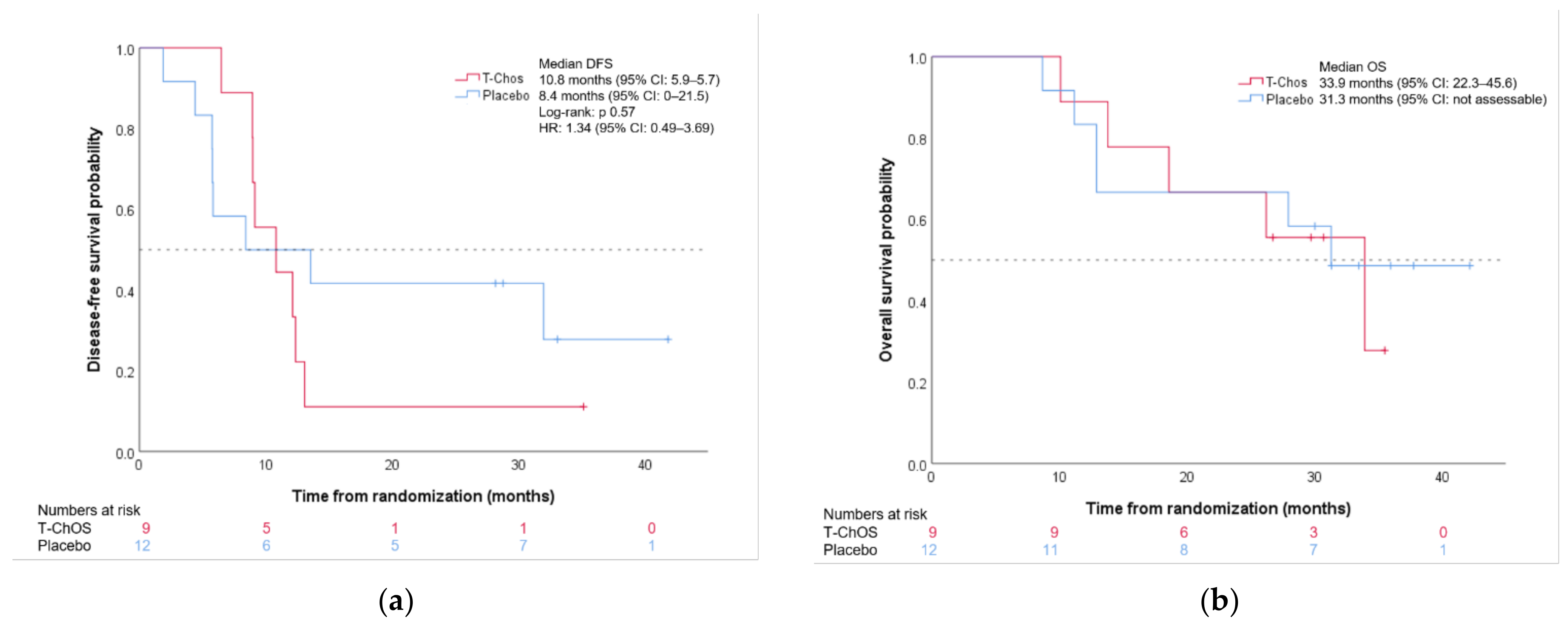
3.3. Efficacy
3.4. Safety
3.5. Translational Research
3.6. Quality of Life
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Carioli, G.; Bertuccio, P.; Boffetta, P.; Levi, F.; La Vecchia, C.; Negri, E.; Malvezzi, M. European cancer mortality predictions for the year 2020 with a focus on prostate cancer. Ann. Oncol. 2020, 31, 650–658. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Lau, S.C.; Cheung, W.Y. Evolving treatment landscape for early and advanced pancreatic cancer. World J. Gastrointest. Oncol. 2017, 9, 281–292. [Google Scholar] [CrossRef]
- Neoptolemos, J.P.; Stocken, D.D.; Friess, H.; Bassi, C.; Dunn, J.A.; Hickey, H.; Beger, H.; Fernandez-Cruz, L.; Dervenis, C.; Lacaine, F.; et al. A randomized trial of chemoradiotherapy and chemotherapy after resection of pancreatic cancer. N. Engl. J. Med. 2004, 350, 1200–1210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oettle, H.; Neuhaus, P.; Hochhaus, A.; Hartmann, J.T.; Gellert, K.; Ridwelski, K.; Niedergethmann, M.; Zulke, C.; Fahlke, J.; Arning, M.B.; et al. Adjuvant chemotherapy with gemcitabine and long-term outcomes among patients with resected pancreatic cancer: The CONKO-001 randomized trial. JAMA 2013, 310, 1473–1481. [Google Scholar] [CrossRef] [Green Version]
- Neoptolemos, J.P.; Palmer, D.H.; Ghaneh, P.; Psarelli, E.E.; Valle, J.W.; Halloran, C.M.; Faluyi, O.; O’Reilly, D.A.; Cunningham, D.; Wadsley, J.; et al. Comparison of adjuvant gemcitabine and capecitabine with gemcitabine monotherapy in patients with resected pancreatic cancer (ESPAC-4): A multicentre, open-label, randomised, phase 3 trial. Lancet 2017, 389, 1011–1024. [Google Scholar] [CrossRef]
- Park, B.K.; Kim, M.M. Applications of chitin and its derivatives in biological medicine. Int. J. Mol. Sci. 2010, 11, 5152–5164. [Google Scholar] [CrossRef] [Green Version]
- Liang, S.; Sun, Y.; Dai, X. A Review of the Preparation, Analysis and Biological Functions of Chitooligosaccharide. Int. J. Mol. Sci. 2018, 19, 2197. [Google Scholar] [CrossRef] [Green Version]
- Zhai, X.; Li, C.; Ren, D.; Wang, J.; Ma, C.; Abd El-Aty, A.M. The impact of chitooligosaccharides and their derivatives on the in vitro and in vivo antitumor activity: A comprehensive review. Carbohydr. Polym. 2021, 266, 118132. [Google Scholar] [CrossRef]
- Park, J.K.; Chung, M.J.; Choi, H.N.; Park, Y.I. Effects of the molecular weight and the degree of deacetylation of chitosan oligosaccharides on antitumor activity. Int. J. Mol. Sci. 2011, 12, 266–277. [Google Scholar] [CrossRef] [Green Version]
