
Hemostatic Alginate/Nano-Hydroxyapatite Composite Aerogel Loaded with Tranexamic Acid for the Potential Protection against Alveolar Osteitis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Methodology
2.2.1. Preparation of Simulated Body Fluid
2.2.2. Preparation of Alginate/Nano-Hydroxyapatite Composite Aerogel Loaded with Tranexamic Acid
Experimental Design
Method of Preparation
2.2.3. In Vitro Characterization of Alginate/Nano-Hydroxyapatite Composite Aerogel Loaded with Tranexamic Acid
Drug Content
Matrix Porosity
Swelling Properties
In Vitro Release of Tranexamic Acid
Linear Regression Analysis
Fourier Transform Infrared Spectroscopy
Scanning Electron Microscopy
2.2.4. Blood Coagulation Study
Assessment of Whole Blood Clotting Time
Plasma Recalcification Time
Platelet Adhesion
In Vitro Dynamic Blood Clotting Index
2.2.5. Indirect Cell Migration Assay
2.2.6. Statistical Analysis
3. Results and Discussion
3.1. Physical Properties of the Prepared Alginate/Nano-Hydroxyapatite Aerogels Loaded with Tranexamic Acid
3.2. Drug Content
3.3. Matrix Porosity
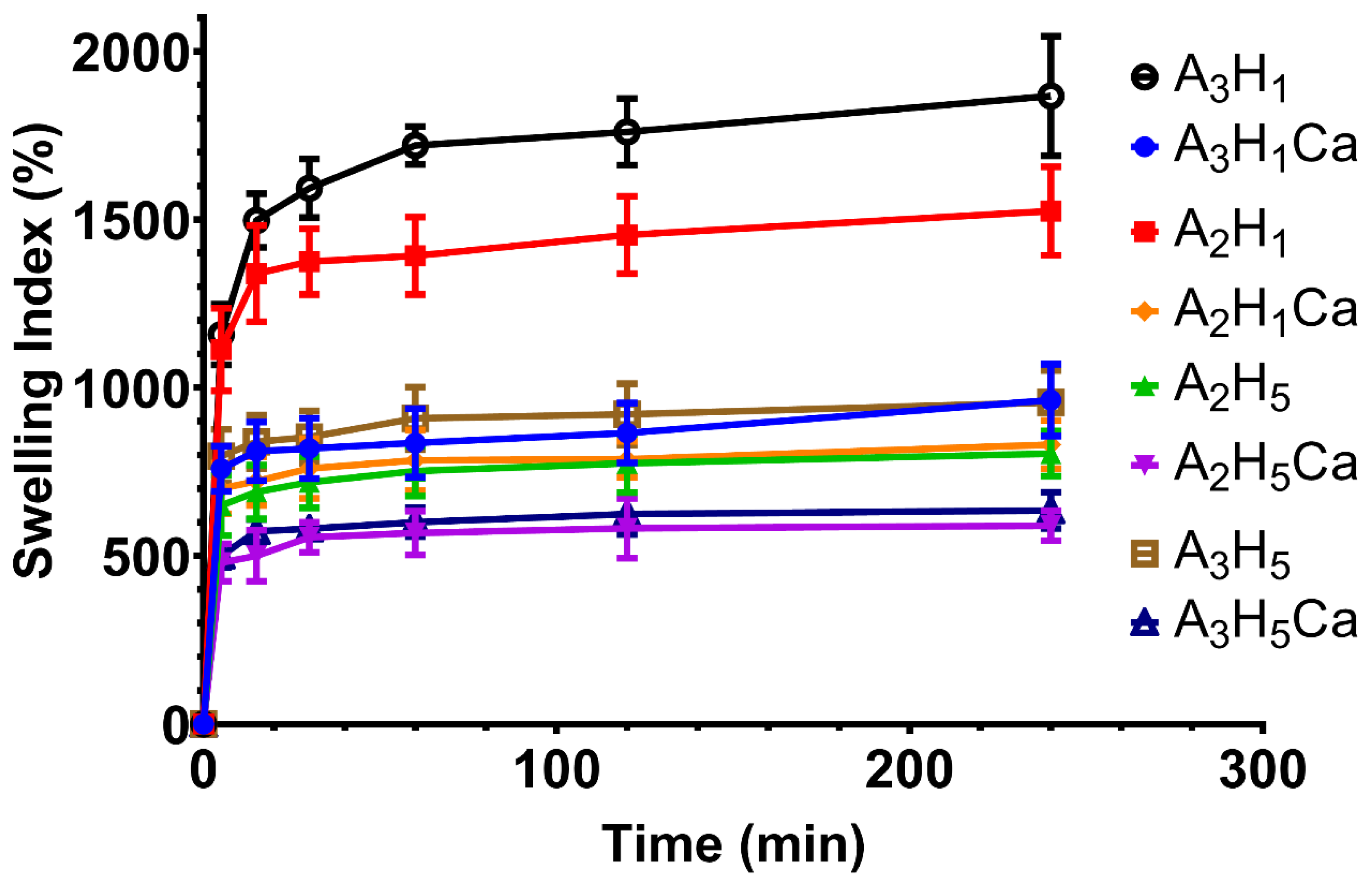
3.4. Determination of Swelling Properties
3.5. In Vitro Drug Release of TXA from Alginate/Nano-Hydroxyapatite Aerogels
3.6. Selection of the Optimized Formula
3.7. Fourier Transform Infrared Spectroscopy
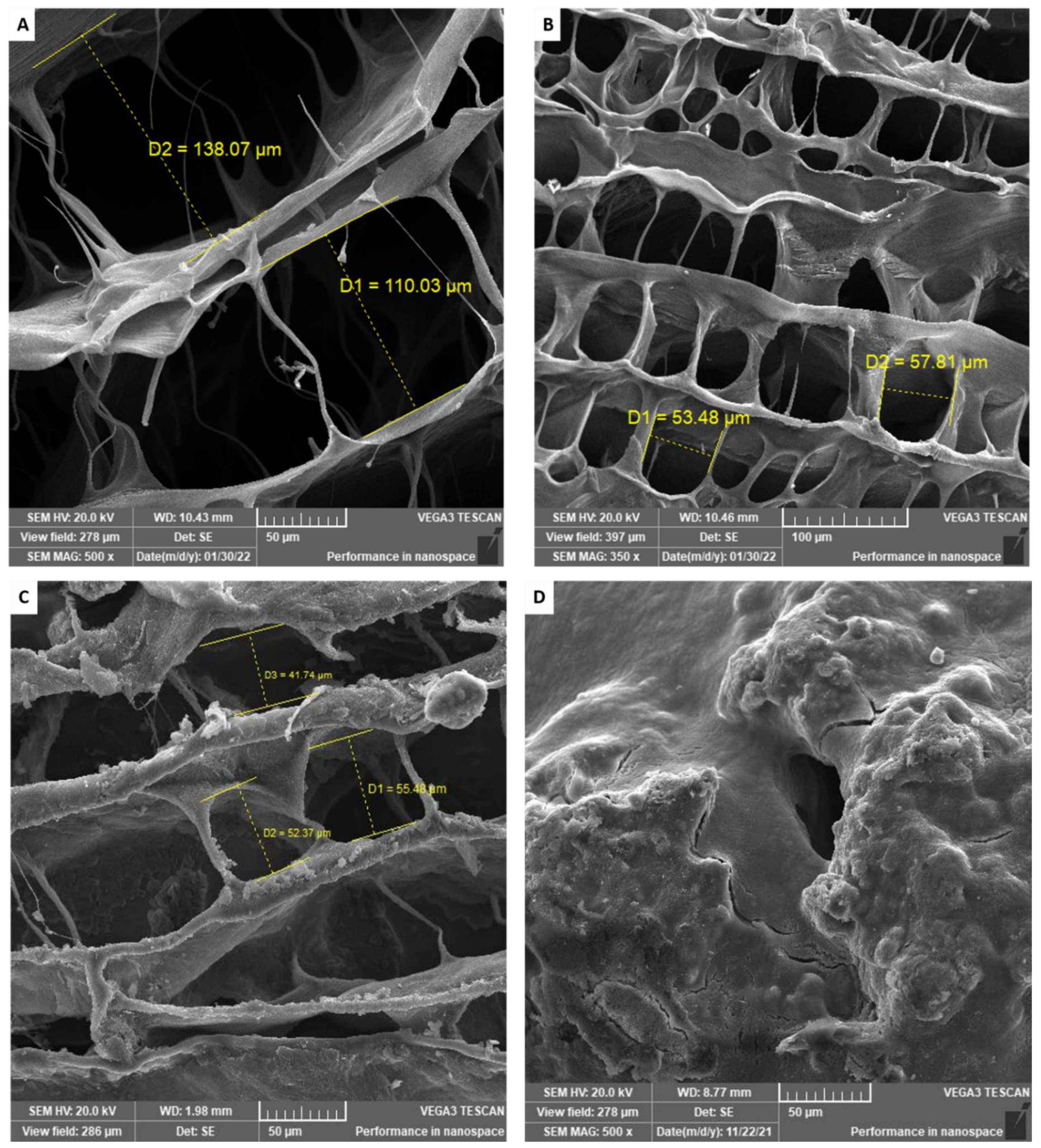
3.8. Scanning Electron Microscopy
3.9. Blood Coagulation Studies
3.9.1. Assessment of Whole Blood Clotting Time
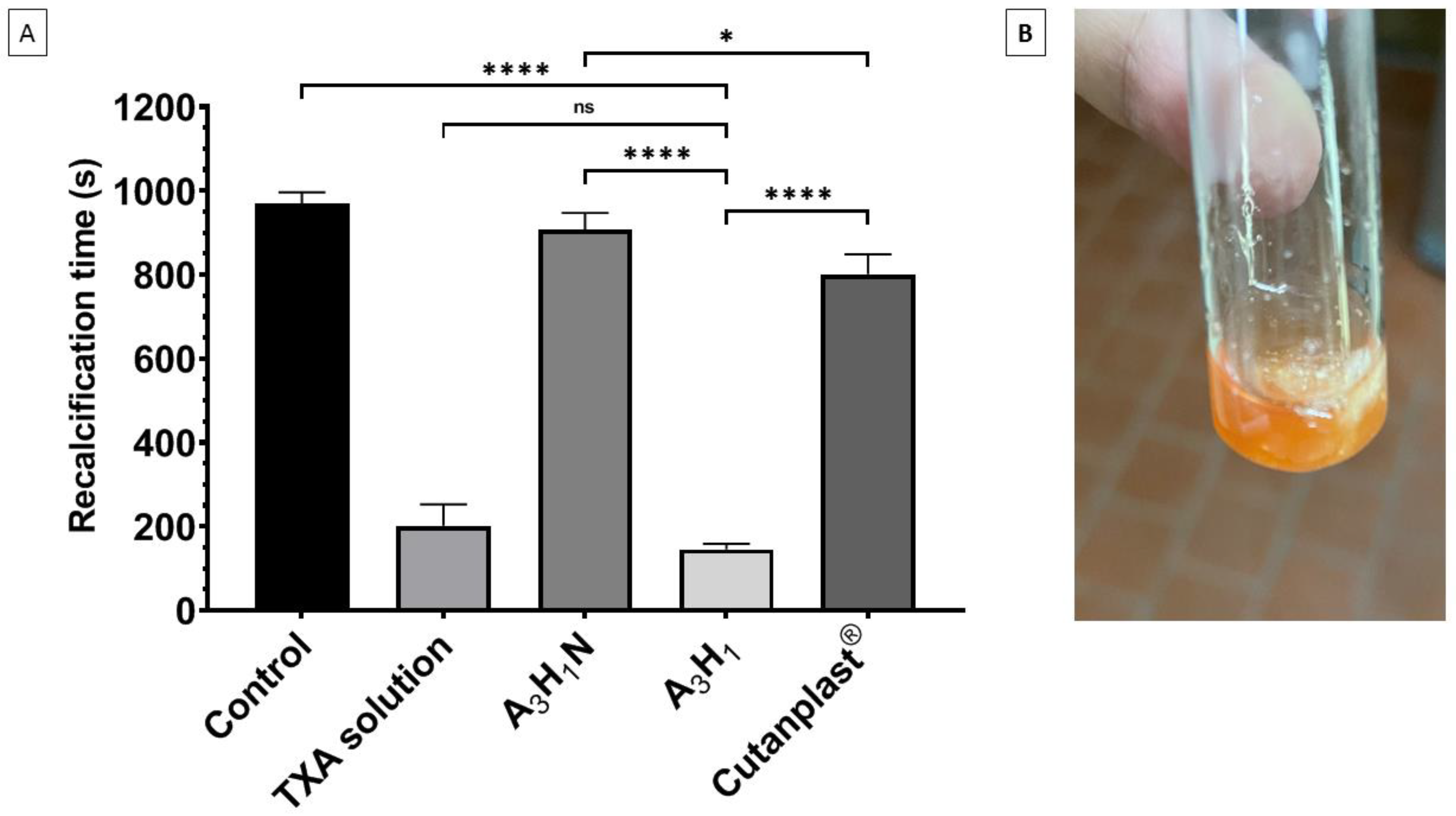
3.9.2. Plasma Recalcification Time
3.9.3. Platelet Adhesion
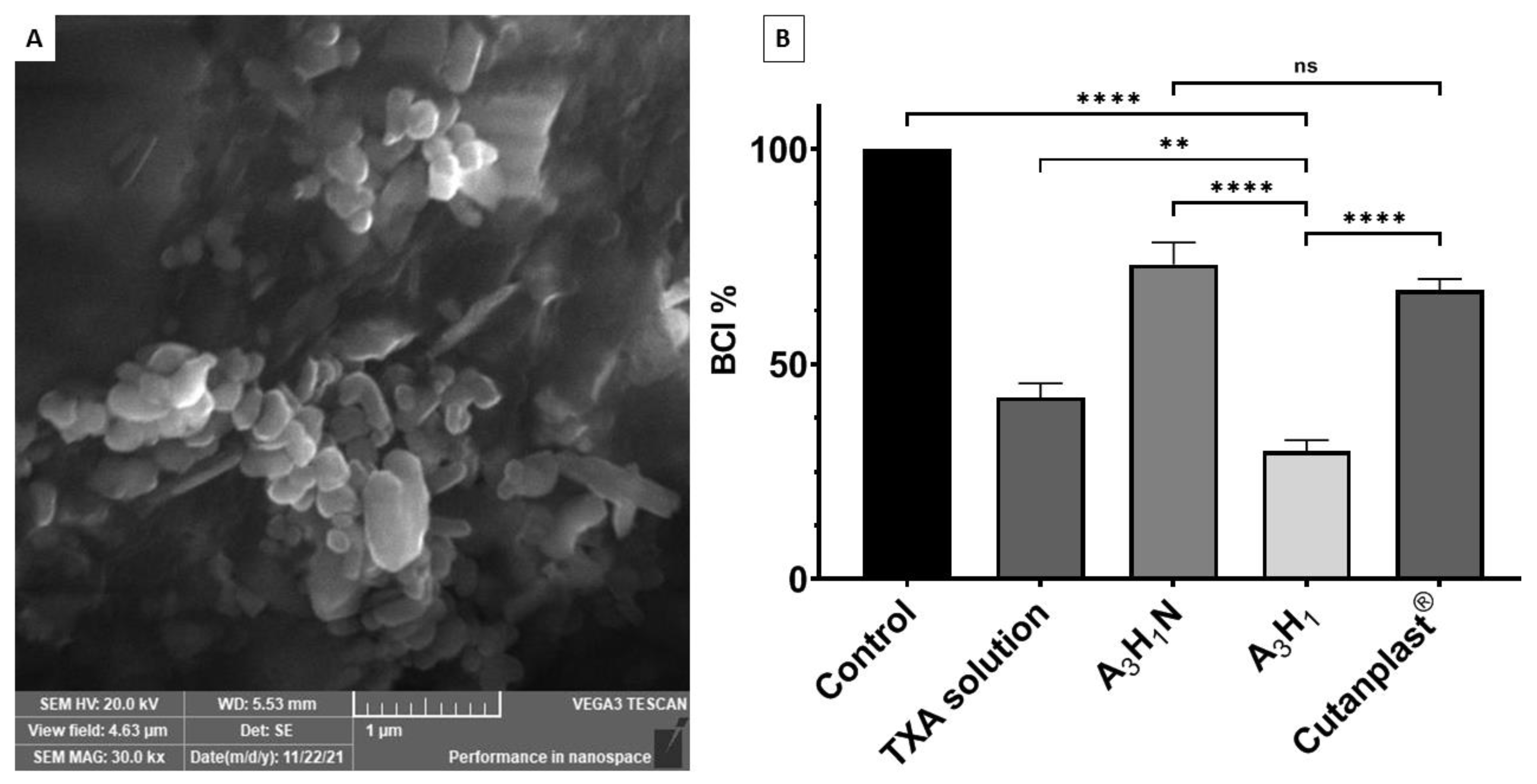
3.9.4. In Vitro Dynamic Blood Clotting Index
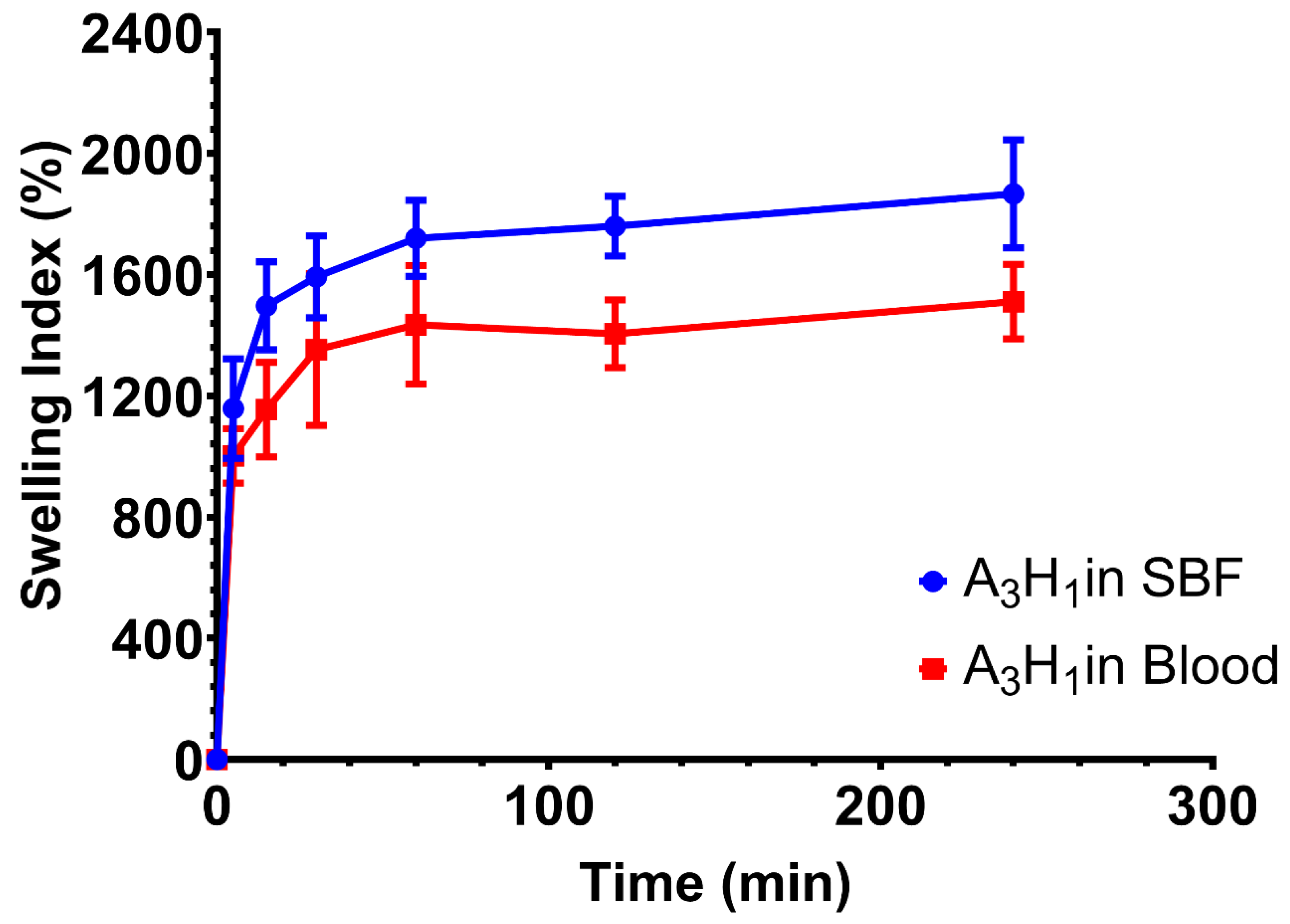
3.10. Swelling of the Optimum Aerogel in Blood
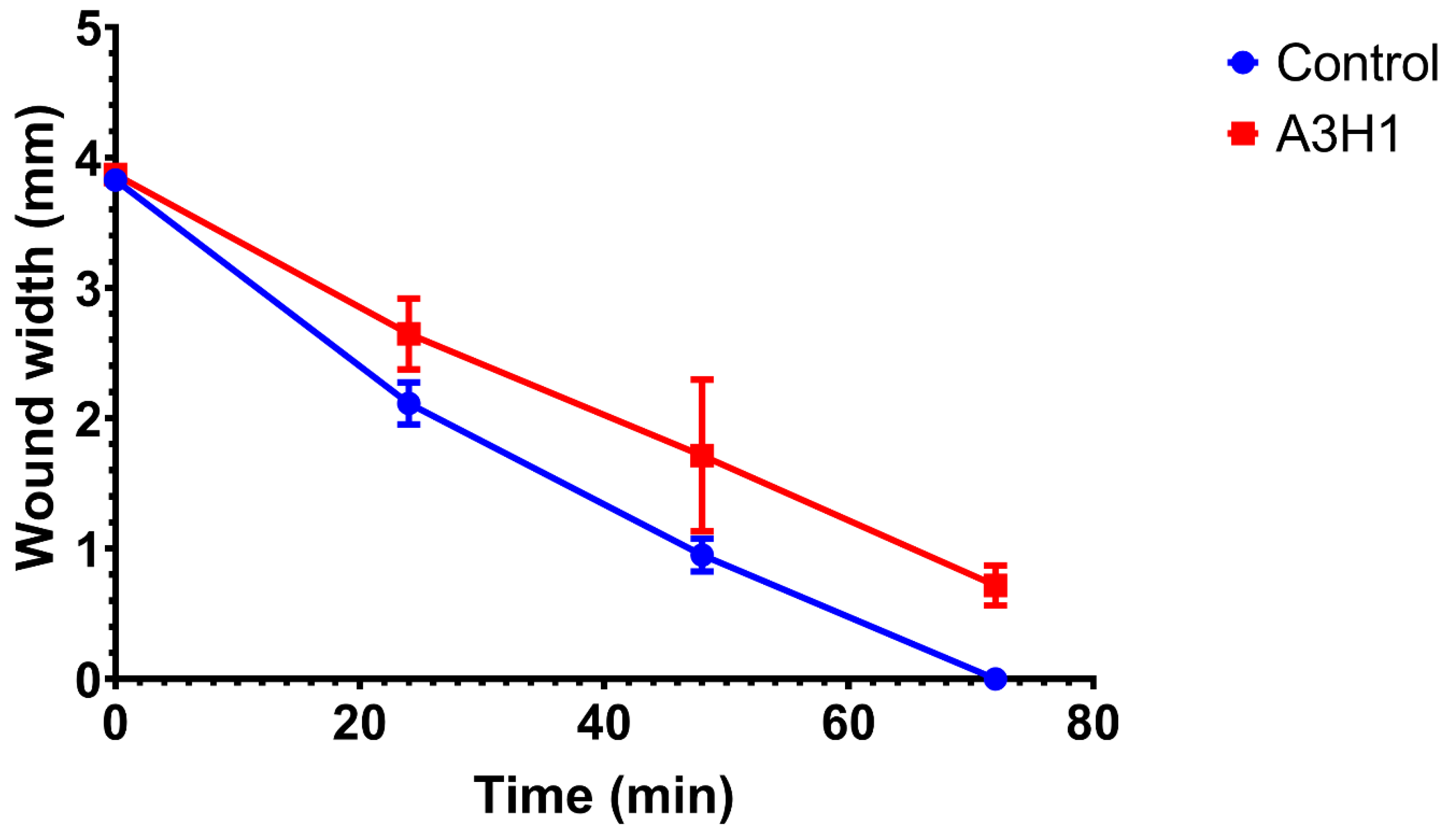
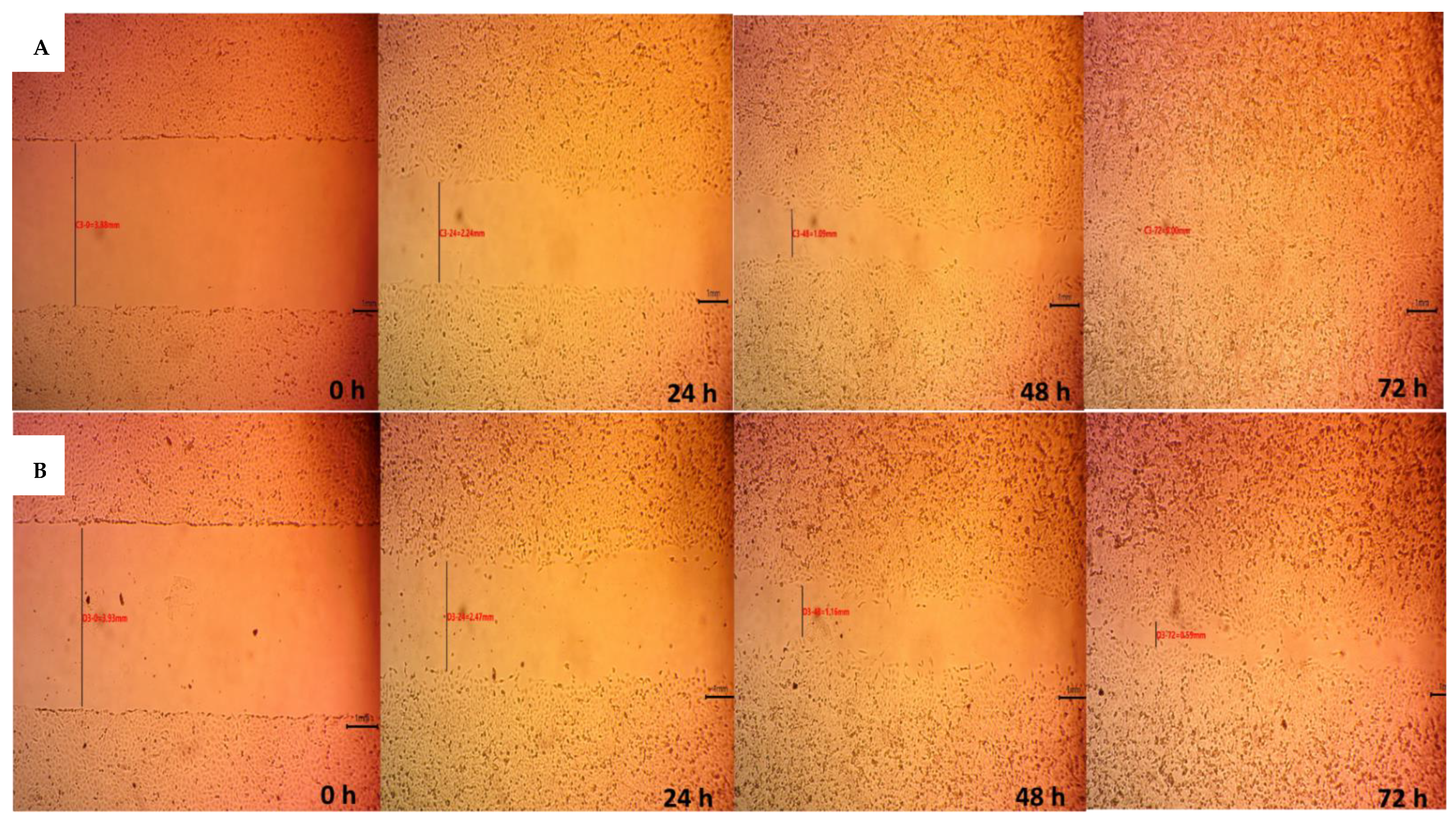
3.11. Indirect Cell Migration Assay
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chow, O.; Wang, R.; Ku, D.; Huang, W. Alveolar osteitis: A review of current concepts. J. Oral Maxillofac. Surg. 2020, 78, 1288–1296. [Google Scholar] [CrossRef]
- Akinbami, B.O.; Godspower, T. Dry socket: Incidence, clinical features, and predisposing factors. Int. J. Dent. 2014, 2014, 796102. [Google Scholar] [CrossRef]
