
Dissolution and Absorption of Inhaled Drug Particles in the Lungs


Abstract
:1. Introduction
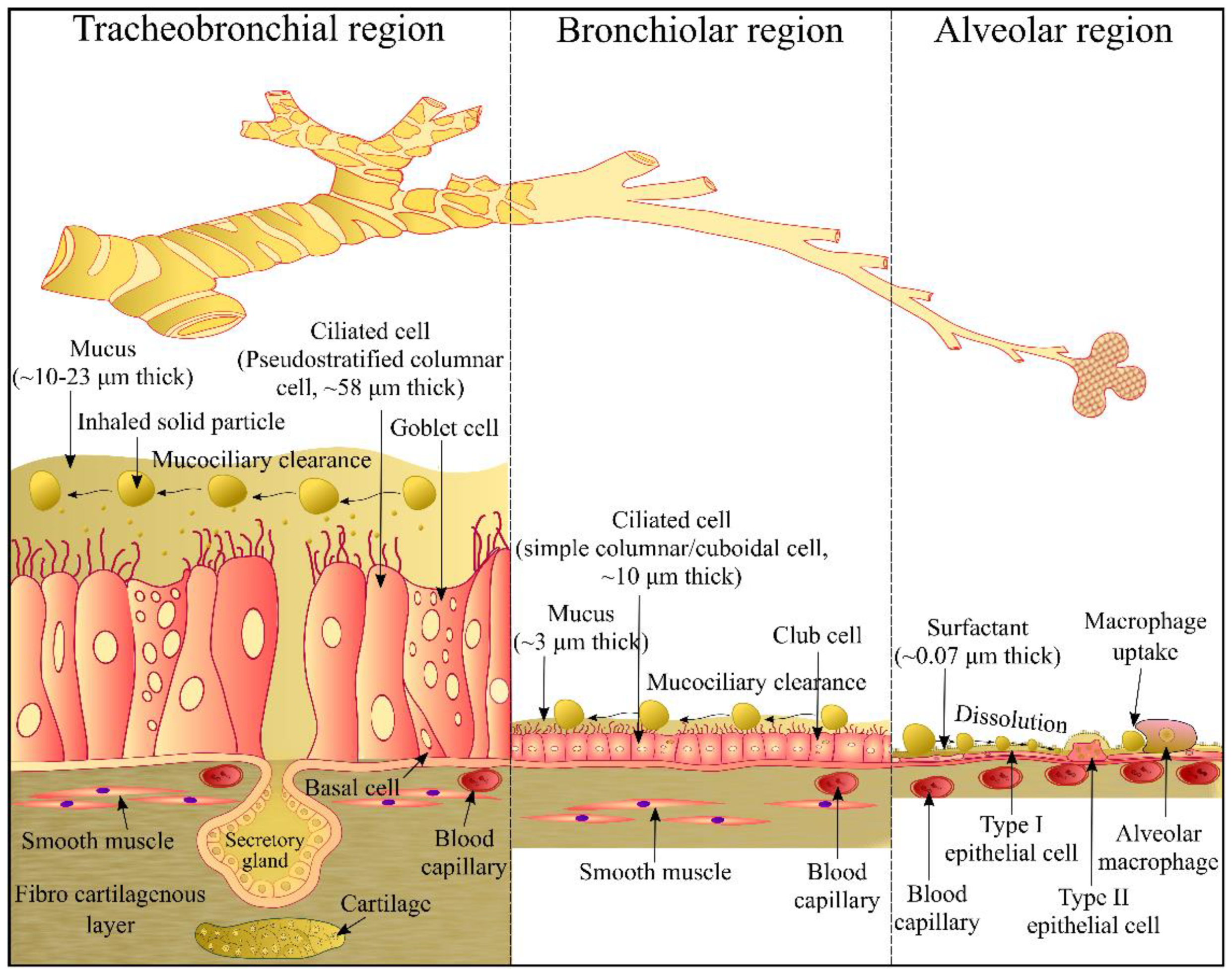
2. Airway Epithelium
3. In Vitro Dissolution Testing of Inhalable Dry Powder Particles
3.1. Hurdles to Develop an In Vitro Dissolution Method for Inhalable Dry Powder Particles
3.2. Fine Particle Dose (FPD) Collection
3.2.1. Andersen Cascade Impactor (ACI)
3.2.2. Next Generation Impactor (NGI)
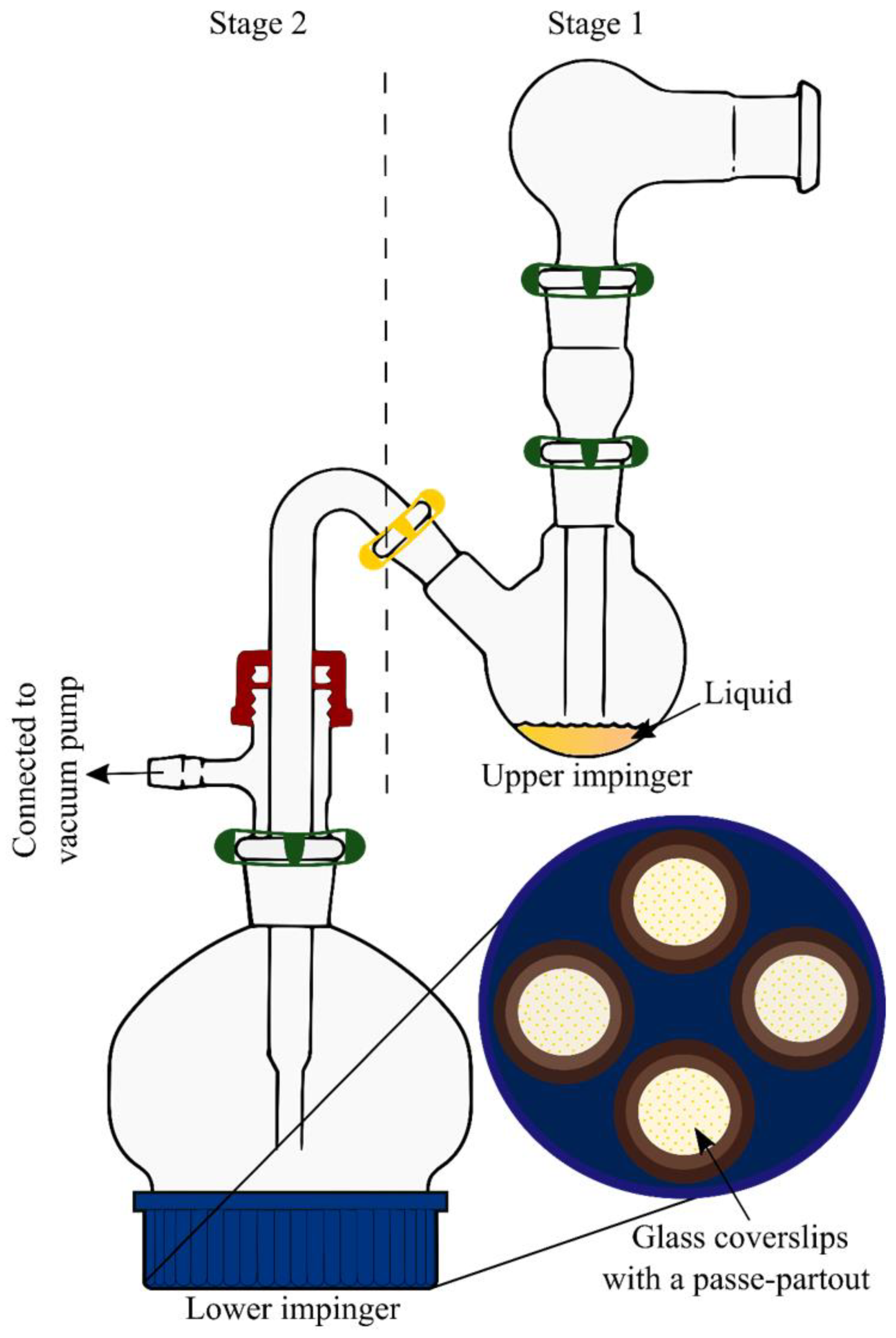
3.2.3. Twin Stage Impinger (TSI)
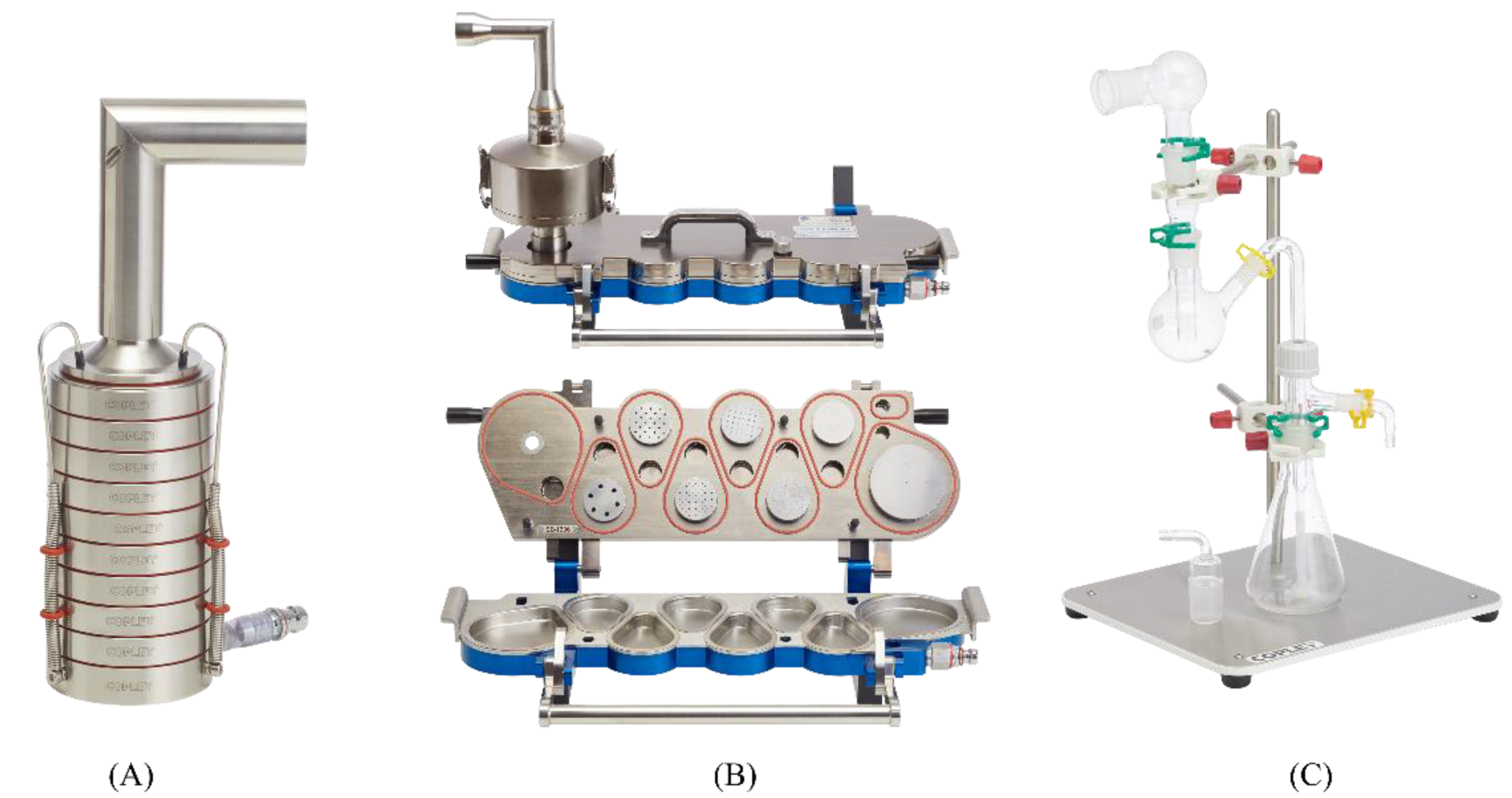
3.2.4. PreciseInhale System
3.3. In Vitro Dissolution Methods
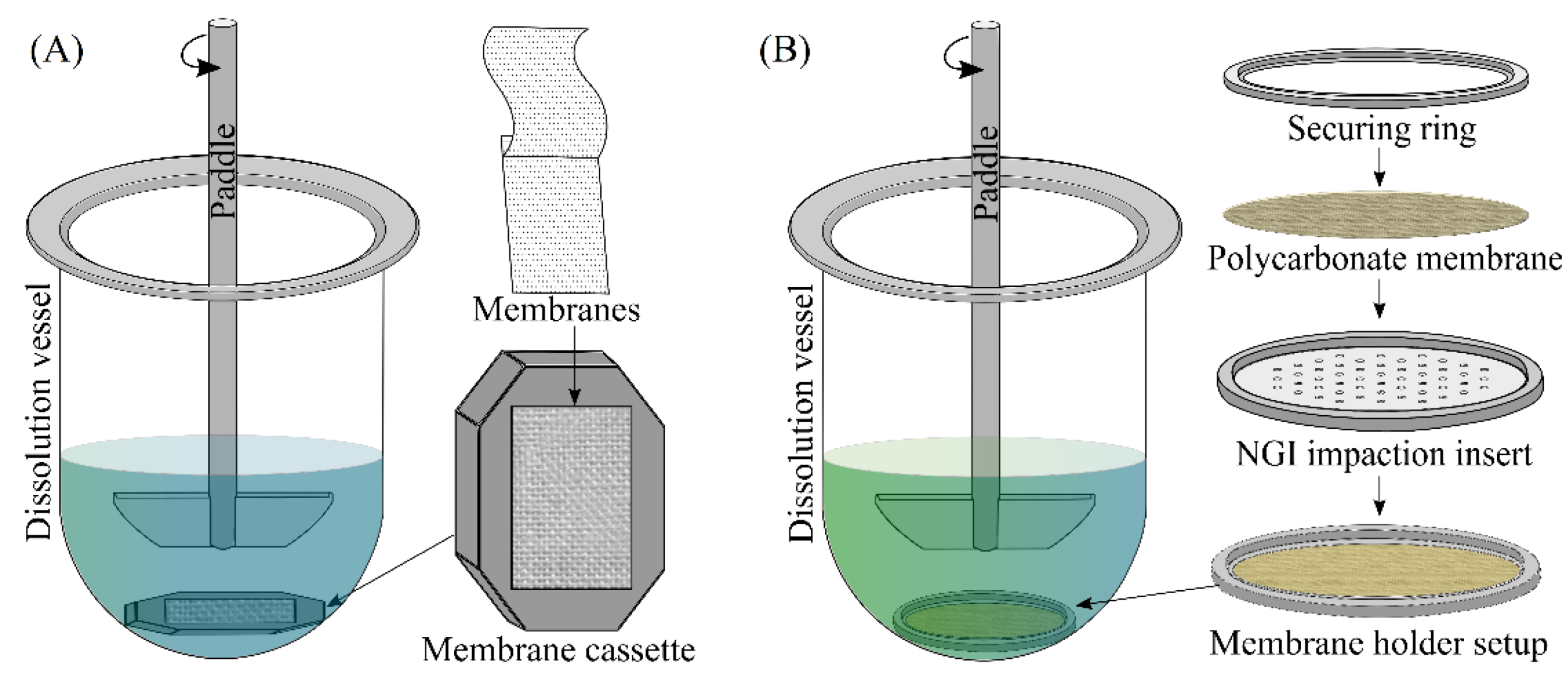
3.3.1. Modified USP 2 (Paddle over Disc) Apparatus
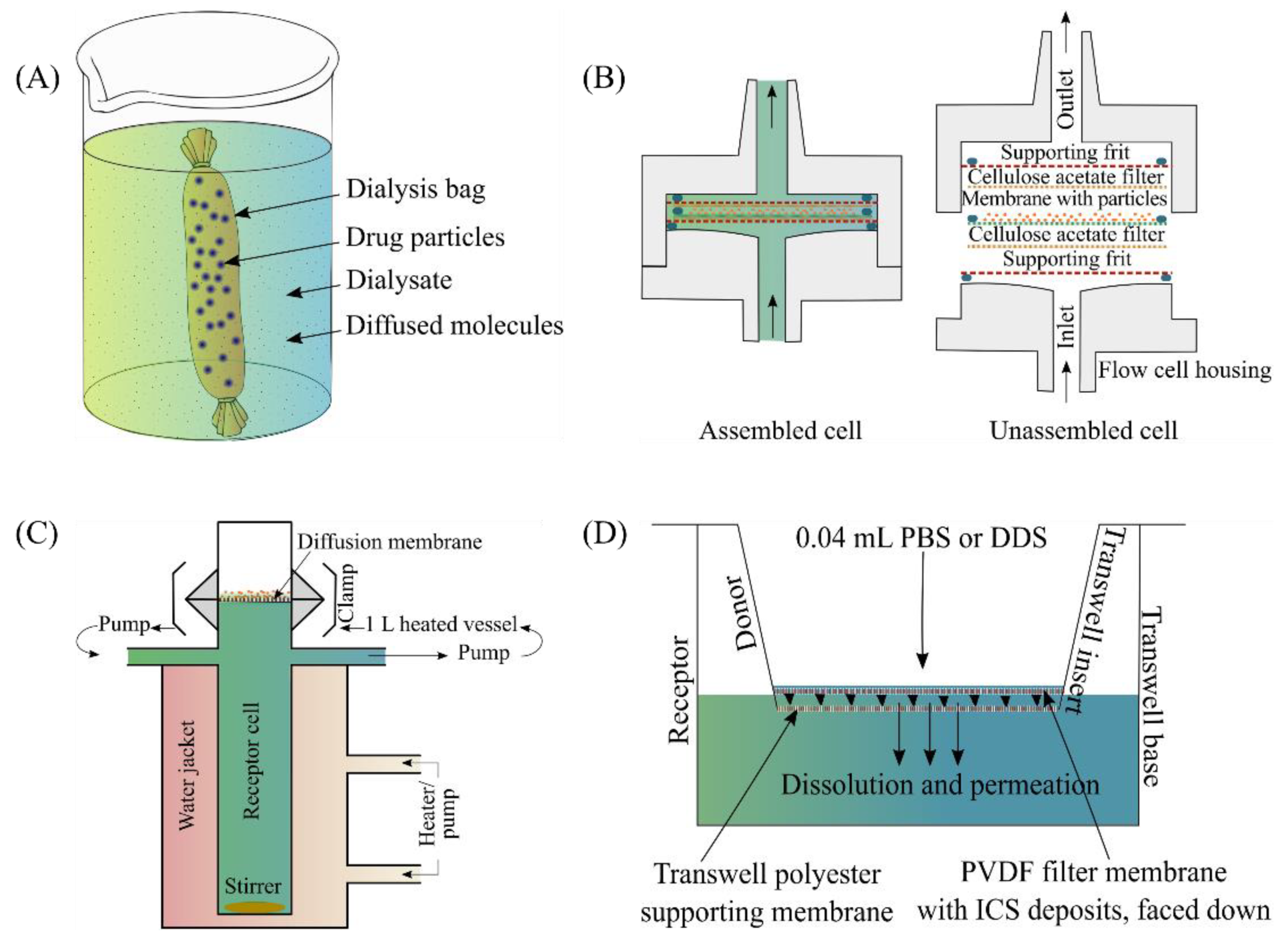
3.3.2. Dialysis Bag
3.3.3. Flow-Through Cell Apparatus
3.3.4. Franz Diffusion Cell
3.3.5. Transwell® System
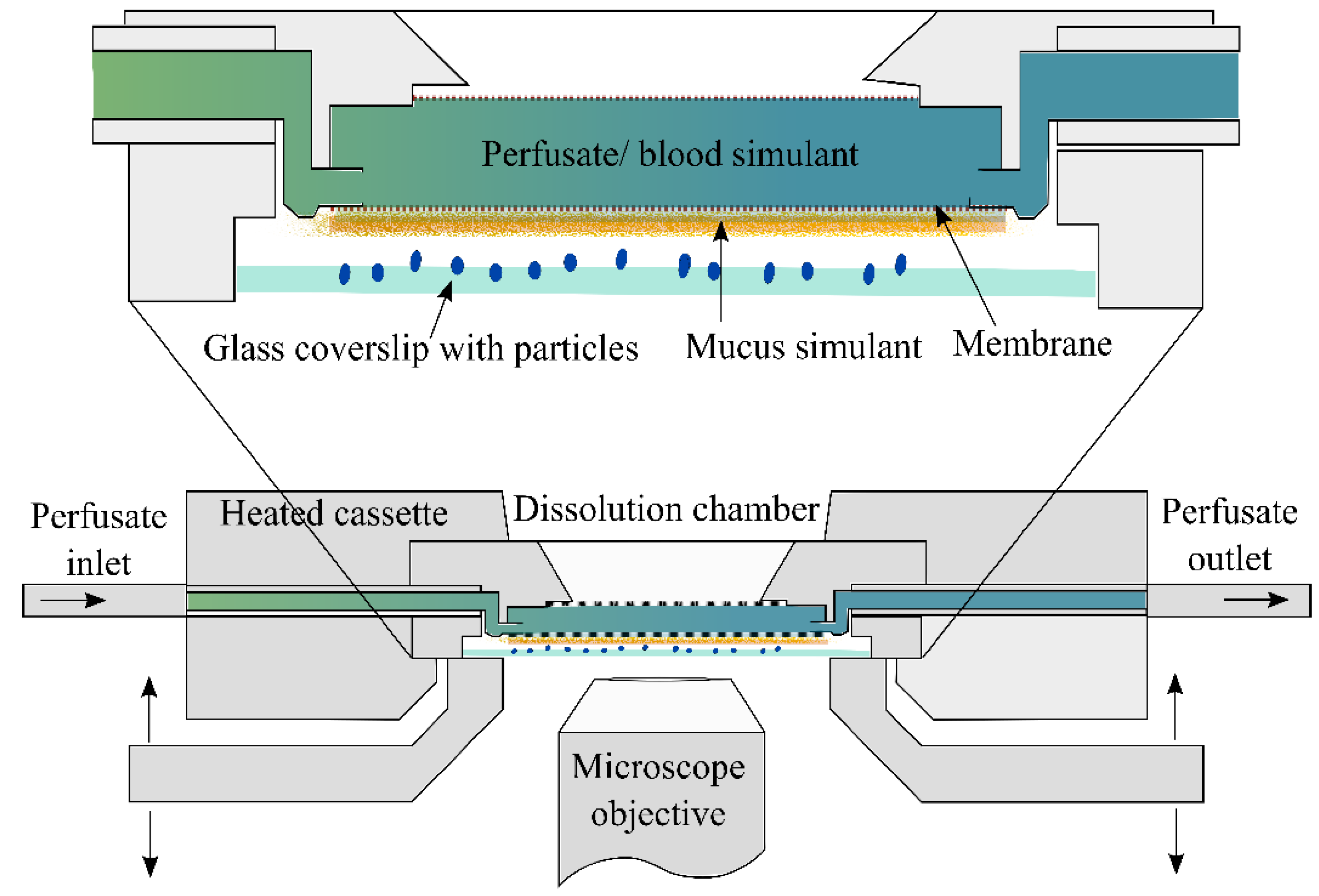
3.3.6. DissolvIt System
3.3.7. Custom Made Flow Perfusion Cell
4. Models for Pulmonary Drug Absorption
5. Future Perspectives
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mehta, P. Dry Powder Inhalers: A Focus on Advancements in Novel Drug Delivery Systems. J. Drug Deliv. 2016, 2016, 8290963. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eedara, B.B.; Alabsi, W.; Encinas-Basurto, D.; Polt, R.; Ledford, J.G.; Mansour, H.M. Inhalation Delivery for the Treatment and Prevention of COVID-19 Infection. Pharmaceutics 2021, 13, 1077. [Google Scholar] [CrossRef] [PubMed]
- Eedara, B.B.; Alabsi, W.; Encinas-Basurto, D.; Polt, R.; Mansour, H.M. Spray-Dried Inhalable Powder Formulations of Therapeutic Proteins and Peptides. AAPS PharmSciTech 2021, 22, 185. [Google Scholar] [CrossRef] [PubMed]
- Alabsi, W.; Eedara, B.B.; Encinas-Basurto, D.; Polt, R.; Mansour, H.M. Nose-to-Brain Delivery of Therapeutic Peptides as Nasal Aerosols. Pharmaceutics 2022, 14, 1870. [Google Scholar] [CrossRef] [PubMed]
- Frijlink, H.W.; De Boer, A.H. Dry powder inhalers for pulmonary drug delivery. Expert Opin. Drug Deliv. 2004, 1, 67–86. [Google Scholar] [CrossRef]
- Muralidharan, P.; Hayes, D.; Mansour, H.M. Dry powder inhalers in COPD, lung inflammation and pulmonary infections. Expert Opin. Drug Deliv. 2015, 12, 947–962. [Google Scholar] [CrossRef] [Green Version]
- Newman, S.P. Inhaler treatment options in COPD. Eur. Respir. Rev. 2005, 14, 102–108. [Google Scholar] [CrossRef] [Green Version]
- Smith, I.J.; Parry-Billings, M. The inhalers of the future? A review of dry powder devices on the market today. Pulm Pharmacol. Ther. 2003, 16, 79–95. [Google Scholar] [CrossRef]
- Svedsater, H.; Dale, P.; Garrill, K.; Walker, R.; Woepse, M.W. Qualitative assessment of attributes and ease of use of the ELLIPTA™ dry powder inhaler for delivery of maintenance therapy for asthma and COPD. BMC Pulm Med. 2013, 13, 72. [Google Scholar] [CrossRef] [Green Version]
