
Infliximab Efficacy May Be Linked to Full TNF-α Blockade in Peripheral Compartment—A Double Central-Peripheral Target-Mediated Drug Disposition (TMDD) Model

 , , ,
, , ,
Abstract
:
1. Introduction
2. Methods
2.1. Data
- -
- A bicentric study of 26 ankylosing spondylitis (AS) patients (SPAXIM, NCT00607403). Inclusion and exclusion criteria were previously described [21]. Patients were treated with infliximab 5 mg/kg infusions at weeks 0, 2, 6, 12, and 18; blood samples were collected to measure infliximab concentrations before, 2 and 4 h after each infusion, and at each intermediate visit at weeks 1, 3, 4, 5, 8, 10, and 14 [21]. One patient was not assessed in the present work because he developed anti-drug antibodies (ADA) starting from the second infliximab administration;
- -
- A retrospective cohort of 133 routine IBD patients treated with infliximab between 2006 and 2012 in the Tours University Hospital (Tours, France). For these patients, individual results were interpreted, sent to the prescriber and discussed in clinic-biological rounds. Infliximab concentrations were therefore not sought for this study and were already used in previous publications [22,23]. This cohort included patients with trough and peak infliximab concentrations measured during treatment initiation and in whom anti-drug antibodies (ADA) were not detected at least within the three first infliximab cycles. Patients were excluded if less than three concentration values were available (which excluded seven patients of our database between 2006 and 2012), if no peak concentrations were available (which excluded two more patients) and if ADA were detected at first, second of third cycles (which excluded three more patients). Of note, if ADA were detected starting for the fourth cycle, patients were not excluded from analysis, but data regarding cycles with ADA were discarded (eight patients).
2.2. Model Development
2.2.1. Structural Model Design
- 1.
- Bicompartimental: two-compartment model with no target interaction;
