
Addition of Regular Insulin to Ternary Parenteral Nutrition: A Stability Study

 , , ,
, , ,
Abstracts
1. Introduction
2. Materials and Methods
2.1. Products
2.2. Sample Quantification Method: Preparation, Instrumentation and Kit
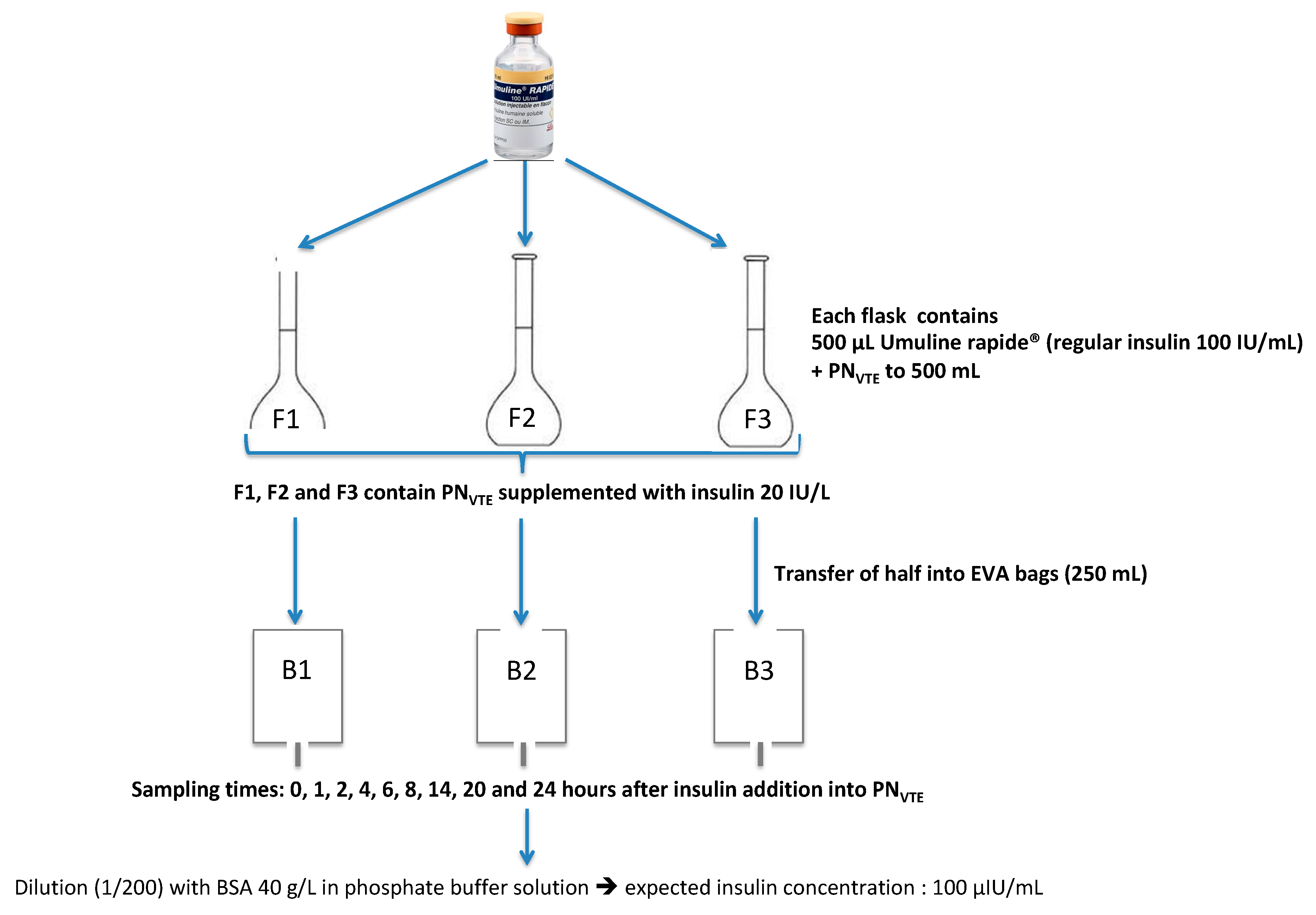
2.3. Preparation of PN Admixtures Containing Insulin
2.4. Study of Parameters Able to Influence Insulin Stability
2.4.1. Interaction between Content and Container: Preconditioning and Conditioning Assays
Preconditioning Assay
Conditioning Assay
2.4.2. Influence of Micro- or Macronutrient Content and pH
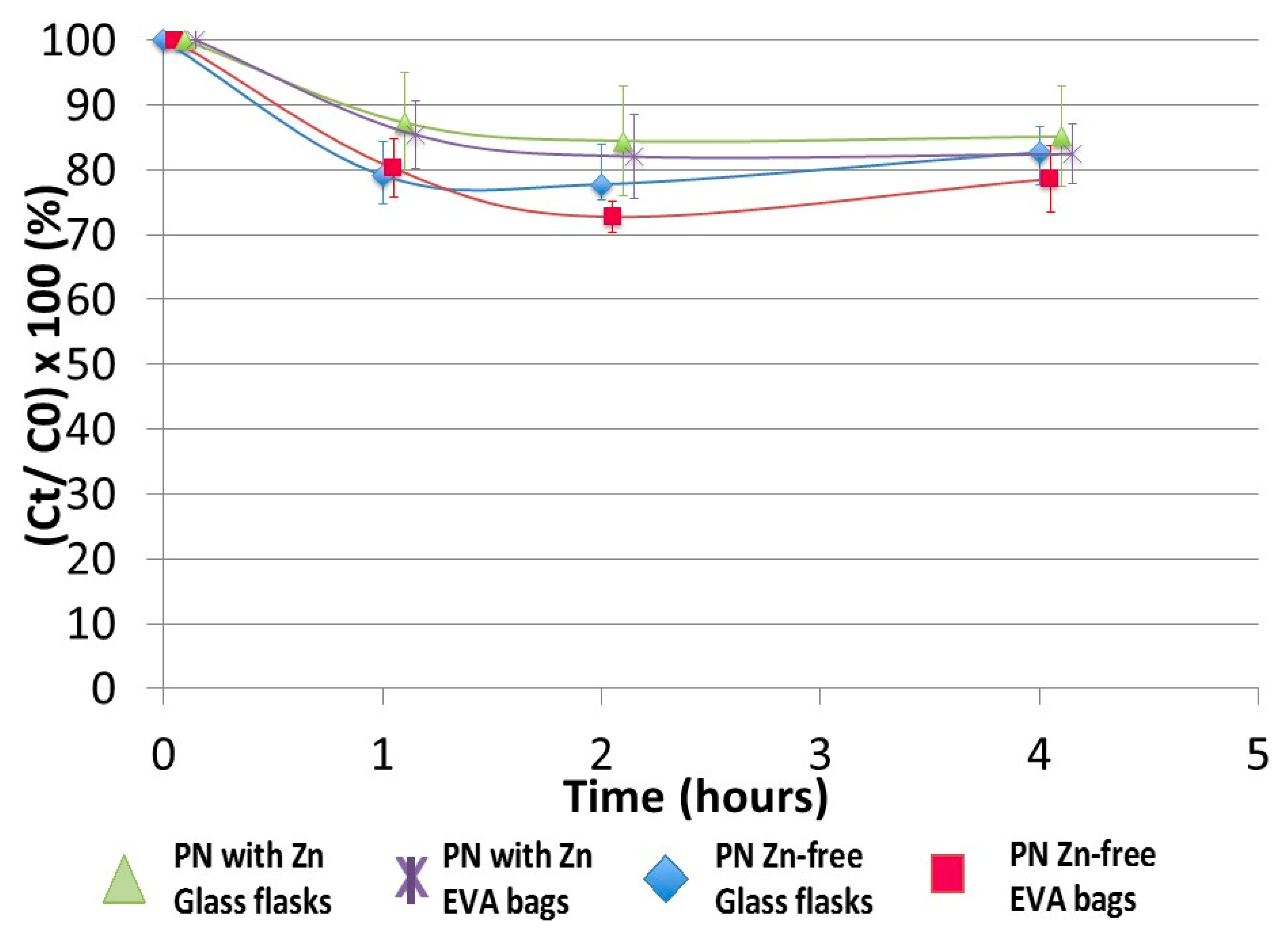
Influence of Zinc (Micronutrient)
Impact of the PN Medium (Macronutrient Content)
Impact of pH
2.5. Data Expression and Statistical Analysis
3. Results
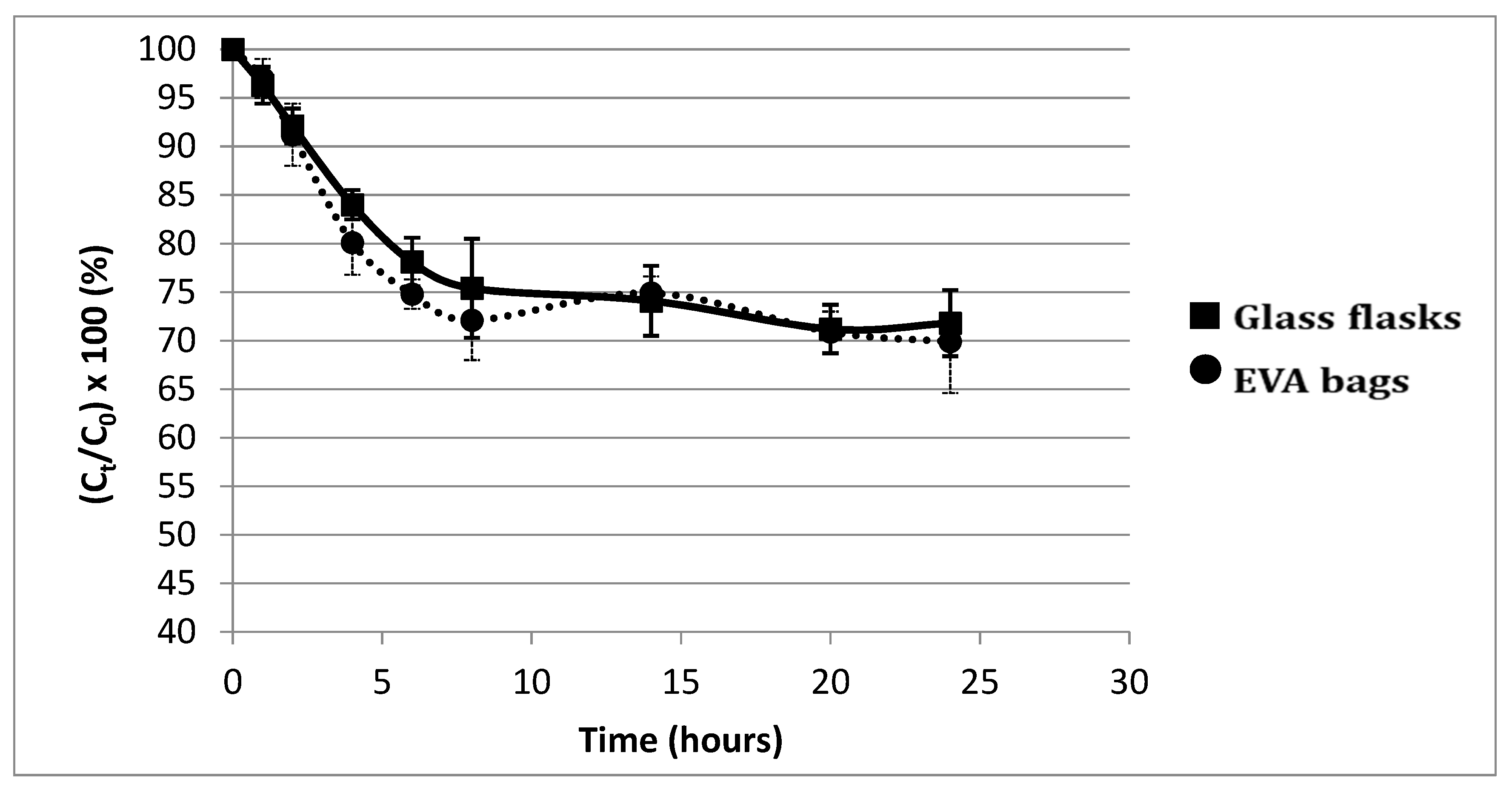
3.1. Study of Insulin Stability Depending on Conditions
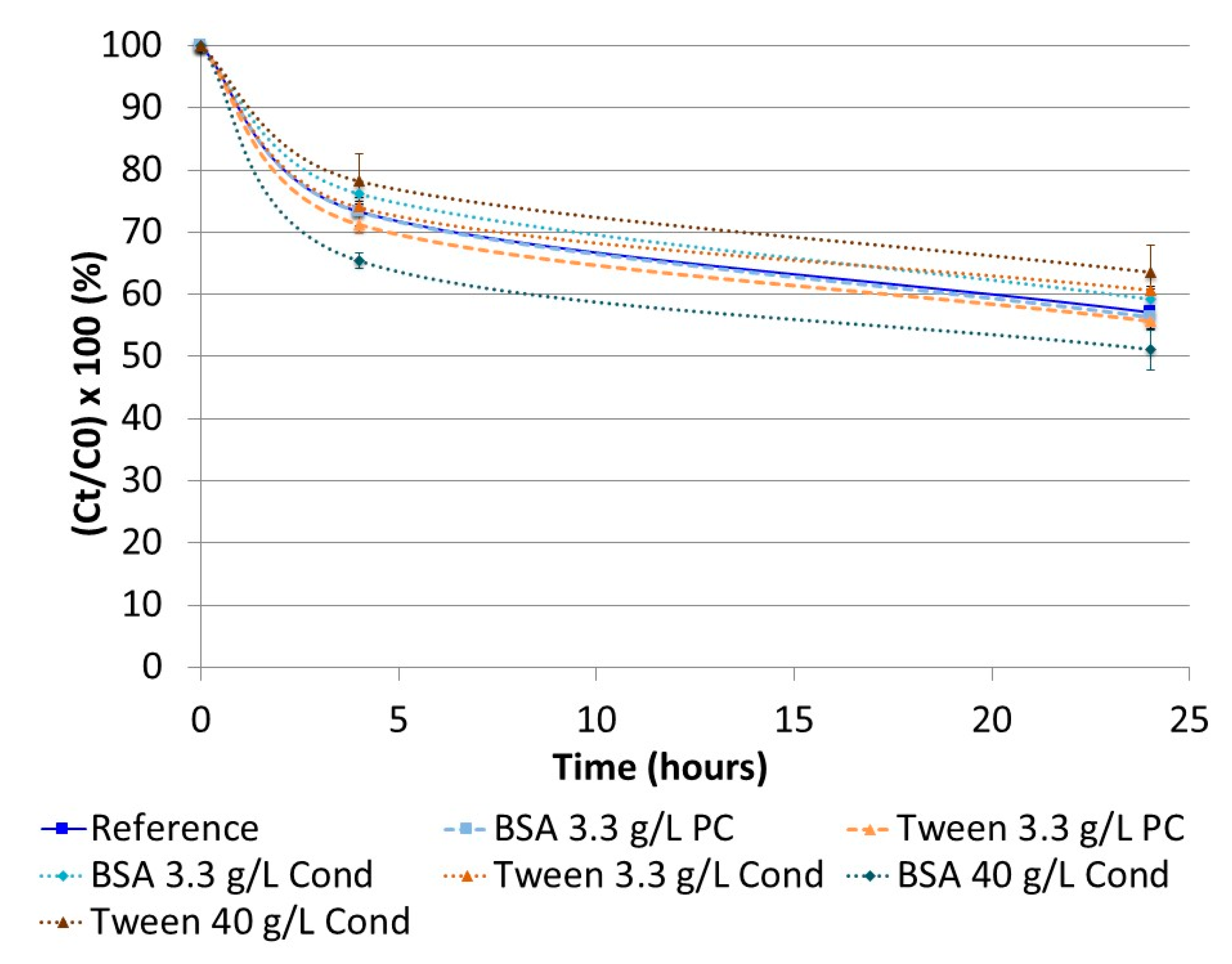
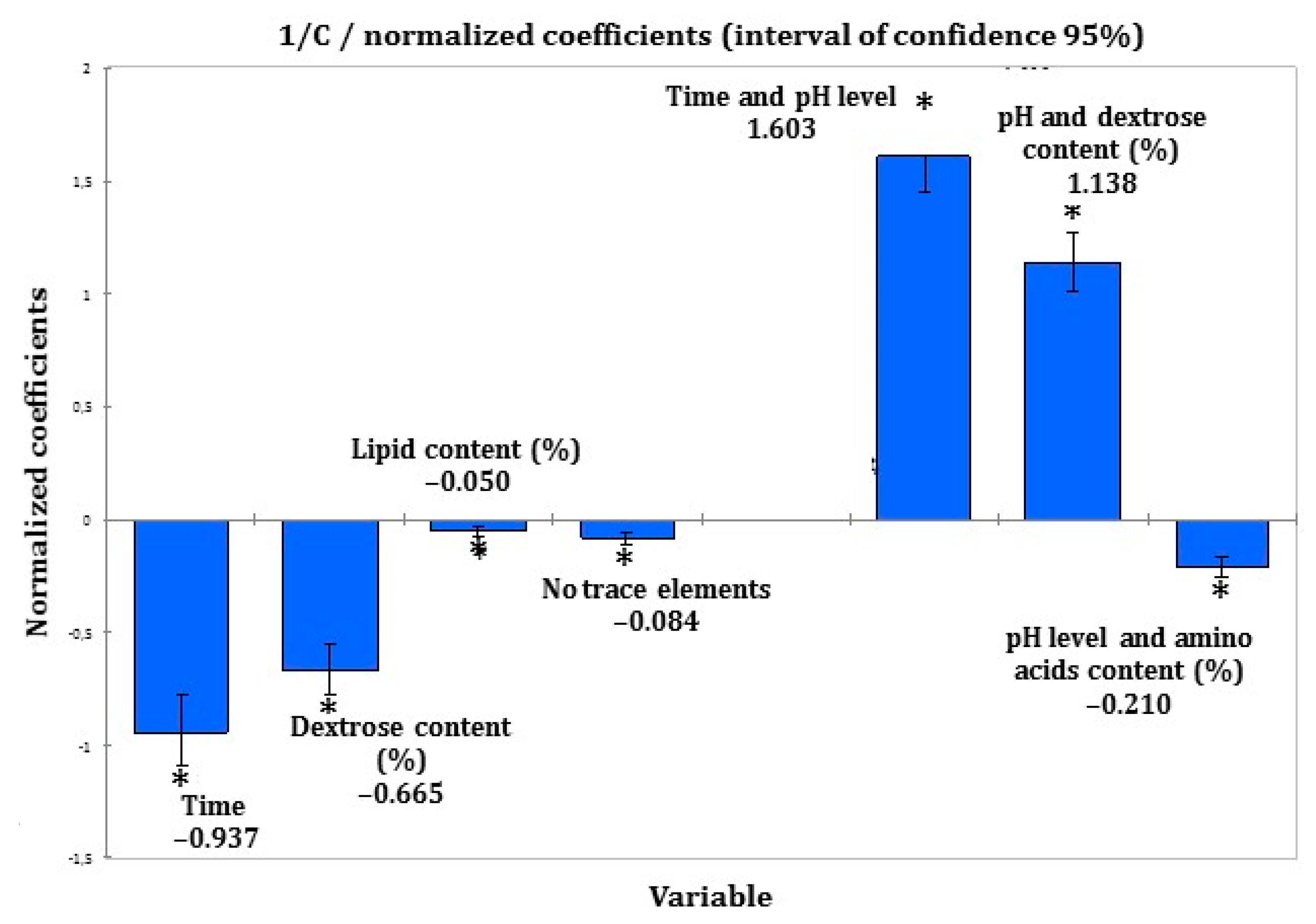
3.2. Identification of Parameters Able to Influence Insulin Stability
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pleva, M.; Mirtallo, J.M.; Steinberg, S.M. Hyperglycemic events in non-intensive care unit patients receiving parenteral nutrition. Nutr. Clin. Pract. 2009, 24, 626–634. [Google Scholar] [CrossRef] [PubMed]
- Sarkisian, S.; Fenton, T.R.; Shaheen, A.A.; Raman, M. Parenteral nutrition-associated hyperglycemia in noncritically ill inpatients is associated with higher mortality. Can. J. Gastroenterol. J. Can. Gastroenterol. 2010, 24, 453–457. [Google Scholar] [CrossRef] [PubMed]
- Pasquel, F.J.; Spiegelman, R.; McCauley, M.; Smiley, D.; Umpierrez, D.; Johnson, R.; Rhee, M.; Gatcliffe, C.; Lin, E.; Umpierrez, E.; et al. Hyperglycemia during total parenteral nutrition: An important marker of poor outcome and mortality in hospitalized patients. Diabetes Care 2010, 33, 739–741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, P.R.; Crotty, P.; Raman, M. Hyperglycemia in Hospitalized Patients Receiving Parental Nutrition Is Associated with Increased Morbidity and Mortality: A Review. Gastroenterol. Res. Pract. 2010, 2011, e760720. [Google Scholar] [CrossRef] [PubMed]
