
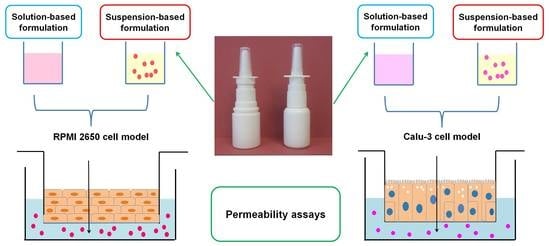
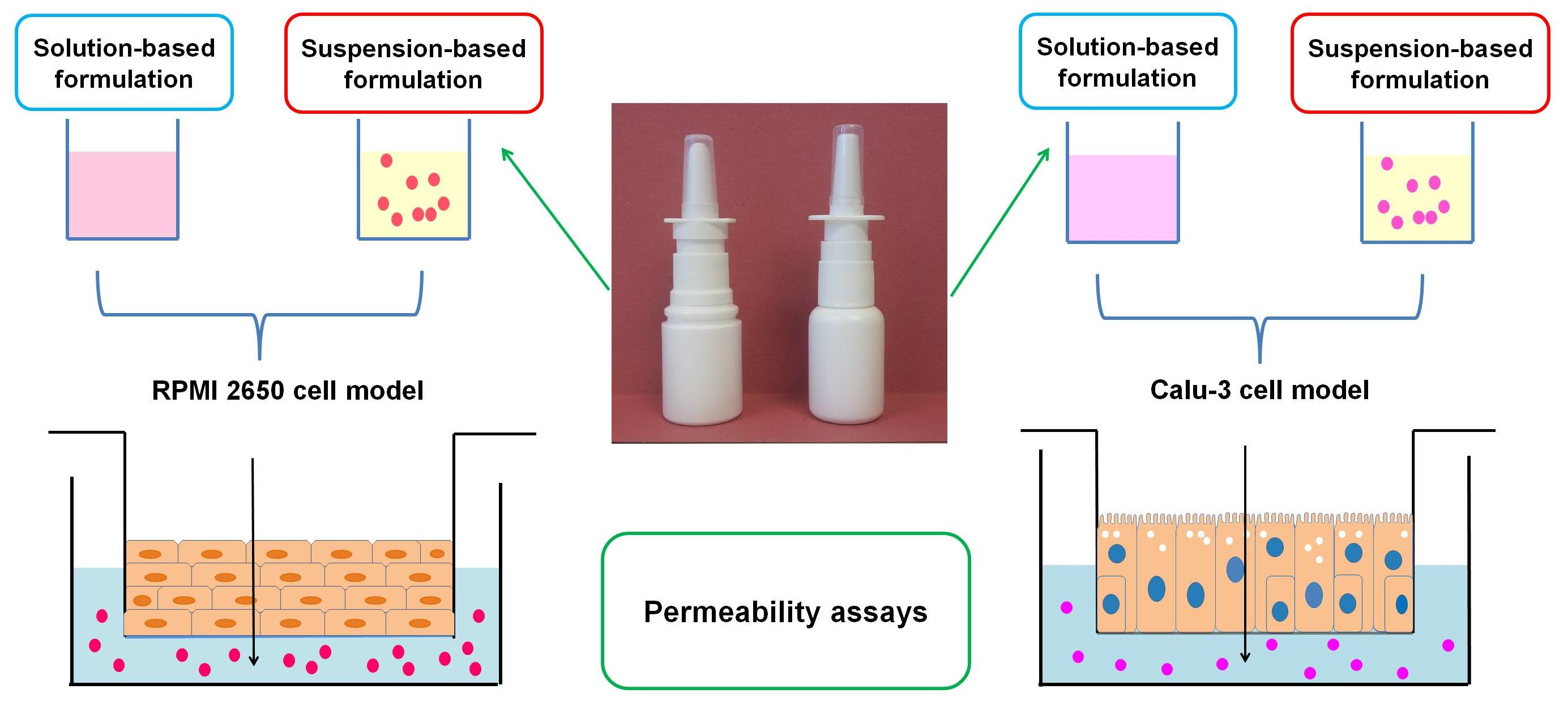
Applicability of RPMI 2650 and Calu-3 Cell Models for Evaluation of Nasal Formulations


Abstract
:
1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Cell Cultures
2.3. Permeability Assays
2.3.1. Permeability Assays of Formulations Containing Intranasal Corticosteroids with Low Aqueous Solubility (Beclomethasone Dipropionate, Fluticasone Propionate, Mometasone Furoate, Ciclesonide)
2.3.2. Permeability Assays for Nasal Formulations of First-Generation Intranasal Corticosteroids with Higher Aqueous Solubility and Other Nasally Administered Drugs
2.4. LDH Cytotoxicity Assay
2.5. Osmolarity Measurement
2.6. Analytical Methods
2.7. Permeability Data Analysis
2.8. Statistical Analysis
3. Results and Discussion
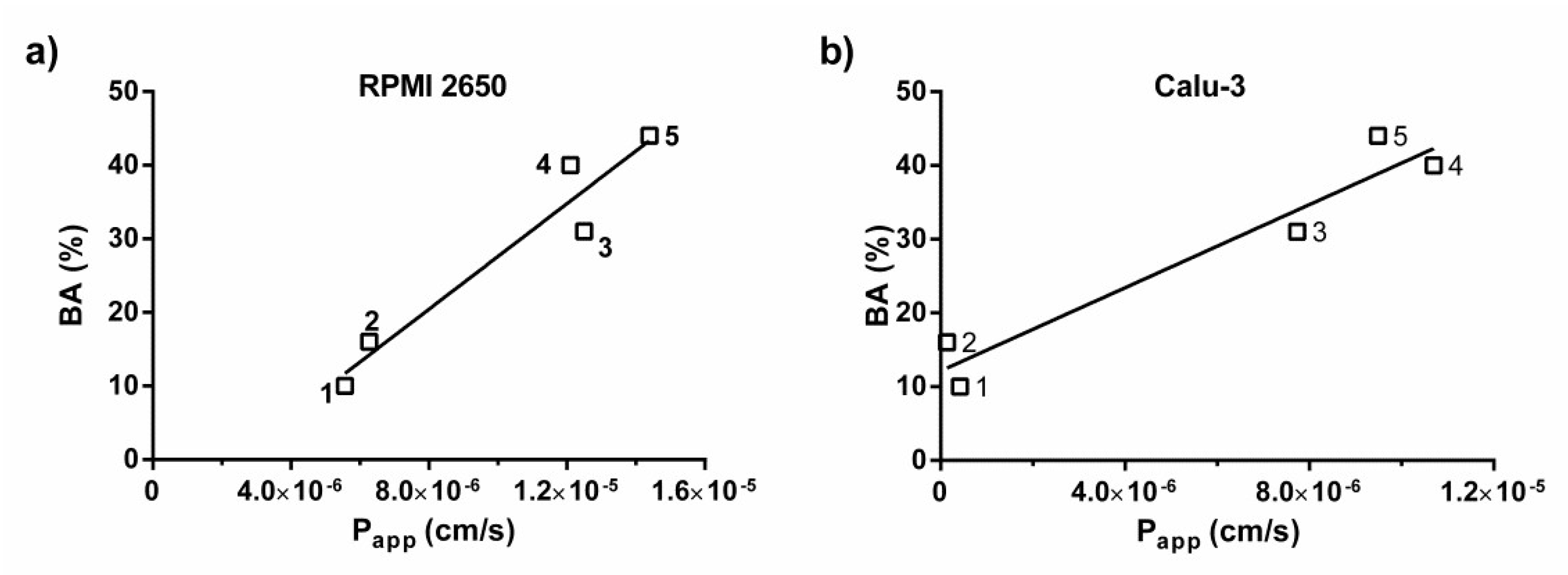
3.1. Permeability of Drugs from Solution-Based Nasal Formulations and Correlation with In Vivo Data
3.2. Permeability of Drugs from Suspension-Based Nasal Formulations
3.3. Applicability of the RPMI 2650 and Calu-3 Cell Models for Permeability Assessment of Nasal Formulations
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Reichl, S.; Becker, K. Cultivation of RPMI 2650 cells as an in-vitro model for human transmucosal nasal drug absorption studies: Optimization of selected culture conditions. J. Pharm. Pharmacol. 2012, 64, 1621–1630. [Google Scholar] [CrossRef]
- Wengst, A.; Reichl, S. RPMI 2650 epithelial model and three-dimensional reconstructed human nasal mucosa as in vitro models for nasal permeation studies. Eur. J. Pharm. Biopharm. 2010, 74, 290–297. [Google Scholar] [CrossRef] [PubMed]
- Wadell, C.; Björk, E.; Camber, O. Permeability of porcine nasal mucosa correlated with human nasal absorption. Eur. J. Pharm. Sci. 2003, 18, 47–53. [Google Scholar] [CrossRef]
- Yoo, J.W.; Kim, Y.S.; Lee, S.H.; Lee, M.K.; Roh, H.J.; Jhun, B.H.; Lee, C.H.; Kim, D.D. Serially Passaged Human Nasal Epithelial Cell Monolayer for in Vitro Drug Transport Studies. Pharm. Res. 2003, 20, 1690–1696. [Google Scholar] [CrossRef]
