
Development and Characterization of Inhaled Ethanol as a Novel Pharmacological Strategy Currently Evaluated in a Phase II Clinical Trial for Early-Stage SARS-CoV-2 Infection

 ,
,  , ,
, ,  , , ,
, , ,  , , , , , , , , add
Show full author list
, , , , , , , , add
Show full author list
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Preparation of the 65° Ethanol Solution and Stability Determination in Disposable Humidifying Bottles
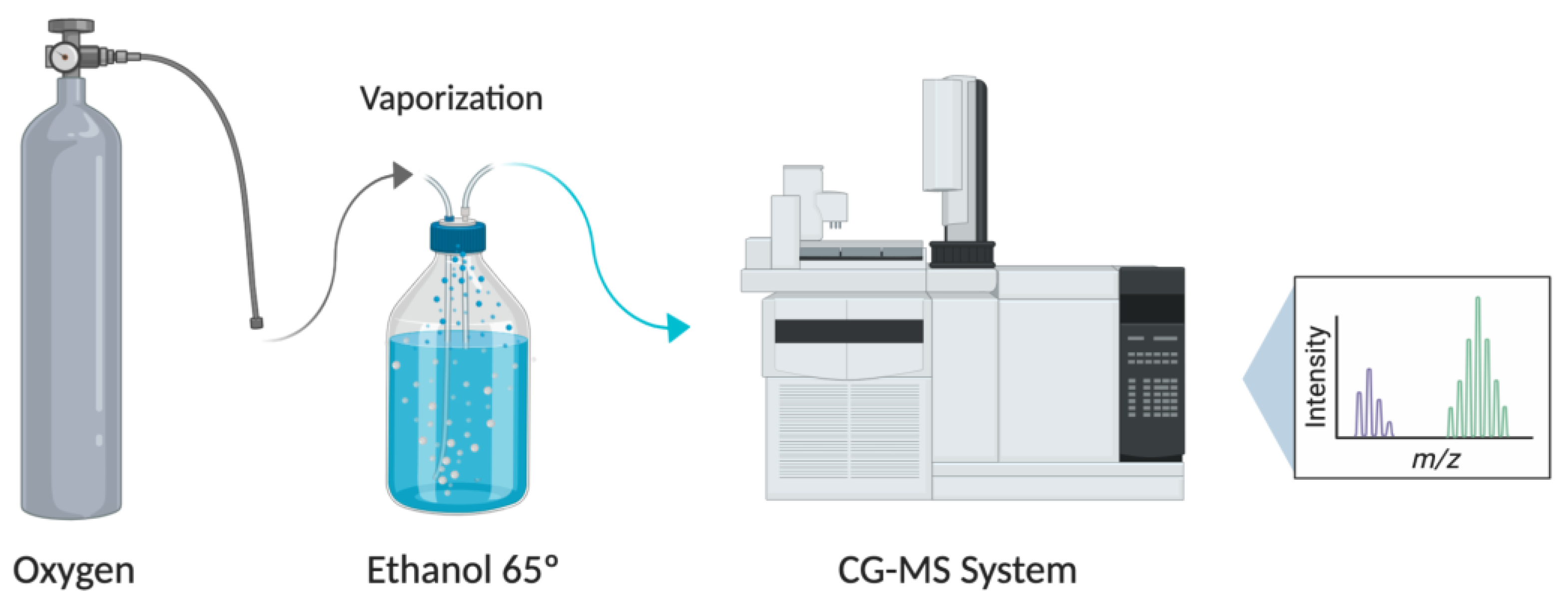
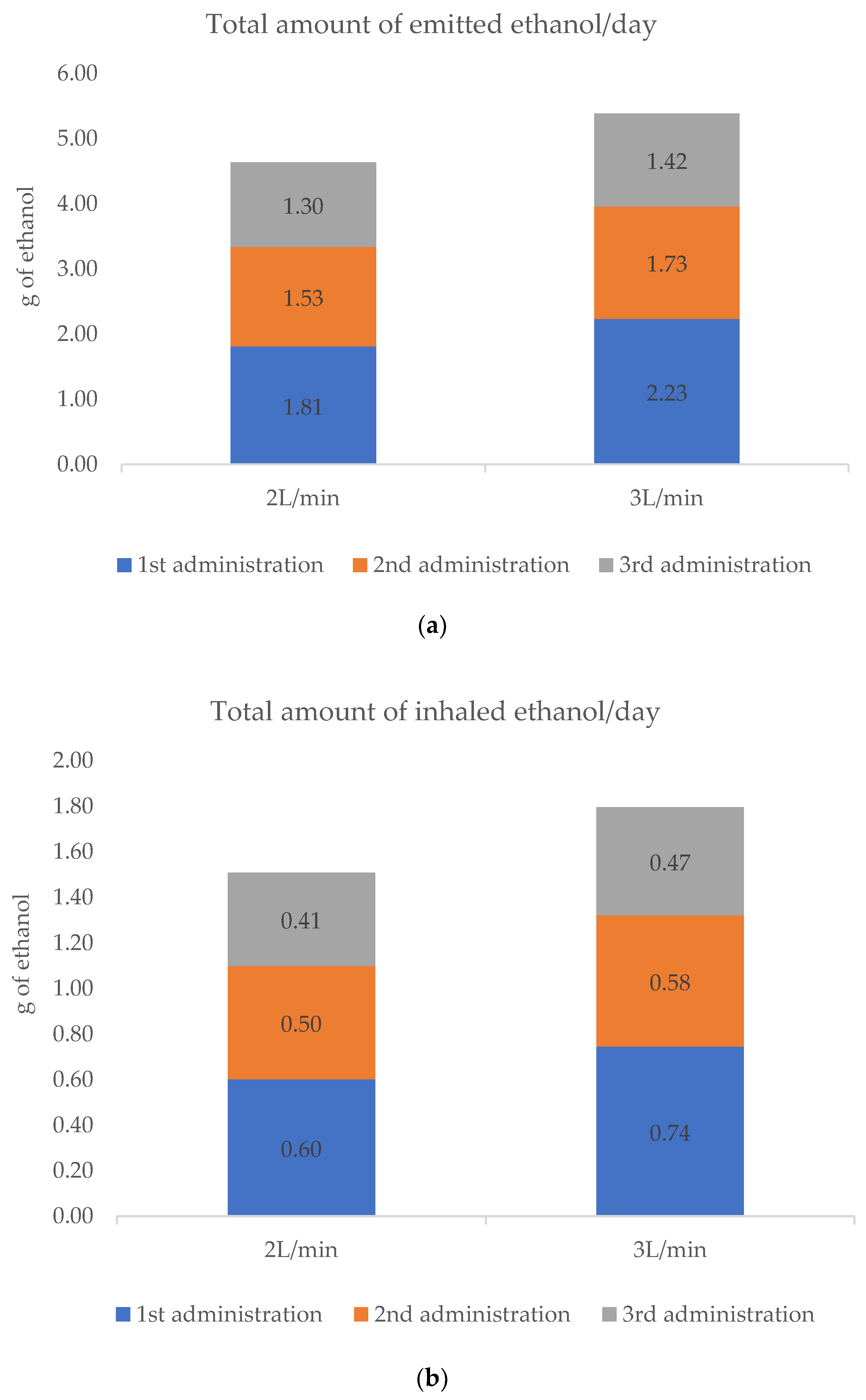
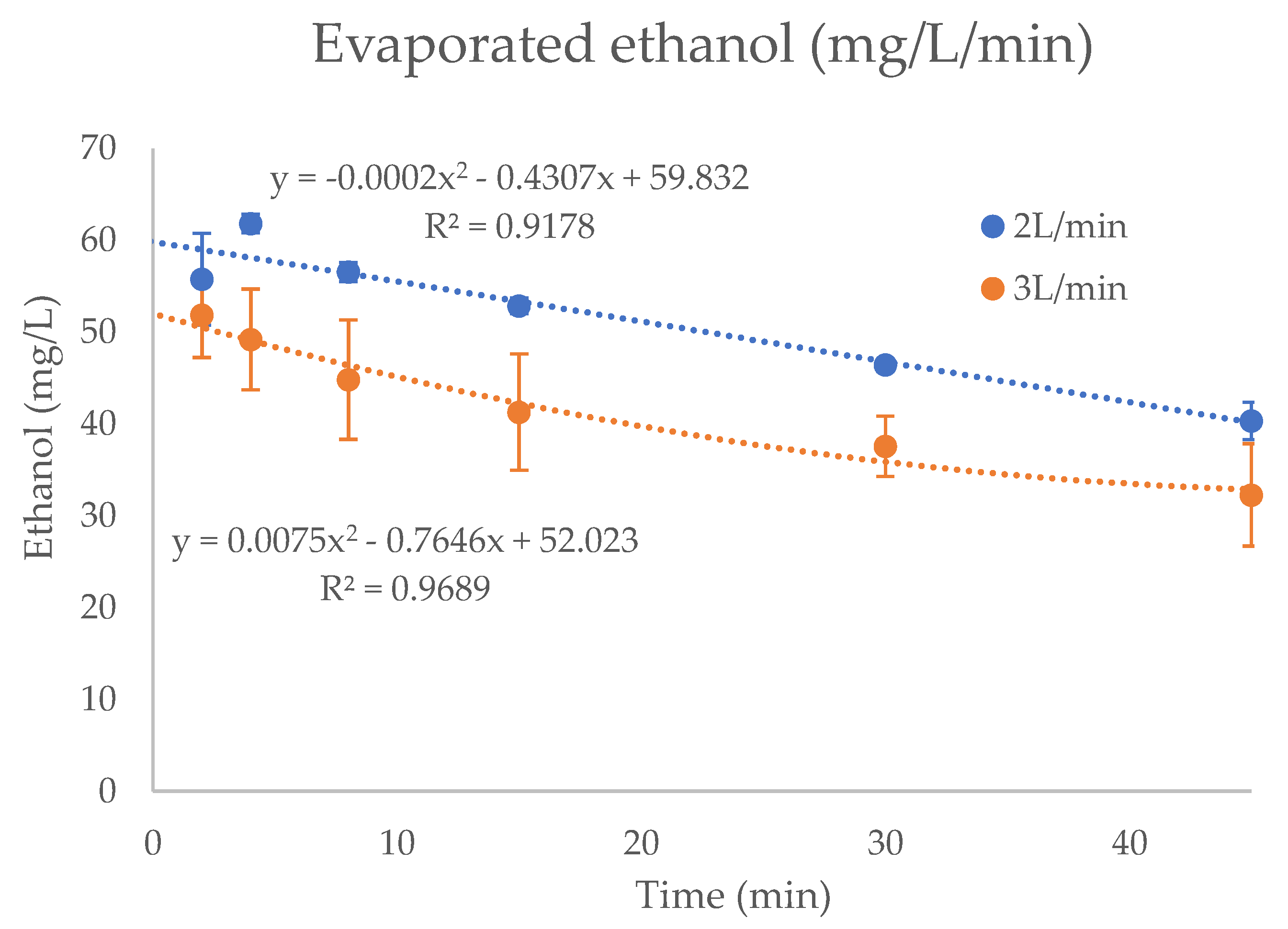
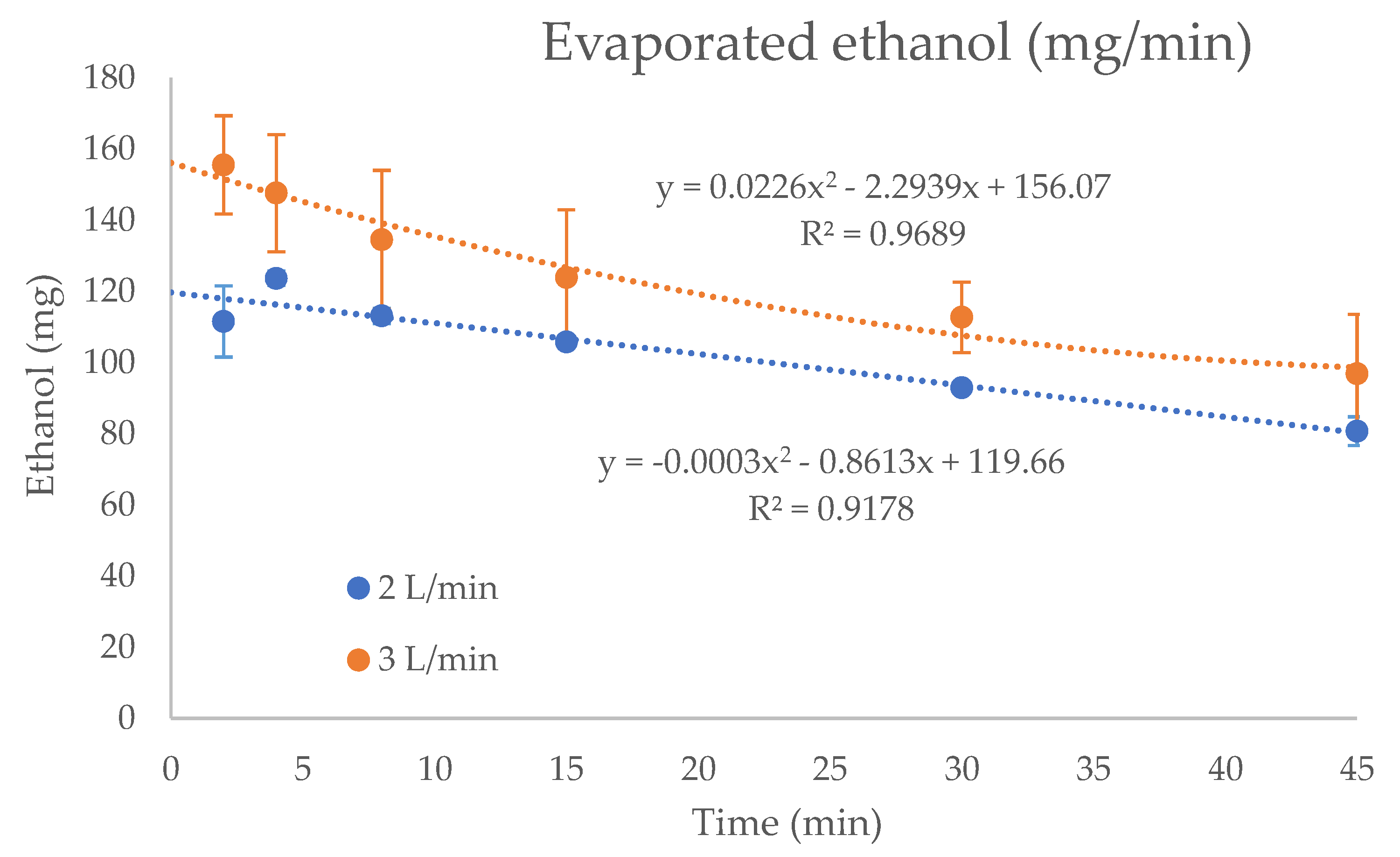
2.2. Determination of Ethanol in the Administered Oxygen Flow
2.3. Preclinical Studies
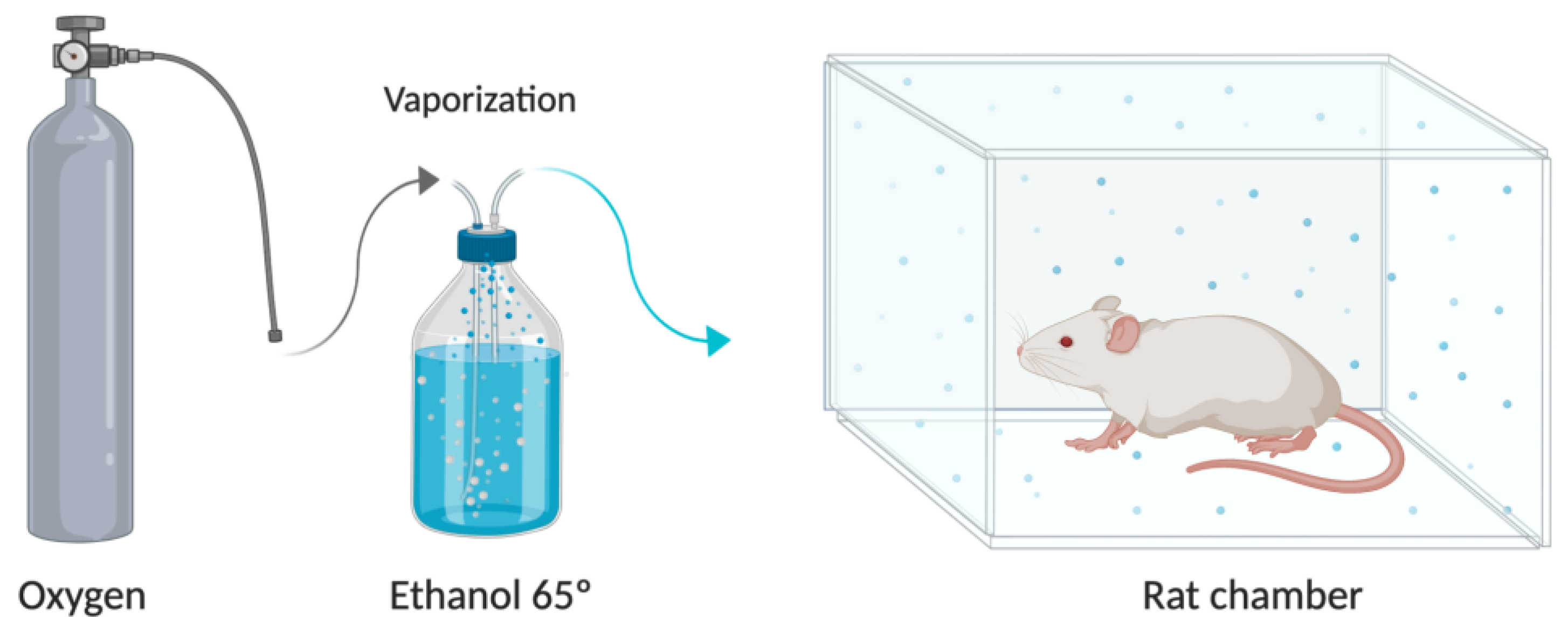
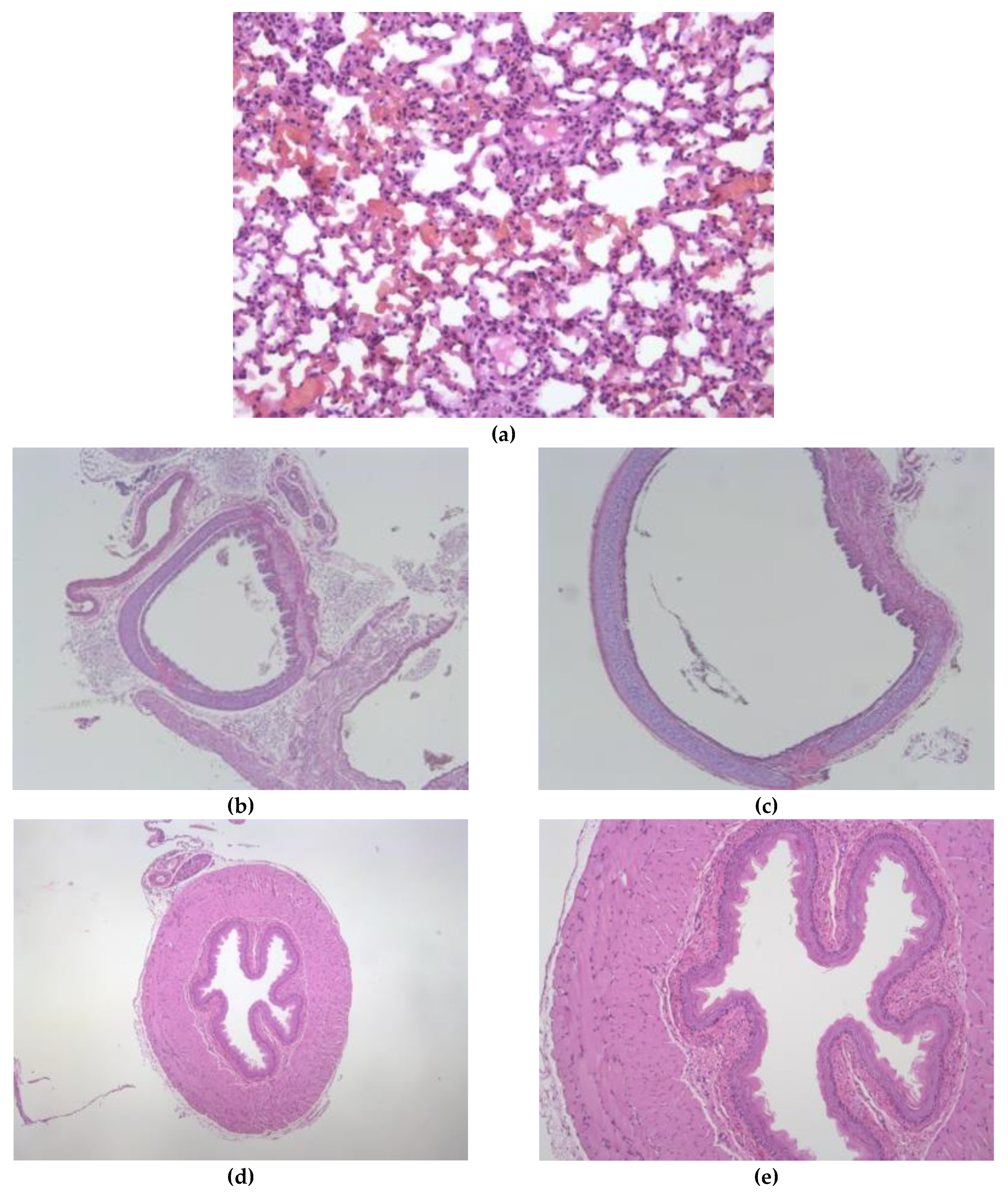
