
Efficacy and Safety of Ablative Fractional Laser-Assisted Delivery of Methotrexate in Adults with Localized Scleroderma: A Randomized and Controlled Clinical Trial
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
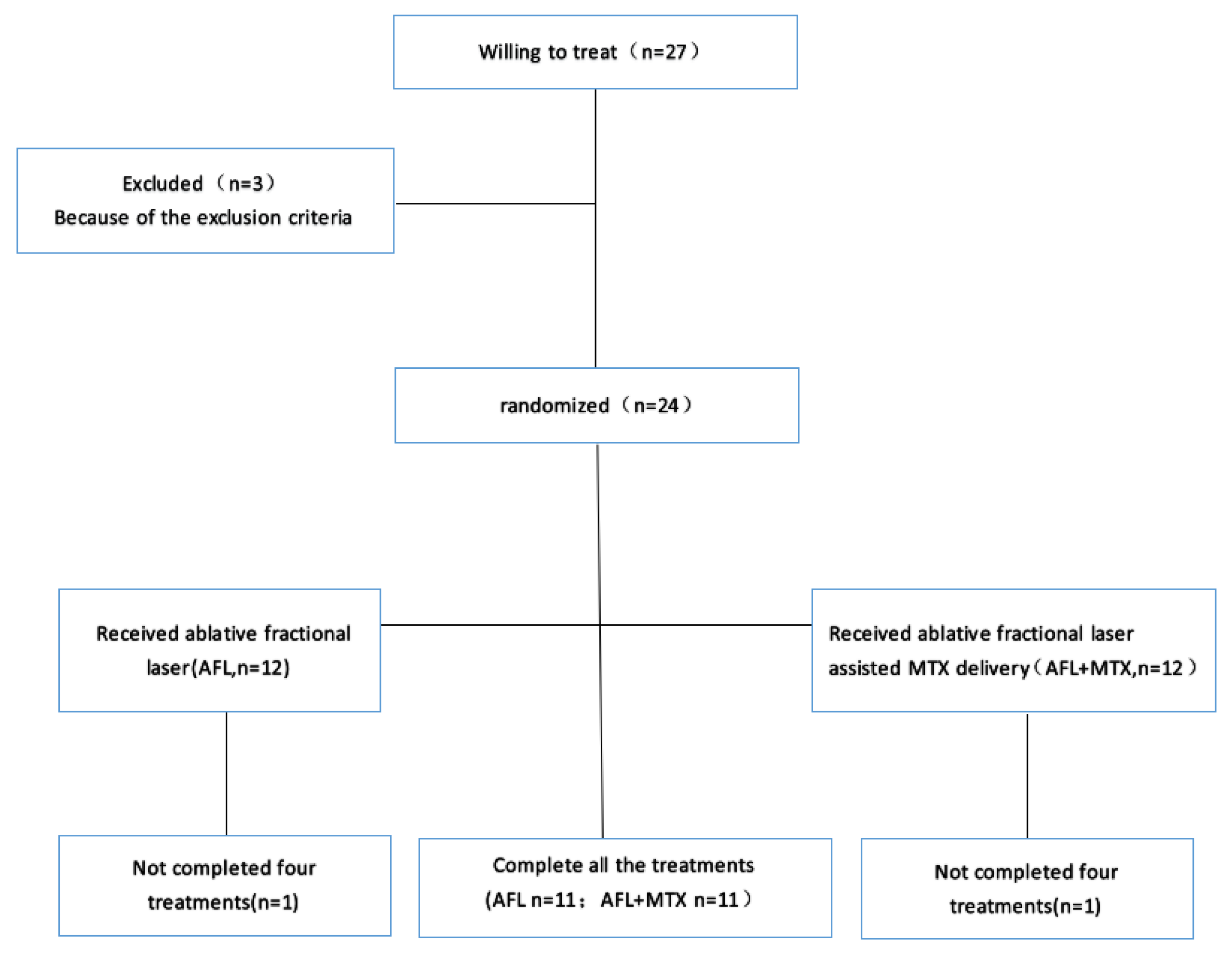
2.1. Patients
2.2. Treatment
2.3. Clinical Evaluation
2.4. Ultrasound and Histopathological Evaluation
2.5. Safety Assessment
2.6. Statistical Analysis
3. Results
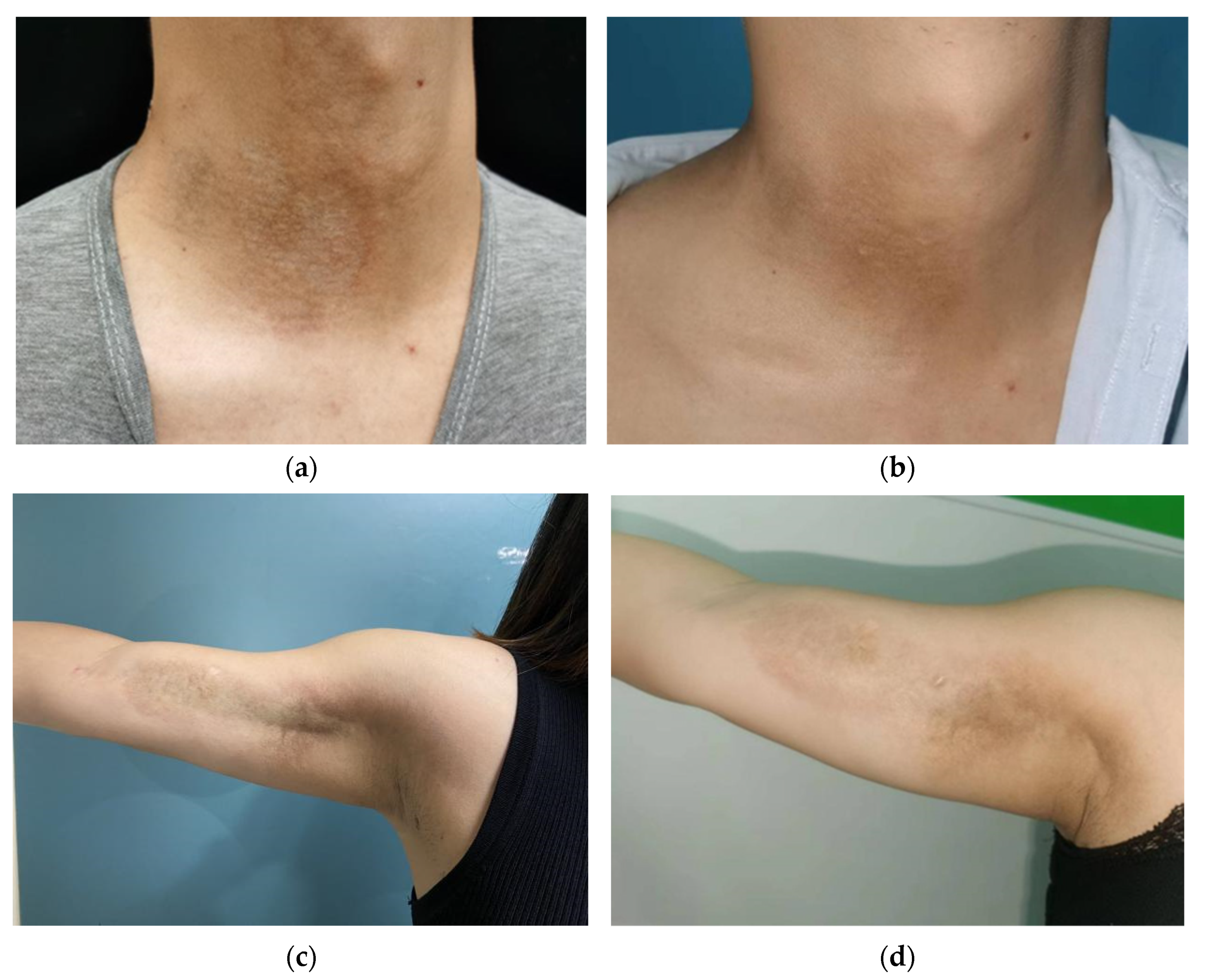
3.1. Clinical Improvement
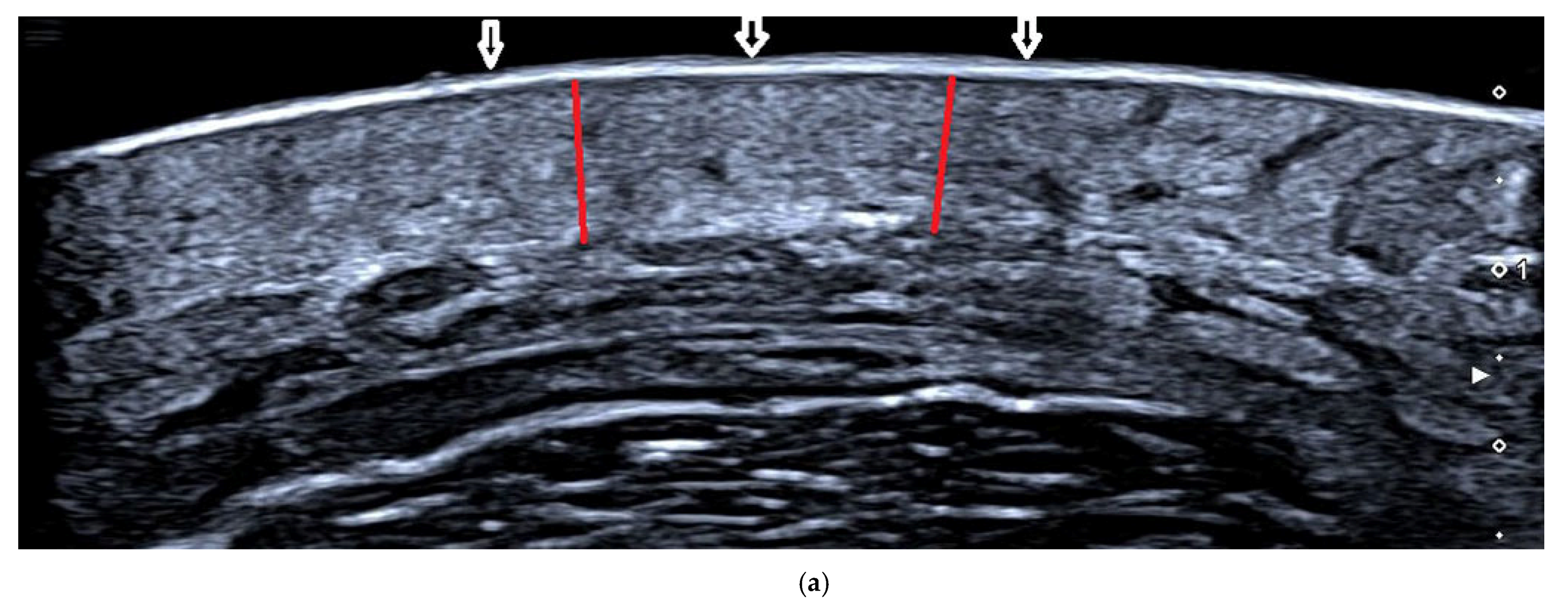
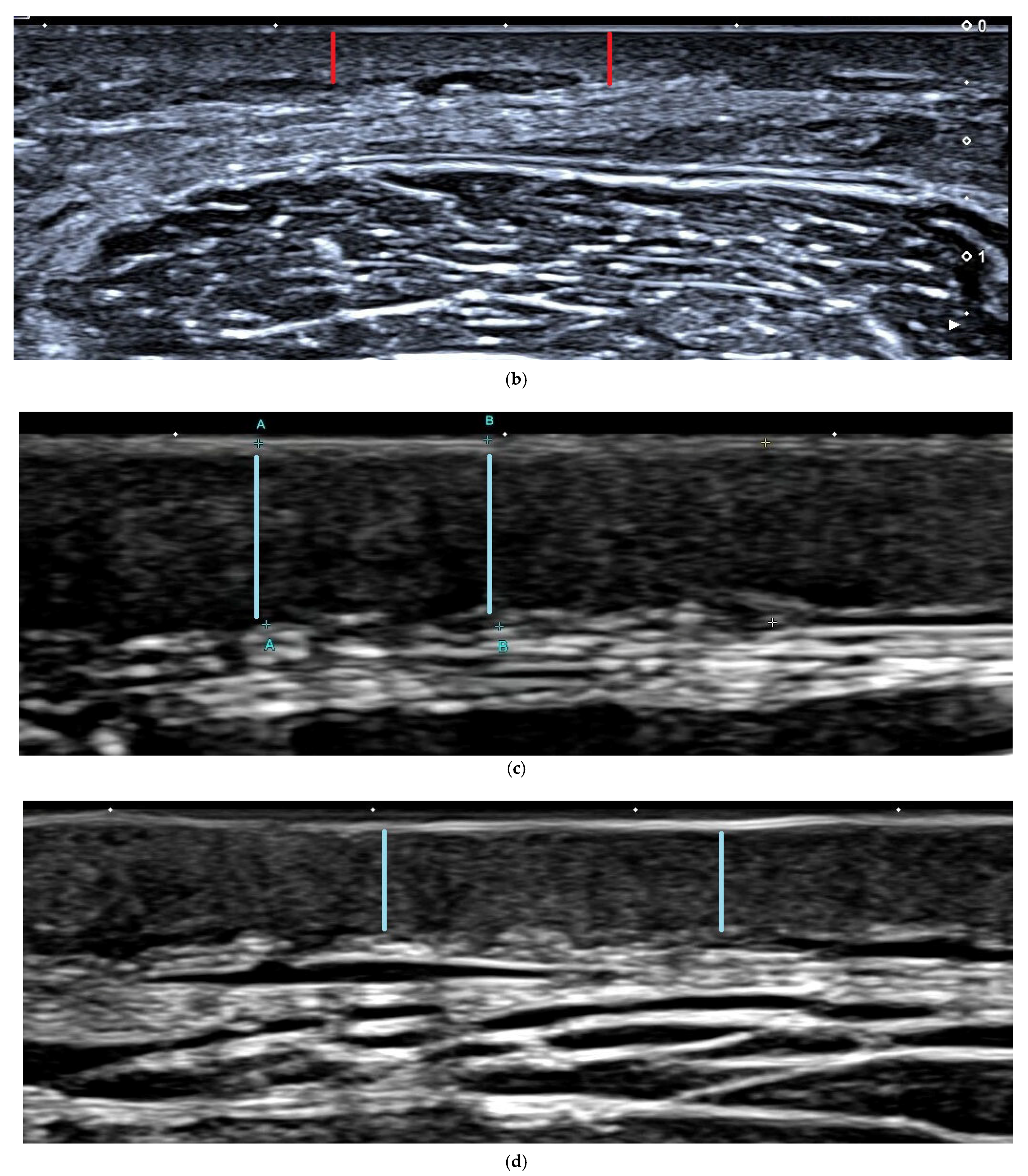
3.2. Ultrasound Assessment of Dermal Thickness
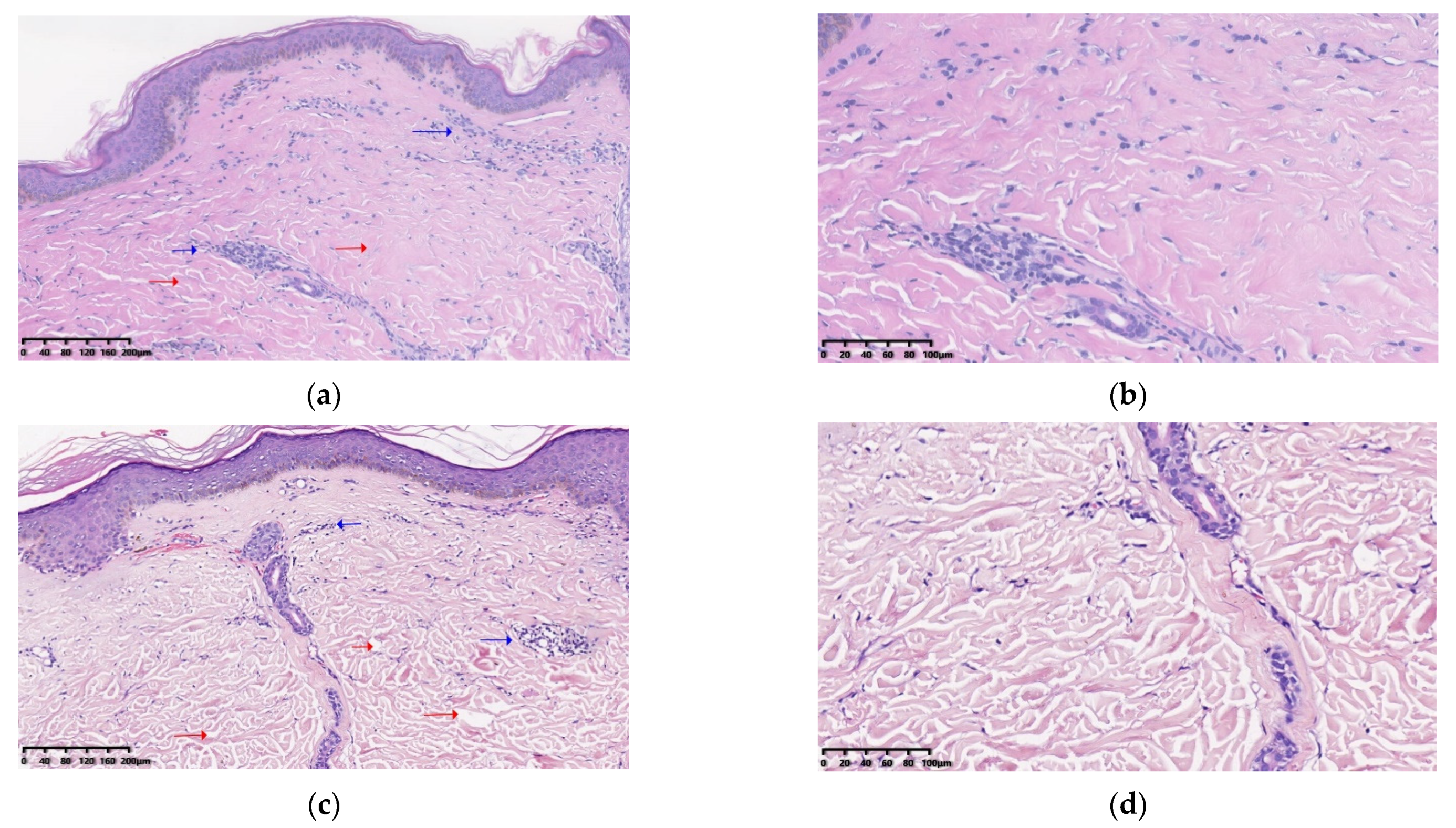
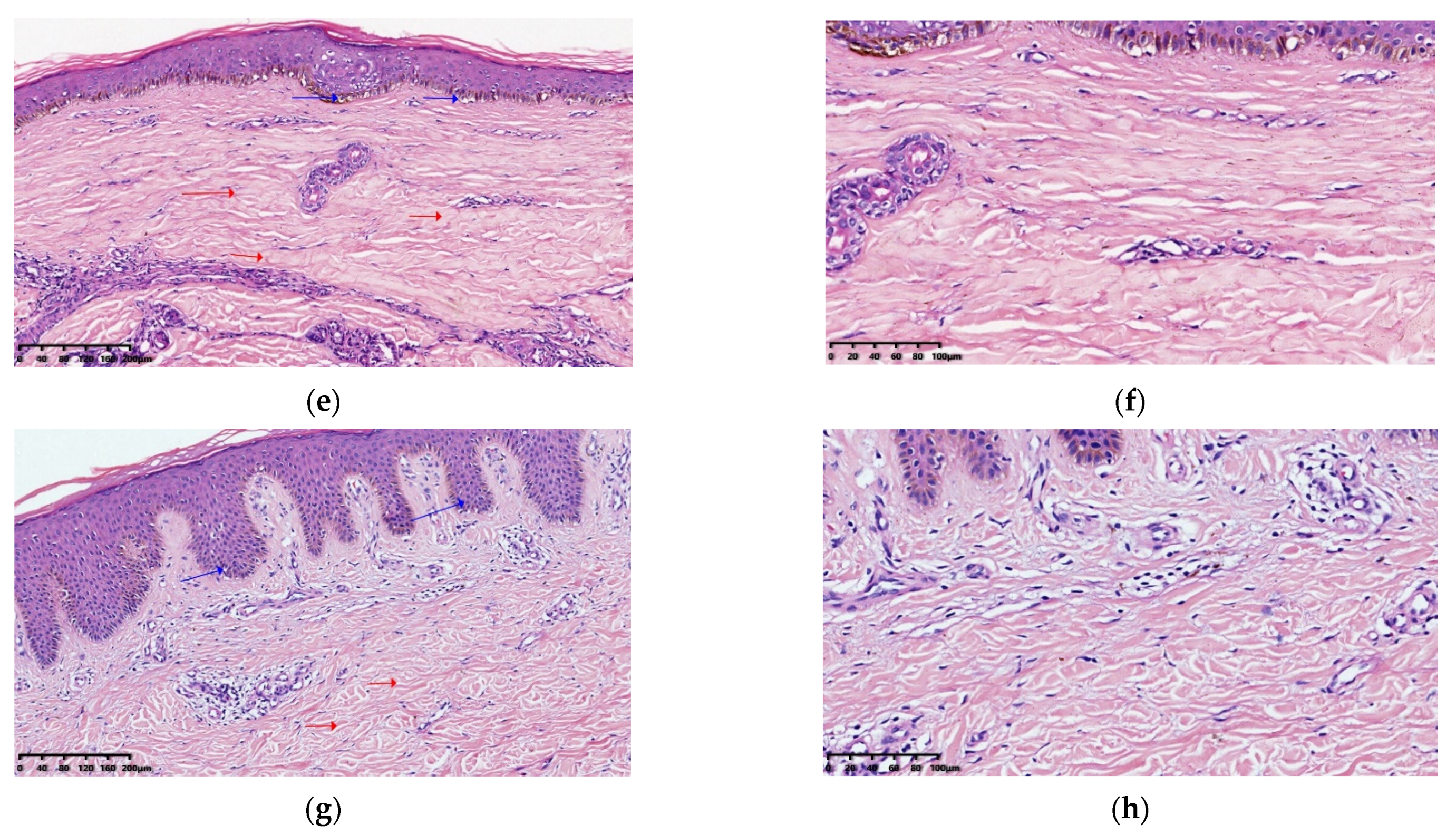
3.3. Histopathological Results
3.4. Safety Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kreuter, A.; Krieg, T.; Worm, M.; Wenzel, J.; Moinzadeh, P.; Kuhn, A.; Aberer, E.; Scharffetter-Kochanek, K.; Horneff, G.; Reil, E.; et al. German guidelines for the diagnosis and therapy of localized scleroderma. JDDG J. Dtsch. Dermatol. Ges. 2016, 14, 199–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peterson, L.S.; Nelson, A.M.; Su, W.P.; Mason, T.; O’Fallon, W.M.; Gabriel, S.E. The epidemiology of morphea (localized scleroderma) in Olmsted County 1960–1993. J. Rheumatol. 1997, 24, 73–80. [Google Scholar] [PubMed]
- Silman, A.; Jannini, S.; Symmons, D.; Bacon, P. An epidemiological study of scleroderma in the West Midlands. Br. J. Rheu. Matol. 1988, 27, 286–290. [Google Scholar] [CrossRef]
- Mayes, M.D. Classification and epidemiology of scleroderma. Semin. Cutan. Med. Surg. 1998, 17, 22–26. [Google Scholar] [CrossRef]