- Bai, S.; Yang, T.; Abbruscato, T.J.; Ahsan, F. Evaluation of human nasal RPMI 2650 cells grown at an air–liquid interface as a model for nasal drug transport studies. J. Pharm. Sci. 2008, 97, 1165–1178. [Google Scholar] [CrossRef] [PubMed]
- Olivier, J.-C.; Djilani, M.; Fahmy, S.; Couet, W. In situ nasal absorption of midazolam in rats. Int. J. Pharm. 2001, 213, 187–192. [Google Scholar] [CrossRef]
- Sibinovska, N.; Žakelj, S.; Kristan, K. Suitability of RPMI 2650 cell models for nasal drug permeability prediction. Eur. J. Pharm. Biopharm. 2019, 145, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Sibinovska, N.; Žakelj, S.; Roškar, R.; Kristan, K. Suitability and functional characterization of two Calu-3 cell models for prediction of drug permeability across the airway epithelial barrier. Int. J. Pharm. 2020, 585, 119484. [Google Scholar] [CrossRef] [PubMed]
- Grassin-Delyle, S.; Buenestado, A.; Naline, E.; Faisy, C.; Blouquit-Laye, S.; Couderc, L.-J.; Le Guen, M.; Fischler, M.; Devillier, P. Intranasal drug delivery: An efficient and non-invasive route for systemic administration: Focus on opioids. Pharmacol. Ther. 2012, 134, 366–379. [Google Scholar] [CrossRef]
- Ong, H.X.; Traini, D.; Young, P.M. Pharmaceutical applications of the Calu-3 lung epithelia cell line. Expert Opin. Drug Deliv. 2013, 10, 1287–1302. [Google Scholar] [CrossRef]
- Salade, L.; Wauthoz, N.; Goole, J.; Amighi, K. How to characterize a nasal product. The state of the art of in vitro and ex vivo specific methods. Int. J. Pharm. 2019, 561, 47–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kreft, M.E.; Jerman, U.D.; Lasič, E.; Rižner, T.L.; Hevir-Kene, N.; Peternel, L.; Kristan, K. The Characterization of the Human Nasal Epithelial Cell Line RPMI 2650 under Different Culture Conditions and Their Optimization for an Appropriate In Vitro Nasal Model. Pharm. Res. 2015, 32, 665–679. [Google Scholar] [CrossRef] [PubMed]
- Dimova, S.; Brewster, M.E.; Noppe, M.; Jorissen, M.; Augustijns, P. The use of human nasal in vitro cell systems during drug discovery and development. Toxicol. Vitr. 2005, 19, 107–122. [Google Scholar] [CrossRef] [PubMed]
