
Clinical Efficacy of Temocillin Standard Dosing in Patients Treated with Outpatient Antimicrobial Therapy
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design, Setting and Study Participants
2.2. tOPAT Program of the University Hospitals Leuven
2.3. Data Collection and Analysis
2.3.1. Demographics, Clinical and Treatment-Related Data
2.3.2. Clinical Outcome
2.3.3. Safety
2.3.4. Statistical Analysis
3. Results
3.1. Demographics
3.2. Clinical and Treatment-Related Data
3.3. Clinical Outcomes
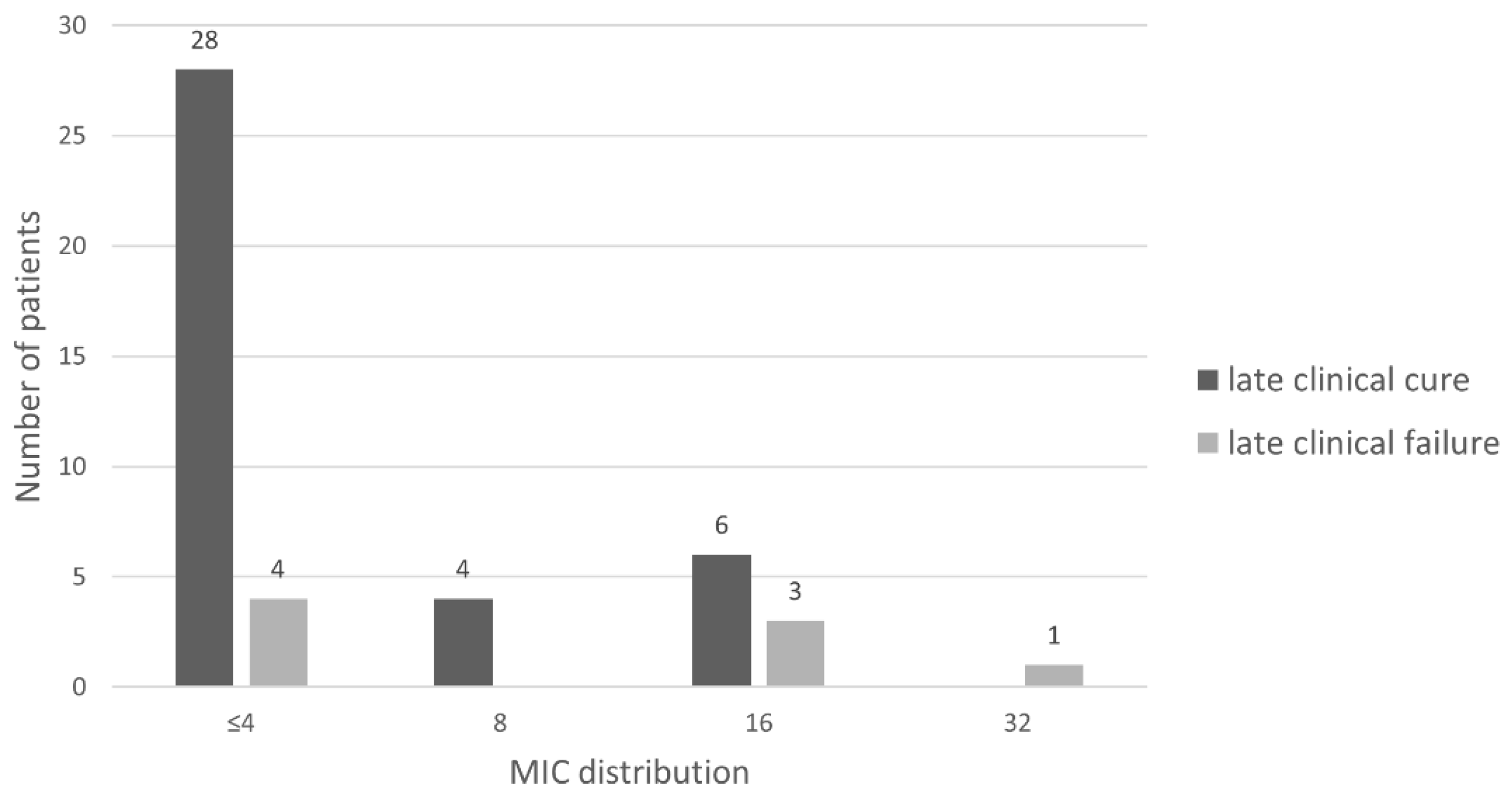
3.3.1. Primary Outcome: Late Clinical Cure
3.3.2. Secondary Outcomes: Clinical Cure at the End of Therapy and Early Clinical Cure
3.4. Safety
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alexandre, K.; Fantin, B. Pharmacokinetics and Pharmacodynamics of Temocillin. Clin. Pharm. 2018, 57, 287–296. [Google Scholar] [CrossRef] [PubMed]
- Alexandre, K.; Leysour de Rohello, F.; Dahyot, S.; Etienne, M.; Tiret, I.; Gillibert, A.; Pestel-Caron, M.; Caron, F. Efficacy of temocillin against MDR Enterobacterales: A retrospective cohort study. J. Antimicrob. Chemother. 2021, 76, 784–788. [Google Scholar] [CrossRef]
- Delory, T.; Gravier, S.; Le Pluart, D.; Gaube, G.; Simeon, S.; Davido, B.; Piet, E.; Lepeule, R.; Lesprit, P.; Lafaurie, M. Temocillin versus carbapenems for urinary tract infection due to ESBL-producing Enterobacteriaceae: A multicenter matched case-control study. Int. J. Antimicrob. Agents 2021, 58, 106361. [Google Scholar] [CrossRef] [PubMed]
- Wagenlehner, F.M.E.; Bjerklund Johansen, T.E.; Cai, T.; Koves, B.; Kranz, J.; Pilatz, A.; Tandogdu, Z. Epidemiology, definition and treatment of complicated urinary tract infections. Nat. Rev. Urol. 2020, 17, 586–600. [Google Scholar] [CrossRef]
- Rodríguez-Baño, J.; Gutiérrez-Gutiérrez, B.; Machuca, I.; Pascual, A. Treatment of Infections Caused by Extended-Spectrum-Beta-Lactamase-, AmpC-, and Carbapenemase-Producing Enterobacteriaceae. Clin. Microbiol. Rev. 2018, 31, e00079-1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heard, K.L.; Killington, K.; Mughal, N.; Moore, L.S.P.; Hughes, S. Clinical outcomes of temocillin use for invasive Enterobacterales infections: A single-centre retrospective analysis. JAC Antimicrob. Resist. 2021, 3, dlab005. [Google Scholar] [CrossRef]
