
Topical Triamcinolone Acetonide-Loaded Liposome Formulation Used as an Adjuvant to Intravitreal Ranibizumab Therapy for Neovascular Age-Related Macular Degeneration

 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Patients
2.3. Clinical Evaluation and Study Treatment
2.4. Safety Assessment
2.5. Efficacy Assessment
2.6. TALF Preparation
2.7. Data Analysis and Statistical Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Friedman, D.S.; O’Colmain, B.J.; Munoz, B.; Tomany, S.C.; McCarty, C.; De Jong, P.; Nemesure, B.; Mitchell, P.; Kempen, J. Prevalence of age-related macular degeneration in the United States. Arch. Ophthalmol. 2004, 122, 564–572. [Google Scholar]
- Resnikoff, S.; Pascolini, D.; Etya’Ale, D.; Kocur, I.; Pararajasegaram, R.; Pokharel, G.P.; Mariotti, S.P. Global data on visual impairment in the year 2002. Bull. World Health Organ. 2004, 82, 844–851. [Google Scholar]
- Wong, W.L.; Su, X.; Li, X.; Cheung, C.M.G.; Klein, R.; Cheng, C.-Y.; Wong, T.Y. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: A systematic review and meta-analysis. Lancet Glob. Health 2014, 2, e106–e116. [Google Scholar] [CrossRef] [Green Version]
- Bressler, N.M. Age-Related Macular Degeneration Is the Leading Cause of Blindness. JAMA 2004, 291, 1900–1901. [Google Scholar] [CrossRef]
- Jonas, J.B.; Cheung, C.M.G.; Panda-Jonas, S. Updates on the epidemiology of age-related macular degeneration. Asia Pac. J. Ophthalmol. 2017, 6, 493–497. [Google Scholar]
- Tsilimbaris, M.K.; López-Gálvez, M.I.; Gallego-Pinazo, R.; Margaron, P.; Lambrou, G.N. Epidemiological and clinical baseline characteristics as predictive biomarkers of response to anti-VEGF treatment in patients with neovascular AMD. J. Ophthalmol. 2016, 2016, 4367631. [Google Scholar] [CrossRef] [Green Version]
- Tsutsumi-Miyahara, C.; Sonoda, K.; Egashira, K.; Ishibashi, M.; Qiao, H.; Oshima, T.; Murata, T.; Miyazaki, M.; Charo, I.; Hamano, S. The relative contributions of each subset of ocular infiltrated cells in experimental choroidal neovascularisation. Br. J. Ophthalmol. 2004, 88, 1217–1222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grossniklaus, H.E.; Ling, J.X.; Wallace, T.M.; Dithmar, S.; Lawson, D.H.; Cohen, C.; Elner, V.M.; Elner, S.G.; Sternberg, P., Jr. Macrophage and retinal pigment epithelium expression of angiogenic cytokines in choroidal neovascularization. Mol. Vis. 2002, 8, 119–126. [Google Scholar] [PubMed]
- Grossniklaus, H.E.; Green, W.R. Choroidal neovascularization. Am. J. Ophthalmol. 2004, 137, 496–503. [Google Scholar] [CrossRef]
- Espinosa-Heidmann, D.G.; Reinoso, M.A.; Pina, Y.; Csaky, K.G.; Caicedo, A.; Cousins, S.W. Quantitative enumeration of vascular smooth muscle cells and endothelial cells derived from bone marrow precursors in experimental choroidal neovascularization. Exp. Eye Res. 2005, 80, 369–378. [Google Scholar] [CrossRef]
- Killingsworth, M.C. Angiogenesis in early choroidal neovascularization secondary to age-related macular degeneration. Graefe Arch. Clin. Exp. Ophthalmol. 1995, 233, 313–323. [Google Scholar] [CrossRef]
- Sheridan, C.M.; Rice, D.; Hiscott, P.S.; Wong, D.; Kent, D.L. The presence of AC133-positive cells suggests a possible role of endothelial progenitor cells in the formation of choroidal neovascularization. Investig. Ophthalmol. Vis. Sci. 2006, 47, 1642–1645. [Google Scholar] [CrossRef] [Green Version]
