
Nitric-Oxide-Releasing Dexamethasone Derivative NCX-1005 Improves Lung Function and Attenuates Inflammation in Experimental Lavage-Induced ARDS


Abstract
:1. Introduction
2. Materials and Methods
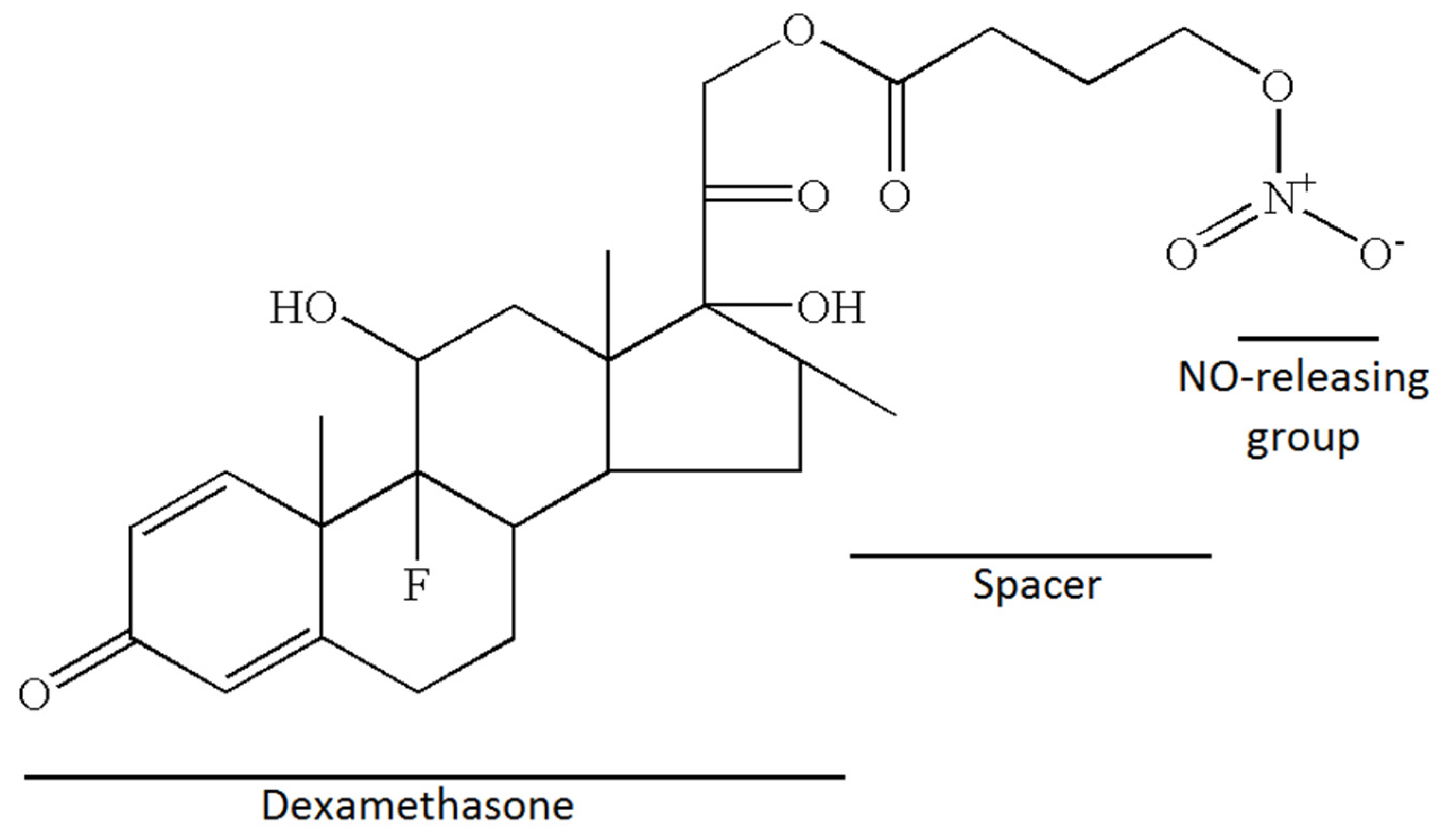
2.1. Nitrate Esters of Corticoid, Chemical Structure and Synthesis
2.2. Animal Instrumentation
2.3. Experimental Protocol
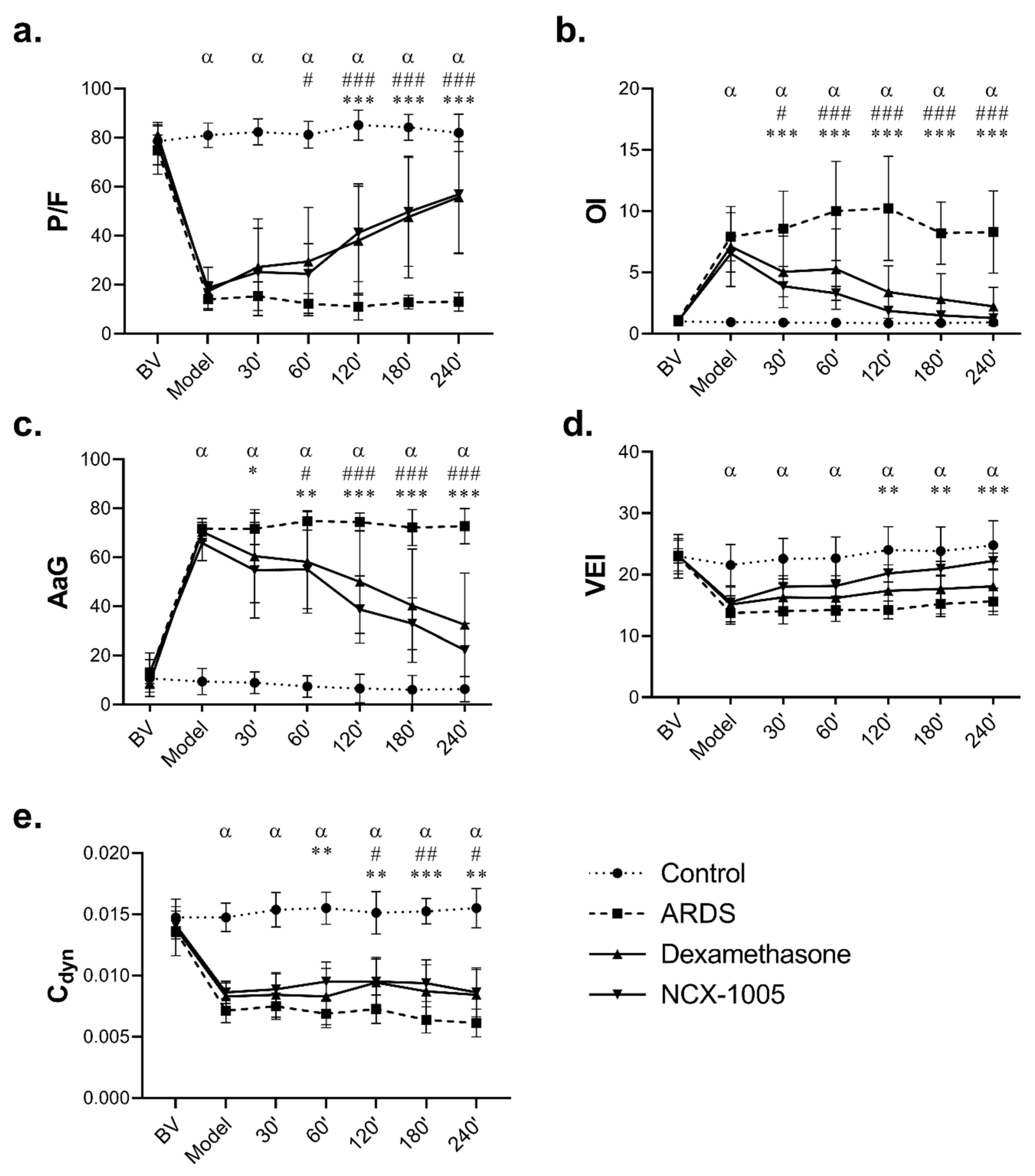
2.4. Lung Function Parameters and Derived Indexes
2.5. White Blood Cells in the Blood and Bronchoalveolar Lavage Fluid
2.6. Post-Mortem Analyses
2.7. Statistical Analysis
3. Results
3.1. Lung Function Parameters
3.2. Total and Differential Leukocyte Count in Blood and Bronchoalveolar Lavage Fluid
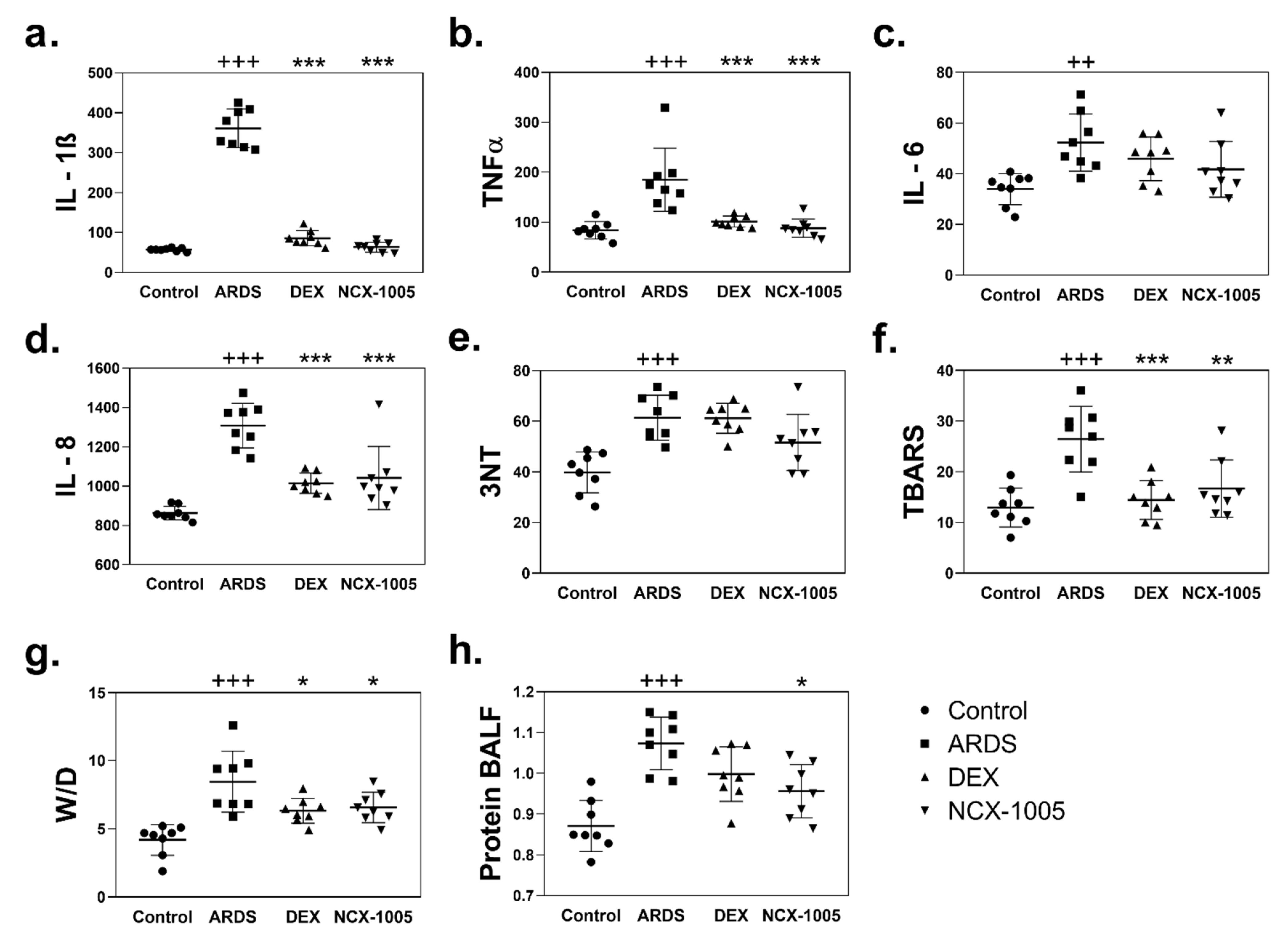
3.3. Inflammation and Oxidation in Plasma and Lung Tissue
3.4. Lung Oedema and Protein Content in Bronchoalveolar Lavage Fluid
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [PubMed]
- Martin, T.R. Lung cytokines and ARDS: Roger S. Mitchell Lecture. Chest 1999, 116, 2S–8S. [Google Scholar] [CrossRef]
- Ware, L.B.; Matthay, M.A. The acute respiratory distress syndrome. N. Engl. J. Med. 2000, 342, 1334–1349. [Google Scholar] [CrossRef]
- Brower, R.G.; Matthay, M.A.; Morris, A.; Schoenfeld, D.; Thompson, B.T.; Wheeler, A. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N. Engl. J. Med. 2000, 342, 1301–1308. [Google Scholar]
- Guérin, C.; Reignier, J.; Richard, J.-C.; Beuret, P.; Gacouin, A.; Boulain, T.; Mercier, E.; Badet, M.; Mercat, A.; Baudin, O.; et al. Prone positioning in severe acute respiratory distress syndrome. N. Engl. J. Med. 2013, 368, 2159–2168. [Google Scholar] [CrossRef]
- Wiedemann, H.P.; Wheeler, A.P.; Bernard, G.R.; Thompson, B.T.; Hayden, D.; deBoisblanc, B.; Connors, A.F.J.; Hite, R.D.; Harabin, A.L. Comparison of two fluid-management strategies in acute lung injury. N. Engl. J. Med. 2006, 354, 2564–2575. [Google Scholar] [CrossRef] [Green Version]
- Mokry, J.; Mokra, D.; Antosova, M.; Bulikova, J.; Calkovska, A.; Nosalova, G. Dexamethasone alleviates meconium-induced airway hyperresponsiveness and lung inflammation in rabbits. Pediatr. Pulmonol. 2006, 41, 55–60. [Google Scholar] [CrossRef]
- Kosutova, P.; Mikolka, P.; Balentova, S.; Adamkov, M.; Kolomaznik, M.; Calkovska, A.; Mokra, D. Intravenous dexamethasone attenuated inflammation and influenced apoptosis of lung cells in an experimental model of acute lung injury. Physiol. Res. 2016, 65, S663–S672. [Google Scholar] [CrossRef]
- Mikolka, P.; Kosutova, P.; Kolomaznik, M.; Topercerova, J.; Kopincova, J.; Calkovska, A.; Mokra, D. Effect of different dosages of dexamethasone therapy on lung function and inflammation in an early phase of acute respiratory distress syndrome model. Physiol. Res. 2019, 68, S253–S263. [Google Scholar] [CrossRef]
