
Reconciling Oxygen and Aerosol Delivery with a Hood on In Vitro Infant and Paediatric Models


Abstract
:1. Introduction
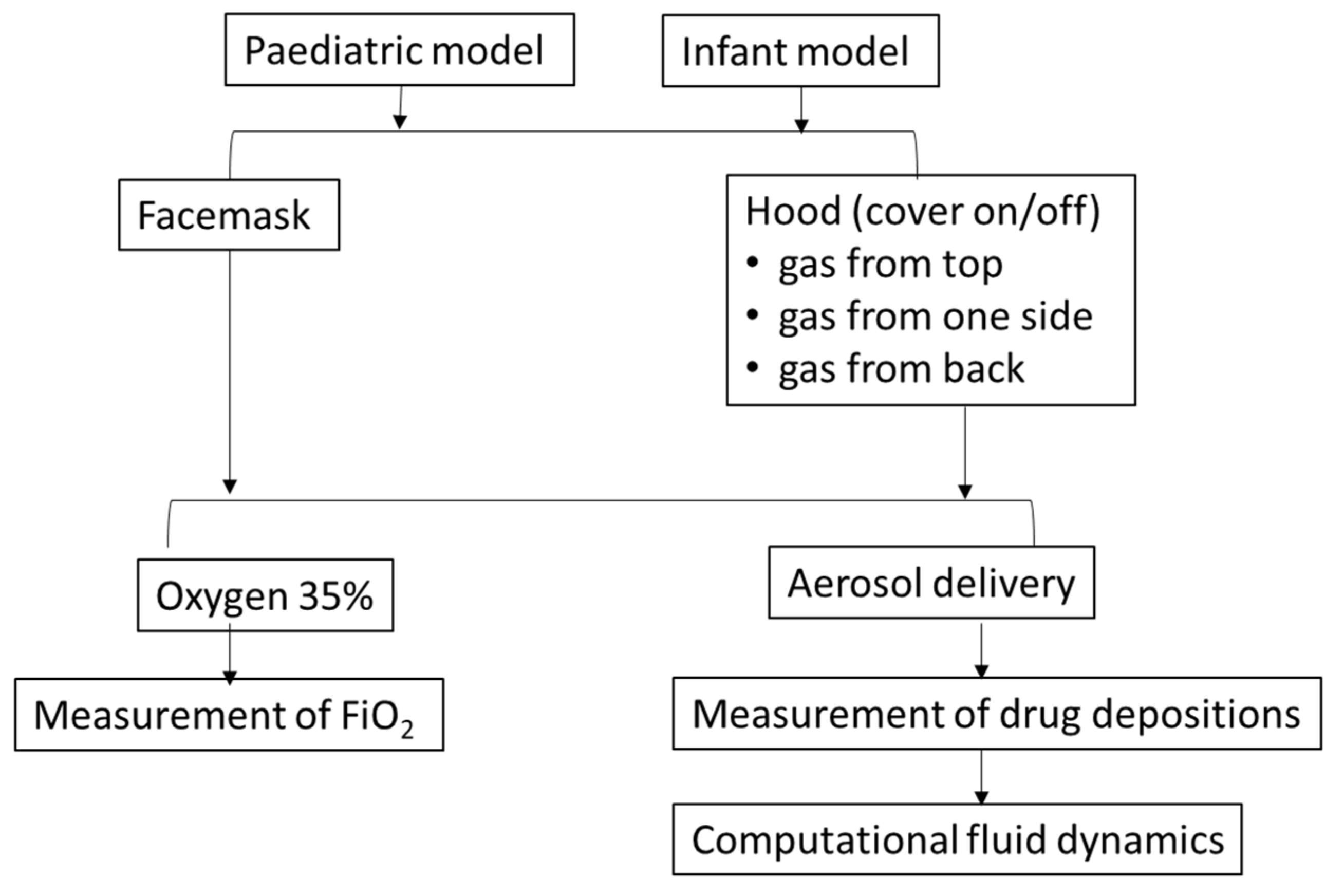
2. Materials and Methods
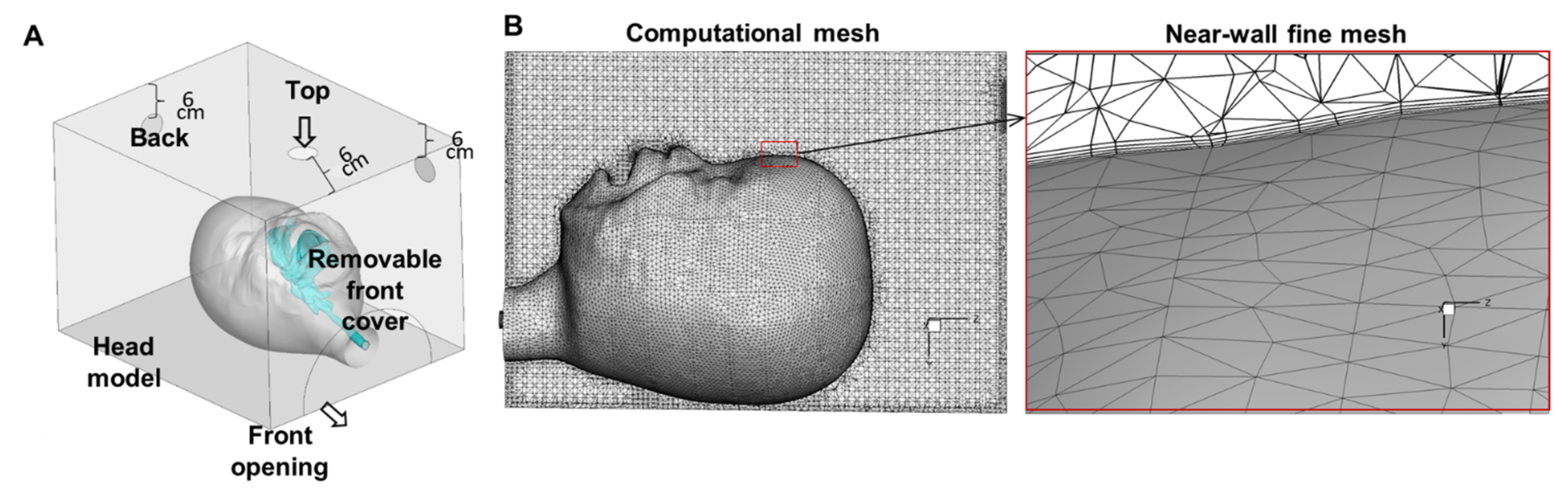
2.1. Experimental Apparatus
2.2. Evaluation of Aerosol Delivery
2.3. Evaluation of Oxygen Delivery
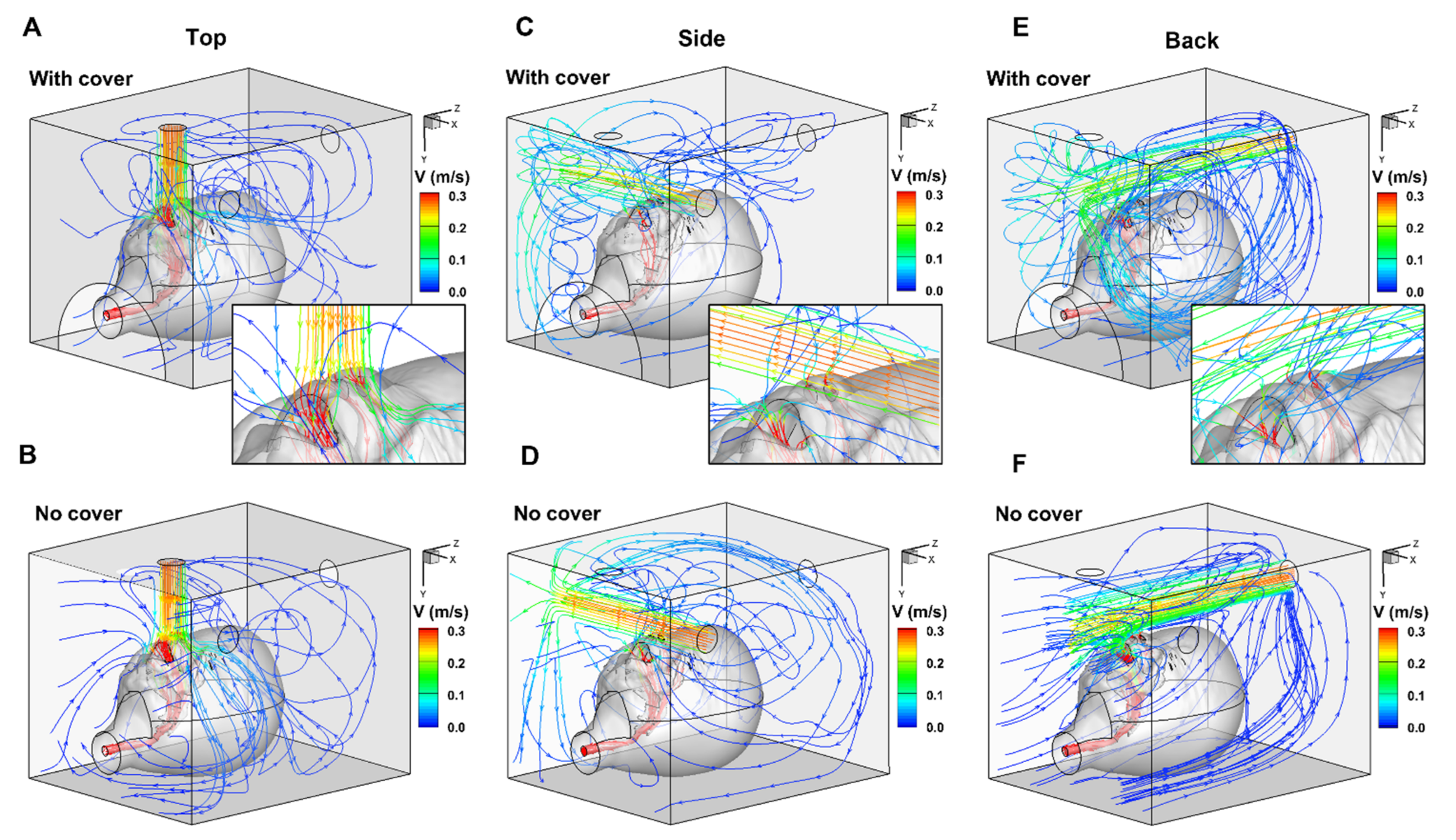
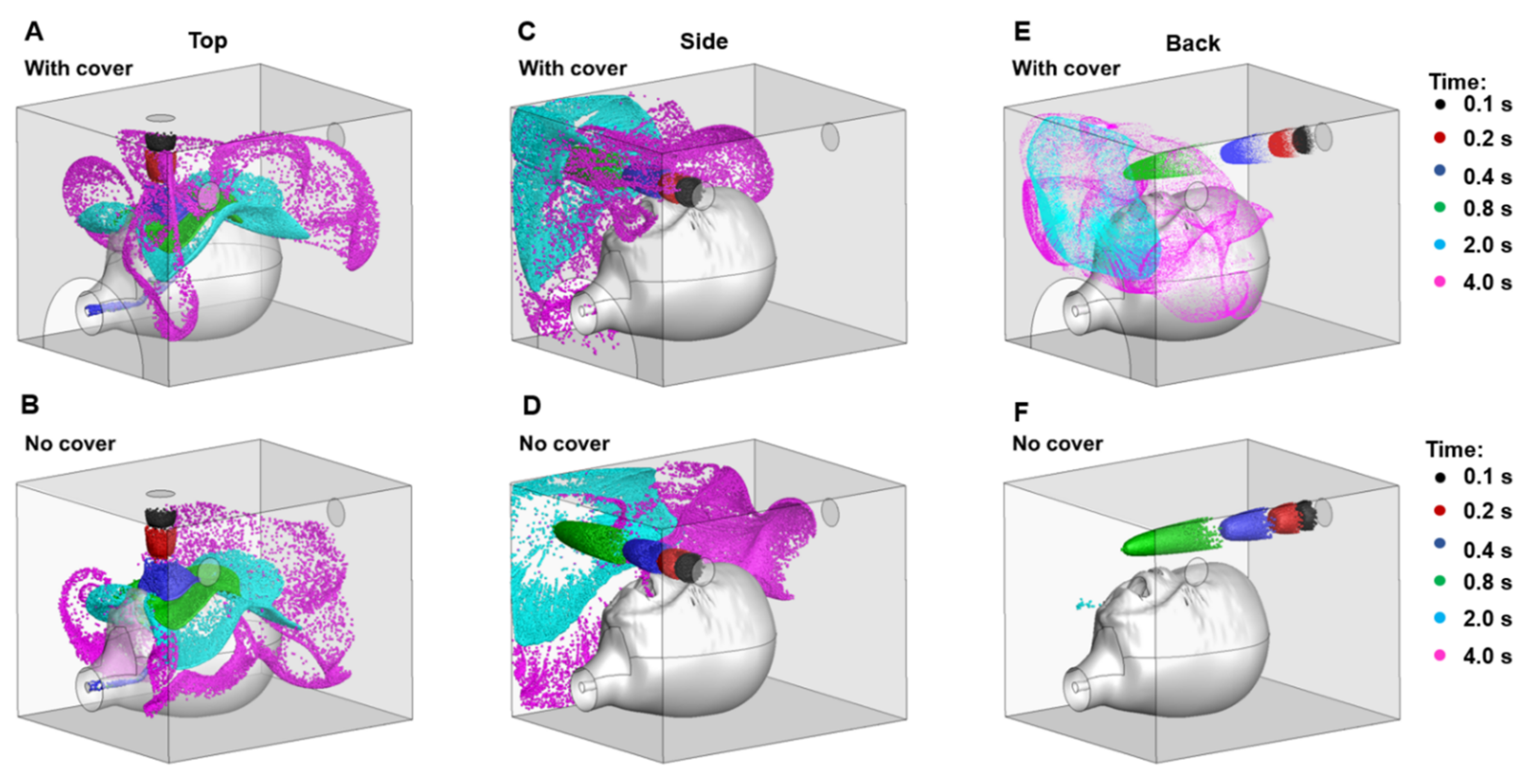
2.4. Numerical Analysis
2.5. Statistical Analysis
3. Results
3.1. Aerosolised Drug Deposition
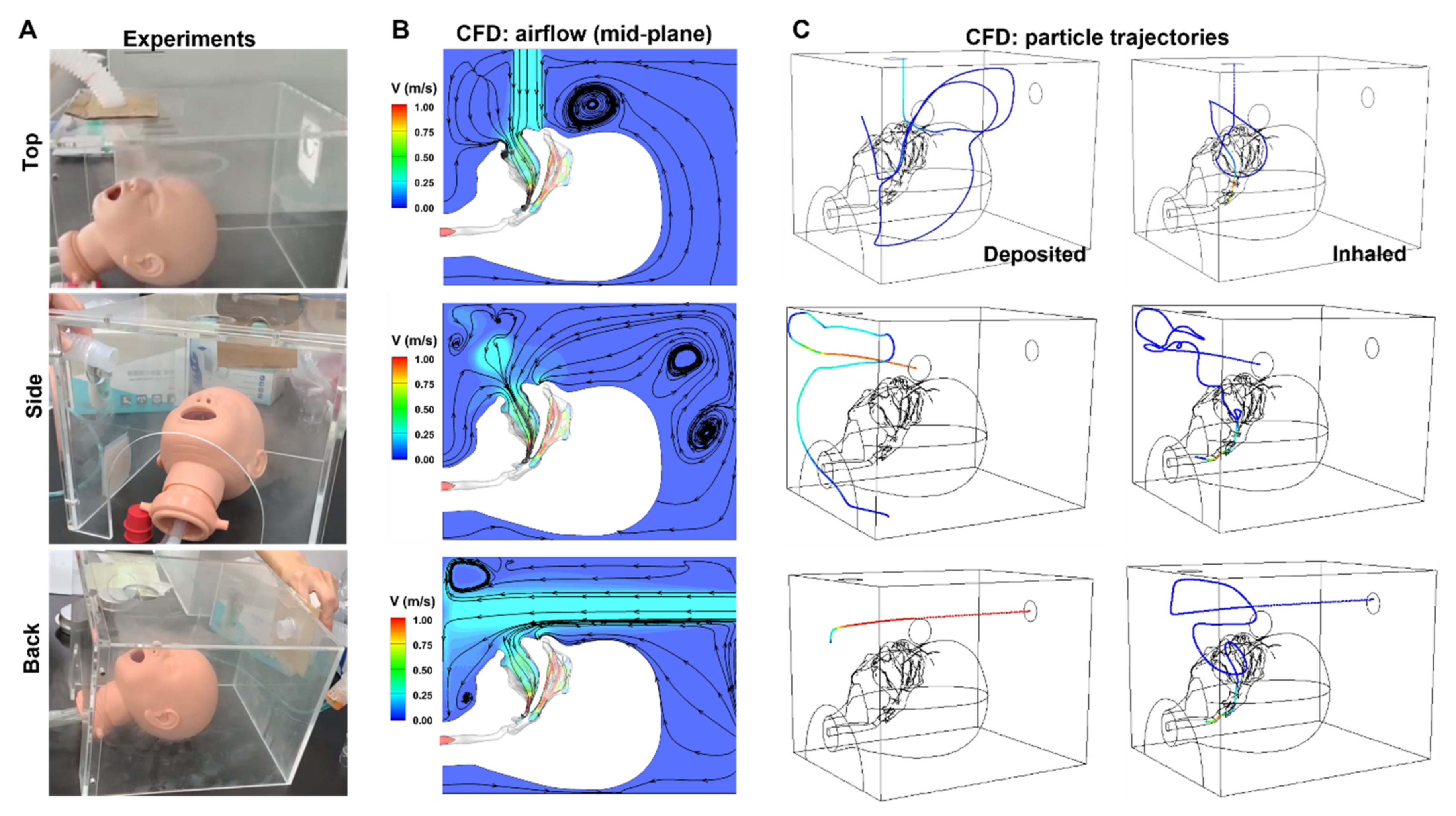
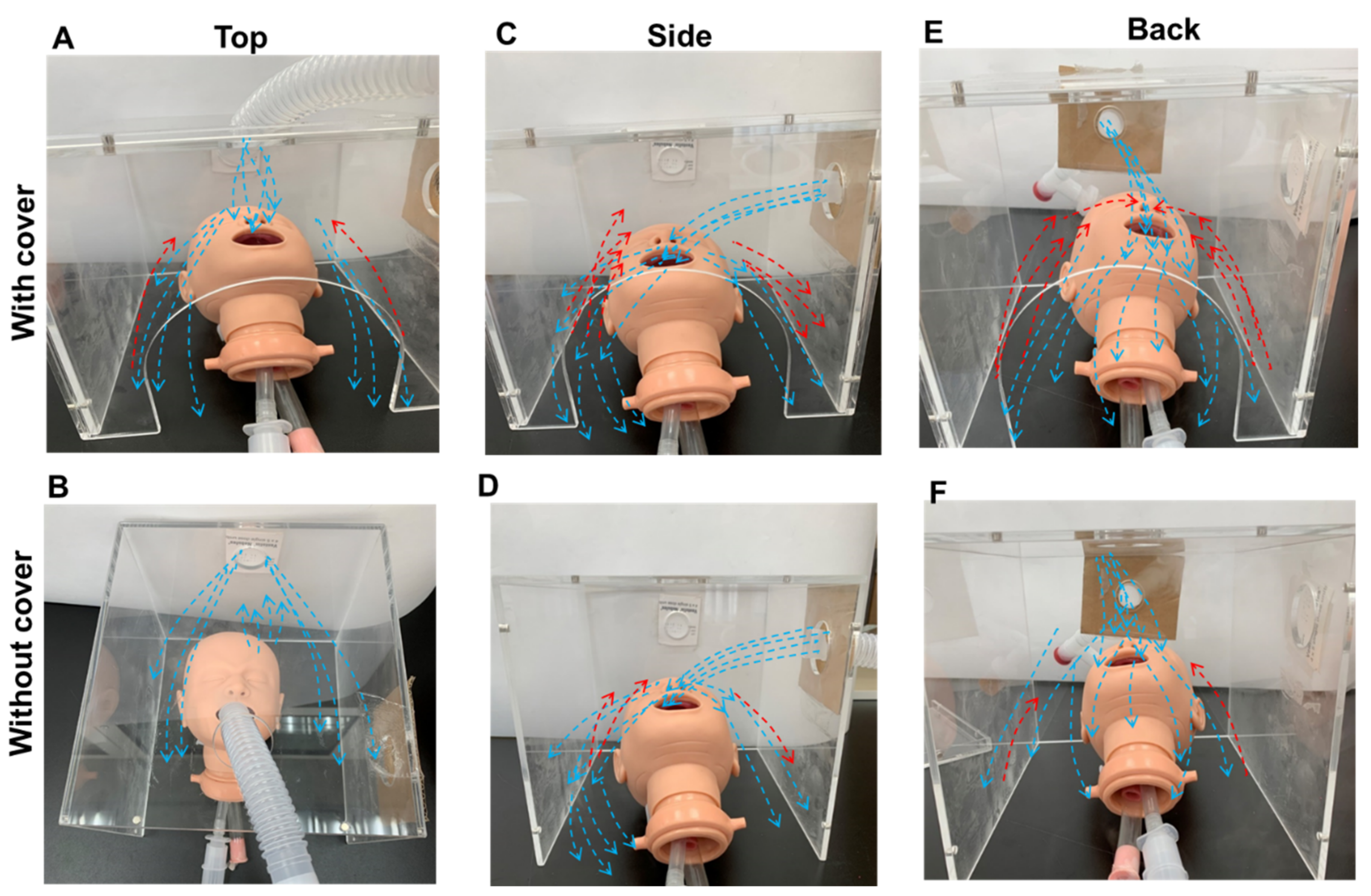
3.2. Numerical Analysis of Hood Delivery
3.3. Oxygen Therapy
4. Discussion
4.1. Aerosol Therapy with a Facemask vs. a Hood in an Infant Model
4.2. Aerosol Therapy with a Facemask vs. a Hood in a Paediatric Model
4.3. Oxygen Concentration
4.4. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Riedler, J. Innovations of the GINA 2020 for Children and the Effects of COVID-19 on Children with Asthma. Padiatr. Padol. 2021, 18, 1–6. [Google Scholar]
- Agache, I.; Eguiluz-Gracia, I.; Cojanu, C.; Laculiceanu, A.; Del Giacco, S.; Zemelka-Wiacek, M.; Kosowska, A.; Akdis, C.A.; Jutel, M. Advances and highlights in asthma in 2021. Allergy 2021, 76, 3390–3407. [Google Scholar] [CrossRef] [PubMed]
- Amirav, I.; Newhouse, M.T. Deposition of small particles in the developing lung. Paediatr. Respir. Rev. 2012, 13, 73–78. [Google Scholar] [CrossRef]