2.3.1. Ethanol Exposure Toxicological Studies and Immunohistochemical Analysis
2.3.2. Preclinical Pharmacokinetics
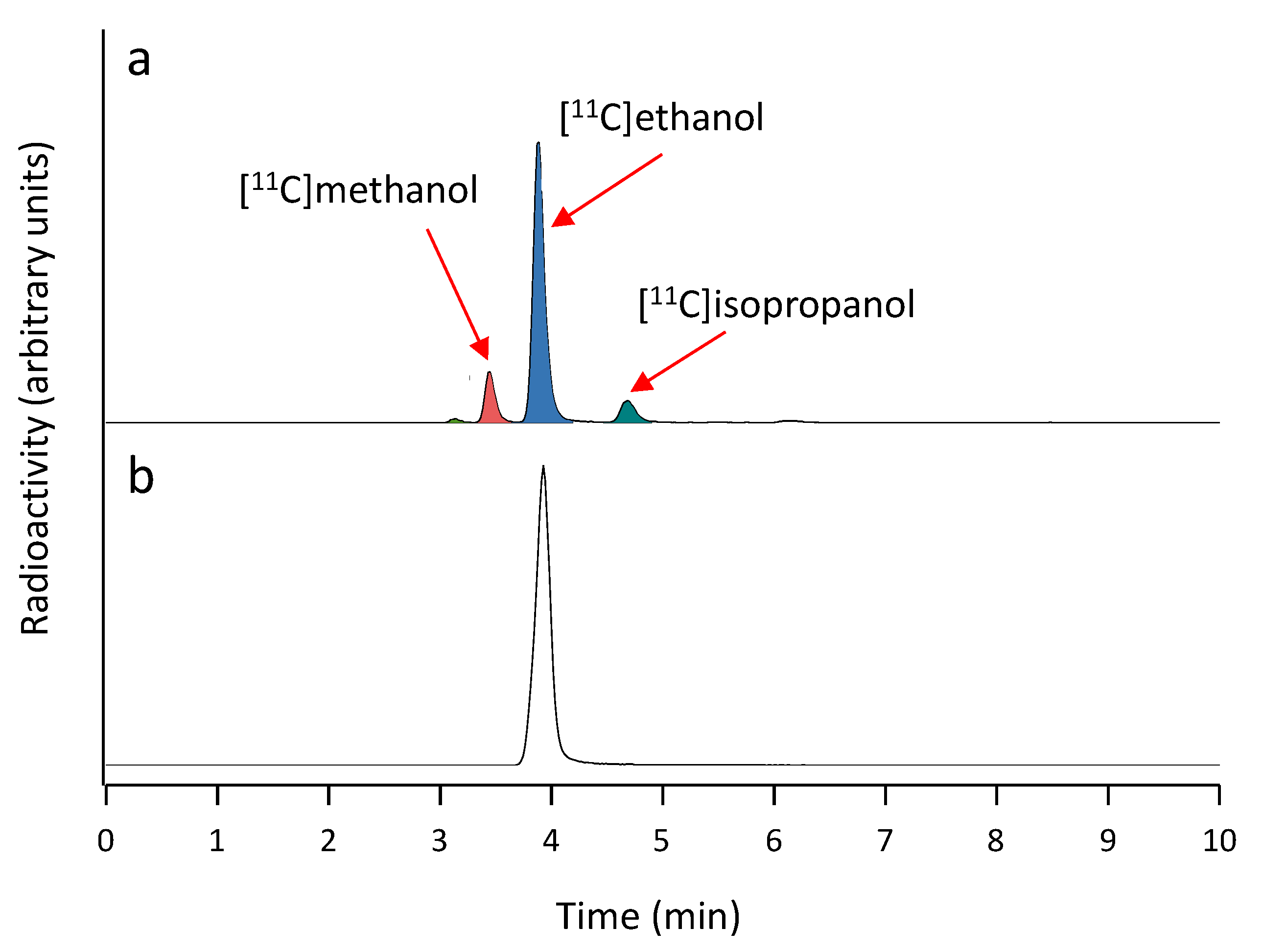
Synthesis of 1-11C-Ethanol
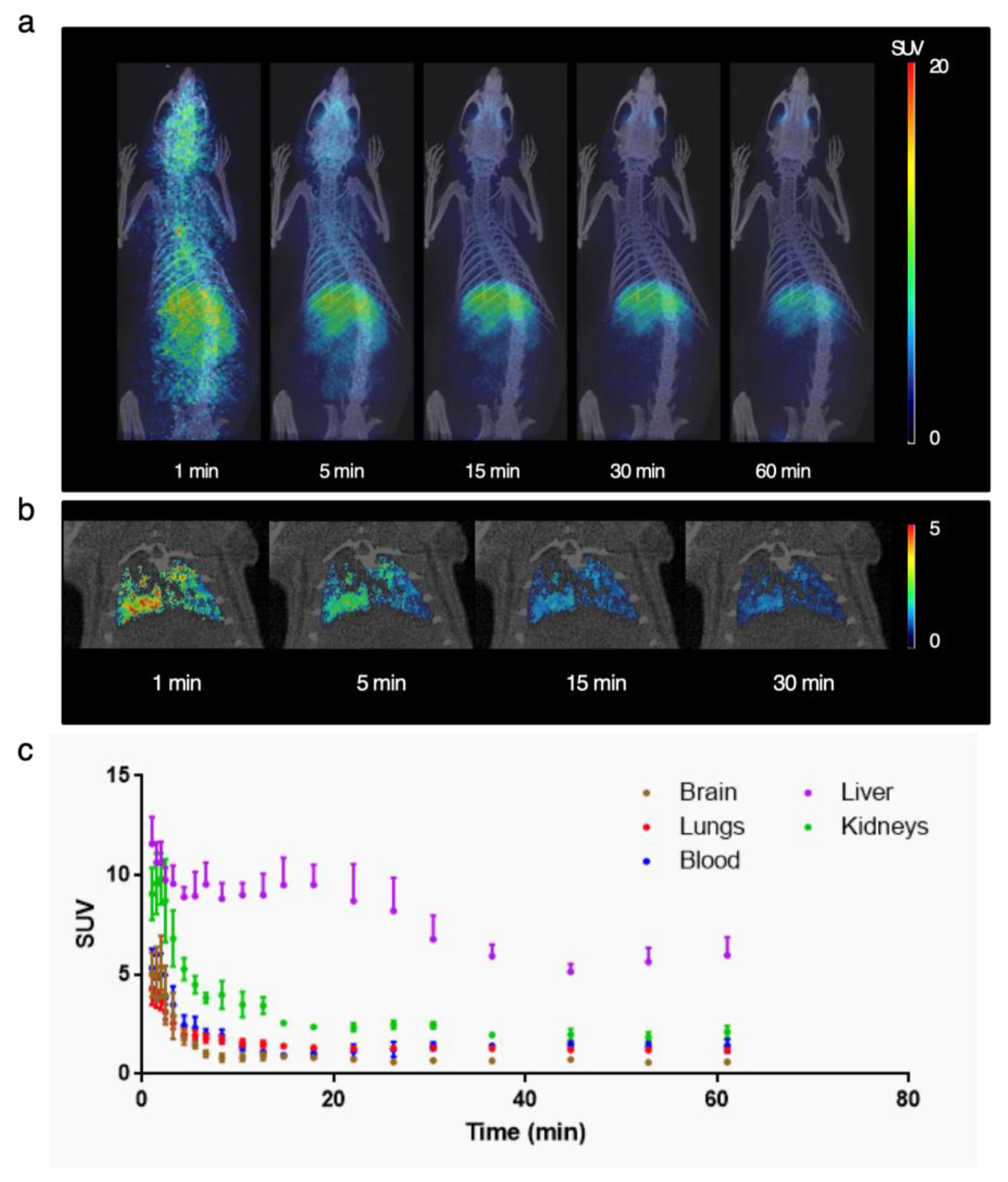
Lung PET Studies
3. Results
3.1. Stability of the 65° Ethanol Pharmaceutical Compounding and Flow Oxygen Effect
3.2. Preclinical Studies
3.2.1. Ethanol Exposure Toxicological Studies and Immunohistochemical Analysis
3.2.2. Pharmacokinetics
Synthesis of 1-11C-Ethanol
Lung PET Studies
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Weiss, S.R.; Leibowitz, J.L. Coronavirus Pathogenesis. Adv. Virus Res. 2011, 81, 85–164. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.; Yang, H.; Ji, W.; Wu, W.; Chen, S.; Zhang, W.; Duan, G. Virology, Epidemiology, Pathogenesis, and Control of COVID-19. Viruses 2020, 12, 372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rothan, H.A.; Byrareddy, S.N. The Epidemiology and Pathogenesis of Coronavirus Disease (COVID-19) Outbreak. J. Autoimmun. 2020, 109, 102433. [Google Scholar] [CrossRef]
- WHO. Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 16 January 2021).
