
Drug Physicochemical Properties and Capsule Fill Determine Extent of Premature Gastric Release from Enteric Capsules

Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Model Drugs
2.3. Methods
2.3.1. Capsule-Fill Level and Diluents
2.3.2. Dissolution Tests
2.3.3. Solubility Assays
2.3.4. pH of Capsule Content on Exposure to Dissolution Media
3. Results
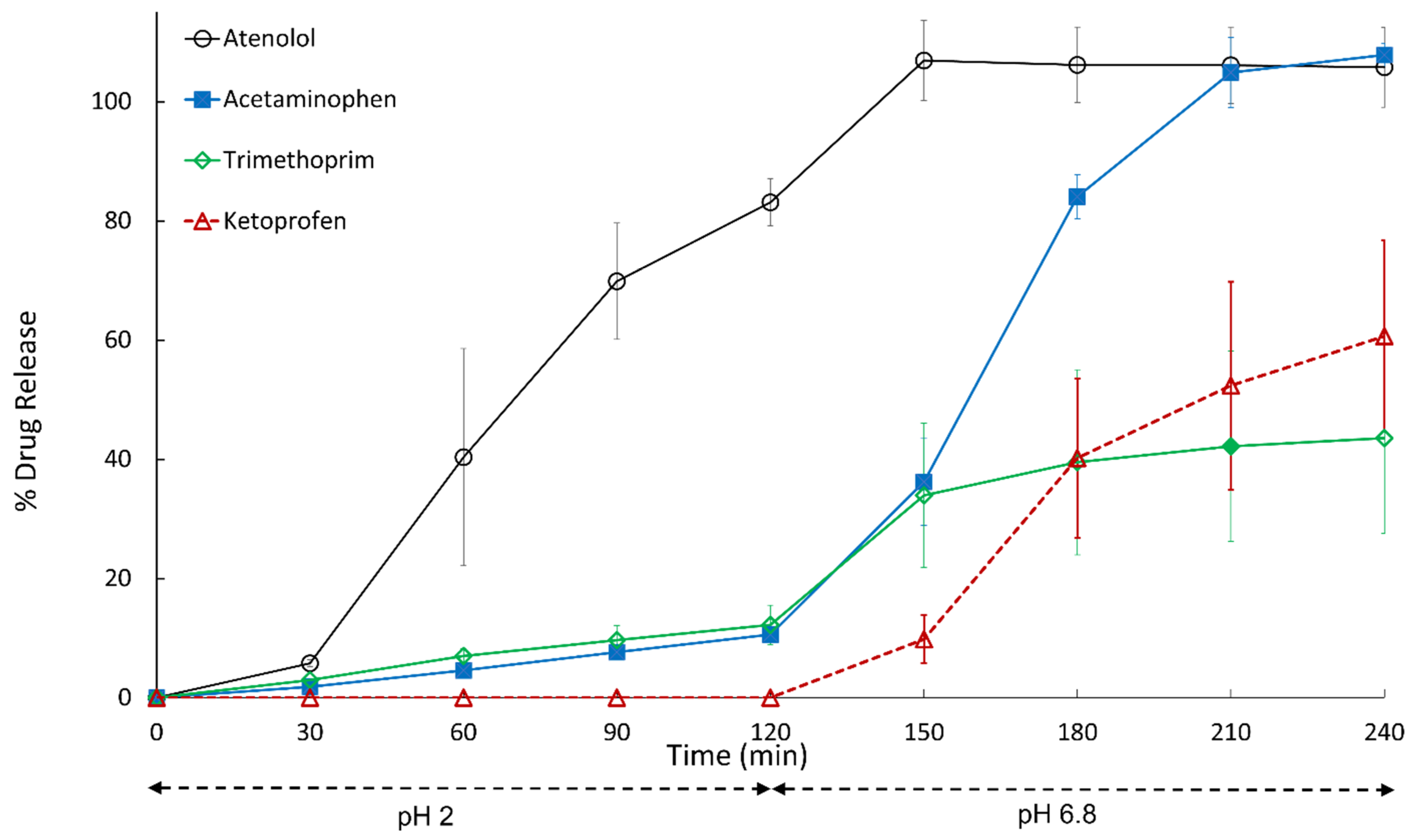
3.1. Effect of Drug Properties on Premature Drug Release in pH 2 Acid Phase
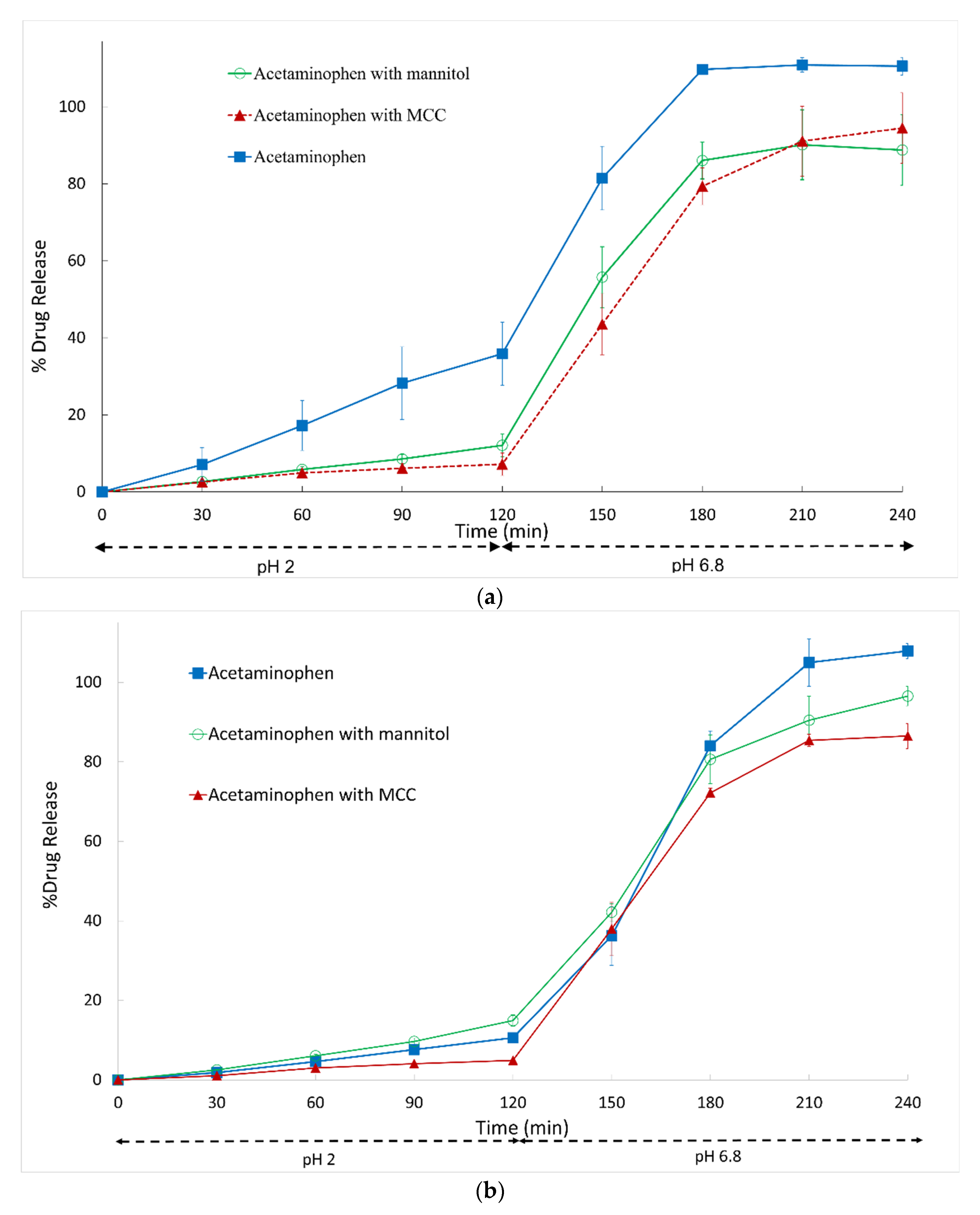