- Xi, J.; Si, X.; Zhou, Y.; Kim, J.; Berlinski, A. Growth of nasal-laryngeal airways in children and their implications in breathing and inhaled aerosol dynamics. Respir. Care 2014, 59, 263–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DiBlasi, R.M. Clinical controversies in aerosol therapy for infants and children. Respir. Care 2015, 60, 894–914. [Google Scholar] [CrossRef] [Green Version]
- Iles, R.; Lister, P.; Edmunds, A.T. Crying significantly reduces absorption of aerosolised drug in infants. Arch. Dis. Child. 1999, 81, 163–165. [Google Scholar] [CrossRef]
- Lin, H.L.; Restrepo, R.D.; Gardenhire, D.S.; Rau, J.L. Effect of face mask design on inhaled mass of nebulized albuterol, using a pediatric breathing model. Respir. Care 2007, 52, 1021–1026. [Google Scholar] [PubMed]
- Rubin, B.K. Bye-bye, blow-by. Respir. Care 2007, 52, 981. [Google Scholar]
- Ari, A. Drug delivery interfaces: A way to optimize inhalation therapy in spontaneously breathing children. World J. Clin. Pediatr. 2016, 5, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Amirav, I.; Balanov, I.; Gorenberg, M.; Groshar, D.; Luder, A.S. Nebuliser hood compared to mask in wheezy infants: Aerosol therapy without tears! Arch. Dis. Child. 2003, 88, 719–723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ari, A. A path to successful patient outcomes through aerosol drug delivery to children: A narrative review. Ann. Transl. Med. 2021, 9, 593. [Google Scholar] [CrossRef]
