
A Quality by Design Framework for Capsule-Based Dry Powder Inhalers

 , ,
, ,
Abstract
:1. Introduction
2. Overview of Quality by Design Approach for cDPIs
3. Critical Material Attributes (CMAs) in cDPIs
3.1. CMAs Related Capsule Properties
3.1.1. Capsule Material
3.1.2. Capsule Dimension
3.1.3. Capsule Hardness and Stiffness
3.1.4. Others
3.2. CMAs Related cDPIs Device Design
3.2.1. Grid Structure
3.2.2. Mouthpiece Length
3.2.3. Capsule Chamber Design
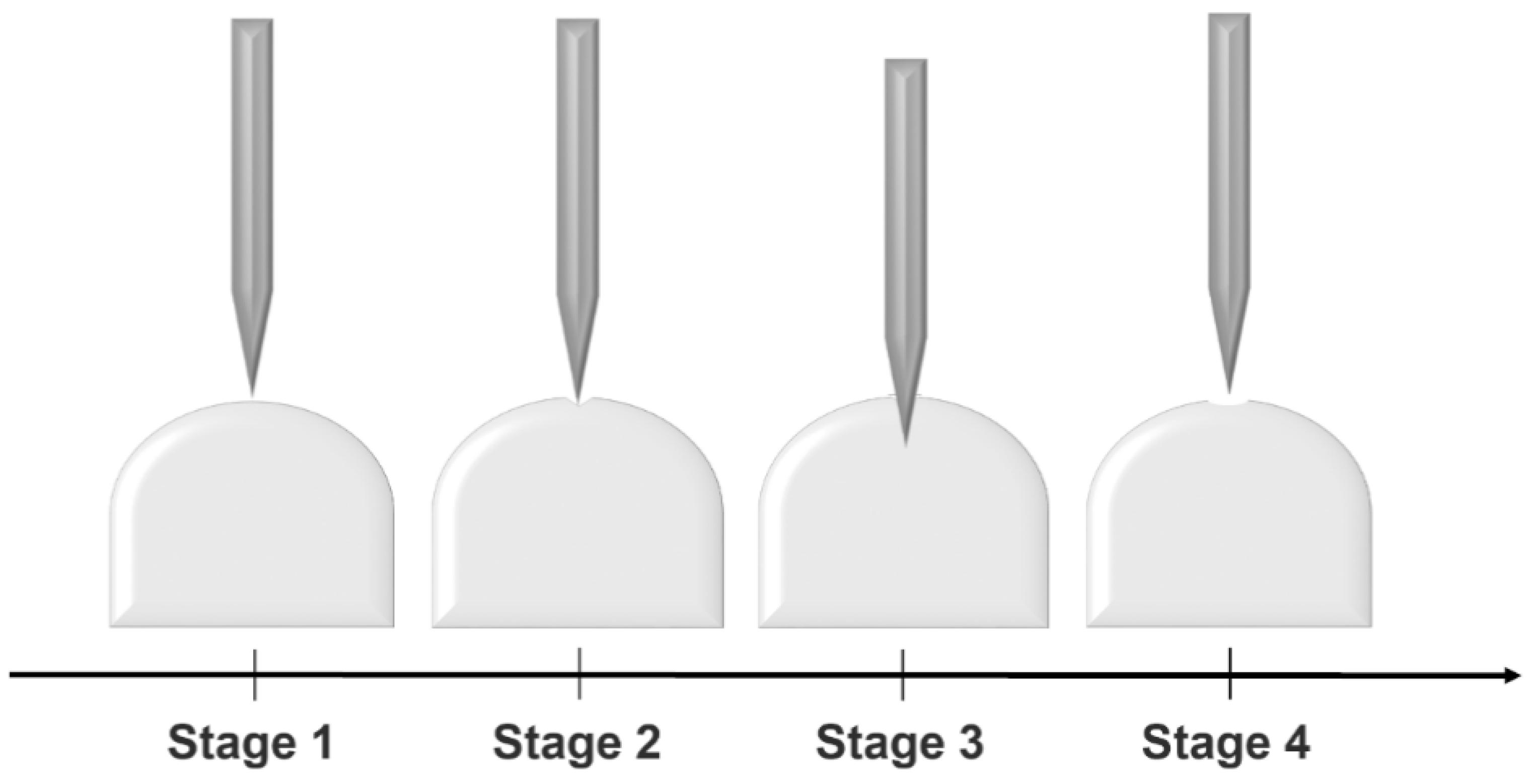
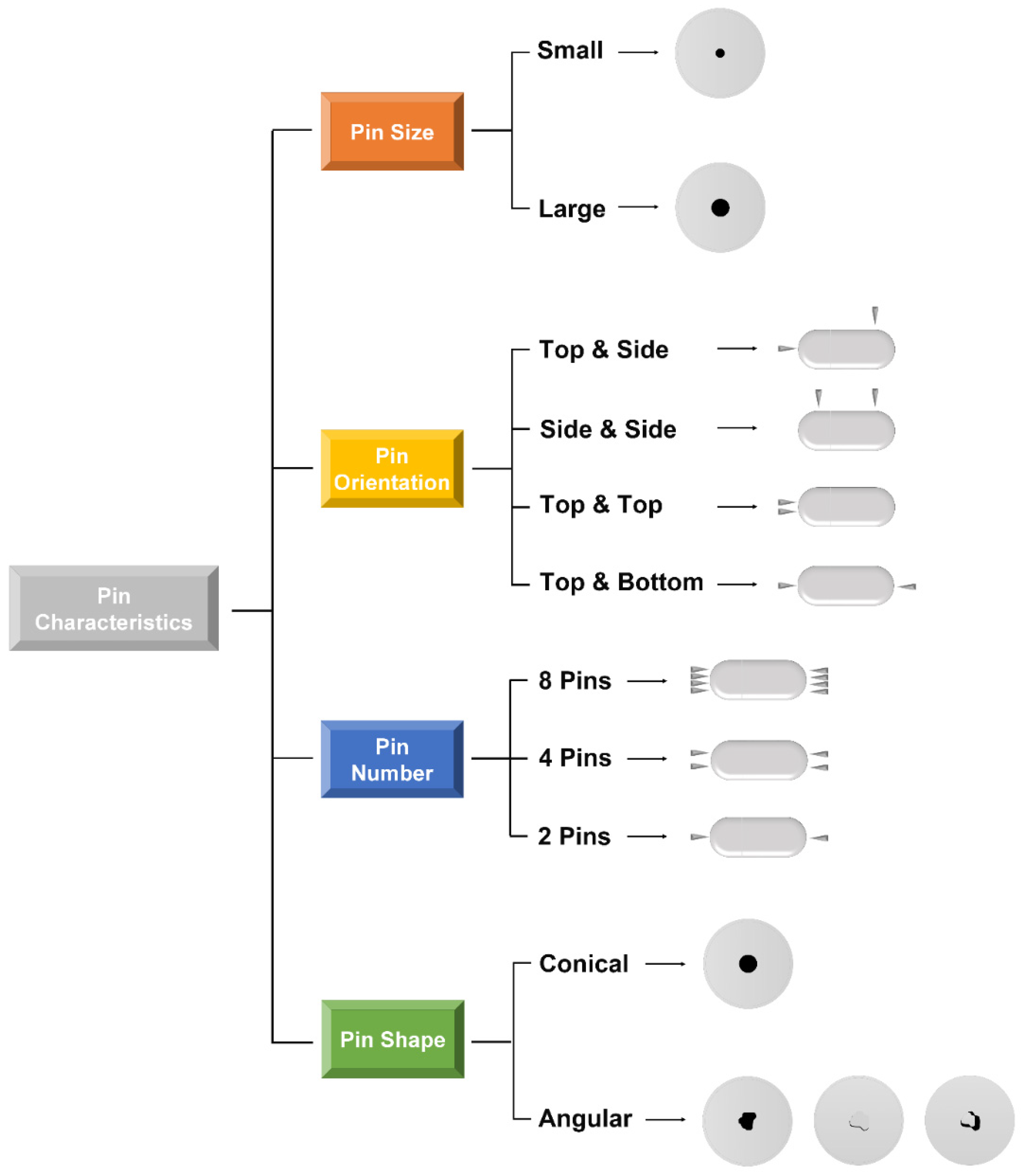
3.2.4. Capsule-Opening Mechanisms
Pin Number
Pin Orientation
Pin Size
Pin Shape
3.3. Dry Powder Related CMAs
3.3.1. Carrier-Free Systems

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dry Powder Related CMAs | CQAs | QTPP | Comments | References |
|---|---|---|---|---|
| API particle morphology | Powder dispersion and de-aggregation | Target drug effects in deep lung | Higher porosity of the API particles gives more lung deposition | [99] |
| API particle size | Powder dispersion and de-aggregation | Target drug effects in deep lung | Smaller size API particles gives more lung deposition | [90,93] |
| API particle density | Powder dispersion and de-aggregation | Target drug effects in deep lung | API particles with lower density gives more lung deposition | [91] |
| API/carrier hygroscopicity | Powder dispersion, de-aggregation, and detachment from carriers | Target drug effects in deep lung | Particle interactions may be dominated by the action of capillary forces in powder systems if humidity has surpassed critical levels | [100] |
| API particle electrostatic charging | Powder dispersion and de-aggregation | Target drug effects in deep lung | API particles with lower charge gives more lung deposition | [49] |
| API stability | Effective dose delivery | Ensuring therapeutic effect, avoiding side effects | API particles with better stability gives more effective dose delivery | [101] |
| API impurity | Effective dose delivery | Ensuring therapeutic effect and avoiding side effects | API particles with less impurity gives more effective dose delivery | [102] |
| API/carrier surface roughness/rugosity | API dispersion and detachment | Target drug effects in deep lung | API particles with rougher gives more lung deposition; the decrease of the surface roughness of lactose carrier particles in terbutaline sulfate delivery case gives more lung deposition | [103,104,105] |
| Carrier electrostatic charging | API dispersion and detachment | Target drug effects in deep lung | API particles with lower charge gives more lung deposition | [49] |
| Carrier particle shape | API dispersion and detachment | Target drug effects in deep lung | The values of either the surface factor or the elongation ratio of lactose in direct proportion to the dispersibility of salbutamol sulfate | [106] |
| Carrier crystallinity/polymorphs | API dispersion and detachment | Target drug effects in deep lung | α-lactose monohydrate has better performance than anhydrous β-lactose | [107] |
| Carrier impurity | API dispersion and detachment | Target drug effects in deep lung | Impurities may be responsible for an increase in the adhesive forces between drug and carrier particles | [108] |
| Carrier particle size | API dispersion and detachment | Target drug effects in deep lung | Reduction of carrier particle size has been proved to ameliorate the aerosolization of various drugs. However, the too-small carrier can also lead to poor flow properties in the powder due to stronger charging interactions caused by increased surface area | [70,109,110] |
3.3.2. Carrier-Based Systems
4. Critical Process Parameters (CPPs) in cDPIs
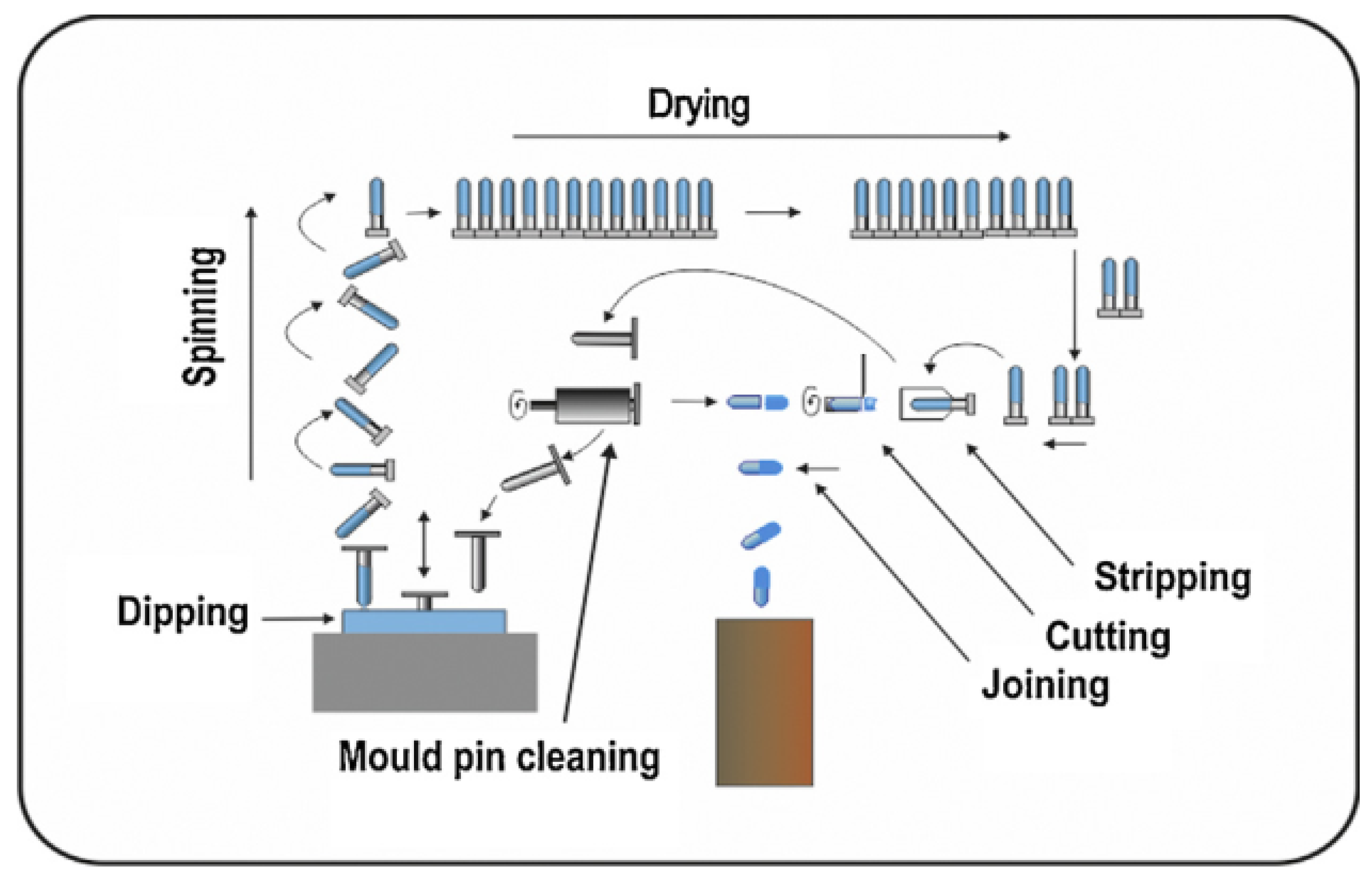
4.1. Capsule Manufacturing
4.2. Capsule Coating Involvement
4.3. Capsule Filling Control
4.3.1. Filling Method
4.3.2. Filling Weight Variability
4.3.3. Capsule Fill Weight Effects
4.4. Capsule Storage Control
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Van der Palen, J.; Klein, J.; Van Herwaarden, C.; Zielhuis, G.; Seydel, E. Multiple inhalers confuse asthma patients. Eur. Respir. J. 1999, 14, 1034–1037. [Google Scholar] [CrossRef] [Green Version]