- Ebrahem, Q.; Minamoto, A.; Hoppe, G.; Anand-Apte, B.; Sears, J.E. Triamcinolone acetonide inhibits IL-6–and VEGF-Induced angiogenesis downstream of the IL-6 and VEGF receptors. Investig. Ophthalmol. Vis. Sci. 2006, 47, 4935–4941. [Google Scholar] [CrossRef]
- Brown, D.M.; Kaiser, P.K.; Michels, M.; Soubrane, G.; Heier, J.S.; Kim, R.Y.; Sy, J.P.; Schneider, S. Ranibizumab versus verteporfin for neovascular age-related macular degeneration. N. Engl. J. Med. 2006, 355, 1432–1444. [Google Scholar] [CrossRef] [Green Version]
- Rosenfeld, P.J.; Brown, D.M.; Heier, J.S.; Boyer, D.S.; Kaiser, P.K.; Chung, C.Y.; Kim, R.Y. Ranibizumab for neovascular age-related macular degeneration. N. Engl. J. Med. 2006, 355, 1419–1431. [Google Scholar] [CrossRef] [Green Version]
- Regillo, C.D.; Brown, D.M.; Abraham, P.; Yue, H.; Ianchulev, T.; Schneider, S.; Shams, N.; The PIER Study Group. Randomized, double-masked, sham-controlled trial of ranibizumab for neovascular age-related macular degeneration: PIER Study year 1. Am. J. Ophthalmol. 2008, 145, 239–248. e235. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, P.; Korobelnik, J.-F.; Lanzetta, P.; Holz, F.G.; Pruente, C.; Schmidt-Erfurth, U.; Tano, Y.; Wolf, S. Ranibizumab (Lucentis) in neovascular age-related macular degeneration: Evidence from clinical trials. Br. J. Ophthalmol. 2010, 94, 2–13. [Google Scholar] [CrossRef] [PubMed]
- Grzybowski, A.; Told, R.; Sacu, S.; Bandello, F.; Moisseiev, E.; Loewenstein, A.; Schmidt-Erfurth, U. 2018 update on intravitreal injections: Euretina expert consensus recommendations. Ophthalmologica 2018, 239, 181–193. [Google Scholar] [CrossRef] [PubMed]
- Platania, C.; Di Paola, L.; Leggio, G.M.; Romano, G.L.; Drago, F.; Salomone, S.; Bucolo, C. Molecular features of interaction between VEGFA and anti-angiogenic drugs used in retinal diseases: A computational approach. Front. Pharmacol. 2015, 6, 248. [Google Scholar] [CrossRef] [Green Version]
- Meyer, C.H.; Michels, S.; Rodrigues, E.B.; Hager, A.; Mennel, S.; Schmidt, J.C.; Helb, H.M.; Farah, M.E. Incidence of rhegmatogenous retinal detachments after intravitreal antivascular endothelial factor injections. Acta Ophthalmol. 2011, 89, 70–75. [Google Scholar] [CrossRef] [PubMed]
- Lyall, D.A.; Tey, A.; Foot, B.; Roxburgh, S.T.; Virdi, M.; Robertson, C.; MacEwen, C.J. Post-intravitreal anti-VEGF endophthalmitis in the United Kingdom: Incidence, features, risk factors, and outcomes. Eye 2012, 26, 1517–1526. [Google Scholar] [CrossRef]
- Munk, M.R.; Ceklic, L.; Ebneter, A.; Huf, W.; Wolf, S.; Zinkernagel, M.S. Macular atrophy in patients with long-term anti-VEGF treatment for neovascular age-related macular degeneration. Acta Ophthalmol. 2016, 94, e757–e764. [Google Scholar] [CrossRef] [Green Version]
- Abdelfattah, N.S.; Zhang, H.; Boyer, D.S.; Sadda, S.R. Progression of macular atrophy in patients with neovascular age-related macular degeneration undergoing antivascular endothelial growth factor therapy. Retina 2016, 36, 1843–1850. [Google Scholar] [CrossRef] [Green Version]
- Dugel, P.U.; Koh, A.; Ogura, Y.; Jaffe, G.J.; Schmidt-Erfurth, U.; Brown, D.M.; Gomes, A.V.; Warburton, J.; Weichselberger, A.; Holz, F.G. HAWK and HARRIER: Phase 3, multicenter, randomized, double-masked trials of brolucizumab for neovascular age-related macular degeneration. Ophthalmology 2020, 127, 72–84. [Google Scholar] [CrossRef]
