Population Pharmacokinetics of Continuous-Infusion Meropenem in Febrile Neutropenic Patients with Hematologic Malignancies: Dosing Strategies for Optimizing Empirical Treatment against Enterobacterales and P. aeruginosa

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Population Pharmacokinetic Modelling
2.3. Monte Carlo Simulation Analysis and Probability of Target Attainment
2.4. Ethics
3. Results
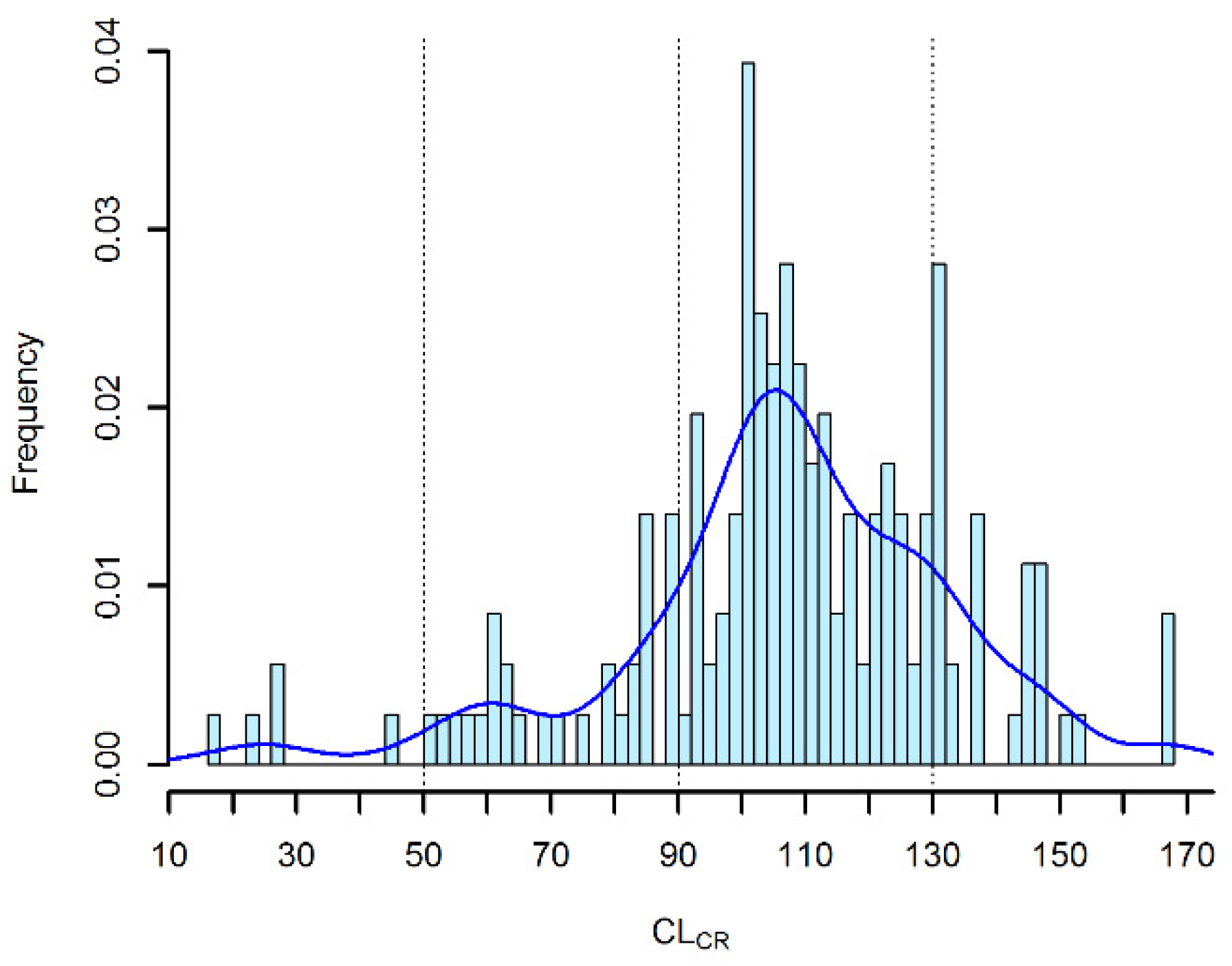
3.1. Patient Population and Meropenem Therapy
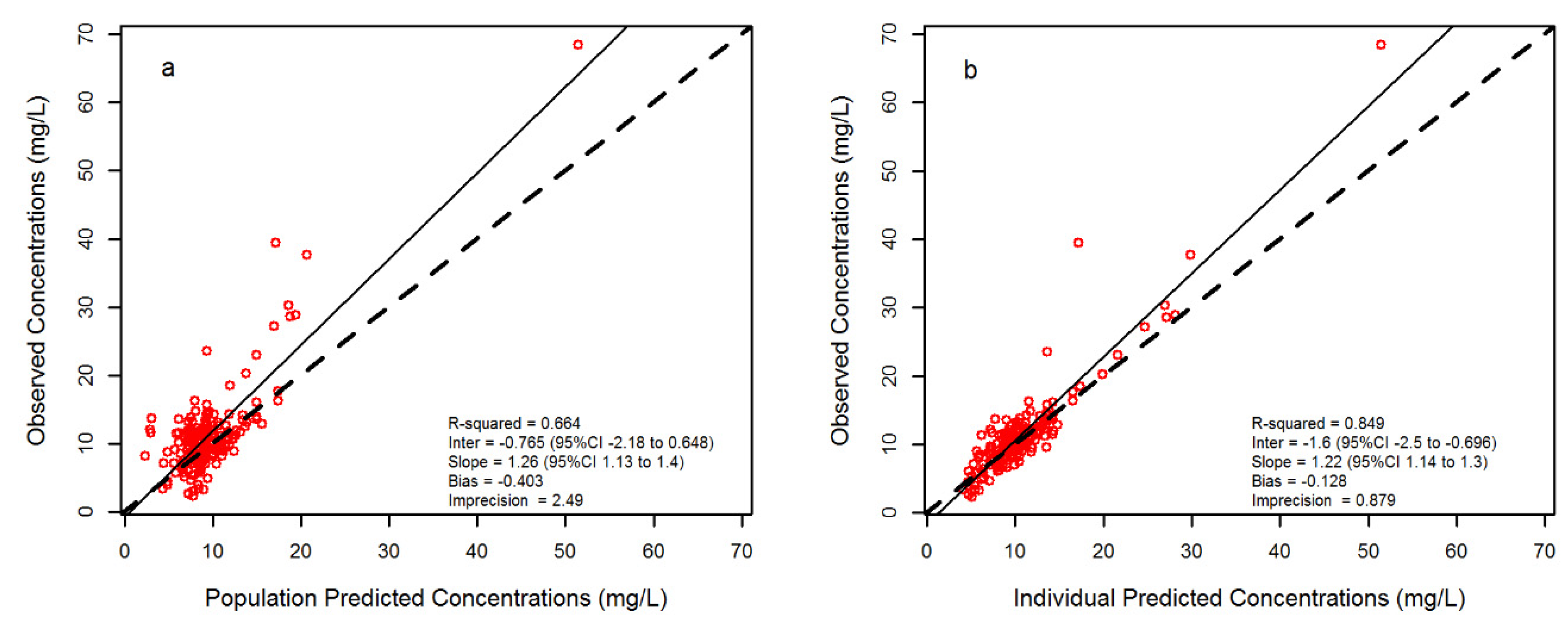
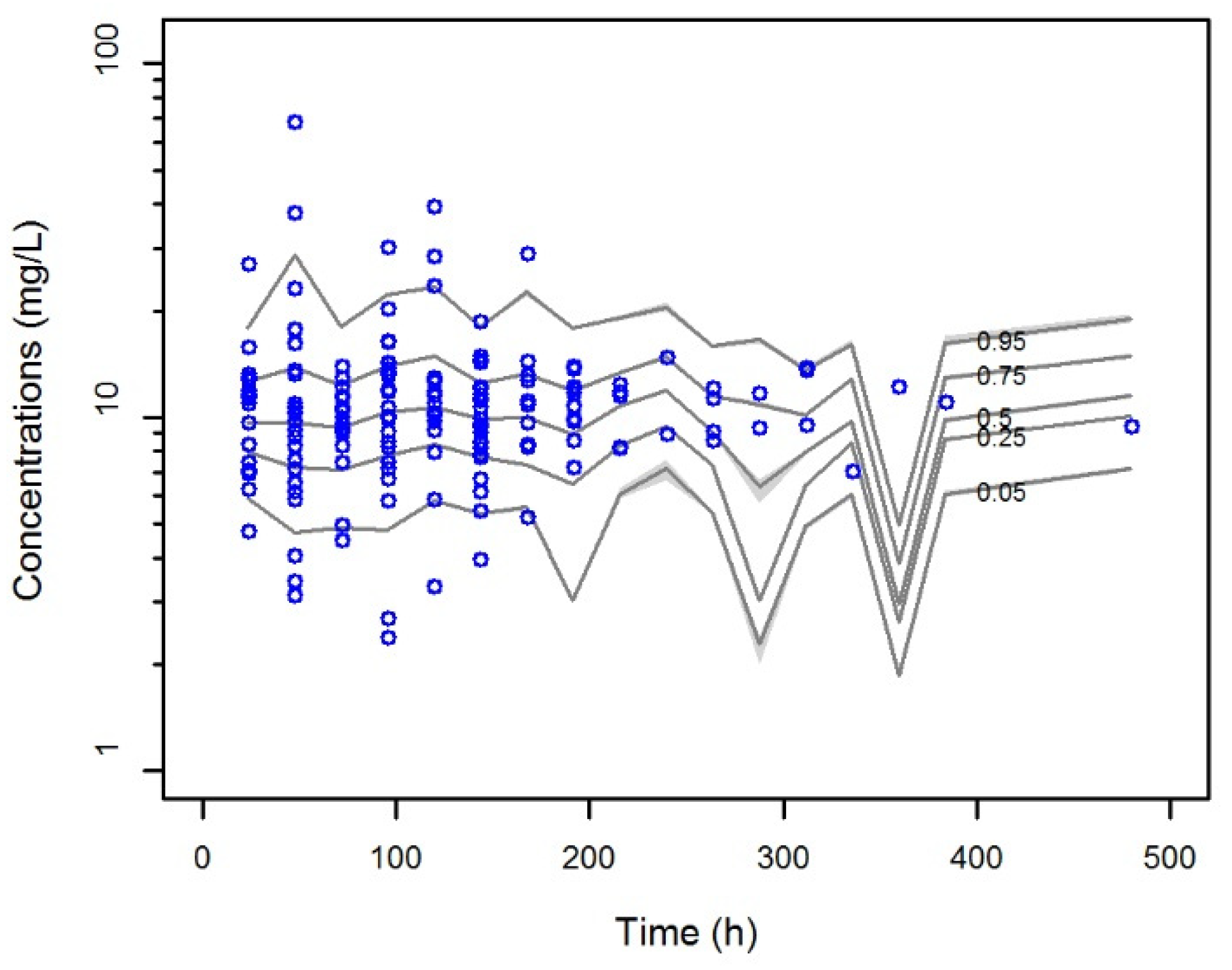
3.2. Population Pharmacokinetic Analysis
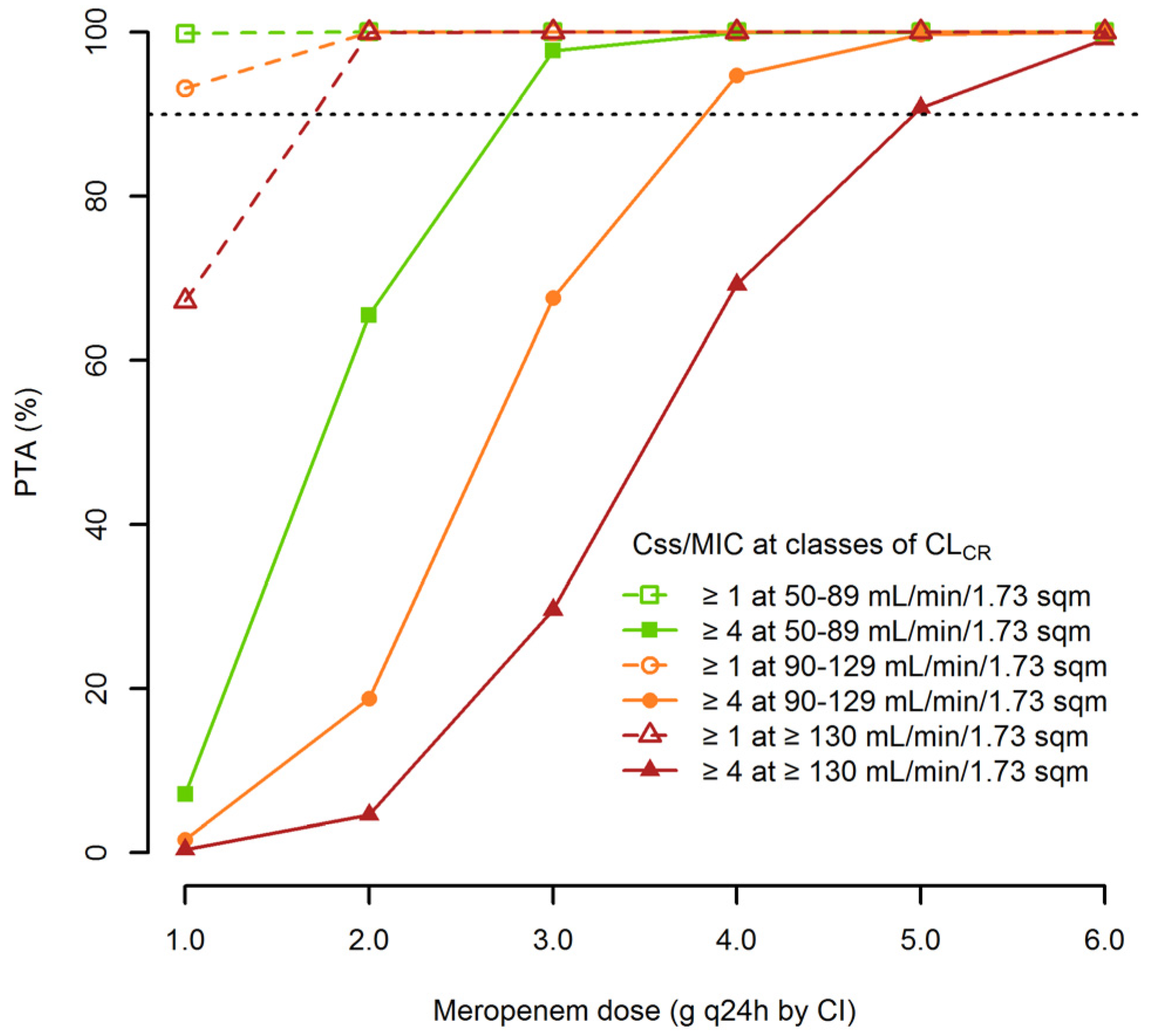
3.3. Monte Carlo Simulation and the Probability of Target Attainment
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Tumbarello, M.; Trecarichi, E.M.; Caira, M.; Candoni, A.; Pastore, D.; Cattaneo, C.; Fanci, R.; Nosari, A.; Spadea, A.; Busca, A.; et al. Derivation and validation of a scoring system to identify patients with bacteremia and hematological malignancies at higher risk for mortality. PLoS ONE 2012, 7, e51612. [Google Scholar] [CrossRef] [PubMed]
- Gudiol, C.; Bodro, M.; Simonetti, A.; Tubau, F.; Gonzalez-Barca, E.; Cisnal, M.; Domingo-Domenech, E.; Jimenez, L.; Carratala, J. Changing aetiology, clinical features, antimicrobial resistance, and outcomes of bloodstream infection in neutropenic cancer patients. Clin. Microbiol. Infect. 2013, 19, 474–479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trecarichi, E.M.; Pagano, L.; Candoni, A.; Pastore, D.; Cattaneo, C.; Fanci, R.; Nosari, A.; Caira, M.; Spadea, A.; Busca, A.; et al. Current epidemiology and antimicrobial resistance data for bacterial bloodstream infections in patients with hematologic malignancies: An Italian multicentre prospective survey. Clin. Microbiol. Infect. 