- Huang, J.; Zhang, H.; Zhang, M.; Zhang, X.; Wang, L. Reference values for resistance and compliance based on the single occlusion technique in healthy infants from Southeast China. J. Thorac. Dis. 2016, 8, 513–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fink, J.B. Aerosol delivery to ventilated infant and pediatric patients. Respir. Care 2004, 49, 653–665. [Google Scholar] [PubMed]
- Restrepo, R.D.; Dickson, S.K.; Rau, J.L.; Gardenhire, D.S. An investigation of nebulized bronchodilator delivery using a pediatric lung model of spontaneous breathing. Respir. Care 2006, 51, 56–61. [Google Scholar] [PubMed]
- Hess, D.; Fisher, D.; Williams, P.; Pooler, S.; Kacmarek, R.M. Medication nebulizer performance. Effects of diluent volume, nebulizer flow, and nebulizer brand. Chest 1996, 110, 498–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.; Xi, J.; Si, X.; Berlinski, A.; Su, W.C. Hood nebulization: Effects of head direction and breathing mode on particle inhalability and deposition in a 7-month-old infant model. J. Aerosol. Med. Pulm. Drug Deliv. 2014, 27, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Xi, J.; Si, X.A.; Nagarajan, R. Effects of mask-wearing on the inhalability and deposition of airborne SARS-CoV-2 Aerosols in human upper airway. Phys. Fluids 2020, 32, 123312. [Google Scholar] [CrossRef] [PubMed]
- Longest, P.W.; Xi, J. Effectiveness of direct Lagrangian tracking models for simulating nanoparticle deposition in the upper airways. Aerosol. Sci. Tech. 2007, 41, 380–397. [Google Scholar] [CrossRef]