- Baker, M.G.; Kvalsvig, A.; Verrall, A.J. New Zealand’s COVID-19 Elimination Strategy. Med. J. Aust. 2020. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; Sahly, H.M.E.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the MRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 MRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Knoll, M.D.; Wonodi, C. Oxford-AstraZeneca COVID-19 Vaccine Efficacy. Lancet 2021, 397, 72–74. [Google Scholar] [CrossRef]
- Stasi, C.; Fallani, S.; Voller, F.; Silvestri, C. Treatment for COVID-19: An Overview. Eur. J. Pharmacol. 2020, 889, 173644. [Google Scholar] [CrossRef]
- Li, Y.; Liu, S.; Zhang, S.; Ju, Q.; Zhang, S.; Yang, Y.; Wang, H. Current Treatment Approaches for COVID-19 and the Clinical Value of Transfusion-Related Technologies. Transfus. Apher. Sci. 2020, 59, 102839. [Google Scholar] [CrossRef]
- Libster, R.; Pérez Marc, G.; Wappner, D.; Coviello, S.; Bianchi, A.; Braem, V.; Esteban, I.; Caballero, M.T.; Wood, C.; Berrueta, M.; et al. Early High-Titer Plasma Therapy to Prevent Severe Covid-19 in Older Adults. N. Engl. J. Med. 2021. [Google Scholar] [CrossRef]
- PharmaMar Multicenter. Randomized, Parallel and Proof of Concept Study to Evaluate the Safety Profile of Three Doses of Plitidepsin in Patients with COVID-19 Requiring Hospitalization. 2020. Available online: clinicaltrials.gov (accessed on 25 January 2021).
- Eli Lilly and Company. Expanded Access Information for Physicians for Bamlanivimab (LY3819253) Emergency Investigational New Drug (EIND). 2021. Available online: clinicaltrials.gov (accessed on 25 February 2021).
- Regeneron Pharmaceuticals. A Master Protocol Assessing the Safety, Tolerability, and Efficacy of Anti-Spike (S) SARS-CoV-2 Monoclonal Antibodies for the Treatment of Ambulatory Patients with COVID-19. 2021. Available online: clinicaltrials.gov (accessed on 25 February 2021).
- Group, T.R.C. Dexamethasone in Hospitalized Patients with Covid-19—Preliminary Report. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- Andersen, P.I.; Ianevski, A.; Lysvand, H.; Vitkauskiene, A.; Oksenych, V.; Bjørås, M.; Telling, K.; Lutsar, I.; Dumpis, U.; Irie, Y.; et al. Discovery and Development of Safe-in-Man Broad-Spectrum Antiviral Agents. Int. J. Infect. Dis. 2020, 93, 268–276. [Google Scholar] [CrossRef] [PubMed]
- Kampf, G.; Todt, D.; Pfaender, S.; Steinmann, E. Persistence of Coronaviruses on Inanimate Surfaces and Their Inactivation with Biocidal Agents. J. Hosp. Infect. 2020, 104, 246–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laboratory Biosafety Guidance Related to Coronavirus Disease (COVID-19). Available online: https://www.who.int/publications-detail-redirect/laboratory-biosafety-guidance-related-to-coronavirus-disease-(covid-19) (accessed on 21 June 2020).
- Kratzel, A.; Todt, D.; V’kovski, P.; Steiner, S.; Gultom, M.; Thao, T.T.N.; Ebert, N.; Holwerda, M.; Steinmann, J.; Niemeyer, D.; et al. Inactivation of Severe Acute Respiratory Syndrome Coronavirus 2 by WHO-Recommended Hand Rub Formulations and Alcohols. Emerg. Infect. Dis. 2020, 26. [Google Scholar] [CrossRef] [PubMed]
- Opilla, M.T.; Kirby, D.F.; Edmond, M.B. Use of Ethanol Lock Therapy to Reduce the Incidence of Catheter-Related Bloodstream Infections in Home Parenteral Nutrition Patients. JPEN J. Parenter. Enteral Nutr. 2007, 31, 302–305. [Google Scholar] [CrossRef] [PubMed]
- Lipton, S. Pain Relief in Active Patients with Cancer: The Early Use of Nerve Blocks Improves the Quality of Life. BMJ 1989, 298, 37–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarin, S.K.; Sachdeva, G.K.; Nanda, R.; Vij, J.C.; Anand, B.S. Endoscopic Sclerotherapy Using Absolute Alcohol. Gut 1985, 26, 120–124. [Google Scholar] [CrossRef] [Green Version]
- Chung, S.C.; Lee, T.W.; Kwok, S.P.; Li, A.K. Injection of Alcohol to Control Bleeding from Ruptured Hepatomas. BMJ 1990, 301, 421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuksel, E.; Novruzlu, S.; Ozmen, M.C.; Bilgihan, K. A Study Comparing Standard and Transepithelial Collagen Cross-Linking Riboflavin Solutions: Epithelial Findings and Pain Scores. J. Ocul. Pharmacol. Ther. 2015, 31, 296–302. [Google Scholar] [CrossRef]
- Sepúlveda, R.A.; Selamé, E.; Roessler, E.; Tagle, R.; Valdivieso, A. Intoxicación Por Etilenglicol, Fisiopatología y Enfrentamiento Clínico. Rev. Med. Chil. 2019, 147, 1572–1578. [Google Scholar] [CrossRef]
- Statement—Older People Are at Highest Risk from COVID-19, but All Must Act to Prevent Community Spread. Available online: http://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/statements/statement-older-people-are-at-highest-risk-from-covid-19,-but-all-must-act-to-prevent-community-spread (accessed on 8 June 2020).