2015, 21, 337–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia-Vidal, C.; Cardozo-Espinola, C.; Puerta-Alcalde, P.; Marco, F.; Tellez, A.; Aguero, D.; Romero-Santana, F.; Diaz-Beya, M.; Gine, E.; Morata, L.; et al. Risk factors for mortality in patients with acute leukemia and bloodstream infections in the era of multiresistance. PLoS ONE 2018, 13, e0199531. [Google Scholar] [CrossRef]
- Heinz, W.J.; Buchheidt, D.; Christopeit, M.; von Lilienfeld-Toal, M.; Cornely, O.A.; Einsele, H.; Karthaus, M.; Link, H.; Mahlberg, R.; Neumann, S.; et al. Diagnosis and empirical treatment of fever of unknown origin (FUO) in adult neutropenic patients: Guidelines of the Infectious Diseases Working Party (AGIHO) of the German Society of Hematology and Medical Oncology (DGHO). Ann. Hematol. 2017, 96, 1775–1792. [Google Scholar] [CrossRef] [Green Version]
- Schmidt-Hieber, M.; Teschner, D.; Maschmeyer, G.; Schalk, E. Management of febrile neutropenia in the perspective of antimicrobial de-escalation and discontinuation. Expert Rev. Anti Infect. Ther. 2019, 17, 983–995. [Google Scholar] [CrossRef]
- Ellis, J.M.; Kuti, J.L.; Nicolau, D.P. Use of Monte Carlo simulation to assess the pharmacodynamics of beta-lactams against Pseudomonas aeruginosa infections in children: A report from the OPTAMA program. Clin. Ther. 2005, 27, 1820–1830. [Google Scholar] [CrossRef]
- Yu, Z.; Pang, X.; Wu, X.; Shan, C.; Jiang, S. Clinical outcomes of prolonged infusion (extended infusion or continuous infusion) versus intermittent bolus of meropenem in severe infection: A meta-analysis. PLoS ONE 2018, 13, e0201667. [Google Scholar] [CrossRef]
- Wong, G.; Brinkman, A.; Benefield, R.J.; Carlier, M.; De Waele, J.J.; El Helali, N.; Frey, O.; Harbarth, S.; Huttner, A.; McWhinney, B.; et al. An international, multicentre survey of beta-lactam antibiotic therapeutic drug monitoring practice in intensive care units. J. Antimicrob. Chemother. 2014, 69, 1416–1423. [Google Scholar] [CrossRef] [Green Version]
