
Development, Characterization and In Vivo Pharmacokinetic Assessment of Rectal Suppositories Containing Combination Antiretroviral Drugs for HIV Prevention

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Manufacture of Rectal Suppositories
2.2. Suppository Characterization
2.3. Humane Care Guidelines
2.4. In Vivo PK Following Rectal Suppository Dosing
2.5. Specimen Collections
2.6. Analysis of Drug Concentrations in Plasma, Rectal Fluids, and Rectal Biopsies Biological Matrices
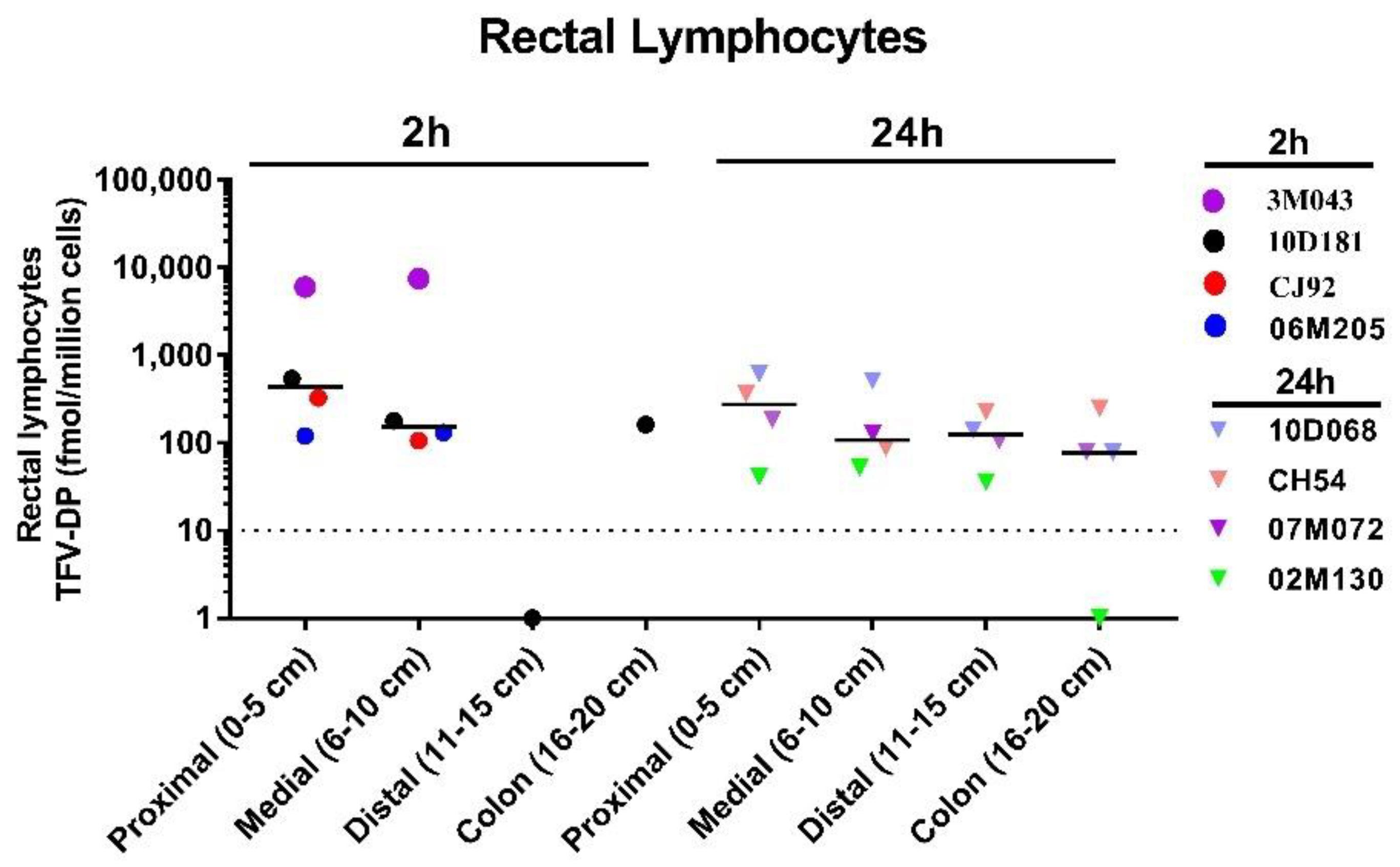
2.7. Analysis of Tenofovir Di-Phosphate (TFV-DP) Concentrations in Rectal Biopsies and Rectal Lymphocytes
2.8. Data and Statistical Analysis
3. Results
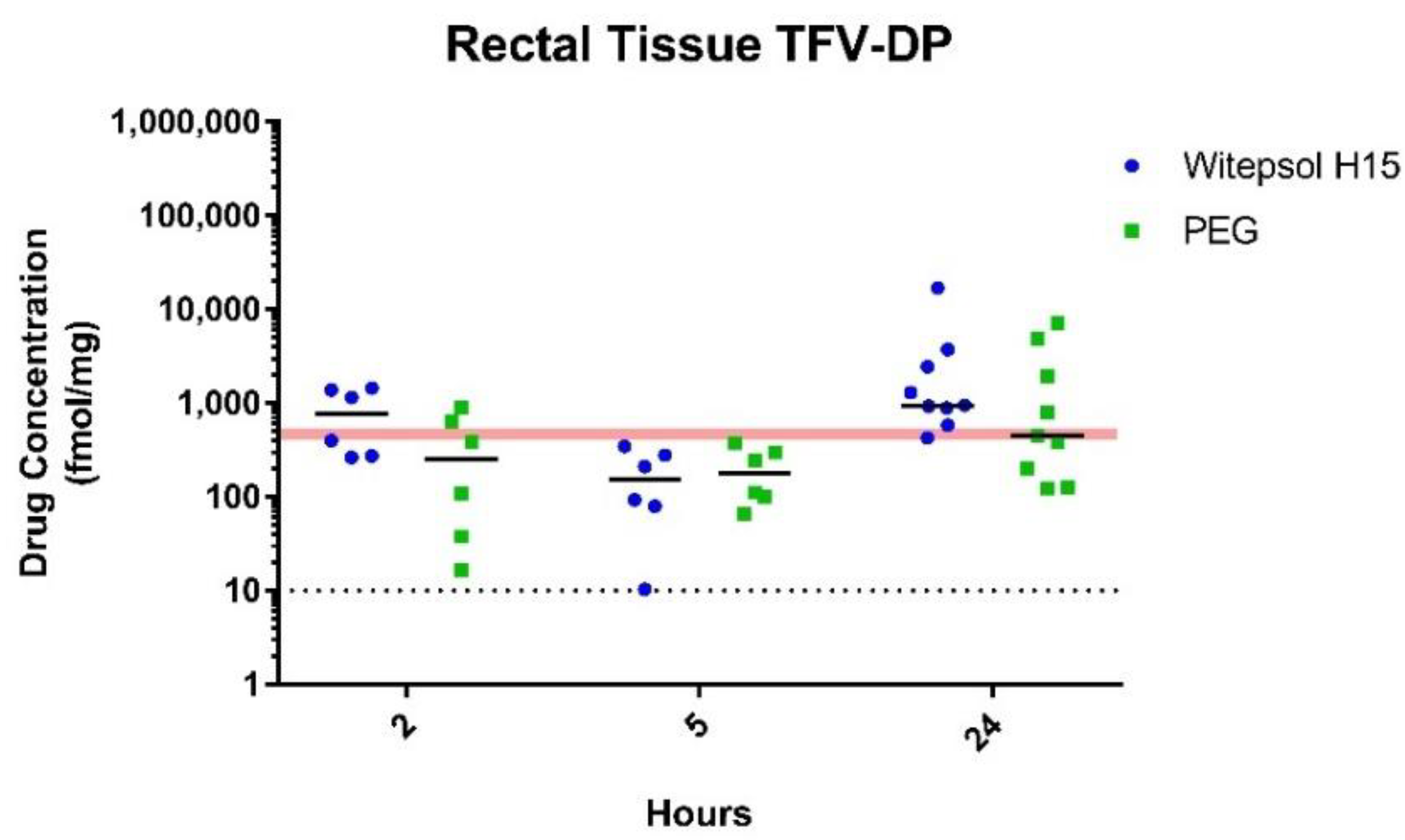
3.1. TFV/EVG (40/40 mg) Suppositories
3.1.1. In Vitro Characterization
3.1.2. In Vivo Pharmacokinetic Assessment
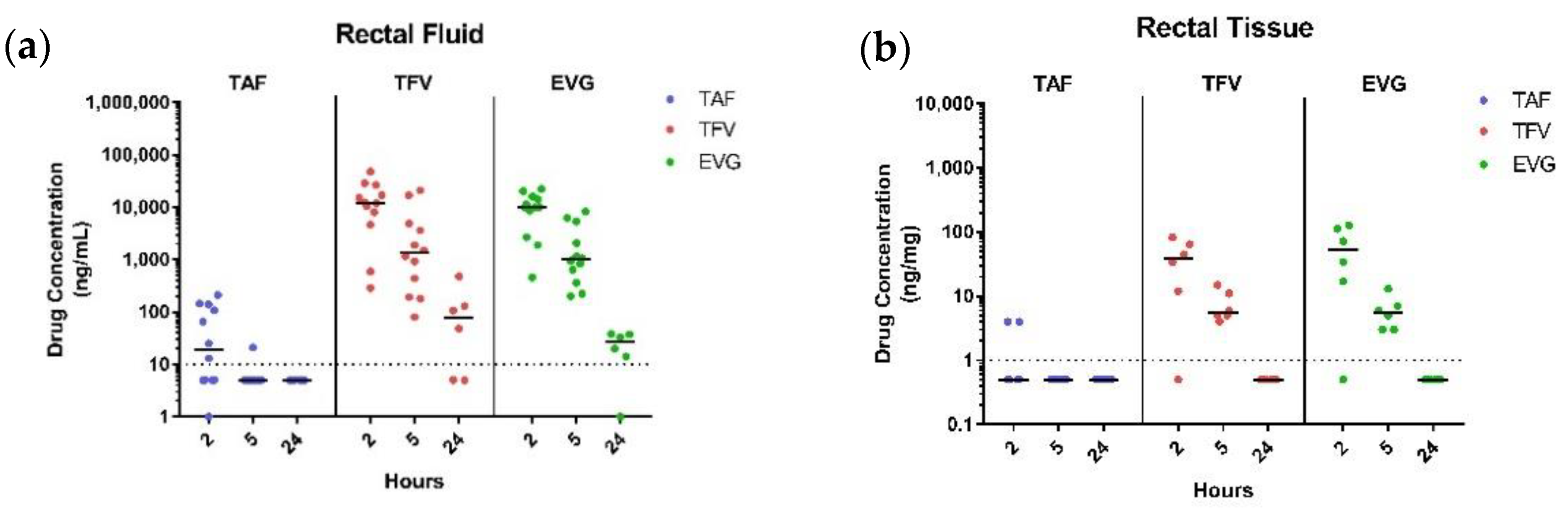
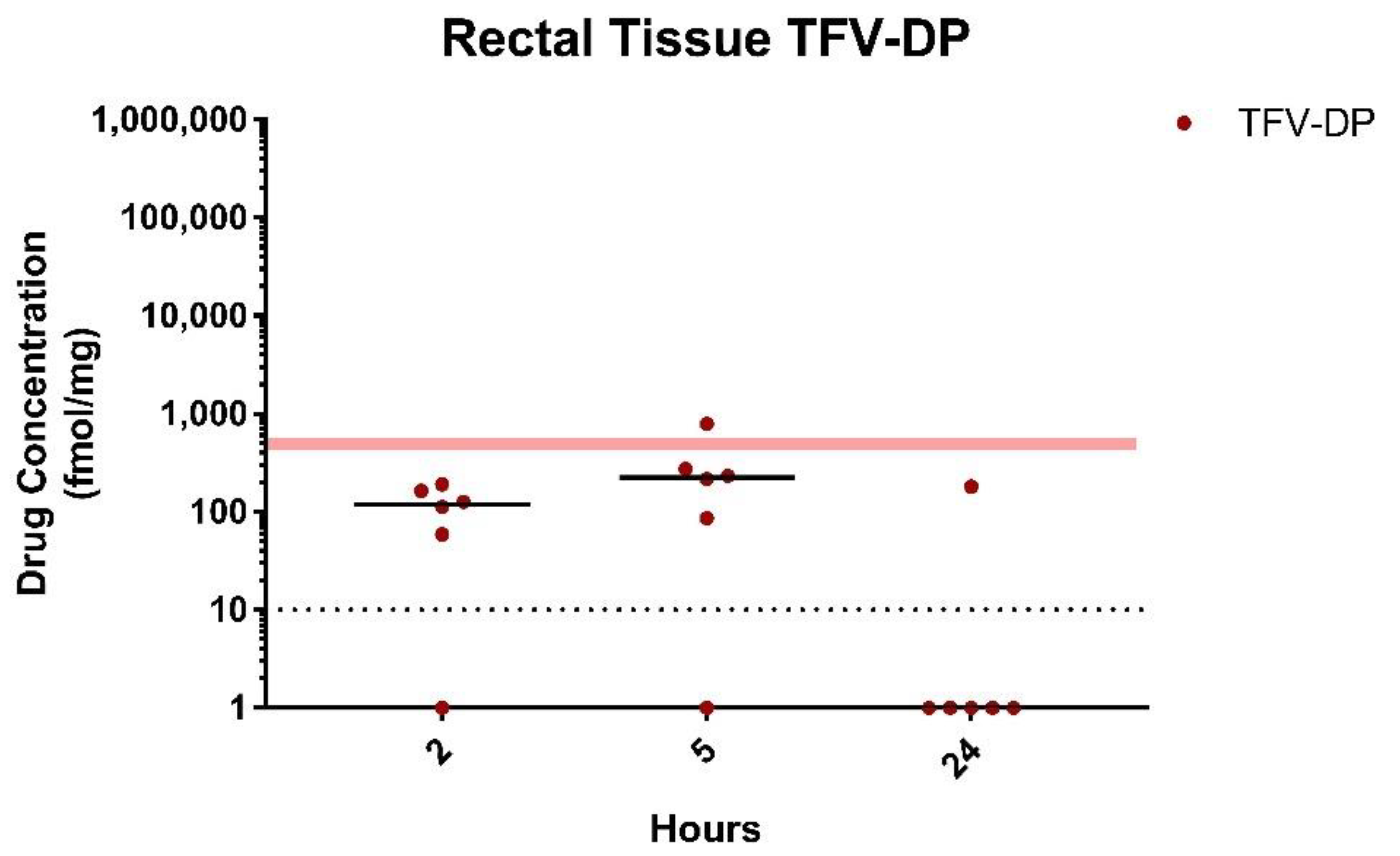
3.2. TAF/EVG (8 mg/8 mg) Suppositories
In Vivo Pharmacokinetic Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention. HIV Surveillance Report, 2018 (Updated), Volume 31. May 2020. Available online: http://www.cdc.gov/hiv/library/reports/hiv-surveillance.html (accessed on 19 April 2021).
- McGowan, I. Microbicides: A new frontier in HIV prevention. Biologicals 2006, 34, 241–255. [Google Scholar] [CrossRef]
- Cutler, B.; Justman, J. Vaginal microbicides and the prevention of HIV transmission. Lancet Infect. Dis. 2008, 8, 685–697. [Google Scholar] [CrossRef] [Green Version]
- Hussain, L.A.; Lehner, T. Comparative investigation of Langerhans’ cells and potential receptors for HIV in oral, genitourinary and rectal epithelia. Immunology 1995, 85, 475–484. [Google Scholar] [PubMed]
- McGowan, I.; Dezzutti, C. Rectal microbicide development. Curr. Top. Microbiol. Immunol. 2014, 383, 117–136. [Google Scholar]
- Rohan, L.C.; Moncla, B.J.; Na Ayudhya, R.P.K.; Cost, M.; Huang, Y.; Gai, F.; Billitto, N.; Lynam, J.D.; Pryke, K.; Graebing, P.; et al. In Vitro and Ex Vivo Testing of Tenofovir Shows it is Effective as an HIV-1 Microbicide. PLoS ONE 2010, 5, e9310. [Google Scholar] [CrossRef] [Green Version]
