Evaluation of the Pharmacokinetic Drug–Drug Interaction between Micronized Fenofibrate and Pitavastatin in Healthy Volunteers

 ,
,
Abstract
:1. Introduction
2. Methods
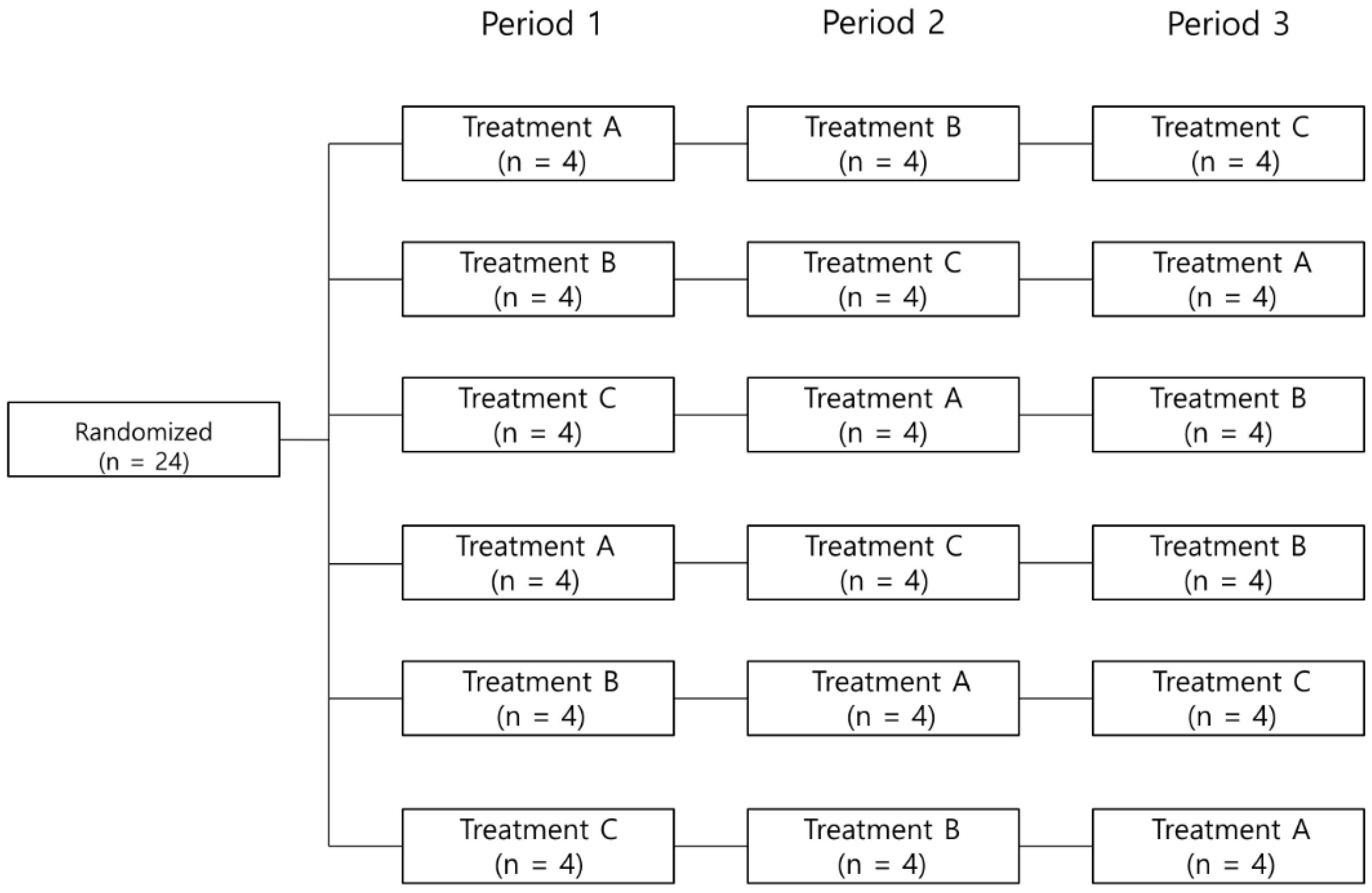
2.1. Study Design and Subjects
2.2. Bioanalytic Methods
2.3. Pharmacokinetic Analysis
2.4. Safety of Subjects
2.5. Statistical Analyses
3. Results
3.1. Subjects
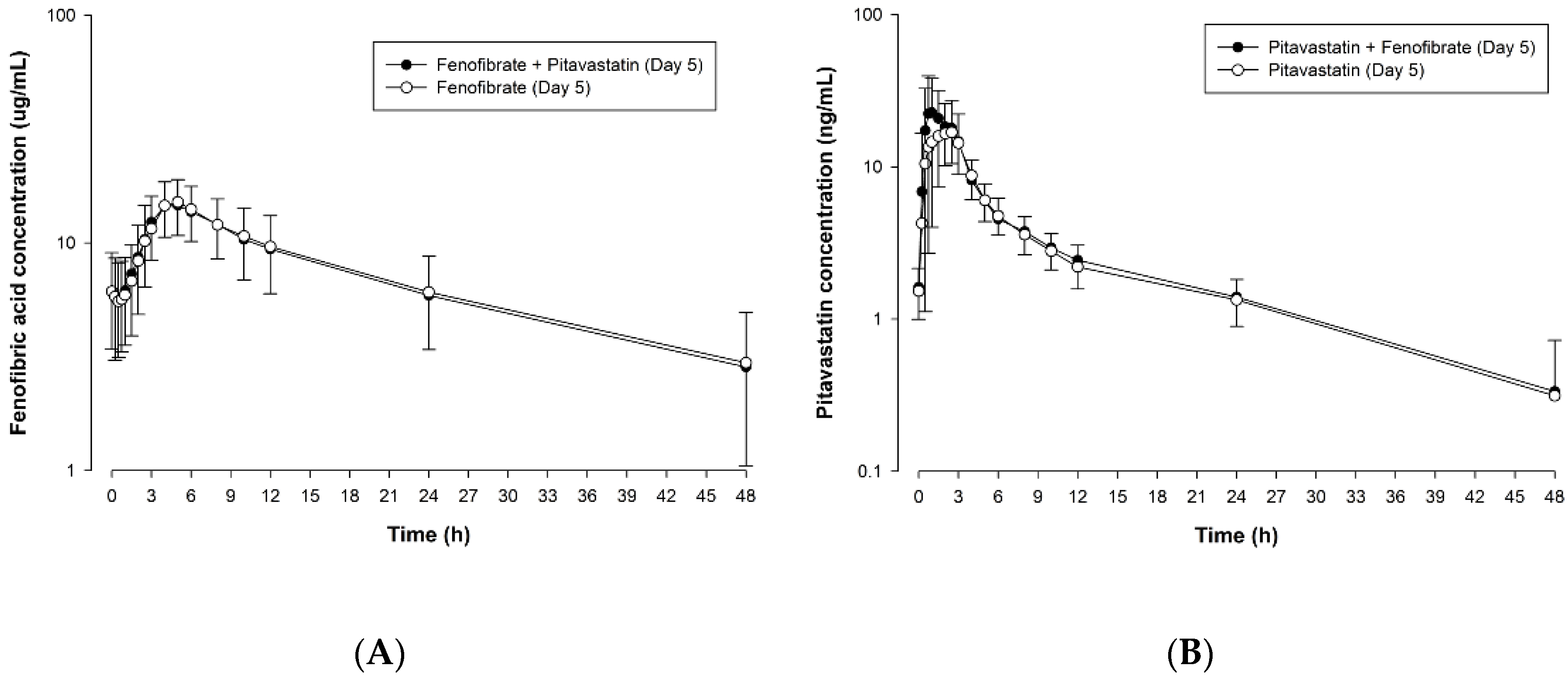
3.2. Pharmacokinetics
3.3. Safety
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kosmas, C.E.; Sourlas, A.; Silverio, D.; Montan, P.D.; Guzman, E. Novel lipid-modifying therapies addressing unmet needs in cardiovascular disease. World J. Cardiol. 2019, 11, 256–265. [Google Scholar] [CrossRef] [PubMed]
- De Goma, E.M.; Knowles, J.W.; Angeli, F.; Budoff, M.J.; Rader, D.J. The evolution and refinement of traditional risk factors for cardiovascular disease. Cardiol. Rev. 2012, 20, 118–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacobson, T.A.; Ito, M.K.; Maki, K.C.; Orringer, C.E.; Bays, H.E.; Jones, P.H.; McKenney, J.M.; Grundy, S.M.; Gill, E.A.; Wild, R.A.; et al. National Lipid Association recommendations for patient-centered management of dyslipidemia: Part 1—executive summary. J. Clin. Lipidol. 