

Comparison of Bitterness Intensity between Prednisolone and Quinine in a Human Sensory Test Indicated Individual Differences in Bitter-Taste Perception
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Eligibility
2.2.1. Inclusion Criteria
- Their age at the time of obtaining consent was between 20 to 55 years; and
- They gave written consent to participate in this study.
2.2.2. Exclusion Criteria
- Persons with a medical history that may affect the evaluation and safety of this study (drug abuse/dependence, alcohol abuse/dependence, gastrointestinal/cardiac/hepatic/renal/pulmonary/hematological disease, etc.); or
- Persons with a history of food allergies or drug hypersensitivity (including allergies); or
- Those who are currently smoking at the time of obtaining consent or those who have been quitting smoking for less than one year; or
- Persons with, or suspected of having an infectious disease requiring systemic or topical treatment; or
- Those who have had taste or smell abnormalities within 4 weeks of the study start date; or
- Those who are otherwise deemed ineligible at the discretion of the research doctor.
2.3. Stimuli
2.4. Sensory Test
2.5. DNA Extraction, PCR, and Sequencing
2.6. Statistical Analysis
3. Results
3.1. Subject Background
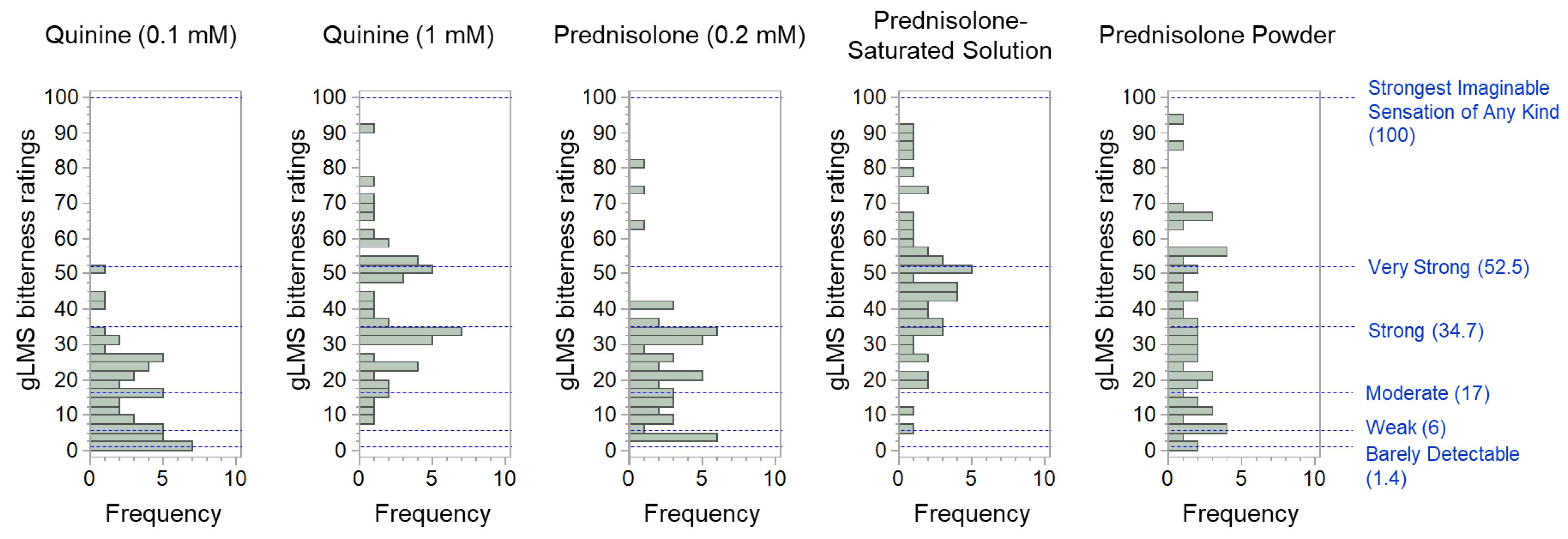
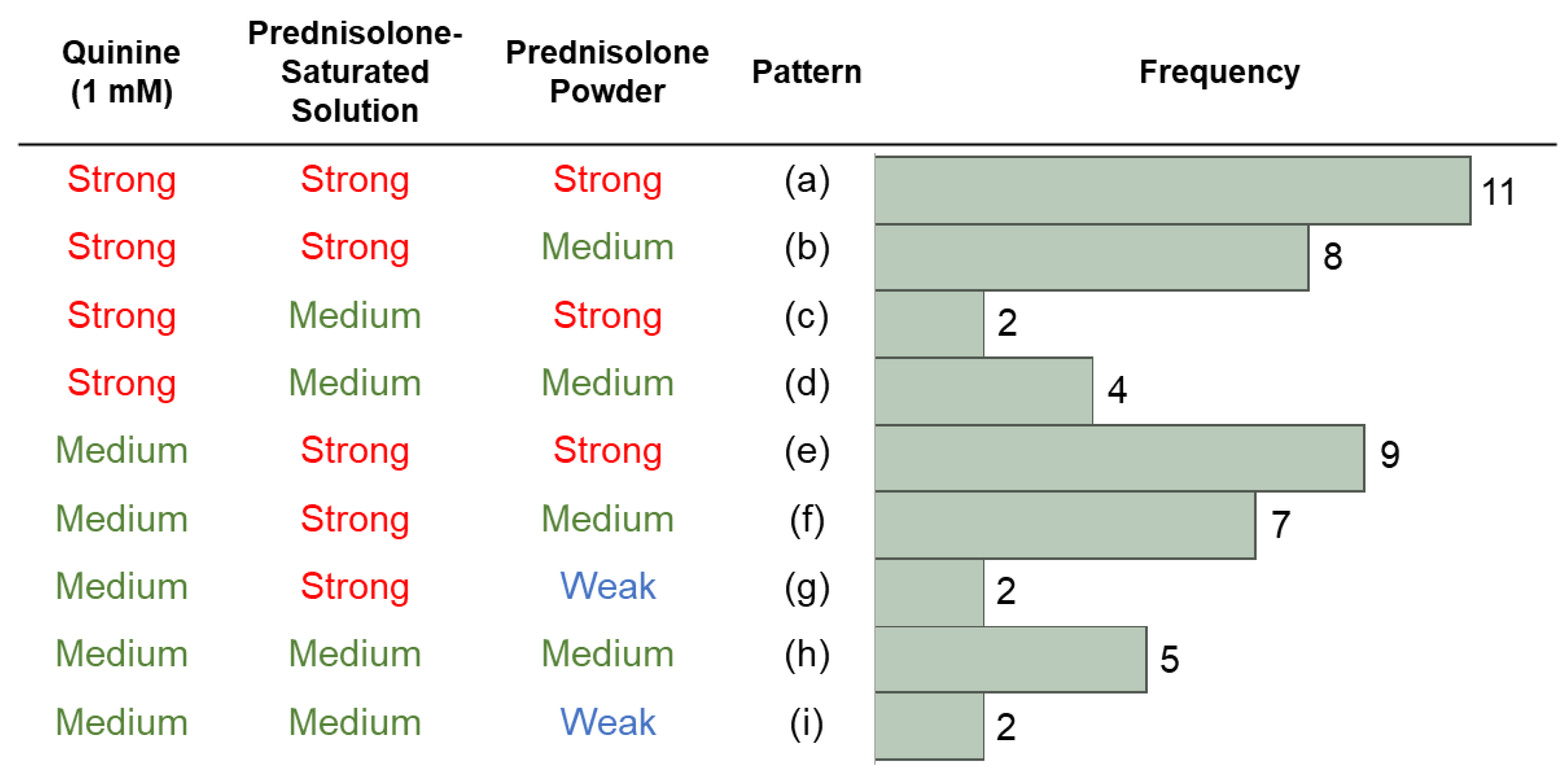
3.2. Bitterness Intensity of the Stimuli
3.3. Genes and gLMS Results
3.4. Sex and gLMS Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Menditto, E.; Orlando, V.; De Rosa, G.; Minghetti, P.; Musazzi, U.M.; Cahir, C.; Kurczewska-Michalak, M.; Kardas, P.; Costa, E.; Sousa Lobo, J.M.; et al. Patient centric pharmaceutical drug product design–the impact on medication adherence. Pharmaceutics 2020, 12, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mennella, J.A.; Spector, A.C.; Reed, D.R.; Coldwell, S.E. The bad taste of medicines: Overview of basic research on bitter taste. Clin. Ther. 2013, 35, 1225–1246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baguley, D.; Lim, E.; Bevan, A.; Pallet, A.; Faust, S.N. Prescribing for children–taste and palatability affect adherence to antibiotics: A review. Arch. Dis. Child. 2012, 97, 293–297. [Google Scholar] [CrossRef] [PubMed]