- Tian, G.; Hindle, M.; Lee, S.; Longest, P.W. Validating CFD predictions of pharmaceutical aerosol deposition with in vivo data. Pharm. Res. 2015, 32, 3170–3187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walenga, R.L.; Tian, G.; Hindle, M.; Yelverton, J.; Dodson, K.; Longest, P.W. Variability in nose-to-lung aerosol Delivery. J. Aerosol. Sci. 2014, 78, 11–29. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.; Xi, J.; Simpson, J.; Irshad, H.; Cheng, Y.-S. aerosol deposition in a nasopharyngolaryngeal replica of a 5-year-old child. Aerosol. Sci. Tech. 2013, 47, 275–282. [Google Scholar] [CrossRef]
- Xi, J.; Yuan, J.E.; Zhang, Y.; Nevorski, D.; Wang, Z.; Zhou, Y. Visualization and quantification of nasal and olfactory deposition in a sectional adult nasal airway cast. Pharm. Res. 2016, 33, 1527–1541. [Google Scholar] [CrossRef]
- Kugelman, A.; Amirav, I.; Mor, F.; Riskin, A.; Bader, D. Hood versus mask nebulization in infants with evolving bronchoPulmonary dysplasia in the neonatal intensive care unit. J. Perinatol. 2006, 26, 31–36. [Google Scholar] [CrossRef] [Green Version]
- Bar-Yishay, E.; Avital, A.; Springer, C.; Amirav, I. Lung function response to bronchodilator nebulization via hood in wheezy infants: A pilot study. Isr. Med. Assoc. J. 2011, 13, 39–43. [Google Scholar] [PubMed]
- Amirav, I.; Shakked, T.; Broday, D.M.; Katoshevski, D. Numerical investigation of aerosol deposition at the eyes when using a hood inhaler for infants—A 3D simulation. J. Aerosol. Med. Pulm. Drug Deliv. 2008, 21, 207–214. [Google Scholar] [CrossRef] [Green Version]
