
Recent Advancements in Drug Delivery of Sinomenine, A Disease-Modifying Anti-Rheumatic Drug

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
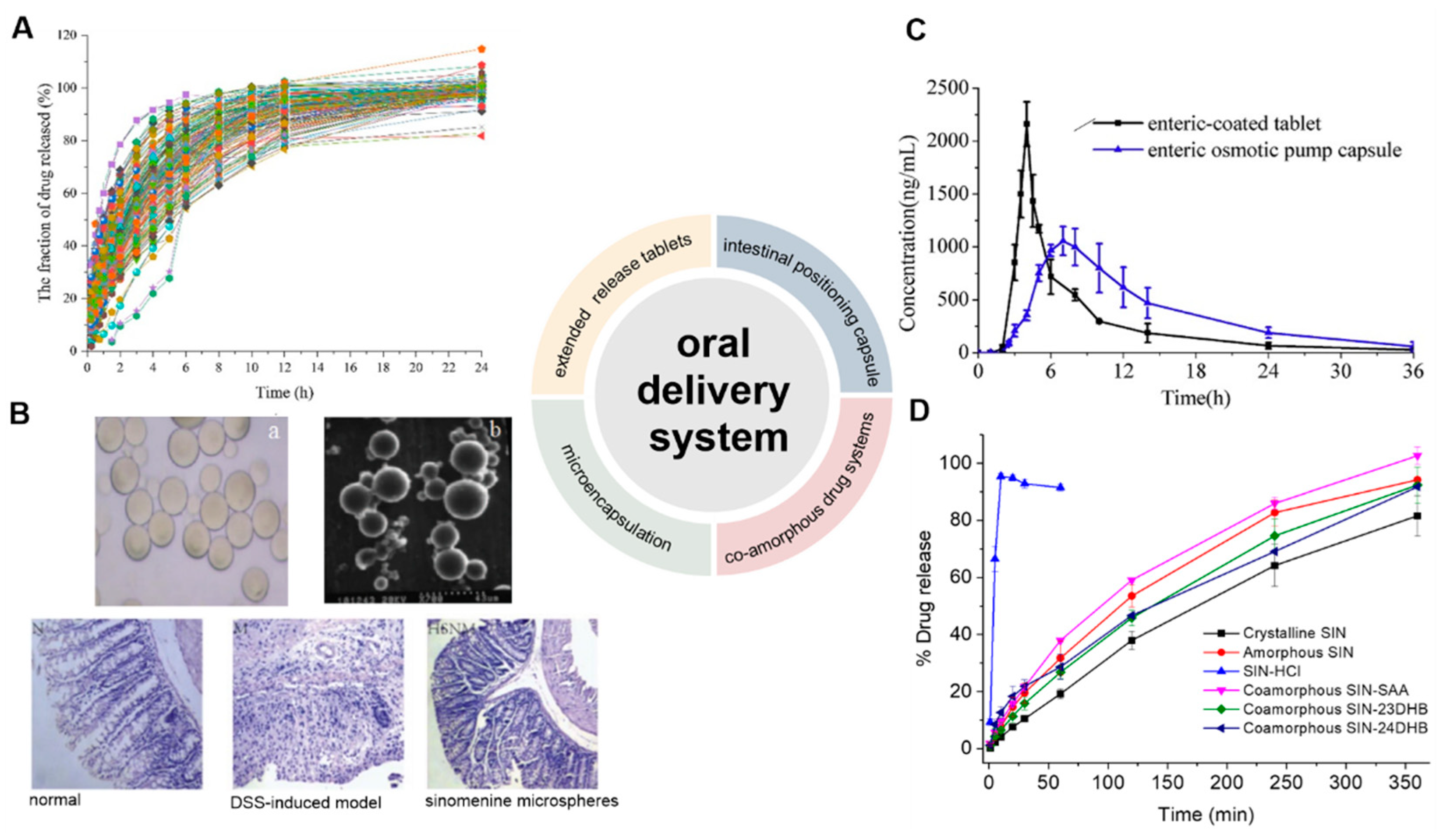
2. Oral Delivery Systems
2.1. Extended-Release Tablets
2.2. Microencapsulation
2.3. Intestinal Positioning Capsule

2.4. Co-Amorphous Drug Systems
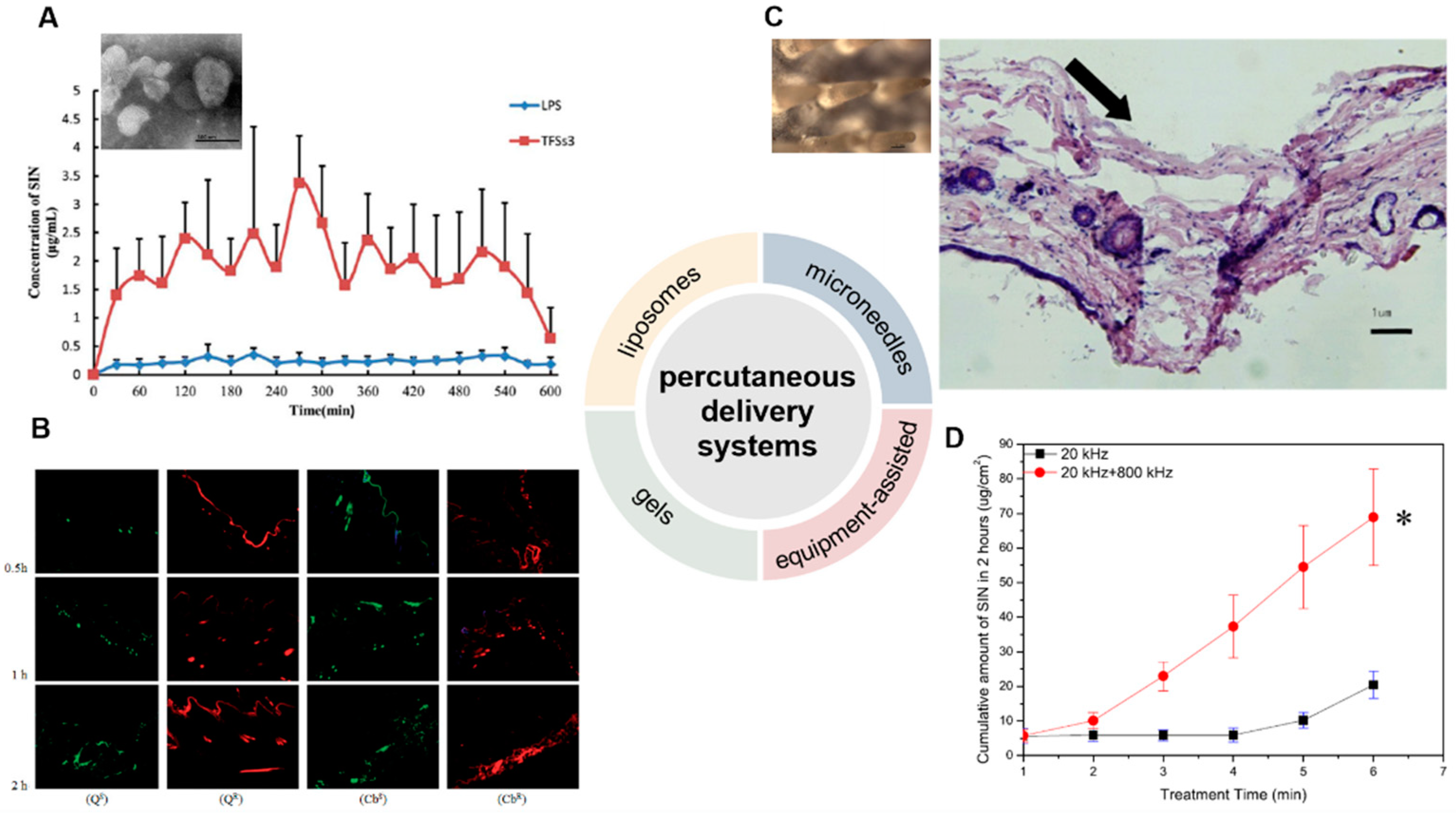
3. Percutaneous Delivery Systems
3.1. Liposomes
3.2. Gels
3.3. Microneedles
3.4. Physically Assisted Delivery Systems
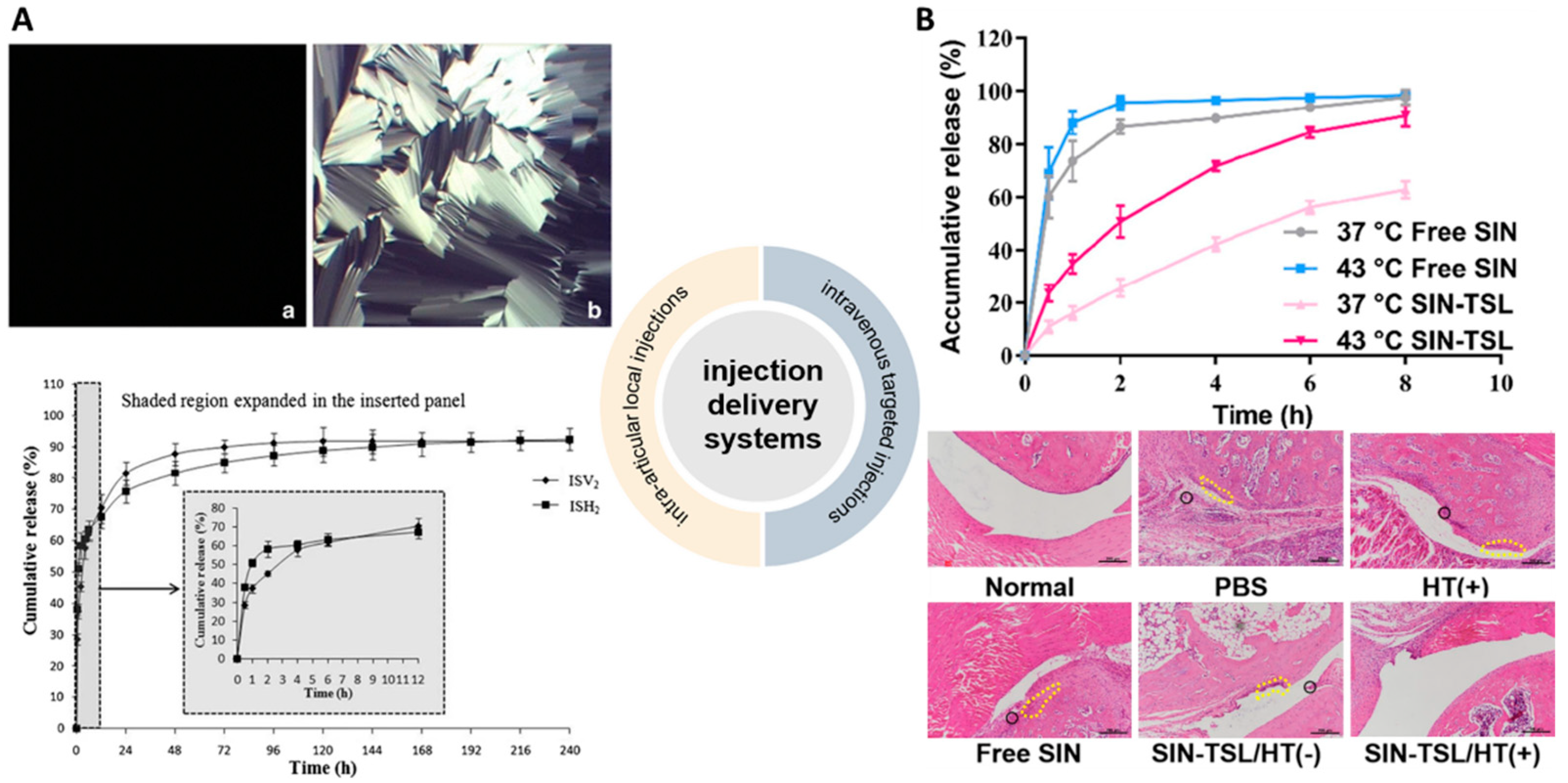
4. Injection Delivery Systems
4.1. Intra-Articular Local Injections
4.2. Intravenous Targeted Injections

5. Other Delivery Systems
6. Perspective
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Choy, E.H.S.; Panayi, G.S. Mechanisms of disease: Cytokine pathways and joint inflammation in rheumatoid arthritis. N. Engl. J. Med. 2001, 344, 907–916. [Google Scholar] [CrossRef]
- Chaudhari, K.; Rizvi, S.; Syed, B.A. Rheumatoid arthritis: Current and future trends. Nat. Rev. Drug Discov. 2016, 15, 305–306. [Google Scholar] [CrossRef]
- Listing, J.; Gerhold, K.; Zink, A. The risk of infections associated with rheumatoid arthritis, with its comorbidity and treatment. Rheumatology 2013, 52, 53–61. [Google Scholar] [CrossRef] [Green Version]
- Crossfield, S.S.R.; Buch, M.H.; Baxter, P.; Kingsbury, S.R.; Pujades-Rodriguez, M.; Conaghan, P.G. Changes in the pharmacological management of rheumatoid arthritis over two decades. Rheumatology 2021, 60, 4141–4151. [Google Scholar] [CrossRef]
- Kok, T.W.; Yue, P.Y.K.; Mak, N.K.; Fan, T.P.D.; Liu, L.; Wong, R.N.S. The anti-angiogenic effect of sinomenine. Angiogenesis 2005, 8, 3–12. [Google Scholar] [CrossRef]
- Liu, W.W.; Xian, Q.; Wei, J.; Yan, L.; Gang, W.; Yue, W. Effects and safety of sinomenine in treatment of rheumatoid arthritis contrast to methotrexate: A systematic review and meta-analysis. J. Tradit. Chin. Med. 2016, 36, 564–577. [Google Scholar] [CrossRef] [Green Version]
- Huang, R.Y.; Pan, H.D.; Wu, J.Q.; Zhou, H.; Li, Z.G.; Qiu, P.; Zhou, Y.Y.; Chen, X.M.; Xie, Z.X.; Xiao, Y.; et al. Comparison of combination therapy with methotrexate and sinomenine or leflunomide for active rheumatoid arthritis: A randomized controlled clinical trial. Phytomedicine Int. J. Phytother. Phytopharm. 2019, 57, 403–410. [Google Scholar] [CrossRef]
- Tong, B.; Yu, J.T.; Wang, T.; Dou, Y.N.; Wu, X.; Kong, L.Y.; Dai, Y.; Xia, Y.F. Sinomenine suppresses collagen-induced arthritis by reciprocal modulation of regulatory t cells and th17 cells in gut-associated lymphoid tissues. Mol. Immunol. 2015, 65, 94–103. [Google Scholar] [CrossRef]
- Xiong, L.; Yang, L.Y. Effects of alkaloid sinomenine on levels of ifn-gamma, il-1 beta, tnf-alpha and il-6 in a rat renal allograft model. Immunotherapy 2012, 4, 785–791. [Google Scholar] [CrossRef]
