1. Introduction
Changes in the formulation composition, as well as in the batch manufacturing process, equipment, and site, are commonplace during various stages of drug development or after its regulatory approval. If one or more of these changes occur, in vivo bioequivalence (BE) studies in humans are required, increasing the development costs and time to market. An established in vitro–in vivo correlation (IVIVC) could be used to support biowaivers, thereby largely reducing the regulatory burden, leading to time and cost savings [
1,
2].
IVIVC has been defined by the U.S. Food and Drug Administration (FDA) as a predictive mathematical model describing the relationship between an in vitro property of a dosage form (e.g., drug dissolution or release profile) and its in vivo response (e.g., concentration–time profile) [
3]. IVIVC can be categorized into five different levels: Levels A, B, C, D, and multiple C. The Level A IVIVC, defined as a point-to-point relationship between the in vitro and in vivo profiles of at least three formulations or batches characterized by different release rates, is considered the most informative and is required to obtain a biowaiver. Indeed, through the successful development and application of an adequate Level A IVIVC, the in vivo plasma concentration of a drug can be predicted from the in vitro release data that can be used as a surrogate for the in vivo bioequivalence assessment.
In 1997, the FDA published a regulatory guidance related to the development, evaluation, and applications of IVIVC for extended-release (ER) oral dosage forms [
3]. This guideline, in agreement with most of the older literature, presented the so-called deconvolution- and convolution-based methods as the standard IVIVC technique [
4,
5], although the development of alternative approaches was encouraged. Since then, the establishment and application of IVIVC have increased and various alternatives to the conventional IVIVC approaches have been introduced [
2,
6,
7,
8]. In few but extremely relevant examples, the IVIVC was developed using nonlinear mixed-effect models [
9] or physiologically based pharmacokinetic (PBPK) models [
10,
11,
12], in the latter cases frequently implemented in closed software such as GastroPlus
TM. However, from a recent screenshot of the IVIVC approaches applied to the ER oral drug, it clearly emerged that, even with their promising potential and advantages, the use of these mathematical methods still requires consolidation and harmonization [
7].
If no established consensus about approaches to implement an IVIVC for ER oral drugs has been reached, methodologies for ER nonoral dosage forms (e.g., parenteral microspheres and implants, ophthalmic compound, intra-muscular suspensions, as well as transdermal and vaginal products) are still at the very early stages of development [
2,
13]. To date, there is no regulatory IVIVC guidance for ER nonoral products, and only few study reports are present in the literature. In these examples, the same principles to develop an IVIVC for ER oral products [
3] have been applied to dosage forms and the route of administration other than oral [
14,
15,
16].
The vagina is a promising site of systemic and local drug delivery and represents an interesting administration route for compounds with poor oral bioavailability [
17,
18,
19,
20]. Between the different types of vaginal drug delivery systems currently available on the market [
21,
22,
23,
24], intravaginal rings (IVRs) offer the possibility of a continuous and controlled drug release over an extended time period of several weeks. IVRs are generally used for the steroid administration in hormone replacement therapy or birth control, but more recently, they have witnessed a surge of new interest in the context of the HIV-prevention strategies [
25]. Even with the increasing number of marketed products and the numerous IVR formulations that are currently in development, no regulatory guidance on the release tests or IVIVC assessment for vaginal rings are available in the United States, Europe, or Japan. This lack of established guidance and standard procedures makes the development of IVIVC for IVRs, already complex due to the unique anatomy and physiology of the vagina, even more challenging.