- Sumi, C.D.; Heffernan, A.J.; Lipman, J.; Roberts, J.A.; Sime, F.B. What Antibiotic Exposures Are Required to Suppress the Emergence of Resistance for Gram-Negative Bacteria? A Systematic Review. Clin. Pharmacokinet. 2019, 58, 1407–1443. [Google Scholar] [CrossRef]
- Ariano, R.E.; Nyhlen, A.; Donnelly, J.P.; Sitar, D.S.; Harding, G.K.M.; Zelenitsky, S.A. Pharmacokinetics and pharmacodynamics of meropenem in febrile neutropenic patients with bacteremia. Ann. Pharmacother. 2005, 39, 32–38. [Google Scholar] [CrossRef]
- Cojutti, P.G.; Lazzarotto, D.; Candoni, A.; Dubbini, M.V.; Zannier, M.E.; Fanin, R.; Pea, F. Real-time TDM-based optimization of continuous infusion meropenem for improving treatment outcome of febrile neutropenia in oncohematologic patients: Results from a prospective, monocentric, interventional study (in press). J. Antimicrob. Chemother. 2020, dkaa267. [Google Scholar] [CrossRef] [PubMed]
- Pea, F.; Viale, P.; Cojutti, P.; Furlanut, M. Dosing nomograms for attaining optimum concentrations of meropenem by continuous infusion in critically ill patients with severe gram-negative infections: A pharmacokinetics/pharmacodynamics-based approach. Antimicrob. Agents Chemother. 2012, 56, 6343–6348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franceschi, L.; Cojutti, P.; Baraldo, M.; Pea, F. Stability of generic meropenem solutions for administration by continuous infusion at normal and elevated temperatures. Ther. Drug Monit. 2014, 36, 674–676. [Google Scholar] [CrossRef] [PubMed]
- Mendez, A.S.L.; Steppe, M.; Schapoval, E.E.S. Validation of HPLC and UV spectrophotometric methods for the determination of meropenem in pharmaceutical dosage form. J. Pharm. Biomed. Anal. 2003, 33, 947–954. [Google Scholar] [CrossRef]