- Xiong, H.F.; Tian, L.; Zhao, Z.H.; Chen, S.P.; Zhao, Q.Y.; Hong, J.B.; Xie, Y.; Zhou, N.J.; Fu, Y.J. The sinomenine enteric-coated microspheres suppressed the tlr/nf-kappa b signaling in dss-induced experimental colitis. Int. Immunopharmacol. 2017, 50, 251–262. [Google Scholar] [CrossRef]
- Liu, W.W.; Zhang, Y.J.; Zhu, W.N.; Ma, C.H.; Ruan, J.; Long, H.Y.; Wang, Y. Sinomenine inhibits the progression of rheumatoid arthritis by regulating the secretion of inflammatory cytokines and monocyte/macrophage subsets. Front. Immunol. 2018, 9, 2228. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Liu, J.X.; Luo, J.F.; Cheng, C.S.; Leung, E.L.H.; Li, Y.; Su, X.H.; Liu, Z.Q.; Chen, T.B.; Duan, F.G.; et al. Suppressing mpges-1 expression by sinomenine ameliorates inflammation and arthritis. Biochem. Pharmacol. 2017, 142, 133–144. [Google Scholar] [CrossRef] [PubMed]
- Mu, H.; Yao, R.B.; Zhao, L.J.; Shen, S.Y.; Zhao, Z.M.; Cai, H. Sinomenine decreases myd88 expression and improves inflammation-induced joint damage progression and symptoms in rat adjuvant-induced arthritis. Inflammation 2013, 36, 1136–1144. [Google Scholar] [CrossRef] [PubMed]
- Zeng, M.Y.; Tong, Q.Y. Anti-inflammation effects of sinomenine on macrophages through suppressing activated tlr4/nf-kappa b signaling pathway. Curr. Med. Sci. 2020, 40, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Peng, C.; Shi, Q.P.; Liu, J.Y.; Lv, Y.J.; Li, J.; Yi, L.; Bai, S.S.; Liu, L.; Wang, P.X.; Zhou, H.; et al. Alpha7 nachr expression is correlated with arthritis development and inhibited by sinomenine in adjuvant-induced arthritic rats. Evid.-Based Complement. Altern. Med. 2019, 2019, 3759304. [Google Scholar] [CrossRef] [Green Version]
- Yi, L.; Lyn, Y.J.; Peng, C.; Zhu, R.L.; Bai, S.S.; Liu, L.; Wang, P.C.; Zhou, H.; Dong, Y. Sinomenine inhibits fibroblast-like synoviocyte proliferation by regulating alpha 7nachr expression via erk/egr-1 pathway. Int. Immunopharmacol. 2018, 56, 65–70. [Google Scholar] [CrossRef]
- Yi, L.; Luo, J.F.; Xie, B.B.; Liu, J.X.; Wang, J.Y.; Liu, L.; Wang, P.C.; Zhou, H.; Dong, Y. Alpha 7 nicotinic acetylcholine receptor is a novel mediator of sinomenine anti-inflammation effect in macrophages stimulated by lipopolysaccharide. Shock 2015, 44, 188–195. [Google Scholar] [CrossRef]
- Zhou, H.; Wong, Y.F.; Wang, J.; Cai, X.; Liu, L. Sinomenine ameliorates arthritis via mmps, timps, and cytokines in rats. Biochem. Biophys. Res. Commun. 2008, 376, 352–357. [Google Scholar] [CrossRef]
- Liao, K.; Su, X.; Lei, K.; Liu, Z.; Lu, L.; Wu, Q.; Pan, H.; Huang, Q.; Zhao, Y.; Wang, M.; et al. Sinomenine protects bone from destruction to ameliorate arthritis via activating p62(thr269)(/)(ser272)-keap1-nrf2 feedback loop. Biomed. Pharmacother. 2021, 135, 111195. [Google Scholar] [CrossRef]