In this context, the aim of the present work was to establish a Level A IVIVC between the in vitro release of progesterone vaginal rings (PVRs) and the corresponding serum concentration profiles observed during clinical studies. The proposed IVIVC model was defined through a direct differential equation-based model that, together with the adoption of a nonlinear mixed-effect approach, allowed us to handle the complex dynamics and the variability affecting the in vivo vaginal absorption. The internal and external predictability of the model was carefully evaluated following the recommendations for the Level A IVIVC assessment reported in the regulatory guidance for ER oral drugs [
3]. The established IVIVC model resulted in the ability to correctly predict the in vivo concentration–time profiles of PVRs from their respective in vitro release profiles, allowing the use of the in vitro testing as a surrogate for bioequivalence studies testing any new PVR batches (scale-up or post-approval changes). Finally, the possible use of the developed population IVIVC model as a simulator of virtual bioequivalence trials was investigated through a case study. To this aim, estimates of the model-expected in vivo relative bioavailability of two tested PVR batches were reported.
4. Discussion
Methodologies for the development and evaluation of IVIVC models are an active area of investigation and a variety of approaches with different degrees of complexity are possible and potentially acceptable. IVIVC principles have been mostly applied to oral products and, in 1997, a specific guidance for ER oral drugs was been established by regulatory authorities [
3]. However, due to the continuous pharmaceutical advancements on drug formulation and administration device, there exists a need to develop methodologies and standards for the development of an IVIVC model of nonoral delivery systems, for which no regulatory guidelines and only sparse literature examples are currently available [
13].
The objective of this work was the development of a mathematical model able to establish an adequate Level A IVIVC between the in vitro release of PVRs and the corresponding serum concentration profiles in humans. A direct, differential-equation-based method and a nonlinear-mixed-effect approach were adopted to develop the IVIVC P-ring model following the same principles generally used to define an IVIVC for ER oral dosage forms [
3].
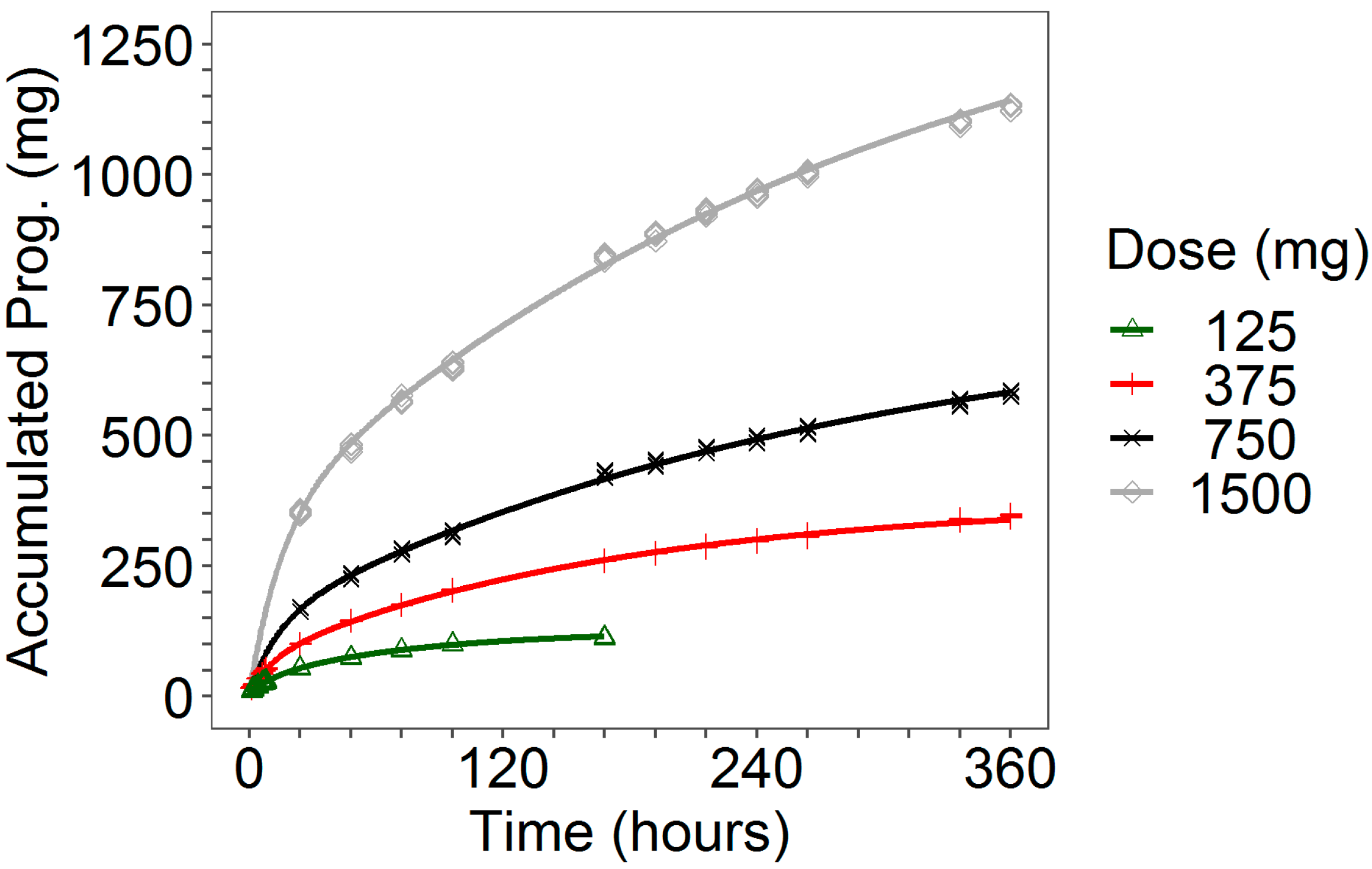
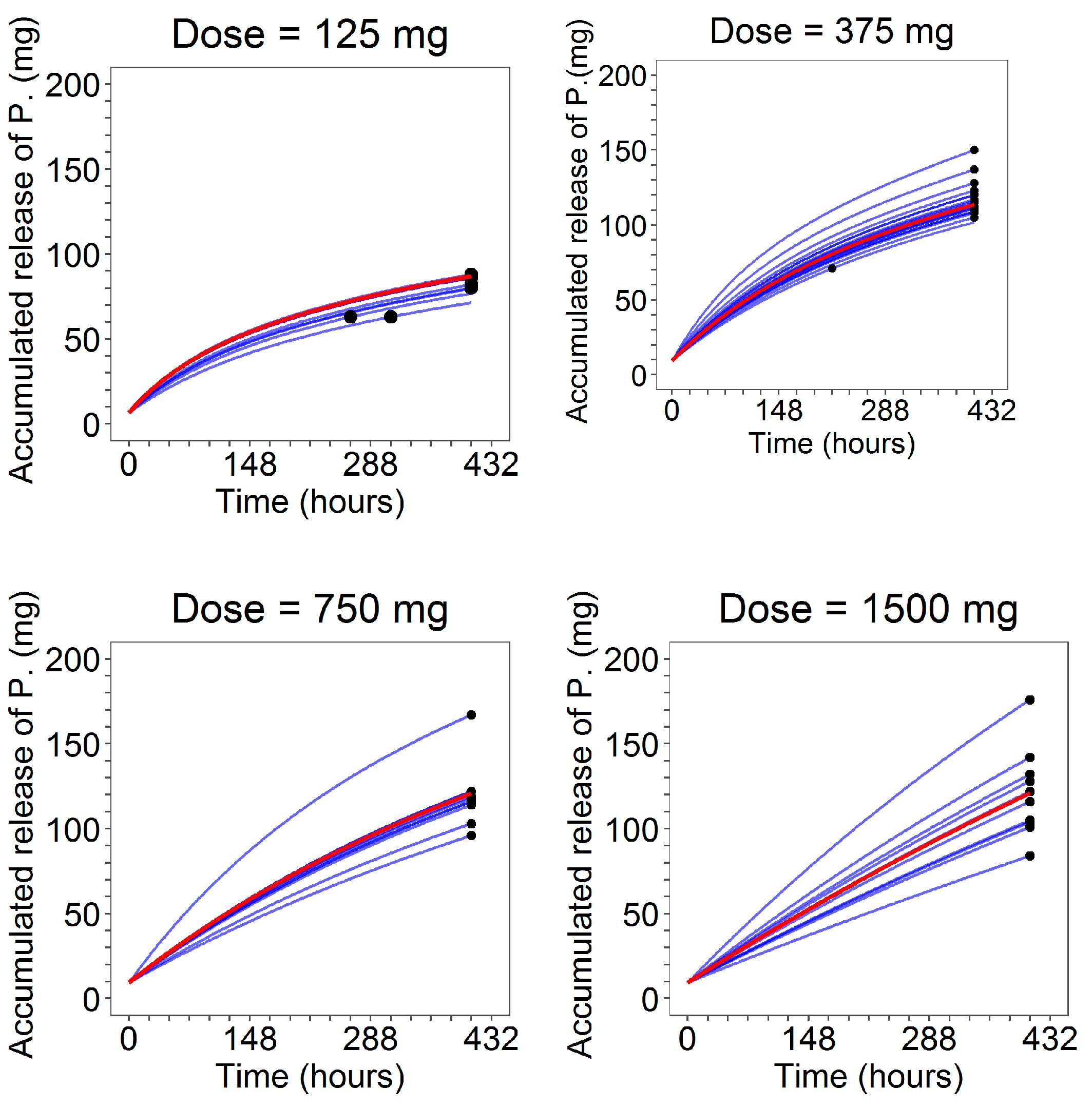
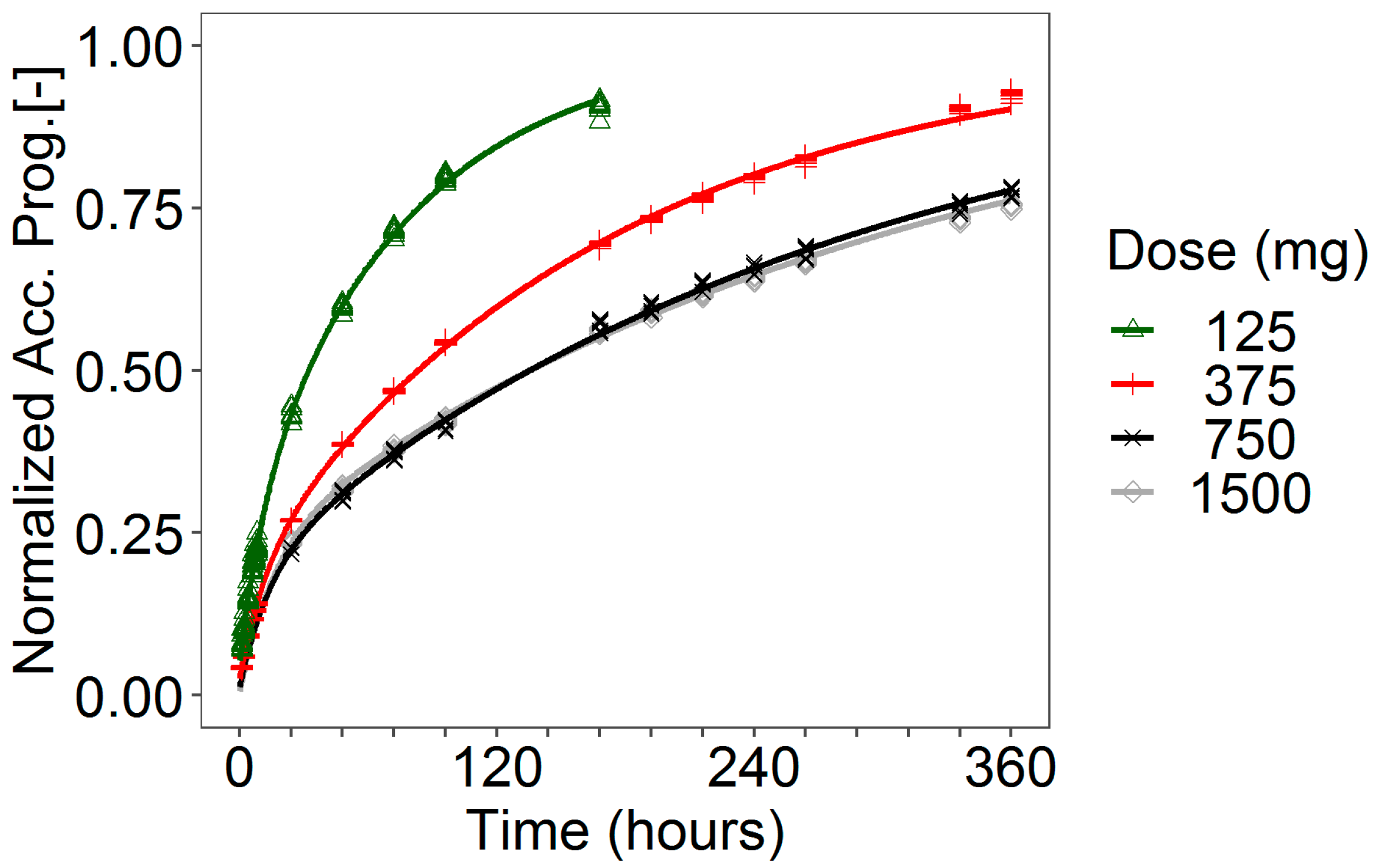
More in detail, in this study, different in vitro release rates obtained at 125, 375, 750 and 1500 mg dose levels were considered. At each dose level, the observed release profiles from the progesterone rings exhibited bi-exponential decays that overlapped almost perfectly. Hence, within each dose level, the individual in vitro release time courses were pooled together and modeled without taking into account inter-ring variability. An initial burst phase was observed in the release profile of the two lower dose levels (125 and 375 mg) for which early sampling timepoints were available. This immediate faster release is due to the progesterone at or near the surface of the matrix ring that has a relatively small diffusional pathway to overcome in order to be released [
28]. The parameter P
0 of the in vitro model was introduced to provide an estimate of this quantity. However, at the higher dose levels (750 and 1500 mg), the lack of observations in the first 24 h hampered the estimation of P
0 that was then fixed to the 375 mg dose value without significantly affecting the quality of the GOFs.
A lack of dose proportionality was observed in the in vitro progesterone release, as it is evident from the release rates computed by Higughi’s formula (see
Table 1) and from the dose-normalized in vitro profiles (
Figure A5 of
Appendix A). This is likely due to the progesterone diffusion process across the ring. Mathematical models accounting for the diffusion step, as well as for the other mechanistic processes affecting the progesterone delivery from the ring, are available in the literature [
29,
30,
31,
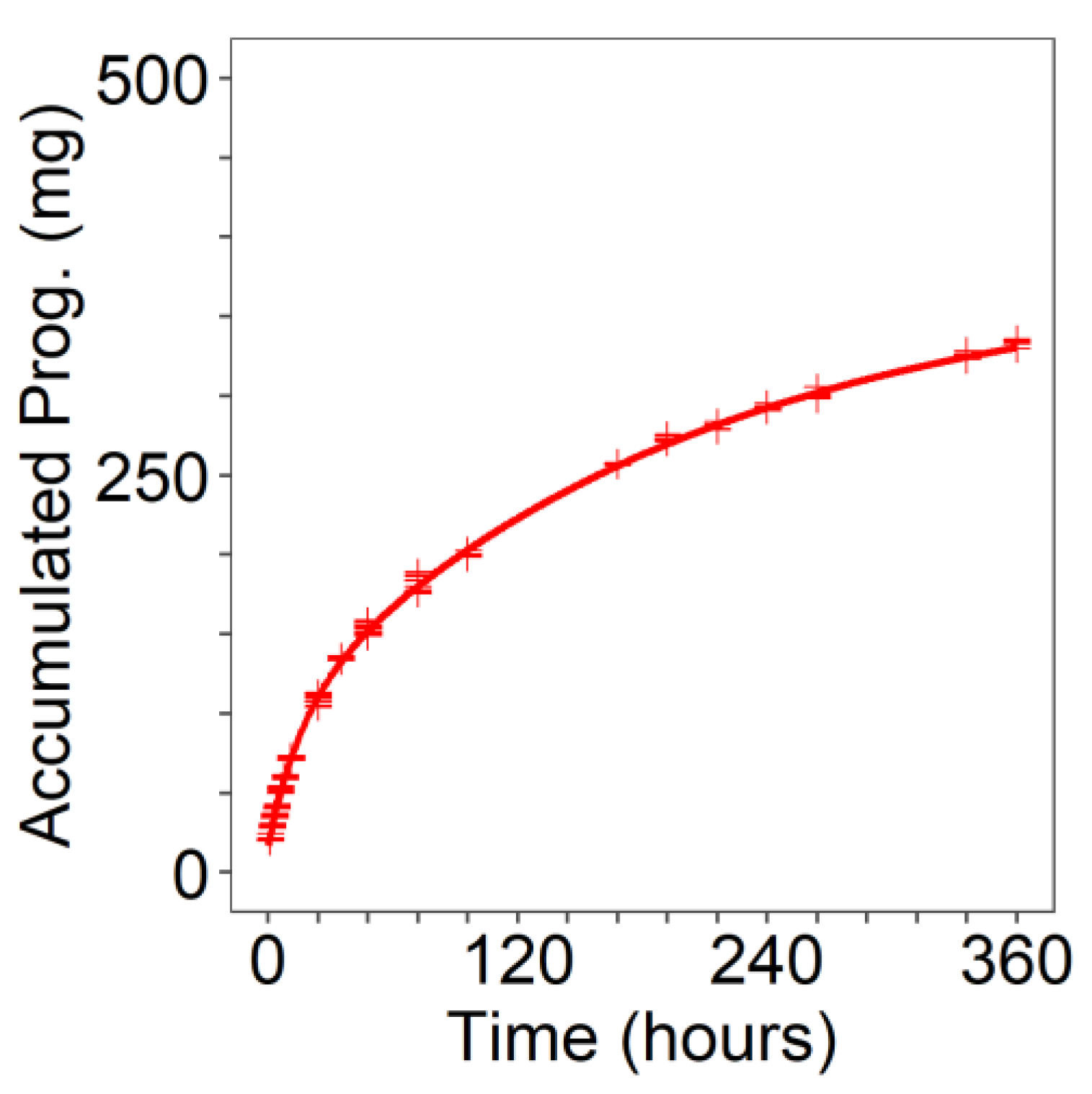
32]. However, because of the scope of this work, the modeling efforts were focused on obtaining a simple progesterone release function,
to subsequently use as input rate for the PK model. Despite its empirical structure, the selected bi-exponential model (Equation (1)) was able to capture almost perfectly the in vitro release data (
Table 5,
Figure 3 and
Figure 4).