- Eedara, B.B.; Alabsi, W.; Encinas-Basurto, D.; Polt, R.; Hayes, D.; Black, S.M.; Mansour, H.M. Pulmonary Drug Delivery. In Organelle and Molecular Targeting; CRC Press: Boca Raton, FL, USA, 2021; pp. 227–278. [Google Scholar]
- El-Sherbiny, I.M.; El-Baz, N.M.; Yacoub, M.H. Inhaled nano- and microparticles for drug delivery. Glob. Cardiol. Sci. Pract. 2015, 2015, 2. [Google Scholar] [CrossRef]
- Newman, S.P. Dry powder inhalers for optimal drug delivery. Expert Opin. Biol. Ther. 2004, 4, 23–33. [Google Scholar] [CrossRef]
- Olsson, B.; Bondesson, E.; Borgström, L.; Edsbäcker, S.; Eirefelt, S.; Ekelund, K.; Gustavsson, L.; Hegelund-Myrbäck, T. Pulmonary drug metabolism, clearance, and absorption. In Controlled Pulmonary Drug Delivery; Springer: Berlin/Heidelberg, Germany, 2011; pp. 21–50. [Google Scholar]
- Patton, J.S.; Brain, J.D.; Davies, L.A.; Fiegel, J.; Gumbleton, M.; Kim, K.-J.; Sakagami, M.; Vanbever, R.; Ehrhardt, C. The Particle has Landed—Characterizing the Fate of Inhaled Pharmaceuticals. J. Aerosol. Med. Pulm. Drug Deliv. 2010, 23, S-71–S-87. [Google Scholar] [CrossRef] [Green Version]
- Eedara, B.B. Slow Dissolving Inhalable Dry Powders for Treatment of Pulmonary Tuberculosis; University of Otago: Dunedin, New Zealand, 2019. [Google Scholar]
- Smyth, H.D.C.; Hickey, A.J. Controlled Pulmonary Drug Delivery, 1st ed.; Springer: New York, NY, USA, 2011. [Google Scholar]
- El-Sherbiny, I.M.; Villanueva, D.G.; Herrera, D.; Smyth, H.D.C. Overcoming Lung Clearance Mechanisms for Controlled Release Drug Delivery. In Controlled Pulmonary Drug Delivery; Smyth, H.D.C., Hickey, A.J., Eds.; Springer: New York, NY, USA, 2011; pp. 101–126. [Google Scholar]
- Eedara, B.B.; Tucker, I.G.; Zujovic, Z.D.; Rades, T.; Price, J.R.; Das, S.C. Crystalline adduct of moxifloxacin with trans-cinnamic acid to reduce the aqueous solubility and dissolution rate for improved residence time in the lungs. Eur. J. Pharm. Sci. 2019, 136, 104961. [Google Scholar] [CrossRef]
- FDAU. Guidance for Industry: Dissolution Testing of Immediate-Release Solid Oral Dosage Forms; Food and Drug Administration: Silver Spring, MD, USA; Center for Drug Evaluation and Research (CDER): Silver Spring, MD, USA, 1997. [Google Scholar]
- Arora, D.; Shah, K.A.; Halquist, M.S.; Sakagami, M. In Vitro Aqueous Fluid-Capacity-Limited Dissolution Testing of Respirable Aerosol Drug Particles Generated from Inhaler Products. Pharm. Res. 2010, 27, 786–795. [Google Scholar] [CrossRef]
- Davies, N.M.; Feddah, M.R. A novel method for assessing dissolution of aerosol inhaler products. Int. J. Pharm. 2003, 255, 175–187. [Google Scholar] [CrossRef]
- Franz, T.J. Percutaneous Absorption. On the Relevance of in Vitro Data. J. Investig. Dermatol. 1975, 64, 190–195. [Google Scholar] [CrossRef] [Green Version]
- Gerde, P.; Malmlöf, M.; Havsborn, L.; Sjöberg, C.-O.; Ewing, P.; Eirefelt, S.; Ekelund, K. DissolvIt: An In Vitro Method for Simulating the Dissolution and Absorption of Inhaled Dry Powder Drugs in the Lungs. ASSAY Drug Dev. Technol. 2017, 15, 77–88. [Google Scholar] [CrossRef] [Green Version]