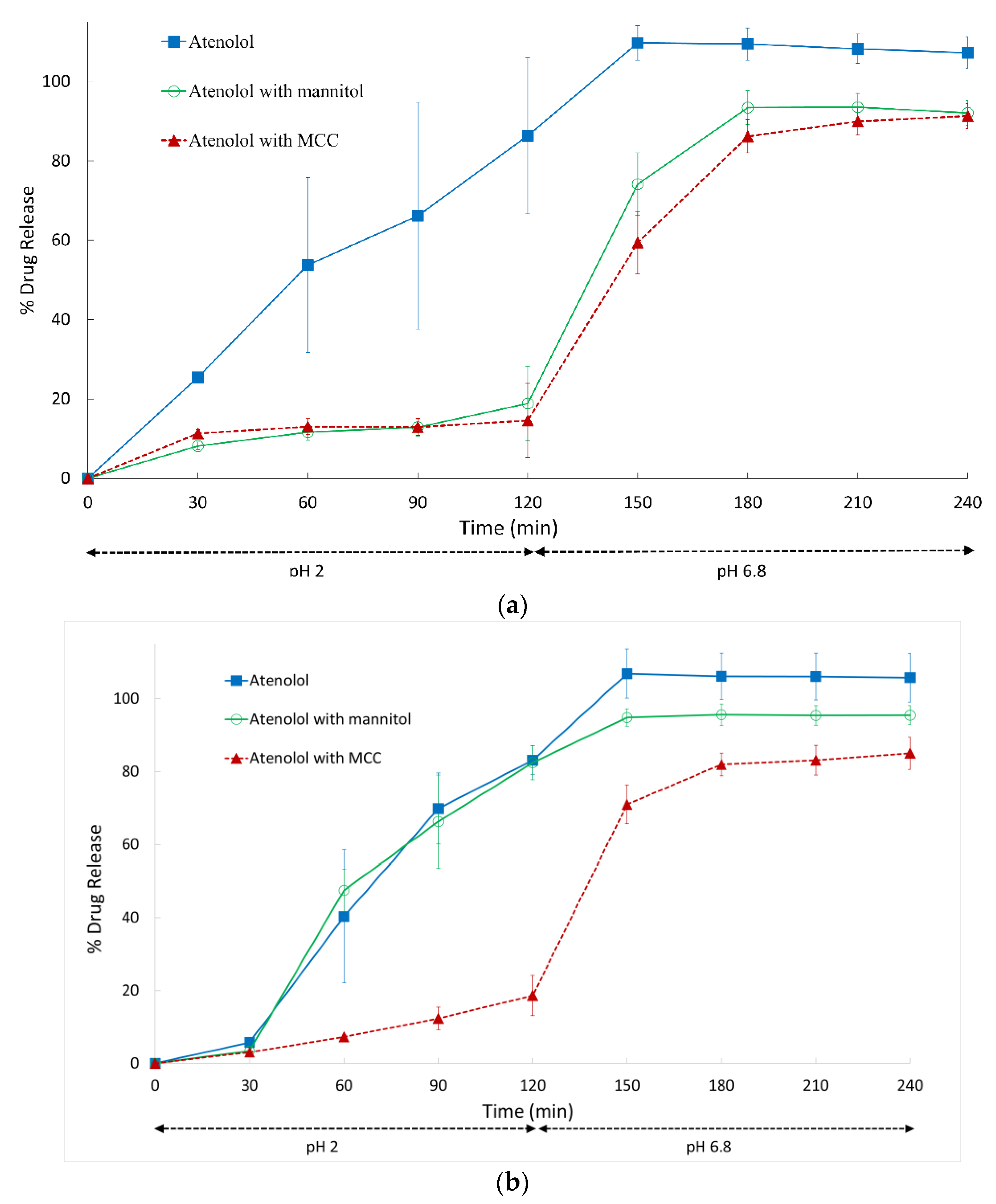
3.2. Effect of Diluent on Premature Gastric Drug Release in pH 2 Acid Phase
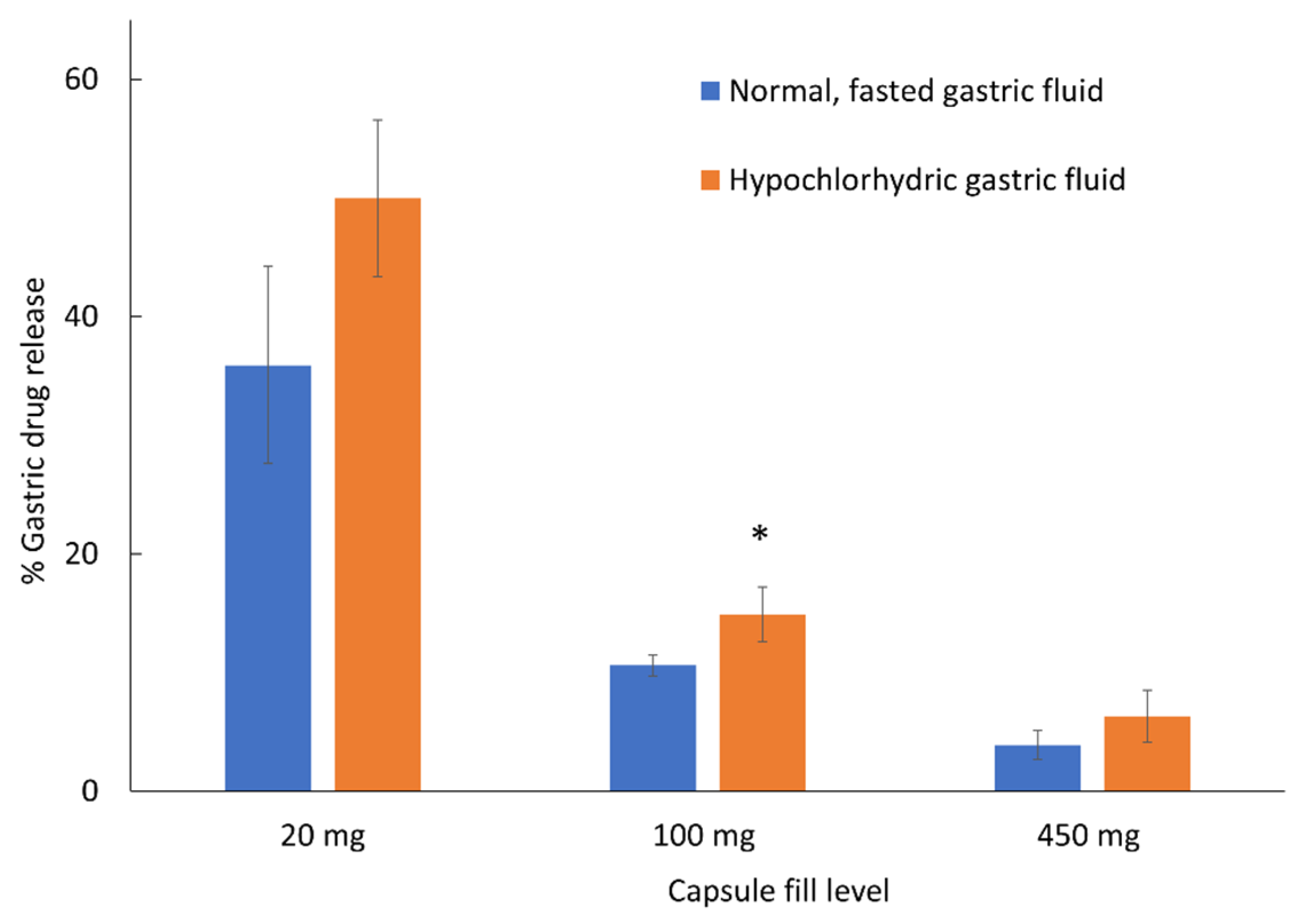
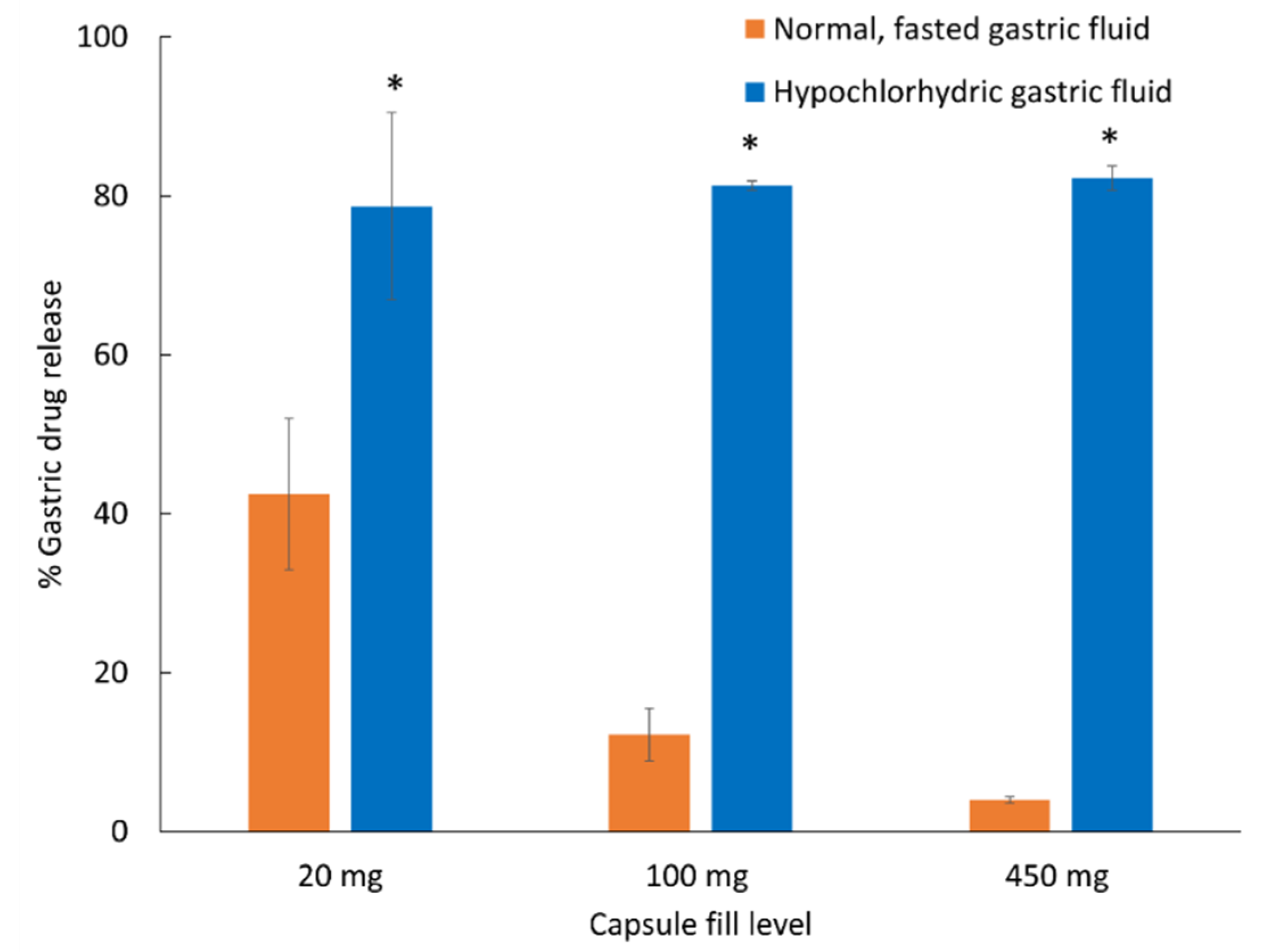
3.3. Effect of Hypochlorhydric, Simulated Fluids on Premature Gastric Drug Release
3.4. Implications of Findings
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kataoka, M.; Nakanishi, R.; Umesaki, M.; Kobayashi, M.; Minami, K.; Higashino, H.; Yamaguchi, S.; Yamashita, S. An enteric polymer mitigates the effects of