- Jiang, W.; Fan, W.M.; Gao, T.L.; Li, T.; Yin, Z.M.; Guo, H.H.; Wang, L.L.; Han, Y.X.; Jiang, J.D. Analgesic mechanism of sinomenine against chronic pain. Pain Res. Manag. 2020, 2020, 1876862. [Google Scholar] [CrossRef]
- Yin, N.N.; Xiong, Y.; Tao, W.T.; Chen, J.J.; Wang, Z.G. Sinomenine alleviates lipopolysaccharide-induced inflammatory responses in raw264.7 macrophages. Immunopharmacol. Immunotoxicol. 2020, 42, 147–155. [Google Scholar] [CrossRef]
- Shen, K.H.; Hung, J.H.; Liao, Y.C.; Tsai, S.T.; Wu, M.J.; Chen, P.S. Sinomenine inhibits migration and invasion of human lung cancer cell through downregulating expression of mir-21 and mmps. Int. J. Mol. Sci. 2020, 21, 3080. [Google Scholar] [CrossRef]
- Yuan, M.L.; Zhao, B.; Jia, H.P.; Zhang, C.; Zuo, X.W. Sinomenine ameliorates cardiac hypertrophy by activating nrf2/are signaling pathway. Bioengineered 2021, 12, 12778–12788. [Google Scholar] [CrossRef]
- Song, W.; Yang, X.T.; Wang, W.Q.; Wang, Z.; Wu, J.; Huang, F.J. Sinomenine ameliorates septic acute lung injury in mice by modulating gut homeostasis via aryl hydrocarbon receptor/nrf2 pathway. Eur. J. Pharmacol. 2021, 912, 174581. [Google Scholar] [CrossRef]
- Singh, D.; Agrawal, A.; Singal, C.M.S.; Pandey, H.S.; Seth, P.; Sharma, S.K. Sinomenine inhibits amyloid beta-induced astrocyte activation and protects neurons against indirect toxicity. Mol. Brain 2020, 13, 30. [Google Scholar] [CrossRef] [Green Version]
- Yang, H.F.; Wang, J.; Chen, X.L.; Jiang, C.M.; He, K.W.; Li, B.; Hu, Y.Y. Effects of sinomenine in lps-associated diseases are related to inhibition of lbp, mac-1, and l-selectin levels. J. Vet. Pharmacol. Ther. 2019, 42, 732–737. [Google Scholar] [CrossRef]
- Li, X.R.; Li, X.Y.; Zhou, Y.X.; Liu, Y.; Guo, M.; Zhu, Q.F.; Xie, Y.C.; Fan, Z.Y. Development of patch and spray formulations for enhancing topical delivery of sinomenine hydrochloride. J. Pharm. Sci. 2010, 99, 1790–1799. [Google Scholar] [CrossRef]
- Sun, Y.L.; Zhu, S.S.; Lu, W.J.; Chen, J.Y.; Sun, C.J.; Guo, Y.X.; Wang, B.; Gao, S.; Fang, W.Y.; Hu, R.F. A novel enteric positioning osmotic pump capsule-based controlled release system of sinomenine hydrochloride: In vitro and in vivo evaluation. J. Drug Deliv. Sci. Technol. 2019, 49, 188–194. [Google Scholar] [CrossRef]
- Zhang, Y.S.; Han, J.Y.; Iqbal, O.; Liang, A.H. Research advances and prospects on mechanism of sinomenin on histamine release and the binding to histamine receptors. Int. J. Mol. Sci. 2019, 20, 70. [Google Scholar] [CrossRef] [Green Version]
- Zeng, Q.; Wang, L.; Wu, S.J.; Fang, G.P.; Liu, H.; Li, Z.; Hu, Y.F.; Li, W.L. Dissolution profiles prediction of sinomenine hydrochloride sustained-release tablets using raman mapping technique. Int. J. Pharm. 2022, 620, 121743. [Google Scholar] [CrossRef]