- Noroozi, A.-R.; Philbert, R.F. Modern concepts in understanding and management of the “dry socket” syndrome: Comprehensive review of the literature. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2009, 107, 30–35. [Google Scholar] [CrossRef]
- Kolokythas, A.; Olech, E.; Miloro, M. Alveolar Osteitis: A Comprehensive Review of Concepts and Controversies. Int. J. Dent. 2010, 2010, 249073. [Google Scholar] [CrossRef] [Green Version]
- Delilbasi, C.; Saracoglu, U.; Keskin, A. Effects of 0.2% chlorhexidine gluconate and amoxicillin plus clavulanic acid on the prevention of alveolar osteitis following mandibular third molar extractions. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2002, 94, 301–304. [Google Scholar] [CrossRef] [PubMed]
- Haraji, A.; Rakhshan, V.; Khamverdi, N.; Alishahi, H. Effects of Intra-alveolar Placement of 0.2% Chlorhexidine Bioadhesive Gel on Dry Socket Incidence and Postsurgical Pain: A Double-Blind Split-Mouth Randomized Controlled Clinical Trial. J. Orofac. Pain 2013, 27, 256–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anand, K.P.; Patro, S.; Mohapatra, A.; Mishra, S. The Efficacy of Tranexamic Acid in the Reduction of Incidence of Dry Socket: An Institutional Double Blind Study. J. Clin. Diagn. Res. 2015, 9, ZC25–ZC28. [Google Scholar] [CrossRef] [PubMed]
- Madrid, C.; Sanz, M. What influence do anticoagulants have on oral implant therapy? A systematic review. Clin. Oral Implant. Res. 2009, 20, 96–106. [Google Scholar] [CrossRef]
- Cho, Y.-W.; Kim, E. Is stopping of anticoagulant therapy really required in a minor dental surgery?—How about in an endodontic microsurgery? Restor. Dent. Endod. 2013, 38, 113–118. [Google Scholar] [CrossRef]
- Isola, G.; Matarese, G.; Cordasco, G.; Rotondo, F.; Crupi, A.; Ramaglia, L. Anticoagulant therapy in patients undergoing dental interventions: A critical review of the literature and current perspectives. Minerva Stomatol. 2015, 64, 21–46. [Google Scholar]
- Bjorlin, G.; Nilsson, I.M. The effect of antifibrinolytic agents on wound healing. Int. J. Oral Maxillofac. Surg. 1988, 17, 275–276. [Google Scholar] [CrossRef]
