
Lung Deposition of Surfactant Delivered via a Dedicated Laryngeal Mask Airway in Piglets

 ,
,
Abstract
:1. Introduction
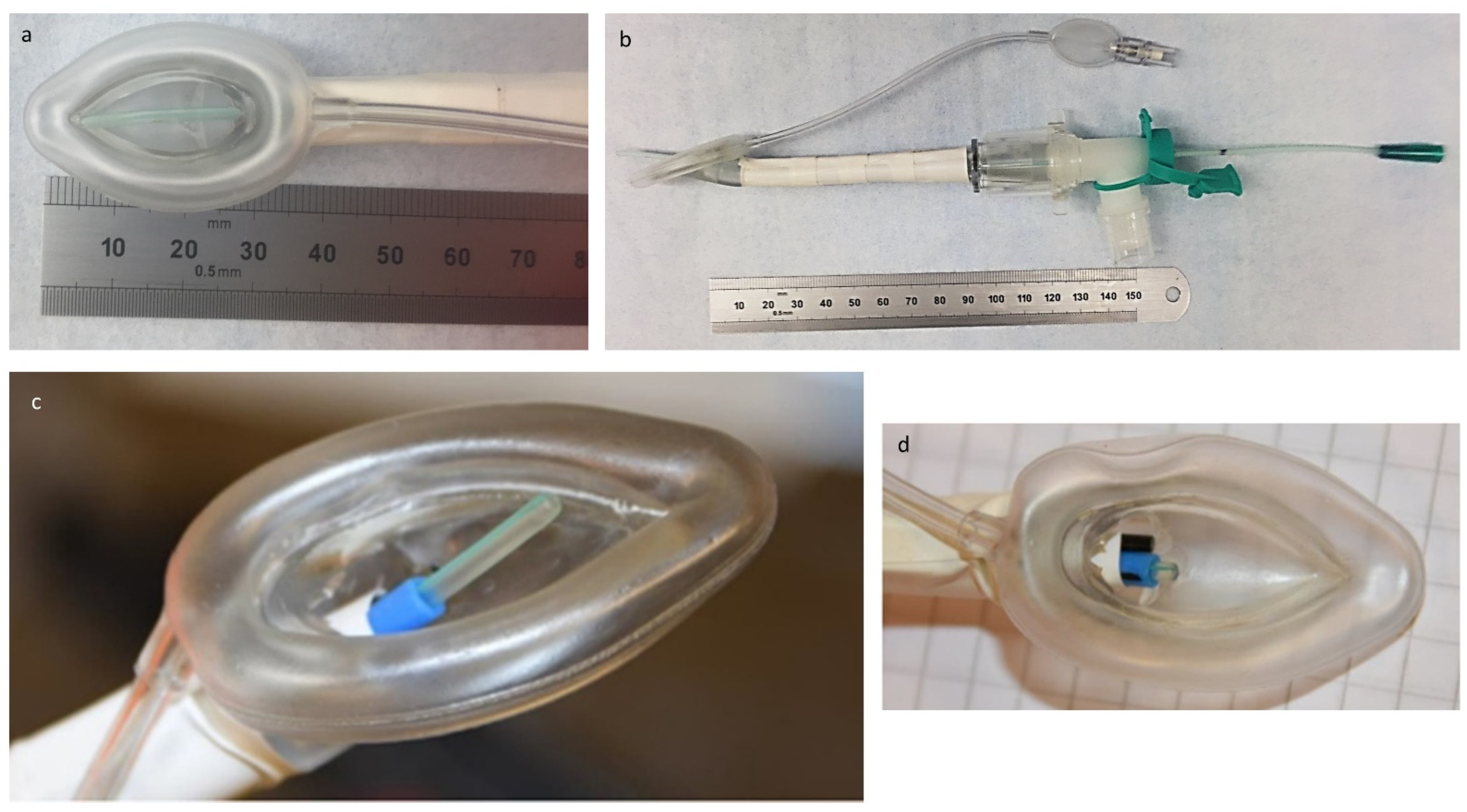
2. Materials and Methods
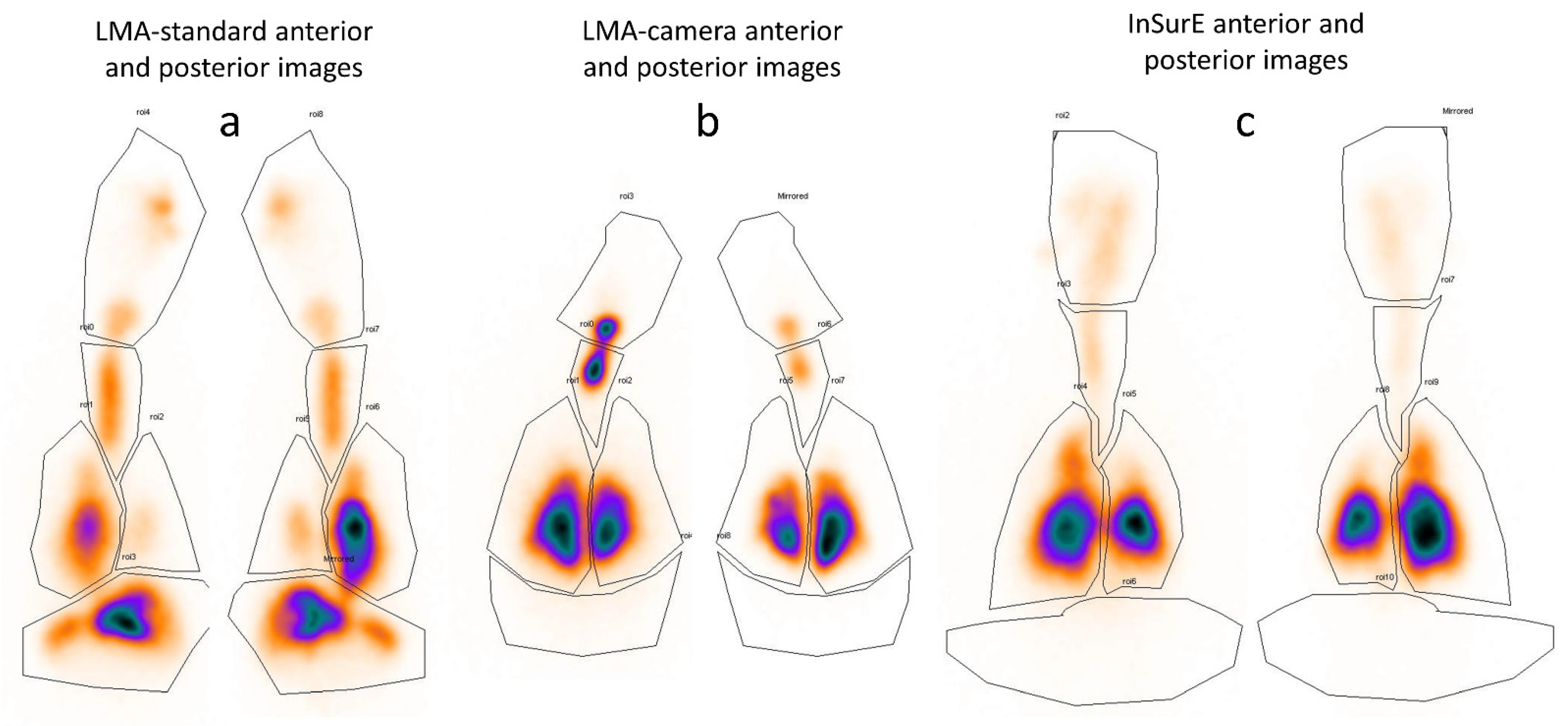
Measurement of Surfactant Deposition and Distribution
3. Results
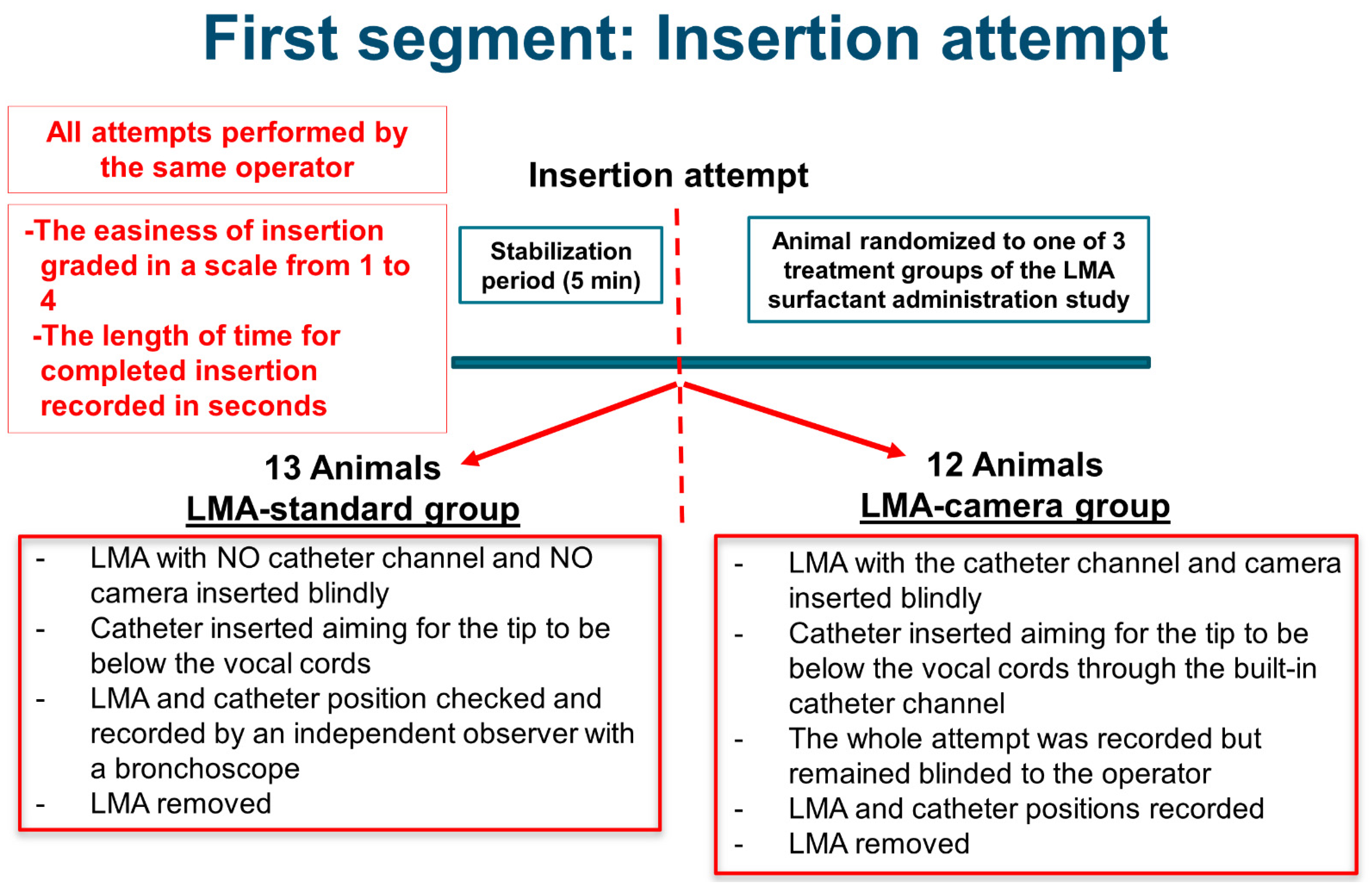
3.1. Insertion Attempt Study
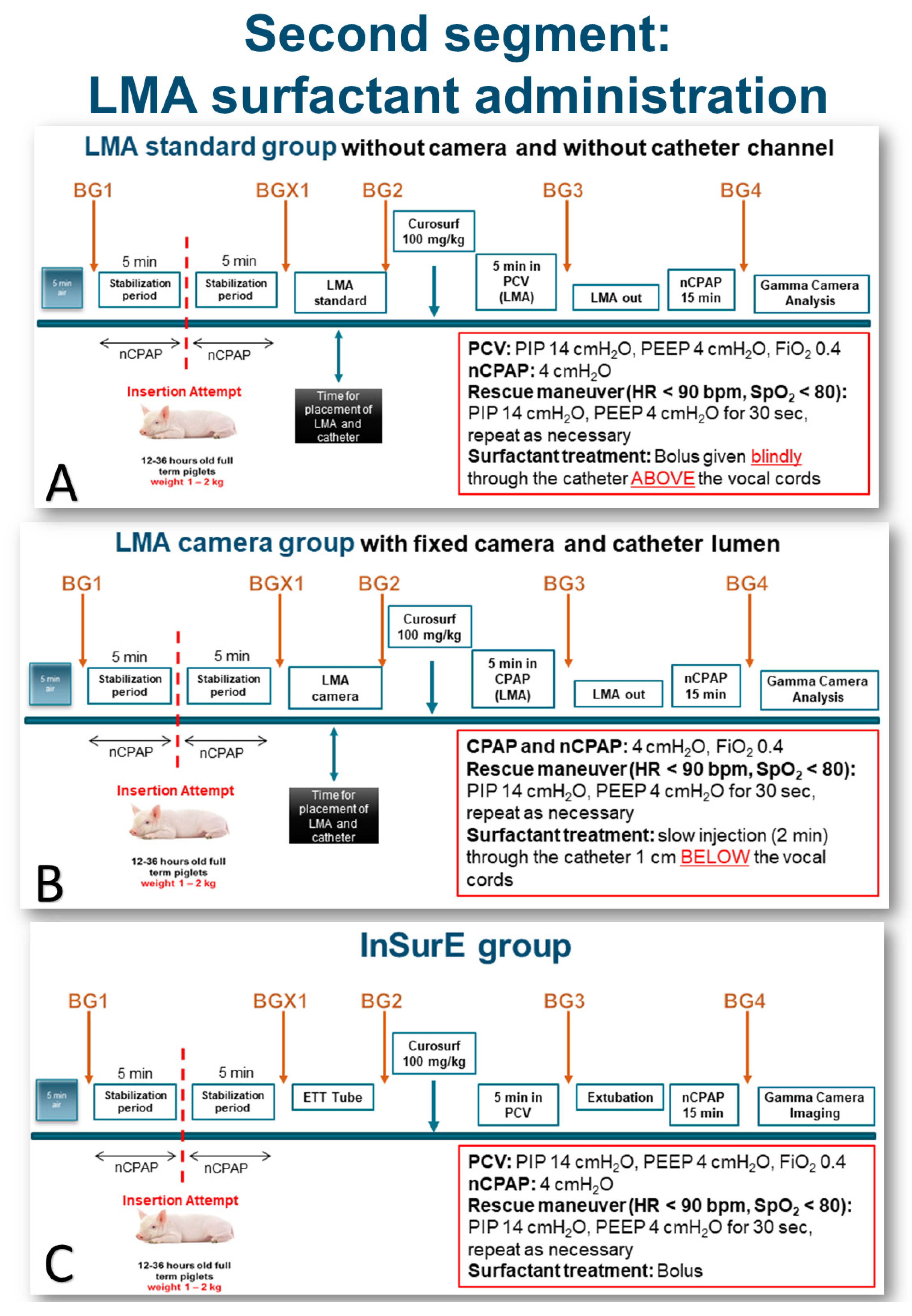
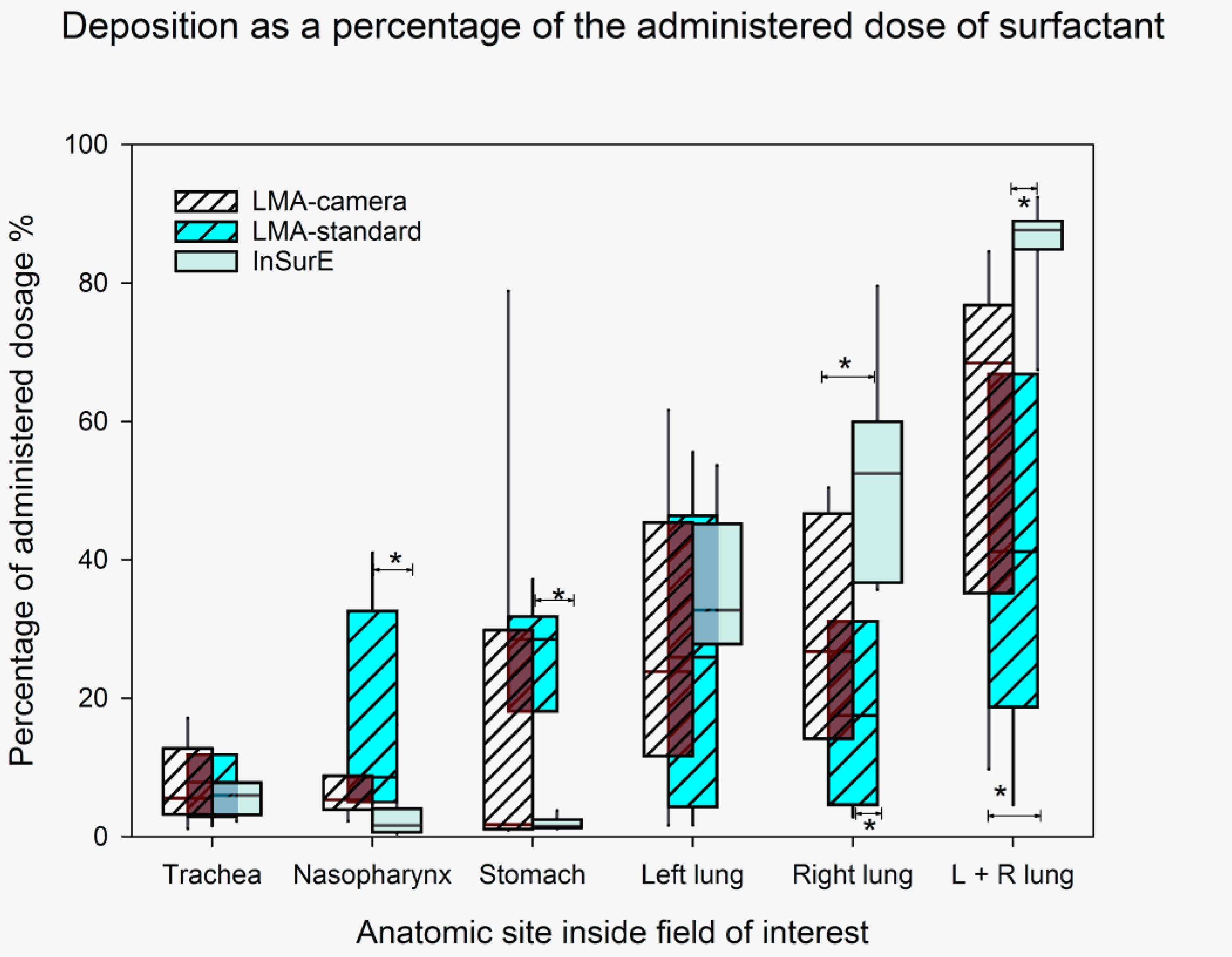
3.2. LMA Surfactant Administration Study
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Avery, M.E.; Mead, J. Surface properties in relation to atelectasis and hyaline membrane disease. AMA J. Dis. Child 1959, 97, 517–523. [Google Scholar] [CrossRef]
- Stoll, B.J.; Hansen, N.I.; Bell, E.F.; Walsh, M.C.; Carlo, W.A.; Shankaran, S.; Laptook, A.R.; Sanchez, P.J.; Van Meurs, K.P.; Wyckoff, M.; et al. Trends in Care Practices, Morbidity, and Mortality of Extremely Preterm Neonates, 1993–2012. JAMA 2015, 314, 1039–1051. [Google Scholar] [CrossRef] [Green Version]
- Dargaville, P.A.; Tingay, D.G. Lung protective ventilation in extremely preterm infants. J. Paediatr. Child Health 2012, 48, 740–746. [Google Scholar] [CrossRef]
- Papile, L. Respiratory support in preterm infants at birth. Pediatrics 2014, 133, 171–174. [Google Scholar] [CrossRef] [Green Version]
- Verder, H.; Agertoft, L.; Albertsen, P.; Christensen, N.C.; Curstedt, T.; Ebbesen, F.; Greisen, G.; Hobolth, N.; Holm, V.; Jacobsen, T.; et al. Surfactant treatment of newborn infants with respiratory distress syndrome primarily treated with nasal continuous positive air pressure. A pilot study. Ugeskr Laeger 1992, 154, 2136–2139. [Google Scholar]