- Wang, X.L.; Huang, Y.; Zhu, J.; Pan, Y.B.; He, R.; Wang, Y.Z. Chitosan-graft poly(p-dioxanone) copolymers: Preparation, characterization, and properties. Carbohydr. Res. 2009, 344, 801–807. [Google Scholar] [CrossRef]
- Zhang, W.; Gao, Y.; Yang, N.; Zhang, H.; Zhang, F.; Chen, H.Q.; Meng, J.Q.; Zhang, S.Y.; Li, W. Sinomenine-loaded microcapsules fabricated by phase reversion emulsification-drying in liquid method: An evaluation of process parameters, characterization, and released properties. J. Bioact. Compat. Polym. 2018, 33, 382–396. [Google Scholar] [CrossRef]
- Shi, D.S.; Greever, R.; Chen, Y.F. Preparation and characterization of novel sinomenine microcapsules for oral controlled drug delivery. Drug Dev. Ind. Pharm. 2010, 36, 482–489. [Google Scholar] [CrossRef]
- Chen, H.Q.; Zhang, W.; Yang, N.; Chen, C.M.; Zhang, M.L. Chitosan-based surface molecularly imprinted polymer microspheres for sustained release of sinomenine hydrochloride in aqueous media. Appl. Biochem. Biotechnol. 2018, 185, 370–384. [Google Scholar] [CrossRef]
- Zhang, W.; Fu, H.L.; Li, X.Y.; Zhang, H.; Wang, N.; Li, W.; Zhang, X.X. Molecularly imprinted polymer doped with hectorite for selective recognition of sinomenine hydrochloride. J. Biomater. Sci.-Polym. Ed. 2016, 27, 144–156. [Google Scholar] [CrossRef]
- Wu, S.; Zeng, Q.; Zhang, Z.; Zhang, X.; Hou, Y.; Li, Z.; Jia, C.; Liu, Y.; Li, W. Development of sinomenine hydrochloride sustained-release pellet using a novel whirlwind fluidized bed. J. Drug Deliv. Sci. Technol. 2022, 78, 103956. [Google Scholar] [CrossRef]
- Chen, X.; Li, D.X.; Zhang, H.L.; Duan, Y.W.; Huang, Y. Sinomenine-phenolic acid coamorphous drug systems: Solubilization, sustained release, and improved physical stability. Int. J. Pharm. 2021, 598, 120389. [Google Scholar] [CrossRef]
- Chen, X.; Li, D.X.; Zhang, H.L.; Duan, Y.W.; Huang, Y. Co-amorphous systems of sinomenine with nonsteroidal anti-inflammatory drugs: A strategy for solubility improvement, sustained release, and drug combination therapy against rheumatoid arthritis. Int. J. Pharm. 2021, 606, 120894. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Li, D.; Duan, Y.; Huang, Y. Characterization of co-amorphous sinomenine-tranilast systems with strong intermolecular interactions and sustained release profiles. J. Drug Deliv. Sci. Technol. 2022, 71, 103296. [Google Scholar] [CrossRef]
- Chen, X.; Li, D.X.; Zhang, H.L.; Duan, Y.W.; Huang, Y. Co-amorphous systems of sinomenine with platensimycin or sulfasalazine: Physical stability and excipient-adjusted release behavior. Mol. Pharm. 2022, 19, 4370–4381. [Google Scholar] [CrossRef]
- Wang, J.; Wei, Y.; Fei, Y.R.; Fang, L.; Zheng, H.S.; Mu, C.F.; Li, F.Z.; Zhang, Y.S. Preparation of mixed monoterpenes edge activated pegylated transfersomes to improve the in vivo transdermal delivery efficiency of sinomenine hydrochloride. Int. J. Pharm. 2017, 533, 266–274. [Google Scholar] [CrossRef]