- Kürti, L.; Veszelka, S.; Bocsik, A.; Ózsvári, B.; Puskás, L.G.; Kittel, Á.; Szabó-Révész, P.; Deli, M.A. Retinoic acid and hydrocortisone strengthen the barrier function of human RPMI 2650 cells, a model for nasal epithelial permeability. Cytotechnology 2013, 65, 395–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mercier, C.; Hodin, S.; He, Z.; Perek, N.; Delavenne, X. Pharmacological Characterization of the RPMI 2650 Model as a Relevant Tool for Assessing the Permeability of Intranasal Drugs. Mol. Pharm. 2018, 15, 2246–2256. [Google Scholar] [CrossRef]
- Furubayashi, T.; Inoue, D.; Nishiyama, N.; Tanaka, A.; Yutani, R.; Kimura, S.; Katsumi, H.; Yamamoto, A.; Sakane, T. Comparison of Various Cell Lines and Three-Dimensional Mucociliary Tissue Model Systems to Estimate Drug Permeability Using an In Vitro Transport Study to Predict Nasal Drug Absorption in Rats. Pharmaceutics 2020, 12, 79. [Google Scholar] [CrossRef] [Green Version]
- Inoue, D.; Furubayashi, T.; Tanaka, A.; Sakane, T.; Sugano, K. Quantitative estimation of drug permeation through nasal mucosa using in vitro membrane permeability across Calu-3 cell layers for predicting in vivo bioavailability after intranasal administration to rats. Eur. J. Pharm. Biopharm. 2020, 149, 145–153. [Google Scholar] [CrossRef]
- Kreft, M.E.; Jerman, U.D.; Lasič, E.; Hevir-Kene, N.; Rižner, T.L.; Peternel, L.; Kristan, K. The characterization of the human cell line Calu-3 under different culture conditions and its use as an optimized in vitro model to investigate bronchial epithelial function. Eur. J. Pharm. Sci. 2015, 69, 1–9. [Google Scholar] [CrossRef]
- Gonçalves, V.S.S.; Matias, A.A.; Poejo, J.; Serra, A.T.; Duarte, C.M.M. Application of RPMI 2650 as a cell model to evaluate solid formulations for intranasal delivery of drugs. Int. J. Pharm. 2016, 515, 1–10. [Google Scholar] [CrossRef]
- Kim, D.; Kim, Y.H.; Kwon, S. Enhanced nasal drug delivery efficiency by increasing mechanical loading using hypergravity. Sci. Rep. 2018, 8, 168. [Google Scholar] [CrossRef] [Green Version]