- Herting, E.; Hartel, C.; Gopel, W. Less invasive surfactant administration (LISA): Chances and limitations. Arch. Dis. Child. Fetal Neonatal Ed. 2019, 104, F655–F659. [Google Scholar] [CrossRef] [PubMed]
- Kribs, A.; Roll, C.; Gopel, W.; Wieg, C.; Groneck, P.; Laux, R.; Teig, N.; Hoehn, T.; Bohm, W.; Welzing, L.; et al. Nonintubated Surfactant Application vs Conventional Therapy in Extremely Preterm Infants: A Randomized Clinical Trial. JAMA Pediatr. 2015, 169, 723–730. [Google Scholar] [CrossRef] [PubMed]
- Dargaville, P.A.; Aiyappan, A.; De Paoli, A.G.; Kuschel, C.A.; Kamlin, C.O.; Carlin, J.B.; Davis, P.G. Minimally-invasive surfactant therapy in preterm infants on continuous positive airway pressure. Arch. Dis. Child. Fetal Neonatal Ed. 2013, 98, F122–F126. [Google Scholar] [CrossRef]
- Aldana-Aguirre, J.C.; Pinto, M.; Featherstone, R.M.; Kumar, M. Less invasive surfactant administration versus intubation for surfactant delivery in preterm infants with respiratory distress syndrome: A systematic review and meta-analysis. Arch. Dis. Child. Fetal Neonatal Ed. 2017, 102, F17–F23. [Google Scholar] [CrossRef]
- Panza, R.; Laforgia, N.; Bellos, I.; Pandita, A. Systematic review found that using thin catheters to deliver surfactant to preterm neonates was associated with reduced bronchopulmonary dysplasia and mechanical ventilation. Acta Paediatr. 2020. [Google Scholar] [CrossRef]
- van Esch, B.F.; Stegeman, I.; Smit, A.L. Comparison of laryngeal mask airway vs tracheal intubation: A systematic review on airway complications. J. Clin. Anesth. 2017, 36, 142–150. [Google Scholar] [CrossRef]
