
Nebuliser Type Influences Both Patient-Derived Bioaerosol Emissions and Ventilation Parameters during Mechanical Ventilation

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
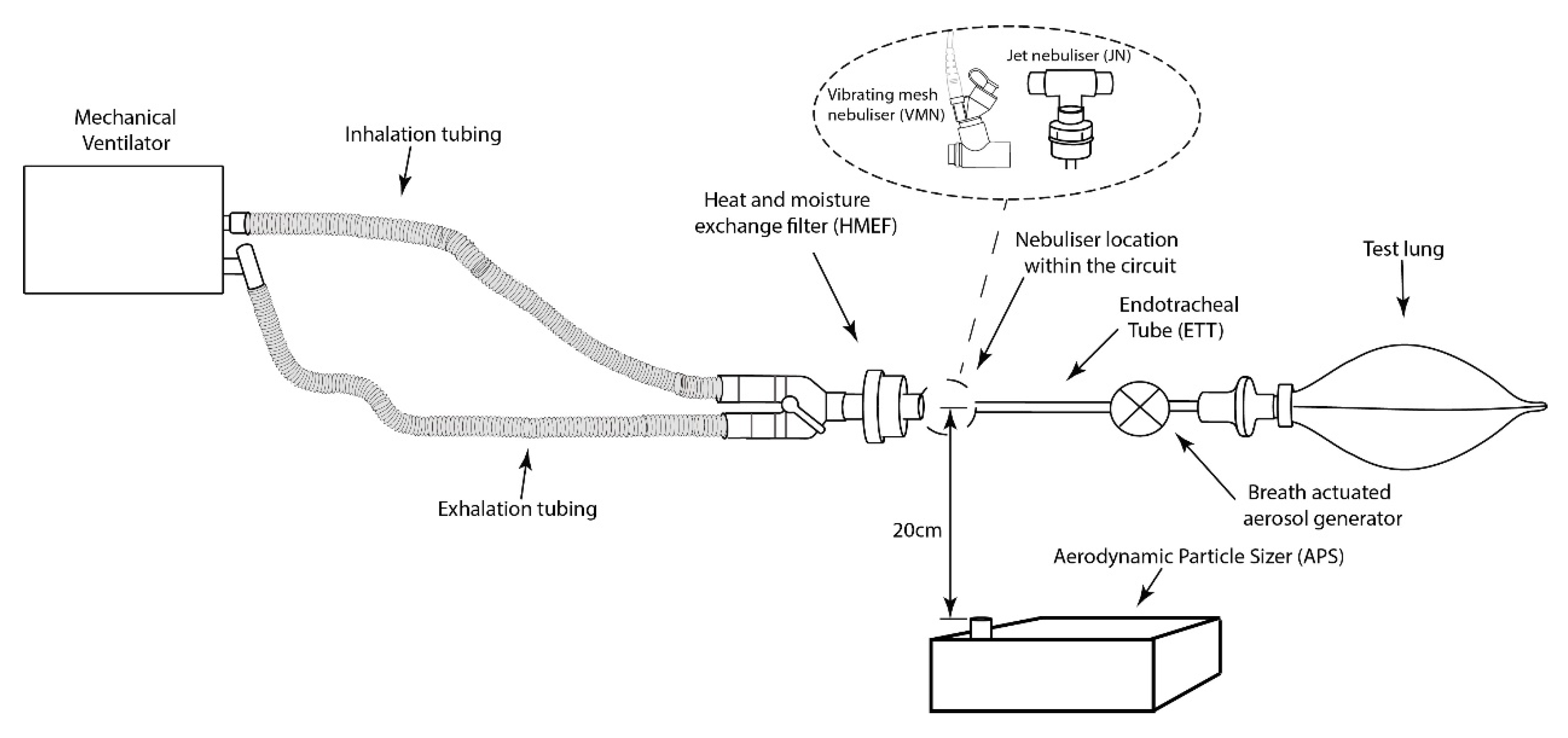
2.1. Experimental Setup
2.2. Simulated Bioaerosol
2.3. Characterisation of Bioaerosol Release to the Local Environment
2.4. Effect of Drug Refill on Ventilator Circuit Pressure
2.5. Statistical Analysis
3. Results
3.1. Bioaerosol Release to the Local Environment
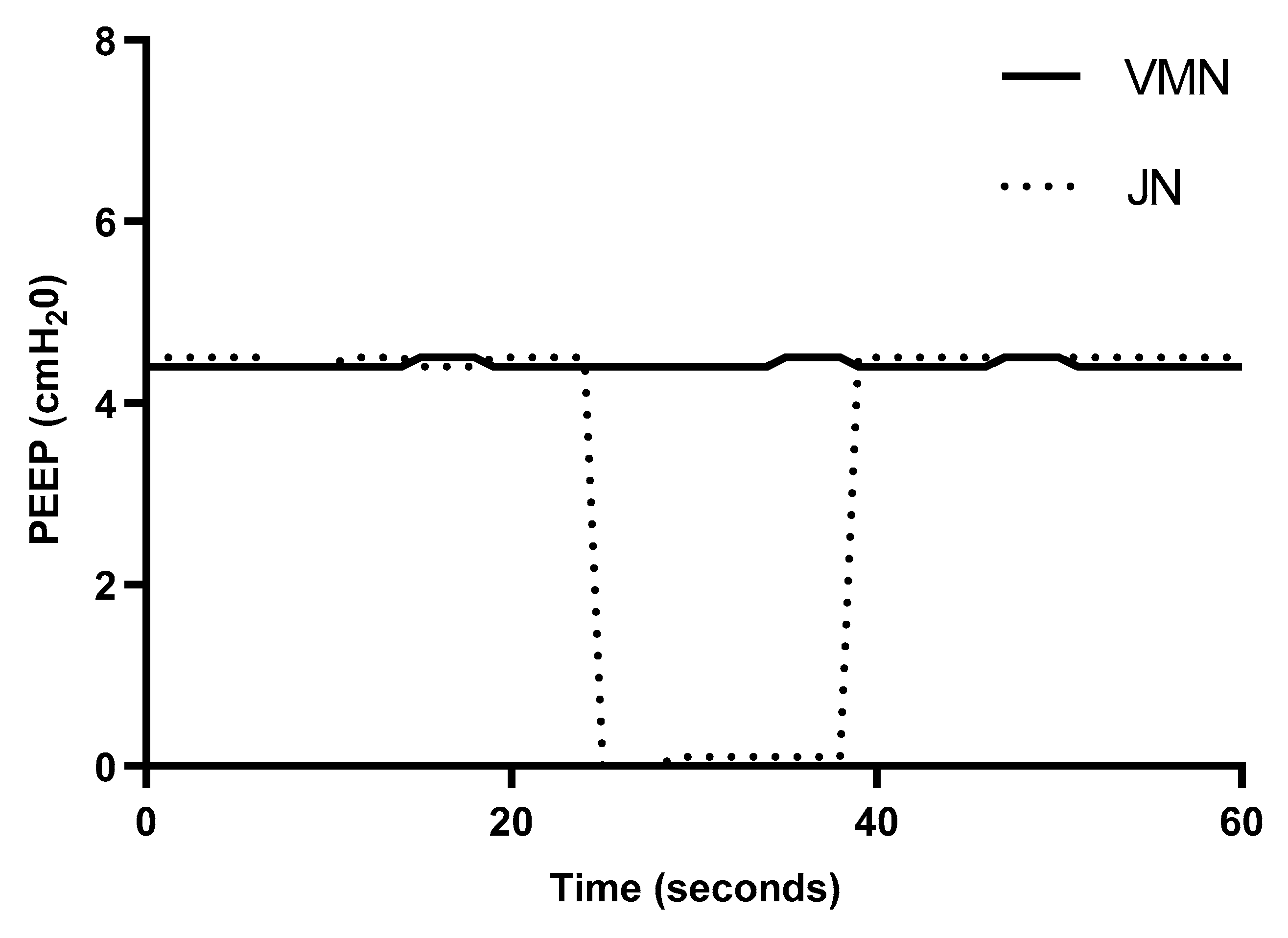
3.2. Ventilator Circuit Pressure
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Infectious Diseases. Available online: https://www.who.int/topics/infectious_diseases/en/ (accessed on 27 October 2020).
- Zhou, P.; Yang, X.L.; Wang, X.G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.R.; Zhu, Y.; Li, B.; Huang, C.L.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Liu, W.; Zhang, Q.; Xu, K.; Ye, G.; Wu, W.; Sun, Z.; Liu, F.; Wu, K.; Zhong, B.; et al. RNA based mNGS approach identifies a novel human coronavirus from two individual pneumonia cases in 2019 Wuhan outbreak. Emerg. Microbes Infect. 2020. [Google Scholar] [CrossRef] [PubMed]
- Coronavirus. Available online: https://www.who.int/health-topics/coronavirus#tab=tab_1 (accessed on 27 October 2020).