- Song, H.; Wen, J.; Li, H.; Meng, Y.; Zhang, Y.J.; Zhang, N.; Zheng, W.S. Enhanced transdermal permeability and drug deposition of rheumatoid arthritis via sinomenine hydrochloride-loaded antioxidant surface transethosome. Int. J. Nanomed. 2019, 14, 3177–3188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ba, W.Q.; Li, Z.; Wang, L.S.; Wang, D.; Liao, W.G.; Fan, W.T.; Wu, Y.N.; Liao, F.Y.; Yu, J.Y. Optimization and evaluation of pluronic lecithin organogels as a transdermal delivery vehicle for sinomenine. Pharm. Dev. Technol. 2016, 21, 535–545. [Google Scholar] [CrossRef] [PubMed]
- Chu, X.Q.; Wang, X.Q.; Tian, C.L.; Liu, L.; Xia, M.Q.; Jiang, J.Q.; Gui, S.Y. Dual drug-loaded cubic liquid crystal gels for transdermal delivery: Inner structure and percutaneous mechanism evaluations. Drug Dev. Ind. Pharm. 2019, 45, 1879–1888. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.J.; Tao, Y.T.; Zhou, Y.J.; Gui, S.Y. Development of sinomenine hydrochloride-loaded polyvinylalcohol/maltose microneedle for transdermal delivery. J. Drug Deliv. Sci. Technol. 2016, 35, 1–7. [Google Scholar] [CrossRef]
- Yan, H.; Yan, M.; Li, H.D.; Jiang, P.; Deng, Y.; Cai, H.L. Pharmacokinetics and penetration into synovial fluid of systemical and electroporation administered sinomenine to rabbits. Biomed. Chromatogr. 2015, 29, 883–889. [Google Scholar] [CrossRef]
- Feng, S.; Zhu, L.J.; Huang, Z.S.; Wang, H.J.; Li, H.; Zhou, H.; Lu, L.L.; Wang, Y.; Liu, Z.Q.; Liu, L. Controlled release of optimized electroporation enhances the transdermal efficiency of sinomenine hydrochloride for treating arthritis in vitro and in clinic. Drug Des. Devel. Ther. 2017, 11, 1737–1752. [Google Scholar] [CrossRef] [Green Version]
- Yin, L.; Qin, F.H.; Zhou, Y.; Qi, X. Enhancing percutaneous permeability of sinomenine hydrochloride using dual-frequency sonophoresis. J. Drug Deliv. Sci. Technol. 2016, 36, 62–67. [Google Scholar] [CrossRef]
- Zhou, L.I.; Wang, Y.; Liu, Q.F.; Ling, J.J. Study on determination of entrapment efficiency of sinomenine liposomes. Zhongguo Zhong Yao Za Zhi 2006, 31, 731–734. (In Chinese) [Google Scholar]
- Wang, Y.; Cong, Z.; Liu, Q.; Ling, J.; Zhou, L. Study on optimization of formulation and preparation process of sinomenine liposomes. Zhongguo Zhong Yao Za Zhi 2009, 34, 275–278. (In Chinese) [Google Scholar]
- Godin, B.; Touitou, E. Ethosomes: New prospects in transdermal delivery. Crit. Rev. Ther. Drug Carr. Syst. 2003, 20, 63–102. [Google Scholar] [CrossRef] [PubMed]
- Yan, Y.; Zhang, H.F.; Sun, J.Y.; Wang, P.C.; Dong, K.; Dong, Y.L.; Xing, J.F. Enhanced transdermal delivery of sinomenine hydrochloride by ethosomes for anti-inflammatory treatment. J. Drug Deliv. Sci. Technol. 2016, 36, 201–207. [Google Scholar] [CrossRef]