- Pacella, E.; Vestri, A.R.; Muscella, R.; Carbotti, M.R.; Castellucci, M.; Coi, L.; Turchetti, P.; Pacella, F. Preliminary results of an intravitreal dexamethasone implant (Ozurdex®) in patients with persistent diabetic macular edema. Clin. Ophthalmol. 2013, 7, 1423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pearson, P.A.; Comstock, T.L.; Ip, M.; Callanan, D.; Morse, L.S.; Ashton, P.; Levy, B.; Mann, E.S.; Eliott, D. Fluocinolone acetonide intravitreal implant for diabetic macular edema: A 3-year multicenter, randomized, controlled clinical trial. Ophthalmology 2011, 118, 1580–1587. [Google Scholar] [CrossRef]
- Campochiaro, P.A.; Marcus, D.M.; Awh, C.C.; Regillo, C.; Adamis, A.P.; Bantseev, V.; Chiang, Y.; Ehrlich, J.S.; Erickson, S.; Hanley, W.D. The port delivery system with ranibizumab for neovascular age-related macular degeneration: Results from the randomized phase 2 ladder clinical trial. Ophthalmology 2019, 126, 1141–1154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.; Jiang, A.; Joshi, M.; Christoforidis, J. Drug Delivery Implants in the Treatment of Vitreous Inflammation. Mediators Inflamm. 2013, 2013, 780634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Humayun, M.; Santos, A.; Altamirano, J.C.; Ribeiro, R.; Gonzalez, R.; de la Rosa, A.; Shih, J.; Pang, C.; Jiang, F.; Calvillo, P.; et al. Implantable micropump for drug delivery in patients with diabetic macular edema. Transl. Vis. Sci. Technol. 2014, 3, 5. [Google Scholar] [CrossRef] [Green Version]
- Bisht, R.; Mandal, A.; Jaiswal, J.K.; Rupenthal, I.D. Nanocarrier mediated retinal drug delivery: Overcoming ocular barriers to treat posterior eye diseases. Wiley Interdiscip. Rev. Nanomed. Nanobiotechnol. 2018, 10, e1473. [Google Scholar] [CrossRef]
- Gaudana, R.; Jwala, J.; Boddu, S.H.; Mitra, A.K. Recent perspectives in ocular drug delivery. Pharm. Res. 2009, 26, 1197–1216. [Google Scholar] [CrossRef] [Green Version]
- F Fangueiro, J.; Veiga, F.; M Silva, A.; B Souto, E. Ocular drug delivery-new strategies for targeting anterior and posterior segments of the eye. Curr. Pharm. Des. 2016, 22, 1135–1146. [Google Scholar] [CrossRef]
- Bravo-Osuna, I.; Andrés-Guerrero, V.; Abal, P.P.; Molina-Martínez, I.; Herrero-Vanrell, R. Pharmaceutical microscale and nanoscale approaches for efficient treatment of ocular diseases. Drug Deliv. Transl. Res. 2016, 6, 686–707. [Google Scholar] [CrossRef]
- Kumar, R. Lipid-based nanoparticles for drug-delivery systems. In Nanocarriers for Drug Delivery; Elsevier: Amsterdam, The Netherlands, 2019; pp. 249–284. [Google Scholar]
- Mishra, G.P.; Bagui, M.; Tamboli, V.; Mitra, A.K. Recent applications of liposomes in ophthalmic drug delivery. J. Drug Deliv. 2011, 2011, 863734. [Google Scholar] [CrossRef] [Green Version]
- Altamirano-Vallejo, J.C.; Navarro-Partida, J.; de la Rosa, A.G.; Hsiao, J.H.; Olguín-Gutierrez, J.S.; Gonzalez-Villegas, A.C.; Keller, B.C.; Bouzo-Lopez, L.; Santos, A. Characterization and pharmacokinetics of triamcinolone acetonide-loaded liposomes topical formulations for vitreoretinal drug delivery. J. Ocul. Pharmacol. Ther. 2018, 34, 416–425. [Google Scholar] [CrossRef]
- Navarro-Partida, J.; Altamirano-Vallejo, J.C.; Armendariz-Borunda, J.; Castro-Castaneda, C.R.; Santos, A. Safety and Tolerability of Topical Ophthalmic Triamcinolone Acetonide-Loaded Liposomes Formulation and Evaluation of Its Biologic Activity in Patients with Diabetic Macular Edema. Pharmaceutics 2021, 13, 322. [Google Scholar] [CrossRef] [PubMed]