- Ghanta, S.; Abdel-Latif, M.E.; Lui, K.; Ravindranathan, H.; Awad, J.; Oei, J. Propofol compared with the morphine, atropine, and suxamethonium regimen as induction agents for neonatal endotracheal intubation: A randomized, controlled trial. Pediatrics 2007, 119, e1248–e1255. [Google Scholar] [CrossRef]
- Cummings, J.J.; Gerday, E.; Minton, S.; Katheria, A.; Albert, G.; Flores-Torres, J.; Famuyide, M.; Lampland, A.; Guthrie, S.; Kuehn, D.; et al. Aerosolized Calfactant for Newborns With Respiratory Distress: A Randomized Trial. Pediatrics 2020, 146. [Google Scholar] [CrossRef]
- Gaertner, V.D.; Bassler, D.; Ruegger, C.M. Does surfactant nebulization prevent early intubation in preterm infants? A protocol for a systematic review and meta-analysis. Syst. Rev. 2021, 10, 9. [Google Scholar] [CrossRef] [PubMed]
- Trevisanuto, D.; Grazzina, N.; Ferrarese, P.; Micaglio, M.; Verghese, C.; Zanardo, V. Laryngeal mask airway used as a delivery conduit for the administration of surfactant to preterm infants with respiratory distress syndrome. Biol. Neonate 2005, 87, 217–220. [Google Scholar] [CrossRef] [PubMed]
- Roberts, C.T.; Manley, B.J.; O’Shea, J.E.; Stark, M.; Andersen, C.; Davis, P.G.; Buckmaster, A. Supraglottic airway devices for administration of surfactant to newborn infants with respiratory distress syndrome: A narrative review. Arch. Dis. Child. Fetal Neonatal Ed. 2021, 106, 336–341. [Google Scholar] [CrossRef] [PubMed]
- Escobedo, M.B.; Shah, B.A.; Song, C.; Makkar, A.; Szyld, E. Recent Recommendations and Emerging Science in Neonatal Resuscitation. Pediatr. Clin. N. Am. 2019, 66, 309–320. [Google Scholar] [CrossRef] [PubMed]
- Aziz, K.; Lee, H.C.; Escobedo, M.B.; Hoover, A.V.; Kamath-Rayne, B.D.; Kapadia, V.S.; Magid, D.J.; Niermeyer, S.; Schmolzer, G.M.; Szyld, E.; et al. 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Pediatrics 2020. [Google Scholar] [CrossRef] [PubMed]