- Cevc, G.; Schäitzlein, A.; Blume, G. Transdermal drug carriers: Basic properties, optimization and transfer efficiency in the case of epicutaneously applied peptides. J. Control. Release 1995, 36, 3–16. [Google Scholar] [CrossRef]
- Cevc, G.; Schatzlein, A.; Richardsen, H. Ultradeformable lipid vesicles can penetrate the skin and other semi-permeable barriers unfragmented. Evidence from double label clsm experiments and direct size measurements. Biochim. Biophys. Acta-Biomembr. 2002, 1564, 21–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaudhary, H.; Kohli, K.; Kumar, V. Nano-transfersomes as a novel carrier for transdermal delivery. Int. J. Pharm. 2013, 454, 367–380. [Google Scholar] [CrossRef]
- Fan, Y.; Lu, Y.; Cheng, B.; Wei, Y.; Wei, Y.; Piao, J.; Li, F.; Zheng, H. Correlation between in vivo microdialysis pharmacokinetics and ex vivo permeation for sinomenine hydrochloride transfersomes with enhanced skin absorption. Int. J. Pharm. 2022, 621, 121789. [Google Scholar] [CrossRef]
- Zheng, H.S.; Xu, C.; Fei, Y.R.; Wang, J.; Yang, M.S.; Fang, L.; Wei, Y.H.; Mu, C.F.; Sheng, Y.J.; Li, F.Z.; et al. Monoterpenes-containing pegylated transfersomes for enhancing joint cavity drug delivery evidenced by clsm and double-sited microdialysis. Mater. Sci. Eng. C-Mater. Biol. Appl. 2020, 113, 110929. [Google Scholar] [CrossRef]
- Jukanti, R.; Devaraj, G.; Devaraj, R.; Apte, S. Drug targeting to inflammation: Studies on antioxidant surface loaded diclofenac liposomes. Int. J. Pharm. 2011, 414, 179–185. [Google Scholar] [CrossRef]
- Rehman, K.; Zulfakar, M.H. Recent advances in gel technologies for topical and transdermal drug delivery. Drug Dev. Ind. Pharm. 2014, 40, 433–440. [Google Scholar] [CrossRef]
- Phan, S.; Fong, W.K.; Kirby, N.; Hanley, T.; Boyd, B.J. Evaluating the link between self-assembled mesophase structure and drug release. Int. J. Pharm. 2011, 421, 176–182. [Google Scholar] [CrossRef]
- Guo, C.Y.; Wang, J.; Cao, F.L.; Lee, R.J.; Zhai, G.X. Lyotropic liquid crystal systems in drug delivery. Drug Discov. Today 2010, 15, 1032–1040. [Google Scholar] [CrossRef] [PubMed]
- Chu, X.Q.; Li, Q.; Gui, S.Y.; Li, Z.G.; Cao, J.J.; Jiang, J.Q. Characterization and in vitro permeation study of cubic liquid crystal containing sinomenine hydrochloride. AAPS PharmSciTech 2018, 19, 2237–2246. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, K.; Yokota, Y.; Zhai, Y.; Quan, Y.S.; Kamiyama, F.; Mukai, Y.; Okada, N.; Nakagawa, S. A low-invasive and effective transcutaneous immunization system using a novel dissolving microneedle array for soluble and particulate antigens. J. Control. Release 2012, 161, 10–17. [Google Scholar] [CrossRef]