- Law, R.H.P.; Wu, G.; Leung, E.W.W.; Hidaka, K.; Quek, A.J.; Caradoc-Davies, T.T.; Jeevarajah, D.; Conroy, P.J.; Kirby, N.M.; Norton, R.S.; et al. X-ray crystal structure of plasmin with tranexamic acid–derived active site inhibitors. Blood Adv. 2017, 1, 766–771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pilbrant, Å.; Schannong, M.; Vessman, J. Pharmacokinetics and bioavailability of tranexamic acid. Eur. J. Clin. Pharmacol. 1981, 20, 65–72. [Google Scholar] [CrossRef]
- Sindet-Pedersen, S.; Ramström, G.; Bernvil, S.; Blombäck, M. Hemostatic Effect of Tranexamic Acid Mouthwash in Anticoagulant-Treated Patients Undergoing Oral Surgery. N. Engl. J. Med. 1989, 320, 840–843. [Google Scholar] [CrossRef] [PubMed]
- Zheng, L.; Zhang, S.; Ying, Z.; Liu, J.; Zhou, Y.; Chen, F. Engineering of Aerogel-Based Biomaterials for Biomedical Applications. Int. J. Nanomed. 2020, 15, 2363–2378. [Google Scholar] [CrossRef] [Green Version]
- Bonnans, C.; Chou, J.; Werb, Z. Remodelling the extracellular matrix in development and disease. Nat. Rev. Mol. Cell Biol. 2014, 15, 786–801. [Google Scholar] [CrossRef]
- Du, A.; Zhou, B.; Zhang, Z.; Shen, J. A Special Material or a New State of Matter: A Review and Reconsideration of the Aerogel. Materials 2013, 6, 941. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sani, N.S.; Malek, N.A.N.N.; Jemon, K.; Kadir, M.R.A.; Hamdan, H. Preparation and characterization of hydroxyapatite incorporated silica aerogel and its effect on normal human dermal fibroblast cells. J. Sol-Gel Sci. Technol. 2019, 90, 422–433. [Google Scholar] [CrossRef]
- Concha, M.; Vidal, A.; Giacaman, A.; Ojeda, J.; Pavicic, F.; Oyarzun-Ampuero, F.A.; Torres, C.; Cabrera, M.; Moreno-Villoslada, I.; Orellana, S.L. Aerogels made of chitosan and chondroitin sulfate at high degree of neutralization: Biological properties toward wound healing. J. Biomed. Mater. Res. Part B Appl. Biomater. 2018, 106, 2464–2471. [Google Scholar] [CrossRef]
- Barrios, E.; Fox, D.; Li Sip, Y.Y.; Catarata, R.; Calderon, J.E.; Azim, N.; Afrin, S.; Zhang, Z.; Zhai, L. Nanomaterials in Advanced, High-Performance Aerogel Composites: A Review. Polymers 2019, 11, 726. [Google Scholar] [CrossRef] [Green Version]