- Danesch, U.; Gloss, B.; Schmid, W.; Schütz, G.; Schüle, R.; Renkawitz, R. Glucocorticoid induction of the rat tryptophan oxygenase gene is mediated by two widely separated glucocorticoid-responsive elements. EMBO J. 1987, 6, 625–630. [Google Scholar] [CrossRef]
- Jantzen, H.M.; Strähle, U.; Gloss, B.; Stewart, F.; Schmid, W.; Boshart, M.; Miksicek, R.; Schütz, G. Cooperativity of glucocorticoid response elements located far upstream of the tyrosine aminotransferase gene. Cell 1987, 49, 29–38. [Google Scholar] [CrossRef] [Green Version]
- Kubes, P.; Suzuki, M.; Granger, D.N. Nitric oxide: An endogenous modulator of leukocyte adhesion. Proc. Natl. Acad. Sci. USA 1991, 88, 4651–4655. [Google Scholar] [CrossRef] [Green Version]
- Paul-Clark, M.J.; Gilroy, D.W.; Willis, D.; Willoughby, D.A.; Tomlinson, A. Nitric oxide synthase inhibitors have opposite effects on acute inflammation depending on their route of administration. J. Immunol. 2001, 166, 1169–1177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaboury, J.P.; Niu, X.F.; Kubes, P. Nitric oxide inhibits numerous features of mast cell-induced inflammation. Circulation 1996, 93, 318–326. [Google Scholar] [CrossRef]
- Park, S.K.; Lin, H.L.; Murphy, S. Nitric oxide regulates nitric oxide synthase-2 gene expression by inhibiting NF-kappaB binding to DNA. Biochem. J. 1997, 322 Pt 2, 609–613. [Google Scholar] [CrossRef] [Green Version]
- Katsuyama, K.; Shichiri, M.; Marumo, F.; Hirata, Y. NO inhibits cytokine-induced iNOS expression and NF-kappaB activation by interfering with phosphorylation and degradation of IkappaB-alpha. Arterioscler. Thromb. Vasc. Biol. 1998, 18, 1796–1802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Connelly, L.; Palacios-Callender, M.; Ameixa, C.; Moncada, S.; Hobbs, A.J. Biphasic Regulation of NF-κB Activity Underlies the Pro- and Anti-Inflammatory Actions of Nitric Oxide. J. Immunol. 2001, 166, 3873–3881. [Google Scholar] [CrossRef] [Green Version]
- Paul-Clark, M.J.; Mancini, L.; Del Soldato, P.; Flower, R.J.; Perretti, M. Potent antiarthritic properties of a glucocorticoid derivative, NCX-1015, in an experimental model of arthritis. Proc. Natl. Acad. Sci. USA 2002, 99, 1677–1682. [Google Scholar] [CrossRef] [Green Version]
- Galassi, F.; Masini, E.; Giambene, B.; Fabrizi, F.; Uliva, C.; Bolla, M.; Ongini, E. A topical nitric oxide-releasing dexamethasone derivative: Effects on intraocular pressure and ocular haemodynamics in a rabbit glaucoma model. Br. J. Ophthalmol. 2006, 90, 1414–1419. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.; Li, H.; Sun, H.; Gong, L.; Guo, L.; Shi, Y.; Cai, C.; Gu, H.; Song, Z.; Yang, L.; et al. A novel nitro-dexamethasone inhibits agr system activity and improves therapeutic effects in MRSA sepsis models without antibiotics. Sci. Rep. 2016, 6, 20307. [Google Scholar] [CrossRef] [PubMed]