- Shakked, T.; Broday, D.M.; Katoshevski, D.; Amirav, I. Administration of aerosolized drugs to infants by a hood: A three-dimensional numerical study. J. Aerosol. Med. Off. J. Int. Soc. Aerosol. Med. 2006, 19, 533–542. [Google Scholar] [CrossRef]
- Amirav, I.; Oron, A.; Tal, G.; Cesar, K.; Ballin, A.; Houri, S.; Naugolny, L.; Mandelberg, A. Aerosol delivery in Respiratory syncytial virus bronchiolitis: Hood or face mask? J. Pediatr. 2005, 147, 627–631. [Google Scholar] [CrossRef] [PubMed]
- Shakked, T.; Katoshevski, D.; Broday, D.M.; Amirav, I. Numerical simulation of air flow and medical-aerosol distribution in an innovative nebulizer hood. J. Aerosol. Med. Off. J. Int. Soc. Aerosol. Med. 2005, 18, 207–217. [Google Scholar] [CrossRef] [PubMed]
- Napolitano, N.; Berlinski, A.; Walsh, B.K.; Ginier, E.; Strickland, S.L. AARC clinical practice guideline: Management of pediatric patients with oxygen in the acute care setting. Respir. Care 2021, 66, 1214–1223. [Google Scholar] [CrossRef]
- Walsh, B.K.; Brooks, T.M.; Grenier, B.M. Oxygen therapy in the neonatal care environment. Respir. Care 2009, 54, 1193–1202. [Google Scholar]
- Dugernier, J.; Hesse, M.; Vanbever, R.; Depoortere, V.; Roeseler, J.; Michotte, J.B.; Laterre, P.F.; Jamar, F.; Reychler, G. SPECT-CT comparison of lung deposition using a system combining a vibrating-mesh nebulizer with a valved holding chamber and a conventional jet nebulizer: A randomized cross-over study. Pharm. Res. 2017, 34, 290–300. [Google Scholar] [CrossRef]