- Boateng, J.; Catanzano, O. Advanced Therapeutic Dressings for Effective Wound Healing—A Review. J. Pharm. Sci. 2015, 104, 3653–3680. [Google Scholar] [CrossRef] [PubMed]
- Blair, S.D.; Jarvis, P.; Salmon, M.; McCollum, C. Clinical trial of calcium alginate haemostatic swabs. Br. J. Surg. 1990, 77, 568–570. [Google Scholar] [CrossRef] [PubMed]
- Rajkumar, M.; Meenakshisundaram, N.; Rajendran, V. Development of nanocomposites based on hydroxyapatite/sodium alginate: Synthesis and characterisation. Mater. Charact. 2011, 62, 469–479. [Google Scholar] [CrossRef]
- Ma, L.; Su, W.; Ran, Y.; Ma, X.; Yi, Z.; Chen, G.; Chen, X.; Deng, Z.; Tong, Q.; Wang, X.; et al. Synthesis and characterization of injectable self-healing hydrogels based on oxidized alginate-hybrid-hydroxyapatite nanoparticles and carboxymethyl chitosan. Int. J. Biol. Macromol. 2020, 165, 1164–1174. [Google Scholar] [CrossRef]
- Gholizadeh, B.S.; Buazar, F.; Hosseini, S.M.; Mousavi, S.M. Enhanced antibacterial activity, mechanical and physical properties of alginate/hydroxyapatite bionanocomposite film. Int. J. Biol. Macromol. 2018, 116, 786–792. [Google Scholar] [CrossRef]
- Sancilio, S.; Gallorini, M.; Di Nisio, C.; Marsich, E.; Di Pietro, R.; Schweikl, H.; Cataldi, A. Alginate/Hydroxyapatite-Based Nanocomposite Scaffolds for Bone Tissue Engineering Improve Dental Pulp Biomineralization and Differentiation. Stem Cells Int. 2018, 2018, 9643721. [Google Scholar] [CrossRef] [Green Version]
- Jin, H.-H.; Kim, D.-H.; Kim, T.-W.; Shin, K.-K.; Jung, J.S.; Park, H.-C.; Yoon, S.-Y. In vivo evaluation of porous hydroxyapatite/chitosan–alginate composite scaffolds for bone tissue engineering. Int. J. Biol. Macromol. 2012, 51, 1079–1085. [Google Scholar] [CrossRef]
- Hench, L.L. Bioceramics: From Concept to Clinic. J. Am. Ceram. Soc. 1991, 74, 1487–1510. [Google Scholar] [CrossRef] [Green Version]
- Oguchi, H. Long-term histological evaluation of hydroxyapatite ceramics in humans. Biomaterials 1995, 16, 33–38. [Google Scholar] [CrossRef]
- Li, D.; Li, P.; Zang, J.; Liu, J. Enhanced Hemostatic Performance of Tranexamic Acid-Loaded Chitosan/Alginate Composite Microparticles. J. Biomed. Biotechnol. 2012, 2012, 981321. [Google Scholar] [CrossRef] [Green Version]