- Bauermeister, J.A.; Giguere, R.; Leu, C.S.; Dolezal, C.; Febo, I.; Cranston, R.D.; Mayer, K.; McGowan, I.; Carballo-Diéguez, A. Patterns of a Rectal Microbicide Placebo Gel Use in a Preparatory Stage for a Phase I Trial Among Young Men Who Have Sex with Men. AIDS Behav. 2018, 22, 412–420. [Google Scholar] [CrossRef] [PubMed]
- Chakrapani, V.; Newman, P.A.; Shunmugam, M.; Mengle, S.; Nelson, R.; Rubincam, C.; Kumar, P. “Like Holding an Umbrella before It Rains”: Acceptability of Future Rectal Microbicides among Men Who Have Sex with Men in India—A Modified Technology Acceptance Model. Qual. Health Res. 2017, 27, 1236–1248. [Google Scholar] [CrossRef]
- Frasca, T.; Giguere, R.; Ibitoye, M.; Dolezal, C.; Febo, I.; Cranston, R.D.; Mayer, K.; McGowan, I.; Carballo-Diéguez, A. Lessons for Rectal Microbicide Development from an Acceptability Trial of a Placebo Gel Applied Prior to Receptive Anal Intercourse. Arch. Sex. Behav. 2017, 46, 1101–1109. [Google Scholar] [CrossRef]
- Hambrick, H.R.; Park, S.H.; Goedel, W.C.; Morganstein, J.G.; Kreski, N.T.; Mgbako, O.; Duncan, D.T. Rectal Douching Among Men Who Have Sex with Men in Paris: Implications for HIV/STI Risk Behaviors and Rectal Microbicide Development. AIDS Behav. 2018, 22, 379–387. [Google Scholar] [CrossRef]
- Cranage, M.; Sharpe, S.; Herrera, C.; Cope, A.; Dennis, M.; Berry, N.; Ham, C.; Heeney, J.; Rezk, N.; Kashuba, A.; et al. Prevention of SIV rectal transmission and priming of T cell responses in macaques after local pre-exposure application of tenofovir gel. PLoS Med. 2008, 5, e157. [Google Scholar] [CrossRef] [PubMed]
- Dobard, C.W.; Taylor, A.; Sharma, S.; Anderson, P.L.; Bushman, L.R.; Chuong, D.; Pau, C.-P.; Hanson, D.; Wang, L.; Garcia-Lerma, J.G.; et al. Protection Against Rectal Chimeric Simian/Human Immunodeficiency Virus Transmission in Macaques by Rectal-Specific Gel Formulations of Maraviroc and Tenofovir. J. Infect. Dis. 2015, 212, 1988–1995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jhunjhunwala, K. Design and Evaluation of a Topical Rectal Specific Microbicide for HIV Prevention. Ph.D. Thesis, University of Pittsburgh, Pittsburgh, PA, USA, 2015. [Google Scholar]