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Dhand, R. Basic techniques for aerosol delivery during mechanical ventilation. Respir. Care 2004, 49, 611–622. [Google Scholar] [PubMed]
- Ari, A. Practical strategies for a safe and effective delivery of aerosolized medications to patients with COVID-19. Respir. Med. 2020, 167. [Google Scholar] [CrossRef]
- Ehrmann, S.; Roche-Campo, F.; Sferrazza Papa, G.F.; Isabey, D.; Brochard, L.; Apiou-Sbirlea, G. Aerosol therapy during mechanical ventilation: An international survey. Intensive Care Med. 2013, 39, 1048–1056. [Google Scholar] [CrossRef]
- Van Haren, F.M.P.; Page, C.; Laffey, J.G.; Artigas, A.; Camprubi-Rimblas, M.; Nunes, Q.; Smith, R.; Shute, J.; Carroll, M.; Tree, J.; et al. Nebulised heparin as a treatment for COVID-19: Scientific rationale and a call for randomised evidence. Crit. Care 2020. [Google Scholar] [CrossRef]
- NCT04360096. Inhaled Aviptadil for the Treatment of Non-Acute Lung Injury in COVID-19; NeuroRx, Inc.: Newport Beach, CA, USA, 2020. [Google Scholar]
- Jackson, T.; Deibert, D.; Wyatt, G.; Durand-Moreau, Q.; Adisesh, A.; Khunti, K.; Khunti, S.; Smith, S.; Chan, X.H.S.; Ross, L.; et al. Classification of aerosol-generating procedures: A rapid systematic review. BMJ Open Respir. Res. 2020, 7, e000730. [Google Scholar] [CrossRef]
- Alhazzani, W.; Møller, M.H.; Arabi, Y.M.; Loeb, M.; Gong, M.N.; Fan, E.; Oczkowski, S.; Levy, M.M.; Derde, L.; Dzierba, A.; et al. Surviving Sepsis Campaign: Guidelines on the management of critically ill adults with Coronavirus Disease 2019 (COVID-19). Intensive Care Med. 2020. [Google Scholar] [CrossRef] [Green Version]
- Hick, J.L.; Hanfling, D.; Wynia, M.K.; Pavia, A.T. Duty to Plan: Health Care, Crisis Standards of Care, and Novel Coronavirus SARS-CoV-2. NAM Perspect. 2020. [Google Scholar] [CrossRef]
- Clinical Management of COVID-19. Available online: https://www.who.int/publications/i/item/clinical-management-of-covid-19 (accessed on 27 October 2020).
- Halpin, D.M.G.; Criner, G.J.; Papi, A.; Singh, D.; Anzueto, A.; Martinez, F.J.; Agusti, A.A.; Vogelmeier, C.F. Global Initiative for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease: The 2020 GOLD Science Committee Report on COVID-19 & COPD. Am. J. Respir. Crit. Care Med. 2020, 203, 24–36. [Google Scholar] [CrossRef]
- Gómez, C.C.; Rodríguez, Ó.P.; Torné, M.L.; Santaolalla, C.E.; Jiménez, J.F.M.; Fernández, J.G.; Perales, J.M.C.; Heili-Frades, S.B.; Monreal, M.F.; de Andrés Nilsson, J.M.; et al. Clinical consensus recommendations regarding non-invasive respiratory support in the adult patient with acute respiratory failure secondary to SARS-CoV-2 infection. Med. Intensiva 2020. [Google Scholar] [CrossRef]
- Respiratory Care Committee of Chinese Thoracic Society. Expert consensus on preventing nosocomial transmission during respiratory care for critically ill patients infected by 2019 novel coronavirus pneumonia. Chin. J. Tuberc. Respir. Dis. 2020, 43, 288–296. [Google Scholar] [CrossRef]
- Fink, J.B.; Ehrmann, S.; Li, J.; Dailey, P.; McKiernan, P.; Darquenne, C.; Martin, A.R.; Rothen-Rutishauser, B.; Kuehl, P.J.; Häussermann, S.; et al. Reducing Aerosol-Related Risk of Transmission in the Era of COVID-19: An Interim Guidance Endorsed by the International Society of Aerosols in Medicine. J. Aerosol. Med. Pulm. Drug Deliv. 2020, 33, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Ari, A. Promoting Safe and Effective Use of Aerosol Devices in Covid-19:Risks and Suggestions for Viral Transmission. Expert Opin. Drug Deliv. 2020, 17, 1509–1513. [Google Scholar] [CrossRef] [PubMed]
- Karagiannidis, C.; Mostert, C.; Hentschker, C.; Voshaar, T.; Malzahn, J.; Schillinger, G.; Klauber, J.; Janssens, U.; Marx, G.; Weber-Carstens, S.; et al. Case characteristics, resource use, and outcomes of 10 021 patients with COVID-19 admitted to 920 German hospitals: An observational study. Lancet Respir. Med. 2020. [Google Scholar] [CrossRef]