- Gray, V.; Hickey, A.J.; Balmer, P.; Davies, N.; Dunbar, C.; Foster, T.S.; Olsson, B.L.; Sakagami, M.; Shah, V.P.; Smurthwaite, M.J.; et al. The Inhalation Ad Hoc Advisory Panel for the USP Performance Tests of Inhalation Dosage Forms. Pharmacop. Forum 2008, 34, 1068–1074. [Google Scholar]
- May, S.; Jensen, B.; Wolkenhauer, M.; Schneider, M.; Lehr, C.M. Dissolution Techniques for In Vitro Testing of Dry Powders for Inhalation. Pharm. Res. 2012, 29, 2157–2166. [Google Scholar] [CrossRef]
- Rohrschneider, M.; Bhagwat, S.; Krampe, R.; Michler, V.; Breitkreutz, J.; Hochhaus, G. Evaluation of the Transwell System for Characterization of Dissolution Behavior of Inhalation Drugs: Effects of Membrane and Surfactant. Mol. Pharm. 2015, 12, 2618–2624. [Google Scholar] [CrossRef]
- Salama, R.O.; Traini, D.; Chan, H.-K.; Young, P.M. Preparation and characterisation of controlled release co-spray dried drug–polymer microparticles for inhalation 2: Evaluation of in vitro release profiling methodologies for controlled release respiratory aerosols. Eur. J. Pharm. Biopharm. 2008, 70, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Son, Y.-J.; McConville, J.T. Development of a standardized dissolution test method for inhaled pharmaceutical formulations. Int. J. Pharm. 2009, 382, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Jaafar-Maalej, C.; Andrieu, V.; Elaissari, A.; Fessi, H. Assessment methods of inhaled aerosols: Technical aspects and applications. Expert Opin. Drug Deliv. 2009, 6, 941–959. [Google Scholar] [CrossRef] [PubMed]
- Bastola, R.; Young, P.M.; Das, S.C. Simulation of respiratory tract lining fluid for in vitro dissolution study. Expert Opin. Drug Deliv. 2021, 18, 1091–1100. [Google Scholar] [CrossRef] [PubMed]
- Hastedt, J.E.; Bäckman, P.; Clark, A.R.; Doub, W.; Hickey, A.; Hochhaus, G.; Kuehl, P.J.; Lehr, C.-M.; Mauser, P.; McConville, J.; et al. Scope and relevance of a pulmonary biopharmaceutical classification system AAPS/FDA/USP Workshop 16–17 March 2015 in Baltimore, MD. AAPS Open 2016, 2, 1. [Google Scholar] [CrossRef] [Green Version]
- Ochs, M.; Weibel, E.R. Functional design of the human lung for gas exchange. In Fishman’s Pulmonary Diseases and Disorders, 5th ed.; Grippi, M.A., Elias, J.A., Fishman, J.A., Kotloff, R.M., Pack, A.L., Senior, R.M., Siegel, M.D., Eds.; McGraw Hill: New York, NY, USA, 2015; Volume 1, p. 7. [Google Scholar]
- Haghi, M.; Ong, H.X.; Traini, D.; Young, P. Across the pulmonary epithelial barrier: Integration of physicochemical properties and human cell models to study pulmonary drug formulations. Pharmacol. Ther. 2014, 144, 235–252. [Google Scholar] [CrossRef]
- Zhang, J.; Wu, L.; Chan, H.-K.; Watanabe, W. Formation, characterization, and fate of inhaled drug nanoparticles. Adv. Drug Deliv. Rev. 2011, 63, 441–455. [Google Scholar] [CrossRef]