- de la Rosa, A.G.; Navarro-Partida, J.; Altamirano-Vallejo, J.C.; Hernandez-Gamez, A.G.; Garcia-Banuelos, J.J.; Armendariz-Borunda, J.; Santos, A. Novel triamcinolone acetonide-loaded liposomes topical formulation for the treatment of cystoid macular edema after cataract surgery: A pilot study. J. Ocul. Pharmacol. Ther. 2019, 35, 106–115. [Google Scholar] [CrossRef] [Green Version]
- Navarro-Partida, J.; Altamirano-Vallejo, J.C.; Lopez-Naranjo, E.J.; de la Rosa, A.G.; Manzano-Ramírez, A.; Apatiga-Castro, L.M.; Armendáriz-Borunda, J.; Santos, A. Topical Triamcinolone Acetonide-Loaded Liposomes as Primary Therapy for Macular Edema Secondary to Branch Retinal Vein Occlusion: A Pilot Study. J. Ocul. Pharmacol. Ther. 2020, 36, 393–403. [Google Scholar] [CrossRef] [PubMed]
- Gopal, L.; Sharma, T. Use of intravitreal injection of triamcinolone acetonide in the treatment of age-related macular degeneration. Indian J. Ophthalmol. 2007, 55, 431. [Google Scholar] [CrossRef] [PubMed]
- Jonas, J.B.; Spandau, U.H.; Kamppeter, B.A.; Degenring, R.F.; Kreissig, I.; Akkoyun, I.; Vossmerbaeumer, U. Duration of the effect of intravitreal triamcinolone acetonide in eyes with exudative age-related macular degeneration. J. Ocul. Pharmacol. Ther. 2006, 22, 194–199. [Google Scholar] [CrossRef]
- Ahmadieh, H.; Taei, R.; Riazi-Esfahani, M.; Piri, N.; Homayouni, M.; Daftarian, N.; Yaseri, M. Intravitreal bevacizumab versus combined intravitreal bevacizumab and triamcinolone for neovascular age-related macular degeneration: Six-month results of a randomized clinical trial. Retina 2011, 31, 1819–1826. [Google Scholar] [CrossRef]
- El Matri, L.; Chebil, A.; Kort, F.; Bouraoui, R.; Baklouti, K.; Mghaieth, F. Intravitreal injection of triamcinolone combined with bevacizumab for choroidal neovascularization associated with large retinal pigment epithelial detachment in age-related macular degeneration. Graefe Arch. Clin. Exp. Ophthalmol. 2010, 248, 779–784. [Google Scholar] [CrossRef] [PubMed]
- Tao, Y.; Jonas, J.B. Intravitreal bevacizumab combined with intravitreal triamcinolone for therapy-resistant exudative age-related macular degeneration. J. Ocul. Pharmacol. Ther. 2010, 26, 207–212. [Google Scholar] [CrossRef]
- Riazi-Esfahani, M.; Ahmadieh, H.; Faghihi, H.; Piri, N.; Taei, R.; Karkhaneh, R.; Alami-Harandi, Z.; Lashay, A.; Mirshahi, A.; Nili-Ahmadabadi, M.; et al. Intravitreal bevacizumab versus combined bevacizumab and triamcinolone acetonide for neovascular age-related macular degeneration. J. Ophthalmic Vis. Res. 2008, 3, 95–101. [Google Scholar] [PubMed]
- Lalwani, G.A.; Rosenfeld, P.J.; Fung, A.E.; Dubovy, S.R.; Michels, S.; Feuer, W.; Davis, J.L.; Flynn, H.W., Jr.; Esquiabro, M. A variable-dosing regimen with intravitreal ranibizumab for neovascular age-related macular degeneration: Year 2 of the PrONTO Study. Am. J. Ophthalmol. 2009, 148, 43–58. [Google Scholar] [CrossRef] [PubMed]
- Umland, S.P.; Nahrebne, D.K.; Razac, S.; Beavis, A.; Pennline, K.J.; Egan, R.W.; Billah, M.M. The inhibitory effects of topically active glucocorticoids on IL-4, IL-5, and interferon-γ production by cultured primary CD4+ T cells. J. Allergy Clin. Immunol. 1997, 100, 511–519. [Google Scholar] [CrossRef]
- Gaudreault, J.; Fei, D.; Rusit, J.; Suboc, P.; Shiu, V. Preclinical pharmacokinetics of Ranibizumab (rhuFabV2) after a single intravitreal administration. Investig. Ophthalmol. Vis. Sci. 2005, 46, 726–733. [Google Scholar] [CrossRef] [PubMed]
