Viral load Reduction in SHIV-Positive Nonhuman Primates via Long-Acting Subcutaneous Tenofovir Alafenamide Fumarate Release from a Nanofluidic Implant

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
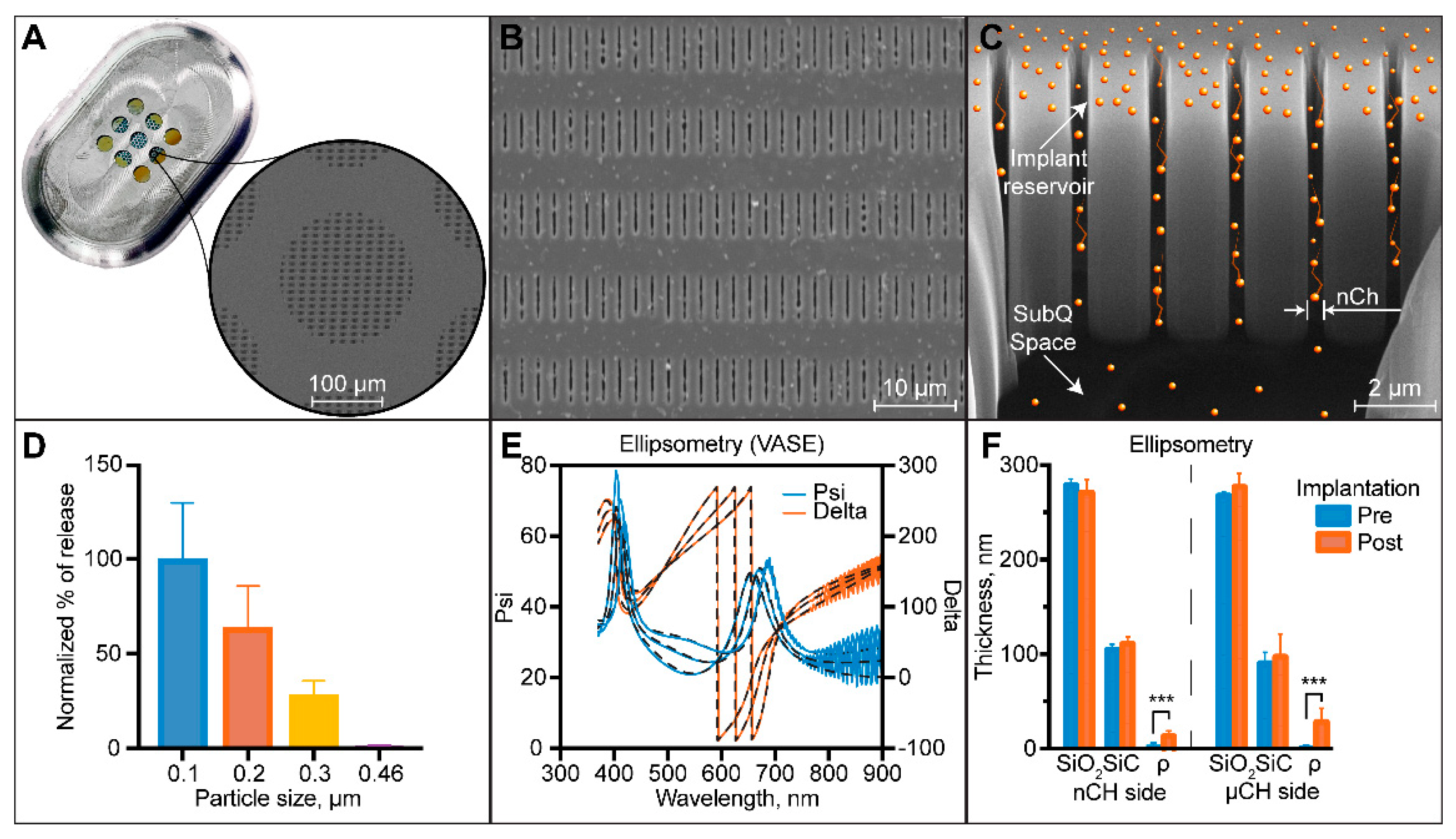
2.1. Nanofluidic Membrane Fabrication and Characterization
2.2. Nanofluidic Implant Assembly
2.3. Ethics Statement
2.4. Study Population
2.5. Blood Collection and Plasma and PBMC Sample Preparation
2.6. Pharmacokinetic Analysis of TFV-DP in PBMC
2.7. Tissue TFV-DP Quantification