- Eedara, B.B.; Rangnekar, B.; Doyle, C.; Cavallaro, A.; Das, S.C. The influence of surface active l-leucine and 1,2-dipalmitoyl-sn-glycero-3-phosphatidylcholine (DPPC) in the improvement of aerosolization of pyrazinamide and moxifloxacin co-spray dried powders. Int. J. Pharm. 2018, 542, 72–81. [Google Scholar] [CrossRef]
- Eedara, B.B.; Rangnekar, B.; Sinha, S.; Doyle, C.; Cavallaro, A.; Das, S.C. Development and characterization of high payload combination dry powders of anti-tubercular drugs for treating pulmonary tuberculosis. Eur. J. Pharm. Sci. 2018, 118, 216–226. [Google Scholar] [CrossRef]
- Eedara, B.B.; Tucker, I.G.; Das, S.C. Phospholipid-based pyrazinamide spray-dried inhalable powders for treating tuberculosis. Int. J. Pharm. 2016, 506, 174–183. [Google Scholar] [CrossRef]
- Rangnekar, B.; Momin, M.A.M.; Eedara, B.B.; Sinha, S.; Das, S.C. Bedaquiline containing triple combination powder for inhalation to treat drug-resistant tuberculosis. Int. J. Pharm. 2019, 570, 118689. [Google Scholar] [CrossRef]
- Fröhlich, E. Toxicity of orally inhaled drug formulations at the alveolar barrier: Parameters for initial biological screening. Drug Deliv. 2017, 24, 891–905. [Google Scholar] [CrossRef] [Green Version]
- Gerde, P.; Scholander, P. A mathematical model of the penetration of polycyclic aromatic hydrocarbons through the bronchial lining layer. Environ. Res. 1987, 44, 321–334. [Google Scholar] [CrossRef]
- Patton, J.S.; Byron, P.R. Inhaling medicines: Delivering drugs to the body through the lungs. Nat. Rev. Drug Discov. 2007, 6, 67–74. [Google Scholar] [CrossRef]
- Parra, E.; Pérez-Gil, J. Composition, structure and mechanical properties define performance of pulmonary surfactant membranes and films. Chem. Phys. Lipids 2015, 185, 153–175. [Google Scholar] [CrossRef]
- Mason, R.J.; Dobbs, L.G. Alveolar Epithelium and Pulmonary Surfactant. In Murray and Nadel’s Textbook of Respiratory Medicine; Broaddus, V.C., Mason, R.J., Ernst, J.D., King, T.E., Lazarus, S.C., Murray, J.F., Nadel, J.A., Slutsky, A.S., Gotway, M.B., Eds.; Elsevier: Amsterdam, The Netherlands, 2016; pp. 134–149.e5. [Google Scholar]
- Carvalho, T.C.; Peters, J.I.; Williams, R.O. Influence of particle size on regional lung deposition—What evidence is there? Int. J. Pharm. 2011, 406, 1–10. [Google Scholar] [CrossRef]
- Cipolla, D.; Shekunov, B.; Blanchard, J.; Hickey, A. Lipid-based carriers for pulmonary products: Preclinical development and case studies in humans. Adv. Drug Deliv. Rev. 2014, 75, 53–80. [Google Scholar] [CrossRef]
- Driving Results in Inhaler Testing [Brochure]. 2020. Available online: https://www.copleyscientific.com/wp-content/uploads/2020/02/Copley-Inhaler-Testing-Brochure-LowRes-0720.pdf (accessed on 21 September 2022).
- May, S.; Jensen, B.; Weiler, C.; Wolkenhauer, M.; Schneider, M.; Lehr, C.-M. Dissolution Testing of Powders for Inhalation: Influence of Particle Deposition and Modeling of Dissolution Profiles. Pharm. Res. 2014, 31, 3211–3224. [Google Scholar] [CrossRef]