- Martin, C.J.; Allender, C.J.; Brain, K.R.; Morrissey, A.; Birchall, J.C. Low temperature fabrication of biodegradable sugar glass microneedles for transdermal drug delivery applications. J. Control. Release 2012, 158, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Vrdoljak, A.; McGrath, M.G.; Carey, J.B.; Draper, S.J.; Hill, A.V.S.; O’Mahony, C.; Crean, A.M.; Moore, A.C. Coated microneedle arrays for transcutaneous delivery of live virus vaccines. J. Control. Release 2012, 159, 34–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, Y.C.; Park, J.H.; Prausnitz, M.R. Microneedles for drug and vaccine delivery. Adv. Drug Deliv. Rev. 2012, 64, 1547–1568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, X.X.; Chen, Y.L.; Gui, S.Y.; Wu, X.Q.; Chen, L.; Cao, Y.J.; Yin, D.K.; Ma, P. Sinomenine hydrochloride-loaded dissolving microneedles enhanced its absorption in rabbits. Pharm. Dev. Technol. 2016, 21, 787–793. [Google Scholar] [CrossRef] [PubMed]
- Gui, Z.P.; Wu, X.X.; Wang, S.Y.; Cao, Y.J.; Wan, J.; Shan, Q.Q.; Yang, Z.Z.; Zhang, J.W.; Gui, S.Y. Dissolving microneedles integrated with liquid crystals facilitate transdermal delivery of sinomenine hydrochloride. J. Pharm. Sci. 2017, 106, 3548–3555. [Google Scholar] [CrossRef]
- Shu, Z.X.; Cao, Y.J.; Tao, Y.T.; Liang, X.; Wang, F.Y.; Li, Z.; Li, Z.B.; Gui, S.Y. Polyvinylpyrrolidone microneedles for localized delivery of sinomenine hydrochloride: Preparation, release behavior of in vitro & in vivo, and penetration mechanism. Drug Deliv. 2020, 27, 642–651. [Google Scholar] [CrossRef] [Green Version]
- Denet, A.R.; Vanbever, R.; Preat, V. Skin electroporation for transdermal and topical delivery. Adv. Drug Deliv. Rev. 2004, 56, 659–674. [Google Scholar] [CrossRef]
- Chen, Y.L.; Liang, X.; Ma, P.; Tao, Y.T.; Wu, X.Q.; Wu, X.X.; Chu, X.Q.; Gui, S.Y. Phytantriol-based in situ liquid crystals with long-term release for intra-articular administration. AAPS PharmSciTech 2015, 16, 846–854. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Cao, J.J.; Li, Z.G.; Chu, X.Q. Cubic liquid crystalline gels based on glycerol monooleate for intra-articular injection. AAPS PharmSciTech 2018, 19, 858–865. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Shao, H.R.; Fang, S.Y.; Cheng, Y.L.; Ling, P.X.; Chen, J.Y. Evaluation of pharmacokinetics and pharmaco-dynamics of sinomenine-hyaluronic acid conjugate after intra-articular administration for osteoarthritis treatment. Drug Des. Devel. Ther. 2019, 13, 657–665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerwin, N.; Hops, C.; Lucke, A. Intraarticular drug delivery in osteoarthritis. Adv. Drug Deliv. Rev. 2006, 58, 226–242. [Google Scholar] [CrossRef] [PubMed]
- Liang, X.; Chen, Y.L.; Wu, L.; Maharjan, A.; Regmi, B.; Zhang, J.W.; Gui, S.Y. In situ hexagonal liquid crystal for intra-articular delivery of sinomenine hydrochloride. Biomed. Pharmacother. 2019, 117, 108993. [Google Scholar] [CrossRef]