- Vennard, K.C.; Selen, D.J.; Gilbert, M.P. The Management of Hyperglycemia in Noncritically ill Hospitalized Patients Treated with Continuous Enteral or Parenteral Nutrition. Endocr. Pr. 2018, 24, 900–906. [Google Scholar] [CrossRef] [PubMed]
- Ayers, P.; Ms, R.S.A.; Boullata, J.; Gervasio, J.; Holcombe, B.; Kraft, M.D.; Marshall, N.; Neal, A.; Sacks, G.; Seres, D.S.; et al. A.S.P.E.N. Parenteral Nutrition Safety Consensus Recommendations. J. Parenter. Enter. Nutr. 2014, 38, 296–333. [Google Scholar] [CrossRef] [Green Version]
- Pironi, L.; Boeykens, K.; Bozzetti, F.; Joly, F.; Klek, S.; Lal, S.; Lichota, M.; Mühlebach, S.; Van Gossum, A.; Wanten, G.; et al. ESPEN guideline on home parenteral nutrition. Clin. Nutr. 2020, 39, 1645–1666. [Google Scholar] [CrossRef] [PubMed]
- Cardona, D.; Nadal, M.; Estelrich, J.; Mangues, M.A. Review of drug stability in parenteral nutrition admixtures. e-SPEN J. 2013, 8, e135–e140. [Google Scholar] [CrossRef]
- Bassons, T.; Maria-Sanchez, J.; Bassas, L.; Cardona, D.; Ordonez, J.; Bonal, J. Insulina recuperada según los componentes de la nutrición parenteral. Rev. SENPE 1985, 4, 93–99. [Google Scholar]
- Trissel, L.A.; Gilbert, D.L.; Martinez, J.F.; Baker, M.B.; Walter, W.V.; Mirtallo, J.M. Compatibility of Medications With 3-in-1 Parenteral Nutrition Admixtures. J. Parenter. Enter. Nutr. 1999, 23, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Marcuard, S.P.; Dunham, B.; Hobbs, A.; Caro, J.F. Availability of Insulin from Total Parenteral Nutrition Solutions. J. Parenter. Enter. Nutr. 1990, 14, 262–264. [Google Scholar] [CrossRef] [PubMed]