- Livermore, D.M.; Tulkens, P.M. Temocillin revived. J. Antimicrob. Chemother. 2009, 63, 243–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Jongh, R.; Hens, R.; Basma, V.; Mouton, J.W.; Tulkens, P.M.; Carryn, S. Continuous versus intermittent infusion of temocillin, a directed spectrum penicillin for intensive care patients with nosocomial pneumonia: Stability, compatibility, population pharmacokinetic studies and breakpoint selection. J. Antimicrob. Chemother. 2008, 61, 382–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- EUCAST. To Clinical Colleagues: On Recent Changes in Clinical Microbiology Susceptibility Reports—New Interpretation of Susceptibility Categories S, I and R; EUCAST: Växjö, Sweden, 2021. [Google Scholar]
- Fuchs, P.C.; Barry, A.L.; Thornsberry, C.; Jones, R.N. Interpretive criteria for temocillin disk diffusion susceptibility testing. Eur J. Clin. Microbiol. 1985, 4, 30–33. [Google Scholar] [CrossRef] [PubMed]
- EUCAST. Temocillin—Rationale for the EUCAST Clinical Breakpoints, Version 1.0; EUCAST: Växjö, Sweden, 2019. [Google Scholar]
- Quintens, C.; Steffens, E.; Jacobs, K.; Schuermans, A.; Van Eldere, J.; Lagrou, K.; De Munter, P.; Derdelinckx, I.; Peetermans, W.E.; Spriet, I. Efficacy and safety of a Belgian tertiary care outpatient parenteral antimicrobial therapy (OPAT) program. Infection 2020, 48, 357–366. [Google Scholar] [CrossRef] [PubMed]
- Gijsen, M.; Wilmer, A.; Meyfroidt, G.; Wauters, J.; Spriet, I. Can augmented renal clearance be detected using estimators of glomerular filtration rate? Crit. Care 2020, 24, 359. [Google Scholar] [CrossRef] [PubMed]
- Gijsen, M.; Huang, C.Y.; Flechet, M.; Van Daele, R.; Declercq, P.; Debaveye, Y.; Meersseman, P.; Meyfroidt, G.; Wauters, J.; Spriet, I. Development and External Validation of an Online Clinical Prediction Model for Augmented Renal Clearance in Adult Mixed Critically Ill Patients: The Augmented Renal Clearance Predictor. Crit. Care Med. 2020, 48, e1260–e1268. [Google Scholar] [CrossRef] [PubMed]
- Laterre, P.F.; Wittebole, X.; Van de Velde, S.; Muller, A.E.; Mouton, J.W.; Carryn, S.; Tulkens, P.M.; Dugernier, T. Temocillin (6 g daily) in critically ill patients: Continuous infusion versus three times daily administration. J. Antimicrob. Chemother. 2015, 70, 891–898. [Google Scholar] [CrossRef]
- Roberts, J.A.; Abdul-Aziz, M.H.; Lipman, J.; Mouton, J.W.; Vinks, A.A.; Felton, T.W.; Hope, W.W.; Farkas, A.; Neely, M.N.; Schentag, J.J.; et al. Individualised antibiotic dosing for patients who are critically ill: Challenges and potential solutions. Lancet Infect. Dis. 2014, 14, 498–509. [Google Scholar] [CrossRef] [Green Version]