- Pozzoli, M.; Ong, H.X.; Morgan, L.; Sukkar, M.; Traini, D.; Young, P.M.; Sonvico, F. Application of RPMI 2650 nasal cell model to a 3D printed apparatus for the testing of drug deposition and permeation of nasal products. Eur. J. Pharm. Biopharm. 2016, 107, 223–233. [Google Scholar] [CrossRef] [PubMed]
- Salade, L.; Wauthoz, N.; Deleu, M.; Vermeersch, M.; De Vriese, C.; Amighi, K.; Goole, J. Development of coated liposomes loaded with ghrelin for nose-to-brain delivery for the treatment of cachexia. Int. J. Nanomed. 2017, 12, 8531–8543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sibinovska, N.; Božič, D.; Ribarski, M.B.; Kristan, K. Prediction of pharmacokinetic studies outcome for locally acting nasal sprays by using different in vitro methods. Int. J. Pharm. 2021, 601, 120569. [Google Scholar] [CrossRef]
- Teijeiro-Osorio, D.; Remuñán-López, C.; Alonso, M.J. New Generation of Hybrid Poly/Oligosaccharide Nanoparticles as Carriers for the Nasal Delivery of Macromolecules. Biomacromolecules 2009, 10, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Lebe, E.; Baka, M.; Yavaşoğlu, A.; Aktuğ, H.; Ates, U.; Uyanikgil, Y. Effects of Preservatives in Nasal Formulations on the Mucosal Integrity: An Electron Microscopic Study. Pharmacology 2004, 72, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Mallants, R.; Jorissen, M.; Augustijns, P. Beneficial effect of antibiotics on ciliary beat frequency of human nasal epithelial cells exposed to bacterial toxins. J. Pharm. Pharmacol. 2010, 60, 437–443. [Google Scholar] [CrossRef]
- Derendorf, H.; Munzel, U.; Petzold, U.; Maus, J.; Mascher, H.; Hermann, R.; Bousquet, J. Bioavailability and disposition of azelastine and fluticasone propionate when delivered by MP29-02, a novel aqueous nasal spray. Br. J. Clin. Pharmacol. 2012, 74, 125–133. [Google Scholar] [CrossRef] [Green Version]
- PRODUCT MONOGRAPH Pr IMITREX DF. 2018. Available online: https://ca.gsk.com/media/527922/imitrex.pdf (accessed on 16 February 2021).