- Gugulothu, D.; Pathak, S.; Suryavanshi, S.; Sharma, S.; Patravale, V. Self-microemulsifiyng suppository formulation of beta-artemether. AAPS PharmSciTech 2010, 11, 1179–1184. [Google Scholar] [CrossRef] [Green Version]
- Fong, T.L.; Lee, B.T.; Tien, A.; Chang, M.; Lim, C.; Ahn, A.; Bae, H.S. Improvement of bone mineral density and markers of proximal renal tubular function in chronic hepatitis B patients switched from tenofovir disoproxil fumarate to tenofovir alafenamide. J. Viral Hepat. 2019, 26, 561–567. [Google Scholar] [CrossRef]
- Gupta, S.K.; Post, F.A.; Arribas, J.R.; Eron, J.J., Jr.; Wohl, D.A.; Clarke, A.E.; Sax, P.E.; Stellbrink, H.J.; Esser, S.; Pozniak, A.L.; et al. Renal safety of tenofovir alafenamide vs tenofovir disoproxil fumarate: A pooled analysis of 26 clinical trials. AIDS 2019, 33, 1455. [Google Scholar] [CrossRef] [PubMed]
- Hamzah, L.; Jones, R.; Post, F.A. Optimizing antiretroviral regimens in chronic kidney disease. Curr. Opin. Infect. Dis. 2019, 32, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Imaz, A.; Niubó, J.; Cottrell, M.L.; Perez, E.; Kashuba, A.D.M.; Tiraboschi, J.M.; Morenilla, S.; Garcia, B.; Podzamczer, D. Seminal Tenofovir Concentrations, Viral Suppression, and Semen Quality with Tenofovir Alafenamide Compared with Tenofovir Disoproxil Fumarate (Spanish HIV/AIDS Research Network, PreEC/RIS 40). Clin. Infect. Dis. 2018, 69, 1403–1409. [Google Scholar] [CrossRef] [PubMed]
- Kaneko, S.; Kurosaki, M.; Tamaki, N.; Itakura, J.; Hayashi, T.; Kirino, S.; Osawa, L.; Watakabe, K.; Okada, M.; Wang, W.; et al. Tenofovir alafenamide for hepatitis B virus infection including switching therapy from tenofovir disoproxil fumarate. J. Gastroenterol. Hepatol. 2019, 34, 2004–2010. [Google Scholar] [CrossRef] [PubMed]