- Tallet, D.; Del Soldato, P.; Oudart, N.; Burgaud, J.-L. NO-steroids: Potent anti-inflammatory drugs with bronchodilating activity in vitro. Biochem. Biophys. Res. Commun. 2002, 290, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Baraldi, P.G.; Romagnoli, R.; Del Carmen Nuñez, M.; Perretti, M.; Paul-Clark, M.J.; Ferrario, M.; Govoni, M.; Benedini, F.; Ongini, E. Synthesis of nitro esters of prednisolone, new compounds combining pharmacological properties of both glucocorticoids and nitric oxide. J. Med. Chem. 2004, 47, 711–719. [Google Scholar] [CrossRef] [PubMed]
- Guillen, J. FELASA guidelines and recommendations. J. Am. Assoc. Lab. Anim. Sci. 2012, 51, 311–321. [Google Scholar] [PubMed]
- Kosutova, P.; Mikolka, P.; Kolomaznik, M.; Balentova, S.; Adamkov, M.; Calkovska, A.; Mokra, D. Reduction of lung inflammation, oxidative stress and apoptosis by the PDE4 inhibitor roflumilast in experimental model of acute lung injury. Physiol. Res. 2018, 67, S645–S654. [Google Scholar] [CrossRef]
- Thompson, B.T.; Chambers, R.C.; Liu, K.D. Acute respiratory distress syndrome. N. Engl. J. Med. 2017, 377, 562–572. [Google Scholar] [CrossRef]
- Robb, C.T.; Regan, K.H.; Dorward, D.A.; Rossi, A.G. Key mechanisms governing resolution of lung inflammation. Semin. Immunopathol. 2016, 38, 425–448. [Google Scholar] [CrossRef] [Green Version]
- Newton, R.; Leigh, R.; Giembycz, M.A. Pharmacological strategies for improving the efficacy and therapeutic ratio of glucocorticoids in inflammatory lung diseases. Pharmacol. Ther. 2010, 125, 286–327. [Google Scholar] [CrossRef]
- Engel, M.; Nowacki, R.M.E.; Jonker, E.M.; Ophelders, D.; Nikiforou, M.; Kloosterboer, N.; Zimmermann, L.J.I.; van Waardenburg, D.A.; Kramer, B.W. A comparison of four different models of acute respiratory distress syndrome in sheep. Respir. Res. 2020, 21, 209. [Google Scholar] [CrossRef]
- Kamiyama, J.; Jesmin, S.; Sakuramoto, H.; Shimojyo, N.; Islam, M.; Hagiya, K.; Sugano, M.; Unoki, T.; Oki, M.; Kawano, S.; et al. Hyperinflation deteriorates arterial oxygenation and lung injury in a rabbit model of ARDS with repeated open endotracheal suctioning. BMC Anesthesiol. 2015, 15, 73. [Google Scholar] [CrossRef] [Green Version]
- Ricci, F.; Catozzi, C.; Murgia, X.; Rosa, B.; Amidani, D.; Lorenzini, L.; Bianco, F.; Rivetti, C.; Catinella, S.; Villetti, G.; et al. Physiological, Biochemical, and Biophysical Characterization of the Lung-Lavaged Spontaneously-Breathing Rabbit as a Model for Respiratory Distress Syndrome. PLoS ONE 2017, 12, e0169190. [Google Scholar] [CrossRef] [Green Version]
- Seehase, M.; Collins, J.J.P.; Kuypers, E.; Jellema, R.K.; Ophelders, D.R.M.G.; Ospina, O.L.; Perez-Gil, J.; Bianco, F.; Garzia, R.; Razzetti, R.; et al. New surfactant with SP-B and C analogs gives survival benefit after inactivation in preterm lambs. PLoS ONE 2012, 7, e47631. [Google Scholar] [CrossRef]