- Khatri, S.; Torok, K.S.; Mirizio, E.; Liu, C.; Astakhova, K. Autoantibodies in Morphea: An Update. Front. Immunol. 2019, 10, 1487. [Google Scholar] [CrossRef] [PubMed]
- Knobler, R.; Moinzadeh, P.; Hunzelmann, N.; Kreuter, A.; Cozzio, A.; Mouthon, L.; Cutolo, M.; Rongioletti, F.; Denton, C.P.; Rudnicka, L.; et al. European Dermatology Forum S1-guideline on the diagnosis and treatment of sclerosing diseases of the skin, Part 1: Localized scleroderma, systemic sclerosis and overlap syndromes. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 1401–1424. [Google Scholar] [CrossRef] [PubMed]
- Uziel, Y.; Feldman, B.M.; Krafchik, B.R.; Yeung, R.S.; Laxer, R.M. Methotrexate and corticosteroid therapy for pediatric localized scleroderma. J. Pediatr. 2000, 136, 91–95. [Google Scholar] [CrossRef]
- Platsidaki, E.; Tzanetakou, V.; Kouris, A.; Stavropoulos, P.G. Methotrexate: An effective monotherapy for refractory generalized morphea. Clin. Cosmet. Investig. Dermatol. 2017, 10, 165–169. [Google Scholar] [CrossRef] [Green Version]
- Cronstein, B.N.; Aune, T.M. Methotrexate and its mechanisms of action in inflammatory arthritis. Nat. Rev. Rheumatol. 2020, 16, 145–154. [Google Scholar] [CrossRef]
- Chan, E.S.; Cronstein, B.N. Methotrexate—How does it really work? Nat. Rev. Rheumatol. 2010, 6, 175–178. [Google Scholar] [CrossRef]
- Cronstein, B.N. Low-dose methotrexate: A mainstay in the treatment of rheumatoid arthritis. Pharmacol. Rev. 2005, 57, 163–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, S.; Fisher, K.H.; Snowden, J.A.; Danson, S.J.; Brown, S.; Zeidler, M.P. Methotrexate Is a JAK/STAT Pathway Inhibitor. PLoS ONE 2015, 10, e0130078. [Google Scholar] [CrossRef] [PubMed]