- Mills, A.; Arribas, J.R.; Andrade-Villanueva, J.; DiPerri, G.; Van Lunzen, J.; Koenig, E.; Elion, R.; Cavassini, M.; Madruga, J.V.; Brunetta, J.; et al. Switching from tenofovir disoproxil fumarate to tenofovir alafenamide in antiretroviral regimens for virologically suppressed adults with HIV-1 infection: A randomised, active-controlled, multicentre, open-label, phase 3, non-inferiority study. Lancet Infect. Dis. 2016, 16, 43–52. [Google Scholar] [CrossRef]
- Mothobi, N.Z.; Masters, J.; Marriott, D.J. Fanconi syndrome due to tenofovir disoproxil fumarate reversed by switching to tenofovir alafenamide fumarate in an HIV-infected patient. Ther. Adv. Infect. Dis. 2018, 5, 91–95. [Google Scholar] [CrossRef]
- Ray, A.S.; Fordyce, M.W.; Hitchcock, M.J. Tenofovir alafenamide: A novel prodrug of tenofovir for the treatment of Human Immunodeficiency Virus. Antiviral. Res. 2016, 125, 63–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruane, P.J.; DeJesus, E.; Berger, D.; Markowitz, M.; Bredeek, U.F.; Callebaut, C.; Zhong, L.; Ramanathan, S.; Rhee, M.S.; Fordyce, M.W.; et al. Antiviral activity, safety, and pharmacokinetics/pharmacodynamics of tenofovir alafenamide as 10-day monotherapy in HIV-1—Positive adults. J. Acquir. Immune Defic. Syndr. 2013, 63, 449–455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubin, M.R.; Bilezikian, J.P.; McMahon, D.J.; Jacobs, T.; Shane, E.; Siris, E.; Udesky, J.; Silverberg, S.J. The natural history of primary hyperparathyroidism with or without parathyroid surgery after 15 years. J. Clin. Endocrinol. Metab. 2008, 93, 3462–3470. [Google Scholar] [CrossRef]
- Sax, P.E.; Zolopa, A.; Brar, I.; Elion, R.; Ortiz, R.; Post, F.; Wang, H.; Callebaut, C.; Martin, H.; Fordyce, M.; et al. Tenofovir alafenamide vs. tenofovir disoproxil fumarate in single tablet regimens for initial HIV-1 therapy: A randomized phase 2 study. J. Acquir. Immune. Defic. Syndr. 2014, 67, 52–58. [Google Scholar] [CrossRef] [Green Version]