- Fatahian, R.; Mirjalili, M.; Khajavi, R.; Rahimi, M.K.; Nasirizadeh, N. A novel hemostat and antibacterial nanofibrous scaffold based on poly(vinyl alcohol)/poly(lactic acid). J. Bioact. Compat. Polym. 2020, 35, 189–202. [Google Scholar] [CrossRef]
- Zhong, Q.-K.; Wu, Z.-Y.; Qin, Y.-Q.; Hu, Z.; Li, S.-D.; Yang, Z.-M.; Li, P.-W. Preparation and Properties of Carboxymethyl Chitosan/Alginate/Tranexamic Acid Composite Films. Membranes 2019, 9, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adel, I.M.; ElMeligy, M.F.; Abdelkhalek, A.A.; Elkasabgy, N.A. Design and characterization of highly porous curcumin loaded freeze-dried wafers for wound healing. Eur. J. Pharm. Sci. 2021, 164, 105888. [Google Scholar] [CrossRef] [PubMed]
- Catanzano, O.; D’Esposito, V.; Formisano, P.; Boateng, J.S.; Quaglia, F. Composite Alginate-Hyaluronan Sponges for the Delivery of Tranexamic Acid in Postextractive Alveolar Wounds. J. Pharm. Sci. 2018, 107, 654–661. [Google Scholar] [CrossRef]
- Olejnik, A.; Goscianska, J.; Nowak, I. Active Compounds Release from Semisolid Dosage Forms. J. Pharm. Sci. 2012, 101, 4032–4045. [Google Scholar] [CrossRef]
- Ansari, T.M.; Raza, A.; Rehman, A.U. Spectrophotometric determination of tranexamic acid in pharmaceutical bulk and dosage forms. Anal. Sci. 2005, 21, 1133–1135. [Google Scholar] [CrossRef] [Green Version]
- Higuchi, T. Mechanism of sustained-action medication. Theoretical analysis of rate of release of solid drugs dispersed in solid matrices. J. Pharm. Sci. 1963, 52, 1145–1149. [Google Scholar] [CrossRef]
- Sasmal, P.; Datta, P. Tranexamic acid-loaded chitosan electrospun nanofibers as drug delivery system for hemorrhage control applications. J. Drug Deliv. Sci. Technol. 2019, 52, 559–567. [Google Scholar] [CrossRef]
- Hu, Z.; Lu, S.; Cheng, Y.; Kong, S.; Li, S.; Li, C.; Yang, L. Investigation of the Effects of Molecular Parameters on the Hemostatic Properties of Chitosan. Molecules 2018, 23, 3147. [Google Scholar] [CrossRef] [Green Version]
- Martinotti, S.; Ranzato, E. Scratch Wound Healing Assay. In Epidermal Cells; Methods in Molecular Biology Series; Springer: New York, NY, USA, 2019; pp. 225–229. [Google Scholar] [CrossRef]