- Seyger, M.M.; van den Hoogen, F.H.; de Boo, T.; de Jong, E.M. Low-dose methotrexate in the treatment of widespread morphea. J. Am. Acad. Dermatol. 1998, 39 Pt 1, 220–225. [Google Scholar] [CrossRef]
- Van den Hoogen, F.H.J.; Boerbooms, A.M.T.; Swaak, A.J.G.; Rasker, J.J.; Van Lier, H.J.J.; Van De Putte, L.B.A. Comparison of methotrexate with placebo in the treatment of systemic sclerosis: A 24 week randomized double-blind trial, followed by a 24 week observational trial. Rheumatology 1996, 35, 364–372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nedelcu, R.I.; Balaban, M.; Turcu, G.; Brinzea, A.; Ion, D.A.; Antohe, M.; Hodorogea, A.; Calinescu, A.; Badarau, A.I.; Popp, C.G.; et al. Efficacy of methotrexate as anti-inflammatory and anti-proliferative drug in dermatology: Three case reports. Exp. Ther. Med. 2019, 18, 905–910. [Google Scholar] [CrossRef] [Green Version]
- Belgi, G.; Friedmann, P.S. Traditional therapies: Glucocorticoids, azathioprine, methotrexate, hydroxyurea. Clin. Exp. Dermatol. 2002, 27, 546–554. [Google Scholar] [CrossRef]
- Shalaby, S.M.; Bosseila, M.; Fawzy, M.M.; Abdel Halim, D.M.; Sayed, S.S.; Allam, R.S.H.M. Fractional carbon dioxide laser versus low-dose UVA-1 phototherapy for treatment of localized scleroderma: A clinical and immunohistochemical randomized controlled study. Lasers Med. Sci. 2016, 31, 1707–1715. [Google Scholar] [CrossRef]
- Wenande, E.; Anderson, R.R.; Haedersdal, M. Fundamentals of fractional laser-assisted drug delivery: An in-depth guide to experimental methodology and data interpretation. Adv. Drug Deliv. Rev. 2019, 153, 169–184. [Google Scholar] [CrossRef]