- May, S.; Kind, S.; Jensen, B.; Wolkenhauer, M.; Schneider, M.; Lehr, C.-M. Miniature in vitro dissolution testing of powders for inhalation. Dissolution Technol. 2015, 22, 40–51. [Google Scholar] [CrossRef]
- Tay, J.Y.S.; Liew, C.V.; Heng, P.W.S. Dissolution of fine particle fraction from truncated Anderson cascade impactor with an enhancer cell. Int. J. Pharm. 2018, 545, 45–50. [Google Scholar] [CrossRef]
- Son, Y.J.; Horng, M.; Copley, M.; McConville, J.T. Optimization of an in vitro dissolution test method for inhalation formulations. Dissolution Technol. 2010, 17, 6–13. [Google Scholar] [CrossRef]
- Son, Y.-J.; McConville, J.T. Preparation of sustained release rifampicin microparticles for inhalation. J. Pharm. Pharmacol. 2012, 64, 1291–1302. [Google Scholar] [CrossRef] [PubMed]
- Duret, C.; Wauthoz, N.; Sebti, T.; Vanderbist, F.; Amighi, K. Solid dispersions of itraconazole for inhalation with enhanced dissolution, solubility and dispersion properties. Int. J. Pharm. 2012, 428, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Pilcer, G.; Rosière, R.; Traina, K.; Sebti, T.; Vanderbist, F.; Amighi, K. New Co-Spray-Dried Tobramycin Nanoparticles-Clarithromycin Inhaled Powder Systems for Lung Infection Therapy in Cystic Fibrosis Patients. J. Pharm. Sci. 2013, 102, 1836–1846. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.G.Y.; Chan, H.-K.; Prestidge, C.A.; Denman, J.A.; Young, P.M.; Traini, D. A novel dry powder inhalable formulation incorporating three first-line anti-tubercular antibiotics. Eur. J. Pharm. Biopharm. 2013, 83, 285–292. [Google Scholar] [CrossRef]
- Grainger, C.I.; Greenwell, L.L.; Martin, G.P.; Forbes, B. The permeability of large molecular weight solutes following particle delivery to air-interfaced cells that model the respiratory mucosa. Eur. J. Pharm. Biopharm. 2009, 71, 318–324. [Google Scholar] [CrossRef]
- Grainger, C.I.; Saunders, M.; Buttini, F.; Telford, R.; Merolla, L.L.; Martin, G.P.; Jones, S.A.; Forbes, B. Critical Characteristics for Corticosteroid Solution Metered Dose Inhaler Bioequivalence. Mol. Pharm. 2012, 9, 563–569. [Google Scholar] [CrossRef]
- Haghi, M.; Traini, D.; Bebawy, M.; Young, P.M. Deposition, Diffusion and Transport Mechanism of Dry Powder Microparticulate Salbutamol, at the Respiratory Epithelia. Mol. Pharm. 2012, 9, 1717–1726. [Google Scholar] [CrossRef]
- Eedara, B.B.; Tucker, I.G.; Das, S.C. In vitro dissolution testing of respirable size anti-tubercular drug particles using a small volume dissolution apparatus. Int. J. Pharm. 2019, 559, 235–244. [Google Scholar] [CrossRef]
- Börjel, M.; Sadler, R.; Gerde, P. (Eds.) The dissolvIt: An in vitro evaluation of the dissolution and absorption of three inhaled dry powder drugs in the lung. In Respiratory Drug Delivery to the Lungs Conference, Poster Stockholm; Karolinska Institutet: Stockholm, Sweden, 2014. [Google Scholar]
- British Pharmacopoeia; TSO: London, UK, 2018.