- Silva, M.d.S.; Neto, N.L.; da Costa, S.A.; da Costa, S.M.; Oliveira, T.M.; Oliveira, R.C.d.; Machado, M.A.A.M. Biophysical and biological characterization of intraoral multilayer membranes as potential carriers: A new drug delivery system for dentistry. Mater. Sci. Eng. C 2017, 71, 498–503. [Google Scholar] [CrossRef]
- Han, F.; Dong, Y.; Su, Z.; Yin, R.; Song, A.; Li, S. Preparation, characteristics and assessment of a novel gelatin–chitosan sponge scaffold as skin tissue engineering material. Int. J. Pharm. 2014, 476, 124–133. [Google Scholar] [CrossRef] [PubMed]
- Quan, K.; Li, G.; Luan, D.; Yuan, Q.; Tao, L.; Wang, X. Black hemostatic sponge based on facile prepared cross-linked graphene. Colloids Surf. B Biointerfaces 2015, 132, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Ahmad Raus, R.; Wan Nawawi, W.M.F.; Nasaruddin, R.R. Alginate and alginate composites for biomedical applications. Asian J. Pharm. Sci. 2021, 16, 280–306. [Google Scholar] [CrossRef] [PubMed]
- Varshosaz, J.; Choopannejad, Z.; Minaiyan, M.; Kharazi, A.Z. Rapid hemostasis by nanofibers of polyhydroxyethyl methacrylate/polyglycerol sebacic acid: An in vitro in vivo study. J. Appl. Polym. Sci. 2020, 138, 49785. [Google Scholar] [CrossRef]
- Draget, K.I.; Taylor, C. Chemical, physical and biological properties of alginates and their biomedical implications. Food Hydrocoll. 2011, 25, 251–256. [Google Scholar] [CrossRef]
- Bialik-Wąs, K.; Pluta, K.; Malina, D.; Majka, T.M. Alginate/PVA-based hydrogel matrices with Echinacea purpurea extract as a new approach to dermal wound healing. Int. J. Polym. Mater. Polym. Biomater. 2019, 70, 195–206. [Google Scholar] [CrossRef]
- Patel, M.A.; AbouGhaly, M.H.H.; Schryer-Praga, J.V.; Chadwick, K. The effect of ionotropic gelation residence time on alginate cross-linking and properties. Carbohydr. Polym. 2017, 155, 362–371. [Google Scholar] [CrossRef]
- Ching, A.L.; Liew, C.V.; Heng, P.W.S.; Chan, L.W. Impact of cross-linker on alginate matrix integrity and drug release. Int. J. Pharm. 2008, 355, 259–268. [Google Scholar] [CrossRef]