2014, 8, 473–488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stone, N.J.; Robinson, J.G.; Lichtenstein, A.H.; Bairey Merz, C.N.; Blum, C.B.; Eckel, R.H.; Goldberg, A.C.; Gordon, D.; Levy, D.; Llyod-Jones, D.M.; et al. American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2014, 63, 2889–2934. [Google Scholar]
- Expert Dyslipidemia Panel of the International Atherosclerosis Society Panel members. An International atherosclerosis Society Position Paper: Global recommendations for the management of dyslipidemia--full report. J. Clin. Lipidol. 2014, 8, 29–60. [Google Scholar] [CrossRef] [Green Version]
- Hoy, S.M. Pitavastatin: A Review in Hypercholesterolemia. Am. J. Cardiovasc. Drugs 2017, 17, 157–168. [Google Scholar] [CrossRef]
- Duggan, S.T. Pitavastatin: A review of its use in the management of hypercholesterolaemia or mixed dyslipidaemia. Drugs 2012, 72, 565–584. [Google Scholar] [CrossRef]
- Livalo® (Pitavastatin) Tablets [Prescribing Information]. Kowa Pharmaceuticals America, Inc., Tokyo, Japan. Available online: https://rsc.niaid.nih.gov/sites/default/files/livalo-pi-current-november-2016.pdf (accessed on 23 March 2020).
- Chan, P.; Shao, L.; Tomlinson, B.; Zhang, Y.; Liu, Z.M. An evaluation of pitavastatin for the treatment of hypercholesterolemia. Expert Opin. Pharmacother. 2019, 20, 103–113. [Google Scholar] [CrossRef]