- Liu, W.G.; Ling, P.X.; Lin, X.K.; Chen, J.Y.; Wang, S.J.; Li, P.; Wu, X.J.; Zhao, D.M.; Liu, S.H. Therapeutic effect of an injectable sustained-release sinomenine hydrochloride and sodium hyaluronate compound in a rabbit model of osteoarthritis. Chin. Med. J. 2012, 125, 2543–2547. [Google Scholar] [CrossRef] [PubMed]
- Shen, Q.Y.; Zhang, X.Z.; Qi, J.; Shu, G.F.; Du, Y.Z.; Ying, X.Y. Sinomenine hydrochloride loaded thermosensitive liposomes combined with microwave hyperthermia for the treatment of rheumatoid arthritis. Int. J. Pharm. 2020, 576, 119001. [Google Scholar] [CrossRef]
- Zhang, T.Y.; Ouyang, X.; Gou, S.H.; Zhang, Y.; Yan, N.; Chang, L.L.; Li, B.B.; Zhang, F.Y.; Liu, H.; Ni, J.M. Novel synovial targeting peptide-sinomenine conjugates as a potential strategy for the treatment of rheumatoid arthritis. Int. J. Pharm. 2022, 617, 121628. [Google Scholar] [CrossRef]
- Lin, Y.; Yi, O.; Hu, M.; Hu, S.; Su, Z.; Liao, J.; Wang, W.; Wang, S.; Liu, L.; Liu, B.; et al. Multifunctional nanoparticles of sinomenine hydrochloride for treat-to-target therapy of rheumatoid arthritis via modulation of proinflammatory cytokines. J. Control. Release 2022, 348, 42–56. [Google Scholar] [CrossRef]
- Sharma, R.; Kambhampati, S.P.; Zhang, Z.; Sharma, A.; Chen, S.; Duh, E.I.; Kannan, S.; Tso, M.O.M.; Kannan, R.M. Dendrimer mediated targeted delivery of sinomenine for the treatment of acute neuroinflammation in traumatic brain injury. J. Control. Release 2020, 323, 361–375. [Google Scholar] [CrossRef]
- Song, J.K.; Bi, H.S.; Xie, X.F.; Guo, J.G.; Wang, X.R.; Liu, D.M. Preparation and evaluation of sinomenine hydrochloride in situ gel for uveitis treatment. Int. Immunopharmacol. 2013, 17, 99–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caramella, C.M.; Rossi, S.; Ferrari, F.; Bonferoni, M.C.; Sandri, G. Mucoadhesive and thermogelling systems for vaginal drug delivery. Adv. Drug Deliv. Rev. 2015, 92, 39–52. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Liu, L.; Gui, S.Y.; Wang, X.Q.; Hu, R.F.; Zhang, Y.; Tian, C.L.; Xia, M.Q.; Chu, X.Q. A novel phytantriol-based in situ liquid crystal gel for vaginal delivery. AAPS PharmSciTech 2019, 20, 185. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, X.; Lu, C.; Duan, Y.; Huang, Y. Recent Advancements in Drug Delivery of Sinomenine, A Disease-Modifying Anti-Rheumatic Drug. Pharmaceutics 2022, 14, 2820. https://doi.org/10.3390/pharmaceutics14122820
Chen X, Lu C, Duan Y, Huang Y. Recent Advancements in Drug Delivery of Sinomenine, A Disease-Modifying Anti-Rheumatic Drug. Pharmaceutics. 2022; 14(12):2820. https://doi.org/10.3390/pharmaceutics14122820
Chicago/Turabian StyleChen, Xin, Chengcheng Lu, Yanwen Duan, and Yong Huang. 2022. "Recent Advancements in Drug Delivery of Sinomenine, A Disease-Modifying Anti-Rheumatic Drug" Pharmaceutics 14, no. 12: 2820. https://doi.org/10.3390/pharmaceutics14122820