- Rušavý, Z.; Sramek, V.; Sucha, R.; Lacigova, S.; Topolcan, O. Effects of Carrier Solution on Insulin Bioavailability. J. Parenter. Enter. Nutr. 2004, 28, 439–441. [Google Scholar] [CrossRef]
- Brange, J.; Langkjaer, L. Chemical stability of insulin. 3. Influence of excipients, formulation, and pH. Acta Pharm. Nord. 1992, 4, 149–158. [Google Scholar] [PubMed]
- Petty, C.; Cunningham, N.L. Insulin adsorption by glass infusion bottles, polyvinylchloride infusion containers, and intravenous tubing. Anesthesiology 1974, 40, 400–404. [Google Scholar] [CrossRef]
- Henry, H.; Lannoy, D.; Simon, N.; Seguy, D.; D’Herbomez, M.; Barthélémy, C.; Décaudin, B.; Dine, T.; Odou, P. Immunoassay quantification of human insulin added to ternary parenteral nutrition containers: Comparison of two methods. Anal. Bioanal. Chem. 2017, 409, 3677–3684. [Google Scholar] [CrossRef]
- Levy-Marchal, C.; Bridel, M.-P.; Sodoyez-Goffaux, F.; Koch, M.; Tichet, J.; Czernichow, P.; Sodoyez, J.-C. Superiority of Radiobinding Assay Over ELISA for Detection of IAAs in Newly Diagnosed Type I Diabetic Children. Diabetes Care 1991, 14, 61–63. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, J.I.; Wood, J.H.; Thomas, R.B. Insulin adsorption to polyolefin infusion bottles and polyvinyl chloride administration sets. Am. J. Health Pharm. 1981, 38, 995–997. [Google Scholar] [CrossRef]
- Hewson, M.P.; Nawadra, V.; Oliver, J.R.; Odgers, C.; Plummer, J.L.; Simmer, K. Insulin infusions in the neonatal unit: Delivery variation due to adsorption. J. Paediatr. Child Health 2000, 36, 216–220. [Google Scholar] [CrossRef] [PubMed]
- Weber, S.S.; Wood, W.A.; Jackson, E.A. Availability of Insulin from Parenteral Nutrient Solutions. Am. J. Health Pharm. 1977, 34, 353–357. [Google Scholar] [CrossRef]
- Seifi, A.; Mowla, A.; Vaziri, M.M.T.; Talei, A.R.; Namazy, M.R. Insulin adsorbance to polyvinylchloride (PVC) surfaces of fluid container and infusion-set. Middle East J. Anaesthesiol. 2004, 17, 81. [Google Scholar]
