
Population Pharmacokinetics of Meropenem in Critically Ill Korean Patients and Effects of Extracorporeal Membrane Oxygenation

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Patients
2.2. ECMO Apparatus
2.3. Study Design
2.4. Meropenem Assay
2.5. Population PK Analysis
2.6. Assessment of Prediction Performance
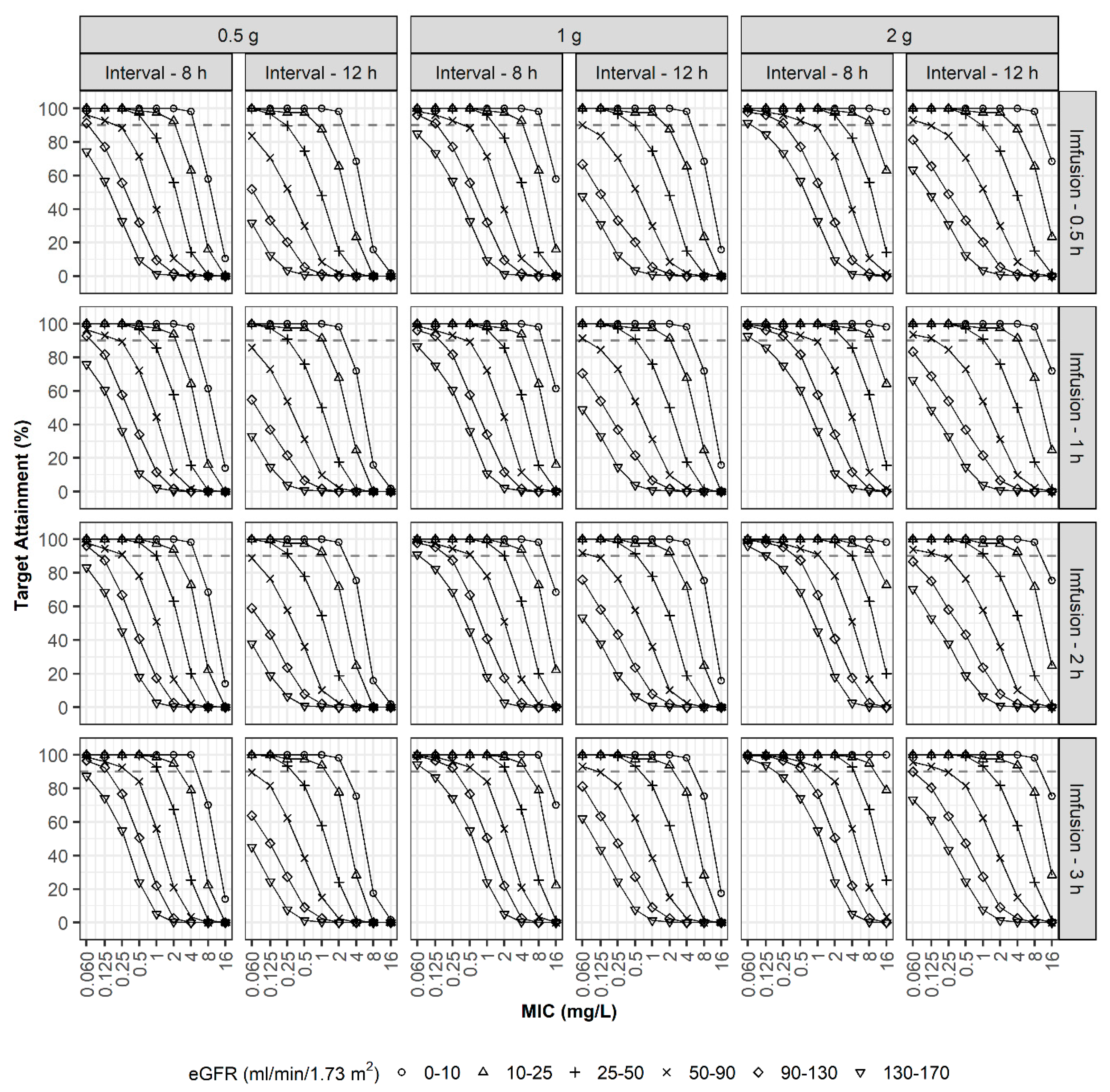
2.7. PD Target Attainment
3. Results
3.1. Patient Characteristics
3.2. Population PK Analysis
3.3. Assessment of Prediction Performance
3.4. PD Target Attainment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Roberts, J.A.; Abdul-Aziz, M.H.; Lipman, J.; Mouton, J.W.; Vinks, A.A.; Felton, T.W.; Hope, W.W.; Farkas, A.; Neely, M.N.; Schentag, J.J.; et al. International society of anti-infective pharmacology and the pharmacokinetics and pharmacodynamics study group of the European Society of Clinical Microbiology and infectious diseases. Individualised antibiotic dosing for patients who are critically ill: Challenges and potential solutions. Lancet Infect. Dis. 2014, 14, 498–509. [Google Scholar] [PubMed] [Green Version]
- Blot, S.I.; Pea, F.; Lipman, J. The effect of pathophysiology on pharmacokinetics in the critically ill patient—Concepts appraised by the example of antimicrobial agents. Adv. Drug Deliv. Rev. 2014, 77, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Goncalves-Pereira, J.; Povoa, P. Antibiotics in critically ill patients: A systematic review of the pharmacokinetics of β-lactams. Crit. Care 2011, 15, R206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mouton, J.W.; van den Anker, J.N. Meropenem clinical pharmacokinetics. Clin. Pharmacokinet. 1995, 28, 275–286. [Google Scholar] [CrossRef]
- Baldwin, C.M.; Lyseng-Williamson, K.A.; Keam, S.J. Meropenem: A review of its use in the treatment of serious bacterial infections. Drugs 2008, 68, 803–838. [Google Scholar] [CrossRef] [PubMed]
- De Rosa, F.G.; Corcione, S.; Pagani, N.; Stella, M.L.; Urbino, R.; Di Perri, G.; Raschke, R.A. High rate of respiratory MDR gram-negative bacteria in H1N1-ARDS treated with ECMO. Intensive Care Med. 2013, 39, 1880–1881. [Google Scholar] [CrossRef]
- Aubron, C.; Cheng, A.C.; Pilcher, D.; Leong, T.; Magrin, G.; Cooper, D.J.; Scheinkestel, C.D.; Pellegrino, V. Infections acquired by adults who receive extracorporeal membrane oxygenation: Risk factors and outcome. Infect. Control Hosp. Epidemiol. 2013, 34, 24–30. [Google Scholar] [CrossRef] [Green Version]