- Galindo-Filho, V.C.; Alcoforado, L.; Rattes, C.; Paiva, D.N.; Brandão, S.C.S.; Fink, J.B.; Dornelas de Andrade, A. A mesh nebulizer is more effective than jet nebulizer to nebulize bronchodilators during non-invasive ventilation of subjects with COPD: A randomized controlled trial with radiolabeled aerosols. Respir. Med. 2019, 153, 60–67. [Google Scholar] [CrossRef]
- Xi, J.; Yuan, J.E.; Si, X.A. Simulation study of electric-guided delivery of 0.4 µm monodisperse and polydisperse aerosols to the ostiomeatal complex. Comput. Biol. Med. 2016, 72, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Longest, P.W.; Xi, J. Condensational growth may contribute to the enhanced deposition of cigarette smoke particles in the upper Respiratory tract. Aerosol. Sci. Tech. 2008, 42, 579–602. [Google Scholar] [CrossRef]
- Xi, J.; Si, X.; Longest, P.W. Electrostatic charge effects on pharmaceutical aerosol deposition in human nasal-laryngeal airways. Pharmaceutics 2013, 6, 26–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.W.; Xi, J.; Si, X.A. Dynamic growth and deposition of hygroscopic aerosols in the nasal airway of a 5-year-old child. Int. J. Num. Method Biomed. Eng. 2013, 29, 17–39. [Google Scholar] [CrossRef] [PubMed]
- Xi, J.; Yuan, J.; Alshaiba, M.; Cheng, D.; Firlit, Z.; Johnson, A.; Nolan, A.; Su, W. Design and testing of electric-guided delivery of charged particles to the olfactory region: Experimental and numerical studies. Curr. Drug Deliv. 2015, 13, 1–10. [Google Scholar] [CrossRef]