- Balakrishnan, I.; Awad-El-Kariem, F.M.; Aali, A.; Kumari, P.; Mulla, R.; Tan, B.; Brudney, D.; Ladenheim, D.; Ghazy, A.; Khan, I.; et al. Temocillin use in England: Clinical and microbiological efficacies in infections caused by extended-spectrum and/or derepressed AmpC β-lactamase-producing Enterobacteriaceae. J. Antimicrob. Chemother. 2011, 66, 2628–2631. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Munting, A.; Regina, J.; Damas, J.; Lhopitallier, L.; Kritikos, A.; Guery, B.; Senn, L.; Viala, B. Impact of 2020 EUCAST criteria on meropenem prescription for the treatment of Pseudomonas aeruginosa infections: An observational study in a university hospital. Clin. Microbiol. Infect. 2022, 28, 558–563. [Google Scholar] [CrossRef] [PubMed]
- Diamantis, S.; Dawudi, Y.; Cassard, B.; Longuet, P.; Lesprit, P.; Gauzit, R. Home intravenous antibiotherapy and the proper use of elastomeric pumps: Systematic review of the literature and proposals for improved use. Infect. Dis. Now 2021, 51, 39–49. [Google Scholar] [CrossRef]


{kind=link}
| Category | Subcategory | |
|---|---|---|
| Demographics | tOPAT episodes, n | 57 |
| Patients, n | 50 | |
| Patients with 1 tOPAT episode, n (%) | 44(88.0) | |
| Patients with 2 tOPAT episodes, n (%) | 5(10.0) | |
| Patients with 3 tOPAT episodes, n (%) | 1(2.0) | |
| Male/female, n | 39/11 | |
| Age (years), median (range) | 65 (20–83) | |
| Medical discipline | Urology | 27 (47.4) |
| General internal medicine, n (%) | 15 (26.3) | |
| Nephrology, n (%) | 10 (17.5) | |
| Cardiology, n (%) | 2 (3.5) | |
| Digestive oncology, n (%) | 1 (1.8) | |
| Geriatric, n (%) | 1 (1.8) | |
| Hepatology, n (%) | 1 (1.8) | |
| Clinical indication | cUTI, n (%) | 50 (87.7) |
| Prostatitis, n (%) | 21 (36.8) | |
| Urosepsis, n (%) | 12 (21.1) | |
| Pyelonephritis, n (%) | 7 (12.3) | |
| Undefined, n (%) | 6 (10.5) | |
| Epididymitis, n (%) | 2 (3.5) | |
| Cystitis, n (%) | 1 (1.8) | |
| Pyelonephritis + prostatitis, n (%) | 1 (1.8) | |
| Cyst infection, n (%) | 6 (10.5) | |
| Cholangitis, n (%) | 1 (1.8) | |
| Causative pathogen(s) | E. coli, n (%) | 38 (66.7) |
| K. pneumonia, n (%) | 10 (17.5) | |
| K. pneumonia + E. coli, n (%) | 2 (3.5) | |
| E. cloacae, n (%) | 2 (3.5) | |
| E. coli + S. marcescens, n (%) | 1 (1.8) | |
| K. oxytoca, n (%) | 1 (1.8) | |
| K. oxytoca + E. coli, n (%) | 1 (1.8) | |
| M. morganii, n (%) | 1 (1.8) | |
| Empirical therapy, n (%) | 1 (1.8) |
| All tOPAT Episodes, n = 56 | Late Clinical Cure, n = 48 | Late Clinical Failure, n = 8 | p-Value | |