gastric pH on oral absorption of poorly soluble weak acid drugs from supersaturable formulations: A case study with dantrolene. Eur. J. Pharm. Biopharm. 2020, 155, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Benameur, H. Enteric capsule drug delivery technology—Achieving protection without coating. Drug Dev. Deliv. 2015, 15, 34–37. [Google Scholar]
- Barbosa, J.A.C.; Al-Kauraishi, M.M.; Smith, A.M.; Conway, B.R.; Merchant, H.A. Achieving gastroresistance without coating: Formulation of capsule shells from enteric polymers. Eur. J. Pharm. Biopharm. 2019, 144, 174–179. [Google Scholar] [CrossRef]
- Vattanagijyingyong, Y.; Kulvanich, P.; Chatchawalsaisin, J. Fabrication of delayed release hard capsule shells from zein/methacrylic acid copolymer blends. Eur. J. Pharm. Sci. 2022, 171, 106124. [Google Scholar] [CrossRef]
- Nober, C.; Manini, G.; Carlier, E.; Raquez, J.M.; Benali, S.; Dubois, P.; Amighi, K.; Goole, J. Feasibility study into the potential use of fused-deposition modeling to manufacture 3D-printed enteric capsules in compounding pharmacies. Int. J. Pharm. 2019, 569, 118581. [Google Scholar] [CrossRef] [PubMed]
- Vcaps Enteric Capsules. Lonza Capsules and Health Ingredients. Available online: https://www.capsugel.com/biopharmaceutical-products/vcaps-enteric-capsules (accessed on 16 September 2022).
- Cade, N.C.; He, X.D. Acid Resistant Capsules. U.S. Patent 8,852,631, 7 October 2014. [Google Scholar]
- Eudracap Functional Ready-to-Fill Capsules. Evonik. Available online: https://health-care.evonik.com/eudracap-brochure (accessed on 16 September 2022).
- Oza, K.; Jain, V.; Guha, A.; Niepoth, P.; Hoelzer, B. Evaluation of Novel Enteric Ready-to-Fill Capsules; AAPS PharmSci360; T6125V; AAPS: Philadelphia, PA, USA, 2021. [Google Scholar]
- IMS Institute for Healthcare Informatics. Medicine Use and Spending Shifts: A Review of the Use of Medicines in the United States in 2014. Available online: https://www.iqvia.com/-/media/iqvia/pdfs/institute-reports/medicines-use-and-spending-shifts-in-the-us-in-2014.pdf (accessed on 16 September 2022).