- Li, P.; Chen, L.; Liu, Z.; Pan, J.; Zhou, D.; Wang, H.; Gong, H.; Fu, Z.; Song, Q.; Min, Q.; et al. Clinical Features and Short-Term Outcomes of Elderly Patients with COVID-19. Int. J. Infect. Dis. 2020, 97, 245–250. [Google Scholar] [CrossRef]
- Kampf, G. Efficacy of Ethanol against Viruses in Hand Disinfection. J. Hosp. Infect. 2018, 98, 331–338. [Google Scholar] [CrossRef]
- Yan, R.; Zhang, Y.; Li, Y.; Xia, L.; Guo, Y.; Zhou, Q. Structural Basis for the Recognition of SARS-CoV-2 by Full-Length Human ACE2. Science 2020, 367, 1444–1448. [Google Scholar] [CrossRef] [Green Version]
- Ensayo Clínico Fase II Para Evaluar La Eficacia y Seguridad de Etanol Inhalado En El Tratamiento de La COVID-19 En Estadio Inicial. Available online: https://reec.aemps.es/reec/estudio/2020-001760-29 (accessed on 9 January 2021).
- Kilkenny, C.; Browne, W.; Cuthill, I.C.; Emerson, M.; Altman, D.G. NC3Rs Reporting Guidelines Working Group Animal Research: Reporting in Vivo Experiments: The ARRIVE Guidelines. Br. J. Pharmacol. 2010, 160, 1577–1579. [Google Scholar] [CrossRef]
- Seoane-Viaño, I.; Gómez-Lado, N.; Lázare-Iglesias, H.; Barreiro-de Acosta, M.; Silva-Rodríguez, J.; Luzardo-Álvarez, A.; Herranz, M.; Otero-Espinar, F.; Antúnez-López, J.R.; Lamas, M.J.; et al. Longitudinal PET/CT Evaluation of TNBS-Induced Inflammatory Bowel Disease Rat Model. Int. J. Pharm. 2018, 549, 335–342. [Google Scholar] [CrossRef] [PubMed]
- U.S. EPA. Exposure Factors Handbook 2011 Edition (Final Report); EPA/600/R-09/052F; U.S. Environmental Protection Agency: Washington, DC, USA, 2011.
- Gulyás, B.; Vas, A.; Halldin, C.; Sóvágó, J.; Sandell, J.; Olsson, H.; Fredriksson, A.; Stone-Elander, S.; Farde, L. Cerebral Uptake of (Ethyl-11C) Vinpocetine and 1-(11C) Ethanol in Cynomolgous Monkeys: A Comparative Preclinical PET Study. Nucl. Med. Biol. 2002, 29, 753–759. [Google Scholar] [CrossRef]
- DeGrazia, J.A.; Rodden, A.F.; Teresi, J.D.; Busick, D.D.; Walz, D.R. Radioscintigraphic Studies of 11C Distribution in Cats given 1-11 C-Ethanol. J. Nucl. Med. 1975, 16, 73–76. [Google Scholar] [PubMed]
- Cossío, U.; Gómez-Vallejo, V.; Flores, M.; Gañán-Calvo, B.; Jurado, G.; Llop, J. Preclinical Evaluation of Aerosol Administration Systems Using Positron Emission Tomography. Eur. J. Pharm. Biopharm. 2018, 130, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Castro-Balado, A.; Varela-Rey, I.; Bandín-Vilar, E.J.; Busto-Iglesias, M.; García-Quintanilla, L.; Mondelo-García, C.; Fernández-Ferreiro, A. Clinical Research in Hospital Pharmacy during the Fight against COVID-19. Farm. Hosp. 2020, 44, 66–70. [Google Scholar] [CrossRef]
- Dai, L.; Gao, G.F. Viral Targets for Vaccines against COVID-19. Nat. Rev. Immunol. 2020. [Google Scholar] [CrossRef]
- Fernández-Ferreiro, A.; González-Barcia, M. The Human Being, the Only Animal That Needs a Master to Live. OFIL·ILAPHAR 2020, 30, 179–182. [Google Scholar]
- Cao, B.; Wang, Y.; Wen, D.; Liu, W.; Wang, J.; Fan, G.; Ruan, L.; Song, B.; Cai, Y.; Wei, M.; et al. A Trial of Lopinavir–Ritonavir in Adults Hospitalized with Severe Covid-19. N. Engl. J. Med. 2020, 2001282. [Google Scholar] [CrossRef] [PubMed]
- RECOVERY Collaborative Group; Horby, P.; Mafham, M.; Linsell, L.; Bell, J.L.; Staplin, N.; Emberson, J.R.; Wiselka, M.; Ustianowski, A.; Elmahi, E.; et al. Effect of Hydroxychloroquine in Hospitalized Patients with Covid-19. N. Engl. J. Med. 2020, 383, 2030–2040. [Google Scholar] [CrossRef] [PubMed]
- Stone, J.H.; Frigault, M.J.; Serling-Boyd, N.J.; Fernandes, A.D.; Harvey, L.; Foulkes, A.S.; Horick, N.K.; Healy, B.C.; Shah, R.; Bensaci, A.M.; et al. Efficacy of Tocilizumab in Patients Hospitalized with Covid-19. N. Engl. J. Med. 2020, 383, 2333–2344. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Zhang, W.; Hu, Y.; Tong, X.; Zheng, S.; Yang, J.; Kong, Y.; Ren, L.; Wei, Q.; Mei, H.; et al. Effect of Convalescent Plasma Therapy on Time to Clinical Improvement in Patients with Severe and Life-Threatening COVID-19: A Randomized Clinical Trial. JAMA 2020, 324, 460–470. [Google Scholar] [CrossRef]