- Han, F.S.; Cui, B.H.; You, X.F.; Xing, Y.F.; Sun, X.W. Anti-proliferation and radiosensitization effects of chitooligosaccharides on human lung cancer line HepG2. Asian Pac. J. Trop. Med. 2015, 8, 757–761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, F.S.; Yang, S.J.; Lin, M.B.; Chen, Y.Q.; Yang, P.; Xu, J.M. Chitooligosaccharides promote radiosensitivity in colon cancer line SW480. World J. Gastroenterol. 2016, 22, 5193–5200. [Google Scholar] [CrossRef]
- Shen, K.T.; Chen, M.H.; Chan, H.Y.; Jeng, J.H.; Wang, Y.J. Inhibitory effects of chitooligosaccharides on tumor growth and metastasis. Food Chem. Toxicol. 2009, 47, 1864–1871. [Google Scholar] [CrossRef]
- Wu, M.; Li, J.; An, Y.; Li, P.; Xiong, W.; Li, J.; Yan, D.; Wang, M.; Zhong, G. Chitooligosaccharides Prevents the Development of Colitis-Associated Colorectal Cancer by Modulating the Intestinal Microbiota and Mycobiota. Front. Microbiol. 2019, 10, 2101. [Google Scholar] [CrossRef] [PubMed]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamisawa, T.; Wood, L.D.; Itoi, T.; Takaori, K. Pancreatic cancer. Lancet 2016, 388, 73–85. [Google Scholar] [CrossRef]
- Kleeff, J.; Korc, M.; Apte, M.; La Vecchia, C.; Johnson, C.D.; Biankin, A.V.; Neale, R.E.; Tempero, M.; Tuveson, D.A.; Hruban, R.H.; et al. Pancreatic cancer. Nat. Rev. Dis. Primers 2016, 2, 16022. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Xu, F.; Lu, T.; Duan, Z.; Zhang, Z. Interleukin-6 signaling pathway in targeted therapy for cancer. Cancer Treat. Rev. 2012, 38, 904–910. [Google Scholar] [CrossRef]
- Hunter, C.A.; Jones, S.A. IL-6 as a keystone cytokine in health and disease. Nat. Immunol. 2015, 16, 448–457. [Google Scholar] [CrossRef]
- Kumari, N.; Dwarakanath, B.S.; Das, A.; Bhatt, A.N. Role of interleukin-6 in cancer progression and therapeutic resistance. Tumour. Biol. 2016, 37, 11553–11572. [Google Scholar] [CrossRef]
- Johnson, D.E.; O’Keefe, R.A.; Grandis, J.R. Targeting the IL-6/JAK/STAT3 signalling axis in cancer. Nat. Rev. Clin. Oncol. 2018, 15, 234–248. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Stone, M.L.; Porrett, P.M.; Thomas, S.K.; Komar, C.A.; Li, J.H.; Delman, D.; Graham, K.; Gladney, W.L.; Hua, X.; et al. Hepatocytes direct the formation of a pro-metastatic niche in the liver. Nature 2019, 567, 249–252. [Google Scholar] [CrossRef]
- Zhao, T.; Su, Z.; Li, Y.; Zhang, X.; You, Q. Chitinase-3 like-protein-1 function and its role in diseases. Signal. Transduct. Target. Ther. 2020, 5, 201. [Google Scholar] [CrossRef] [PubMed]