- Kalanuria, A.A.; Peterlin, B.L. A Review of the Pharmacokinetics, Pharmacodynamics and Efficacy of Zolmitriptan in the Acute Abortive Treatment of Migraine. In Clinical Medicine: Therapeutics; SAGE Publications: Thousand Oaks, CA, USA, 2009. [Google Scholar]
- Canada, A. PRODUCT MONOGRAPH Pr ZOMIG ® (Zolmitriptan) Tablets 2.5 mg ZOMIG RAPIMELT ® (Zolmitriptan) Orally Disintegrating Tablets 2.5 mg Pr ZOMIG ® NASAL SPRAY (Zolmitriptan) Nasal Spray 2.5 and 5 mg 5-HT1 Receptor Agonist MIGRAINE THERAPY. 1998. Available online: https://www.astrazeneca.ca/content/dam/az-ca/downloads/productinformation/zomig-product-monograph-en.pdf (accessed on 16 February 2021).
- Wood, C.C.; Fireman, P.; Grossman, J.; Wecker, M.; MacGregor, T. Product characteristics and pharmacokinetics of intranasal ipratropium bromide. J. Allergy Clin. Immunol. 1995, 95, 1111–1116. [Google Scholar] [CrossRef]
- Daley-Yates, P.T.; Baker, R.C. Systemic bioavailability of fluticasone propionate administered as nasal drops and aqueous nasal spray formulations. Br. J. Clin. Pharmacol. 2001, 51, 103–105. [Google Scholar] [CrossRef] [Green Version]
- Public Assessment Report. Scientific Discussion Septanazal pro Dospělé 1 mg/ 50 mg v 1 ml Septanazal pro děti 0,5 mg/ 50 mg v 1 ml Nosní Spray, Roztok, Xylometazoline Hydrochloride, Dexpanthenol CZ/H/170/01-02/DC. 2012. Available online: https://mri.cts-mrp.eu/human/downloads/CZ_H_0170_001_PAR.pdf (accessed on 3 April 2021).
- Zhao, G.H.; Kapur, N.; Carlin, B.; Selinger, E.; Guthrie, J.T. Characterisation of the interactive properties of microcrystalline cellulose–carboxymethyl cellulose hydrogels. Int. J. Pharm. 2011, 415, 95–101. [Google Scholar] [CrossRef]
- Pu, Y.; Goodey, A.P.; Fang, X.; Jacob, K. A Comparison of the Deposition Patterns of Different Nasal Spray Formulations Using a Nasal Cast. Aerosol Sci. Technol. 2014, 48, 930–938. [Google Scholar] [CrossRef] [Green Version]
- Panduga, V.; Stocks, M.J.; Bosquillon, C. Ipratropium is ‘luminally recycled’ by an inter-play between apical uptake and efflux transporters in Calu-3 bronchial epithelial cell layers. Int. J. Pharm. 2017, 532, 328–336. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.; Zeng, S. Transport characteristics of zolmitriptan in a human intestinal epithelial cell line Caco-2. J. Pharm. Pharmacol. 2010, 59, 655–660. [Google Scholar] [CrossRef]
- Pontier, C.; Pachot, J.; Botham, R.; Lenfant, B.; Arnaud, P. HT29-MTX and Caco-2/TC7 Monolayers as Predictive Models for Human Intestinal Absorption: Role of the Mucus Layer. J. Pharm. Sci. 2001, 90, 1608–1619. [Google Scholar] [CrossRef] [PubMed]
- FDA. CDER ASTELIN-Azelastine Hydrochloride Spray, Metered. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/020114s023lbl.pdf (accessed on 11 February 2021).