- Shekar, K.; Fraser, J.F.; Smith, M.T.; Roberts, J.A. Pharmacokinetic changes in patients receiving extracorporeal membrane oxygenation. J. Crit. Care 2012, 27, 741.e9–741.e18. [Google Scholar] [CrossRef]
- Ha, M.A.; Sieg, A.C. Evaluation of altered drug pharmacokinetics in critically ill adults receiving extracorporeal membrane oxygenation. Pharmacotherapy 2017, 32, 221–235. [Google Scholar] [CrossRef] [PubMed]
- Shekar, K.; Fraser, J.F.; Taccone, F.S.; Welch, S.; Wallis, S.C.; Mullany, D.V.; Lipman, J.; Roberts, J.A.; ASAP ECMO Study Investigators. The combined effects of extracorporeal membrane oxygenation and renal replacement therapy on meropenem pharmacokinetics: A matched cohort study. Crit. Care 2014, 18, 565. [Google Scholar] [CrossRef] [Green Version]
- Hanberg, P.; Obrink-Hansen, K.; Thorsted, A.; Bue, M.; Tottrup, M.; Friberg, L.E.; Hardlei, T.F.; Søballe, K.; Gjedsted, J. Population pharmacokinetics of meropenem in plasma and subcutis from patients on extracorporeal membrane oxygenation treatment. Antimicrob. Agents Chemother. 2018, 62, e02390-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gijsen, M.; Dreesen, E.; Annaert, P.; Nicolai, J.; Debaveye, Y.; Wauters, J.; Spriet, I. Meropenem pharmacokinetics and target attainment in critically ill patients are not affected by extracorporeal membrane oxygenation: A matched cohort analysis. Microorganisms 2021, 9, 1310. [Google Scholar] [CrossRef]
- Dosne, A.G.; Bergstrand, M.; Karlsson, M.O. A strategy for residual error modeling incorporating scedasticity of variance and distribution shape. J. Pharmacokinet. Pharmacodyn. 2016, 43, 137–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pea, F.; Della Siega, P.; Cojutti, P.; Sartor, A.; Crapis, M.; Scarparo, C.; Bassetti, M. Might real-time pharmacokinetic/pharmacodynamic optimisation of high-dose continuous-infusion meropenem improve clinical cure in infections caused by KPC-producing Klebsiella pneumoniae? Int. J. Antimicrob. Agents 2017, 49, 255–258. [Google Scholar] [CrossRef]
- Heil, E.L.; Nicolau, D.P.; Farkas, A.; Roberts, J.A.; Thom, K.A. Pharmacodynamic target attainment for cefepime, meropenem, and piperacillin-tazobactam using a pharmacokinetic/pharmacodynamic-based dosing calculator in critically ill patients. Antimicrob. Agents Chemother. 2018, 62, e01008-18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liebchen, U.; Klose, M.; Paal, M.; Vogeser, M.; Zoller, M.; Schroeder, I.; Schmitt, L.; Huisinga, W.; Michelet, R.; Zander, J.; et al. Evaluation of the MeroRisk calculator, a use-friendly tool to predict the risk of meropenem target non-attainment in critically ill patients. Antibiotics 2021, 10, 468. [Google Scholar] [CrossRef] [PubMed]