- Jarvis, S.; Ind, P.W.; Shiner, R.J. Inhaled Therapy in Elderly COPD Patients; Time for Re-Evaluation? Oxford University Press: Oxford, UK, 2007. [Google Scholar]
- Schuster, A.; Haliburn, C.; Döring, G.; Goldman, M.H.; Group, F.S. Safety, efficacy and convenience of colistimethate sodium dry powder for inhalation (Colobreathe DPI) in patients with cystic fibrosis: A randomised study. Thorax 2013, 68, 344–350. [Google Scholar] [CrossRef] [Green Version]
- Ding, L.; Wang, J.; Cai, S.; Smyth, H.; Cui, Z. Pulmonary Biofilm-Based Chronic Infections and Inhaled Treatment Strategies. Int. J. Pharm. 2021, 604, 120768. [Google Scholar] [CrossRef] [PubMed]
- Brunaugh, A.D.; Seo, H.; Warnken, Z.; Ding, L.; Seo, S.H.; Smyth, H.D.C. Development and Evaluation of Inhalable Composite Niclosamide-Lysozyme Particles: A Broad-Spectrum, Patient-Adaptable Treatment for Coronavirus Infections and Sequalae. PLoS ONE 2021, 16, e0246803. [Google Scholar] [CrossRef]
- Klonoff, D.C. Afrezza Inhaled Insulin: The Fastest-Acting FDA-Approved Insulin on the Market Has Favorable Properties; SAGE: Los Angeles, CA, USA, 2014. [Google Scholar]
- Anderson, P.J. History of aerosol therapy: Liquid nebulization to MDIs to DPIs. Respir. Care 2005, 50, 1139–1150. [Google Scholar]
- Berkenfeld, K.; Lamprecht, A.; McConville, J.T. Devices for dry powder drug delivery to the lung. AAPS PharmSciTech 2015, 16, 479–490. [Google Scholar] [CrossRef] [PubMed]
- Wauthoz, N.; Hennia, I.; Dejaeger, B.; Ecenarro, S.; Amighi, K. Proposed algorithm for healthcare professionals based on product characteristics and in vitro performances in different use conditions using formoterol-based marketed products for inhalation. Int. J. Pharm. 2017, 530, 415–429. [Google Scholar] [CrossRef]
- Edwards, D. Applications of capsule dosing techniques for use in dry powder inhalers. Ther. Deliv. 2010, 1, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Chrystyn, H. The DiskusTM: A review of its position among dry powder inhaler devices. Int. J. Clin. Pract. 2007, 61, 1022–1036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, M.Y.; Chan, J.G.Y.; Chan, H.-K. Pulmonary drug delivery by powder aerosols. J. Control. Release 2014, 193, 228–240. [Google Scholar] [CrossRef]
- Islam, N.; Gladki, E. Dry powder inhalers (DPIs)—A review of device reliability and innovation. Int. J. Pharm. 2008, 360, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Birchall, J.; Jones, B.; Morrissey, A.; Jones, B. A comparison of the puncturing properties of gelatin and hypromellose capsules for use in dry powder inhalers. Drug Dev. Ind. Pharm. 2008, 34, 870–876. [Google Scholar] [CrossRef] [PubMed]
- Muralidharan, P.; Hayes, D., Jr.; Mansour, H.M. Dry powder inhalers in COPD, lung inflammation and pulmonary infections. Expert Opin. Drug Deliv. 2015, 12, 947–962. [Google Scholar] [CrossRef] [Green Version]
- Martinelli, F.; Balducci, A.G.; Rossi, A.; Sonvico, F.; Colombo, P.; Buttini, F. “Pierce and inhale” design in capsule based dry powder inhalers: Effect of capsule piercing and motion on aerodynamic performance of drugs. Int. J. Pharm. 2015, 487, 197–204. [Google Scholar] [CrossRef]
- Elkins, M.R.; Robinson, P.; Anderson, S.D.; Perry, C.P.; Daviskas, E.; Charlton, B. Inspiratory flows and volumes in subjects with cystic fibrosis using a new dry powder inhaler device. Open Respir. Med. J. 2014, 8, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanders, M. Inhalation therapy: An historical review. Prim. Care Respir. J. 2007, 16, 71. [Google Scholar] [CrossRef] [Green Version]
- Bell, J.; Hartley, P.; Cox, J. Dry powder aerosols I: A new powder inhalation device. J. Pharm. Sci. 1971, 60, 1559–1564. [Google Scholar] [CrossRef]
- Lawrence, X.Y.; Li, B.V. FDA Bioequivalence Standards; Springer: New York, NY, USA, 2014; Volume 13. [Google Scholar]
- Weers, J.G.; Miller, D.P. Formulation design of dry powders for inhalation. J. Pharm. Sci. 2015, 104, 3259–3288. [Google Scholar] [CrossRef] [PubMed]
- Donovan, M.J.; Kim, S.H.; Raman, V.; Smyth, H.D. Dry powder inhaler device influence on carrier particle performance. J. Pharm. Sci. 2012, 101, 1097–1107. [Google Scholar] [CrossRef]