- Thompson, C.D.; Vital-Carona, J.; Faustino, E.V.S. The Effect of Tubing Dwell Time on Insulin Adsorption during Intravenous Insulin Infusions. Diabetes Technol. Ther. 2012, 14, 912–916. [Google Scholar] [CrossRef]
- Jakobsson, T.; Shulman, R.; Gill, H.; Taylor, K. The Impact of Insulin Adsorption onto the Infusion Sets in the Adult Intensive Care Unit. J. Diabetes Sci. Technol. 2009, 3, 213–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peterson, L.; Caldwell, J.; Hoffman, J. Insulin adsorbance to polyvinylchloride surfaces with implications for constant-infusion therapy. Diabetes 1976, 25, 72–74. [Google Scholar] [CrossRef]
- Brange, J.; Havelund, S.; Hommel, E.; Sørensen, E.; Kuhl, C. Neutral Insulin Solutions Physically Stabilized by Addition of Zn2+. Diabet. Med. 1986, 3, 532–536. [Google Scholar] [CrossRef] [PubMed]
- Brange, J. Chemical stability of insulin. 4. Mechanisms and kinetics of chemical transformations in pharmaceutical formulation. Acta Pharm. Nord. 1992, 4, 209–222. [Google Scholar]
- Kinnare, K.F.; Bacon, C.A.; Chen, Y.; Sowa, D.C.; Peterson, S.J. Risk Factors for Predicting Hypoglycemia in Patients Receiving Concomitant Parenteral Nutrition and Insulin Therapy. J. Acad. Nutr. Diet. 2013, 113, 263–268. [Google Scholar] [CrossRef] [PubMed]
- McMahon, M.M. Management of Parenteral Nutrition in Acutely Ill Patients with Hyperglycemia. Nutr. Clin. Pr. 2004, 19, 120–128. [Google Scholar] [CrossRef]
- Gosmanov, A.R.; Umpierrez, G.E. Management of hyperglycemia during enteral and parenteral nutrition therapy. Curr. Diabetes Rep. 2012, 13, 155–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sajbel, T.; Dutro, M.; Radway, P. Use of separate insulin infusions with total parenteral nutrition. J. Parenter. Enter. Nutr. 1987, 11, 97–99. [Google Scholar] [CrossRef] [PubMed]