- Gosho, M.; Tanahashi, M.; Hounslow, N.; Teramoto, T. Pitavastatin therapy in polymedicated patients is associated with a low risk of drug-drug interactions: Analysis of real-world and phase 3 clinical trial data. Int. J. Clin. Pharmacol. Ther. 2015, 53, 635–646. [Google Scholar] [CrossRef]
- Shirasaka, Y.; Suzuki, K.; Shichiri, M.; Nakanishi, T.; Tamai, I. Intestinal absorption of HMG-CoA reductase inhibitor pitavastatin mediated by organic anion transporting polypeptide and P-glycoprotein/multidrug resistance 1. Drug Metab. Pharmacokinet. 2011, 26, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Gupta, K.K.; Ali, S.; Sanghera, R.S. Pharmacological Options in Atherosclerosis: A Review of the Existing Evidence. Cardiol. Ther. 2019, 8, 5–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moutzouri, E.; Kei, A.; Elisaf, M.S.; Milionis, H.J. Management of dyslipidemias with fibrates, alone and in combination with statins: Role of delayed-release fenofibric acid. Vasc. Health Risk Manag. 2010, 6, 525–539. [Google Scholar] [PubMed] [Green Version]
- Fenofibrate Capsules (micronized) [Prescribing Information]. Teva Canada Ltd., Toronto, Canada. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/075753s005lbl.pdf (accessed on 16 June 2020).