- Kleine-Brueggeney, M.; Gottfried, A.; Nabecker, S.; Greif, R.; Book, M.; Theiler, L. Pediatric supraglottic airway devices in clinical practice: A prospective observational study. BMC Anesthesiol. 2017, 17, 119. [Google Scholar] [CrossRef] [Green Version]
- Calevo, M.G.; Veronese, N.; Cavallin, F.; Paola, C.; Micaglio, M.; Trevisanuto, D. Supraglottic airway devices for surfactant treatment: Systematic review and meta-analysis. J. Perinatol. 2019, 39, 173–183. [Google Scholar] [CrossRef]
- Linner, R.; Perez-de-Sa, V.; Cunha-Goncalves, D. Lung deposition of nebulized surfactant in newborn piglets. Neonatology 2015, 107, 277–282. [Google Scholar] [CrossRef]
- Glantz, S.A. Primer of Biostatistics, 6th ed.; McGraw-Hill: New York, NY, USA, 2005; 520p. [Google Scholar]
- Sweet, D.G.; Carnielli, V.; Greisen, G.; Hallman, M.; Ozek, E.; Te Pas, A.; Plavka, R.; Roehr, C.C.; Saugstad, O.D.; Simeoni, U.; et al. European Consensus Guidelines on the Management of Respiratory Distress Syndrome—2019 Update. Neonatology 2019, 115, 432–451. [Google Scholar] [CrossRef] [Green Version]
- Musharaf, I.; Daspal, S.; Shatzer, J. Is Video Laryngoscopy the Optimal Tool for Successful Intubation in a Neonatal Simulation Setting? A Single-Center Experience. AJP Rep. 2020, 10, e5–e10. [Google Scholar] [CrossRef] [Green Version]
- Herrick, H.M.; Glass, K.M.; Johnston, L.C.; Singh, N.; Shults, J.; Ades, A.; Nadkarni, V.; Nishisaki, A.; Foglia, E.E.; for the NEAR4NEOS Investigators. Comparison of Neonatal Intubation Practice and Outcomes between the Neonatal Intensive Care Unit and Delivery Room. Neonatology 2020, 117, 65–72. [Google Scholar] [CrossRef]