- 2.
- Central TMDD: two-compartment model with target interaction in central compartment;
- 3.
- Peripheral TMDD: two-compartment model with target interaction in peripheral compartment;
- 4.
- Double TMDD: two-compartment model with target interaction in both central and peripheral compartments.
2.2.2. Statistical Models
- Interindividual and error models
- Influence of covariates
2.2.3. Model Evaluation
- Model comparison
- Model goodness of fit
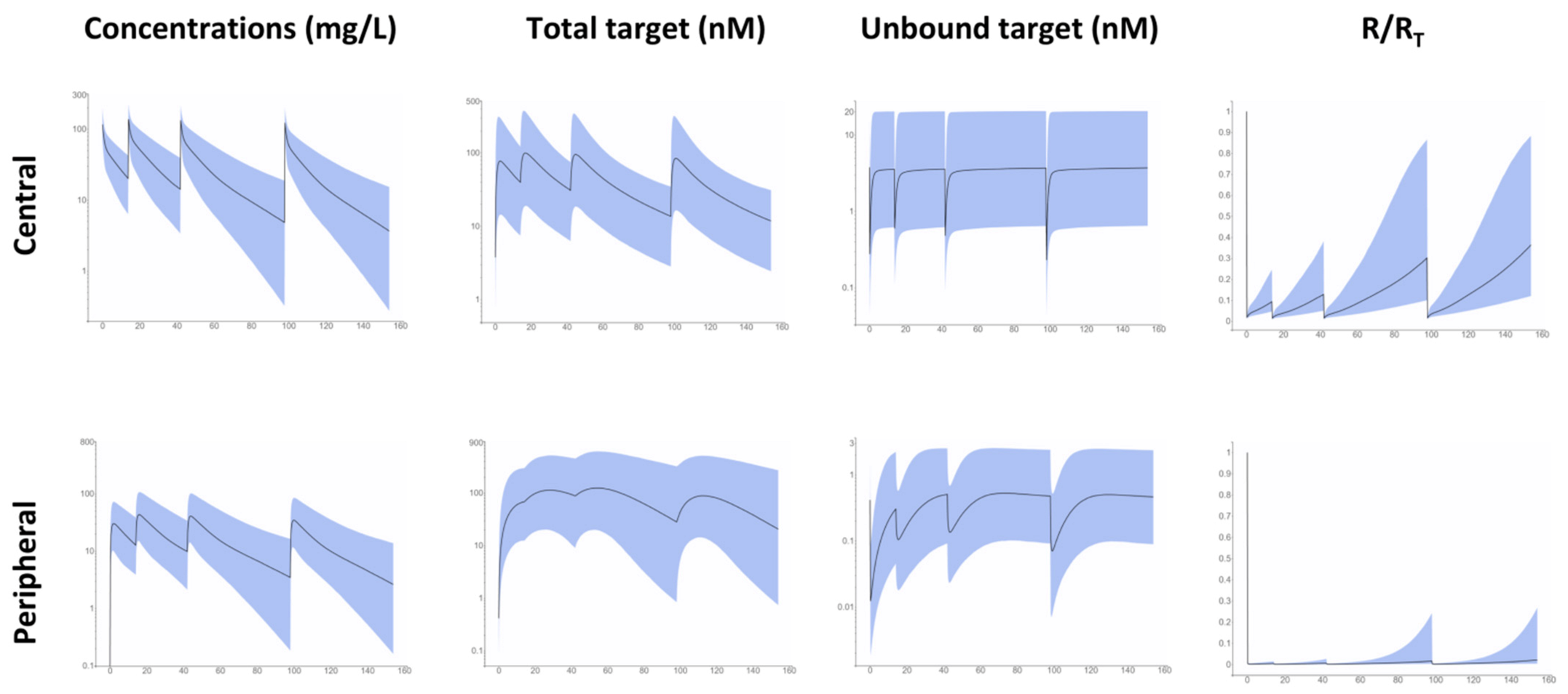
2.3. Simulations
3. Results
3.1. Base Model
3.2. Final Model
3.3. Simulations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
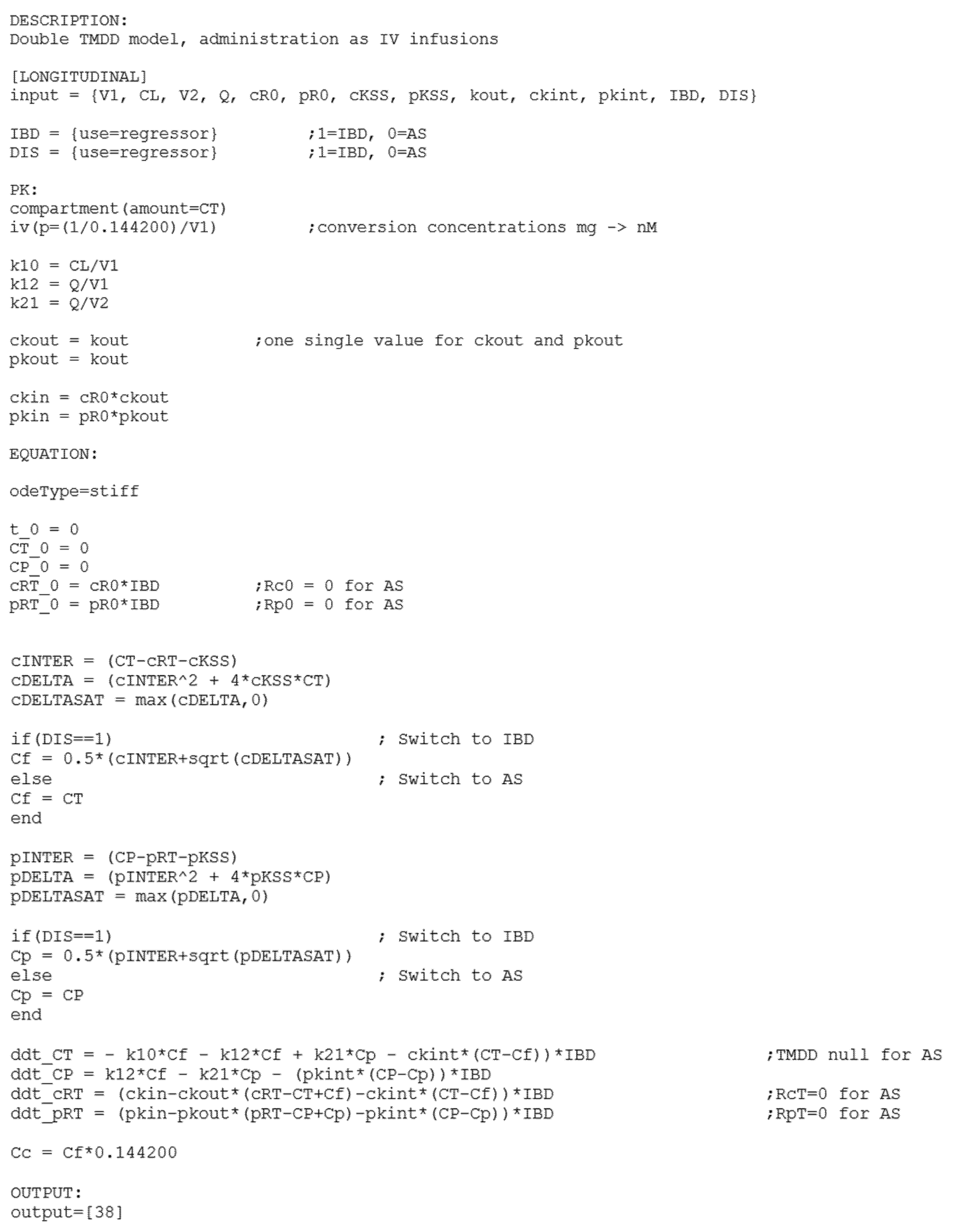
Appendix A. Monolix Code for Double TMDD Model

References
- Paintaud, G.; Passot, C.; Ternant, D.; Bertolotto, A.; Bejan-Angoulvant, T.; Pascual-Salcedo, D.; Mulleman, D. Rationale for Therapeutic Drug Monitoring of Biopharmaceuticals in Inflammatory Diseases. Ther. Drug Monit. 2017, 39, 339–343. [Google Scholar] [CrossRef] [PubMed]
- Eser, A.; Primas, C.; Reinisch, S.; Vogelsang, H.; Novacek, G.; Mould, D.R.; Reinisch, W. Prediction of Individual Serum Infliximab Concentrations in Inflammatory Bowel Disease by a Bayesian Dashboard System. J. Clin. Pharm. 2018, 58, 790–802. [Google Scholar] [CrossRef] [PubMed]
- Ternant, D.; Passot, C.; Aubourg, A.; Goupille, P.; Desvignes, C.; Picon, L.; Lecomte, T.; Mulleman, D.; Paintaud, G. Model-Based Therapeutic Drug Monitoring of Infliximab Using a Single Serum Trough Concentration. Clin. Pharm. 2017, 2017, 017–0621. [Google Scholar] [CrossRef] [PubMed]
- Xiong, Y.; Mizuno, T.; Colman, R.; Hyams, J.; Noe, J.D.; Boyle, B.; Tsai, Y.T.; Dong, M.; Jackson, K.; Punt, N.; et al. Real-World Infliximab Pharmacokinetic Study Informs an Electronic Health Record-Embedded Dashboard to Guide Precision Dosing in Children with Crohn’s Disease. Clin. Pharm. Ther. 2021, 109, 1639–1647. [Google Scholar] [CrossRef]