- Roehl, K.A.; Lach, K.; Coltman, A.E.; Bacon, C.A.; Singh, S.; Peterson, S.J.; Sowa, D.C. Predictors of Insulin Requirements Among Hospitalized Adults Receiving Parenteral Nutrition. J. Parenter. Enter. Nutr. 2013, 37, 755–762. [Google Scholar] [CrossRef]
- Olveira, G.; Abuín, J.; López, R.; Herranz, S.; García-Almeida, J.M.; García-Malpartida, K.; Ferrer, M.; Cancer, E.; Luengo-Pérez, L.M.; Álvarez, J.; et al. Regular insulin added to total parenteral nutrition vs subcutaneous glargine in non-critically ill diabetic inpatients, a multicenter randomized clinical trial: INSUPAR trial. Clin. Nutr. 2020, 39, 388–394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hakeam, H.A.; Mulia, H.A.; Azzam, A.; Amin, T. Glargine Insulin Use Versus Continuous Regular Insulin in Diabetic Surgical Noncritically Ill Patients Receiving Parenteral Nutrition: Randomized Controlled Study. J. Parenter. Enter. Nutr. 2016, 41, 1110–1118. [Google Scholar] [CrossRef] [PubMed]
- Truong, S.; Park, A.; Kamalay, S.; Hung, N.; Meyer, J.G.; Nguyen, N.; Momenzadeh, A. Glycemic Control in Adult Surgical Patients Receiving Regular Insulin Added to Parenteral Nutrition vs Insulin Glargine: A Retrospective Chart Review. Nutr. Clin. Pr. 2019, 34, 775–782. [Google Scholar] [CrossRef] [PubMed]
- Oghazian, M.B.; Javadi, M.R.; Radfar, M.; Torkamandi, H.; Sadeghi, M.; Hayatshahi, A.; Gholami, K. Effectiveness of Regular Versus Glargine Insulin in Stable Critical Care Patients Receiving Parenteral Nutrition: A Randomized Controlled Trial. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2015, 35, 148–157. [Google Scholar] [CrossRef]
- Jakoby, M.G.; Nannapaneni, N. An Insulin Protocol for Management of Hyperglycemia in Patients Receiving Parenteral Nutrition Is Superior to Ad Hoc Management. J. Parenter. Enter. Nutr. 2011, 36, 183–188. [Google Scholar] [CrossRef] [PubMed]