- Kühn, D.; Metz, C.; Seiler, F.; Wehrfritz, H.; Roth, S.; Alqudrah, M.; Becker, A.; Bracht, H.; Wagenpfeil, S.; Hoffmann, M.; et al. Antibiotic therapeutic drug monitoring in intensive care patients treated with different modalities of extracorporeal membrane oxygenation (ECMO) and renal replacement therapy: A prospective, observational single-center study. Crit. Care 2020, 24, 664. [Google Scholar] [CrossRef]
- Patel, T.S.; Nagel, J.L. Clinical outcomes of Enterobacteriaceae infections stratified by carbapenem MICs. J. Clin. Microbiol. 2015, 53, 201–205. [Google Scholar] [CrossRef] [Green Version]
- Esterly, J.S.; Wagner, J.; McLaughlin, M.M.; Postelnick, M.J.; Qi, C.; Scheetz, M.H. Evaluation of clinical outcomes in patients with bloodstream infections due to Gram-negative bacteria according to carbapenem MIC stratification. Antimicrob. Agents Chemother. 2012, 56, 4885–4890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Donnell, J.N.; Rhodes, N.J.; Biehle, L.R.; Esterly, J.S.; Patel, T.S.; McLaughlin, M.M.; Hirsch, E.B. Assessment of mortality stratified by meropenem minimum inhibitory concentration in patients with Enterobacteriaceae bacteremia: A patient-level analysis of published data. Int. J. Antimicrob. Agents 2020, 55, 105849. [Google Scholar] [CrossRef]
- De Waele, J.J.; Akova, M.; Antonelli, M.; Canton, R.; Carlet, J.; De Backer, D.; Dimopoulos, G.; Garnacho-Montero, J.; Kesecioglu, J.; Lipman, J.; et al. Antimicrobial resistance and antibiotic stewardship programs in the ICU: Insistence and persistence in the fight against resistance. A position statement from ESICM/ESCMID/WAAAR round table on multi-drug resistance. Intensive Care Med. 2018, 44, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Sjövall, F.; Alobaid, A.S.; Wallis, S.C.; Perner, A.; Lipman, J.; Roberts, J.A. Maximally effective dosing regimens of meropenem in patients with septic shock. J. Antimicrob. Chemother. 2018, 73, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Lertwattanachai, T.; Montakantikul, P.; Tangsujaritvijit, V.; Sanguanwit, P.; Sueajai, J.; Auparakkitanon, S.; Dilokpattanamongkol, P. Clinical outcomes of empirical high-dose meropenem in critically ill patients with sepsis and septic shock: A randomized controlled trial. J. Intensive Care 2020, 8, 26. [Google Scholar] [CrossRef]