- Cojutti, P.; Maximova, N.; Pea, F. Pharmacokinetics and pharmacodynamics of continuous-infusion meropenem in pediatric hematopoietic stem cell transplant patients. Antimicrob. Agents Chemother. 2015, 59, 5535–5541. [Google Scholar] [CrossRef] [Green Version]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro 3rd, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Neely, M.N.; van Guilder, M.G.; Yamada, W.M.; Schumitzky, A.; Jelliffe, R.W. Accurate detection of outliers and subpopulations with Pmetrics, a nonparametric and parametric pharmacometric modeling and simulation package for R. Ther. Drug Monit. 2012, 34, 467–476. [Google Scholar] [CrossRef] [Green Version]
- Brendel, K.; Comets, E.; Laffont, C.; Laveille, C.; Mentre, F. Metrics for external model evaluation with an application to the population pharmacokinetics of gliclazide. Pharm. Res. 2006, 23, 2036–2049. [Google Scholar] [CrossRef] [Green Version]
- The European Committee on Antimicrobial Susceptibility Testing-EUCAST. Available online: https://www.eucast.org/mic_distributions_and_ecoffs (accessed on 16 June 2020).
- Lee, D.-G.; Choi, S.-M.; Shin, W.-S.; Lah, H.-O.; Yim, D.-S. Population pharmacokinetics of meropenem in febrile neutropenic patients in Korea. Int. J. Antimicrob. Agents 2006, 28, 333–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeitany, R.G.; El Saghir, N.S.; Santhosh-Kumar, C.R.; Sigmon, M.A. Increased aminoglycoside dosage requirements in hematologic malignancy. Antimicrob. Agents Chemother. 1990, 34, 702–708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romano, S.; Fdez de Gatta, M.M.; Calvo, M.V.; Caballero, D.; Dominguez-Gil, A.; Lanao, J.M. Population pharmacokinetics of amikacin in patients with haematological malignancies. J. Antimicrob. Chemother. 