- Hui, D.S.; Chow, B.K.; Chu, L.C.Y.; Ng, S.S.; Hall, S.D.; Gin, T.; Chan, M.T.V. Exhaled air and aerosolized droplet dispersion during application of a jet nebulizer. Chest 2009, 135, 648–654. [Google Scholar] [CrossRef]
- Jacob, M.; Ruivo, E.; Portela, I.; Tavares, J.; Varela, M.; Moutinho, S.; Costa, H.; Nunez, D. An innovative endotracheal tube clamp for use in COVID-19. Can. J. Anesth. 2020. [Google Scholar] [CrossRef]
- Ari, A.; Alwadeai, K.S.; Fink, J.B. Effects of heat and moisture exchangers and exhaled humidity on aerosol deposition in a simulated ventilator-dependent adult lung model. Respir. Care 2017, 62, 538–543. [Google Scholar] [CrossRef] [Green Version]
- Gattinoni, L.; Caironi, P.; Cressoni, M.; Chiumello, D.; Ranieri, V.M.; Quintel, M.; Russo, S.; Patroniti, N.; Cornejo, R.; Bugedo, G. Lung Recruitment in Patients with the Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2006. [Google Scholar] [CrossRef]
- ISO 27427:2013. Anaesthetic and Respiratory Equipment—Nebulizing Systems and Components; ISO: Geneva, Switzerland, 2013. [Google Scholar]
- McGrath, J.A.; O’Sullivan, A.; Bennett, G.; O’Toole, C.; Joyce, M.; Byrne, M.A.; MacLoughlin, R. Investigation of the quantity of exhaled aerosols released into the environment during nebulisation. Pharmaceutics 2019, 11, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGrath, J.A.; O’Toole, C.; Bennett, G.; Joyce, M.; Byrne, M.A.; Macloughlin, R. Investigation of fugitive aerosols released into the environment during high-flow therapy. Pharmaceutics 2019, 11, 254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Toole, C.; McGrath, J.A.; Joyce, M.; Bennett, G.; Byrne, M.A.; Macloughlin, R. Fugitive aerosol therapy emissions during mechanical ventilation: In vitro assessment of the effect of tidal volume and use of protective filters. Aerosol Air Qual. Res. 2020. [Google Scholar] [CrossRef]
- Ari, A.; Fink, J.B.; Pilbeam, S.P. Secondhand aerosol exposure during mechanical ventilation with and without expiratory filters: An in-vitro study Recommended Citation. Indian J. Respir. Care 2016, 5, 677–682. [Google Scholar]
- O’Toole, C.; Joyce, M.; McGrath, J.A.; O’Sullivan, A.; Byrne, M.A.; MacLoughlin, R. Fugitive aerosols in the intensive care unit: A narrative review. Ann. Transl. Med. 2020. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Particulate Number Concentrations (#/cm−3) Median and IQR | ||
|---|---|---|
| Vibrating Mesh Nebuliser | Jet Nebuliser | JN with Endotracheal Tube Clamped |
| 0 (0.1–0.6) | 710 (265–1211) | 60 (31–140) |
| PEEP (cmH2O) Average ± SD | |
|---|---|
| Vibrating Mesh Nebuliser | Jet Nebuliser |
| 4.4 ± 0.0 | 3.5 ± 1.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Joyce, M.; McGrath, J.A.; Mac Giolla Eain, M.; O’Sullivan, A.; Byrne, M.; MacLoughlin, R. Nebuliser Type Influences Both Patient-Derived Bioaerosol Emissions and Ventilation Parameters during Mechanical Ventilation. Pharmaceutics 2021, 13, 199. https://doi.org/10.3390/pharmaceutics13020199
Joyce M, McGrath JA, Mac Giolla Eain M, O’Sullivan A, Byrne M, MacLoughlin R. Nebuliser Type Influences Both Patient-Derived Bioaerosol Emissions and Ventilation Parameters during Mechanical Ventilation. Pharmaceutics. 2021; 13(2):199. https://doi.org/10.3390/pharmaceutics13020199
Chicago/Turabian StyleJoyce, Mary, James A. McGrath, Marc Mac Giolla Eain, Andrew O’Sullivan, Miriam Byrne, and Ronan MacLoughlin. 2021. "Nebuliser Type Influences Both Patient-Derived Bioaerosol Emissions and Ventilation Parameters during Mechanical Ventilation" Pharmaceutics 13, no. 2: 199. https://doi.org/10.3390/pharmaceutics13020199