- Smee, N.J.; Boyd, D.; Conetta, H.; O’Shea, J. Laryngeal mask airway surfactant administration: Case series of 60 infants. Arch. Dis. Child. Fetal Neonatal Ed. 2020. [Google Scholar] [CrossRef] [PubMed]
- Efrat, R.; Kadari, A.; Katz, S. The laryngeal mask airway in pediatric anesthesia: Experience with 120 patients undergoing elective groin surgery. J. Pediatr. Surg. 1994, 29, 206–208. [Google Scholar] [CrossRef]
- Madar, J.; Roehr, C.C.; Ainsworth, S.; Ersdal, H.; Morley, C.; Rudiger, M.; Skare, C.; Szczapa, T.; Te Pas, A.; Trevisanuto, D.; et al. European Resuscitation Council Guidelines 2021: Newborn resuscitation and support of transition of infants at birth. Resuscitation 2021, 161, 291–326. [Google Scholar] [CrossRef] [PubMed]
- Wyckoff, M.H.; Wyllie, J.; Aziz, K.; de Almeida, M.F.; Fabres, J.W.; Fawke, J.; Guinsburg, R.; Hosono, S.; Isayama, T.; Kapadia, V.S.; et al. Neonatal Life Support 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Resuscitation 2020, 156, A156–A187. [Google Scholar] [CrossRef]
- Eschen, C. Laryngeal mask used as a guideway for brief access to the inter tracheal space in premature infants. Acta Paediatr. 1992, 81, 1–20. [Google Scholar]
- Roberts, K.D.; Brown, R.; Lampland, A.L.; Leone, T.A.; Rudser, K.D.; Finer, N.N. Laryngeal mask airway for surfactant administration in neonates: A randomized, controlled trial. J. Pediatr. 2018, 193. [Google Scholar] [CrossRef]
- Pinheiro, J.M.B.; Santana-Rivas, Q.; Pezzano, C. Randomized trial of laryngeal mask airway versus endotracheal intubation for surfactant delivery. J. Perinatol. 2016, 36. [Google Scholar] [CrossRef]