- Thorsson, L.; Borgâ, O.; Edsbäcker, S. Systemic availability of budesonide after nasal administration of three different formulations: Pressurized aerosol, aqueous pump spray, and powder. Br. J. Clin. Pharmacol. 1999, 47, 619–624. [Google Scholar] [CrossRef] [Green Version]
- Kågedal, M.; Zingmark, P.-H.; Hedlund, C.; Yates, R. True Nasopharyngeal Absorption of Zolmitriptan after Administration via Nasal Spray in Healthy Male Volunteers. Am. J. Drug Deliv. 2005, 3, 133–140. [Google Scholar] [CrossRef]
- Obaidi, M.; Offman, E.; Messina, J.; Carothers, J.; Djupesland, P.G.; Mahmoud, R.A. Improved Pharmacokinetics of Sumatriptan with B reath P owered™ Nasal Delivery of Sumatriptan Powder. Headache 2013, 53, 1323–1333. [Google Scholar] [CrossRef] [Green Version]
- Hirsh, J.; Tibbetts, D. (No Title). Available online: https://patentimages.storage.googleapis.com/08/20/a4/b1c41ffa1c9f82/US20050153946A1.pdf (accessed on 20 May 2021).
- Chong, L.Y.; Head, K.; Hopkins, C.; Philpott, C.; Burton, M.; Schilder, A.G.M. Different types of intranasal steroids for chronic rhinosinusitis. Cochrane Database Syst. Rev. 2016, 4, CD011993. [Google Scholar] [CrossRef] [Green Version]
- Edsbäcker, S.; Johansson, C.-J. Airway Selectivity: An Update of Pharmacokinetic Factors Affecting Local and Systemic Disposition of Inhaled Steroids. Basic Clin. Pharmacol. Toxicol. 2006, 98, 523–536. [Google Scholar] [CrossRef]
- Baumann, D.; Bachert, C.; Högger, P. Dissolution in nasal fluid, retention and anti-inflammatory activity of fluticasone furoate in human nasal tissue ex vivo. Clin. Exp. Allergy 2009, 39, 1540–1550. [Google Scholar] [CrossRef]
- Li, J.; Hidalgo, I.J.; Parran, D. The Evolving Role of the Caco-2 Cell Model to Estimate Intestinal Absorption Potential and Elucidate Transport Mechanisms. In The Process of New Drug Discovery and Development, 2nd ed.; CRC Press: Boca Raton, FL, USA, 2006; pp. 161–186. [Google Scholar] [CrossRef]
- Hardy, J.G.; Lee, S.W.; Wilson, C.G. Intranasal drug delivery by spray and drops. J. Pharm. Pharmacol. 1985, 37, 294–297. [Google Scholar] [CrossRef] [PubMed]
- Berger, W.E.; Bachert, C.; Allara, R.; Koltun, A.; Kopietz, F.; Maus, J.G.; D’Addio, A.D. Evaluation of In Vitro Penetration of Fluticasone Propionate from MP-AzeFlu and Fluticasone Propionate Nasal Spray Through EpiAirway™606 Tissues Using Vertical Diffusion Cells. J. Asthma Allergy 2020, 13, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Gao, M.; Shen, X.; Mao, S. Factors influencing drug deposition in the nasal cavity upon delivery via nasal sprays. J. Pharm. Investig. 2020, 50, 251–259. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Drug | Tested Formulation | Concentration (mg/mL) | A–L RPMI 2650 Model | A–L Calu-3 Model | Nasal Bioavailability (%) | ||