- Van Welzen, B.J.; Thielen, M.A.; Mudrikova, T.; Arends, J.E.; Hoepelman, A.I. Switching tenofovir disoproxil fumarate to tenofovir alafenamide results in a significant decline in parathyroid hormone levels: Uncovering the mechanism of tenofovir disoproxil fumarate-related bone loss? Aids 2019, 33, 1531–1534. [Google Scholar] [CrossRef] [PubMed]
- Sax, P.E.; Wohl, D.; Yin, M.T.; Post, F.; DeJesus, E.; Saag, M.; Pozniak, A.; Thompson, M.; Podzamczer, D.; Molina, J.M.; et al. Tenofovir alafenamide versus tenofovir disoproxil fumarate, coformulated with elvitegravir, cobicistat, and emtricitabine, for initial treatment of HIV-1 infection: Two randomised, double-blind, phase 3, non-inferiority trials. Lancet 2015, 385, 2606–2615. [Google Scholar] [CrossRef]
- Dobard, C.; Peet, M.M.; Nishiura, K.; Singh, O.N.; McCormick, T.J.; Mitchell, J.; Garcia-Lerma, G.; Agrahari, V.; Gupta, P.; Jonnalagadda, S.; et al. Protection against vaginal SHIV infection with an insert containing TAF and EVG. Presented at the Conference on Retroviruses and Opportunistic Infections, Seattle, WA, USA, 4–9 March 2019. Abstract Number 101. [Google Scholar]
- Dobard, C.; Sharma, S.; Parikh, U.M.; West, R.; Taylor, A.; Martin, A.; Pau, C.-P.; Hanson, D.L.; Lipscomb, J.; Smith, J.; et al. Postexposure protection of macaques from vaginal SHIV infection by topical integrase inhibitors. Sci. Transl. Med. 2014, 6, 227ra35. [Google Scholar] [CrossRef]
- Dobard, C.; Peet, M.M.; Nishiura, K.; Holder, A.; Singh, O.N.; McCormick, T.J.; Mitchell, J.; Khalil, G.; Garcίa-Lerma, G.; Agrahari, V.; et al. On-Demand Pre- and Post-Exposure Prophylaxis by Vaginal Inserts Containing TAF and EVG in Macaques. Presented at the Conference on Retroviruses and Opportunistic Infections, Boston, MA, USA, 8–11 March 2020. Abstract Number 88. [Google Scholar]
- Makarova, M.; Singletary, T.; Peet, M.M.; Mitchell, J.; Holder, A.; Dinh, C.; Heneine, W.; Garcia-Lerma, G.; Clark, M.; Smith, J.; et al. Pharmacokinetics of TAF/EVG rectal inserts in macaques and impact of rectal wash. Presented at the Conference on Retroviruses and Opportunistic Infections, Virtually, Atlanta, GA, USA, 6–10 March 2021. Abstract Number 715. [Google Scholar]