- Barbosa, R.F.; Simoes, E.S.A.C.; Silva, Y.P. A randomized controlled trial of the laryngeal mask airway for surfactant administration in neonates. J. Pediatr. 2017, 93, 343–350. [Google Scholar] [CrossRef]
- Sadeghnia, A.; Tanhaei, M.; Mohammadizadeh, M.; Nemati, M. A comparison of surfactant administration through i-gel and ET-tube in the treatment of respiratory distress syndrome in newborns weighing more than 2000 grams. Adv. Biomed. Res. 2014, 3, 160. [Google Scholar] [CrossRef]
- Attridge, J.T.; Stewart, C.; Stukenborg, G.J.; Kattwinkel, J. Administration of rescue surfactant by laryngeal mask airway: Lessons from a pilot trial. Am. J. Perinatol. 2013, 30, 201–206. [Google Scholar] [CrossRef]
- Vannozzi, I.; Ciantelli, M.; Moscuzza, F.; Scaramuzzo, R.T.; Panizza, D.; Sigali, E.; Boldrini, A.; Cuttano, A. Catheter and Laryngeal Mask Endotracheal Surfactant Therapy: The CALMEST approach as a novel MIST technique. J. Matern. Fetal Neonatal Med. 2017, 30, 2375–2377. [Google Scholar] [CrossRef] [PubMed]
- Bonadies, L.; Doglioni, N.; Trevisanuto, D. Catheter and laryngeal mask endotracheal surfactant therapy: Does the mannequin count? J. Matern Fetal Neonatal Med. 2019, 32, 700. [Google Scholar] [CrossRef] [PubMed]
- Gaitini, L.A.; Yanovski, B.; Mustafa, S.; Hagberg, C.A.; Mora, P.C.; Vaida, S.J. A feasibility study using the VivaSight Single Lumen to intubate the trachea through the Fastrach laryngeal mask airway: A preliminary report of 50 cases. Anesth. Analg. 2013, 116, 604–608. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.; Hei, M.; Xue, Z.; Zhao, Y.; Zhang, X.; Wang, C. Effects of less invasive surfactant administration (LISA) via a gastric tube on the treatment of respiratory distress syndrome in premature infants aged 32 to 36 weeks. Medicine 2020, 99, e19216. [Google Scholar] [CrossRef]