- Kothekar, A.T.; Divatia, J.V.; Myatra, S.N.; Patil, A.; Krishnamurthy, M.N.; Maheshwarappa, H.M.; Siddiqui, S.S.; Gurjar, M.; Biswas, S.; Gota, V. Clinical pharmacokinetics of 3-h extended infusion of meropenem in adult patients with severe sepsis and septic shock: Implications for empirical therapy against Gram-negative bacteria. Ann. Intensive Care 2020, 10, 4. [Google Scholar] [CrossRef] [PubMed]
- Eisert, A.; Lanckohr, C.; Frey, J.; Frey, O.; Wicha, S.G.; Horn, D.; Ellger, B.; Schuerholzi, T.; Marx, G.; Simond, T.-P. Comparison of two empirical prolonged infusion dosing regimens for meropenem in patients with septic shock: A two-center pilot study. Int. J. Antimicrob. Agents 2021, 57, 106289. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, N.; Jen, S.P.; Altshuler, D.; Papadopoulos, J.; Pham, V.P.; Dubrovskaya, Y. Evaluation of meropenem extended versus intermittent infusion dosing protocol in critically ill patients. J. Intensive Care Med. 2020, 35, 763–771. [Google Scholar] [CrossRef]
- Roberts, J.A.; Abdul-Aziz, M.H.; Davis, J.S.; Dulhunty, J.M.; Cotta, M.O.; Myburgh, J.; Bellomo, R.; Lipman, J. Continuous versus intermittent beta-lactam infusion in severe sepsis. A meta-analysis of individual patient data from randomized trials. Am. J. Respir. Crit. Care Med. 2016, 194, 681–691. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.A.; Kirkpatrick, C.M.; Roberts, M.S.; Robertson, T.A.; Dalley, A.J.; Lipman, J. Meropenem dosing in critically ill patients with sepsis and without renal dysfunction: Intermittent bolus versus continuous administration? Monte Carlo dosing simulations and subcutaneous tissue distribution. J. Antimicrob. Chemother. 2009, 64, 142–150. [Google Scholar] [CrossRef] [Green Version]
- Jaruratanasirikul, S.; Thengyai, S.; Wongpoowarak, W.; Wattanavijitkul, T.; Tangkitwanitjaroen, K.; Sukarnjanaset, W.; Jullangkoon, M.; Samaeng, M. Population pharmacokinetics and Monte Carlo dosing simulations of meropenem during the early phase of severe sepsis and septic shock in critically ill patients in intensive care units. Antimicrob. Agents Chemother. 2015, 59, 2995–3001. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.K.; Lee, D.H.; Jeon, J.; Jang, H.J.; Kim, H.K.; Jin, K.; Lim, S.-N.; Lee, S.S.; Park, B.S.; Kim, W.; et al. Population pharmacokinetic analysis of meropenem after intravenous infusion in Korean patients with acute infections. Clin. Ther. 2018, 40, 1384–1395. [Google Scholar] [CrossRef]
- Tsai, D.; Jamal, J.A.; Davis, J.S.; Lipman, J.; Roberts, J.A. Interethnic differences in pharmacokinetics of antibacterials. Clin. Pharmacokinet. 2015, 54, 243–260. [Google Scholar] [CrossRef]