- Janet, C.G.; Wayne, B.R.; Joseph, T.B.; Leigh, A.C.; John, C.D.; Dennis, F.K.; Neil, S.L.; Paul, A.L.; John, M.; Fred, W.Q.; et al. Guide for the Care and Use of Laboratory Animals, 8th ed.; The National Academies Press: Washington, DC, USA, 2011. [Google Scholar]
- Massud, I.; Mitchell, J.; Babusis, D.; Deyounks, F.; Ray, A.S.; Rooney, J.F.; Heneine, W.; Miller, M.D.; García-Lerma, J.G. Chemoprophylaxis with Oral Emtricitabine and Tenofovir Alafenamide Combination Protects Macaques from Rectal Simian/Human Immunodeficiency Virus Infection. J. Infect. Dis. 2016, 214, 1058–1062. [Google Scholar] [CrossRef] [Green Version]
- Kuklenyik, Z.; Martin, A.; Pau, C.-P.; Garcia-Lerma, J.G.; Heneine, W.; Pirkle, J.L.; Barr, J.R. Effect of mobile phase pH and organic content on LC-MS analysis of nucleoside and nucleotide HIV reverse transcriptase inhibitors. J. Chromatogr. Sci. 2009, 47, 365–372. [Google Scholar] [CrossRef] [Green Version]
- Anton, P.A.; Cranston, R.D.; Kashuba, A.; Hendrix, C.W.; Bumpus, N.N.; Richardson-Harman, N.; Elliott, J.; Janocko, L.; Khanukhova, E.; Dennis, R.; et al. RMP-02/MTN-006: A phase 1 rectal safety, acceptability, pharmacokinetic, and pharmacodynamic study of tenofovir 1% gel compared with oral tenofovir disoproxil fumarate. AIDS Res. Hum. Retrovir. 2012, 28, 1412–1421. [Google Scholar] [CrossRef] [Green Version]
- Nuttall, J.; Kashuba, A.; Wang, R.; White, N.; Allen, P.; Roberts, J.; Romano, J. Pharmacokinetics of tenofovir following intravaginal and intrarectal administration of tenofovir gel to rhesus macaques. Antimicrob. Agents Chemother. 2012, 56, 103–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neogi, U.; Singh, K.; Aralaguppe, S.P.G.; Rogers, L.C.; Njenda, D.T.; Sarafianos, S.G.; Hejdeman, B.; Sönnerborg, A. Ex-vivo antiretroviral potency of newer integrase strand transfer inhibitors cabotegravir and bictegravir in HIV type 1 non-B subtypes. AIDS 2018, 32, 469–476. [Google Scholar] [CrossRef] [PubMed]