- Kaymakcalan, Z.; Sakorafas, P.; Bose, S.; Scesney, S.; Xiong, L.; Hanzatian, D.K.; Salfeld, J.; Sasso, E.H. Comparisons of affinities, avidities, and complement activation of adalimumab, infliximab, and etanercept in binding to soluble and membrane tumor necrosis factor. Clin. Immunol. 2009, 131, 308–316. [Google Scholar] [CrossRef]
- Kim, M.S.; Lee, S.H.; Song, M.Y.; Yoo, T.H.; Lee, B.K.; Kim, Y.S. Comparative analyses of complex formation and binding sites between human tumor necrosis factor-alpha and its three antagonists elucidate their different neutralizing mechanisms. J. Mol. Biol. 2007, 374, 1374–1388. [Google Scholar] [CrossRef]
- Scallon, B.; Cai, A.; Solowski, N.; Rosenberg, A.; Song, X.Y.; Shealy, D.; Wagner, C. Binding and functional comparisons of two types of tumor necrosis factor antagonists. J Pharm. Exp. Ther. 2002, 301, 418–426. [Google Scholar] [CrossRef] [Green Version]
- MacDonald, T.T.; Hutchings, P.; Choy, M.Y.; Murch, S.; Cooke, A. Tumour necrosis factor-alpha and interferon-gamma production measured at the single cell level in normal and inflamed human intestine. Clin. Exp. Immunol. 1990, 81, 301–305. [Google Scholar] [CrossRef]
- Murch, S.H.; Lamkin, V.A.; Savage, M.O.; Walker-Smith, J.A.; MacDonald, T.T. Serum concentrations of tumour necrosis factor alpha in childhood chronic inflammatory bowel disease. Gut 1991, 32, 913–917. [Google Scholar] [CrossRef] [Green Version]
- Schulz, M.; Dotzlaw, H.; Neeck, G. Ankylosing spondylitis and rheumatoid arthritis: Serum levels of TNF-α and Its soluble receptors during the course of therapy with etanercept and infliximab. BioMed Res. Int. 2014, 2014, 24. [Google Scholar] [CrossRef] [Green Version]
- Ternant, D.; Pfister, M.; Le Tilly, O.; Mulleman, D.; Picon, L.; Willot, S.; Passot, C.; Bejan-Angoulvant, T.; Lecomte, T.; Paintaud, G.; et al. Infliximab Treatment Does Not Lead to Full TNF-α Inhibition: A Target-Mediated Drug Disposition Model. Clin. Pharm. 2021, 2021, 021–01057. [Google Scholar]