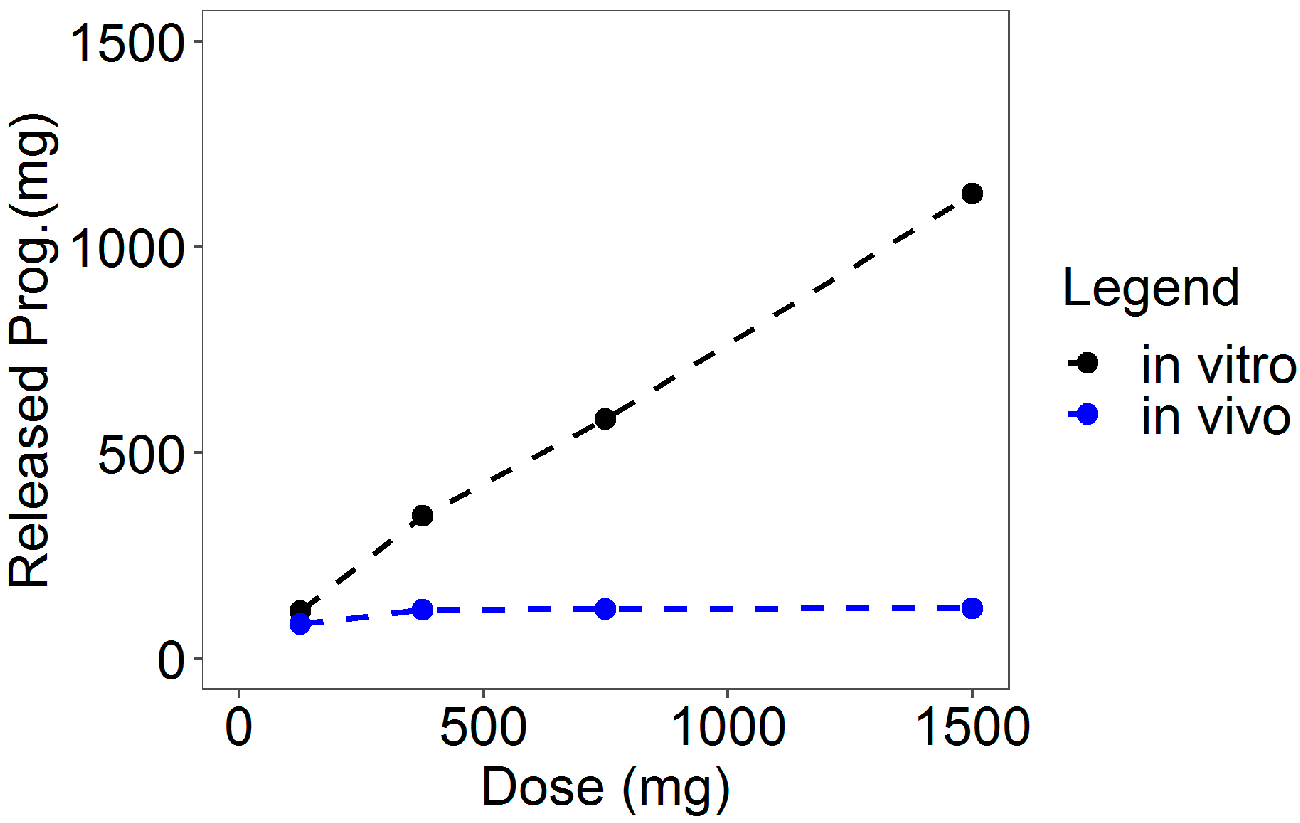
A comparison of the in vitro and the in vivo cumulative release at the end of the experiments gave evidence of a decreased in vivo release rate compared to that in vitro (see
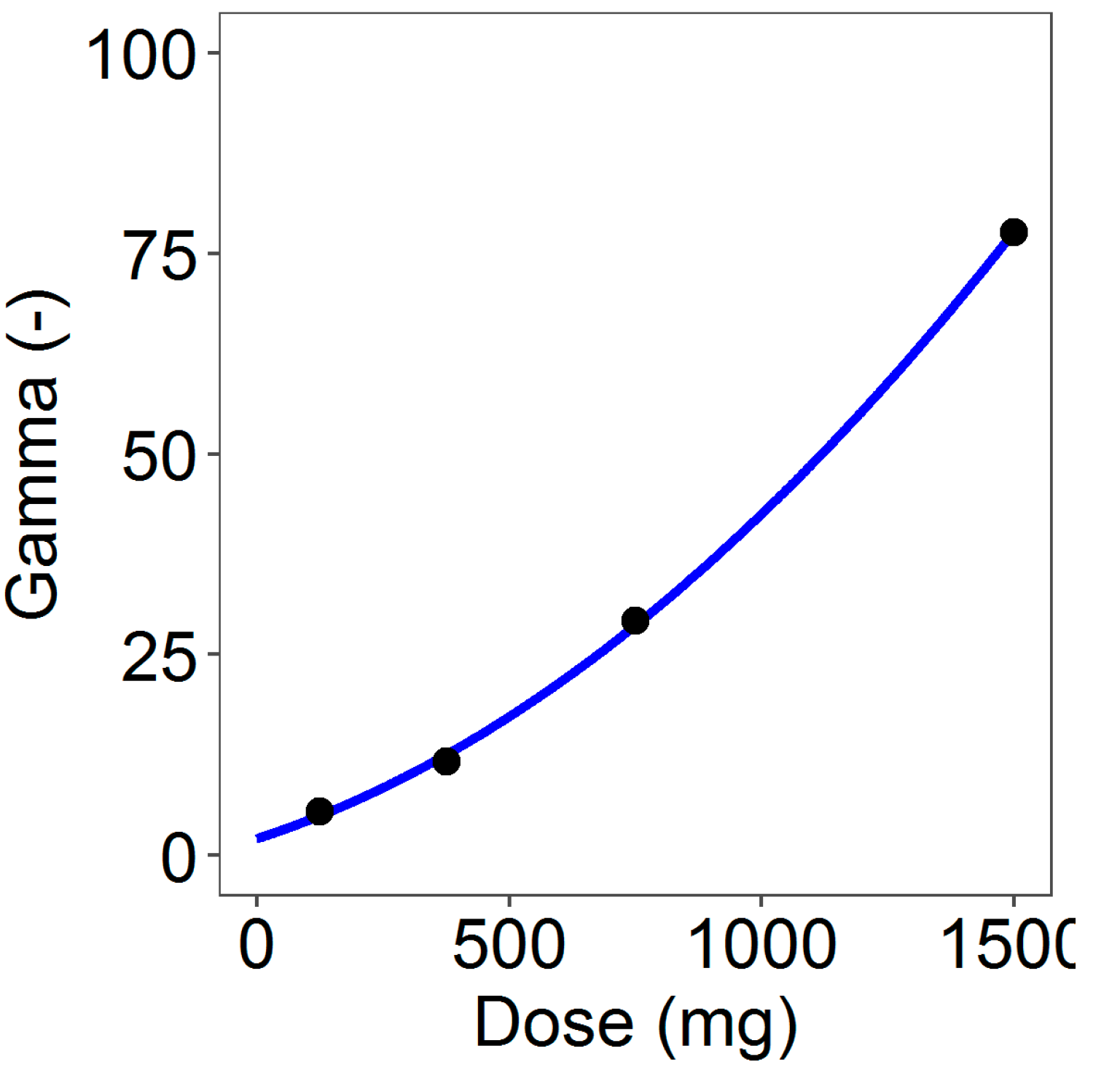
Table 3). In addition, the total amount of the in vivo released progesterone within the observation period resulted similarly for the three higher dose rings irrespective of the amount charged in the ring. This was caused by the inhibition of the progesterone release due to the vaginal fluid saturation. Indeed, in vivo, the progesterone has to be released from the ring into the vaginal fluids from which it has to be absorbed through the vaginal epithelium. As the daily production of vaginal fluids is approximately 6 mL/day with a constant volume of 0.5–075 mL and the progesterone solubility is very low [
20,
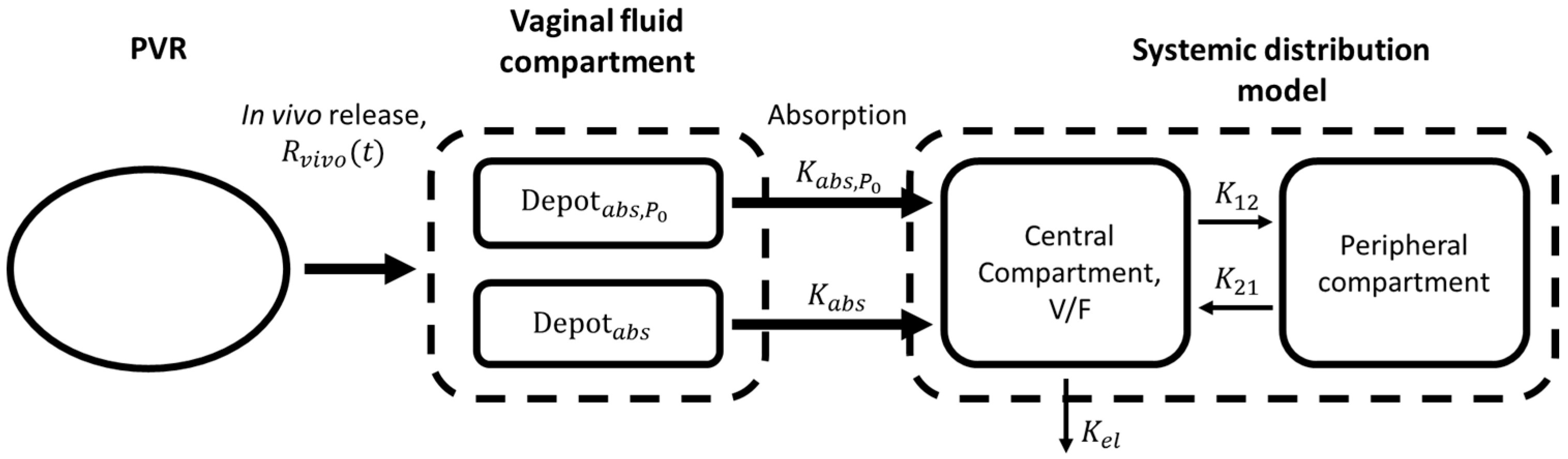
33], the system is saturated and progesterone solubility results in the rate-controlling mechanism. Drug saturation of vaginal fluids was reached and maintained already with the 375 mg rings, and then no further significant release and absorption was reached by increasing the progesterone in the rings. This inhibition was modeled in the in vivo release model by a suitable inhibition function driven by a dose-dependent in vitro–in vivo factor γ acting on the exponential release rates of the in vitro model. Thus, the in vivo release in input to the PK model was obtained by combining the in vitro release model (for any specific dose) with the inhibition function governed by the parameter γ.