- Stewart, M.W.; Rosenfeld, P.J.; Penha, F.M.; Wang, F.; Yehoshua, Z.; Bueno-Lopez, E.; Lopez, P.F. Pharmacokinetic rationale for dosing every 2 weeks versus 4 weeks with intravitreal ranibizumab, bevacizumab, and aflibercept (vascular endothelial growth factor Trap-eye). Retina 2012, 32, 434–457. [Google Scholar] [CrossRef] [PubMed]
- Martin, D.F.; Maguire, M.G.; Fine, S.L.; Ying, G.-S.; Jaffe, G.J.; Grunwald, J.E.; Toth, C.; Redford, M.; Ferris, F.L., 3rd; Comparison of Age-Related Macular Degeneration Treatments Trials (CATT) Research Group. Ranibizumab and bevacizumab for treatment of neovascular age-related macular degeneration: Two-year results. Ophthalmology 2012, 119, 1388–1398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chakravarthy, U.; Harding, S.P.; Rogers, C.A.; Downes, S.M.; Lotery, A.J.; Culliford, L.A.; Reeves, B.C.; IVAN Study Investigators. Alternative treatments to inhibit VEGF in age-related choroidal neovascularisation: 2-year findings of the IVAN randomised controlled trial. Lancet 2013, 382, 1258–1267. [Google Scholar] [CrossRef]
- Chen, Y.; Han, F. Profile of ranibizumab: Efficacy and safety for the treatment of wet age-related macular degeneration. Ther. Clin. Risk Manag. 2012, 8, 343. [Google Scholar] [PubMed] [Green Version]
- Heier, J.S.; Brown, D.M.; Chong, V.; Korobelnik, J.-F.; Kaiser, P.K.; Nguyen, Q.D.; Kirchhof, B.; Ho, A.; Ogura, Y.; Yancopoulos, G.D.; et al. Intravitreal aflibercept (VEGF trap-eye) in wet age-related macular degeneration. Ophthalmology 2012, 119, 2537–2548. [Google Scholar] [CrossRef] [PubMed]
- Falavarjani, K.G.; Nguyen, Q. Adverse events and complications associated with intravitreal injection of anti-VEGF agents: A review of literature. Eye 2013, 27, 787–794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azad, R.; Chandra, P.; Gupta, R. The economic implications of the use of anti-vascular endothelial growth factor drugs in age-related macular degeneration. Indian J. Ophthalmol. 2007, 55, 441. [Google Scholar] [CrossRef]
- Droege, K.M.; Muether, P.S.; Hermann, M.M.; Caramoy, A.; Viebahn, U.; Kirchhof, B.; Fauser, S. Adherence to ranibizumab treatment for neovascular age-related macular degeneration in real life. Graefe Arch. Clin. Exp. Ophthalmol. 2013, 251, 1281–1284. [Google Scholar] [CrossRef]
- Barthelmes, D.; Nguyen, V.; Daien, V.; Campain, A.; Walton, R.; Guymer, R.; Morlet, N.; Hunyor, A.P.; Essex, R.W.; Arnold, J.J.; et al. Two year outcomes of “treat and extend” intravitreal therapy using aflibercept preferentially for neovascular age-related macular degeneration. Retina 2018, 38, 20–28. [Google Scholar] [CrossRef]
- Gillies, M.C.; Campain, A.; Barthelmes, D.; Simpson, J.M.; Arnold, J.J.; Guymer, R.H.; McAllister, I.L.; Essex, R.W.; Morlet, N.; Hunyor, A.P. Long-term outcomes of treatment of neovascular age-related macular degeneration: Data from an observational study. Ophthalmology 2015, 122, 1837–1845. [Google Scholar] [CrossRef]
- Fung, A.E.; Lalwani, G.A.; Rosenfeld, P.J.; Dubovy, S.R.; Michels, S.; Feuer, W.J.; Puliafito, C.A.; Davis, J.L.; Flynn Jr, H.W.; Esquiabro, M. An optical coherence tomography-guided, variable dosing regimen with intravitreal ranibizumab (Lucentis) for neovascular age-related macular degeneration. Am. J. Ophthalmol. 2007, 143, 566–583.e562. [Google Scholar] [CrossRef]
- Johnston, R.L.; Carius, H.-J.; Skelly, A.; Ferreira, A.; Milnes, F.; Mitchell, P. A retrospective study of ranibizumab treatment regimens for neovascular age-related macular degeneration (nAMD) in Australia and the United Kingdom. Adv. Ther. 2017, 34, 703–712. [Google Scholar] [CrossRef] [Green Version]