- Bay, C.; Lerche, C.M.; Ferrick, B.; Philipsen, P.A.; Togsverd-Bo, K.; Haedersdal, M. Comparison of Physical Pretreatment Regimens to Enhance Protoporphyrin IX Uptake in Photodynamic Therapy: A Randomized Clinical Trial. JAMA Dermatol. 2017, 153, 270–278. [Google Scholar] [CrossRef]
- Arkachaisri, T.; Vilaiyuk, S.; Torok, K.S.; Medsger, T.A., Jr. Development and initial validation of the localized scleroderma skin damage index and physician global assessment of disease damage: A proof-of-concept study. Rheumatology 2009, 49, 373–381. [Google Scholar] [CrossRef]
- Verrecchia, F.; Laboureau, J.; Verola, O.; Roos, N.; Porcher, R.; Bruneval, P.; Ertault, M.; Tiev, K.; Michel, L.; Mauviel, A.; et al. Skin involvement in scleroderma--where histological and clinical scores meet. Rheumatology 2007, 46, 833–841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kineston, D.; Kwan, J.M.; Uebelhoer, N.S.; Shumaker, P.R. Use of a fractional ablative 10.6-μm carbon dioxide laser in the treatment of a morphea-related contracture. Arch. Dermatol. 2011, 147, 1148–1150. [Google Scholar] [CrossRef] [PubMed]
- Farmer, C.; Griffith, J.L.; Lim, H.W.; Ozog, D.M. Fractionated CO2 laser for treatment of linear morphea: A case series. J. Am. Acad. Dermatol. 2018, 79, AB143. [Google Scholar] [CrossRef]
- Jiang, X.; Ge, H.; Zhou, C.; Chai, X.; Deng, H. The role of transforming growth factor β1 in fractional laser resurfacing with a carbon dioxide laser. Lasers Med. Sci. 2013, 29, 681–687. [Google Scholar] [CrossRef]