- Zhou, Q.T.; Tong, Z.; Tang, P.; Citterio, M.; Yang, R.; Chan, H.-K. Effect of device design on the aerosolization of a carrier-based dry powder inhaler—A case study on Aerolizer® Foradile®. AAPS J. 2013, 15, 511–522. [Google Scholar] [CrossRef] [Green Version]
- Coates, M.S.; Chan, H.-K.; Fletcher, D.F.; Raper, J.A. Influence of air flow on the performance of a dry powder inhaler using computational and experimental analyses. Pharm. Res. 2005, 22, 1445–1453. [Google Scholar] [CrossRef]
- Shetty, N.; Cipolla, D.; Park, H.; Zhou, Q.T. Physical stability of dry powder inhaler formulations. Expert Opin. Drug Deliv. 2020, 17, 77–96. [Google Scholar] [CrossRef] [Green Version]
- de Boer, A.H.; Hagedoorn, P.; Hoppentocht, M.; Buttini, F.; Grasmeijer, F.; Frijlink, H.W. Dry powder inhalation: Past, present and future. Expert Opin. Drug Deliv. 2017, 14, 499–512. [Google Scholar] [CrossRef] [Green Version]
- Levy, M.L.; Carroll, W.; Izquierdo Alonso, J.L.; Keller, C.; Lavorini, F.; Lehtimäki, L. Understanding Dry Powder Inhalers: Key Technical and Patient Preference Attributes. Adv Ther. 2019, 36, 2547–2557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lavorini, F.; Pistolesi, M.; Usmani, O.S. Recent advances in capsule-based dry powder inhaler technology. Multidiscip Respir. Med. 2017, 12, 11. [Google Scholar] [CrossRef]
- Mishra, V.; Thakur, S.; Patil, A.; Shukla, A. Quality by design (QbD) approaches in current pharmaceutical set-up. Expert Opin. Drug Deliv. 2018, 15, 737–758. [Google Scholar] [CrossRef] [PubMed]
- Haleem, R.M.; Salem, M.Y.; Fatahallah, F.A.; Abdelfattah, L.E. Quality in the pharmaceutical industry–A literature review. Saudi Pharm. J. 2015, 23, 463–469. [Google Scholar] [CrossRef] [Green Version]
- Buttini, F.; Rozou, S.; Rossi, A.; Zoumpliou, V.; Rekkas, D.M. The application of quality by design framework in the pharmaceutical development of dry powder inhalers. Eur. J. Pharm. Sci. 2018, 113, 64–76. [Google Scholar] [CrossRef]
- Brunaugh, A.D.; Smyth, H.D. Formulation techniques for high dose dry powders. Int. J. Pharm. 2018, 547, 489–498. [Google Scholar] [CrossRef]
- Seville, P.C.; Li, H.-y.; Learoyd, T.P. Spray-dried powders for pulmonary drug delivery. Crit. Rev. Ther. Drug Carr. Syst. 2007, 24, 307–360. [Google Scholar] [CrossRef]
- Mansour, H.M.; Rhee, Y.S.; Wu, X. Nanomedicine in pulmonary delivery. Int. J. Nanomed. 2009, 4, 299–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brunaugh, A.D.; Sharma, S.; Smyth, H. Inhaled fixed-dose combination powders for the treatment of respiratory infections. Expert Opin. Drug Deliv. 2021, 18, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Dal Negro, R.W.; Turco, P.; Povero, M. Patients’ usability of seven most used dry-powder inhalers in COPD. Multidiscip. Respir. Med. 2019, 14, 1–9. [Google Scholar]
- Renswouw, D.C.V.; Laarhoven, A.C.V.; Haren, M.J.V.; Bouvy, M.L.; Weda, M. Storage instructions for inhalation capsules: Consequences of incorrect storage and adherence in daily practice. J. Pharm. Pract. 2010, 23, 548–552. [Google Scholar] [CrossRef]
- Perera, A.D.; Kapitza, C.; Nosek, L.; Fishman, R.S.; Shapiro, D.A.; Heise, T.; Heinemann, L. Absorption and metabolic effect of inhaled insulin: Intrapatient variability after inhalation via the Aerodose insulin inhaler in patients with type 2 diabetes. Diabetes Care 2002, 25, 2276–2281. [Google Scholar] [CrossRef] [Green Version]
- Lee, A.Y.; Cho, M.-H.; Kim, S. Recent advances in aerosol gene delivery systems using non-viral vectors for lung cancer therapy. Expert Opin. Drug Deliv. 2019, 16, 757–772. [Google Scholar] [CrossRef]
- Wenzler, E.; Fraidenburg, D.R.; Scardina, T.; Danziger, L.H. Inhaled Antibiotics for Gram-Negative Respiratory Infections. Clin. Microbiol. Rev. 2016, 29, 581–632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawrence, X.Y.; Amidon, G.; Khan, M.A.; Hoag, S.W.; Polli, J.; Raju, G.; Woodcock, J. Understanding pharmaceutical quality by design. AAPS J. 2014, 16, 771–783. [Google Scholar]
- Jones, B.E. Manufacture and Properties of Two-Piece Hard Capsules; Pharmaceutical Capsules, Pharmaceutical Press: London, UK, 2004; pp. 79–100. [Google Scholar]
- Stegemann, S.; Connolly, P.; Matthews, W.; Barnett, R.; Aylott, M.; Schrooten, K.; Cadé, D.; Taylor, A.; Bresciani, M. Application of QbD principles for the evaluation of empty hard capsules as an input parameter in formulation development and manufacturing. AAPS PharmSciTech 2014, 15, 542–549. [Google Scholar] [CrossRef] [Green Version]