- Xiao, P.; Gumber, S.; Marzinke, M.A.; Date, A.; Hoang, T.; Hanes, J.; Ensign, L.M.; Wang, L.; Rohan, L.; Fuchs, E.J.; et al. Hypo-osmolar Formulation of Tenofovir (TFV) Enema Promotes Uptake and Metabolism of TFV in Tissues, Leading to Prevention of SHIV/SIV Infection. Antimicrob. Agents Chemother. 2018, 62, e01644-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bauermeister, J.A.; Tingler, R.; Liu, A.; Chariyalertsak, S.; Hoesley, G.; Gonzales, P.; Ho, K.; Kayange, N.; Palanee-Phillips, T.; Johnson, S.; et al. Acceptability and Choice for 3 Placebo Products Used with Receptive Anal Sex. Presented at the Conference on Retroviruses and Opportunistic Infections, Virtually, Philadelphia, PA, USA, 6–10 March 2021. Abstract Number 716. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Suppository Bases | Weight (g) (avg ± SD) n = 3 | Hardness (kgs) (avg ± SD) n = 4 | Disintegration (min) Time Ranges * | Thermal Transition Using DSC (°C) n = 2 |
|---|---|---|---|---|
| Suppocire A | 1.18 ± 0.01 | 2.83 ± 0.28 | 7–8 | 37.79 |
| Witepsol H15 | 1.22 ± 0.01 | 5.08 ± 0.98 | 6–8 | 34.77 |
| Cocoa Butter | 1.18 ± 0.01 | 0.38 ± 0.29 | 3–4 | 32.97 |
| PEG 8000/400 (60:40) | 1.48 ± 0.01 | 2.57 ±0.21 | 12–15 | 56.39 |
| PEG 3350/1000 (25:75) | 1.50 ± 0.01 | 2.05 ± 0.20 | 8–9 | 37.86 |
| PEG 3350/1000/400 (60:30:10) | 1.49 ± 0.01 | 1.31 ± 0.14 | 7–8 | 55.08 |
| Tenofovir | Elvitegravir | |||||
|---|---|---|---|---|---|---|
| PK Parameter | Cmax, Median (range) | Tmax | AUC0–24 | Cmax, Median (range) | Tmax | AUC0–24 |
| Plasma | (ng/mL) | (h) | (ng × h/mL) | (ng/mL) | (h) | (ng × h/mL) |
| PEG | 24.5 (14–106.0) | 0.5 | 29.7 | BLOQ (BLOQ–15) | - | 5.6 |
| Witepsol | BLOQ (BLOQ–22.0) | 0.5 | 27.8 | BLOQ (BLOQ–8.0) | - | 5.1 |
| Rectal Fluid | (µg/mL) | (h) | (µg × h/mL) | (µg/mL) | (h) | (µg × h/mL) |
| PEG | 13.4 (0.63–71.2) | 2 | 26.4 | 17.3 (1.6–37.0) | 2 | 15 |