1999, 44, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Pea, F.; Viale, P.; Damiani, D.; Pavan, F.; Cristini, F.; Fanin, R.; Furlanut, M. Ceftazidime in acute myeloid leukemia patients with febrile neutropenia: Helpfulness of continuous intravenous infusion in maximizing pharmacodynamic exposure. Antimicrob. Agents Chemother. 2005, 49, 3550–3553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamoth, F.; Buclin, T.; Csajka, C.; Pascual, A.; Calandra, T.; Marchetti, O. Reassessment of recommended imipenem doses in febrile neutropenic patients with hematological malignancies. Antimicrob. Agents Chemother. 2009, 53, 785–787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cojutti, P.G.; Candoni, A.; Ramos-Martin, V.; Lazzarotto, D.; Zannier, M.E.; Fanin, R.; Hope, W.; Pea, F. Population pharmacokinetics and dosing considerations for the use of daptomycin in adult patients with haematological malignancies. J. Antimicrob. Chemother. 2017, 72, 2342–2350. [Google Scholar] [CrossRef]
- Feher, C.; Rovira, M.; Soriano, A.; Esteve, J.; Martinez, J.A.; Marco, F.; Carreras, E.; Martinez, C.; Fernandez-Aviles, F.; Suarez-Lledo, M.; et al. Effect of meropenem administration in extended infusion on the clinical outcome of febrile neutropenia: A retrospective observational study. J. Antimicrob. Chemother. 2014, 69, 2556–2562. [Google Scholar] [CrossRef] [Green Version]
- Abdul-Aziz, M.H.; Lipman, J.; Akova, M.; Bassetti, M.; De Waele, J.J.; Dimopoulos, G.; Dulhunty, J.; Kaukonen, K.-M.; Koulenti, D.; Martin, C.; et al. Is prolonged infusion of piperacillin/tazobactam and meropenem in critically ill patients associated with improved pharmacokinetic/pharmacodynamic and patient outcomes? An observation from the Defining Antibiotic Levels in Intensive care unit patients (DALI) cohort. J. Antimicrob. Chemother. 2016, 71, 196–207. [Google Scholar]