- Kirchheiner, J.; Glatt, S.; Fuhr, U.; Klotz, U.; Meineke, I.; Seufferlein, T.; Brockmoller, J. Relative potency of proton-pump inhibitors-comparison of effects on intragastric pH. Eur. J. Clin. Pharmacol. 2009, 65, 19–31. [Google Scholar] [CrossRef]
- Russell, T.L.; Berardi, R.R.; Barnett, J.L.; O’Sullivan, T.L.; Wagner, J.G.; Dressman, J.B. pH-related changes in the absorption of dipyridamole in the elderly. Pharm. Res. 1994, 11, 136–143. [Google Scholar] [CrossRef]
- Kalantzi, L.; Reppas, C.; Dressman, J.B.; Amidon, G.L.; Junginger, H.E.; Midha, K.K.; Shah, V.P.; Stavchansky, S.A.; Barends, D.M. Biowaiver monographs for immediate release solid oral dosage forms: Acetaminophen (paracetamol). J. Pharm. Sci. 2006, 95, 4–14. [Google Scholar] [CrossRef] [Green Version]
- Yalkowsky, S.; Hey, Y.; Jain, P. Handbook of Aqueous Solubility Data, 2nd ed.; CRC Press: Boca Raton, FL, USA, 2010. [Google Scholar]
- Lindenberg, M.; Kopp, S.; Dressman, J.B. Classification of orally administered drugs on the World Health Organization Model list of Essential Medicines according to the biopharmaceutics classification system. Eur. J. Pharm. Biopharm. 2004, 58, 265–278. [Google Scholar] [CrossRef]
- NIH National Library of Medicine, National Center for Biotechnology Information. PubChem. Available online: https://pubchem.ncbi.nlm.nih.gov/ (accessed on 27 September 2022).
- Yang, Y.; Faustino, P.J.; Volpe, D.A.; Ellison, C.D.; Lyon, R.C.; Yu, L.X. Biopharmaceutics classification of selected beta-blockers: Solubility and permeability class membership. Mol. Pharm. 2007, 4, 608–614. [Google Scholar] [CrossRef]
- Tubic-Grozdanism, M.; Bolger, M.B.; Langguth, P. Application of gastrointestinal simulation for extensions of biowaivers of highly permeable compounds. AAPS J. 2008, 10, 213–226. [Google Scholar] [CrossRef] [PubMed]
- Sheng, J.J.; Kasim, N.A.; Chandrasekharan, R.; Amidon, G.L. Solubilization and dissolution of insoluble weak acid, ketoprofen: Effects of pH combined with surfactant. Eur. J. Pharm. Sci. 2006, 29, 306–314. [Google Scholar] [CrossRef] [PubMed]
- Noyes, A.A.; Whitney, W.R. The rate of solution of solid substances in their own solutions. J. Am. Chem. Soc. 1897, 19, 930–934. [Google Scholar] [CrossRef] [Green Version]
- Serajuddin, A.T.; Jarowski, C.I. Effect of diffusion layer pH and solubility on the dissolution rate of pharmaceutical acids and their sodium salts. II: Salicylic acid, theophylline, and benzoic acid. J. Pharm. Sci. 1985, 74, 148–154. [Google Scholar] [CrossRef]
- Marais, A.F.; van der Watt, J.G. Relationship between the pH of the diffusion layer and the dissolution rate of furosemide. Drug Dev. Ind. Pharm. 1991, 17, 1715–1720. [Google Scholar]
- Capsugel, L. New Intrinsically Enteric Capsule Technology for Pharmaceutical Drug Development. Available online: https://www.youtube.com/watch?v=yKAb_oKMuTY (accessed on 27 September 2022).