- Gentry, P.A.; Liptrap, R.M. Comparative hemostatic protein alterations accompanying pregnancy and parturition. Can. J. Physiol. Pharmacol. 1988, 66, 671–678. [Google Scholar] [CrossRef]
- Janvikul, W.; Uppanan, P.; Thavornyutikarn, B.; Krewraing, J.; Prateepasen, R. In vitro comparative hemostatic studies of chitin, chitosan, and their derivatives. J. Appl. Polym. Sci. 2006, 102, 445–451. [Google Scholar] [CrossRef]
- Abraham, S.; So, A.; Unsworth, L.D. Poly(carboxybetaine methacrylamide)-modified nanoparticles: A model system for studying the effect of chain chemistry on film properties, adsorbed protein conformation, and clot formation kinetics. Biomacromolecules 2011, 12, 3567–3580. [Google Scholar] [CrossRef] [PubMed]
- Grimaldi, A.; Rosso, F.; Barbarisi, A. Biotechnological Approaches to Hemostasis and Molecular Mechanisms of Wound Healing. In Biotechnology in Surgery; Barbarisi, A., Ed.; Springer: Milan, Italy, 2011; pp. 105–114. [Google Scholar] [CrossRef]
- Pleines, I.; Eckly, A.; Elvers, M.; Hagedorn, I.; Eliautou, S.; Bender, M.; Wu, X.; Lanza, F.; Gachet, C.; Brakebusch, C.; et al. Multiple alterations of platelet functions dominated by increased secretion in mice lacking Cdc42 in platelets. Blood 2010, 115, 3364–3373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Unnithan, A.R.; Gnanasekaran, G.; Sathishkumar, Y.; Lee, Y.S.; Kim, C.S. Electrospun antibacterial polyurethane–cellulose acetate–zein composite mats for wound dressing. Carbohydr. Polym. 2014, 102, 884–892. [Google Scholar] [CrossRef] [PubMed]
- Su, H.; Wei, S.; Chen, F.; Cui, R.; Liu, C. Tranexamic acid-loaded starch hemostatic microspheres. RSC Adv. 2019, 9, 6245–6253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pastar, I.; Liang, L.; Sawaya, A.P.; Wikramanayake, T.C.; Glinos, G.D.; Drakulich, S.; Chen, V.; Stojadinovic, O.; Davis, S.C.; Tomic-Canic, M. Preclinical models for wound-healing studies. In Skin Tissue Models for Regenerative Medicine; Elsevier: Amsterdam, The Netherlands, 2018; pp. 223–253. [Google Scholar] [CrossRef]
- Wang, F.; Wang, S.-G.; Yang, Q.; Nan, L.-P.; Cai, T.-C.; Wu, D.-S.; Zhang, L. Cytotoxicity and Effect of Topical Application of Tranexamic Acid on Human Fibroblast in Spine Surgery. World Neurosurg. 2021, 153, e380–e391. [Google Scholar] [CrossRef]