- Lorente, L.; Lorenzo, L.; Martin, M.M.; Jimenez, A.; Mora, M.L. Meropenem by continuous versus intermittent infusion in ventilator-associated pneumonia due to gram-negative bacilli. Ann. Pharmacother. 2006, 40, 219–223. [Google Scholar] [CrossRef]
- Taccone, F.S.; Cotton, F.; Roisin, S.; Vincent, J.-L.; Jacobs, F. Optimal meropenem concentrations to treat multidrug-resistant Pseudomonas aeruginosa septic shock. Antimicrob. Agents Chemother. 2012, 56, 2129–2131. [Google Scholar] [CrossRef] [Green Version]
- Cojutti, P.G.; Barbarino, C.; De Monte, A.; Hope, W.; Pea, F. Higher than standard meropenem and linezolid dosages needed for appropriate treatment of an intracerebral hemorrhage patient with augmented renal clearance. Eur. J. Clin. Pharmacol. 2018, 74, 1091–1092. [Google Scholar] [CrossRef]
- Cojutti, P.; Sartor, A.; Righi, E.; Scarparo, C.; Bassetti, M.; Pea, F. Population Pharmacokinetics of High-Dose Continuous-Infusion Meropenem and Considerations for Use in the Treatment of Infections Due to KPC-Producing Klebsiella pneumoniae. Antimicrob. Agents Chemother. 2017, 61, e00794-17. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient demographics | ||
| Total number of patients | 61 | |
| Age (years) | 55 (54–60) | |
| Gender (male/female) | 37/24 | |
| Body weight (kg) | 77 (63–85) | |
| CLCR (mL/min/1.73 m2) | 107.3 (96.1–123.6) | |
| Patients with ARC | 14 (22.9) | |
| Underlying hematological disease | ||
| AML | 35 (57.4) | |
| Lymphoma | 12 (19.7) | |
| ALL | 11 (18.0) | |
| MM | 3 (4.9) | |
| Clinically documented infections | ||
| Overall | 30 (49.2) | |
| Pneumonia | 11 (18.0) | |
| BSI | 10 (16.4) | |
| Intra-abdominal infection | 5 (8.2) | |
| SSTI | 2 (3.4) | |
| UTI | 1 (1.6) | |
| Septic shock | 1 (1.6) | |
| Gram-negative isolates | ||
| Escherichia coli | 5 (8.2) | |
| Klebsiella pneumonia | 1 (1.6) | |