- Vainer, N.; Dehlendorff, C.; Johansen, J.S. Systematic literature review of IL-6 as a biomarker or treatment target in patients with gastric, bile duct, pancreatic and colorectal cancer. Oncotarget 2018, 9, 29820–29841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bian, B.; Li, L.; Yang, J.; Liu, Y.; Xie, G.; Zheng, Y.; Zeng, L.; Zeng, J.; Shen, L. Prognostic value of YKL-40 in solid tumors: A meta-analysis of 41 cohort studies. Cancer Cell Int. 2019, 19, 259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xavier, C.P.R.; Castro, I.; Caires, H.R.; Ferreira, D.; Cavadas, B.; Pereira, L.; Santos, L.L.; Oliveira, M.J.; Vasconcelos, M.H. Chitinase 3-like-1 and fibronectin in the cargo of extracellular vesicles shed by human macrophages influence pancreatic cancer cellular response to gemcitabine. Cancer Lett. 2021, 501, 210–223. [Google Scholar] [CrossRef]
- Einarsson, J.M.; Bahrke, S.; Sigurdsson, B.T.; Ng, C.H.; Petersen, P.H.; Sigurjonsson, O.E.; Jonsson, H., Jr.; Gislason, J.; Thormodsson, F.R.; Peter, M.G. Partially acetylated chitooligosaccharides bind to YKL-40 and stimulate growth of human osteoarthritic chondrocytes. Biochem. Biophys. Res. Commun. 2013, 434, 298–304. [Google Scholar] [CrossRef]
- Conroy, T.; Hammel, P.; Hebbar, M.; Ben Abdelghani, M.; Wei, A.C.; Raoul, J.L.; Chone, L.; Francois, E.; Artru, P.; Biagi, J.J.; et al. FOLFIRINOX or Gemcitabine as Adjuvant Therapy for Pancreatic Cancer. N. Engl. J. Med. 2018, 379, 2395–2406. [Google Scholar] [CrossRef]
- Detlefsen, S. Nationale Retningslinjer—Kapitel 3—Patologisk Anatomi; Danish Pancreas Cancer Group: Odense, Denmark, 2015. [Google Scholar]
- Knudsen, L.S.; Christensen, I.J.; Lottenburger, T.; Svendsen, M.N.; Nielsen, H.J.; Nielsen, L.; Horslev-Petersen, K.; Jensen, J.E.; Kollerup, G.; Johansen, J.S. Pre-analytical and biological variability in circulating interleukin 6 in healthy subjects and patients with rheumatoid arthritis. Biomarkers 2008, 13, 59–78. [Google Scholar] [CrossRef]
- Bojesen, S.E.; Johansen, J.S.; Nordestgaard, B.G. Plasma YKL-40 levels in healthy subjects from the general population. Clin. Chim. Acta 2011, 412, 709–712. [Google Scholar] [CrossRef]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; Haes, J.C.J.M.d.; et al. The European Organization for Research and Treatment of Cancer QLQ-C30: A Quality-of-Life Instrument for Use in International Clinical Trials in Oncology. J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Bjordal, K.; de Graeff, A.; Fayers, P.M.; Hammerlid, E.; van Pottelsberghe, C.; Curran, D.; Ahlner-Elmqvist, M.; Maher, E.J.; Meyza, J.W.; Bredart, A.; et al. A 12 country field study of the EORTC QLQ-C30 (version 3.0) and the head and neck cancer specific module (EORTC QLQ-H&N35) in head and neck patients. EORTC Quality of Life Group. Eur. J. Cancer 2000, 36, 1796–1807. [Google Scholar] [CrossRef]