- Son, Y.-J.; McConville, J.T. A new respirable form of rifampicin. Eur. J. Pharm. Biopharm. 2011, 78, 366–376. [Google Scholar] [CrossRef]
- Eedara, B.B.; Tucker, I.G.; Das, S.C. A STELLA simulation model for in vitro dissolution testing of respirable size particles. Sci. Rep. 2019, 9, 18522. [Google Scholar] [CrossRef]
- Al ayoub, Y.; Buzgeia, A.; Almousawi, G.; Mazhar, H.R.A.; Alzouebi, B.; Gopalan, R.C.; Assi, K.H. In-Vitro In-Vivo Correlation (IVIVC) of Inhaled Products Using Twin Stage Impinger. J. Pharm. Sci. 2022, 111, 395–402. [Google Scholar] [CrossRef]
- Gerde, P.; Ewing, P.; Låstbom, L.; Ryrfeldt, Å.; Waher, J.; Lidén, G. A Novel Method to Aerosolize Powder for Short Inhalation Exposures at High Concentrations: Isolated Rat Lungs Exposed to Respirable Diesel Soot. Inhal. Toxicol. 2004, 16, 45–52. [Google Scholar] [CrossRef]
- Jaspart, S.; Bertholet, P.; Piel, G.; Dogné, J.-M.; Delattre, L.; Evrard, B. Solid lipid microparticles as a sustained release system for pulmonary drug delivery. Eur. J. Pharm. Biopharm. 2007, 65, 47–56. [Google Scholar] [CrossRef]
- Ortiz, M.; Jornada, D.S.; Pohlmann, A.R.; Guterres, S.S. Development of Novel Chitosan Microcapsules for Pulmonary Delivery of Dapsone: Characterization, Aerosol Performance, and In Vivo Toxicity Evaluation. AAPS PharmSciTech 2015, 16, 1033–1040. [Google Scholar] [CrossRef] [Green Version]
- Asada, M.; Takahashi, H.; Okamoto, H.; Tanino, H.; Danjo, K. Theophylline particle design using chitosan by the spray drying. Int. J. Pharm. 2004, 270, 167–174. [Google Scholar] [CrossRef]
- Huang, Y.C.; Yeh, M.K.; Cheng, S.N.; Chiang, C.H. The characteristics of betamethasone-loaded chitosan microparticles by spray-drying method. J. Microencapsul. 2003, 20, 459–472. [Google Scholar] [CrossRef]
- Learoyd, T.P.; Burrows, J.L.; French, E.; Seville, P.C. Chitosan-based spray-dried respirable powders for sustained delivery of terbutaline sulfate. Eur. J. Pharm. Biopharm. 2008, 68, 224–234. [Google Scholar] [CrossRef]
- Depreter, F.; Burniat, A.; Blocklet, D.; Lacroix, S.; Cnop, M.; Fery, F.; Van Aelst, N.; Pilcer, G.; Deleers, M.; Goldman, S.; et al. Comparative pharmacoscintigraphic and pharmacokinetic evaluation of two new formulations of inhaled insulin in type 1 diabetic patients. Eur. J. Pharm. Biopharm. 2012, 80, 4–13. [Google Scholar] [CrossRef]
- Parikh, R.; Dalwadi, S. Preparation and characterization of controlled release poly-ε-caprolactone microparticles of isoniazid for drug delivery through pulmonary route. Powder Technol. 2014, 264, 158–165. [Google Scholar] [CrossRef]
- Arora, S.; Haghi, M.; Loo, C.-Y.; Traini, D.; Young, P.M.; Jain, S. Development of an Inhaled Controlled Release Voriconazole Dry Powder Formulation for the Treatment of Respiratory Fungal Infection. Mol. Pharm. 2015, 12, 2001–2009. [Google Scholar] [CrossRef] [PubMed]
- Pai, R.V.; Jain, R.R.; Bannalikar, A.S.; Menon, M.D. Development and Evaluation of Chitosan Microparticles Based Dry Powder Inhalation Formulations of Rifampicin and Rifabutin. J. Aerosol Med. Pulm. Drug Deliv. 2016, 29, 179–195. [Google Scholar] [CrossRef] [PubMed]
- Maretti, E.; Rustichelli, C.; Romagnoli, M.; Balducci, A.G.; Buttini, F.; Sacchetti, F.; Leo, E.; Iannuccelli, V. Solid Lipid Nanoparticle assemblies (SLNas) for an anti-TB inhalation treatment—A Design of Experiments approach to investigate the influence of pre-freezing conditions on the powder respirability. Int. J. Pharm. 2016, 511, 669–679. [Google Scholar] [CrossRef] [PubMed]
- Kumaresan, C.; Sathishkumar, K. Development of an Inhaled Sustained Release Dry Powder Formulation of Salbutamol Sulphate, an Antiasthmatic Drug. Indian J. Pharm. Sci. 2016, 78, 136–142. [Google Scholar] [PubMed] [Green Version]
- Taylor, M.K.; Hickey, A.J.; VanOort, M. Manufacture, Characterization, and Pharmacodynamic Evaluation of Engineered Ipratropium Bromide Particles. Pharm. Dev. Technol. 2006, 11, 321–336. [Google Scholar] [CrossRef]
- Cook, R.O.; Pannu, R.K.; Kellaway, I.W. Novel sustained release microspheres for pulmonary drug delivery. J. Control. Release 2005, 104, 79–90. [Google Scholar] [CrossRef]
- Adi, H.; Young, P.M.; Chan, H.-K.; Salama, R.; Traini, D. Controlled release antibiotics for dry powder lung delivery. Drug Dev. Ind. Pharm. 2010, 36, 119–126. [Google Scholar] [CrossRef]
- Möbus, K.; Siepmann, J.; Bodmeier, R. Zinc–alginate microparticles for controlled pulmonary delivery of proteins prepared by spray-drying. Eur. J. Pharm. Biopharm. 2012, 81, 121–130. [Google Scholar] [CrossRef]
- Scalia, S.; Salama, R.; Young, P.; Traini, D. Preparation and in vitro evaluation of salbutamol-loaded lipid microparticles for sustained release pulmonary therapy. J. Microencapsul. 2012, 29, 225–233. [Google Scholar] [CrossRef]
- Buttini, F.; Miozzi, M.; Balducci, A.G.; Royall, P.G.; Brambilla, G.; Colombo, P.; Bettini, R.; Forbes, B. Differences in physical chemistry and dissolution rate of solid particle aerosols from solution pressurised inhalers. Int. J. Pharm. 2014, 465, 42–51. [Google Scholar] [CrossRef]
- Balducci, A.G.; Steckel, H.; Guarneri, F.; Rossi, A.; Colombo, G.; Sonvico, F.; Cordts, E.; Bettini, R.; Colombo, P.; Buttini, F. High shear mixing of lactose and salmeterol xinafoate dry powder blends: Biopharmaceutic and aerodynamic performances. J. Drug Deliv. Sci. Technol. 2015, 30, 443–449. [Google Scholar] [CrossRef]
- Langenbucher, F.; Benz, D.; Kürth, W.; Möller, H.; Otz, M. Standardized flow-cell method as an alternative to existing pharmacopoeial dissolution testing. Pharm. Ind. 1989, 51, 1276–1281. [Google Scholar]
- Fotaki, N. Flow-through cell apparatus (USP apparatus 4): Operation and features. Dissolut. Technol. 2011, 18, 46–49. [Google Scholar] [CrossRef]
- Kanapilly, G.M.; Raabe, O.G.; Goh, C.H.T.; Chimenti, R.A. Measurement of in Vitro Dissolution of Aerosol Particles for Comparison to in Vivo Dissolution in the Lower Respiratory Tract after Inhalation. Health Phys. 1973, 24, 497–507. [Google Scholar] [CrossRef]
- Riley, T.C.D.; Arp, J.; Casazzza, A.; Colombani, A.; Cooper, A.; Dey, M.; Maas, J.; Mitchell, J.; Reiners, M.; Sigari, N.; et al. Challenges with developing in vitro dissolution tests for orally inhaled products (OIPs). Aaps Pharmscitech 2012, 13, 978–989. [Google Scholar] [CrossRef] [Green Version]
- Hassoun, M.; Malmlöf, M.; Scheibelhofer, O.; Kumar, A.; Bansal, S.; Selg, E.; Nowenwik, M.; Gerde, P.; Radivojev, S.; Paudel, A.; et al. Use of PBPK modeling to evaluate the performance of dissolv it, a biorelevant dissolution assay for orally inhaled drug products. Mol. Pharm. 2019, 16, 1245–1254. [Google Scholar] [CrossRef] [Green Version]
- Saha, T.; Sinha, S.; Harfoot, R.; Quiñones-Mateu, M.E.; Das, S.C. Manipulation of Spray-Drying Conditions to Develop an Inhalable Ivermectin Dry Powder. Pharmaceutics 2022, 14, 1432. [Google Scholar] [CrossRef]