- Tyrer, J.H.; Eadie, M.J.; Sutherland, J.M.; Hooper, W.D. Outbreak of anticonvulsant intoxication in an Australian city. Br. Med. J. 1970, 4, 271–273. [Google Scholar] [CrossRef] [Green Version]
- Fadda, H.M.; Hellstrom, P.M.; Webb, D.L. Intra- and inter-subject variability in gastric pH following a low-fat, low-calorie meal. Int. J. Pharm. 2022, 625, 122069. [Google Scholar] [CrossRef]
- Abuhelwa, A.Y.; Foster, D.J.; Upton, R.N. A Quantitative Review and Meta-models of the Variability and Factors Affecting Oral Drug Absorption-Part II: Gastrointestinal Transit Time. AAPS J. 2016, 18, 1322–1333. [Google Scholar] [CrossRef]
- Koziolek, M.; Grimm, M.; Schneider, F.; Jedamzik, P.; Sager, M.; Kuhn, J.P.; Siegmund, W.; Weitschies, W. Navigating the human gastrointestinal tract for oral drug delivery: Uncharted waters and new frontiers. Adv. Drug Deliv. Rev. 2016, 101, 75–88. [Google Scholar] [CrossRef]
- Stillhart, C.; Vucicevic, K.; Augustijns, P.; Basit, A.W.; Batchelor, H.; Flanagan, T.R.; Gesquiere, I.; Greupink, R.; Keszthelyi, D.; Koskinen, M.; et al. Impact of gastrointestinal physiology on drug absorption in special populations—An UNGAP review. Eur. J. Pharm. Sci. 2020, 147, 105280. [Google Scholar] [CrossRef]
- Wilding, I.R.; Hardy, J.G.; Sparrow, R.A.; Davis, S.S.; Daly, P.B.; English, J.R. In vivo evaluation of enteric-coated naproxen tablets using gamma scintigraphy. Pharm. Res. 1992, 9, 1436–1441. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Drug | Chemical Structure | Ionization | pKa | Solubility (mg/mL) | Dose/ Solubility Ratio (mL) f | ||
|---|---|---|---|---|---|---|---|
| pH 2 | pH 4.5 | pH 6.8 | |||||
| Acetaminophen |  | Practically non-ionizable | 9.4 a,* | 14 b | 14 b | 14 b | 7.1 |
| Trimethoprim |  | Weak base | 7.12 a | 3.2 c | 0.3 c | - | 31.3 |
| Atenolol |  | Weak base | 9.6 a | 20.4 c | - | - | 4.9 |
| Ketoprofen |  | Weak acid | 4.39 d | 0.21 d | 0.49 e | 40.8 e | 476.2 |
| Powder Blend | pHd |
|---|---|
| Acetaminophen only | 2.3 ± 0.02 |
| Acetaminophen with microcrystalline cellulose | |
| 20/280 mg | 2.2 ± 0.03 |
| 100/200 mg | 2.0 ± 0.04 |
| Acetaminophen with mannitol | |
| 20/280 mg | 2.0 ± 0.03 |
| 100/200 mg | 2.0 ± 0.02 |
| Atenolol only | 10.3 ± 0.05 |
| Atenolol with microcrystalline cellulose | |
| 20/280 mg | 10.3 ± 0.04 |
| 100/200 mg | 10.6 ± 0.01 |
| Atenolol with mannitol | |
| 20/280 mg | 10.3 ± 0.03 |
| 100/200 mg | 10.5 ± 0.04 |
| Trimethoprim only | 6.3 ± 0.07 |
| Ketoprofen only | 2.0 ± 0.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moghrabi, F.S.; Fadda, H.M. Drug Physicochemical Properties and Capsule Fill Determine Extent of Premature Gastric Release from Enteric Capsules. Pharmaceutics 2022, 14, 2505. https://doi.org/10.3390/pharmaceutics14112505
Moghrabi FS, Fadda HM. Drug Physicochemical Properties and Capsule Fill Determine Extent of Premature Gastric Release from Enteric Capsules. Pharmaceutics. 2022; 14(11):2505. https://doi.org/10.3390/pharmaceutics14112505
Chicago/Turabian StyleMoghrabi, Fouad S., and Hala M. Fadda. 2022. "Drug Physicochemical Properties and Capsule Fill Determine Extent of Premature Gastric Release from Enteric Capsules" Pharmaceutics 14, no. 11: 2505. https://doi.org/10.3390/pharmaceutics14112505