- Mei, X.; Etzler, F.M.; Wang, Z. Use of Texture Analysis to Study Hydrophilic Solvent Effects on the Mechanical Properties of Hard Gelatin Capsules. Int. J. Pharm. 2006, 324, 128–135. [Google Scholar] [CrossRef]
- Majee, S.B.; Avlani, D.; Biswas, G. HPMC as capsule shell material: Physicochemical, pharmaceutical and biopharmaceutical properties. Int. J. Pharm. Pharm. Sci. 2017, 9, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Chang, R.K.; Raghavan, K.S.; Hussain, M.A. A study on gelatin capsule brittleness: Moisture tranfer between the capsule shell and its content. J. Pharm. Sci. 1998, 87, 556–558. [Google Scholar] [CrossRef] [PubMed]
- Stegemann, S. Non-Gelatin-Based Capsules. In Pharmaceutical Dosage Forms; CRC Press: London, UK, 2017; pp. 111–130. [Google Scholar]
- Tan, S.; Newton, J. Influence of capsule dosator wall texture and powder properties on the angle of wall friction and powder-wall adhesion. Int. J. Pharm. 1990, 64, 227–234. [Google Scholar] [CrossRef]
- Heng, D.; Lee, S.H.; Ng, W.K.; Chan, H.-K.; Kwek, J.W.; Tan, R.B. Novel alternatives to reduce powder retention in the dry powder inhaler during aerosolization. Int. J. Pharm. 2013, 452, 194–200. [Google Scholar] [CrossRef]
- Holgate, S. Inhaled sodium cromoglycate. Respir. Med. 1996, 90, 387–390. [Google Scholar] [CrossRef] [Green Version]
- Saim, S.; Horhota, S.T. Process for overcoming drug retention in hard gelatin inhalation capsules. Drug Dev. Ind. Pharm. 2002, 28, 641–654. [Google Scholar] [CrossRef]
- Araujo, R.; Soares, M.; Mazzei, J.L.; Ramos, M.; Siani, A.C. A Comparative Study of Hard Gelatin and Hypromellose Capsules Containing a Dry Extract of Senna (Cassia Angustifolia) under Controlled Temperature and Relative Humidity. Ind.J. Pharm. Sci. 2020, 82, 718–723. [Google Scholar]
- Torrisi, B.M.; Birchall, J.C.; Jones, B.E.; Díez, F.; Coulman, S.A. The development of a sensitive methodology to characterise hard shell capsule puncture by dry powder inhaler pins. Int. J. Pharm. 2013, 456, 545–552. [Google Scholar] [CrossRef]
- Testing and Comparison of Puncturing Forces for Gelatin and HPMC Inhalation Capsules. Available online: https://www.inhalationmag.com/wp-content/uploads/pdf/inh_20190601_0019.pdf (accessed on 1 April 2011).
- Jones, B. Quali-V®-I: A new key for dry powder inhalers. Drug Deliv. Technol. 2003, 3, 2–7. [Google Scholar]
- Wauthoz, N.; Hennia, I.; Ecenarro, S.; Amighi, K. Impact of capsule type on aerodynamic performance of inhalation products: A case study using a formoterol-lactose binary or ternary blend. Int. J. Pharm. 2018, 553, 47–56. [Google Scholar] [CrossRef]
- Podczeck, F. The strength and brittleness of hard shell capsules made from different materials. Bus. Brief. Pharm. Technol. 2002, 128–135. [Google Scholar]
- Chong, R.H.; Jones, B.E.; Díez, F.; Birchall, J.C.; Coulman, S.A. Evaluating the sensitivity, reproducibility and flexibility of a method to test hard shell capsules intended for use in dry powder inhalers. Int. J. Pharm. 2016, 500, 316–325. [Google Scholar] [CrossRef] [Green Version]
- Nakate, T.; Yoshida, H.; Ohike, A.; Tokunaga, Y.; Ibuki, R.; Kawashima, Y. Formulation development of inhalation powders for FK888 using the E-haler® to improve the inhalation performance at a high dose, and its absorption in healthy volunteers. Eur. J. Pharm. Biopharm. 2005, 59, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Benke, E.; Varga, P.; Szabó-Révész, P.; Ambrus, R. Stability and In Vitro Aerodynamic Studies of Inhalation Powders Containing Ciprofloxacin Hydrochloride Applying Different DPI Capsule Types. Pharmaceutics 2021, 13, 689. [Google Scholar] [CrossRef]
- Telko, M.J.; Kujanpää, J.; Hickey, A.J. Investigation of triboelectric charging in dry powder inhalers using electrical low pressure impactor (ELPI™). Int. J. Pharm. 2007, 336, 352–360. [Google Scholar] [CrossRef]
- Richardson, M. Impact of Capsule Selection on Formulation Stability in Dry Powder Inhalers (DPIs). 2011. Available online: https://www.inhalationmag.com/white-papers/capsugel/ (accessed on 1 April 2011).