- Kim, K.; Johnson, J.A.; Derendorf, H. Differences in drug pharmacokinetics between East Asians and Caucasians and the role of genetic polymorphisms. J. Clin. Pharmacol. 2004, 44, 1083–1105. [Google Scholar] [CrossRef]
- Isla, A.; Rodriguez-Gascon, A.; Troconiz, I.F.; Bueno, L.; Solinis, M.A.; Maynar, J.; Izquierdo, J.A.; Pedraz, J.L. Population pharmacokinetics of meropenem in critically ill patients undergoing continuous renal replacement therapy. Clin. Pharmacokinet. 2008, 47, 173–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, E.K.; Cheatham, S.C.; Fleming, M.R.; Healy, D.P.; Kays, M.B. Population pharmacokinetics and pharmacodynamics of meropenem in nonobese, obese, and morbidly obese patients. J. Clin. Pharmacol. 2017, 57, 356–368. [Google Scholar] [CrossRef]
- Ehmann, L.; Zoller, M.; Minichmayr, I.K.; Scharf, C.; Huisinga, W.; Zander, J.; Kloft, C. Development of a dosing algorithm for meropenem in critically ill patients based on a population pharmacokinetic/pharmacodynamic analysis. Int. J. Antimicrob. Agents 2019, 54, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Frippiat, F.; Musuamba, F.T.; Seidel, L.; Albert, A.; Denooz, R.; Charlier, C.; Van Bambeke, F.; Wallemacq, P.; Descy, J.; Lambermont, B.; et al. Modelled target attainment after meropenem infusion in patients with severe nosocomial pneumonia: The PROMESSE study. J. Antimicrob. Chemother. 2015, 70, 207–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bloomfield, C.; Staatz, C.E.; Unwin, S.; Hennig, S. Assessing predictive performance of published population pharmacokinetic models of intravenous tobramycin in pediatric patients. Antimicrob. Agents Chemother. 2016, 60, 3407–3414. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | ECMO (n = 8) | Non-ECMO (n = 18) | p-Value |
|---|---|---|---|
| ECMO type | VA 7/VV 1 | ||
| CRRT | Yes 3/No 5 | Yes 1/No 17 | |
| Sex | male 4/female 4 | male 14/female 4 | |
| Age (year) | 64.0 (56.3–66.5) | 72.0 (66.0–80.3) | 0.0167 c |
| Height (cm) | 162 (153–169) | 165 (156–170) | 0.6544 d |
| Weight (kg) | 63.5 (61.9–66.3) | 54.4 (50.5–64.5) | 0.1731 d |
| Body surface area (m2) | 1.67 (1.61–1.75) | 1.63 (1.51–1.72) | 0.5074 c |
| ICU duration (days) | 25.0 (6.00–43.5) | 6.50 (4.00–17.8) | 0.1249 d |
| APACHE II | 21.0 (19.5–22.5) | 16.0 (12.0–18.0) | 0.0321 c |
| SOFA | 9.50 (8.00–12.5) | 5.00 (3.00–7.75) | 0.0051c |
| BUN (mg/dL) | 26.9 (22.0–33.0) | 22.6 (10.8–46.6) | 0.8675 d |
| Scr (mg/dL) | 0.820 (0.518–1.15) | 0.615 (0.458–1.43) | 0.9557 d |