- Soukka, H.; Halkola, L.; Aho, H.; Rautanen, M.; Kero, P.; Kääpä, P. Methylprednisolone Attenuates the Pulmonary Hypertensive Response in Porcine Meconium Aspiration. Pediatr. Res. 1997, 42, 145–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holopainen, R.; Laine, J.; Halkola, L.; Aho, H.; Kääpä, P. Dexamethasone treatment attenuates pulmonary injury in piglet meconium aspiration. Pediatr. Res. 2001, 49, 162–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, H.G. Mechanisms of glucocorticoid action in pulmonary disease. Chest 1985, 88, 133S–141S. [Google Scholar] [CrossRef]
- Zielińska, K.A.; Van Moortel, L.; Opdenakker, G.; De Bosscher, K.; Van den Steen, P.E. Endothelial Response to Glucocorticoids in Inflammatory Diseases. Front. Immunol. 2016, 7, 592. [Google Scholar] [CrossRef] [PubMed]
- Mokra, D.; Mokry, J.; Drgova, A.; Bulikova, J.; Petraskova, M.; Calkovska, A. Single-dose versus two-dose dexamethasone effects on lung inflammation and airway reactivity in meconium-instilled rabbits. J. Physiol. Pharmacol. Off. J. Polish Physiol. Soc. 2007, 58 (Suppl. 5), 379–387. [Google Scholar]
- Meduri, G.U.; Golden, E.; Freire, A.X.; Taylor, E.; Zaman, M.; Carson, S.J.; Gibson, M.; Umberger, R. Methylprednisolone Infusion in Early Severe ARDS: Results of a Randomized Controlled Trial. Chest 2007, 131, 954–963. [Google Scholar] [CrossRef] [Green Version]
- Tang, B.M.P.; Craig, J.C.; Eslick, G.D.; Seppelt, I.; McLean, A.S. Use of corticosteroids in acute lung injury and acute respiratory distress syndrome: A systematic review and meta-analysis. Crit. Care Med. 2009, 37, 1594–1603. [Google Scholar] [CrossRef]
- Tongyoo, S.; Permpikul, C.; Mongkolpun, W.; Vattanavanit, V.; Udompanturak, S.; Kocak, M.; Meduri, G.U. Hydrocortisone treatment in early sepsis-associated acute respiratory distress syndrome: Results of a randomized controlled trial. Crit. Care 2016, 20, 329. [Google Scholar] [CrossRef] [Green Version]
- Villar, J.; Blanco, J.; Kacmarek, R.M. Current incidence and outcome of the acute respiratory distress syndrome. Curr. Opin. Crit. Care 2016, 22, 1–6. [Google Scholar] [CrossRef]
- Villar, J.; Ferrando, C.; Martínez, D.; Ambrós, A.; Muñoz, T.; Soler, J.A.; Aguilar, G.; Alba, F.; González-Higueras, E.; Conesa, L.A.; et al. Dexamethasone treatment for the acute respiratory distress syndrome: A multicentre, randomised controlled trial. Lancet Respir. Med. 2020, 8, 267–276. [Google Scholar] [CrossRef]