- Murachanian, D. An Introduction to Two-Piece Hard Capsules and Their Marketing Benefits. In Pharmaceutical Dosage Forms; CRC Press: London, UK, 2017; pp. 15–30. [Google Scholar]
- Coates, M.S.; Fletcher, D.F.; Chan, H.-K.; Raper, J.A. The role of capsule on the performance of a dry powder inhaler using computational and experimental analyses. Pharm. Res. 2005, 22, 923–932. [Google Scholar] [CrossRef] [Green Version]
- Kuentz, M.; Rothenhäusler, B.; Röthlisberger, D. Time domain 1H NMR as a new method to monitor softening of gelatin and HPMC capsule shells. Drug Dev. Ind. Pharm. 2006, 32, 1165–1173. [Google Scholar] [CrossRef] [PubMed]
- Wachtel, H. Respiratory drug delivery. In Microsystems for Pharmatechnology; Springer: Cham, Switzerland, 2016; pp. 257–274. [Google Scholar]
- Kondo, T.; Tanigaki, T.; Yokoyama, H.; Hibino, M.; Tajiri, S.; Akazawa, K.; Yamada, Y.; Cassan, S.M. Impact of holding position during inhalation on drug release from a reservoir-, blister-and capsule-type dry powder inhaler. J. Asthma 2017, 54, 792–797. [Google Scholar] [CrossRef]
- Murachanian, D. Two-piece hard capsules for pharmaceutical formulations. J. GXP Compliance 2010, 14, 31. [Google Scholar]
- Chew, N.Y.; Chan, H.-K. Influence of particle size, air flow, and inhaler device on the dispersion of mannitol powders as aerosols. Pharm. Res. 1999, 16, 1098–1103. [Google Scholar] [CrossRef]
- Steckel, H.; Müller, B.W. In vitro evaluation of dry powder inhalers I: Drug deposition of commonly used devices. Int. J. Pharm. 1997, 154, 19–29. [Google Scholar] [CrossRef]
- Coates, M.S.; Fletcher, D.F.; Chan, H.-K.; Raper, J.A. Effect of design on the performance of a dry powder inhaler using computational fluid dynamics. Part 1: Grid structure and mouthpiece length. J. Pharm. Sci. 2004, 93, 2863–2876. [Google Scholar] [CrossRef] [PubMed]
- Tuteric, T.; Vulovic, A.; Cvijic, S.; Ibric, S.; Filipovic, N. Effect of Circulation Chamber Dimensions on Aerosol Delivery Efficiency of a Commercial Dry Powder Inhaler Aerolizer®. In Proceedings of the 2017 IEEE 17th International Conference on Bioinformatics and Bioengineering (BIBE), Washington, DC, USA, 23–25 October 2017; pp. 555–558. [Google Scholar]
- Shur, J.; Lee, S.; Adams, W.; Lionberger, R.; Tibbatts, J.; Price, R. Effect of device design on the in vitro performance and comparability for capsule-based dry powder inhalers. AAPS J. 2012, 14, 667–676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benque, B.; Khinast, J.G. Understanding the motion of hard-shell capsules in dry powder inhalers. Int. J. Pharm. 2019, 567, 118481. [Google Scholar] [CrossRef]
- Sim, S.; Margo, K.; Parks, J.; Howell, R.; Hebbink, G.A.; Orlando, L.; Larson, I.; Leslie, P.; Ho, L.; Morton, D.A. An insight into powder entrainment and drug delivery mechanisms from a modified Rotahaler®. Int. J. Pharm. 2014, 477, 351–360. [Google Scholar] [CrossRef]
- Behara, S.R.; Farkas, D.R.; Hindle, M.; Longest, P.W. Development of a high efficiency dry powder inhaler: Effects of capsule chamber design and inhaler surface modifications. Pharm. Res. 2014, 31, 360–372. [Google Scholar] [CrossRef] [Green Version]
- Farkas, D.; Bonasera, S.; Bass, K.; Hindle, M.; Longest, P.W. Advancement of a Positive-Pressure Dry Powder Inhaler for Children: Use of a Vertical Aerosolization Chamber and Three-Dimensional Rod Array Interface. Pharm. Res. 2020, 37, 1–14. [Google Scholar] [CrossRef]
- Behara, S.R.; Longest, P.W.; Farkas, D.R.; Hindle, M. Development and comparison of new high-efficiency dry powder inhalers for carrier-free formulations. J. Pharm. Sci. 2014, 103, 465–477. [Google Scholar] [CrossRef] [Green Version]
- Lefebvre, Y.; Barthes-Biesel, D. Motion of a Capsule in a Cylindrical Tube: Effect of Membrane Pre-Stress. J. Fluid Mech. 2007, 589, 157–181. [Google Scholar] [CrossRef]
- Saleem, I.; Diez, F.; Jones, B.; Kayali, N.; Polo, L. Investigation on the aerosol performance of dry powder inhalation hypromellose capsules with different lubricant levels. Int. J. Pharm. 2015, 492, 258–263. [Google Scholar] [CrossRef] [Green Version]
- Son, Y.-J.; Longest, P.W.; Tian, G.; Hindle, M. Evaluation and modification of commercial dry powder inhalers for the aerosolization of a submicrometer excipient enhanced growth (EEG) formulation. Eur. J. Pharm. Sci. 2013, 49, 390–399. [Google Scholar] [CrossRef] [Green Version]
- Coates, M.S.; Chan, H.-K.; Fletcher, D.F.; Raper, J.A. Effect of design on the performance of a dry powder inhaler using computational fluid dynamics. Part 2: Air inlet size. J. Pharm. Sci. 2006, 95, 1382–1392. [Google Scholar] [CrossRef]
- Chew, N.Y.; Chan, H.-K.; Bagster, D.F.; Mukhraiya, J. Characterization of pharmaceutical powder inhalers: Estimation of energy input for powder dispersion and effect of capsule device configuration. J. Aerosol Sci. 2002, 33, 999–1008. [Google Scholar] [CrossRef]
- Behara, S.R.B.; Larson, I.; Kippax, P.; Morton, D.A.; Stewart, P. The kinetics of cohesive powder de-agglomeration from three inhaler devices. Int. J. Pharm. 2011, 421, 72–81. [Google Scholar] [CrossRef]
- Weers, J.; Clark, A. The impact of inspiratory flow rate on drug delivery to the lungs with dry powder inhalers. Pharm. Res. 2017, 34, 507–528. [Google Scholar] [CrossRef] [PubMed]
- Newman, S.P.; Chan, H.-K. In vitro/in vivo comparisons in pulmonary drug delivery. J. Aerosol Med. Pulm. Drug Deliv. 2008, 21, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Visser, J. Van der Waals and other cohesive forces affecting powder fluidization. Powder Technol. 1989, 58, 1–10. [Google Scholar] [CrossRef]