| Witepsol | 16.3 (14.4–24.4) | 2 | 12.2 | 24.6 (15.1–27.5) | 2 | 15.6 |
| Biopsy | (ng/mg) | (h) | (ng × h/mg) | (ng/mg) | (h) | (ng × h/mg) |
| PEG | 109.1 (BLOQ–945.6) | 2 | 124 | 45.5 (BLOQ–253.1) | 2 | 42.3 |
| Witepsol | 42.6 (26.5–253.1) | 2 | 107.1 | 15.6 (9.2–184.4) | 2 | 58.7 |
| Rectal Fluid | Tissue (Biopsy) | |||||
|---|---|---|---|---|---|---|
| Variable | Cmax, µg/mL, Median (Range) | Tmax, h | AUC0–24, µg × h/mL | Cmax, ng/mg, Median [Range] | Tmax, h | AUC0–24, ng × h/mL |
| TAF (8 mg) | ||||||
| PEG suppository | 0.019 (BLOQ–0.210) | 2 | 0.03 | BLOQ (BLOQ–4.0) | 2 | 0.67 |
| TFV (from TAF) | ||||||
| PEG suppository | 12.2 (0.284–48.1) | 2 | 12.1 | 39.5 (BLOQ–82.0) | 2 | 13.9 |
| EVG (8 mg) | ||||||
| PEG suppository | 9.99 (0.457–22.4) | 2 | 7.6 | 53.0 (BLOQ–127.0) | 2 | 36.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jhunjhunwala, K.; Dobard, C.W.; Sharma, S.; Makarova, N.; Holder, A.; Dinh, C.; Mitchell, J.; Wang, L.; Zhang, J.; Patel, S.K.; et al. Development, Characterization and In Vivo Pharmacokinetic Assessment of Rectal Suppositories Containing Combination Antiretroviral Drugs for HIV Prevention. Pharmaceutics 2021, 13, 1110. https://doi.org/10.3390/pharmaceutics13081110
Jhunjhunwala K, Dobard CW, Sharma S, Makarova N, Holder A, Dinh C, Mitchell J, Wang L, Zhang J, Patel SK, et al. Development, Characterization and In Vivo Pharmacokinetic Assessment of Rectal Suppositories Containing Combination Antiretroviral Drugs for HIV Prevention. Pharmaceutics. 2021; 13(8):1110. https://doi.org/10.3390/pharmaceutics13081110
Chicago/Turabian StyleJhunjhunwala, Kunal, Charles W. Dobard, Sunita Sharma, Natalia Makarova, Angela Holder, Chuong Dinh, James Mitchell, Lin Wang, Junmei Zhang, Sravan Kumar Patel, and et al. 2021. "Development, Characterization and In Vivo Pharmacokinetic Assessment of Rectal Suppositories Containing Combination Antiretroviral Drugs for HIV Prevention" Pharmaceutics 13, no. 8: 1110. https://doi.org/10.3390/pharmaceutics13081110