- Fayers, P.; Aaronson, N.K.; Bjordal, K.; Groenvold, M.; Curran, D.; Bottomley, A. EORTC QLQ-C30 Scoring Manual., 3rd ed.; European Organisation for Research and Treatment of Cancer: Brussels, Belgium, 2001. [Google Scholar]
- Neoptolemos, J.P.; Palmer, D.; Ghaneh, P.; Valle, J.W.; Cunningham, D.; Wadsley, J.; Meyer, T.; Anthoney, A.; Glimelius, B.; Falk, S.; et al. ESPAC-4: A multicenter, international, open-label randomized controlled phase III trial of adjuvant combination chemotherapy of gemcitabine (GEM) and capecitabine (CAP) versus monotherapy gemcitabine in patients with resected pancreatic ductal adenocarcinoma. J. Clin. Oncol. 2016, 34, LBA4006. [Google Scholar] [CrossRef]
- Conroy, T.; Hammel, P.; Hebbar, M.; Abdelghani, M.B.; Wei, A.C.-c.; Raoul, J.-L.; Chone, L.; Francois, E.; Artru, P.; Biagi, J.J.; et al. Unicancer GI PRODIGE 24/CCTG PA.6 trial: A multicenter international randomized phase III trial of adjuvant mFOLFIRINOX versus gemcitabine (gem) in patients with resected pancreatic ductal adenocarcinomas. J. Clin. Oncol. 2018, 36, LBA4001. [Google Scholar] [CrossRef]
- Oettle, H.; Post, S.; Neuhaus, P.; Gellert, K.; Langrehr, J.; Ridwelski, K.; Schramm, H.; Fahlke, J.; Zuelke, C.; Burkart, C.; et al. Adjuvant chemotherapy with gemcitabine vs observation in patients undergoing curative-intent resection of pancreatic cancer: A randomized controlled trial. JAMA 2007, 297, 267–277. [Google Scholar] [CrossRef] [PubMed]
- Neoptolemos, J.P.; Stocken, D.D.; Bassi, C.; Ghaneh, P.; Cunningham, D.; Goldstein, D.; Padbury, R.; Moore, M.J.; Gallinger, S.; Mariette, C.; et al. Adjuvant chemotherapy with fluorouracil plus folinic acid vs gemcitabine following pancreatic cancer resection: A randomized controlled trial. JAMA 2010, 304, 1073–1081. [Google Scholar] [CrossRef]
- Chen, Y.; Zhang, S.; Wang, Q.; Zhang, X. Tumor-recruited M2 macrophages promote gastric and breast cancer metastasis via M2 macrophage-secreted CHI3L1 protein. J. Hematol. Oncol. 2017, 10, 36. [Google Scholar] [CrossRef] [Green Version]
- Bakens, M.J.; van der Geest, L.G.; van Putten, M.; van Laarhoven, H.W.; Creemers, G.-J.; Besselink, M.G.; Lemmens, V.E.; de Hingh, I.H.; Dutch Pancreatic Cancer, G. The use of adjuvant chemotherapy for pancreatic cancer varies widely between hospitals: A nationwide population-based analysis. Cancer Med. 2016, 5, 2825–2831. [Google Scholar] [CrossRef]