- Buhl, S.; Dorn-Rasmussen, M.; Brynskov, J.; Ainsworth, M.A.; Bendtzen, K.; Klausen, P.H.; Bolstad, N.; Warren, D.J.; Steenholdt, C. Therapeutic thresholds and mechanisms for primary non-response to infliximab in inflammatory bowel disease. Scand. J. Gastroenterol. 2020, 55, 884–890. [Google Scholar] [CrossRef]
- Deora, A.; Hegde, S.; Lee, J.; Choi, C.H.; Chang, Q.; Lee, C.; Eaton, L.; Tang, H.; Wang, D.; Lee, D.; et al. Transmembrane TNF-dependent uptake of anti-TNF antibodies. MAbs 2017, 9, 680–695. [Google Scholar] [CrossRef]
- Olesen, C.M.; Coskun, M.; Peyrin-Biroulet, L.; Nielsen, O.H. Mechanisms behind efficacy of tumor necrosis factor inhibitors in inflammatory bowel diseases. Pharm. Ther. 2016, 159, 110–119. [Google Scholar] [CrossRef]
- Mager, D.E.; Jusko, W.J. General pharmacokinetic model for drugs exhibiting target-mediated drug disposition. J. Pharm. Pharmacodyn. 2001, 28, 507–532. [Google Scholar] [CrossRef]
- Ternant, D.; Azzopardi, N.; Raoul, W.; Bejan-Angoulvant, T.; Paintaud, G. Influence of Antigen Mass on the Pharmacokinetics of Therapeutic Antibodies in Humans. Clin. Pharm. 2019, 58, 169–187. [Google Scholar] [CrossRef]
- Berends, S.E.; van Steeg, T.J.; Ahsman, M.J.; Singh, S.; Brandse, J.F.; D’Haens, G.; Mathôt, R.A.A. Tumor necrosis factor-mediated disposition of infliximab in ulcerative colitis patients. J. Pharm. Pharm. 2019, 46, 543–551. [Google Scholar] [CrossRef] [Green Version]
- Furuya, Y.; Ozeki, T.; Takayanagi, R.; Yokoyama, H.; Okuyama, K.; Yamada, Y. Theory based analysis of anti-inflammatory effect of infliximab on Crohn’s disease. Drug Metab. Pharmacokinet. 2007, 22, 20–25. [Google Scholar] [CrossRef]
- Kimura, K.; Takayanagi, R.; Yokoyama, H.; Yamada, Y. Theory-based analysis of anti-inflammatory effect of infliximab on Crohn’s disease and rheumatoid arthritis. Rheumatol. Int. 2012, 32, 145–150. [Google Scholar] [CrossRef]
- Kimura, K.; Yoshida, A.; Katagiri, F.; Takayanagi, R.; Yamada, Y. Prediction of clinical effects of infliximab administered for inflammatory bowel disease based on pharmacokinetic and pharmacodynamic modeling. Biopharm. Drug Dispos. 2019, 40, 250–261. [Google Scholar] [CrossRef]