- Holz, F.G.; Amoaku, W.; Donate, J.; Guymer, R.H.; Kellner, U.; Schlingemann, R.O.; Weichselberger, A.; Staurenghi, G.; SUSTAIN Study Group. Safety and efficacy of a flexible dosing regimen of ranibizumab in neovascular age-related macular degeneration: The SUSTAIN study. Ophthalmology 2011, 118, 663–671. [Google Scholar] [CrossRef] [PubMed]
- Wykoff, C.C.; Croft, D.E.; Brown, D.M.; Wang, R.; Payne, J.F.; Clark, L.; Abdelfattah, N.S.; Sadda, S.R.; Group, T.-A.S. Prospective trial of treat-and-extend versus monthly dosing for neovascular age-related macular degeneration: TREX-AMD 1-year results. Ophthalmology 2015, 122, 2514–2522. [Google Scholar] [CrossRef] [Green Version]
- Brand, C.; Lacey, S. One-year outcomes with ranibizumab in treatment naïve patients with neovascular age-related macular degeneration: An interim analysis from the LUMINOUS™ study. Investig. Ophthalmol. Vis. Sci. 2016, 57, 515. [Google Scholar]
- Rosenfeld, P.; Brown, D.; Heier, J.; Boyer, D.; Kaiser, P.; Chung, C.; Kim, R. MARINA Study Group Ranibizumab for age-related macular degeneration. N. Engl. J. Med. 2006, 355, 1419–1431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brooks, H.L.; Caballero, S.; Newell, C.K.; Steinmetz, R.L.; Watson, D.; Segal, M.S.; Harrison, J.K.; Scott, E.W.; Grant, M.B. Vitreous Levels of Vascular Endothelial Growth Factor and Stromal-DerivedFactor 1 in Patients With Diabetic Retinopathy and Cystoid Macular Edema Beforeand After Intraocular Injection of Triamcinolone. Arch. Ophthalmol. 2004, 122, 1801–1807. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuda, S.; Gomi, F.; Oshima, Y.; Tohyama, M.; Tano, Y. Vascular endothelial growth factor reduced and connective tissue growth factor induced by triamcinolone in ARPE19 cells under oxidative stress. Investig. Ophthalmol. Vis. Sci. 2005, 46, 1062–1068. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edelman, J.L.; Lutz, D.; Castro, M.R. Corticosteroids inhibit VEGF-induced vascular leakage in a rabbit model of blood–retinal and blood-aqueous barrier breakdown. Exp. Eye Res. 2005, 80, 249–258. [Google Scholar] [CrossRef]
- Obata, R.; Iriyama, A.; Inoue, Y.; Takahashi, H.; Tamaki, Y.; Yanagi, Y. Triamcinolone acetonide suppresses early proangiogenic response in retinal pigment epithelial cells after photodynamic therapy in vitro. Br. J. Ophthalmol. 2007, 91, 100–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Floman, N.; Zor, U. Mechanism of steroid action in ocular inflammation: Inhibition of prostaglandin production. Investig. Ophthalmol. Vis. Sci. 1977, 16, 69–73. [Google Scholar]
- Kang, B.-S.; Chung, E.-Y.; Yun, Y.-P.; Lee, M.K.; Lee, Y.R.; Lee, K.-S.; Min, K.R.; Kim, Y. Inhibitory effects of anti-inflammatory drugs on interleukin-6 bioactivity. Biol. Pharm. Bull. 2001, 24, 701–703. [Google Scholar] [CrossRef] [Green Version]
- Sarao, V.; Veritti, D.; Boscia, F.; Lanzetta, P. Intravitreal steroids for the treatment of retinal diseases. Sci. World J. 2014, 2014, 989501. [Google Scholar] [CrossRef] [Green Version]