- Makboul, M.; Makboul, R.; Abdelhafez, A.H.; Hassan, S.S.; Youssif, S.M. Evaluation of the effect of fractional CO2 laser on histopathological picture and TGF-β1 expression in hypertrophic scar. J. Cosmet. Dermatol. 2014, 13, 169–179. [Google Scholar] [CrossRef]
- Szczepanik-Kułak, P.; Michalska-Jakubus, M.; Krasowska, D. Laser Therapy for the Treatment of Morphea: A Systematic Review of Literature. J. Clin. Med. 2021, 10, 3409. [Google Scholar] [CrossRef] [PubMed]
- Klimek, P.; Placek, W.; Owczarczyk-Saczonek, A. Fractional Ablative Carbon Dioxide Lasers for the Treatment of Morphea: A Case Series and Literature Review. Int. J. Environ. Res. Public Health 2022, 19, 8133. [Google Scholar] [CrossRef] [PubMed]
- Taudorf, E.H.; Lerche, C.M.; Vissing, A.C.; Philipsen, P.A.; Hannibal, J.; D’Alvise, J.; Hansen, S.H.; Janfelt, C.; Paasch, U.; Anderson, R.R.; et al. Topically applied methotrexate is rapidly delivered into skin by fractional laser ablation. Expert Opin. Drug Deliv. 2015, 12, 1059–1069. [Google Scholar] [CrossRef]
- Taudorf, E.H.; Lerche, C.M.; Erlendsson, A.M.; Philipsen, P.A.; Hansen, S.H.; Janfelt, C.; Paasch, U.; Anderson, R.R.; Hædersdal, M. Fractional laser-assisted drug delivery: Laser channel depth influences biodistribution and skin deposition of methotrexate. Lasers Surg. Med. 2016, 48, 519–529. [Google Scholar] [CrossRef]
- Nguyen, H.X.; Banga, A.K. Delivery of Methotrexate and Characterization of Skin Treated by Fabricated PLGA Micronee- dles and Fractional Ablative Laser. Pharm. Res. 2018, 35, 68. [Google Scholar] [CrossRef]