- Talavera, B.; García-Azorín, D.; Martínez-Pías, E.; Trigo, J.; Hernández-Pérez, I.; Valle-Peñacoba, G.; Simón-Campo, P.; de Lera, M.; Chavarría-Miranda, A.; López-Sanz, C.; et al. Anosmia Is Associated with Lower In-Hospital Mortality in COVID-19. J. Neurol. Sci. 2020, 419, 117163. [Google Scholar] [CrossRef]
- Shintake, T. Possibility of Disinfection of SARS-CoV-2 (COVID-19) in Human Respiratory Tract by Controlled Ethanol Vapor Inhalation. arXiv 2020, arXiv:2003.12444. [Google Scholar]
- Ly, T.D.A.; Zanini, D.; Laforge, V.; Arlotto, S.; Gentile, S.; Mendizabal, H.; Finaud, M.; Morel, D.; Quenette, O.; Malfuson-Clot-Faybesse, P.; et al. Pattern of SARS-CoV-2 Infection among Dependant Elderly Residents Living in Long-Term Care Facilities in Marseille, France, March–June 2020. Int. J. Antimicrob. Agents 2020, 56, 106219. [Google Scholar] [CrossRef]
- Durst, H.D.; Gokel, G.W. Química Orgánica Experimental; Editorial Reverté: Barcelona, Spain, 1985; ISBN 978-84-291-7155-6. [Google Scholar]
- Bessonneau, V.; Thomas, O. Assessment of Exposure to Alcohol Vapor from Alcohol-Based Hand Rubs. Int. J. Environ. Res. Public Health 2012, 9, 868–879. [Google Scholar] [CrossRef] [Green Version]
- Luisada, A.A.; Goldmann, M.A.; Weyl, R. Alcohol Vapor by Inhalation in the Treatment of Acute Pulmonary Edema. Circulation 1952, 5, 363–369. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.; Kleinstreuer, C.; Kim, C.S. Transport and Uptake of MTBE and Ethanol Vapors in a Human Upper Airway Model. Inhal. Toxicol. 2006, 18, 169–184. [Google Scholar] [CrossRef]
- Rogers, J.; Wiener, S.G.; Bloom, F.E. Long-Term Ethanol Administration Methods for Rats: Advantages of Inhalation over Intubation or Liquid Diets. Behav. Neural Biol. 1979, 27, 466–486. [Google Scholar] [CrossRef]
- MacLean, R.R.; Valentine, G.W.; Jatlow, P.I.; Sofuoglu, M. Inhalation of Alcohol Vapor: Measurement and Implications. Alcohol. Clin. Exp. Res. 2017, 41, 238–250. [Google Scholar] [CrossRef] [PubMed]
- Gilpin, N.W.; Richardson, H.N.; Cole, M.; Koob, G.F. Vapor Inhalation of Alcohol in Rats. Curr. Protoc. Neurosci. 2008. [Google Scholar] [CrossRef] [PubMed]
- Choi, W.S.; Murthy, G.G.K.; Edwards, D.A.; Langer, R.; Klibanov, A.M. Inhalation Delivery of Proteins from Ethanol Suspensions. Proc. Natl. Acad. Sci. USA 2001, 98, 11103–11107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bavis, R.W.; Johnson, R.A.; Ording, K.M.; Otis, J.P.; Mitchell, G.S. Respiratory Plasticity after Perinatal Hypercapnia in Rats. Respir. Physiol. Neurobiol. 2006, 153, 78–91. [Google Scholar] [CrossRef]
- Gifford, A.N.; Espaillat, M.P.; Gatley, S.J. Biodistribution of Radiolabeled Ethanol in Rodents. Drug Metab. Dispos. 2008, 36, 1853–1858. [Google Scholar] [CrossRef] [Green Version]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castro-Balado, A.; Mondelo-García, C.; Barbosa-Pereira, L.; Varela-Rey, I.; Novo-Veleiro, I.; Vázquez-Agra, N.; Antúnez-López, J.R.; Bandín-Vilar, E.J.; Sendón-García, R.; Busto-Iglesias, M.; et al. Development and Characterization of Inhaled Ethanol as a Novel Pharmacological Strategy Currently Evaluated in a Phase II Clinical Trial for Early-Stage SARS-CoV-2 Infection. Pharmaceutics 2021, 13, 342. https://doi.org/10.3390/pharmaceutics13030342
Castro-Balado A, Mondelo-García C, Barbosa-Pereira L, Varela-Rey I, Novo-Veleiro I, Vázquez-Agra N, Antúnez-López JR, Bandín-Vilar EJ, Sendón-García R, Busto-Iglesias M, et al. Development and Characterization of Inhaled Ethanol as a Novel Pharmacological Strategy Currently Evaluated in a Phase II Clinical Trial for Early-Stage SARS-CoV-2 Infection. Pharmaceutics. 2021; 13(3):342. https://doi.org/10.3390/pharmaceutics13030342
Chicago/Turabian StyleCastro-Balado, Ana, Cristina Mondelo-García, Letricia Barbosa-Pereira, Iria Varela-Rey, Ignacio Novo-Veleiro, Néstor Vázquez-Agra, José Ramón Antúnez-López, Enrique José Bandín-Vilar, Raquel Sendón-García, Manuel Busto-Iglesias, and et al. 2021. "Development and Characterization of Inhaled Ethanol as a Novel Pharmacological Strategy Currently Evaluated in a Phase II Clinical Trial for Early-Stage SARS-CoV-2 Infection" Pharmaceutics 13, no. 3: 342. https://doi.org/10.3390/pharmaceutics13030342