- Labori, K.J.; Katz, M.H.; Tzeng, C.W.; Bjornbeth, B.A.; Cvancarova, M.; Edwin, B.; Kure, E.H.; Eide, T.J.; Dueland, S.; Buanes, T.; et al. Impact of early disease progression and surgical complications on adjuvant chemotherapy completion rates and survival in patients undergoing the surgery first approach for resectable pancreatic ductal adenocarcinoma—A population-based cohort study. Acta Oncol. 2016, 55, 265–277. [Google Scholar] [CrossRef]
- Skau Rasmussen, L.; Vittrup, B.; Ladekarl, M.; Pfeiffer, P.; Karen Yilmaz, M.; Ostergaard Poulsen, L.; Osterlind, K.; Palnaes Hansen, C.; Bau Mortensen, M.; Viborg Mortensen, F.; et al. The effect of postoperative gemcitabine on overall survival in patients with resected pancreatic cancer: A nationwide population-based Danish register study. Acta Oncol. 2019, 58, 864–871. [Google Scholar] [CrossRef] [Green Version]
- Altman, A.M.; Wirth, K.; Marmor, S.; Lou, E.; Chang, K.; Hui, J.Y.C.; Tuttle, T.M.; Jensen, E.H.; Denbo, J.W. Completion of Adjuvant Chemotherapy After Upfront Surgical Resection for Pancreatic Cancer Is Uncommon Yet Associated With Improved Survival. Ann. Surg. Oncol. 2019, 26, 4108–4116. [Google Scholar] [CrossRef] [PubMed]
- Valle, J.W.; Palmer, D.; Jackson, R.; Cox, T.; Neoptolemos, J.P.; Ghaneh, P.; Rawcliffe, C.L.; Bassi, C.; Stocken, D.D.; Cunningham, D.; et al. Optimal Duration and Timing of Adjuvant Chemotherapy After Definitive Surgery for Ductal Adenocarcinoma of the Pancreas: Ongoing Lessons From the ESPAC-3 Study. J. Clin. Oncol. 2014, 32, 504–512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chikhladze, S.; Lederer, A.K.; Kousoulas, L.; Reinmuth, M.; Sick, O.; Fichtner-Feigl, S.; Wittel, U.A. Adjuvant chemotherapy after surgery for pancreatic ductal adenocarcinoma: Retrospective real-life data. World J. Surg. Oncol. 2019, 17, 185. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| T-ChOS n = 9 | Placebo n = 12 | All Included Patients n = 21 | ||
|---|---|---|---|---|
| Characteristics | Number of Patients (%) | Number of Patients (%) | Number of Patients (%) | |
| Median age, years (range) | 68 (61–72) | 71 (59–80) | 71 (59–80) | |
| Gender | ||||
| Male | 3 (33.3) | 6 (50.0) | 9 (42.9) | |
| Female | 6 (66.7) | 6 (50.0) | 12 (57.1) | |
| ECOG Performance status | ||||
| 0 | 6 (66.7) | 10 (83.3) | 16 (76.2) | |
| 1 | 3 (33.3) | 2 (16.7) | 5 (23.8) | |
| Resection status | ||||
| R0 | 7 (77.8) | 9 (75.0) | 16 (76.2) | |
| R1 | 2 (22.2) | 3 (25.0) | 5 (23.8) | |
| Nodal status | ||||
| Lymph node negative | 1 (11.1) | 3 (25.0) | 4 (19.0) | |
| Lymph node positive | 8 (88.9) | 9 (75.0) | 17 (81.0) | |
| Tumor stage AJCC/UICC 8th edition | ||||
| IB | 1 (11.1) | 1 (8.3) | 2 (9.5) | |
| IIA | 0 | 2 (16.7) | 2 (9.5) | |
| IIB | 5 (55.6) | 5 (41.7) | 10 (47.6) | |
| III | 3 (33.3) | 4 (33.3) | 7 (33.3) | |