- Zulian, F.; Vallongo, C.; Patrizi, A.; Belloni-Fortina, A.; Cutrone, M.; Alessio, M.; Martino, S.; Gerloni, V.; Vittadello, F.; Martini, G. A long-term follow-up study of methotrexate in juvenile localized scleroderma (morphea). J. Am. Acad. Dermatol. 2012, 67, 1151–1156. [Google Scholar] [CrossRef] [PubMed]
- Segal, R.; Yaron, M.; Tartakovsky, B. Methotrexate: Mechanism of action in rheumatoid arthritis. Semin. Arthritis Rheum. 1990, 20, 190–200. [Google Scholar] [CrossRef]
- Zulian, F.; Martini, G.; Vallongo, C.; Vittadello, F.; Falcini, F.; Patrizi, A.; Alessio, M.; Torre, F.L.; Podda, R.A.; Gerloni, V.; et al. Methotrexate treatment in juvenile localized scleroderma: A randomized, double- blind, placebo-controlled trial. Arthritis Rheum. 2011, 63, 1998–2006. [Google Scholar] [CrossRef]
- Barrera, P.; Haagsma, C.J.; Boerbooms, A.M.; Van Riel, P.L.C.M.; Borm, G.F.; Van de Putte, L.B.A.; van der Meer, J.W. Effect of methotrexate alone or in combination with sulphasalazine on the production and circulating concentrations of cytokines and their antagonists. Longitudinal evaluation in patients with rheumatoid arthritis. Rheumatology 1995, 34, 747–755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ihn, H.; Sato, S.; Fujimoto, M.; Kikuchi, K.; Takehara, K. Demonstration of interleukin-2, interleukin-4 and interleukin-6 in sera from patients with localized scleroder ma. Arch. Dermatol. Res. 1995, 287, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Nieboer, M.J.; Meesters, A.A.; Almasian, M.; Georgiou, G.; de Rie, M.A.; Verdaasdonk, R.M.; Wolkerstorfer, A. Enhanced topical cutaneous delivery of indocyanine green after various pretreatment regimens: Comparison of fractional CO2 laser, fractional Er:YAG laser, microneedling, and radiofrequency. Lasers Med. Sci. 2020, 35, 1357–1365. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | AFL | AFL+MTX | p Value |