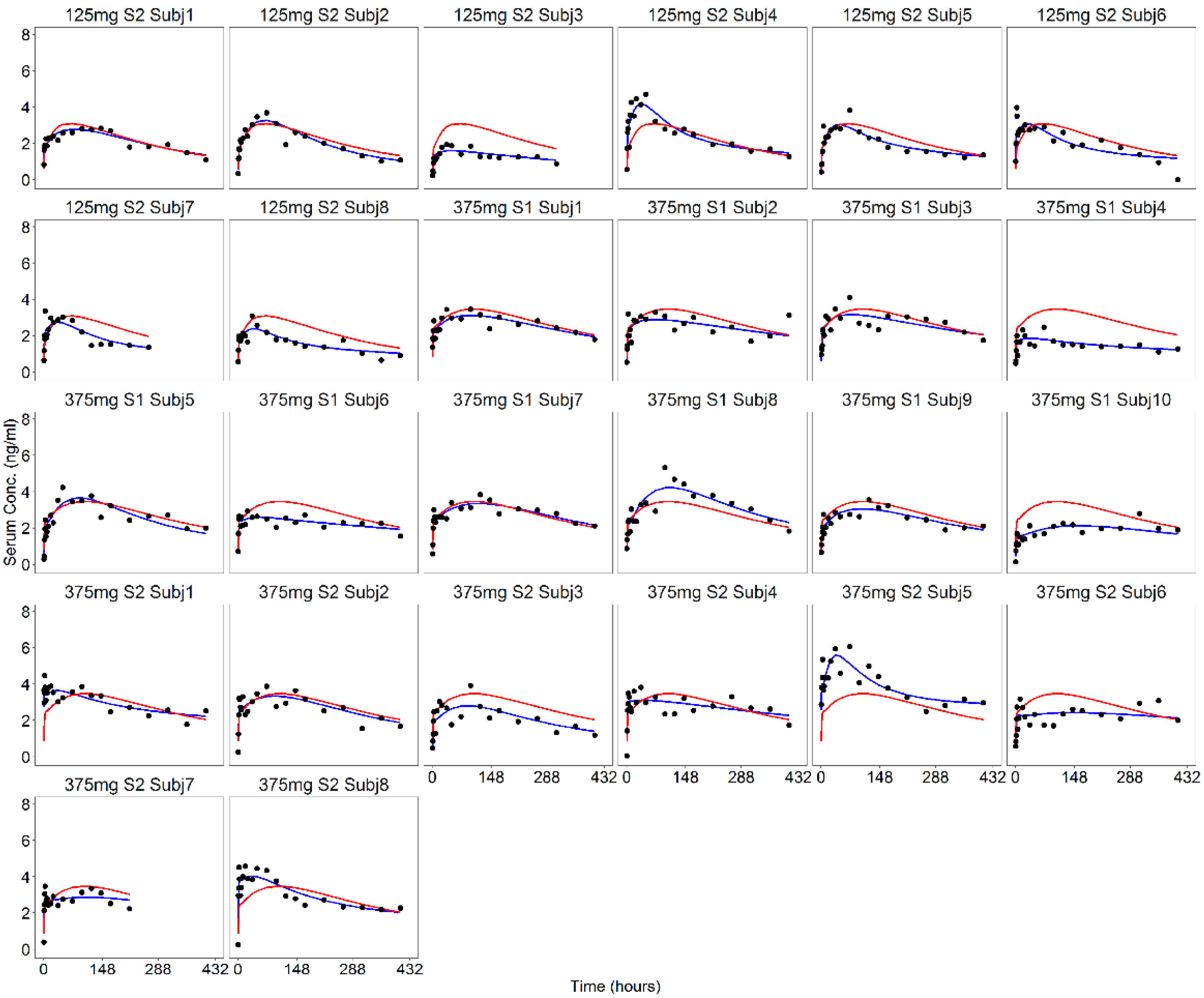
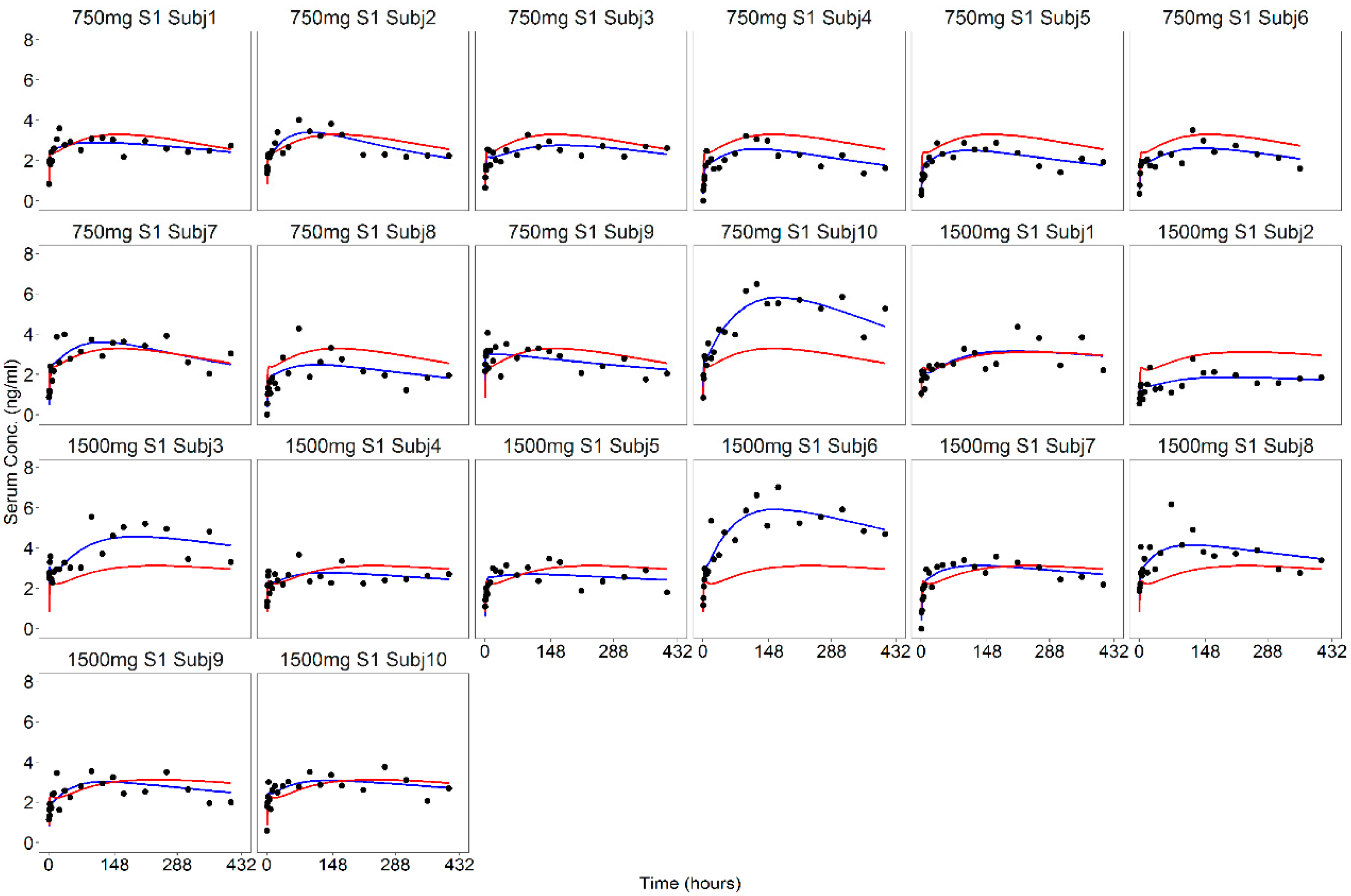
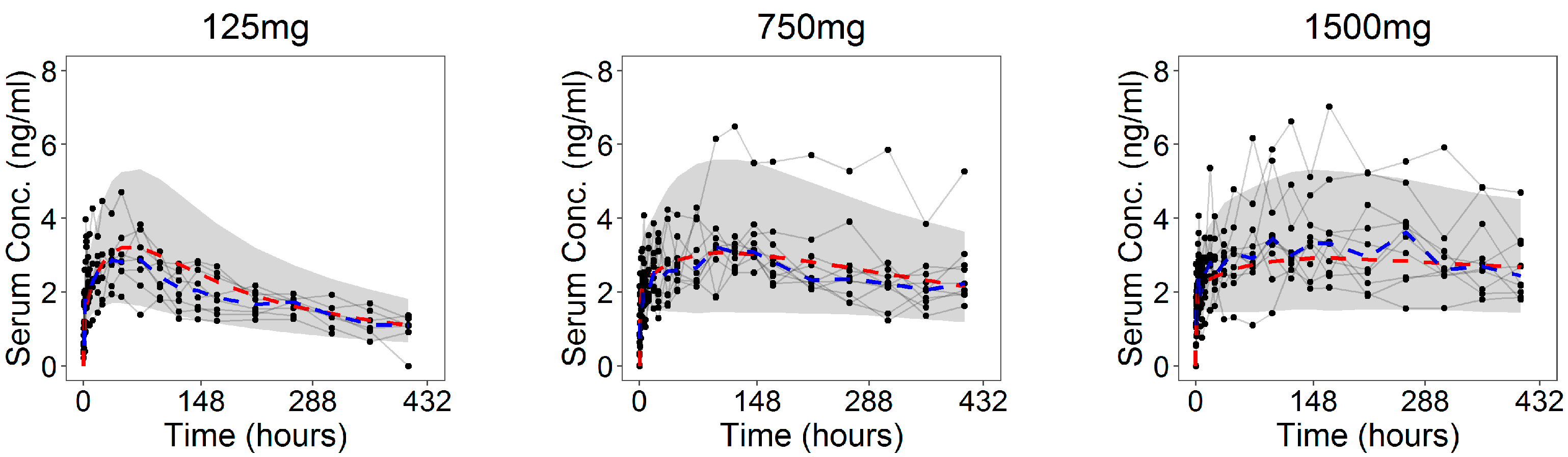
The PK model incorporated two absorption mechanisms, one (
) for the immediate progesterone release and the other (
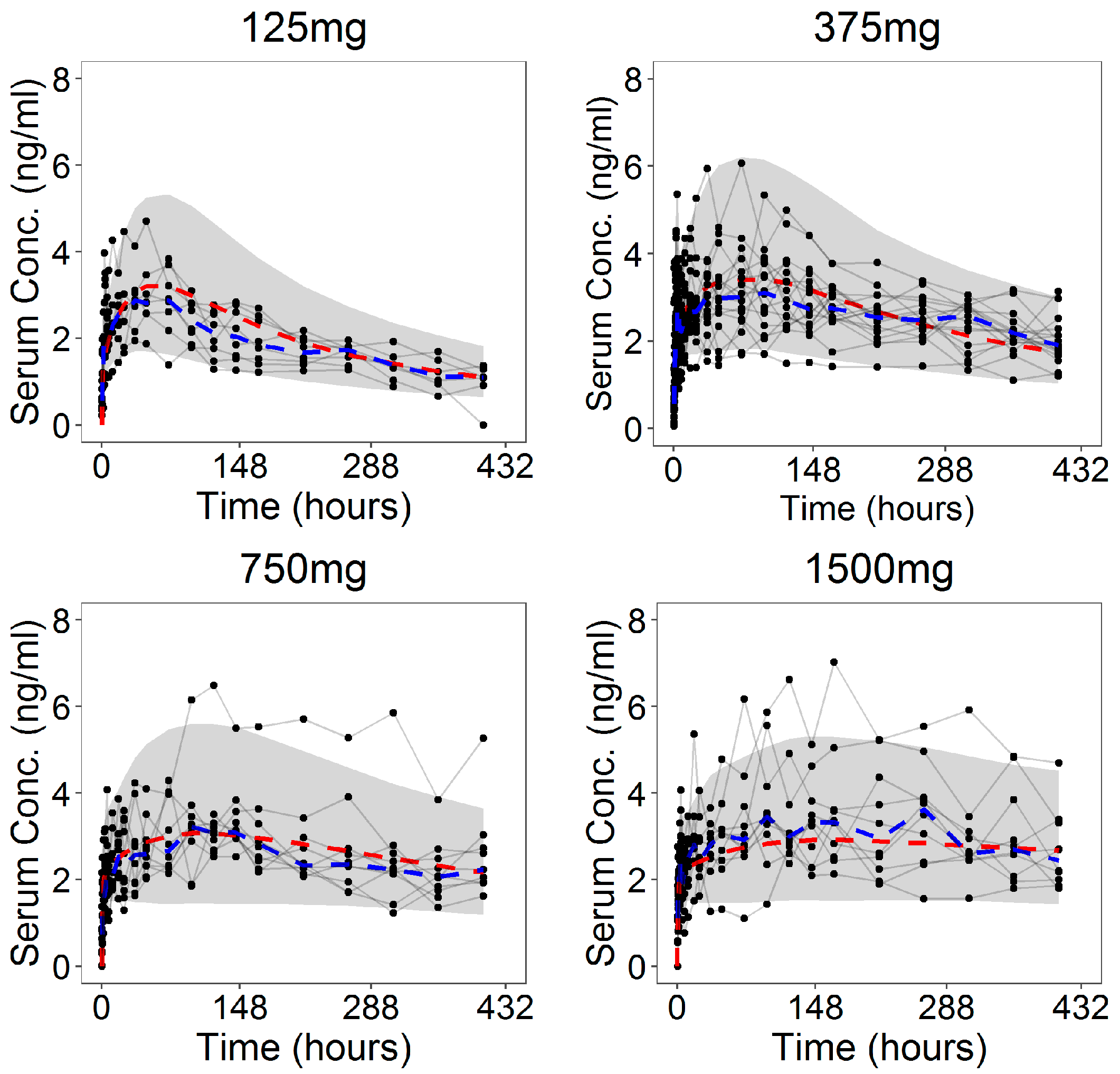
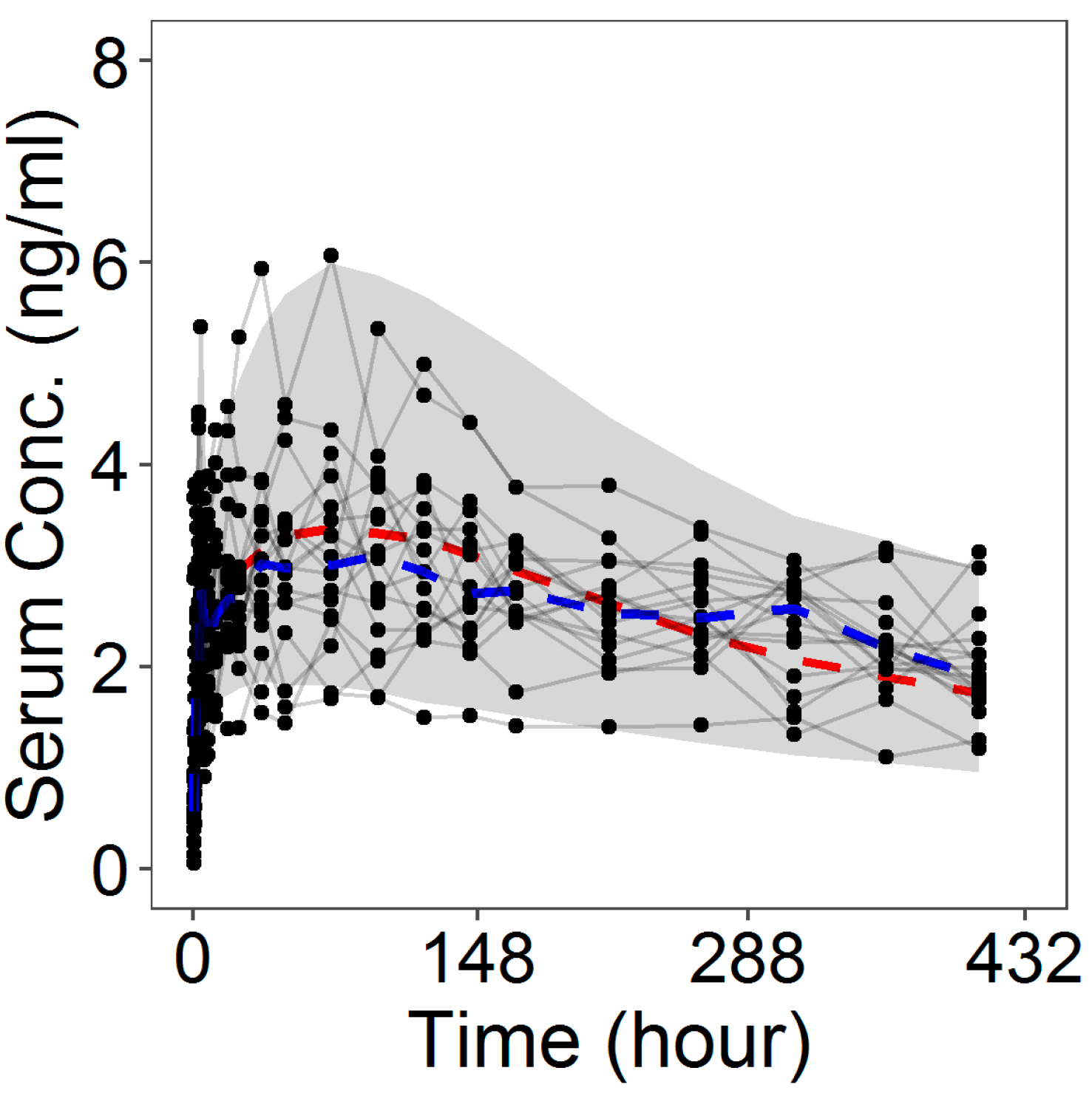
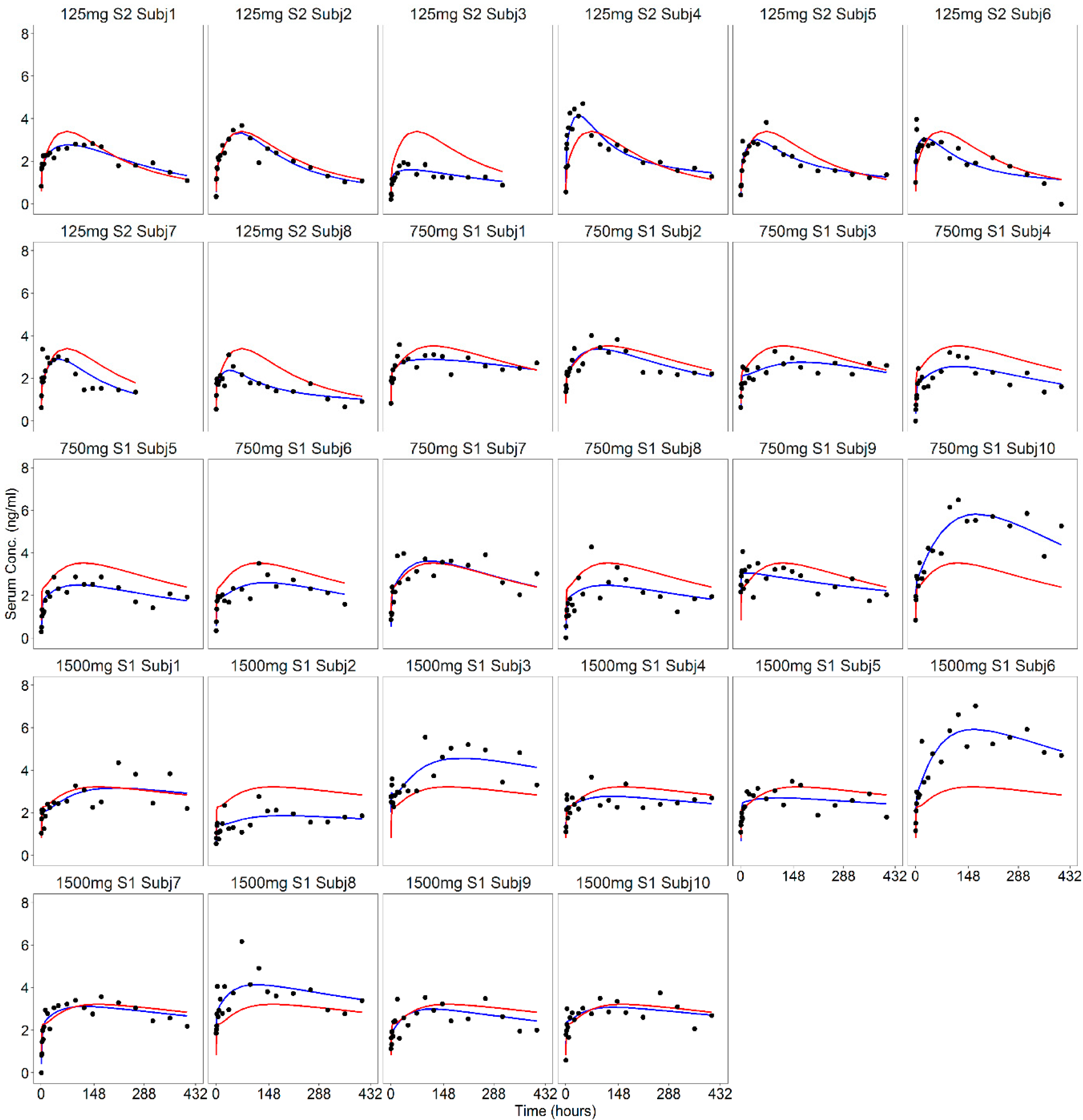
) for the remaining part of the release. A two-compartment model was assumed for progesterone kinetics in serum. Unlike