| Localization of primary tumor | ||||
| Head | 8 (88.9) | 8 (66.7) | 16 (76.2) | |
| Other | 1 (11.1) | 4 (33.3) | 5 (23.8) | |
| Type of resection | ||||
| Whipple resection | 7 (77.8) | 6 (50.0) | 13 (61.9) | |
| Distal pancreatectomy | 1 (1.11) | 4 (33.3) | 5 (23.8) | |
| Total pancreatectomy | 1 (11.1) | 2 (16.7) | 3 (14.3) | |
| Tumor grade | ||||
| Well differentiated | 0 | 1 (8.3) | 1 (4.8) | |
| Moderately differentiated | 5 (55.6) | 6 (50.0) | 9 (42.9) | |
| Poorly differentiated | 3 (33.3) | 3 (25.0) | 6 (28.6) | |
| Unknown | 1 (11.1) | 2 (16.7) | 3 (14.3) | |
| Local invasion | ||||
| No | 0 | 2 (16.7) | 2 (9.5) | |
| Yes | 7 (77.8) | 9 (75.0) | 16 (76.2) | |
| Unknown | 2 (22.2) | 1 (8.3) | 3 (14.3) | |
| Perineural invasion | ||||
| No | 3 (33.3) | 1 (8.3) | 4 (19.0) | |
| Yes | 6 (66.7) | 10 (83.3) | 16 (76.2) | |
| Unknown | 0 | 1 (8.3) | 1 (4.8) | |
| Postoperative complication | ||||
| No | 5 (55.6) | 8 (66.7) | 13 (61.9) | |
| Yes | 3 (33.3) | 4 (33.3) | 7 (33.3) | |
| Unknown | 1 (11.1) | 0 | 1 (4.8) | |
| Time from surgery to randomization | ||||
| Median days (range) | 42 (29–50) | 42 (28–87) | 42 (28–87) | |
| Baseline CA19-9 | ||||
| Median 103 IU/L (range) | 20 (3–73) | 44 (4–1430) | 26 (3–1430) | |
| T-ChOS n = 9 | Placebo n = 12 | All Included Patients n = 21 | |
|---|---|---|---|
| Gemcitabine | |||
| Median cycles received (range) | 6 (1–6) | 6 (1–6) | 6 (1–6) |
| Patients receiving 6 cycles, n (%) | 7 (77.8) | 7 (58.3) | 14 (66.7) |
| Median RDI % (range) | 88.9 (33.3–100) | 86.1 (38.9–100) | 88.9 (33.3–100) |
| Patients with RDI >80%, n (%) | 7 (77.8) | 7 (58.3) | 14 (66.7) |
| Capecitabine | |||
| Median cycles received (range) | 6 (1–6) | 4 (1–6) | 5 (1–6) |
| Patients receiving 6 cycles, n (%) | 5 (55.6) | 5 (41.7) | 10 (47.6) |
| Median RDI % (range) | 65.3 (4.8–100) | 73.1 (31.7–100) | 69.7 (4.8–100) |
| Patients with RDI >80%, n (%) | 3 (33.3) | 4 (33.3) | 7 (33.3) |
| T-ChOS™/Placebo | |||
| At time of unblinding | |||
| Median total exposure in days (range) | 279 (73–402) | 143 (11–589) | 212 (11–589) |
| Median actual exposure in days (range) | 276 (73–399) | 143 (11–558) | 212 (11–558) |
| At time of data cut-off | |||
| Median total exposure in days (range) | 374 (212–1078) | NA | 284 (11–1078) |
| Median actual exposure in days (range) | 374 (212–1078) | NA | 279 (11–1078) |
| Gemcitabine + Capecitabine + T-ChOS n = 9 | Gemcitabine + Capecitabine + Placebo n = 12 | |||
|---|---|---|---|---|
| All Grades | Grade 3–4 | All Grades | Grade 3–4 | |
| Any AE | 9 (100) | 7 (77.8) | 12 (100) | 11 (91.7) |