- Ternant, D.; Mulleman, D.; Lauferon, F.; Vignault, C.; Ducourau, E.; Wendling, D.; Goupille, P.; Paintaud, G. Influence of methotrexate on infliximab pharmacokinetics and pharmacodynamics in ankylosing spondylitis. Br. J. Clin. Pharm. 2011, 2011, 1365–2125. [Google Scholar] [CrossRef] [Green Version]
- Aubourg, A.; Picon, L.; Lecomte, T.; Bejan-Angoulvant, T.; Paintaud, G.; Ternant, D. A robust estimation of infliximab pharmacokinetic parameters in Crohn’s disease. Eur. J. Clin. Pharm. 2015, 71, 1541–1542. [Google Scholar] [CrossRef]
- Ternant, D.; Aubourg, A.; Magdelaine-Beuzelin, C.; Degenne, D.; Watier, H.; Picon, L.; Paintaud, G. Infliximab pharmacokinetics in inflammatory bowel disease patients. Ther. Drug Monit. 2008, 30, 523–529. [Google Scholar] [CrossRef]
- Ternant, D.; Mulleman, D.; Degenne, D.; Willot, S.; Guillaumin, J.M.; Watier, H.; Goupille, P.; Paintaud, G. An enzyme-linked immunosorbent assay for therapeutic drug monitoring of infliximab. Ther. Drug Monit. 2006, 28, 169–174. [Google Scholar] [CrossRef]
- Dua, P.; Hawkins, E.; van der Graaf, P.H. A Tutorial on Target-Mediated Drug Disposition (TMDD) Models. CPT Pharmacomet. Syst. Pharm. 2015, 4, 324–337. [Google Scholar] [CrossRef]
- Gibiansky, L.; Gibiansky, E. Target-mediated drug disposition model: Approximations, identifiability of model parameters and applications to the population pharmacokinetic-pharmacodynamic modeling of biologics. Expert Opin. Drug Metab Toxicol. 2009, 5, 803–812. [Google Scholar] [CrossRef]
- Ternant, D.; Picon, L.; Cartron, G.; Mulleman, D.; Campone, M.; Merlin, J.; Goupille, P.; Büchler, M.; Lecomte, T.; Paintaud, G. Revisiting Target-Mediated Elimination of Therapeutic Antibodies: The Irreversible Binding Approximation. PAGE 28 (2019) Abstr 9169. Available online: www.page-meeting.org/?abstract=9169 (accessed on 18 October 2021).