- Niemarkt, H.J.; Kuypers, E.; Jellema, R.; Ophelders, D.; Hutten, M.; Nikiforou, M.; Kribs, A.; Kramer, B.W. Effects of less-invasive surfactant administration on oxygenation, pulmonary surfactant distribution, and lung compliance in spontaneously breathing preterm lambs. Pediatr. Res. 2014, 76, 166–170. [Google Scholar] [CrossRef] [Green Version]
- Ricci, F.; Bresesti, I.; LaVerde, P.A.M.; Salomone, F.; Casiraghi, C.; Mersanne, A.; Storti, M.; Catozzi, C.; Tigli, L.; Zecchi, R.; et al. Surfactant lung delivery with LISA and InSurE in adult rabbits with respiratory distress. Pediatr. Res. 2021. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Blood Gas Parameter | Baseline (BG1) | Before Instillation (BG2) | 5 Min after Instillation (BG3) | 20 Min after Instillation (BG4) |
|---|---|---|---|---|
| InSurE (Intubation-Surfactant-Extubation) | ||||
| SaO2 (%) | 98 (93–100) | 100 (98–100) | 99 (93–100) | 97 (85–100) |
| PaO2 (mm Hg) | 65 (56–74) | 91 (67–157) * | 84 (53–126) | 68 (44–107) |
| PaCO2 (kPa) | 38 (32–41) | 38 (28–50) | 31 (26–43) * | 45 (32–53) * |
| pH | 7.54 (7.48–7.58) | 7.53 (7.43–7.58) | 7.56 (7.47–7.69) | 7.46 (7.35–7.52) * |
| LMA-standard (no camera, no catheter channel) | ||||
| SaO2 (%) | 98 (95–100) | 100 (97–100) | 100 (99–100) * | 100 (94–100) |
| PaO2 (mm Hg) | 71 (60–75) | 107 (83–180) * | 110 (73–193) | 101 (55–171) |
| PaCO2 (mm Hg) | 36 (32–47) | 39 (35–52) | 32 (22–42) | 39 (36–59) |
| pH | 7.54 (7.45–7.56) | 7.51 (7.38–7.58) | 7.61 (7.50–7.75) * | 7.48 (7.36–7.58) |
| LMA-camera (with built-in camera and catheter channel) | ||||
| SaO2 (%) | 97 (86–100) | 100 (92–100) | 96 (76–100) | 97 (95–100) |
| PaO2 (mm Hg) | 62 (44–71) | 92 (62–151) * | 65 (45–119) † | 71 (59–157) |