- Hegeman, M.A.; Hennus, M.P.; Cobelens, P.M.; Kavelaars, A.; Jansen, N.J.G.; Schultz, M.J.; van Vught, A.J.; Heijnen, C.J. Dexamethasone attenuates VEGF expression and inflammation but not barrier dysfunction in a murine model of ventilator-induced lung injury. PLoS ONE 2013, 8, e57374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, B.; Wang, D.-X.; Deng, W. Protective effects of dexamethasone on early acute lung injury induced by oleic acid in rats. Int. J. Clin. Exp. Med. 2014, 7, 4698–4709. [Google Scholar]
- Wen, S.; Wu, H.; Lin, L.; Chong, L.; Zhu, L.; Zhang, W.; Zhang, H.; Li, C. Adjunctive dexamethasone therapy improves lung injury by inhibiting inflammation and reducing RIP3 expression during Staphylococcus aureus pneumonia in mice. Int. Immunopharmacol. 2014, 23, 709–718. [Google Scholar] [CrossRef]
- Zemans, R.L.; Matthay, M.A. What drives neutrophils to the alveoli in ARDS? Thorax 2017, 72, 1–3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Folkesson, H.G.; Matthay, M.A.; Hébert, C.A.; Broaddus, V.C. Acid aspiration-induced lung injury in rabbits is mediated by interleukin-8-dependent mechanisms. J. Clin. Investig. 1995, 96, 107–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinho, V.; de Castro Russo, R.; Amaral, F.A.; de Sousa, L.P.; Barsante, M.M.; de Souza, D.G.; Alves-Filho, J.C.; Cara, D.C.; Hayflick, J.S.; Rommel, C.; et al. Tissue- and stimulus-dependent role of phosphatidylinositol 3-kinase isoforms for neutrophil recruitment induced by chemoattractants in vivo. J. Immunol. 2007, 179, 7891–7898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janciauskiene, S.; Wrenger, S.; Immenschuh, S.; Olejnicka, B.; Greulich, T.; Welte, T.; Chorostowska-Wynimko, J. The Multifaceted Effects of Alpha1-Antitrypsin on Neutrophil Functions. Front. Pharmacol. 2018, 9, 341. [Google Scholar] [CrossRef] [PubMed]
- Petri, B.; Sanz, M.-J. Neutrophil chemotaxis. Cell Tissue Res. 2018, 371, 425–436. [Google Scholar] [CrossRef]
- Paul-Clark, M.; Del Soldato, P.; Fiorucci, S.; Flower, R.J.; Perretti, M. 21-NO-prednisolone is a novel nitric oxide-releasing derivative of prednisolone with enhanced anti-inflammatory properties. Br. J. Pharmacol. 2000, 131, 1345–1354. [Google Scholar] [CrossRef] [PubMed]
- Bouros, D.; Alexandrakis, M.G.; Antoniou, K.M.; Agouridakis, P.; Pneumatikos, I.; Anevlavis, S.; Pataka, A.; Patlakas, G.; Karkavitsas, N.; Kyriakou, D. The clinical significance of serum and bronchoalveolar lavage inflammatory cytokines in patients at risk for Acute Respiratory Distress Syndrome. BMC Pulm. Med. 2004, 4, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meduri, G.U.; Annane, D.; Chrousos, G.P.; Marik, P.E.; Sinclair, S.E. Activation and regulation of systemic inflammation in ARDS: Rationale for prolonged glucocorticoid therapy. Chest 2009, 136, 1631–1643. [Google Scholar] [CrossRef]
- Chimenti, L.; Morales-Quinteros, L.; Puig, F.; Camprubi-Rimblas, M.; Guillamat-Prats, R.; Gómez, M.N.; Tijero, J.; Blanch, L.; Matute-Bello, G.; Artigas, A. Comparison of direct and indirect models of early induced acute lung injury. Intensive Care Med. Exp. 2020, 8, 62. [Google Scholar] [CrossRef]