|---|---|---|---|
| Sex (n) | 11 | 11 | 1.000 |
| Male (n, %) | 2 (18.2) | 2 (18.2) | |
| Female (n, %) | 9 (81.8) | 9 (81.8) | |
| Age (mean ± SD), y | 34.82 ± 13.31 | 34.09 ± 9.75 | 0.885 |
| Disease type (n, %) | 1.000 | ||
| plaque type | 7 (63.6) | 6 (54.5) | |
| generalized type | 2 (18.2) | 2 (18.2) | |
| line type | 2 (18.2) | 3 (27.3) | |
| Disease stage (n, %) | 0.586 | ||
| edema stage | 0 (0.0) | 1 (9.1) | |
| sclerotic stage | 8 (72.7) | 9 (81.8) | |
| atrophic stage | 3 (27.3) | 1 (9.1) | |
| Total lesions (n) | 2 (1–3) | 2 (1–4) | 0.906 |
| Lesion area (cm2) | 36.00 (18.00–64.00) | 64.00 (35.00–154.00) | 0.156 |
| Duration (mean ± SD), y | 12.40 ± 9.52 | 6.29 ± 3.94 | 0.070 |
| AFL | AFL+MTX | p Value | |
|---|---|---|---|
| Before | 9 (8–14) | 11 (9–15) | 0.296 |
| After | 8 (6–14) | 4 (4–11) | 0.042 |
| p value | 0.041 | 0.005 | / |
| Dermal Thickness (mm) | AFL | AFL+MTX | p Value |
|---|---|---|---|
| Before | 1.723 (1.352–2.382) | 2.084 (1.653–2.383) | / |
| After | 1.589 (1.206–2.296) | 1.800 (1.393–2.154) | / |
| Δd | 0.138 ± 0.085 | 0.323 ± 0.205 | 0.016 |
| p value | 0.001 | 0.001 | / |
| Group | Treatment | n | Grade 1 | Grade 2 | Grade 3 | p Value |
|---|---|---|---|---|---|---|
| AFL | Before | 11 | 0 | 5 | 6 | 0.035 |
| After | 11 | 2 | 8 | 1 | ||
| AFL+MTX | Before | 11 | 0 | 5 | 6 | 0.004 |
| After | 11 | 4 | 7 | 0 |
| AFL (n = 11) | AFL+MTX (n = 11) | p Value | ||
|---|---|---|---|---|