| Pseudomonas aeruginosa | 1 (1.6) | |
| Meropenem treatment | ||
| Median dose (g) | 1 g q8h CI (1 g q8h CI–1 g q8h CI) | |
| Length of treatment (days) | 9 (7–12.3) | |
| No. of TDM assessments per patient | 3 (3–4) | |
| Meropenem Css (mg/L) | 10.5 (8.3–10.2) | |
| Clinical outcome | ||
| Cured | 56 (91.8) | |
| Failed | 5 (8.2) | |
| Parameter | Mean | Standard Deviation | Coefficient of Variation (%) | Median |
|---|---|---|---|---|
| CLi (L/h) = θ1 + θ2 × CLCRi | ||||
| θ1 | 0.27 | 0.13 | 48.53 | 0.20 |
| θ2 | 0.12 | 0.03 | 27.44 | 0.13 |
| V (L) | 21.88 | 5.85 | 26.71 | 20.00 |
| CI-Meropenem Dosages at Classes of Renal Function | E. coli | K. pneumoniae | E. cloacae | P. aeruginosa | ||||
|---|---|---|---|---|---|---|---|---|
| Css/MIC ≥ 4 | Css/MIC ≥ 1 | Css/MIC ≥ 4 | Css/MIC ≥ 1 | Css/MIC ≥ 4 | Css/MIC ≥ 1 | Css/MIC ≥ 4 | Css/MIC ≥ 1 | |
| CLCR: 50–89 mL/min/1.73 m2 | ||||||||
| 0.25 g q6h CI | 99.92 | 99.97 | 99.04 | 99.64 | 98.79 | 99.58 | 65.83 | 84.14 |
| 0.5 g q6h CI | 99.96 | 99.98 | 99.40 | 99.80 | 99.33 | 99.75 | 76.71 | 90.11 |
| 1 g q8h CI | 99.97 | 99.97 | 99.55 | 99.88 | 99.50 | 99.86 | 81.41 | 93.72 |
| 1 g q6h CI | 99.97 | 100.00 | 99.64 | 99.93 | 99.57 | 99.92 | 84.08 | 96.15 |
| 1.25 g q6h CI | 99.98 | 100.00 | 99.70 | 99.96 | 99.63 | 99.95 | 86.13 | 97.74 |
| 1.5 g q6h CI | 99.9 | 100.00 | 99.75 | 99.98 | 99.68 | 99.97 | 87.78 | 98.57 |
| CLCR: 90–129 mL/min/1.73 m2 | ||||||||
| 0.25 g q6h CI | 99.86 | 99.96 | 98.72 | 99.52 | 98.24 | 99.46 | 56.76 | 80.12 |
| 0.5 g q6h CI | 99.95 | 99.98 | 99.23 | 99.72 | 99.09 | 99.65 | 71.25 | 86.71 |
| 1 g q8h CI | 99.96 | 99.98 | 99.41 | 99.81 | 99.34 | 99.76 | 76.91 | 90.21 |
| 1 g q6h CI | 99.96 | 99.99 | 99.52 | 99.86 | 99.46 | 99.83 | 80.20 | 92.59 |
| 1.25 g q6h CI | 99.97 | 99.99 | 99.58 | 99.90 | 99.53 | 99.88 | 82.28 | 94.47 |