- McCulloch, A.; Bansiya, V.; Woodward, J.M. Addition of Insulin to Parenteral Nutrition for Control of Hyperglycemia. J. Parenter. Enter. Nutr. 2017, 42, 846–854. [Google Scholar] [CrossRef] [PubMed]
- Andersen, S.; Andersen, A.; Ringholm, L.; Hansen, C.P.; Storkholm, J.; Lillpers, K.; Schiøtz, C.; Mathiesen, E.R. Parenteral nutrition and insulin per protocol improve diabetes management after total pancreatectomy. Dan. Med. J. 2018, 65, A5475. [Google Scholar]
- Ramos, A.; Rabasa, F.; Mendoza, L.; Cardenete, J.; Gill, P.; Morilla, A.; Cardona, D.; Pérez, A. Differences in Glycemic Control in Diabetic and Non-diabetic Patients with Parenteral Nutrition Using a Basal plus Correction Insulin Regimen: An Observational, Retrospective Study. Diabetes Ther. Res. Treat. Educ. Diabetes Relat. Disord. 2018, 9, 1359–1367. [Google Scholar] [CrossRef]
- Yilmaz, B.; Kadioglu, Y.; Capoglu, I. Determination of Insulin in Humans with Insulin-Dependent Diabetes Mellitus Patients by HPLC with Diode Array Detection. J. Chromatogr. Sci. 2012, 50, 586–590. [Google Scholar] [CrossRef]
- Hoyer, G.L.; Nolan, P.E.; LeDoux, J.H.; Moore, L.A. Selective stability-indicating high-performance liquid chromatographic assay for recombinant human regular insulin. J. Chromatogr. A 1995, 699, 383–388. [Google Scholar] [CrossRef]
- Yu, K.-H.; Tsao, H.-L.; Lin, S.-J.; Chen, C.-Y. Quantitative analysis of insulin in total parenteral nutrition bag in Taiwan. J. Food Drug Anal. 2016, 24, 214–219. [Google Scholar] [CrossRef] [Green Version]
- Oliva, A.; Fariña, J.; Llabrés, M. Development of two high-performance liquid chromatographic methods for the analysis and characterization of insulin and its degradation products in pharmaceutical preparations. J. Chromatogr. B: Biomed. Sci. Appl. 2000, 749, 25–34. [Google Scholar] [CrossRef]
- Roche laboratory. Insulin Elecsys Kit: Instructions for Use [Internet]. Roche Diagn. Available online: http://www.Diagnostics.roche.com (accessed on 1 April 2020).