| Pain | Number of patients | 11 | 11 | |
| Duration (day) | 1.64 ± 0.81 | 1.82 ± 0.75 | 0.618 | |
| Redness | Number of patients | 11 | 11 | |
| Duration (day) | 2.00 ± 0.632 | 2.09 ± 0.632 | 0.465 | |
| Crust | Number of patients | 11 | 11 | |
| Decrustation (day) | 7.82 ± 1.25 | 6.91 ± 1.30 | 0.110 | |
| Pigmentation | Number of patients | 6 | 6 | |
| Duration (day) | 34.00 ± 15.52 | 39.67 ± 20.63 | 0.603 | |
| Infection | Number of patients | 0 | 0 | |
| Scarring | Number of patients | 0 | 0 | |
| DLQI score | 3.91 ± 5.15 | 6.36 ± 5.46 | 0.291 | |
| Satisfaction score | 1.73 ± 1.19 | 2.18 ± 0.87 | 0.401 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, Q.; He, M.; Cen, J.; Huang, D.; Hao, S.; Tang, Z.; Xiong, H. Efficacy and Safety of Ablative Fractional Laser-Assisted Delivery of Methotrexate in Adults with Localized Scleroderma: A Randomized and Controlled Clinical Trial. Pharmaceutics 2022, 14, 2261. https://doi.org/10.3390/pharmaceutics14112261
Guo Q, He M, Cen J, Huang D, Hao S, Tang Z, Xiong H. Efficacy and Safety of Ablative Fractional Laser-Assisted Delivery of Methotrexate in Adults with Localized Scleroderma: A Randomized and Controlled Clinical Trial. Pharmaceutics. 2022; 14(11):2261. https://doi.org/10.3390/pharmaceutics14112261
Chicago/Turabian StyleGuo, Qing, Mingjie He, Junjie Cen, Danqi Huang, Shaoyun Hao, Zengqi Tang, and Hui Xiong. 2022. "Efficacy and Safety of Ablative Fractional Laser-Assisted Delivery of Methotrexate in Adults with Localized Scleroderma: A Randomized and Controlled Clinical Trial" Pharmaceutics 14, no. 11: 2261. https://doi.org/10.3390/pharmaceutics14112261