|---|---|---|---|---|
| Age (years), median (range) | 66 (20–83) | 63 (20–83) | 74 (41–79) | 0.17 |
| Female, n (%) | 13 (23.2) | 11 (22.9) | 2 (25.0) | 0.95 |
| Infection focus | ||||
| Prostatitis, n (%) | 21 (37.5) | 21 (43.8) | 0 (0) | <0.001 |
| Urosepsis, n (%) | 12 (21.4) | 7 (14.6) | 5 (62.5) | reference |
| Pyelonephritis, n (%) | 7 (12.5) | 6 (12.5) | 1 (12.5) | 0.065 |
| Undefined cUTI, n (%) | 6 (10.7) | 6 (12.5) | 0 (0) | <0.001 |
| Cyst, n (%) | 5 (8.9) | 4 (8.3) | 1 (12.5) | 0.152 |
| Epididymitis, n (%) | 2 (3.6) | 2 (4.2) | 0 (0) | <0.001 |
| Pyelonephritis and prostatitis, n (%) | 1 (1.8) | 1 (2.1) | 0 (0) | <0.001 |
| Cystitis, n (%) | 1 (1.8) | 1 (2.1) | 0 (0) | <0.001 |
| Cholangitis, n (%) | 1 (1.8) | 0 (0) | 1 (12.5) | <0.001 |
| MIC ≤ 8 mg/L, n (%) | 36 (78.3) a | 32 (84.2) a | 4 (50.0) | <0.001 |
| Intermittent infusion, n (%) | 47 (83.9) | 40 (83.3) | 7 (87.5) | 0.92 |
| Duration antibiotic therapy (days), median (range) | 21 (10–49) | 21 (10–49) | 18 (10–42) | 0.45 |
| Duration OPAT (days), median (range) | 15 (3–43) | 15 (3–43) | 13 (4–38) | 0.86 |
| eGFR at start temocillin (mL/min/1.73 m2), median (range) | 66 (5–140) | 66 (5–140) | 51 (20–95) | 0.27 |
| eGFR at discharge (mL/min/1.73 m2), median (range) | 74 (5–140) | 76 (5–140) | 55 (20–95) | 0.46 |
| Augmented renal clearance, n (%) b | 10 (17.9) | 10 (20.8) | 0 (0) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Van den Broucke, E.; Thijs, L.; Desmet, S.; Vander Elst, L.; Gijsen, M.; Mylemans, M.; Van de Gaer, O.; Peetermans, W.E.; Quintens, C.; Spriet, I. Clinical Efficacy of Temocillin Standard Dosing in Patients Treated with Outpatient Antimicrobial Therapy. Pharmaceutics 2022, 14, 2289. https://doi.org/10.3390/pharmaceutics14112289
Van den Broucke E, Thijs L, Desmet S, Vander Elst L, Gijsen M, Mylemans M, Van de Gaer O, Peetermans WE, Quintens C, Spriet I. Clinical Efficacy of Temocillin Standard Dosing in Patients Treated with Outpatient Antimicrobial Therapy. Pharmaceutics. 2022; 14(11):2289. https://doi.org/10.3390/pharmaceutics14112289
Chicago/Turabian StyleVan den Broucke, Evelyne, Lore Thijs, Stefanie Desmet, Lotte Vander Elst, Matthias Gijsen, Marnix Mylemans, Otto Van de Gaer, Willy E. Peetermans, Charlotte Quintens, and Isabel Spriet. 2022. "Clinical Efficacy of Temocillin Standard Dosing in Patients Treated with Outpatient Antimicrobial Therapy" Pharmaceutics 14, no. 11: 2289. https://doi.org/10.3390/pharmaceutics14112289