| Cystatin C (mg/dL) | 1.48 (1.43–1.90) | 1.34 (0.985–1.86) | 0.5411 c |
| Albumin (g/dL) | 3.00 (2.83–3.20) | 2.55 (2.30–2.98) | 0.0364 c |
| Protein (g/dL) | 5.15 (4.88–5.75) | 5.05 (4.70–5.75) | 0.5448 d |
| CLCR, Cockcroft-Gault (mL/min) | 76.9 (59.5–105) | 73.4 (32.7–92.6) | 0.4367 d |
| GFR, MDRD (mL/min/1.73 m2) | 86.9 (67.1–132) | 111 (47.5–160) | 0.9119 c |
| GFR, modified MDRD (mL/min) b | 88.7 (67.0–115) | 95.1 (45.0–153) | 0.8676 d |
| GFR, CKD-EPI (mL/min/1.73 m2) | 87.7 (70.0–105) | 91.6 (45.6–103) | 0.7145 c |
| GFR, modified CKD-EPI (mL/min) b | 82.4 (70.0–94.9) | 77.7 (43.6–97.0) | 0.5883 c |
| Parameter | Estimates | RSE (%) [Shrinkage (%)] | Bootstrap Median (95% CI) |
|---|---|---|---|
| Structural model | |||
| CL = θ1 × (1 + θ2 × (CE − 91.57)) | |||
| θ1 (L/h) | 6.37 | 7.41 | 6.32 (5.42–7.23) |
| θ2 | 0.00925 | 10.3 | 0.00932 (0.00680–0.0110) |
| VC (L) | 9.07 | 12.2 | 8.97 (3.92–12.0) |
| Q (L/h) | 10.7 | 21.5 | 10.6 (4.73–31.0) |
| VP (L) | 7.91 | 13.6 | 8.17 (5.35–11.1) |
| Inter-individual variability | |||
| CL (%) | 31.4 | 15.8 [3.70] | 29.9 (18.0–38.7) |
| VC (%) | 43.6 | 22.5 [14.7] | 41.0 (0.000–95.4) |
| VP (%) | 36.6 | 21.0 [41.3] | 34.5 (0.000–55.7) |
| Residual variability | |||
| Proportional error (%) | 24.6 | 29.3 [24.2] | 24.1 (10.3–41.5) |
| Power parameter | 0.865 | 10.0 | 0.897 (0.533–1.38) |
| Parameter | ECMO | non ECMO | p-Value |
|---|---|---|---|
| CL | 6.34 (4.84–7.92) | 5.05 (3.43–7.37) | 0.5782 b |
| VC (L) | 8.37 (7.35–8.89) | 8.53 (7.21–11.7) | 0.6567 c |
| VP (L) | 8.11 (7.75–8.86) | 8.28 (6.55–8.64) | 0.4258 b |
| VSS (L) | 16.2 (15.6–17.9) | 17.2 (14.7–21.0) | 0.6140 b |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, D.-H.; Kim, H.-S.; Park, S.; Kim, H.-i.; Lee, S.-H.; Kim, Y.-K. Population Pharmacokinetics of Meropenem in Critically Ill Korean Patients and Effects of Extracorporeal Membrane Oxygenation. Pharmaceutics 2021, 13, 1861. https://doi.org/10.3390/pharmaceutics13111861
Lee D-H, Kim H-S, Park S, Kim H-i, Lee S-H, Kim Y-K. Population Pharmacokinetics of Meropenem in Critically Ill Korean Patients and Effects of Extracorporeal Membrane Oxygenation. Pharmaceutics. 2021; 13(11):1861. https://doi.org/10.3390/pharmaceutics13111861
Chicago/Turabian StyleLee, Dong-Hwan, Hyoung-Soo Kim, Sunghoon Park, Hwan-il Kim, Sun-Hee Lee, and Yong-Kyun Kim. 2021. "Population Pharmacokinetics of Meropenem in Critically Ill Korean Patients and Effects of Extracorporeal Membrane Oxygenation" Pharmaceutics 13, no. 11: 1861. https://doi.org/10.3390/pharmaceutics13111861