- Tee, S.; Marriott, C.; Zeng, X.; Martin, G. The use of different sugars as fine and coarse carriers for aerosolised salbutamol sulphate. Int. J. Pharm. 2000, 208, 111–123. [Google Scholar] [CrossRef]
- Edwards, D.; Dunbar, C. Therapeutic aerosol bioengineering. Annu. Rev. Biomed. Eng 2002, 4, 93–107. [Google Scholar] [CrossRef]
- Bosquillon, C.; Lombry, C.; Preat, V.; Vanbever, R. Influence of formulation excipients and physical characteristics of inhalation dry powders on their aerosolization performance. J. Control. Release 2001, 70, 329–339. [Google Scholar] [CrossRef]
- Brunaugh, A.D.; Wu, T.; Kanapuram, S.R.; Smyth, H.D. Effect of particle formation process on characteristics and aerosol performance of respirable protein powders. Mol. Pharm. 2019, 16, 4165–4180. [Google Scholar] [CrossRef]
- Duong, T.; López-Iglesias, C.; Szewczyk, P.K.; Stachewicz, U.; Barros, J.; Alvarez-Lorenzo, C.; Alnaief, M.; García-González, C.A. A pathway from porous particle technology toward tailoring aerogels for pulmonary drug administration. Front. Bioeng. Biotechnol. 2021, 9, 323. [Google Scholar]
- Brunaugh, A.D.; Jan, S.U.; Ferrati, S.; Smyth, H.D. Excipient-free pulmonary delivery and macrophage targeting of clofazimine via air jet micronization. Mol. Pharm. 2017, 14, 4019–4031. [Google Scholar] [CrossRef]
- Ariane, M.; Sommerfeld, M.; Alexiadis, A. Wall collision and drug-carrier detachment in dry powder inhalers: Using DEM to devise a sub-scale model for CFD calculations. Powder Technol. 2018, 334, 65–75. [Google Scholar] [CrossRef]
- Thornton, C.; Liu, L. How do agglomerates break? Powder Technol. 2004, 143, 110–116. [Google Scholar] [CrossRef]
- Subero, J.; Ning, Z.; Ghadiri, M.; Thornton, C. Effect of interface energy on the impact strength of agglomerates. Powder Technol. 1999, 105, 66–73. [Google Scholar] [CrossRef]
- Moreno, R.; Ghadiri, M.; Antony, S. Effect of the impact angle on the breakage of agglomerates: A numerical study using DEM. Powder Technol. 2003, 130, 132–137. [Google Scholar] [CrossRef]
- Moreno-Atanasio, R.; Ghadiri, M. Mechanistic analysis and computer simulation of impact breakage of agglomerates: Effect of surface energy. Chem. Eng. Sci. 2006, 61, 2476–2481. [Google Scholar] [CrossRef] [Green Version]
- Chan, H.-K. What is the role of particle morphology in pharmaceutical powder aerosols? Expert Opin. Drug Deliv. 2008, 5, 909–914. [Google Scholar] [CrossRef] [PubMed]
- Smyth, H.D.; Hickey, A.J. Carriers in drug powder delivery. Am. J. Drug Deliv. 2005, 3, 117–132. [Google Scholar] [CrossRef]
- Ellis, G. The maillard reaction. In Advances in Carbohydrate Chemistry; Elsevier: New York, NY, USA, 1959; Volume 14, pp. 63–134. [Google Scholar]
- Görög, S. The Importance and the Challenges of Impurity Profiling in Modern Pharmaceutical Analysis; Elsevier: New York, NY, USA, 2006. [Google Scholar]
- Flament, M.-P.; Leterme, P.; Gayot, A. The influence of carrier roughness on adhesion, content uniformity and the in vitro deposition of terbutaline sulphate from dry powder inhalers. Int. J. Pharm. 2004, 275, 201–209. [Google Scholar] [CrossRef]
- Newman, S.; Busse, W. Evolution of dry powder inhaler design, formulation, and performance. Respir. Med. 2002, 96, 293–304. [Google Scholar] [CrossRef] [Green Version]
- Adi, S.; Adi, H.; Chan, H.-K.; Tong, Z.; Yang, R.; Yu, A. Effects of mechanical impaction on aerosol performance of particles with different surface roughness. Powder Technol. 2013, 236, 164–170. [Google Scholar] [CrossRef]
- Zeng, X.M.; Martin, G.P.; Marriott, C.; Pritchard, J. The effects of carrier size and morphology on the dispersion of salbutamol sulphate after aerosolization at different flow rates. J. Pharm. Pharmacol. 2000, 52, 1211–1221. [Google Scholar] [CrossRef]
- Traini, D.; Young, P.M.; Thielmann, F.; Acharya, M. The influence of lactose pseudopolymorphic form on salbutamol sulfate–lactose interactions in DPI formulations. Drug Dev. Ind. Pharm. 2008, 34, 992–1001. [Google Scholar] [CrossRef] [PubMed]
- De Boer, A.; Hagedoorn, P.; Gjaltema, D.; Goede, J.; Kussendrager, K.; Frijlink, H. Air classifier technology (ACT) in dry powder inhalation Part 2. The effect of lactose carrier surface properties on the drug-to-carrier interaction in adhesive mixtures for inhalation. Int. J. Pharm. 2003, 260, 201–216. [Google Scholar] [CrossRef]
- French, D.L.; Edwards, D.A.; Niven, R.W. The influence of formulation on emission, deaggregation and deposition of dry powders for inhalation. J. Aerosol Sci. 1996, 27, 769–783. [Google Scholar] [CrossRef]
- Telko, M.; Hickey, A. Aerodynamic and electrostatic properties of model dry powder aerosols: A comprehensive study of formulation factors. AAPS PharmSciTech 2014, 15, 1378–1397. [Google Scholar] [CrossRef] [Green Version]
- Hamishehkar, H.; Rahimpour, Y.; Javadzadeh, Y. The Role of Carrier in Dry Powder Inhaler; InTech: New York, NY, USA, 2012; Volume 3. [Google Scholar]
- Voss, A.; Finlay, W.H. Deagglomeration of dry powder pharmaceutical aerosols. Int. J. Pharm. 2002, 248, 39–50. [Google Scholar] [CrossRef]
- Xu, Z.; Mansour, H.M.; Mulder, T.; McLean, R.; Langridge, J.; Hickey, A.J. Dry powder aerosols generated by standardized entrainment tubes from drug blends with lactose monohydrate: 1. Albuterol sulfate and disodium cromoglycate. J. Pharm. Sci. 2010, 99, 3398–3414. [Google Scholar] [CrossRef]
- Begat, P.; Morton, D.A.; Staniforth, J.N.; Price, R. The cohesive-adhesive balances in dry powder inhaler formulations I: Direct quantification by atomic force microscopy. Pharm. Res. 2004, 21, 1591–1597. [Google Scholar] [CrossRef]
- Telko, M.J.; Hickey, A.J. Dry powder inhaler formulation. Respir. Care 2005, 50, 1209–1227. [Google Scholar] [PubMed]