- Creaven, P.J.; Plager, J.E.; Dupere, S.; Huben, R.P.; Takita, H.; Mittelman, A.; Proefrock, A. Phase I clinical trial of recombinant human tumor necrosis factor. Cancer Chemother. Pharmacol. 1987, 20, 137–144. [Google Scholar] [CrossRef]
- Greischel, A.; Zahn, G. Pharmacokinetics of recombinant human tumor necrosis factor alpha in rhesus monkeys after intravenous administration. J. Pharm. Exp. Ther. 1989, 251, 358–361. [Google Scholar]
- Zahn, G.; Greischel, A. Pharmacokinetics of tumor necrosis factor alpha after intravenous administration in rats. Dose dependence and influence of tumor necrosis factor beta. Arzneimittelforschung 1989, 39, 1180–1182. [Google Scholar]
- Beutler, B.A.; Milsark, I.W.; Cerami, A. Cachectin/tumor necrosis factor: Production, distribution, and metabolic fate in vivo. J. Immunol. 1985, 135, 3972–3977. [Google Scholar]
- Bensalem, A.; Ternant, D. Pharmacokinetic Variability of Therapeutic Antibodies in Humans: A Comprehensive Review of Population Pharmacokinetic Modeling Publications. Clin Pharm. 2020. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Le Tilly, O.; Bejan-Angoulvant, T.; Paintaud, G.; Ternant, D. Letter to Dreesen et al. on their article “Modelling of the Relationship Between Infliximab Exposure, Faecal Calprotectin, and Endoscopic Remission in Patients With Crohn’s Disease”-A comprehensive review of infliximab population pharmacokinetic modelling publications. Br. J. Clin. Pharm. 2021, 2020, 14554. [Google Scholar]
- Kimura, K.; Takayanagi, R.; Yokoyama, H.; Yamada, Y. Theory-based analysis of the anti-inflammatory effect of TNF inhibitors on rheumatoid arthritis. Drug 2014, 29, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Peletier, L.A.; Gabrielsson, J. Dynamics of target-mediated drug disposition: Characteristic profiles and parameter identification. J. Pharm. Pharm. 2012, 39, 429–451. [Google Scholar] [CrossRef] [Green Version]
- Smith, R.A.; Kirstein, M.; Fiers, W.; Baglioni, C. Species specificity of human and murine tumor necrosis factor. A comparative study of tumor necrosis factor receptors. J. Biol. Chem. 1986, 261, 14871–14874. [Google Scholar] [CrossRef]
- van Schie, K.A.; Ooijevaar-de Heer, P.; Dijk, L.; Kruithof, S.; Wolbink, G.; Rispens, T. Therapeutic TNF Inhibitors can Differentially Stabilize Trimeric TNF by Inhibiting Monomer Exchange. Sci. Rep. 2016, 6, 32747. [Google Scholar] [CrossRef] [Green Version]
- Corti, A.; Fassina, G.; Marcucci, F.; Barbanti, E.; Cassani, G. Oligomeric tumour necrosis factor alpha slowly converts into inactive forms at bioactive levels. Biochem. J. 1992, 284, 905–910. [Google Scholar] [CrossRef] [Green Version]