- Coutinho, A.E.; Chapman, K.E. The anti-inflammatory and immunosuppressive effects of glucocorticoids, recent developments and mechanistic insights. Mol. Cell. Endocrinol. 2011, 335, 2–13. [Google Scholar] [CrossRef] [PubMed]
- Khilnani, G.C.; Hadda, V. Corticosteroids and ARDS: A review of treatment and prevention evidence. Lung India 2011, 28, 114–119. [Google Scholar] [CrossRef] [PubMed]
- Montón, C.; Ewig, S.; Torres, A.; El-Ebiary, M.; Filella, X.; Rañó, A.; Xaubet, A. Role of glucocorticoids on inflammatory response in nonimmunosuppressed patients with pneumonia: A pilot study. Eur. Respir. J. 1999, 14, 218–220. [Google Scholar] [CrossRef] [Green Version]
- Matthay, M.A.; Zemans, R.L. The acute respiratory distress syndrome: Pathogenesis and treatment. Annu. Rev. Pathol. 2011, 6, 147–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cunha, F.Q.; Teixeira, M.M.; Ferreira, S.H. Pharmacological modulation of secondary mediator systems--cyclic AMP and cyclic GMP--on inflammatory hyperalgesia. Br. J. Pharmacol. 1999, 127, 671–678. [Google Scholar] [CrossRef] [Green Version]
- Coxon, A.; Cullere, X.; Knight, S.; Sethi, S.; Wakelin, M.W.; Stavrakis, G.; Luscinskas, F.W.; Mayadas, T.N. Fc gamma RIII mediates neutrophil recruitment to immune complexes. A mechanism for neutrophil accumulation in immune-mediated inflammation. Immunity 2001, 14, 693–704. [Google Scholar] [CrossRef] [Green Version]
- Pedrazza, L.; Cunha, A.A.; Luft, C.; Nunes, N.K.; Schimitz, F.; Gassen, R.B.; Breda, R.V.; Donadio, M.V.F.; de Souza Wyse, A.T.; Pitrez, P.M.C.; et al. Mesenchymal stem cells improves survival in LPS-induced acute lung injury acting through inhibition of NETs formation. J. Cell. Physiol. 2017, 232, 3552–3564. [Google Scholar] [CrossRef] [PubMed]
- Matthay, M.A.; Ware, L.B.; Zimmerman, G.A. The acute respiratory distress syndrome. J. Clin. Investig. 2012, 122, 2731–2740. [Google Scholar] [CrossRef] [Green Version]
- Matthay, M.A.; Ware, L.B. Resolution of Alveolar Edema in Acute Respiratory Distress Syndrome. Physiology and Biology. Am. J. Respir. Crit. Care Med. 2015, 192, 124–125. [Google Scholar] [CrossRef]
- Yang, Z.-G.; Lei, X.-L.; Li, X.-L. Early application of low-dose glucocorticoid improves acute respiratory distress syndrome: A meta-analysis of randomized controlled trials. Exp. Ther. Med. 2017, 13, 1215–1224. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| BV | Model | 30′ | 60′ | 120′ | 180′ | 240′ | |
|---|---|---|---|---|---|---|---|
| MAP (kPa) | |||||||
| Control | 0.78 ± 0.04 | 0.76 ± 0.05 | 0.73 ± 0.05 | 0.72 ± 0.04 | 0.71 ± 0.03 | 0.72 ± 0.04 | 0.73 ± 0.05 |
| ARDS | 0.81 ± 0.07 | 1.13 ± 0.09 ††† | 1.08 ± 0.07 ††† | 1.09 ± 0.08 ††† | 1.15 ± 0.11 ††† | 1.16 ± 0.11 ††† | 1.16 ± 0.12 ††† |