- Fowkes, F.M. Attractive forces at interfaces. Ind. Eng. Chem. 1964, 56, 40–52. [Google Scholar] [CrossRef]
- Pilcer, G.; Wauthoz, N.; Amighi, K. Lactose characteristics and the generation of the aerosol. Adv. Drug Deliv. Rev. 2012, 64, 233–256. [Google Scholar] [CrossRef] [Green Version]
- van Wachem, B.; Thalberg, K.; Remmelgas, J.; Niklasson-Björn, I. Simulation of dry powder inhalers: Combining micro-scale, meso-scale and macro-scale modeling. AIChE J. 2017, 63, 501–516. [Google Scholar] [CrossRef] [Green Version]
- Podczeck, F.; Jones, B.E. Pharmaceutical Capsules; Pharmaceutical Press: London, UK, 2004. [Google Scholar]
- Ayala, G.; Díez, F.; Gassó, M.T.; Jones, B.E.; Martín-Portugués, R.; Ramiro-Aparicio, J. Statistical tools and control of internal lubricant content of inhalation grade HPMC capsules during manufacture. Int. J. Pharm. 2016, 503, 36–40. [Google Scholar] [CrossRef]
- Rhodes, C.T.; Banker, G.S. Modern Pharmaceutics; Marcel Dekker: New York, NY, USA, 2002. [Google Scholar]
- Gullapalli, R.P.; Mazzitelli, C.L. Gelatin and non-gelatin capsule dosage forms. J. Pharm. Sci. 2017, 106, 1453–1465. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Abe, K.; Matsuura, S. Hard Capsule for Pharmaceutical Drugs and Method for Producing the Same. U.S. Patent No. 5,431,917, 11 July 1993. [Google Scholar]
- Cade, D.; Scott, R.; He, X. Polymer Film Compositions for Capsules. U.S. Patent No. US6,517,865B2, 11 February 2003. [Google Scholar]
- Yang, J.H. Cellulose Capsule Using Mixed Solution of Pectin and Glycerin and the Manufacturing Process Thereof. U.S. Patent No. 6,410,050, 25 June 2002. [Google Scholar]
- Al-Tabakha, M.M. HPMC capsules: Current status and future prospects. J. Pharm. Pharm. Sci. 2010, 13, 428–442. [Google Scholar] [CrossRef]
- Djabourov, M.; Grillon, Y.; Leblond, J. The sol-gel transition in gelatin viewed by diffusing colloidal probes. Polym. Gels Netw. 1995, 3, 407–428. [Google Scholar] [CrossRef]
- Haque, A.; Richardson, R.K.; Morris, E.R.; Gidley, M.J.; Caswell, D.C. Thermogelation of methylcellulose. Part II: Effect of hydroxypropyl substituents. Carbohydr. Polym. 1993, 22, 175–186. [Google Scholar] [CrossRef]
- Sarkar, N. Thermal gelation properties of methyl and hydroxypropyl methylcellulose. J. Appl. Polym. Sci. 1979, 24, 1073–1087. [Google Scholar] [CrossRef]
- Kalafat, J.; Powale, S.; Bhat, J.; Almeida, D.; Solanki, A. Impact of Different Capsules for Dry Powder Inhalation on Efficacy and Aerodynamic Performance of Salbutamol Inhalation Formulation. In Proceedings of the Drug Delivery to the Lung (DDL), Edinburgh, UK, 11–13 December 2019. [Google Scholar]
- Diez, F.; Bhat, J.; Powale, S.; Almeida, D.; Kalafat, J. Impact of Internal Capsule Lubricant on the Aerosol Performance of Dry Powder Inhalers. In Proceedings of the Respiratory Drug Delivery (RDD), Lisbon, Portugal, 9–10 May 2019. [Google Scholar]
- Lowell, J.; Rose-Innes, A. Contact electrification. Adv. Phys. 1980, 29, 947–1023. [Google Scholar] [CrossRef]
- Stegemann, S. Improving Pulmonary drug delivery in Capsule Inhaler Systems: Optimizing capsule based on formulation-capsule-device interactions. In Respiratory Drug Delivery Asia 2014; RDD: Goa, India, 2014; pp. 1–8. [Google Scholar]
- Bolhuis, G. Film formation by magnesium stearate during mixing and its effect on tabletting. Pharm. Weekblad. 1975, 110, 317–325. [Google Scholar]
- Hussain, M.H.; York, P.; Timmins, P. A study of the formation of magnesium stearate film on sodium chloride using energy-dispersive X-ray analysis. Int. J. Pharm. 1988, 42, 89–95. [Google Scholar] [CrossRef]
- Uzunović, A.; Vranić, E. Effect of magnesium stearate concentration on dissolution properties of ranitidine hydrochloride coated tablets. Bosn. J. Basic Med. Sci. 2007, 7, 279. [Google Scholar] [CrossRef]
- Wang, J.; Wen, H.; Desai, D. Lubrication in tablet formulations. Eur. J. Pharm. Biopharm. 2010, 75, 1–15. [Google Scholar] [CrossRef]
- Hindle, M.; Longest, P.W. Condensational growth of combination drug-excipient submicrometer particles for targeted high-efficiency pulmonary delivery: Evaluation of formulation and delivery device. J. Pharm. Pharmacol. 2012, 64, 1254–1263. [Google Scholar] [CrossRef] [Green Version]
- Longest, P.W.; Tian, G.; Li, X.; Son, Y.-J.; Hindle, M. Performance of combination drug and hygroscopic excipient submicrometer particles from a softmist inhaler in a characteristic model of the airways. Ann. Biomed. Eng. 2012, 40, 2596–2610. [Google Scholar] [CrossRef]
- Small, L.E.; Augsburger, L. Instrumentation of an automatic capsule-filling machine. J. Pharm. Sci. 1977, 66, 504–509. [Google Scholar] [CrossRef]
- Tan, S.; Newton, J. Powder flowability as an indication of capsule filling performance. Int. J. Pharm. 1990, 61, 145–155. [Google Scholar] [CrossRef]
- Faulhammer, E.; Llusa, M.; Wahl, P.; Paudel, A.; Lawrence, S.; Biserni, S.; Calzolari, V.; Khinast, J. Development of a design space and predictive statistical model for capsule filling of low-fill-weight inhalation products. Drug Dev. Ind. Pharm. 2016, 42, 221–230. [Google Scholar] [CrossRef]
- Podczeck, F. The development of an instrumented tamp-filling capsule machine II: Investigations of plug development and tamping pressure at different filling stations. Eur. J. Pharm. Sci. 2001, 12, 515–521. [Google Scholar] [CrossRef]
- Bryant, S.; Gill, I.; Edwards, D.; Smith, I.J. Advances in powder-dosing technology. Innov. Pharm. Technol. 2002, 124, 95–100. [Google Scholar]
- Available online: https://www.capsugel.com/knowledge-center/xcelodose-s-powder-micro-dosing-system-brochure (accessed on 11 August 2019).