- Ling, H.; Luoma, J.T.; Hilleman, D. A review of currently available fenofibrate and fenofibric acid formulations. Cardiol. Res. 2013, 4, 47–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keating, G.M.; Ormrod, D. Micronised fenofibrate: An updated review of its clinical efficacy in the management of dyslipidemia. Drugs 2002, 62, 1909–1944. [Google Scholar] [CrossRef]
- Rhee, E.J.; Kim, H.C.; Kim, J.H.; Lee, E.Y.; Kim, B.J.; Kim, E.M.; Song, Y.J.; Lim, J.H.; Kim, H.J.; Choi, S.; et al. 2018 Guidelines for the Management of Dyslipidemia. Korean J. Int. Med. 2019, 34, 723–771. [Google Scholar] [CrossRef] [Green Version]
- Catapano, A.L.; Graham, I.; De Backer, G.; Wiklund, O.; Chapman, M.J.; Drexel, H.; Hoes, A.W.; Jennings, C.S.; Landmesser, U.; Pedersen, T.R.; et al. ESC Scientific Document Group. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias. Eur. Heart J. 2016, 37, 2999–3058. [Google Scholar] [CrossRef] [Green Version]
- Da Silva, P.M. Are all statins the same? Focus on the efficacy and tolerability of pitavastatin. Am. J. Cardiovasc. Drugs 2011, 11, 93–107. [Google Scholar] [CrossRef] [Green Version]
- Bhavesh, D.; Shah, S. Determination of fenofibric acid in human plasma by ultra performance liquid chromatography-electrospray ionization mass spectrometry: Application to a bioequivalence study. Biomed. Chromatogr. 2009, 23, 922–928. [Google Scholar] [CrossRef]
- Lv, H.; Sun, J.G.; Wang, G.J.; Zhu, X.Y.; Zhang, Y.; Gu, S.H.; Liang, Y.; Sun, J. Determination of pitavastatin in human plasma via HPLC-ESI-MS/MS and subsequent application to a clinical study in healthy Chinese volunteers. Clin. Chim. Acta 2007, 386, 25–30. [Google Scholar] [CrossRef]
- Di, B.; Su, M.X.; Yu, F.; Qu, L.J.; Zhao, L.P.; Cheng, M.C.; He, L.P. Solid-phase extraction and liquid chromatography/tandem mass spectrometry assay for the determination of pitavastatin in human plasma and urine for application to Phase I clinical pharmacokinetic studies. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2008, 868, 95–101. [Google Scholar] [CrossRef]
- US Food and Drug Administration. [Webpage on the Internet] Guidance for Industry: Clinical Drug Interaction Studies—Study Design, Data Analysis, and Clinical Implications. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/clinical-drug-interaction-studies-cytochrome-p450-enzyme-and-transporter-mediated-drug-interactions (accessed on 17 June 2020).
- Yamazaki, M.; Li, B.; Louie, S.W.; Pudvah, N.T.; Stocco, R.; Wong, W.; Abramovitz, M.; Demartis, A.; Laufer, R.; Hochman, J.H.; et al. Effects of fibrates on human organic anion-transporting polypeptide 1B1-, multidrug resistance protein 2- and P-glycoprotein-mediated transport. Xenobiotica 2005, 35, 737–753. [Google Scholar] [CrossRef] [PubMed]
- Betteridge, J. Pitavastatin—Results from phase III & IV. Atheroscler. Suppl. 2010, 11, 8–14. [Google Scholar] [PubMed]
- Sponseller, C.A.; Morgan, R.E.; Kryzhanovski, V.A.; Campbell, S.E.; Davidson, M.H. Comparison of the lipid-lowering effects of pitavastatin 4 mg versus pravastatin 40 mg in adults with primary hyperlipidemia or mixed (combined) dyslipidemia: A Phase IV, prospective, US, multicenter, randomized, double-blind, superiority trial. Clin. Ther. 2014, 36, 1211–1222. [Google Scholar] [CrossRef] [PubMed]