| 1.5 g q6h CI | 99.97 | 100.00 | 99.64 | 99.93 | 99.57 | 99.92 | 84.21 | 96.30 |
| CLCR: ≥130 mL/min/1.73 m2 | ||||||||
| 0.25 g q6h CI | 99.80 | 99.96 | 98.43 | 99.41 | 97.62 | 99.33 | 48.90 | 76.66 |
| 0.5 g q6h CI | 99.92 | 99.97 | 99.05 | 99.64 | 98.81 | 99.57 | 66.20 | 84.17 |
| 1 g q8h CI | 99.95 | 99.99 | 99.28 | 99.74 | 99.17 | 99.67 | 77.91 | 87.62 |
| 1 g q6h CI | 99.96 | 99.99 | 99.41 | 99.81 | 99.34 | 99.75 | 76.87 | 90.14 |
| 1.25 g q6h CI | 99.96 | 99.99 | 99.49 | 99.85 | 99.44 | 99.81 | 79.60 | 92.13 |
| 1.5 g q6h CI | 99.97 | 99.99 | 99.55 | 99.88 | 99.49 | 99.85 | 81.30 | 93.59 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cojutti, P.G.; Candoni, A.; Lazzarotto, D.; Filì, C.; Zannier, M.; Fanin, R.; Pea, F. Population Pharmacokinetics of Continuous-Infusion Meropenem in Febrile Neutropenic Patients with Hematologic Malignancies: Dosing Strategies for Optimizing Empirical Treatment against Enterobacterales and P. aeruginosa. Pharmaceutics 2020, 12, 785. https://doi.org/10.3390/pharmaceutics12090785
Cojutti PG, Candoni A, Lazzarotto D, Filì C, Zannier M, Fanin R, Pea F. Population Pharmacokinetics of Continuous-Infusion Meropenem in Febrile Neutropenic Patients with Hematologic Malignancies: Dosing Strategies for Optimizing Empirical Treatment against Enterobacterales and P. aeruginosa. Pharmaceutics. 2020; 12(9):785. https://doi.org/10.3390/pharmaceutics12090785
Chicago/Turabian StyleCojutti, Pier Giorgio, Anna Candoni, Davide Lazzarotto, Carla Filì, Maria Zannier, Renato Fanin, and Federico Pea. 2020. "Population Pharmacokinetics of Continuous-Infusion Meropenem in Febrile Neutropenic Patients with Hematologic Malignancies: Dosing Strategies for Optimizing Empirical Treatment against Enterobacterales and P. aeruginosa" Pharmaceutics 12, no. 9: 785. https://doi.org/10.3390/pharmaceutics12090785