- Rojewska, M.; Smułek, W.; Kaczorek, E.; Prochaska, K. Langmuir Monolayer Techniques for the Investigation of Model Bacterial Membranes and Antibiotic Biodegradation Mechanisms. Membranes 2021, 11, 707. [Google Scholar] [CrossRef]
- Cingolani, E.; Alqahtani, S.; Sadler, R.C.; Prime, D.; Stolnik, S.; Bosquillon, C. In vitro investigation on the impact of airway mucus on drug dissolution and absorption at the air-epithelium interface in the lungs. Eur. J. Pharm. Biopharm. 2019, 141, 210–220. [Google Scholar] [CrossRef]
- Eriksson, J.; Thörn, H.; Sjögren, E.; Holmstén, L.; Rubin, K.; Lennernäs, H. Pulmonary dissolution of poorly soluble compounds studied in an ex vivo rat lung model. Mol. Pharm. 2019, 16, 3053–3064. [Google Scholar] [CrossRef]
- Khadka, P.; Sinha, S.; Tucker, I.G.; Dummer, J.; Hill, P.C.; Katare, R.; Das, S.C. Pharmacokinetics of rifampicin after repeated intra-tracheal administration of amorphous and crystalline powder formulations to Sprague Dawley rats. Eur. J. Pharm. Biopharm. 2021, 162, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Garcia Contreras, L.; Sung, J.; Ibrahim, M.; Elbert, K.; Edwards, D.; Hickey, A. Pharmacokinetics of inhaled rifampicin porous particles for tuberculosis treatment: Insight into rifampicin absorption from the lungs of guinea pigs. Mol. Pharm. 2015, 12, 2642–2650. [Google Scholar] [CrossRef] [PubMed]
- Bitonti, A.J.; Dumont, J.A.; Low, S.C.; Peters, R.T.; Kropp, K.E.; Palombella, V.J.; Stattel, J.M.; Lu, Y.; Tan, C.A.; Song, J.J.; et al. Pulmonary delivery of an erythropoietin Fc fusion protein in non-human primates through an immunoglobulin transport pathway. Proc. Natl. Acad. Sci. USA 2004, 101, 9763–9768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ratjen, F.; Rietschel, E.; Kasel, D.; Schwiertz, R.; Starke, K.; Beier, H.; Van Koningsbruggen, S.; Grasemann, H. Pharmacokinetics of inhaled colistin in patients with cystic fibrosis. J. Antimicrob. Chemother. 2006, 57, 306–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakagami, M. In vitro, ex vivo and in vivo methods of lung absorption for inhaled drugs. Adv. Drug Deliv. Rev. 2020, 161–162, 63–74. [Google Scholar] [CrossRef]
- Sakagami, M. In vivo, in vitro and ex vivo models to assess pulmonary absorption and disposition of inhaled therapeutics for systemic delivery. Adv. Drug Deliv. Rev. 2006, 58, 1030–1060. [Google Scholar] [CrossRef]
- Nahar, K.; Gupta, N.; Gauvin, R.; Absar, S.; Patel, B.; Gupta, V.; Khademhosseini, A.; Ahsan, F. In vitro, in vivo and ex vivo models for studying particle deposition and drug absorption of inhaled pharmaceuticals. Eur. J. Pharm. Sci. 2013, 49, 805–818. [Google Scholar] [CrossRef]
- Radivojev, S.; Zellnitz, S.; Paudel, A.; Fröhlich, E. Searching for physiologically relevant in vitro dissolution techniques for orally inhaled drugs. Int. J. Pharm. 2019, 556, 45–56. [Google Scholar] [CrossRef]
- Ibrahim, B.M.; Park, S.; Han, B.; Yeo, Y. A strategy to deliver genes to cystic fibrosis lungs: A battle with environment. J. Control. Release 2011, 155, 289–295. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Apparatus | Drugs | Inhaler and Loading Dose | Collection Method | Ref. |
|---|---|---|---|---|
| Andersen Cascade Impactor (ACI) | Budesonide (BD), Fluticasone propionate (FP), Triamcinolone acetonide (TA) | Pulmicort Turbuhaler, BD, 200 µg Flixotide Accuhaler®, FP, 250 µg Azmacort®, TA, 200 µg | Collected onto a GF filter at the connection point of the induction port and inlet of ACI | [21] |
| Flunisolide (FN), TA, BD, FP, Beclomethasone dipropionate (BDP) | Aerobid®, FN, 250–2500 µg Azmacort®, TA, 200–2000 µg Pulmicort Turbuhaler®, BD, 50–500 µg Flovent® HFA and Diskus, FP, 150–1250 µg Vanceril® and QVAR® (BDP, 350–700 µg) | Collected onto 6 PVDF membranes placed at the stage 4 of ACI operated at an air flow of 28.3 L/min | [20] | |
| BD, Fenoterol HBr (FNH), Substance A dibromide (SAD), Substance A crystalline base (SAC), Substance A amorphous base (SAA) | Micronized BD, FN, SAD and SAC; spray dried SA (SAA) HandiHaler® (1 mg (BD, SA) 10 mg (FN)) | Collected onto the RC membrane (pore size 0.45 µm) at standard USP conditions (4 kPa, 4 L) | [25] | |
| BD, SAD, SAC, SAA | Micronized BD, SAD and SAC; spray dried SA (SAA) HandiHaler® (0.5 to 4 mg) | Collected onto the RC membrane at standard USP conditions (4 kPa, 4 L) using ACI with stage extension between stage 1 and filter stage, and modified/standard filter stage | [47] | |
| BD, SAD, SAC, SAA | Micronized BD, SAD and SAC; spray dried SA (SAA) HandiHaler® (0.5 to 4 mg) | Collected onto the PE, PC, IPC and RC membranes at standard USP conditions (4 kPa, 4 L) using ACI with stage extension between stage 1 and F, and modified/standard filter stage | [48] | |
| BD, Ciclesonide (CIC), FP | Symbicort® (BD) Alvesco® (CIC) Flixotide® (FP), (5 doses (BD-80 µg/dose, CIC-60 µg/dose and FP-110 µg/dose)) | Collected onto the 24 mm GF filters or Fisherbrand Q8 filter papers at the stage 4 of ACI at an air flow of 28.3 L/min | [26] | |
| Salbutamol sulfate (SS), FP, Salmeterol xinafoate (SX) | Micronized SS blend, Rotahaler® (6–10 doses (2% w/w SS blend, 30 mg/dose) Seretide® 50/100 Diskus® (FP and SX, 50 µg SX and 100 µg FP/dose)) | Collected onto an adhesive tape using the truncated ACI with a PTFE funnel and a collection plate at the filter stage (Stage F) operated at a pressure drop of 4 kPa at 60 L/min air flow rate | [49] | |
| Next Generation Impactor (NGI) | Hydrocortisone (HC) | Bulk HC (50 mg) micronized HC blend Aerolizer® (150 mg micronized HC blend, ~10 mg of HC) | Collected onto the PC (0.05 µm) and CA (MWCO 3500, 12,000) at each dose plate of NGI | [28] |
| Albuterol sulfate (AS), BD | Ventolin HFA® (AS,15–20 doses) Pulmicort Flexhaler® (BD, 1–10 doses) | Collected onto the impaction inserts at stage 2–5 of NGI at 30 L/min (AS) or 60 L/min (BD) air flow rate | [50] | |
| Rifampicin (RIF) | Microparticles; Aerolizer® (7 mg to 20 mg) | Collected onto the impaction insert at stage 3 of NGI operated at 60 L/min air flow rate for 4 s | [51] | |
| Itraconazole (ITZ) | Spray dried solid dispersions, Axahaler® | Collected onto the impaction inserts at each dose plate of NGI operated at 60 L/min air flow rate | [52] | |
| Tobramycin Clarithromycin | Nanoparticulate spray dried powders (TCn2), Physical blend (TCb), Axahaler® | Collected onto the impaction insert at stage 3 of NGI operated at 100 L/min air flow rate | [53] | |
| Pyrazinamide (PYR), RIF, Isoniazid (IZD) | Spray dried powders, Aerolizer® (Two 20 mg doses) | Collected onto a NC membrane at stage 3 of NGI operated at 100 L/min air flow rate | [54] | |
| FP | Flixotide® (FP, 5 doses of 110 µg/dose) | Collected onto the 24 mm Fisherbrand Q8 filter papers at stage 2 and 4 of NGI | [26] | |