- Mennella, J.A.; Roberts, K.M.; Mathew, P.S.; Reed, D.R. Children’s perceptions about medicines: Individual differences and taste. BMC Pediatr. 2015, 15, 130. [Google Scholar] [CrossRef] [PubMed]
- Aljebab, F.; Alanazi, M.; Choonara, I.; Conroy, S. Observational study on the palatability and tolerability of oral prednisolone and oral dexamethasone in children in Saudi Arabia and the UK. Arch. Dis. Child. 2018, 103, 83–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hames, H.; Seabrook, J.A.; Matsui, D.; Rieder, M.J.; Joubert, G.I. A palatability study of a flavored dexamethasone preparation versus prednisolone liquid in children. Can. J. Clin. Pharmacol. 2008, 15, e95–e98. [Google Scholar] [PubMed]
- Uchida, T.; Kobayashi, Y.; Miyanaga, Y.; Toukubo, R.; Ikezaki, H.; Taniguchi, A.; Nishikata, M.; Matsuyama, K. A new method for evaluating the bitterness of medicines by semi-continuous measurement of adsorption using a taste sensor. Chem. Pharm. Bull. 2001, 49, 1336–1339. [Google Scholar] [CrossRef] [PubMed]
- Chandrashekar, J.; Mueller, K.L.; Hoon, M.A.; Adler, E.; Feng, L.; Guo, W.; Zuker, C.S.; Ryba, N.J. T2Rs function as bitter taste receptors. Cell 2000, 100, 703–711. [Google Scholar] [CrossRef] [Green Version]
- Adler, E.; Hoon, M.A.; Mueller, K.L.; Chandrashekar, J.; Ryba, N.J.; Zuker, C.S. A novel family of mammalian taste receptors. Cell 2000, 100, 693–702. [Google Scholar] [CrossRef] [Green Version]
- Roudnitzky, N.; Behrens, M.; Engel, A.; Kohl, S.; Thalmann, S.; Hübner, S.; Lossow, K.; Wooding, S.P.; Meyerhof, W. Receptor polymorphism and genomic structure interact to shape bitter taste perception. PLoS Genet. 2015, 11, e1005530. [Google Scholar] [CrossRef] [PubMed]
- Bartoshuk, L.M.; Duffy, V.B.; Green, B.G.; Hoffman, H.J.; Ko, C.W.; Lucchina, L.A.; Marks, L.E.; Snyder, D.J.; Weiffenbach, J.M. Valid across-group comparisons with labeled scales: The gLMS versus magnitude matching. Physiol. Behav. 2004, 82, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Teva Takeda Pharma Ltd. Prednisolone Tablets 5 mg/Prednisolone Powder 1% Drug Interview Form. Available online: https://www.med.takeda-teva.com/di-net/product/doc/1/06/1106_Prednisolone_tab_powder_TAKEDA_IF.pdf (accessed on 26 July 2022).