|---|---|---|---|---|---|---|---|
| Papp ± SD (×10−7 cm/s) | Papp ± SD (×10−7 cm/s) | ||||||
| Undiluted Formulation | 10-Fold Diluted Formulation | Undiluted Formulation | 10-Fold Diluted Formulation | ||||
| Naphazoline | Benil® drops | 1 | 6.29 ± 0.29 | 3.58 ± 0.39 | 3.21 ± 0.24 | 2.51 ± 0.34 | No data available |
| Oxymetazoline | Operil® drops | 0.25 | 52.9 ± 3.69 | 58.9 ± 1.67 | 5.85 ± 0.32 | 5.95 ± 0.37 | No data available |
| Operil® drops | 0.5 | 50.5 ± 3.99 | 49.4 ± 3.91 | 5.31 ± 0.57 | 5.96 ± 0.66 | ||
| Xylometazoline | Maresyl spray | 1 | 74.0 ± 4.54 | 68.9 ± 2.49 | 23.0 ± 1.43 | 32.1 ± 3.32 | No data available |
| Xylometazoline + Dexpanthenol | Septanazal® spray | 0.5 a | 53.2 ± 1.46 | 50.8 ± 1.94 | 12.3 ± 2.16 | 12.1 ± 1.78 | No data available |
| Septanazal® spray | 1 a | 53.6 ± 4.65 | 56.3 ± 4.36 | 9.35 ± 1.40 | 14.2 ± 2.45 | ||
| Xylometazoline + Ipratropium | Otrivin® Duo spray | 0.5 a | 48.8 ± 11.50 | 41.6 ± 5.40 | 17.2 ± 1.27 | 17.3 ± 0.81 | No data available |
| Azelastine | Allergodil® Akut | 1 | cell layer integrity not maintained | 121 ± 11.3 | cell layer integrity not maintained | 106 ± 9.4 | 40 [27] |
| Azelastine HCl Nasal Solution 0.15%, Perrigo | 1.5 | 121 ± 24.0 | 107 ± 16.6 | ||||
| Azelastine HCl Nasal Solution 0.15%, Apotex Corp. | 1.5 | 136 ± 14.7 | 102 ± 5.66 | ||||
| Solution in assay buffer with 1% MeOH | 0.01 b | 80.1 ± 4.84 | / | 97.9 ± 16.6 | / | ||
| Azelastine +Fluticasone propionate | Dymista® spray | 1 a | cell layer integrity not maintained | 61.2 ± 5.84 | cell layer integrity not maintained | 60.3 ± 2.80 | |
| Sumatriptan | Sumatriptan Sandoz Nasal spray 20 mg | 200 | NT * | 62.7 ± 6.19 | NT * | 1.39 ± 0.28 | 16 [28] |
| Solution in assay buffer | 0.14 c | 107 ± 18.1 | / | 3.38 ± 1.12 | / | ||
| Zolmitriptan | Zomig® 5 mg Nasal spray | 50 | NT * | 15.9 ± 1.63 | NT * | 0.73 ± 0.17 | 42 [29,30] |
| Solution in assay buffer with 1% DMSO | 0.1 | 89.6 ± 4.09 | / | 2.77 ± 0.20 | / | ||
| Ipratropium | Solution in assay buffer | 0.6/3 d | 50.62 ± 8.95 | / | 1.74 ± 0.73 | / | 10 [31] |
| Ipratropium + Xylometazoline | Otrivin® Duo | 0.6 a | 55.4 ± 13.44 | 55.7 ± 5.31 | 4.33 ± 0.29 | NT * | No data available |