from the in vitro data, the serum progesterone levels showed different profiles among the subjects with a significant intra- and inter-individual variability. These findings were in agreement with the PK variability reported for the drug administered through the vaginal route and represented an intrinsic characteristic and limitation of this type of administration [
28]. Indeed, several physiological factors, such as changes in the epithelial thickness, alteration of the volume and pH of the vaginal fluids, can potentially affect progesterone release from the ring and alter its absorption rate [
20,
28,
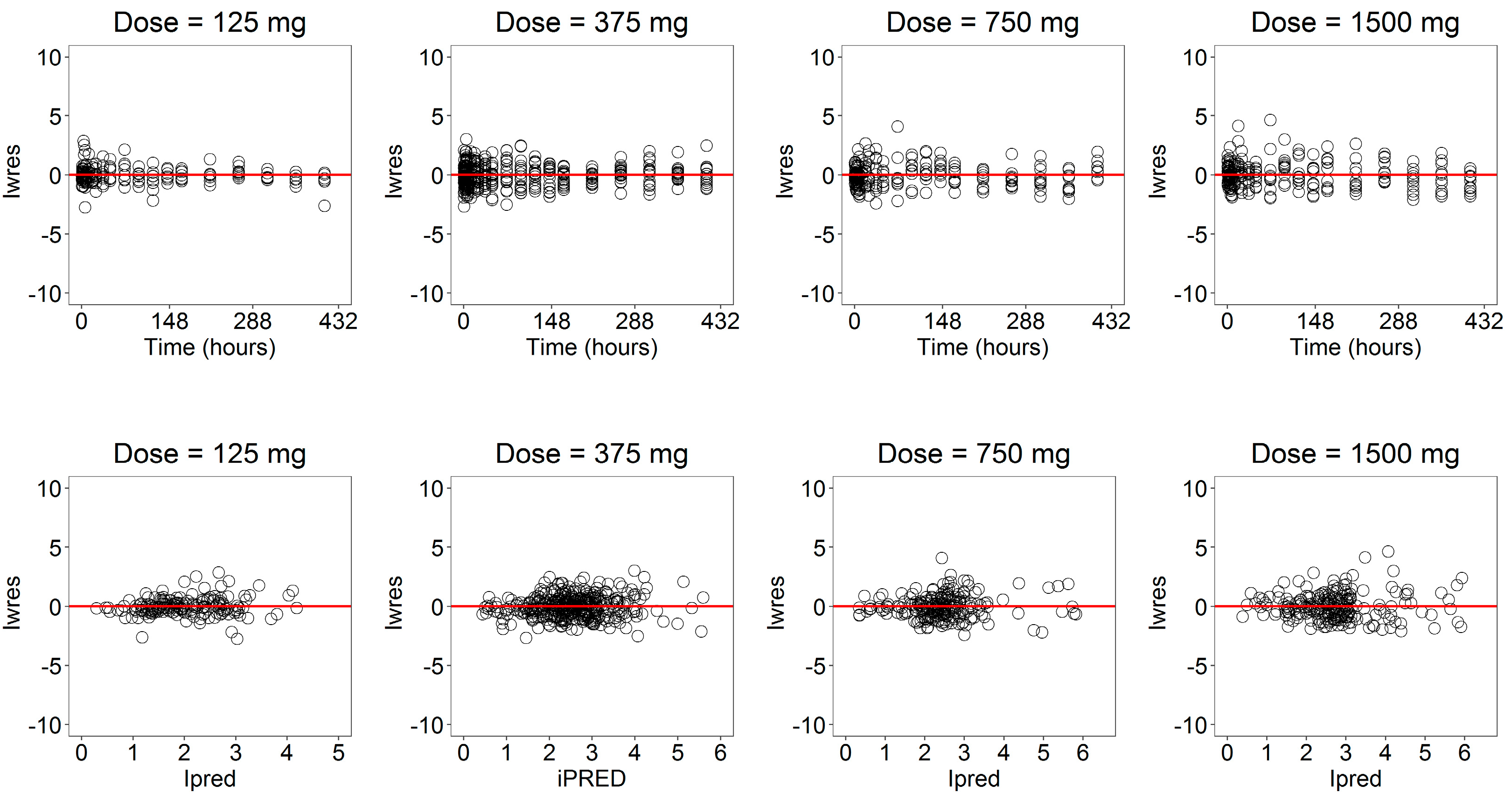
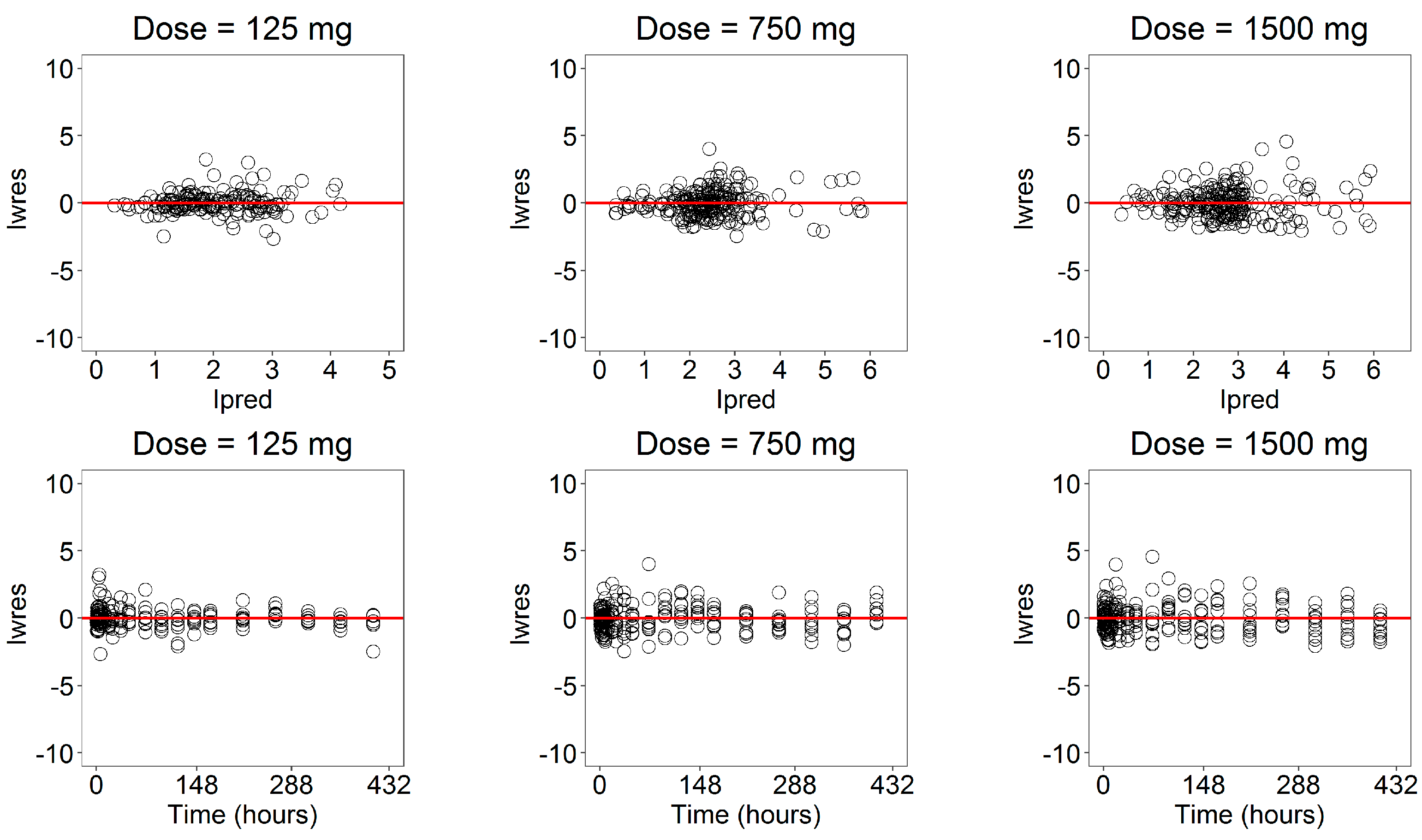
34]. A population (nonlinear-mixed effect) approach was used to account for this relevant in vivo variability. The simultaneous fitting of the in vivo parameters yielded very satisfactory results at all doses in terms of both residuals and visual predictive checks.