| Treatment-related AE | 9 (100) | 7 (77.8) | 12 (100) | 8 (66.7) |
| Anemia | 3 (33.3) | 1 (11.1) | 2 (16.7) | 0 |
| Neutropenia | 7 (77.8) | 4 (44.4) | 8 (66.7) | 7 (58.3) |
| Febrile neutropenia | 0 | 0 | 2 (16.7) | 2 (16.7) |
| Thrombocytopenia | 4 (44.4) | 1 (11.1) | 2 (16.7) | 0 |
| Fatigue | 6 (66.7) | 0 | 8 (66.7) | 0 |
| Diarrhea | 6 (66.7) | 1 (11.1) | 7 (58.3) | 0 |
| Nausea | 5 (55.6) | 0 | 5 (41.7) | 0 |
| Vomiting | 2 (22.2) | 0 | 3 (25.0) | 0 |
| Anorexia | 4 (44.4) | 0 | 7 (58.3) | 0 |
| Mucositis | 5 (55.6) | 1 (11.1) | 7 (58.3) | 0 |
| Other GI toxicity | 1 (11.1) | 0 | 1 (8.3) | 0 |
| Hand-Foot syndrome | 7 (77.8) | 0 | 9 (75.0) | 1 (8.3) |
| Rash | 1 (11.1) | 0 | 4 (33.3) | 0 |
| Pruritus | 1 (11.1) | 0 | 0 | 0 |
| Other skin toxicity | 2 (22.2) | 0 | 1 (8.3) | 0 |
| Flu-like symptoms | 2 (22.2)0 | 0 | 2 (16.7) | 0 |
| Fever | 2 (22.2) | 0 | 3 (25.0) | 0 |
| Infection | 4 (44.4) | 0 | 5 (41.7) | 1 (8.3) |
| Pneumonitis | 1 (11.1) | 1 (11.1) | 0 | 0 |
| Thrombophlebitis | 1 (11.1) | 0 | 1 (8.3) | 0 |
| Cerebral infarction | 0 | 0 | 1 (8.3) | 0 |
| Chest pain-cardiac | 0 | 0 | 1 (8.3) | 0 |
| Pain | 2 (22.2) | 0 | 2 (16.7) | 0 |
| Edema limbs | 2 (22.2) | 0 | 2 (16.7) | 0 |
| Myalgia | 1 (11.1) | 0 | 1 (8.3) | 0 |
| Hypokalemia | 1 (11.1) | 1 (11.1) | 1 (8.3) | 1 (8.3) |
| Injection site reaction | 0 | 0 | 2 (16.7) | 0 |
| Peripheral sensory neuropathy | 1 (11.1) | 0 | 0 | 0 |
| Dysuria | 0 | 0 | 1 (8.3) | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Theile, S.; Johansen, J.S.; Nielsen, D.L.; Jensen, B.V.; Hansen, C.P.; Hasselby, J.P.; Eiríksson, S.V.; Chen, I.M. A Randomized Placebo-Controlled Phase 2 Study of Gemcitabine and Capecitabine with or without T-ChOS as Adjuvant Therapy in Patients with Resected Pancreatic Cancer (CHIPAC). Pharmaceutics 2022, 14, 509. https://doi.org/10.3390/pharmaceutics14030509
Theile S, Johansen JS, Nielsen DL, Jensen BV, Hansen CP, Hasselby JP, Eiríksson SV, Chen IM. A Randomized Placebo-Controlled Phase 2 Study of Gemcitabine and Capecitabine with or without T-ChOS as Adjuvant Therapy in Patients with Resected Pancreatic Cancer (CHIPAC). Pharmaceutics. 2022; 14(3):509. https://doi.org/10.3390/pharmaceutics14030509
Chicago/Turabian StyleTheile, Susann, Julia Sidenius Johansen, Dorte Lisbet Nielsen, Benny Vittrup Jensen, Carsten Palnæs Hansen, Jane Preuss Hasselby, Sverrir Vídalín Eiríksson, and Inna Markovna Chen. 2022. "A Randomized Placebo-Controlled Phase 2 Study of Gemcitabine and Capecitabine with or without T-ChOS as Adjuvant Therapy in Patients with Resected Pancreatic Cancer (CHIPAC)" Pharmaceutics 14, no. 3: 509. https://doi.org/10.3390/pharmaceutics14030509