- Lim, H.; Lee, S.H.; Lee, H.T.; Lee, J.U.; Son, J.Y.; Shin, W.; Heo, Y.S. Structural Biology of the TNF-α Antagonists Used in the Treatment of Rheumatoid Arthritis. Int. J. Mol. Sci. 2018, 19, 768. [Google Scholar] [CrossRef] [Green Version]
- Daub, H.; Traxler, L.; Ismajli, F.; Groitl, B.; Itzen, A.; Rant, U. The trimer to monomer transition of Tumor Necrosis Factor-Alpha is a dynamic process that is significantly altered by therapeutic antibodies. Sci. Rep. 2020, 10, 9265. [Google Scholar] [CrossRef]
- Tran, B.N.; Chan, S.L.; Ng, C.; Shi, J.; Correia, I.; Radziejewski, C.; Matsudaira, P. Higher order structures of Adalimumab, Infliximab and their complexes with TNFα revealed by electron microscopy. Protein Sci. 2017, 26, 2392–2398. [Google Scholar] [CrossRef]
- Ait-Oudhia, S.; Ovacik, M.A.; Mager, D.E. Systems pharmacology and enhanced pharmacodynamic models for understanding antibody-based drug action and toxicity. MAbs 2017, 9, 15–28. [Google Scholar] [CrossRef] [Green Version]
- Konecki, C.; Feliu, C.; Cazaubon, Y.; Giusti, D.; Tonye-Libyh, M.; Brixi, H.; Cadiot, G.; Biron, A.; Djerada, Z. External Evaluation of Population Pharmacokinetic Models and Bayes-Based Dosing of Infliximab. Pharmaceutics 2021, 13, 1191. [Google Scholar] [CrossRef]
- Passot, C.; Mulleman, D.; Bejan-Angoulvant, T.; Aubourg, A.; Willot, S.; Lecomte, T.; Picon, L.; Goupille, P.; Paintaud, G.; Ternant, D. The underlying inflammatory chronic disease influences infliximab pharmacokinetics. MAbs 2016, 8, 1407–1416. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | AS Cohort | IBD Cohort |
|---|---|---|
| Number of patients | 25 | 133 |
| Number of samples | 488 | 845 |
| Starting dose (mg) | 400 (300–400) | 300 (280–370) |
| Body weight (kg) | 75 (65–85) | 64 (56–72) |
| Age (years) | 43 (35–52) | 34 (25–41) |
| Sex (females/males) | 6/19 | 53/80 |
| Ankylosing spondylitis | 25 | ─ |
| Crohn’s disease | ─ | 108 |
| Ulcerative colitis | ─ | 25 |
| Parameter | Unit | Model | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Base 2 Compartments | Base TMDD Peripheral | Base TMDD Central | Base TMDD Central + Peripheral | Final TMDD Central + Peripheral | |||||||
| Estimate | RSE% | Estimate | RSE% | Estimate | RSE% | Estimate | RSE% | Estimate | RSE% | ||
| V1 | L | 3.0 | 2.4 | 2.8 | 2.6 | 2.9 | 2.5 | 2.8 | 2.5 | 2.6 | 3.3 |
| CL | L.day−1 | 0.29 | 7.9 | 0.28 | 4.0 | 0.18 | 7.1 | 0.20 | 6.7 | 0.16 | 9.3 |
| V2 | L | 2.2 | 6.9 | 1.8 | 8.3 | 1.9 | 9.8 | 1.9 | 11 | 1.9 | 8.8 |
| Q | L.day−1 | 0.29 | 5.1 | 1.6 | 6.6 | 0.30 | 7.8 | 1.5 | 2.2 | 1.8 | 2.0 |