- Forchielli, M.L.; Bongiovanni, F.; Platé, L.; Piazza, G.; Puggioli, C.; D’Alise, A.; Bersani, G. Insulin Instability in Parenteral Nutrition Admixtures. J. Parenter. Enter. Nutr. 2018, 42, 907–912. [Google Scholar] [CrossRef] [PubMed]
- McCulloch, A.; Bansiya, V.; Woodward, J. The addition of insulin to home parenteral nutrition for the control of hyperglycaemia: A case series. Clin. Nutr. ESPEN 2019, 30, 204–207. [Google Scholar] [CrossRef]
- Goebel-Stengel, M.; Stengel, A.; Taché, Y.; Reeve, J.R. The importance of using the optimal plasticware and glassware in studies involving peptides. Anal. Biochem. 2011, 414, 38–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuatrecasas, P.; Hollenberg, M.D. Binding of insuling and other hormones to non-receptor materials: Saturability, specificity and apparent “negative cooperativity”. Biochem. Biophys. Res. Commun. 1975, 62, 31–41. [Google Scholar] [CrossRef]
- Cecil, R.; Robinson, G.B. The “specific” binding of insulin to polyethene and other materials. Biochim. Biophys. Acta 1975, 404, 164–168. [Google Scholar] [CrossRef]
- Zahid, N.; Taylor, K.M.; Gill, H.; Maguire, F.; Shulman, R. Adsorption of insulin onto infusion sets used in adult intensive care unit and neonatal care settings. Diabetes Res. Clin. Pr. 2008, 80, e11–e13. [Google Scholar] [CrossRef]
- Ley, S.; Ammann, J.; Herder, C.; Hartmann, M.; Kindgen-Milles, D. Variable adsorption of insulin at catheter materials used in intensive care units: Polyethylene vs. polyurethane—possible cause for hypoglycemia during intensive insulin treatment? Crit. Care 2007, 11, 127. [Google Scholar] [CrossRef] [Green Version]
- Chantelau, E.; Lange, G.; Gasthaus, M.; Boxberger, M.; Berger, M. Interaction between Plastic Catheter Tubings and Regular Insulin Preparations Used for Continuous Subcutaneous Insulin-Infusion Therapy. Diabetes Care 1987, 10, 348–351. [Google Scholar] [CrossRef] [PubMed]
- Mollmann, S.; Bukrinsky, J.T.; Frokjaer, S.; Elofsson, U.M. Adsorption of human insulin and AspB28 insulin on a PTFE-like surface. J. Colloid Interface Sci. 2005, 286, 28–35. [Google Scholar] [CrossRef]
- Nault, L.; Guo, P.; Jain, B.; Bréchet, Y.; Bruckert, F.; Weidenhaupt, M. Human insulin adsorption kinetics, conformational changes and amyloidal aggregate formation on hydrophobic surfaces. Acta Biomater. 2013, 9, 5070–5079. [Google Scholar] [CrossRef]
- Pandey, L.M.; Le Denmat, S.; Delabouglise, D.; Bruckert, F.; Pattanayek, S.K.; Weidenhaupt, M. Surface chemistry at the nanometer scale influences insulin aggregation. Colloids Surf. B Biointerfaces 2012, 100, 69–76. [Google Scholar] [CrossRef]
- Livesey, J.; Donald, R. Prevention of adsorption losses during radioimmunoassay of polypeptide hormones: Effectiveness of albumins, gelatin, caseins, tween 20 and plasma. Clin. Chim. Acta 1982, 123, 193–198. [Google Scholar] [CrossRef]
- Suelter, C.; DeLuca, M. How to prevent losses of protein by adsorption to glass and plastic. Anal. Biochem. 1983, 135, 112–119. [Google Scholar] [CrossRef]
- Grand, A.; Jalabert, A.; Mercier, G.; Florent, M.; Hansel-Esteller, S.; Cambonie, G.; Steghens, J.-P.; Picaud, J.-C. Influence of Vitamins, Trace Elements, and Iron on Lipid Peroxidation Reactions in All-in-One Admixtures for Neonatal Parenteral Nutrition. J. Parenter. Enter. Nutr. 2011, 35, 505–510. [Google Scholar] [CrossRef] [PubMed]
- Jalabert, A.; Grand, A.; Steghens, J.-P.; Barbotte, E.; Pigue, C.; Picaud, J.-C. Lipid peroxidation in all-in-one admixtures for preterm neonates: Impact of amount of lipid, type of lipid emulsion and delivery condition. Acta Paediatr. 2011, 100, 1200–1205. [Google Scholar] [CrossRef]
- Miloudi, K.; Comte, B.; Rouleau, T.; Montoudis, A.; Levy, E.; Lavoie, J.-C. The mode of administration of total parenteral nutrition and nature of lipid content influence the generation of peroxides and aldehydes. Clin. Nutr. 2012, 31, 526–534. [Google Scholar] [CrossRef] [PubMed]