- Freeman, T.; Moolchandani, V.; Hoag, S.; Fu, X. Capsule filling performance of powdered formulations in relation to flow characteristics. In Particulate Materials; RSC Publishing: New York, NY, USA, 2011; pp. 131–136. [Google Scholar]
- Faulhammer, E.; Fink, M.; Llusa, M.; Lawrence, S.M.; Biserni, S.; Calzolari, V.; Khinast, J.G. Low-dose capsule filling of inhalation products: Critical material attributes and process parameters. Int. J. Pharm. 2014, 473, 617–626. [Google Scholar] [CrossRef] [PubMed]
- Stranzinger, S.; Faulhammer, E.; Calzolari, V.; Biserni, S.; Dreu, R.; Šibanc, R.; Paudel, A.; Khinast, J. The effect of material attributes and process parameters on the powder bed uniformity during a low-dose dosator capsule filling process. Int. J. Pharm. 2017, 516, 9–20. [Google Scholar] [CrossRef]
- Llusa, M.; Faulhammer, E.; Biserni, S.; Calzolari, V.; Lawrence, S.; Bresciani, M.; Khinast, J. The effect of capsule-filling machine vibrations on average fill weight. Int. J. Pharm. 2013, 454, 381–387. [Google Scholar] [CrossRef]
- Yazdi, A.K.; Smyth, H.D. Carrier-free high-dose dry powder inhaler formulation of ibuprofen: Physicochemical characterization and in vitro aerodynamic performance. Int. J. Pharm. 2016, 511, 403–414. [Google Scholar] [CrossRef] [PubMed]
- Fassihi, A.; Parker, M. Influence of gamma radiation on the gel rigidity index and binding capability of gelatin. J. Pharm. Sci. 1988, 77, 876–879. [Google Scholar] [CrossRef]
- Tochio, S.; Nagata, S.; Yamashita, S. The influence of the composition of test fluids on dissolution from HPMC capsules. AAPS PharmSci 2002, 4, W4340. [Google Scholar]
- Podczeck, F.; Jones, B.E. The in vitro dissolution of theophylline from different types of hard shell capsules. Drug Dev. Ind. Pharm. 2002, 28, 1163–1169. [Google Scholar] [CrossRef]
- Bell, J.; Stevenson, N.; Taylor, J. A moisture transfer effect in hard gelatin capsules of sodium cromoglycate. J. Pharm. Pharmacol. 1973, 25, 96. [Google Scholar]
- Missaghi, S.; Fassihi, R. Evaluation and comparison of physicomechanical characteristics of gelatin and hypromellose capsules. Drug Dev. Ind. Pharm. 2006, 32, 829–838. [Google Scholar] [CrossRef]
- Kontny, M.J.; Mulski, C.A. Gelatin capsule brittleness as a function of relative humidity at room temperature. Int. J. Pharm. 1989, 54, 79–85. [Google Scholar] [CrossRef]
- Geuns, E.R.; Toren, J.S.; Barends, D.M.; Bult, A. Decrease of the stage-2 deposition in the twin impinger during storage of beclomethasone dipropionate dry powder inhalers in controlled and uncontrolled humidities. Eur. J. Pharm. Biopharm. 1997, 44, 187–194. [Google Scholar] [CrossRef]
- Young, P.M.; Price, R. The influence of humidity on the aerosolisation of micronised and SEDS produced salbutamol sulphate. Eur. J. Pharm. Sci. 2004, 22, 235–240. [Google Scholar] [CrossRef]
- Price, R.; Young, P.; Edge, S.; Staniforth, J. The influence of relative humidity on particulate interactions in carrier-based dry powder inhaler formulations. Int. J. Pharm. 2002, 246, 47–59. [Google Scholar] [CrossRef]
- Das, S.; Larson, I.; Young, P.; Stewart, P. Influence of storage relative humidity on the dispersion of salmeterol xinafoate powders for inhalation. J. Pharm. Sci. 2009, 98, 1015–1027. [Google Scholar] [CrossRef]
- Nagata, S. Cellulosecapsules–Analternative To Gelatin. Biomed. Polym. Polym. Ther. 2001, 53, 53–62. [Google Scholar]







| Capsule-Based DPIs | Drug(s) Delivered | U.S. Marketed Product | Capsule Types | References |
|---|---|---|---|---|
| Aerohaler® | Ipratropium bromide | - | - | [8,11,12] |
| Aerohaler®/Cyclohaler® | Formoterol fumarate * | Foradil® Aerohaler® | Gelatin | [8,11,12,13,14,15] |
| Salbutamol sulfate | ||||
| Beclomethasone | ||||
| Dipropionate | ||||
| Ipratropium bromide | ||||
| Budesonide | ||||
| Formoterol | ||||
| Eclipse® | Sodium cromoglycate | - | - | [13,15] |
| FlowCaps® | N/A | - | HPMC | [13] |
| HandiHaler® | Tiotropium bromide | SPIRIVA® HandiHaler® | Gelatin | [8,11,12,13,15] |
| Inhalator™ | Fenoterol | - | - | [11,12,13] |
| Podhaler™ | Tobramycin | TOBI™ Podhaler™ | HPMC | [8,15] |
| Rotahaler®/DPIhaler® | Salbutamol sulfate | - | - | [8,11,12,13] |
| Beclomethasone | ||||
| Dipropionate | ||||
| RS01 | Mannitol | Aridol® | Gelatin | [16,17] |
| Spinhaler® | Sodium cromoglycate | Intal® Spincaps® † | Gelatin | [8,11,12,13,15,18,19] |
| Turbospin® | Colistimethate sodium | - | - | [8,15] |
| Neohaler® | Glycopyrrolate | Seebri™ Neohaler® | HPMC | [8,15] |
| Indacaterol | Arcapta® Neohaler® | Gelatin |
| Properties | Capsule Material | |
|---|---|---|
| Gelatin | HPMC | |
| Moisture content | 13–16% | Less than 9% |
| Moisture transfer | Hysteretic | Sensitive |
| Required puncture force | More | Less |
| Aperture shape after piercing | Irregular | Regular |
| Shedding of pieces after piercing | More | Less |
| Brittleness | More brittle | Less brittle |
| Generation of “flap” after piercing | More | Less |
| Capsule filling | Easy | Relatively hard |
| Powder retention after inhalation | High | Low |
| FPF after inhalation | High | Low |
| Capsule Shell Brand | Name Manufacturer | Registered Year in the U.S. | Gelling Aid |
|---|---|---|---|
| Quali-V | Shionogi Qualicaps | July 2002 | Carrageenan |
| Vcaps Plus | Capsugel (A division of Pfizer) | - | None |
| Vcaps | Capsugel (A division of Pfizer) | April 2003 | Gellan gum |
| VegiCaps | G S Technologies Inc. (now R.P. Scherer Technologies ownership) | May 1989 | None |
| Embo Caps -Vg | Suheung Capsule Co., Ltd. | - | Pectin and glycerin |
| Capstech’s HPMC Capsule | Baotou Capstech Co., Ltd. | - | None |
| Natural Plant Capsule | Zhejiang LinFeng Capsules Co. Ltd. | - | Carrageenan |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ding, L.; Brunaugh, A.D.; Stegemann, S.; Jermain, S.V.; Herpin, M.J.; Kalafat, J.; Smyth, H.D.C. A Quality by Design Framework for Capsule-Based Dry Powder Inhalers. Pharmaceutics 2021, 13, 1213. https://doi.org/10.3390/pharmaceutics13081213
Ding L, Brunaugh AD, Stegemann S, Jermain SV, Herpin MJ, Kalafat J, Smyth HDC. A Quality by Design Framework for Capsule-Based Dry Powder Inhalers. Pharmaceutics. 2021; 13(8):1213. https://doi.org/10.3390/pharmaceutics13081213
Chicago/Turabian StyleDing, Li, Ashlee D. Brunaugh, Sven Stegemann, Scott V. Jermain, Matthew J. Herpin, Justin Kalafat, and Hugh D. C. Smyth. 2021. "A Quality by Design Framework for Capsule-Based Dry Powder Inhalers" Pharmaceutics 13, no. 8: 1213. https://doi.org/10.3390/pharmaceutics13081213