| KCSS | nM | ─ | ─ | ─ | ─ | 13.5 | 8.8 | 13.7 | 16 | 15.4 | 21 |
| RC0 | nM | ─ | ─ | ─ | ─ | 7.2 | 21 | 2.6 | 21 | 3.3 | 28 |
| kCint | day−1 | ─ | ─ | ─ | ─ | 0.089 | 11 | 0.13 | 17 | 0.17 | 11 |
| KPSS | nM | ─ | ─ | 0.49 | 5.5 | ─ | ─ | 0.45 | 5.1 | 0.49 | 11 |
| RP0 | nM | ─ | ─ | 0.68 | 25 | ─ | ─ | 0.30 | 9.2 | 0.46 | 22 |
| kPint | day−1 | ─ | ─ | 0.013 | 37 | ─ | ─ | 0.0050 | 33 | 0.0079 | 36 |
| kout | day−1 | ─ | ─ | 20 | (fixed) | 20 | (fixed) | 20 | (fixed) | 20 | (fixed) |
| BW_V1 | ─ | ─ | ─ | ─ | ─ | ─ | ─ | ─ | ─ | 0.33 | 35 |
| SX_V1 | ─ | ─ | ─ | ─ | ─ | ─ | ─ | ─ | ─ | 0.13 | 40 |
| SX_CL | ─ | ─ | ─ | ─ | ─ | ─ | ─ | ─ | ─ | 0.36 | 26 |
| UC_RC0 | ─ | ─ | ─ | ─ | ─ | ─ | ─ | ─ | ─ | 0.57 | 47 |
| ωV1 | ─ | 0.28 | 6.8 | 0.29 | 6.8 | 0.26 | 7.0 | 0.29 | 6.8 | 0.27 | 7.0 |
| ωCL | ─ | 0.46 | 6.2 | 0.50 | 7.0 | 0.38 | 15 | 0.38 | 13.0 | 0.35 | 13 |
| ωV2 | ─ | 0.62 | 9.8 | 0.32 | 24 | 0.71 | 12 | 0.36 | 24 | 0.39 | 25 |
| ωRC0 | ─ | ─ | ─ | ─ | ─ | 0.98 | 15 | 1.0 | 14 | 1.0 | 15 |
| ωRP0 | ─ | ─ | ─ | 0.31 | 6.8 | ─ | ─ | 1.2 | 20 | 1.1 | 16 |
| σadd | mg/L | 1.8 | 10 | 1.8 | 11 | 1.9 | 10 | 1.8 | 9.8 | 1.8 | 9.8 |
| σprop | ─ | 0.20 | 3.1 | 0.20 | 3.4 | 0.20 | 3.2 | 0.20 | 3.0 | 0.20 | 3.0 |
| −2LL | ─ | 10,870.99 | ─ | 10,826.96 | ─ | 10,818.28 | ─ | 10,793.76 | ─ | 10,750.05 | ─ |
| AIC | ─ | 10,888.99 | ─ | 10,852.96 | ─ | 10,844.28 | ─ | 10,827.76 | ─ | 10,792.05 | ─ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ternant, D.; Le Tilly, O.; Picon, L.; Moussata, D.; Passot, C.; Bejan-Angoulvant, T.; Desvignes, C.; Mulleman, D.; Goupille, P.; Paintaud, G. Infliximab Efficacy May Be Linked to Full TNF-α Blockade in Peripheral Compartment—A Double Central-Peripheral Target-Mediated Drug Disposition (TMDD) Model. Pharmaceutics 2021, 13, 1821. https://doi.org/10.3390/pharmaceutics13111821
Ternant D, Le Tilly O, Picon L, Moussata D, Passot C, Bejan-Angoulvant T, Desvignes C, Mulleman D, Goupille P, Paintaud G. Infliximab Efficacy May Be Linked to Full TNF-α Blockade in Peripheral Compartment—A Double Central-Peripheral Target-Mediated Drug Disposition (TMDD) Model. Pharmaceutics. 2021; 13(11):1821. https://doi.org/10.3390/pharmaceutics13111821
Chicago/Turabian StyleTernant, David, Olivier Le Tilly, Laurence Picon, Driffa Moussata, Christophe Passot, Theodora Bejan-Angoulvant, Céline Desvignes, Denis Mulleman, Philippe Goupille, and Gilles Paintaud. 2021. "Infliximab Efficacy May Be Linked to Full TNF-α Blockade in Peripheral Compartment—A Double Central-Peripheral Target-Mediated Drug Disposition (TMDD) Model" Pharmaceutics 13, no. 11: 1821. https://doi.org/10.3390/pharmaceutics13111821