- Dolhofer, R.; Wieland, O.H. Preparation and biological properties of glycosylated insulin. FEBS Lett. 1979, 100, 133–136. [Google Scholar] [CrossRef] [Green Version]
- O’Harte, F.P.; Højrup, P.; Barnett, C.R.; Flatt, P.R. Identification of the site of glycation of human insulin. Pept. 1996, 17, 1323–1330. [Google Scholar] [CrossRef]
- Farah, M.A.; Bose, S.; Lee, J.-H.; Jung, H.-C.; Kim, Y. Analysis of glycated insulin by MALDI-TOF mass spectrometry. Biochim. Biophys. Acta (BBA) Gen. Subj. 2005, 1725, 269–282. [Google Scholar] [CrossRef] [PubMed]
- Boyd, A.C.; Abdel-Wahab, Y.H.; McKillop, A.M.; McNulty, H.; Barnett, C.R.; O’Harte, F.P.; Flatt, P.R. Impaired ability of glycated insulin to regulate plasma glucose and stimulate glucose transport and metabolism in mouse abdominal muscle. Biochim. Biophys. Acta (BBA) Gen. Subj. 2000, 1523, 128–134. [Google Scholar] [CrossRef]
- Hunter, S.J.; Boyd, A.C.; O’Harte, F.P.; McKillop, A.M.; Wiggam, M.I.; Mooney, M.H.; McCluskey, J.T.; Lindsay, J.R.; Ennis, C.N.; Gamble, R.; et al. Demonstration of Glycated Insulin in Human Diabetic Plasma and Decreased Biological Activity Armed During Storage of Neutral Formulation of Human Insulin. Pharm. Res. 2015, 32, 2072–2085. [Google Scholar]
- Quinn, R.; Andrade, J.D. Minimizing the aggregation of neutral insulin solutions. J. Pharm. Sci. 1983, 72, 1472–1473. [Google Scholar] [CrossRef] [PubMed]
- Hjorth, C.F.; Hubálek, F.; Andersson, J.; Poulsen, C.; Otzen, D.; Naver, H. Purification and Identification of High Molecular Weight Products Fonature of lipid content influence the generation of peroxides and aldehydes. Clin. Nutr. 2012, 31, 526–534. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Media | Composition | pH |
|---|---|---|
| Ternary (3-in-1) | A + B + C | 6.34 |
| Binary (2-in-1) | A + B | 6.34 |
| Dextrose | A | 3.6 |
| Amino acids | B | 6.5 |
| Lipids | C | >7.0 |
| Brand Name | Nature of Lipids (Oil Origin) | Concentrations (%) |
|---|---|---|
| OlimelTM lipid emulsion | Olive oil (80%) + soybean oil (20%) | 5, 10, 20 |
| MedialipideTM | Soybean oil (50%) + medium-chain fatty acids (50%) | 20 |
| IntralipideTM | Soybean oil | 20 |
| OmegavenTM | Fish oil | 10 |
| SmoflipidTM | Medium-chain fatty acids (30%) + soybean oil (30%) + olive oil (25%) + fish oil (15%) | 20 |
| Quantitative Data | Qualitative Data |
|---|---|
| 1/Ct | Trace elements |
| Time | Zn |
| pH level (3.5 or 6.5) | Pre conditioning |
| Dextrose content (%) | Conditioning |
| Amino acid content (%) | Nature of lipid emulsion |
| Lipid content (%) | Container |
| Independent Variables | Correspondence with Equation (2) | Variables in Interaction | Correspondence with Equation (2) |
|---|---|---|---|
| Time (hours) | A | Time and pH level | E |
| Dextrose content (%) | B | pH level and dextrose content | F |
| Lipid content (%) | C | pH level and amino acid content | G |
| Absence of trace-elements | D |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Henry, H.; Lannoy, D.; Maboudou, P.; Seguy, D.; Dine, T.; Pigny, P.; Odou, P. Addition of Regular Insulin to Ternary Parenteral Nutrition: A Stability Study. Pharmaceutics 2021, 13, 458. https://doi.org/10.3390/pharmaceutics13040458
Henry H, Lannoy D, Maboudou P, Seguy D, Dine T, Pigny P, Odou P. Addition of Regular Insulin to Ternary Parenteral Nutrition: A Stability Study. Pharmaceutics. 2021; 13(4):458. https://doi.org/10.3390/pharmaceutics13040458
Chicago/Turabian StyleHenry, Heloise, Damien Lannoy, Patrice Maboudou, David Seguy, Thierry Dine, Pascal Pigny, and Pascal Odou. 2021. "Addition of Regular Insulin to Ternary Parenteral Nutrition: A Stability Study" Pharmaceutics 13, no. 4: 458. https://doi.org/10.3390/pharmaceutics13040458