- Arikan, G.; Osman Saatci, A.; Hakan Oner, F. Immediate intraocular pressure rise after intravitreal injection of ranibizumab and two doses of triamcinolone acetonide. Int. J. Ophthalmol. 2011, 4, 402–405. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.K.; Fan, D.S.; Chan, W.M.; Lai, W.W.; Lee, V.Y.; Lam, D.S. Ocular-hypertensive response and corneal endothelial changes after intravitreal triamcinolone injections in Chinese subjects: A 6-month follow-up study. Eye 2005, 19, 625–630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veritti, D.; Di Giulio, A.; Sarao, V.; Lanzetta, P. Drug safety evaluation of intravitreal triamcinolone acetonide. Expert Opin. Drug Saf. 2012, 11, 331–340. [Google Scholar] [CrossRef]
- Chu, Y.K.; Chung, E.J.; Kwon, O.W.; Lee, J.H.; Koh, H.J. Objective evaluation of cataract progression associated with a high dose intravitreal triamcinolone injection. Eye 2008, 22, 895–899. [Google Scholar] [CrossRef] [PubMed]
- Smithen, L.M.; Ober, M.D.; Maranan, L.; Spaide, R.F. Intravitreal triamcinolone acetonide and intraocular pressure. Am. J. Ophthalmol. 2004, 138, 740–743. [Google Scholar] [CrossRef]
- Colucciello, M. Intravitreal bevacizumab and triamcinolone acetonide combination therapy for exudative neovascular age-related macular degeneration: Short-term optical coherence tomography results. J. Ocul. Pharmacol. Ther. 2008, 24, 15–24. [Google Scholar] [CrossRef]
- Jonas, J.B.; Libondi, T.; Golubkina, L.; Spandau, U.H.; Schlichtenbrede, F.; Rensch, F. Combined intravitreal bevacizumab and triamcinolone in exudative age-related macular degeneration. Acta Ophthalmol. 2010, 88, 630–634. [Google Scholar] [CrossRef]
- Kamppeter, B.A.; Cej, A.; Jonas, J.B. Intraocular concentration of triamcinolone acetonide after intravitreal injection in the rabbit eye. Ophthalmology 2008, 115, 1372–1375. [Google Scholar] [CrossRef]
- Campochiaro, P.A.; Brown, D.M.; Pearson, A.; Chen, S.; Boyer, D.; Ruiz-Moreno, J.; Garretson, B.; Gupta, A.; Hariprasad, S.M.; Bailey, C.; et al. Sustained delivery fluocinolone acetonide vitreous inserts provide benefit for at least 3 years in patients with diabetic macular edema. Ophthalmology 2012, 119, 2125–2132. [Google Scholar] [CrossRef]
- Hauser, D.; Bukelman, A.; Pokroy, R.; Katz, H.; Len, A.; Thein, R.; Parness-Yossifon, R.; Pollack, A. Intravitreal triamcinolone for diabetic macular edema: Comparison of 1, 2, and 4 mg. Retina 2008, 28, 825–830. [Google Scholar] [CrossRef]
- Kane, F.E.; Green, K.E. Ocular pharmacokinetics of fluocinolone acetonide following Iluvien implantation in the vitreous humor of rabbits. J. Ocul Pharm. 2015, 31, 11–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campochiaro, P.A.; Nguyen, Q.D.; Hafiz, G.; Bloom, S.; Brown, D.M.; Busquets, M.; Ciulla, T.; Feiner, L.; Sabates, N.; Billman, K.; et al. Aqueous levels of fluocinolone acetonide after administration of fluocinolone acetonide inserts or fluocinolone acetonide implants. Ophthalmology 2013, 120, 583–587. [Google Scholar] [CrossRef] [PubMed]
- Valamanesh, F.; Berdugo, M.; Sennlaub, F.; Savoldelli, M.; Goumeaux, C.; Houssier, M.; Jeanny, J.C.; Torriglia, A.; Behar-Cohen, F. Effects of triamcinolone acetonide on vessels of the posterior segment of the eye. Mol. Vis. 2009, 15, 2634–2648. [Google Scholar] [PubMed]
- Li, J.; Cheng, T.; Tian, Q.; Cheng, Y.; Zhao, L.; Zhang, X.; Qu, Y. A more efficient ocular delivery system of triamcinolone acetonide as eye drop to the posterior segment of the eye. Drug Deliv. 2019, 26, 188–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shubber, S.; Vllasaliu, D.; Rauch, C.; Jordan, F.; Illum, L.; Stolnik, S. Mechanism of mucosal permeability enhancement of CriticalSorb® (Solutol® HS15) investigated in vitro in cell cultures. Pharm. Res. 2015, 32, 516–527. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| RBZ-PRN | RBZ-TALF | p | |