| Twin Stage Impinger (TSI) | Dextrans labelled with fluorescein isothiocyanate (FITC-dex; 4, 10, 20, 40 and 70 kDa) | A custom-made glass dry powder insufflator (5 mg) | Collected onto the Calu-3 bronchial epithelial cells in a Transwell® insert using TSI at 60 L/min air flow rate for 5 s | [55] |
| BDP | QVAR® and Sanasthmax® (100–250 μg/dose; 1.2 ± 0.12 mg deposited) | Collected on a NC membrane (0.45 μm) at stage 2 of a modified TSI | [56] | |
| Salbutamol base (SB), SS | Micronized SB and SS (5 mg) | Collected onto a Transwell® PE insert (0.4 μm) using modified TSI at 60 L/min air flow rate for 4 s | [57] | |
| Moxifloxacin Ethionamide | Aerolizer® device (20 mg) | Collected on a glass coverslip at 60 L/min air flow rate for 4 s | [58] | |
| PreciseInhale system | BD, FP | Micronized powders (2.5 mg) | Collected onto the glass coverslips of 13 mm diameter at 1.2 L/min air flow rate | [23,59] |
| Dissolution Apparatus | Membrane (Pore Size, μm or MWCO, kDa) | Dissolution Medium and Conditions | Ref. |
|---|---|---|---|
| USP 1 (basket) apparatus | Glass fiber filters, GF/F grade | PBS, pH 7.4, basket rotation- 150 rpm | [65] |
| - | PBS, pH 7.4, 900 mL, basket rotation- 100 rpm | [66] | |
| USP 2 [paddle) apparatus | - | Water, 300 mL, paddle rotation- 50 rpm | [68] |
| - | Buffer, pH 1.2 or pH 6.8, 1000 mL, paddle rotation- 100 rpm | [67] | |
| - | PBS, pH 6.8, 1000 mL, paddle rotation- 50 rpm | [69] | |
| Modified USP 2 (paddle over disc) apparatus | - | PBS, pH 7.4, 1000 mL, paddle rotation- 50 rpm | [27] |
| Polycarbonate membranes (0.05 and 1 μm) Cellulose acetate membranes (3.5, 12 kDa) | SLF and modified SLF with DPPC (0.02% w/v), pH 7.4, 100 mL, paddle rotation- 50 rpm | [28] | |
| Polycarbonate membrane (0.05 μm) | SLF, 0.2 M PB, pH 7.4, PBS, modified PBS with DPPC, tween 80 (0.02 and 0.2% w/v), pH 7.4, 300 mL, paddle rotation- 50, 75, 100 rpm | [50] | |
| Polycarbonate membrane (0.05 μm) | PBS, pH 7.4 or 0.2 M citrate buffer with ascorbic acid (0.02% w/v), pH 5.2, 300 mL, paddle rotation- 75 rpm | [51] | |
| Polycarbonate membrane (0.4 μm) | Water with SLS (0.3%), buffer, pH 1.2, 300 mL, paddle rotation- 75 rpm | [52] | |
| Regenerated cellulose membrane (0.45 μm) | PBS, pH 7.4, 1000 mL, paddle rotation- 50, 100, and 140 rpm | [25,47] | |
| Polycarbonate membrane (0.4 μm) | PBS, pH 7.4, 300 mL, paddle rotation- 75 rpm | [53,70] | |
| Dialysis membrane (>900 kDa) | Gamble’s solution, pH 7.4 and alveolar lung fluid, pH 4.5, 900 mL, paddle rotation- 150 rpm | [71] | |
| - | Modified SLF with tween 80 (0.2% v/v), 50 mL; paddle rotation- 50 rpm | [49] | |
| Dialysis bag | Dialysis membrane (12 kDa) | 10 mM PBS with tween 80 (0.1% v/v), pH 7.4, 20 mL, rotation- 900 rpm | [72] |
| Dialysis membrane (12–14 kDa) | SLF, pH 7.4, 50 mL | [73] | |
| Dialysis membrane (12–14 kDa) | SLF, pH 7.4, 30 mL, | [74] | |
| Dialysis membrane (14 kDa) | PBS, pH 7.4, 250 mL, rotation- 100 rpm | [75] | |
| Flow-through cell system | Cellulose acetate membrane (0.45 μm) | SLF, modified SLF with DPPC (0.02% w/v), flow rate- 0.7 mL/min, | [21] |
| - | Deionized water, pH 5.5, medium flow rate- 5–16 mL/min, | [76] | |
| Nitrocellulose membrane (0.45 μm) | 0.05 M PBS, pH 7.4, 1000 mL, medium flow rate- 0.5 mL/min | [27] | |
| Regenerated cellulose membrane (0.45 μm) | PBS, pH 7.4, medium flow rate- 0.5 mL/min | [25] | |
| Franz diffusion cell | Nylon membrane (0.45 μm) | Degassed 0.05 M PB, pH 7.4, 17.5 mL, rotation- 240 rpm | [77] |
| Nitrocellulose membrane (0.45 μm) | 0.05 M PBS, pH 7.4, 1000 mL, medium flow rate- 5 mL/min | [27] | |
| MF™ membrane (0.45 μm) | PB, pH 7.4, 250 mL, medium flow rate- 5 mL/min | [78] | |
| Nitrocellulose membrane (0.45 μm) | PB, pH 7.4 containing 0.1% w/v SDS | [56] | |
| Polyester membrane (0.4 μm) | HBSS or SLF with DPPC (0.02% w/v), 50 mL, medium flow rate- 5 mL/min | [57] | |
| Regenerated cellulose membrane (0.45 μm) | PBS, pH 7.4, 1000 mL, magnet rotation- 100 rpm | [25] | |
| Regenerated cellulose membrane (0.45 μm) | Water, PB, pH 7.4, or modified SLF, pH 7.4, 10 mL, 75 rpm | [79] | |
| Cellulose acetate membrane (0.2 μm) | 0.05 M degassed PB, pH 7.4, or SLF, 0.15 mL in donor compartment and 27 mL in receiver compartment | [80] | |
| Nitrocellulose membrane (0.45 μm) | SLF, pH 7.4, 22.7 mL | [54] | |
| Polycarbonate membrane (0.4 μm) | SLF with SDS (0.5% w/v), 4.2 mL | [81] | |
| Filter paper | PBS, pH 7.4, 21.5 mL | [82] | |
| Transwell® system | Polyester membrane (0.4 μm) | PBS, pH 7.4 or distilled deionized water, pH 7.0, 0.04 mL in donor compartment and 1.4 mL in well plate | [20] |
| Polycarbonate membrane (0.4 μm) or Polyester membrane (0.4 μm) | PBS, pH 7.4, 2.6 mL or 3.85 mL | [48] | |
| Polyester membrane (0.4 μm) | PBS with SDS (0.5% w/v), 0.1 mL in donor compartment and 1.5 mL in well plate | [26] | |
| Dissolvit® | Polycarbonate membranes (0.03 μm) | 1.5% w/v PEO in 0.1 M PB with DPPC (0.02 and 0.4% w/w) | [23] |
| Custom-made flow perfusion cell | dialysis membrane (MWCO = 12,400 Da) | 1.0, 1.5, 2.0% w/v PEO in PBS, pH 7.4 1.5% w/v PEO in PBS, pH 7.4 with Curosurf® | [58] |
| Apparatus | Advantages | Disadvantages/limitations |
|---|---|---|
| Paddle over disc apparatus |
|
|
| Dialysis bag |
|
|
| Flow through cell |
|
|
| Franz diffusion cell |
|
|
| Transwell® system |
|
|
| DissolvIt® system |
|
|
| Models | Drugs | Ref. | |
|---|---|---|---|
| In vitro | Air-liquid interfaced layers Calu-3/Transwell system | Salbutamol Indomethacin | [90] |
| DissolvIt system | Budesonide Fluticasone propionate | [23] | |
| Custom made flow perfusion cell | Moxifloxacin Ethionamide | [58] | |
| Ex vivo | Isolated perfused rat lung | AZD5423 (developmental nonsteroidal glucocorticoid) Budesonide Fluticasone furoate Fluticasone propionate | [91] |
| In vivo | Rats | Rifampicin | [92] |
| Guinea pigs | Rifampicin | [93] | |
| Cynomolgus monkeys (non-human primates) | Erythropoietin Fc fusion protein | [94] | |
| Patients with cystic fibrosis (Clinical study) | Colistin | [95] | |
| Alveolar Epithelial Models | Tracheobronchial Epithelial Models |
|---|---|
| Primary alveolar epithelial cell cultures | Primary cell cultures
|
Alveolar epithelial cell lines
| Bronchial epithelial cell lines
|
| Co-culture models or human bronchial/alveolar cells |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eedara, B.B.; Bastola, R.; Das, S.C. Dissolution and Absorption of Inhaled Drug Particles in the Lungs. Pharmaceutics 2022, 14, 2667. https://doi.org/10.3390/pharmaceutics14122667
Eedara BB, Bastola R, Das SC. Dissolution and Absorption of Inhaled Drug Particles in the Lungs. Pharmaceutics. 2022; 14(12):2667. https://doi.org/10.3390/pharmaceutics14122667
Chicago/Turabian StyleEedara, Basanth Babu, Rakesh Bastola, and Shyamal C. Das. 2022. "Dissolution and Absorption of Inhaled Drug Particles in the Lungs" Pharmaceutics 14, no. 12: 2667. https://doi.org/10.3390/pharmaceutics14122667