Even if progesterone is characterized by a nonnarrow therapeutic index, in accordance with the more restricting FDA recommendations [
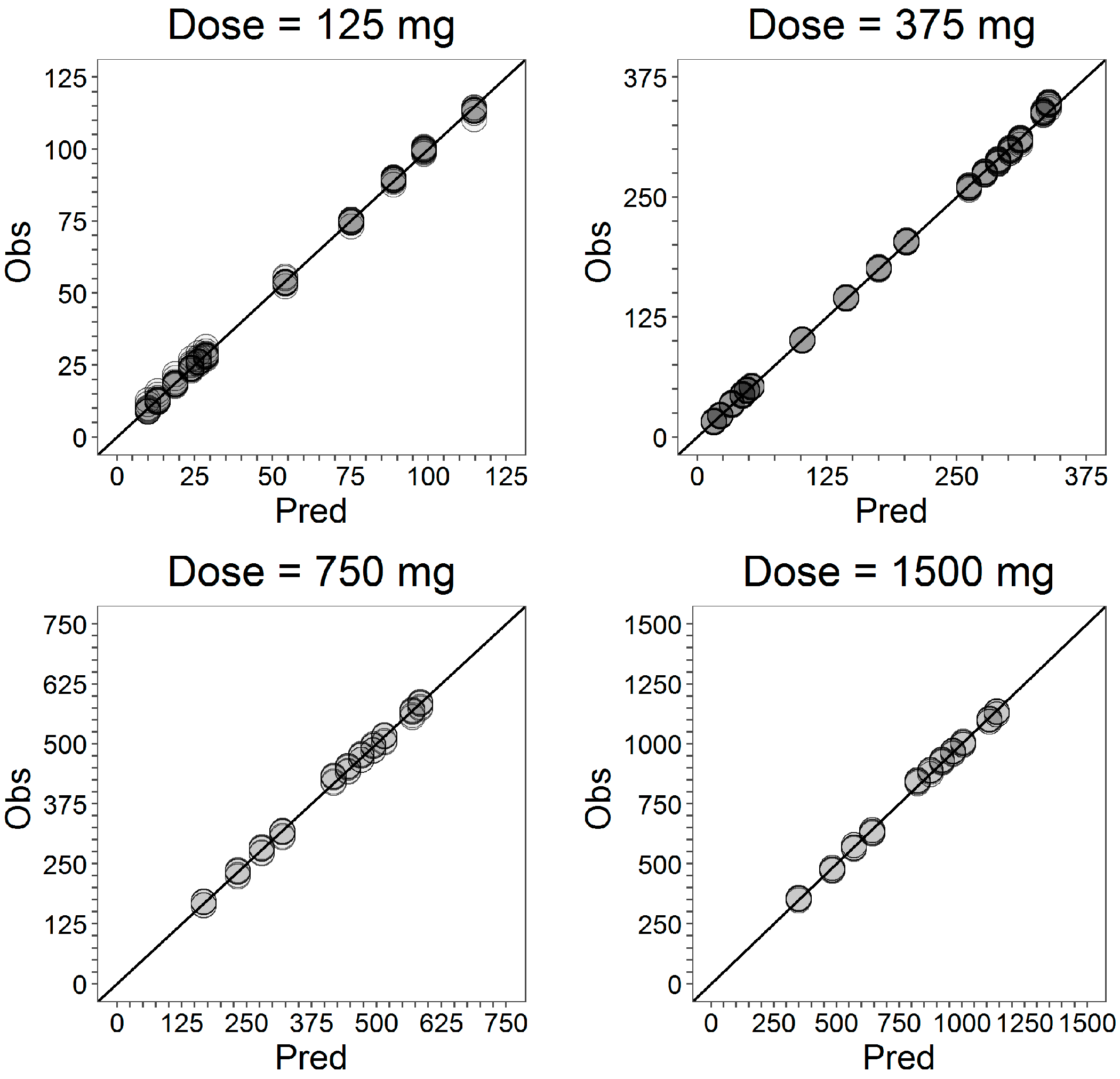
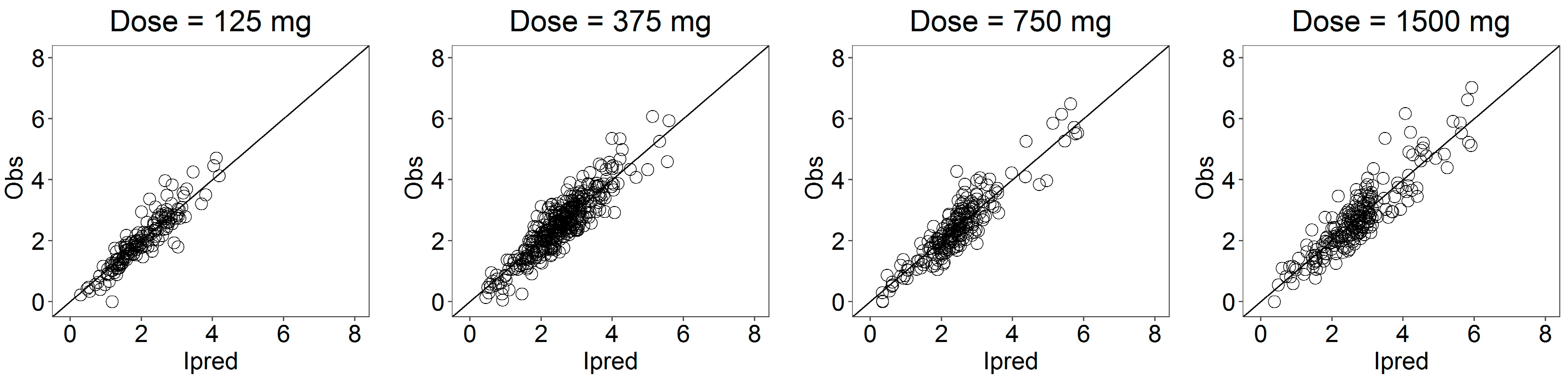
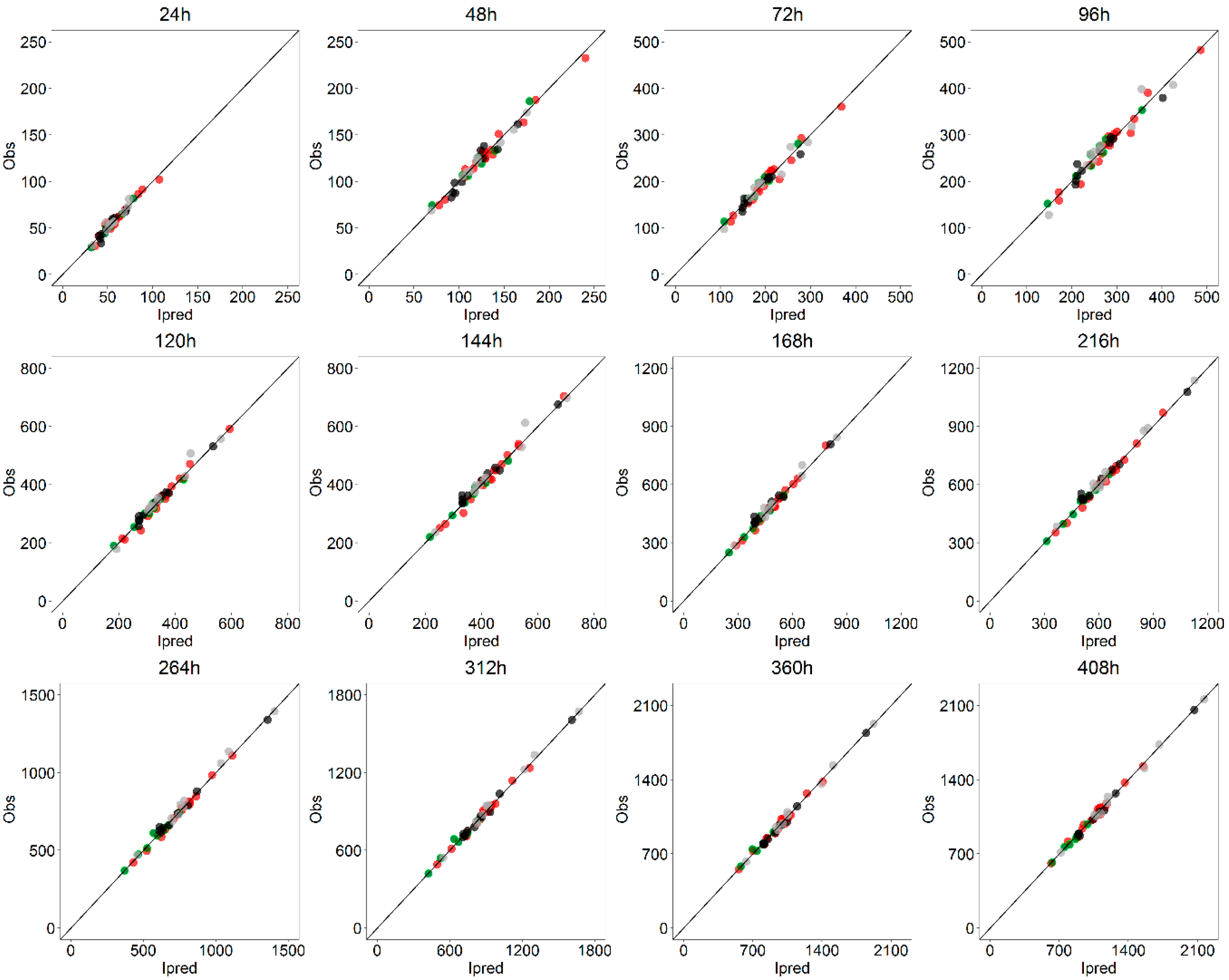
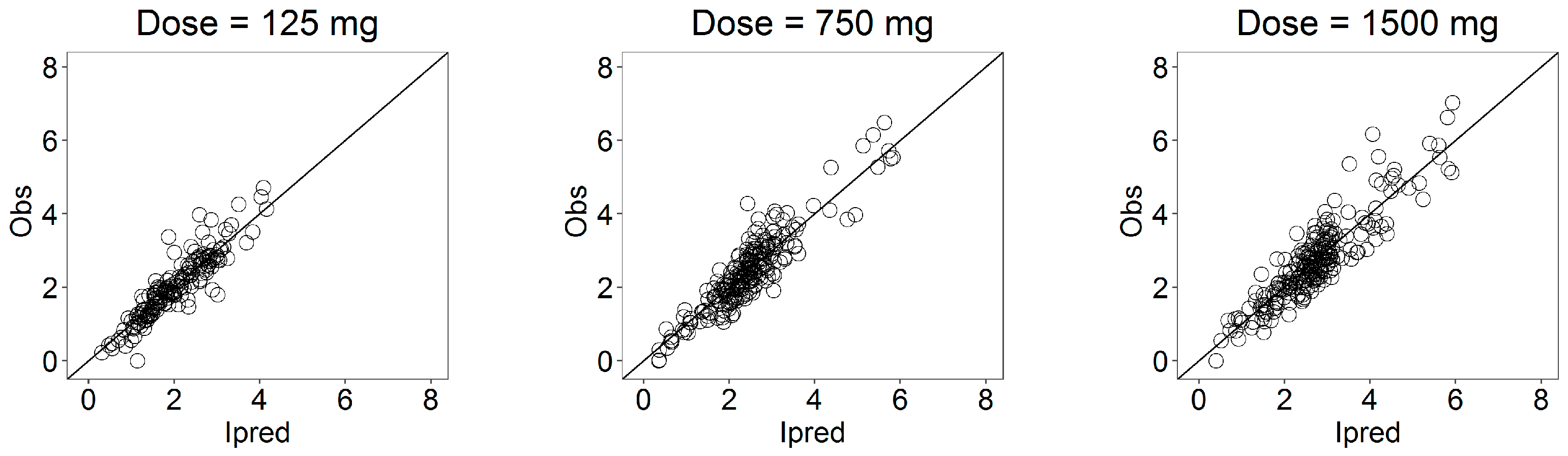
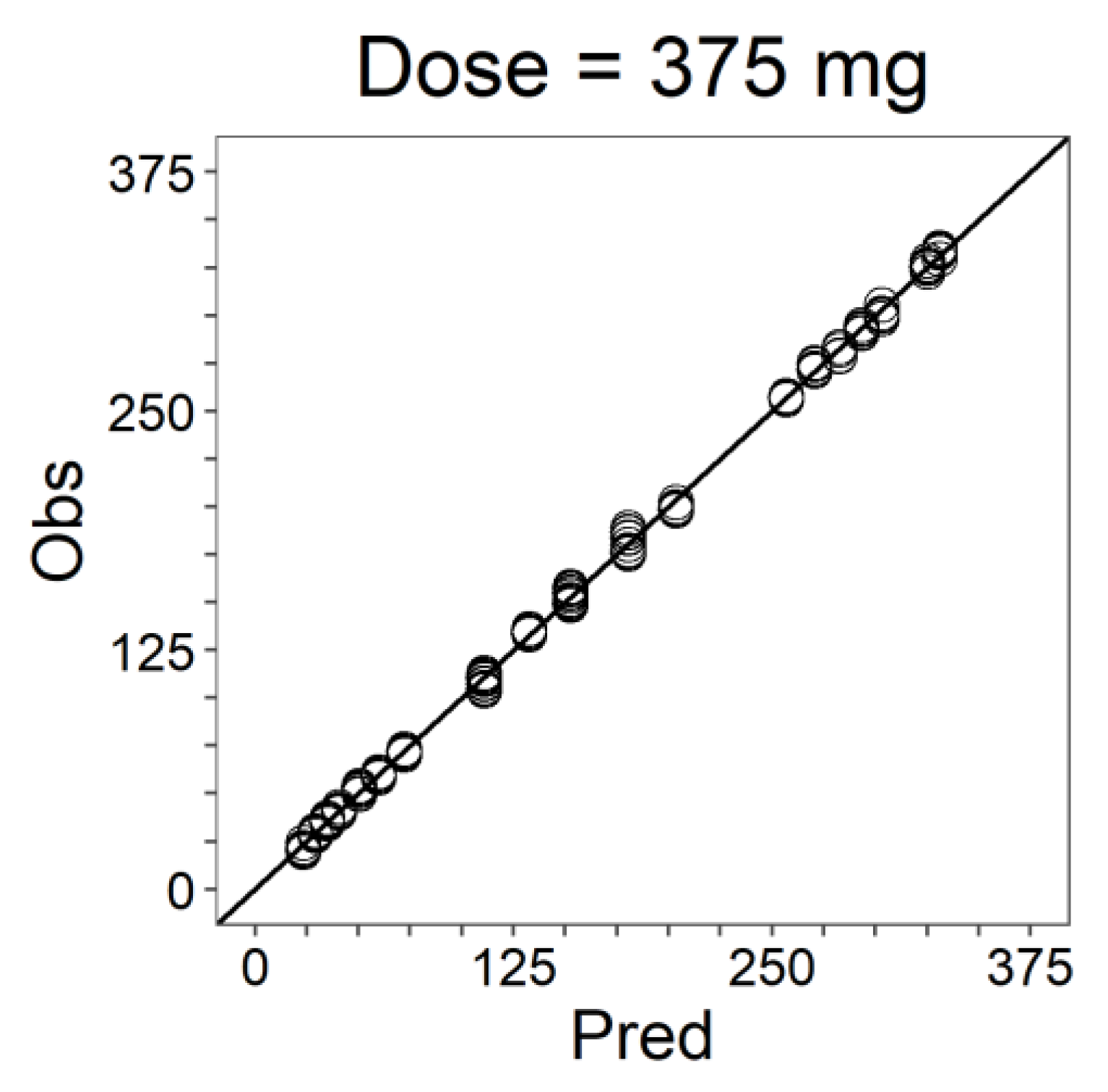
3], both the internal and external predictability of the IVIVC P-ring model were evaluated. First, the internal validity of the model was confirmed by GOF comparing the predicted and observed curves and the very low PE on AUCs. At any sampling time, the average (across all subjects and doses) PE on AUC(0-t) was less than 5% (
Table 8). At the latest times (t ≥ 144 h), the individual PE for each dose was less than 3%. A higher error was observed for
Cmax whose PE on average was 16.4% (
Table 9). This was somehow expected in view of the marked variability in the individual serum profiles, with observed T
max values in the range of 3–408 h. Such a
Cmax PE below 20% was taken as satisfactory even if the FDA guideline for ER oral drugs suggests an average PE lower than 10% with 15% as a maximum bound for individual PEs. In fact, it has to be considered that this kind of formulation is somehow atypical with respect to guidelines for oral administration and that progesterone is a nonnarrow therapeutic index drug. To further confirm the predictive capability of the model, an external validation was set-up. The data relative to batch
B at dose 375 mg were left apart as a test dataset, and the population IVIVC P-ring model was re-estimated using only data at doses 125, 750 and 1500 mg (ring batches A, C and D). Then, using the in vitro model derived from the 375 mg data, the obtained population model was used to simulate the serum profile of 500 distinct individuals. Validation was performed by means of external VPCs and the PE on the average AUC(0-t) and
Cmax. In particular, all the subjects fell within the 90% predicted intervals of the VPCs, and the PE on AUCs and
Cmax were all below 10%. Based on the previous results and observations, the proposed IVIVC P-ring model was considered meeting all the FDA validation criteria and can be used to support in vivo bioequivalence studies.
Adequately predicting the in vivo performances from in vitro release data for vaginal drug delivery systems, such us PVRs, is extremely challenging due to a multitude of factors including the vaginal physiology, the complex dynamics of vaginal absorption, the significant inter-individual variability of the PK, the absence of compendial apparatus and methods for the in vitro release testing [
28], as well as the inability of directly measuring the in vivo release in the vagina during the whole study period. For this reason, as in the majority of IVIVC applications, the progesterone serum concentration–time profiles were used as surrogates to reflect the in vivo drug release. Here, in addition to the serum concentration levels, the total amounts of released progesterone at the end of the study were available, providing a fundamental piece of information for the complete definition of the proposed IVIVC P-ring model. First, similar amounts of progesterone remaining in the rings in the in vivo experiments at the three higher doses (375, 750 and 1500 mg) suggested the consideration that the absence of dose-proportionality observed in the corresponding serum progesterone exposures could be essentially due to factors inhibiting the in vivo release (like solubility in the vagina). Secondly, they allowed the successful identification of the in vitro–in vivo inhibition release model. Finally, although for practical reasons, the data on the in vivo-released amount of progesterone were available only at the end of the trials, the goodness of the fittings suggested the exclusion of the presence of important transient nonlinear behaviors.