- Hatley, R.H.; Byrne, S.M. Variability in delivered dose and respirable delivered dose from nebulizers: Are current regulatory testing guidelines sufficient to produce meaningful information? Med. Devices 2017, 10, 17–28. [Google Scholar] [CrossRef] [Green Version]
- Talaat, K.; Xi, J. Computational modeling of aerosol transport, dispersion, and deposition in rhythmically expanding and contracting terminal alveoli. J. Aerosol. Sci. 2017, 112, 19–33. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Model | Placement | Deposition (%) | ||
|---|---|---|---|---|
| Facemask | With Cover | No Cover | ||
| Infant | ||||
| Inhaled | 1.11 ± 0.22 | |||
| Top | 1.03 ± 0.09 | 0.84 ± 0.1 | ||
| Side | 1.13 ± 0.17 | 0.89 ± 0.14 | ||
| Back | 1.68 ± 0.27 *,† | 1.2 ± 0.13 | ||
| Face | 4.15 ± 0.26 | |||
| Top | 4.31 ± 0.29 | 4.55 ± 0.51 | ||
| Side | 2.34 ± 0.39 † | 1.67 ± 0.2 | ||
| Back | 4.39 ± 0.61 † | 3.18 ± 0.23 | ||
| Residual dose | 50.1 ± 3.22 | |||
| Top | 51.98 ± 4.55 | 52.42 ± 4.53 | ||
| Side | 51.36 ± 5.09 | 50.45 ± 4.67 | ||
| Back | 50.37 ± 3.84 | 50.85 ± 3.74 | ||
| Paediatric | ||||
| Inhaled | 1.89 ± 0.17 * | |||
| Top | 1.37 ± 0.19 | 1.13 ± 0.17 | ||
| Side | 1.22 ± 0.24 | 1.07 ± 0.17 | ||
| Back | 1.37 ± 0.27 | 1.13 ± 0.18 | ||
| Face | 4.71 ± 0.43 | |||
| Top | 4.42 ± 0.64 ** | 4.29 ± 0.55 | ||
| Side | 1.67 ± 0.3 † | 1.45 ± 0.17 | ||
| Back | 2.47 ± 0.29 † | 2.26 ± 0.34 | ||
| Residual dose | 48.47 ± 2 | |||
| Top | 46.41 ± 3.79 | 47.82 ± 4.6 | ||
| Side | 48.94 ± 4.92 | 48.78 ± 2.8 | ||
| Back | 50.51 ± 6.65 | 49.82 ± 5.29 | ||
| Model | With Cover | No Cover | ||