- Cox, S.; Cole, M.; Mankarious, S.; Tawil, N. Effect of tranexamic acid incorporated in fibrin sealant clots on the cell behavior of neuronal and nonneuronal cells. J. Neurosci. Res. 2003, 72, 734–746. [Google Scholar] [CrossRef]
- Lishko, V.K.; Novokhatny, V.V.; Yakubenko, V.; Skomorovska-Prokvolit, H.V.; Ugarova, T.P. Characterization of plasminogen as an adhesive ligand for integrins alphaMbeta2 (Mac-1) and alpha5beta1 (VLA-5). Blood 2004, 104, 719–726. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Independent Variables | Levels | |
|---|---|---|
| X1: Concentration of sodium alginate | 2% (w/v) | 3% (w/v) |
| X2: Concentration of nano-hydroxyapatite | 1% (w/v) | 5% (w/v) |
| X3: Addition of CaCl2 solution | 0 | 0.5 M |
| Responses | Constraints | |
| Y1: Porosity | High | |
| Y2: Fluid uptake | High | |
| Y3: Biphasic release profile | Exist | |
| Aerogel Code | Factors Levels in Actual Values | ||
|---|---|---|---|
| X1: Concentration of Sodium Alginate (%) | X2: Concentration of Nano-Hydroxyapatite (%) | X3: Addition of CaCl2 Solution (M) | |
| A2H1 | 2 | 1 | - |
| A2H5 | 2 | 5 | - |
| A3H1 | 3 | 1 | - |
| A3H5 | 3 | 5 | - |
| A2H1Ca | 2 | 1 | 0.5 |
| A2H5Ca | 2 | 5 | 0.5 |
| A3H1Ca | 3 | 1 | 0.5 |
| A3H5Ca | 3 | 5 | 0.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
El Halawany, M.; Latif, R.; AbouGhaly, M.H.H. Hemostatic Alginate/Nano-Hydroxyapatite Composite Aerogel Loaded with Tranexamic Acid for the Potential Protection against Alveolar Osteitis. Pharmaceutics 2022, 14, 2255. https://doi.org/10.3390/pharmaceutics14102255
El Halawany M, Latif R, AbouGhaly MHH. Hemostatic Alginate/Nano-Hydroxyapatite Composite Aerogel Loaded with Tranexamic Acid for the Potential Protection against Alveolar Osteitis. Pharmaceutics. 2022; 14(10):2255. https://doi.org/10.3390/pharmaceutics14102255
Chicago/Turabian StyleEl Halawany, Mai, Randa Latif, and Mohamed H. H. AbouGhaly. 2022. "Hemostatic Alginate/Nano-Hydroxyapatite Composite Aerogel Loaded with Tranexamic Acid for the Potential Protection against Alveolar Osteitis" Pharmaceutics 14, no. 10: 2255. https://doi.org/10.3390/pharmaceutics14102255