Another issue that further increased the challenging IVIVC development was the in vitro release system adopted for PVRs that was only partially physiological. Indeed, in aqueous systems (or vaginal fluids), the in vitro progesterone release from rings loaded with 375, 750 and 1500 mg was identical and corresponds to the saturation of the receiving medium. Therefore, for quality control, it was needed to include surfactants that increased the progesterone solubility in the receiving medium and allowed us to discriminate releases from rings charged with different progesterone amounts. The establishment of an IVIVC based on a nonfully physiological in vitro release system represents an important achievement of this modeling exercise.
Finally, a case study, exemplifying the possible use of the developed IVIVC P-ring model to the BE assessment of any new batch of progesterone rings, is proposed here. A new batch of vaginal rings (batch E) charged with 375 mg of progesterone was available. Batches B and E were expected to be bioequivalent and were considered as the reference and test batch, respectively. As a Level A IVIV relationship was defined by the IVIVC P-ring, clinical BE studies can be avoided and the BE assessment can be based only on the comparison of the in vitro release profiles. Thus, the time course of the accumulated amount of progesterone released in vitro was also derived for 12 rings of the test batch (batch E). Comparison of the in vitro release profiles of the two batches at the 375 mg dose level was performed by computing the difference and similarity factors (Equations (10) and (11)). Obtained values for both the parameters ( and ) fell within the FDA criteria allowing the assessment of the BE of the batches.
In addition to the standard model-independent procedure, the population IVIVC P-ring model approach developed here allows us to perform a virtual BE trial providing estimates of the relative bioavailability in vivo (F = AUC
test/AUC
ref). With this scope, the in vitro release model (Equation (1)) was identified on the in vitro release data of the test batch, and parameters were estimated (
Appendix B). Then, a 500 individual population treated with vaginal rings from the reference batch (batch B at 375 mg) was simulated using the IVIVC P-ring model and the correspondent release profile from batch B. A second independent population (500 subject) treated with vaginal rings of the test batch (batch E) was simulated using the same IVIVC P-ring model with the exception of the in vitro release parameters identified on batch E. Generally, in vivo BE is assessed in a unique population receiving treatments from reference and test batches in two different moments. However, because no information about intra-individual variability was available from the clinical data, a virtual BE trial was performed under the conservative assumption that intra-individual variability was equal to the inter-individual variability (even if it was expected to be lower). The simulated concentration profiles for the reference and test populations were then used to derive the correspondent
AUC. Finally, the relative bioavailability in vivo (F = AUC
test/AUC
ref = 0.913) and its 90% confidence interval (90%CI = [0.878, 0.948]) were computed. From the virtual BE trial, it emerged that the reference and test batches respected the 80–125% bioequivalence criteria, further confirming the bioequivalence of this case study.


 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}



