| PaCO2 (mm Hg) | 39 (37–44) | 50 (39–64) *,† | 52 (32–75) *,† | 42 (36–53) |
| pH | 7.48 (7.45–7.56) | 7.41 (7.33–7.51) † | 7.38 (7.33–7.51) † | 7.45 (7.39–7.55) |
| Group | Trachea | Nasopharynx | Stomach | Left Lung | Right Lung | Both Lungs |
|---|---|---|---|---|---|---|
| LMA-camera % | 5.6 (1.2–17.2) | 5.4 (2.3–12.5) | 1.8 (1–78.9) | 23.9 (1.7–61.7) | 26.8 * (5.3–50.5) | 68.5 * (9.8–84.6) |
| LMA-standard % | 8 (2.9–12.8) | 8.7 * (3.3–41.1) | 28.6 * (1.6–37.2) | 26 (1.7–55.6) | 17.6 * (2.9–42.7) | 41.2 * (4.6–88) |
| InSurE % | 6 (2.3–9.1) | 1.7 (0.5–16.2) | 1.6 (1.2–3.9) | 32.8 (8.2–53.7) | 52.5 (35.7–79.6) | 87.7 (67.5–92.4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nord, A.; Cunha-Goncalves, D.; Linnér, R.; Bianco, F.; Salomone, F.; Ricci, F.; Lombardini, M.; Micaglio, M.; Trevisanuto, D.; Perez-de-Sa, V. Lung Deposition of Surfactant Delivered via a Dedicated Laryngeal Mask Airway in Piglets. Pharmaceutics 2021, 13, 1858. https://doi.org/10.3390/pharmaceutics13111858
Nord A, Cunha-Goncalves D, Linnér R, Bianco F, Salomone F, Ricci F, Lombardini M, Micaglio M, Trevisanuto D, Perez-de-Sa V. Lung Deposition of Surfactant Delivered via a Dedicated Laryngeal Mask Airway in Piglets. Pharmaceutics. 2021; 13(11):1858. https://doi.org/10.3390/pharmaceutics13111858
Chicago/Turabian StyleNord, Anders, Doris Cunha-Goncalves, Rikard Linnér, Federico Bianco, Fabrizio Salomone, Francesca Ricci, Marta Lombardini, Massimo Micaglio, Daniele Trevisanuto, and Valeria Perez-de-Sa. 2021. "Lung Deposition of Surfactant Delivered via a Dedicated Laryngeal Mask Airway in Piglets" Pharmaceutics 13, no. 11: 1858. https://doi.org/10.3390/pharmaceutics13111858