- Yamaki, M.; Saito, H.; Isono, K.; Goto, T.; Shirakawa, H.; Shoji, N.; Satoh-Kuriwada, S.; Sasano, T.; Okada, R.; Kudoh, K.; et al. Genotyping analysis of bitter-taste receptor genes TAS2R38 and TAS2R46 in Japanese patients with gastrointestinal cancers. J. Nutr. Sci. Vitaminol. 2017, 63, 148–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cruickshanks, K.J.; Schubert, C.R.; Snyder, D.J.; Bartoshuk, L.M.; Huang, G.H.; Klein, B.E.; Klein, R.; Nieto, F.J.; Pankow, J.S.; Tweed, T.S.; et al. Measuring taste impairment in epidemiologic studies: The Beaver Dam Offspring Study. Ann. N. Y. Acad. Sci. 2009, 1170, 543–552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bufe, B.; Breslin, P.A.; Kuhn, C.; Reed, D.R.; Tharp, C.D.; Slack, J.P.; Kim, U.K.; Drayna, D.; Meyerhof, W. The molecular basis of individual differences in phenylthiocarbamide and propylthiouracil bitterness perception. Curr. Biol. 2005, 15, 322–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reed, D.R.; Zhu, G.; Breslin, P.A.; Duke, F.F.; Henders, A.K.; Campbell, M.J.; Montgomery, G.W.; Medland, S.E.; Martin, N.G.; Wright, M.J. The perception of quinine taste intensity is associated with common genetic variants in a bitter receptor cluster on chromosome 12. Hum. Mol. Genet. 2010, 19, 4278–4285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayes, J.E.; Feeney, E.L.; Nolden, A.A.; McGeary, J.E. Quinine bitterness and grapefruit liking associate with allelic variants in TAS2R31. Chem. Senses 2015, 40, 437–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duffy, V.B.; Peterson, J.M.; Bartoshuk, L.M. Associations between taste genetics, oral sensation and alcohol intake. Physiol. Behav. 2004, 82, 435–445. [Google Scholar] [CrossRef] [PubMed]
- Barragán, R.; Coltell, O.; Portolés, O.; Asensio, E.M.; Sorlí, J.V.; Ortega-Azorín, C.; González, J.I.; Sáiz, C.; Fernández-Carrión, R.; Ordovas, J.M.; et al. Bitter, sweet, salty, sour and umami taste perception decreases with age: Sex-specific analysis, modulation by genetic variants and taste-preference associations in 18 to 80 year-old subjects. Nutrients 2018, 10, 1539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, A.M.; Ali, S.; Jameela, R.V.; Muhamood, M.; Haqh, M.F. Impact of fungiform papillae count on taste perception and different methods of taste assessment and their clinical applications: A comprehensive review. Sultan Qaboos Univ. Med. J. 2019, 19, e184–e191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayes, J.E.; Feeney, E.L.; Allen, A.L. Do polymorphisms in chemosensory genes matter for human ingestive behavior? Food Qual. Prefer. 2013, 30, 202–216. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Name of Stimuli | Weight and Name of Active Constituent | Solvent/Dispersion Medium | Total Volume/Weight |