| DEX | 0.81 ± 0.04 | 1.06 ± 0.11 | 0.94 ± 0.10 # | 1.00 ± 0.08 | 0.91 ± 0.09 ### | 0.94 ± 0.16 ### | 0.97 ± 0.19 ### |
| NCX-1005 | 0.79 ± 0.04 | 1.02 ± 0.11 | 0.93 ± 0.08 * | 0.93 ± 0.10 * | 0.91 ± 0.15 *** | 0.89 ± 0.19 *** | 0.90 ± 0.18 *** |
| Cstat (mL/kPa) | |||||||
| Control | 0.016 ± 0.001 | 0.016 ± 0.001 | 0.017 ± 0.001 | 0.017 ± 0.002 | 0.017 ± 0.002 | 0.017 ± 0.001 | 0.017 ± 0.001 |
| ARDS | 0.015 ± 0.003 | 0.009 ± 0.002 ††† | 0.009 ± 0.001 ††† | 0.008 ± 0.002 ††† | 0.008 ± 0.001 ††† | 0.008 ± 0.001 ††† | 0.008 ± 0.001 ††† |
| DEX | 0.016 ± 0.002 | 0.009 ± 0.002 | 0.010 ± 0.003 | 0.010 ± 0.003 | 0.011 ± 0.002 | 0.010 ± 0.003 | 0.010 ± 0.002 |
| NCX-1005 | 0.016 ± 0.002 | 0.009 ± 0.001 | 0.010 ± 0.001 | 0.011 ± 0.001 * | 0.011 ± 0.001 * | 0.011 ± 0.001 * | 0.010 ± 0.001 * |
| Raw (kPa/l/s) | |||||||
| Control | 4.68 ± 0.76 | 4.79 ± 0.95 | 5.27 ± 0.90 | 4.81 ± 0.81 | 4.99 ± 0.72 | 4.67 ± 0.67 | 4.58 ± 0.82 |
| ARDS | 5.02 ± 1.51 | 12.17 ± 5.35 ††† | 14.44 ± 5.27 ††† | 15.96 ± 5.76 ††† | 17.02 ± 6.95 ††† | 16.19 ± 7.14 ††† | 17.14 ± 6.67 ††† |
| DEX | 4.72 ± 0.77 | 7.69 ± 1.72 | 8.70 ± 2.23 ## | 8.99 ± 1.81 ### | 7.66 ± 1.90 ### | 8.58 ± 3.36 ### | 9.07 ± 2.88 ### |
| NCX-1005 | 4.28 ± 1.01 | 9.12 ± 1.54 | 7.88 ± 2.08 ** | 7.77 ± 2.69 *** | 8.01 ± 4.10 *** | 8.10 ± 3.43 *** | 8.69 ± 3.47 *** |
| PaCO2 (kPa) | |||||||
| Control | 4.23 ± 0.69 | 4.49 ± 0.64 | 4.29 ± 0.61 | 4.29 ± 0.71 | 4.06 ± 0.78 | 4.08 ± 0.68 | 3.93 ± 0.70 |
| ARDS | 4.05 ± 0.61 | 7.03 ± 1.00 ††† | 6.82 ± 1.33 ††† | 6.76 ± 1.05 ††† | 6.75 ± 0.75 ††† | 6.37 ± 0.69 ††† | 6.41 ± 0.88 ††† |
| DEX | 3.99 ± 0.21 | 6.5 ± 1.01 | 5.97 ± 0.86 | 6.17 ± 0.97 | 5.86 ± 0.99 | 5.94 ± 1.53 | 5.70 ± 1.31 |
| NCX-1005 | 4.10 ± 0.63 | 6.06 ± 1.12 | 5.77 ± 1.33 | 5.61 ± 1.28 | 4.91 ± 0.95 *** | 4.67 ± 0.73 ** | 4.32 ± 0.72 ***@ |
| SaO2 (%) | |||||||
| Control | 99.90 ± 0.00 | 99.90 ± 0.00 | 99.90 ± 0.00 | 99.90 ± 0.00 | 99.90 ± 0.00 | 99.90 ± 0.00 | 99.89 ± 0.04 |
| ARDS | 99.90 ± 0.00 | 94.34 ± 3.59 | 95.83 ± 2.06 | 89.47 ± 12.42 ††† | 88.74 ± 9.07 ††† | 91.24 ± 5.19 †† | 84.67 ± 14.41 ††† |
| DEX | 99.90 ± 0.00 | 97.39 ± 1.72 | 97.47 ± 1.92 | 97.16 ± 2.48 ## | 98.76 ± 1.10 ### | 99.20 ± 0.79 ## | 99.49 ± 0.49 ### |
| NCX-1005 | 99.91 ± 0.04 | 96.63 ± 4.49 | 96.41 ± 5.88 | 99.00 ± 1.20 *** | 99.69 ± 0.24 *** | 99.76 ± 0.11 ** | 99.83 ± 0.09 *** |
| pH | |||||||
| Control | 7.49 ± 0.05 | 7.44 ± 0.08 | 7.40 ± 0.03 | 7.37 ± 0.03 | 7.33 ± 0.07 | 7.29 ± 0.04 | 7.27 ± 0.04 |
| ARDS | 7.54 ± 0.03 | 7.23 ± 0.04 ††† | 7.23 ± 0.06 ††† | 7.21 ± 0.06 ††† | 7.15 ± 0.06 ††† | 7.12 ± 0.07 ††† | 7.08 ± 0.04 ††† |
| DEX | 7.47 ± 0.08 | 7.25 ± 0.05 | 7.26 ± 0.04 | 7.24 ± 0.05 | 7.23 ± 0.04 | 7.19 ± 0.07 | 7.15 ± 0.07 |