| Triamcinolone acetonide | Solution in assay buffer with 1% DMSO | 0.02 | 143.9 ± 8.96 | / | 94.9 ± 5.03 | / | 44 [32] |
| Budesonide | Solution in assay buffer with 1% DMSO | 0.02 | 124.8 ± 11.31 | / | 77.4 ± 22.3 | / | 31 [32] |
| Drug | Tested Formulation | A–L RPMI 2650 Model | A–L Calu-3 Model | ||
|---|---|---|---|---|---|
| Mean flux ± SD (×10−2 µg/cm2/h) | Papp ± SD (×10−7 cm/s) | Mean flux ± SD (×10−2 µg/cm2/h) | Papp ± SD (×10−7 cm/s) | ||
| Budesonide | Tafen® (undiluted) | 214 ± 37 | NA * | 166 ± 15 | NA * |
| Tafen® (10-fold diluted) | 191 ± 13 | NA * | 73 ± 0.09 | NA * | |
| Assay buffer with 1% DMSO | 68.5 ± 6.88 | 125 ± 11 | 40.0 ± 9.86 | 77.4 ± 22.3 | |
| Triamcinolone acetonide | Nasacort® AQ (undiluted) | 81 ± 7 | NA * | 100 ± 8 | NA * |
| Nasacort® AQ (10-fold diluted) | 66 ± 4 | NA * | 49 ± 9 | NA * | |
| Tri-Nasal® (undiluted) | 60.3 ± 9.94 | 3.35 ± 0.55 | 45.2 ± 5.96 | 2.51 ± 0.33 | |
| Assay buffer with 1% DMSO | 105 ± 11 | 143 ±14.6 | 69.7 ± 3.7 | 94.9 ± 5.03 | |
| Drug | Tested Formulation | A–L RPMI 2650 Model | A–L Calu-3 Model | ||
|---|---|---|---|---|---|
| Mean Flux ± SD (×10−2 µg/cm2/h) | |||||
| Undiluted Formulation | 10-Fold Diluted Formulation | Undiluted Formulation | 10-Fold Diluted Formulation | ||
| Beclomethasone dipropionate | Beconase AQ® | 0.77 ± 0.24 | 0.66 ± 0.25 | 0.28 ± 0.13 | 0.28 ± 0.09 |
| Ciclesonide | Omnaris® | 0.41 ± 0.16 | 0.63 ± 0.20 | 0.47 ± 0.07 | 0.61 ± 0.17 |
| Fluticasone propionate | Flixonase® nasal drops | 1.57 ± 0.14 | 1.40 ± 0.27 | 1.82 ± 0.21 | 1.60 ± 0.34 |
| Flixonase® nasal spray | 1.21 ± 0.14 | 1.32 ± 0.07 | 1.25 ± 0.11 | 1.31 ± 0.22 | |
| Fluticasone propionate+Azelastine | Dymista® | 1.29 ± 0.13 | 1.63 ± 0.32 | 1.73 ± 0.13 | 2.07 ± 0.08 |
| Mometasone furoate | Mommox® | 0.78 ± 0.37 | 0.87 ± 0.22 | 0.91 ± 0.12 | 1.15 ± 0.20 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sibinovska, N.; Žakelj, S.; Trontelj, J.; Kristan, K. Applicability of RPMI 2650 and Calu-3 Cell Models for Evaluation of Nasal Formulations. Pharmaceutics 2022, 14, 369. https://doi.org/10.3390/pharmaceutics14020369
Sibinovska N, Žakelj S, Trontelj J, Kristan K. Applicability of RPMI 2650 and Calu-3 Cell Models for Evaluation of Nasal Formulations. Pharmaceutics. 2022; 14(2):369. https://doi.org/10.3390/pharmaceutics14020369
Chicago/Turabian StyleSibinovska, Nadica, Simon Žakelj, Jurij Trontelj, and Katja Kristan. 2022. "Applicability of RPMI 2650 and Calu-3 Cell Models for Evaluation of Nasal Formulations" Pharmaceutics 14, no. 2: 369. https://doi.org/10.3390/pharmaceutics14020369