- Stender, S.; Budinski, D.; Hounslow, N. Pitavastatin demonstrates long-term efficacy, safety and tolerability in elderly patients with primary hypercholesterolaemia or combined (mixed) dyslipidaemia. Eur. J. Prev. Cardiol. 2013, 20, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.; Wang, F.; Dai, Y.; Lin, L.; Tong, Q.; Liao, Y.; Yin, Y.; Wang, G.; Yan, Y.; Li, X.; et al. Efficacy and safety of fenofibrate as an add-on in patients with elevated triglyceride despite receiving statin treatment. Int. J. Cardiol. 2016, 22, 832–836. [Google Scholar] [CrossRef] [PubMed]
- Wakida, Y.; Suzuki, S.; Nomura, H.; Isomura, T. Additional treatment with fenofibrate for patients treated with pitavastatin under ordinary medical practice for hypertriglyceridemia in Japan (APPROACH-J Study). Jpn. Clin. Med. 2011, 2, 57–66. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | p-Value ‡ | ||
| Fenofibric Acid | Fenofibric Acid + Pitavastatin | ||
| Fenofibric acid | |||
| AUCτ,ss (ng∙h/mL) | 228.5 ± 76.3 | 225.1 ± 72.2 | 0.331 ** |
| Cmax,ss (ng/mL) | 15.8 ± 3.7 | 15.5 ± 3.7 | 0.595 * |
| Tmax,ss (h) † | 5.0 (2.5–6.0) | 4.5 (2.0–6.0) | 0.635 ** |
| t1/2 (h) | 20.7 ± 5.3 | 20.5 ± 5.1 | 0.689 ** |
| CLss/F (L/h) | 0.8 ± 0.2 | 0.8 ± 0.2 | 0.837 * |
| Pitavastatin | Pitavastatin + Fenofibric acid | ||
| Pitavastatin AUCτ,ss (ng∙h/mL) | 106.1 ± 28.1 | 119.8 ± 34.4 | 0.007 * |
| Cmax,ss (ng/mL) | 22.4 ± 7.6 | 31.5 ±13.3 | 0.001 * |
| Tmax,ss (h) † | 2.0 (0.5–4.0) | 1.25 (0.33–3.0) | 0.199 ** |
| t1/2 (h) | 15.2 ± 5.1 | 15.0 ± 4.2 | 0.817 * |
| CLss/F (L/h) | 20.6 ± 7.3 | 18.4 ± 6.5 | 0.002 ** |
| Variable | Geometric Mean Ratio (90% CI) | |
|---|---|---|
| Fenofibric acid | Pitavastatin | |
| AUCτ,ss | 0.9900 (0.9545–1.0269) | 1.1237 (1.0575–1.1941) |
| Cmax,ss | 0.9827 (0.9295–1.0390) | 1.3576 (1.2056–1.5288) |
| System Organ Class/Preferred Term | Fenofibrate | Pitavastatin | Pitavastatin + Fenofibrate | Total |
|---|---|---|---|---|
| No. of events with ADRs | 8 | 9 | 15 | 32 |
| Investigations | ||||
| CPK increased | 5 | 4 | 4 | 13 |
| ALT increased | 3 | 3 | ||
| WBC decreased | 1 | 1 | 2 | |
| AST increased | 2 | 2 | ||
| Hyperuricemia | 1 | 1 | ||
| LDH increased | 1 | 1 | ||
| Urinary OB abnormal | 2 | 1 | 3 | |
| Urinary RBC abnormal | 2 | 1 | 3 | |
| Gastrointestinal disorders | ||||
| Diarrhea | 1 | 1 | 2 | |
| Musculoskeletal and connective tissue disorder | ||||
| Back pain | 1 | 1 | ||
| Both leg myalgia | 1 | 1 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.W.; Kang, W.Y.; Jung, W.; Gwon, M.-R.; Cho, K.; Yang, D.H.; Yoon, Y.-R.; Seong, S.J. Evaluation of the Pharmacokinetic Drug–Drug Interaction between Micronized Fenofibrate and Pitavastatin in Healthy Volunteers. Pharmaceutics 2020, 12, 869. https://doi.org/10.3390/pharmaceutics12090869
Lee HW, Kang WY, Jung W, Gwon M-R, Cho K, Yang DH, Yoon Y-R, Seong SJ. Evaluation of the Pharmacokinetic Drug–Drug Interaction between Micronized Fenofibrate and Pitavastatin in Healthy Volunteers. Pharmaceutics. 2020; 12(9):869. https://doi.org/10.3390/pharmaceutics12090869
Chicago/Turabian StyleLee, Hae Won, Woo Youl Kang, Wookjae Jung, Mi-Ri Gwon, Kyunghee Cho, Dong Heon Yang, Young-Ran Yoon, and Sook Jin Seong. 2020. "Evaluation of the Pharmacokinetic Drug–Drug Interaction between Micronized Fenofibrate and Pitavastatin in Healthy Volunteers" Pharmaceutics 12, no. 9: 869. https://doi.org/10.3390/pharmaceutics12090869