|---|---|---|---|---|
| Infant | ||||
| FiO2 (%) | Facemask | 35.89 ± 0.12 * | ||
| Top | 35.7 ± 0.14 | 35.48 ± 0.16 | ||
| Side | 35.17 ± 0.23 † | 26.8 ± 0.26 | ||
| Back | 35.27 ± 0.25 † | 23.72 ± 0.26 | ||
| Stabilisation time, min | ||||
| Facemask | 4.82 ± 0.14 | |||
| Top | 3.77 ± 0.6 | 4.11 ± 1.01 | ||
| Side | 4.91 ± 0.65 | 5.03 ± 0.87 | ||
| Back | 5.03 ± 0.82 | 4.47 ± 0.6 | ||
| Paediatric | ||||
| Facemask | 33.97 ± 0.15 * | |||
| Top | 35.22 ± 0.17 † | 29.89 ± 0.2 | ||
| Side | 34.83 ± 0.12 † | 25.82 ± 0.17 | ||
| Back | 35.4 ± 0.14 † | 23 ± 0.14 | ||
| Stabilisation time, min | ||||
| Facemask | 3.8 ± 0.57 | |||
| Top | 4.41 ± 0.34 | 4.09 ± 0.47 | ||
| Side | 4.72 ± 0.27 | 4.57 ± 0.72 | ||
| Back | 4.36 ± 0.37 | 4.71 ± 0.79 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, S.-H.; Chang, H.-C.; Chien, M.-Y.; Xi, J.; Lin, H.-L. Reconciling Oxygen and Aerosol Delivery with a Hood on In Vitro Infant and Paediatric Models. Pharmaceutics 2022, 14, 91. https://doi.org/10.3390/pharmaceutics14010091
Chen S-H, Chang H-C, Chien M-Y, Xi J, Lin H-L. Reconciling Oxygen and Aerosol Delivery with a Hood on In Vitro Infant and Paediatric Models. Pharmaceutics. 2022; 14(1):91. https://doi.org/10.3390/pharmaceutics14010091
Chicago/Turabian StyleChen, Shu-Hsin, Hsiu-Chu Chang, Ming-Yi Chien, Jinxiang Xi, and Hui-Ling Lin. 2022. "Reconciling Oxygen and Aerosol Delivery with a Hood on In Vitro Infant and Paediatric Models" Pharmaceutics 14, no. 1: 91. https://doi.org/10.3390/pharmaceutics14010091