|---|---|---|---|
| Quinine solution (0.1 mM) | 0.40 mg quinine hydrochloride | Water | 10 mL |
| Quinine solution (1 mM) | 4.0 mg quinine hydrochloride | Water | 10 mL |
| Prednisolone solution (0.2 mM) | 0.72 mg prednisolone | Water | 10 mL |
| Prednisolone-saturated solution | Approximately 2.93 mg prednisolone | Water | 10 mL |
| Prednisolone powder (1%) | 2.0 mg prednisolone | Lactose | 0.2 g |
| Quinine (0.1 mM) | Quinine (1 mM) | Prednisolone (0.2 mM) | Prednisolone-Saturated Solution | Prednisolone Powder | |
|---|---|---|---|---|---|
| Mean | 15.9 | 40.1 | 24.5 | 46.8 | 34.1 |
| Min. | 0.7 | 8.7 | 2.7 | 6.0 | 2.0 |
| Max. | 50.7 | 90.0 | 80.0 | 92.0 | 94.7 |
| SD | 12.2 | 18.0 | 16.8 | 19.7 | 23.0 |
| CV | 0.77 | 0.45 | 0.69 | 0.42 | 0.67 |
| TAS2R19 Genotype | Strong | Medium or Weak | p-Value |
|---|---|---|---|
| GG | 11 | 15 | 0.0266 |
| AG | 14 | 6 | |
| AA | 0 | 3 | |
| 25 | 24 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deng, M.; Hida, N.; Yamazaki, T.; Morishima, R.; Kato, Y.; Fujita, Y.; Nakamura, A.; Harada, T. Comparison of Bitterness Intensity between Prednisolone and Quinine in a Human Sensory Test Indicated Individual Differences in Bitter-Taste Perception. Pharmaceutics 2022, 14, 2454. https://doi.org/10.3390/pharmaceutics14112454
Deng M, Hida N, Yamazaki T, Morishima R, Kato Y, Fujita Y, Nakamura A, Harada T. Comparison of Bitterness Intensity between Prednisolone and Quinine in a Human Sensory Test Indicated Individual Differences in Bitter-Taste Perception. Pharmaceutics. 2022; 14(11):2454. https://doi.org/10.3390/pharmaceutics14112454
Chicago/Turabian StyleDeng, Mengyan, Noriko Hida, Taigi Yamazaki, Ryo Morishima, Yuka Kato, Yoshiaki Fujita, Akihiro Nakamura, and Tsutomu Harada. 2022. "Comparison of Bitterness Intensity between Prednisolone and Quinine in a Human Sensory Test Indicated Individual Differences in Bitter-Taste Perception" Pharmaceutics 14, no. 11: 2454. https://doi.org/10.3390/pharmaceutics14112454