| NCX-1005 | 7.48 ± 0.09 | 7.26 ± 0.09 | 7.27 ± 0.11 | 7.25 ± 0.10 | 7.23 ± 0.09 | 7.19 ± 0.10 | 7.17 ± 0.09 * |
| BLOOD | |||||
| Control | ARDS | DEX | NCX-1005 | ||
| Total leukocyte count (×106/mL) | |||||
| BV | 2.56 ± 1.72 | 2.54 ± 2.27 | 2.57 ± 1.71 | 2.65 ± 1.59 | |
| 4 h Th | 3.11 ± 2.13 | 1.15 ± 0.61 † | 3.00 ± 0.91 * | 3.13 ± 1.60 * | |
| Differential count (%) | |||||
| Neutrophils | BV | 2.54 ± 1.82 | 2.07 ± 1.58 | 2.04 ± 1.20 | 2.19 ± 2.55 |
| 4 h Th | 56.23 ± 13.68 | 19.59 ± 5.50 †† | 50.64 ± 17.67 ** | 43.90 ± 10.71 * | |
| Lymphocytes | BV | 94.18 ± 3.95 | 96.23 ± 2.51 | 95.47 ± 2.06 | 95.16 ± 3.68 |
| 4 h Th | 42.10 ± 13.26 | 77.43 ± 7.69 †† | 47.59 ± 17.34 ** | 53.98 ± 10.56 * | |
| Monocytes | BV | 1.13 ± 0.55 | 0.93 ± 0.34 | 1.21 ± 0.52 | 0.86 ± 0.29 |
| 4 h Th | 1.32 ± 0.44 | 0.78 ± 0.39 | 1.07 ± 0.60 | 1.01 ± 0.62 | |
| Eosinophils | BV | 0.85 ± 0.71 | 0.96 ± 1.04 | 1.27 ± 1.63 | 1.49 ± 1.43 |
| 4 h Th | 0.36 ± 0.31 | 0.44 ± 0.42 | 0.70 ± 0.55 | 0.94 ± 0.54 | |
| BALF | |||||
| Control | ARDS | DEX | NCX-1005 | ||
| Total count (×103/mL) | 2.29 ± 0.76 | 66.67 ± 20.41 ††† | 8.14 ± 6.34 *** | 9.43 ± 7.00 *** | |
| Monocytes (%) | 96.22 ± 3.18 | 20.43 ± 11.44 ††† | 33.60 ± 28.47 | 55.86 ± 17.49 **@ | |
| Neutrophils (%) | 2.74 ± 2.31 | 76.67 ± 12.08 ††† | 63.50 ± 27.34 | 41.26 ± 18.26 *@ | |
| Eosinophils (%) | 0.85 ± 0.76 | 3.23 ± 1.87 † | 2.74 ± 1.69 | 3.19 ± 1.79 | |
| 3NT | TBARS | IL-1β | TNFα | IL-6 | IL-8 | |
|---|---|---|---|---|---|---|
| Control | 18.1 ± 0.9 | 6.4 ± 2.4 | 14.5 ± 16.7 | 57.5 ± 60.4 | 9.7 ± 6.3 | 424.0 ± 270.9 |
| ARDS | 21.9 ± 4.1 † | 10.0 ± 2.6 †† | 130.8 ± 98.2 † | 251.6 ± 117.7 †† | 88.0 ± 66.9 † | 1050.0 ± 308.7 ††† |
| DEX | 18.3 ± 1.3 | 7.2 ± 0.7 | 81.5 ± 63.1 | 115.2 ± 145.8 | 58.4 ± 62.1 | 677.2 ± 449.1 |
| NCX-1005 | 19.5 ± 2.4 | 7.9 ± 1.1 | 81.3 ± 83.1 | 151.4 ± 80.8 | 66.1 ± 46.5 | 641.7 ± 289.1 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kosutova, P.; Kolomaznik, M.; Calkovska, A.; Mokra, D.; Mikolka, P. Nitric-Oxide-Releasing Dexamethasone Derivative NCX-1005 Improves Lung Function and Attenuates Inflammation in Experimental Lavage-Induced ARDS. Pharmaceutics 2021, 13, 2092. https://doi.org/10.3390/pharmaceutics13122092
Kosutova P, Kolomaznik M, Calkovska A, Mokra D, Mikolka P. Nitric-Oxide-Releasing Dexamethasone Derivative NCX-1005 Improves Lung Function and Attenuates Inflammation in Experimental Lavage-Induced ARDS. Pharmaceutics. 2021; 13(12):2092. https://doi.org/10.3390/pharmaceutics13122092
Chicago/Turabian StyleKosutova, Petra, Maros Kolomaznik, Andrea Calkovska, Daniela Mokra, and Pavol Mikolka. 2021. "Nitric-Oxide-Releasing Dexamethasone Derivative NCX-1005 Improves Lung Function and Attenuates Inflammation in Experimental Lavage-Induced ARDS" Pharmaceutics 13, no. 12: 2092. https://doi.org/10.3390/pharmaceutics13122092