|---|---|---|---|
| Age | 70.9 ± 10.46 | 71.5 ± 6.65 | 0.6795 |
| Gender | 0.9577 | ||
| Male (n) | 5 | 3 | |
| Female (n) | 5 | 5 | |
| Eye | 0.6353 | ||
| OD (n) | 5 | 4 | |
| OS (n) | 5 | 4 | |
| Morbidity | 0.1675 | ||
| Hipertension (n) | 5 | 2 | |
| Diabetes Mellitus (n) | 0 | 3 | |
| Ocular findings | |||
| Pseudophakic (n) | 2 | 4 | 0.2732 |
| Basal BCVA (ETDRS letters) | 57.5 ± 13.2 | 56.1 ± 14.8 | 0.8113 |
| Basal CFT (μm) | 334.5 ± 106.9 | 399.1 ± 75.6 | 0.1522 |
| BCVA | CFT | IOP | |||||||
|---|---|---|---|---|---|---|---|---|---|
| (ETDRS Letters) | (μm) | (mmHg) | |||||||
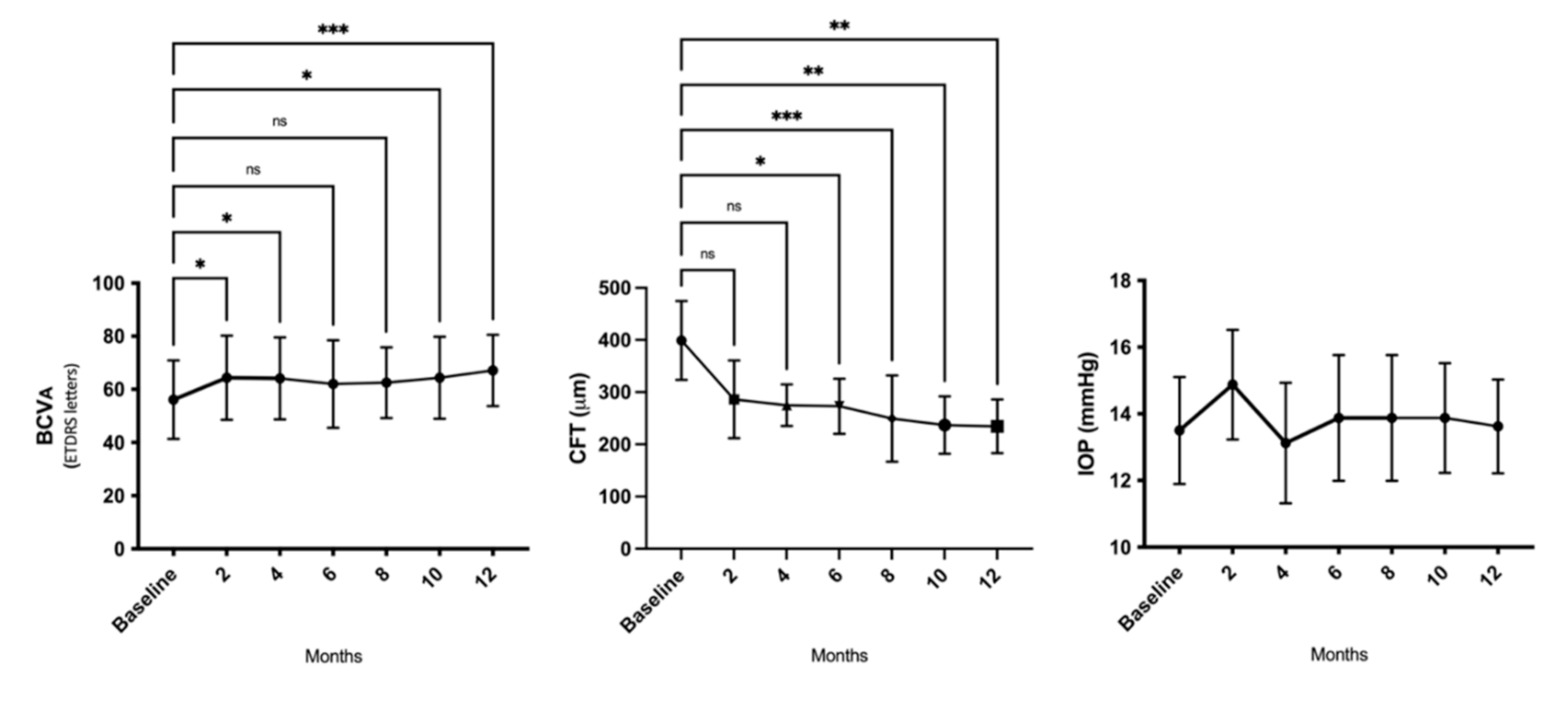
| Patient | Baseline | Month 6 | Month 12 | Baseline | Month 6 | Month 12 | Baseline | Month 6 | Month 12 |
| 1 | 75 | 75 | 80 | 413 | 334 | 333 | 14 | 14 | 15 |
| 2 | 60 | 79 | 80 | 316 | 215 | 225 | 13 | 12 | 15 |
| 3 | 68 | 76 | * | 319 | 245 | * | 13 | 16 | * |
| 4 | 65 | 65 | 70 | 323 | 286 | 287 | 13 | 14 | 13 |
| 5 | 39 | 40 | 57 | 452 | 223 | 211 | 14 | 12 | 13 |
| 6 | 54 | 58 | 65 | 453 | 353 | 182 | 15 | 17 | 14 |
| 7 | 34 | 35 | 40 | 446 | 272 | 198 | 16 | 16 | 15 |
| 8 | 72 | 72 | 76 | 493 | 284 | 199 | 12 | 12 | 11 |
| 9 | 48 | * | * | 320 | * | * | 14 | * | * |
| 10 | 50 | 72 | 69 | 297 | 217 | 241 | 11 | 14 | 13 |
| Mean ± SD | 56.1 ± 14.8 | 62.0 ± 16.5 | 67.1 ± 13.4 † | 399.1 ± 75.6 | 273 ± 52.7 † | 234.5 ± 51.4 † | 13.5 ± 1.6 | 13.9 ± 1.9 | 13.6 ± 1.4 |
| RBZ-PRN | RBZ-TALF | p | |||
|---|---|---|---|---|---|
| Baseline | Month 12 | Baseline | Month 12 | between Groups | |
| Average BCVA (ETDRS letters) | 57.5 ± 13.2 | 63 ± 15.49 | 56.1 ± 14.8 | 67.1 ± 13.4 | 0.6484 |
| Gain in ETDRS letters | 5.5 ± 14.99 | 11.0 ± 7.0 | 0.4445 | ||
| Average CFT(μm) | 334.5 ± 106.9 | 237.2 ± 31.13 | 399.1 ± 75.6 | 234.5 ± 51.4 | 0.6484 |
| CFT change (μm) | 97.3 ± 95.29 | 97.3 ± 95.29 | 164.6 ± 108.1 | 0.1525 | |
| Intravitreal injections (n) | 6.1 ± 1.28 | 2.5 ± 1.41 | 0.0004 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Navarro-Partida, J.; Altamirano-Vallejo, J.C.; Aceves Franco, L.A.; Gonzalez-Cortes, J.; Hernandez-Da Mota, S.; García-Aguirre, J.G.; Azuara-Galindo, C.D.; Castro-Castaneda, C.R.; Armendariz-Borunda, J.; Santos, A. Topical Triamcinolone Acetonide-Loaded Liposome Formulation Used as an Adjuvant to Intravitreal Ranibizumab Therapy for Neovascular Age-Related Macular Degeneration. Pharmaceutics 2021, 13, 1491. https://doi.org/10.3390/pharmaceutics13091491
Navarro-Partida J, Altamirano-Vallejo JC, Aceves Franco LA, Gonzalez-Cortes J, Hernandez-Da Mota S, García-Aguirre JG, Azuara-Galindo CD, Castro-Castaneda CR, Armendariz-Borunda J, Santos A. Topical Triamcinolone Acetonide-Loaded Liposome Formulation Used as an Adjuvant to Intravitreal Ranibizumab Therapy for Neovascular Age-Related Macular Degeneration. Pharmaceutics. 2021; 13(9):1491. https://doi.org/10.3390/pharmaceutics13091491
Chicago/Turabian StyleNavarro-Partida, Jose, Juan Carlos Altamirano-Vallejo, Luis Abraham Aceves Franco, Jesús Gonzalez-Cortes, Sergio Hernandez-Da Mota, Jose Gerardo García-Aguirre, Carlos David Azuara-Galindo, Carlos Rodrigo Castro-Castaneda, Juan Armendariz-Borunda, and Arturo Santos. 2021. "Topical Triamcinolone Acetonide-Loaded Liposome Formulation Used as an Adjuvant to Intravitreal Ranibizumab Therapy for Neovascular Age-Related Macular Degeneration" Pharmaceutics 13, no. 9: 1491. https://doi.org/10.3390/pharmaceutics13091491