2.8. Infection Monitoring by SHIV RNA in Plasma
2.9. TAF Stability Analysis in Drug Reservoir
2.10. Assessment of Treatment nTAF Safety and Tolerability
2.11. Statistical Analysis
3. Results
3.1. Nanofluidic Implant Assembly for Treatment
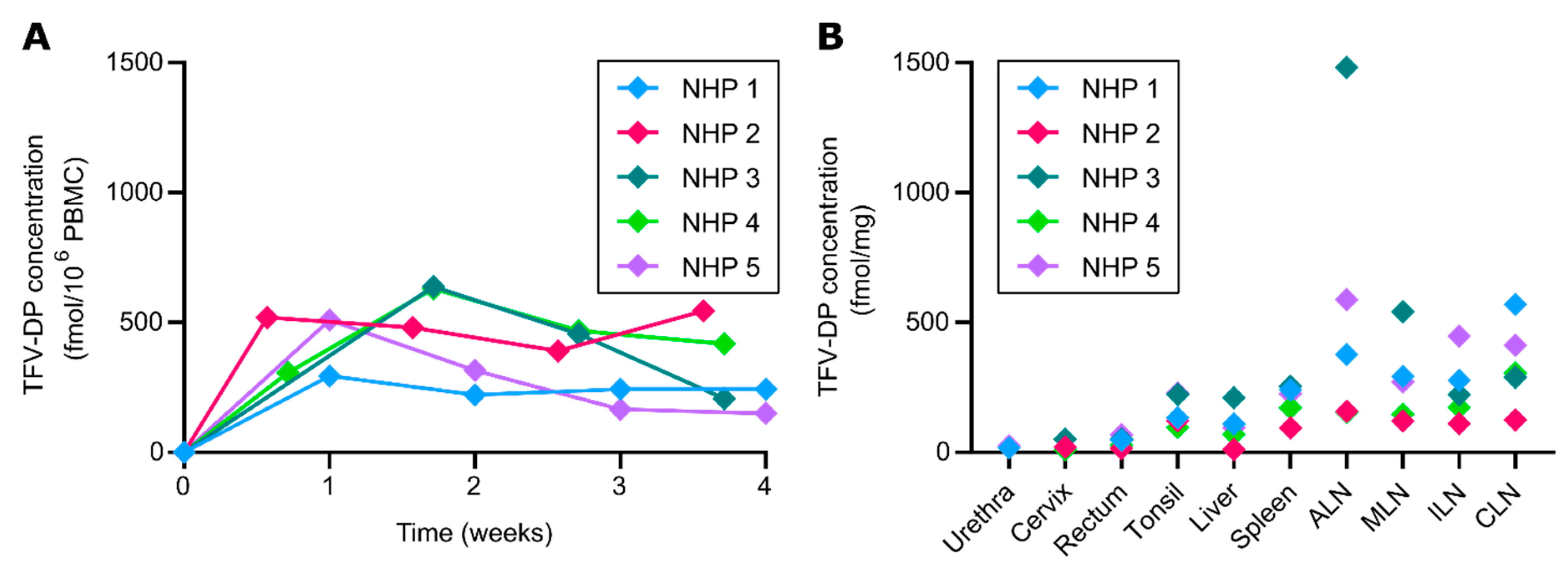
3.2. TFV-DP Concentration in PBMC and Tissues
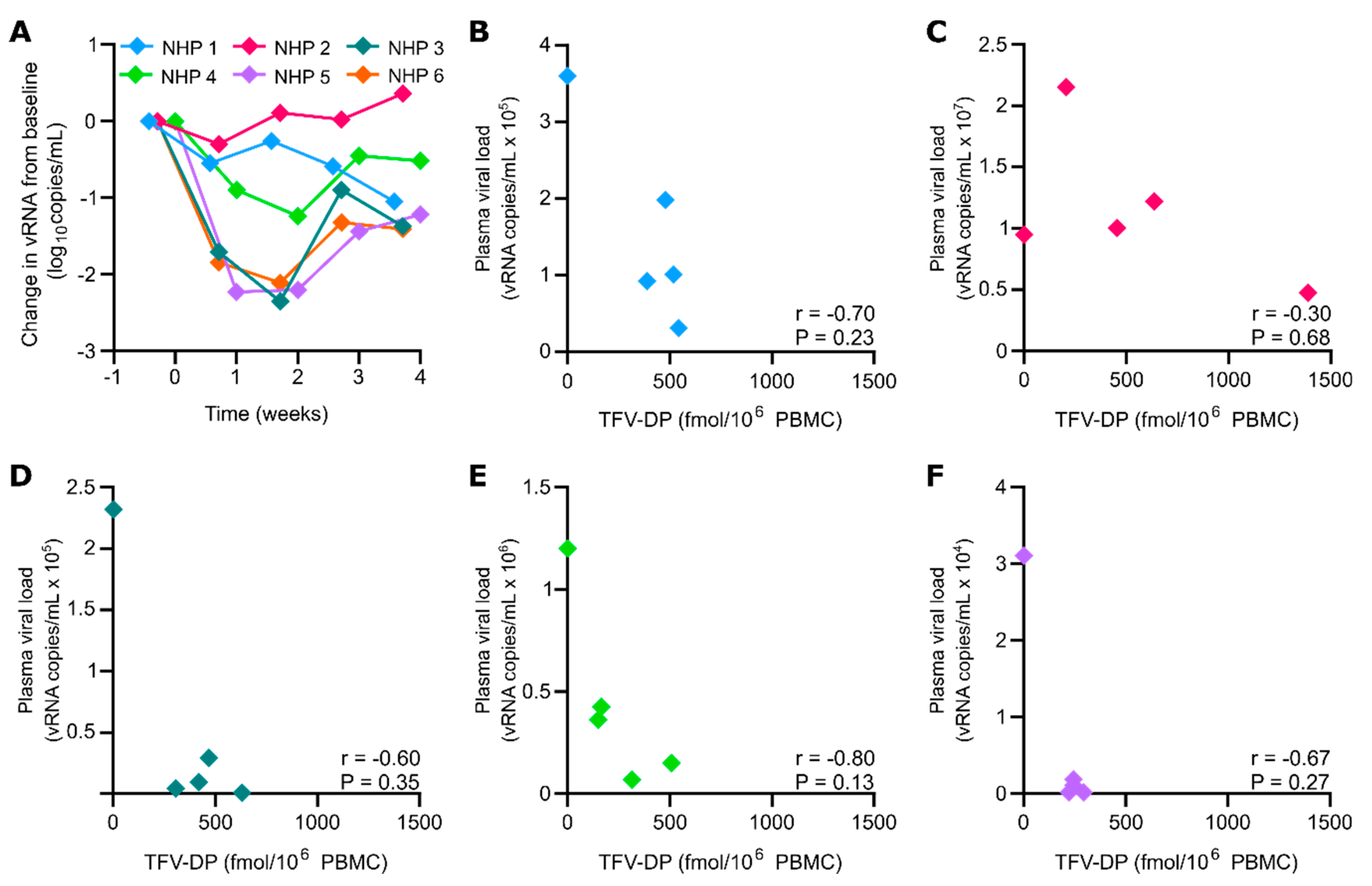
3.3. nTAF Treatment Viral Load Reduction
3.4. TAF Stability in Drug Reservoir
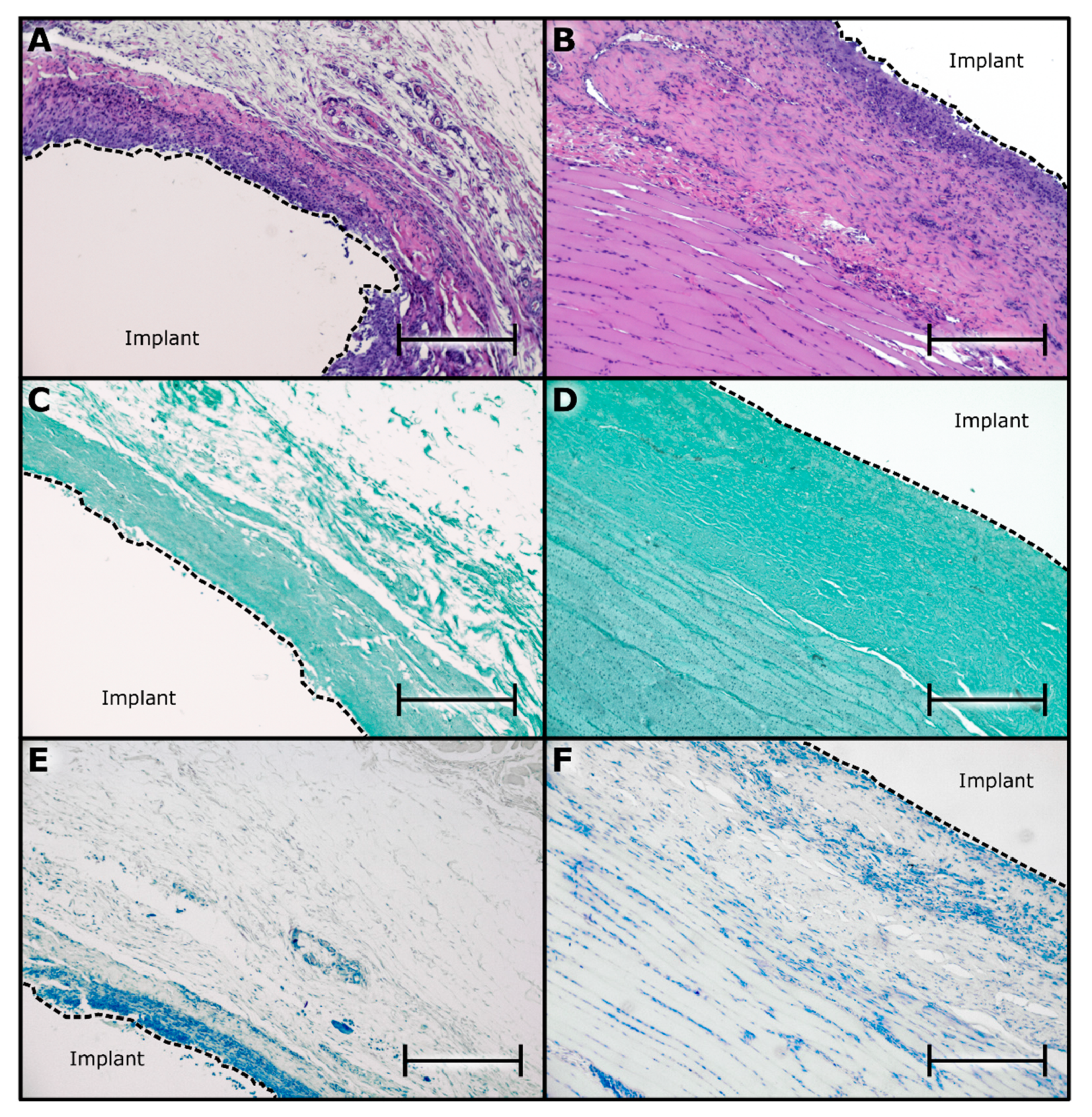
3.5. Histological Assessment of nTAFt Safety and Tolerability
4. Discussions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Deeks, S.G.; Lewin, S.R.; Havlir, D.V. The end of AIDS: HIV infection as a chronic disease. Lancet 2013, 382, 1525–1533. [Google Scholar] [CrossRef] [Green Version]
- Joint United Nations Programme on HIV/AIDS (UNAIDS). 90-90-90 An ambitious treatment target to help end the AIDS epidemic; UNAIDS Information Production Unit, 2014; p. 40. Available online: https://www.unaids.org/sites/default/files/media_asset/90-90-90_en.pdf (accessed on 22 April 2020).
- Joint United Nations Programme on HIV/AIDS (UNAIDS). Fact sheet—World AIDS day 2019. 2019, p. 6. Available online: https://www.unaids.org/sites/default/files/media_asset/UNAIDS_FactSheet_en.pdf (accessed on 22 April 2020).
- Conway, B. The Role of Adherence to Antiretroviral Therapy in the Management of HIV Infection. JAIDS J. Acquir. Immune Defic. Syndr. 2007, 45, S14–S18. [Google Scholar] [CrossRef] [PubMed]
- Hughes, A.J.; Mattson, C.L.; Scheer, S.; Beer, L.; Skarbinski, J. Discontinuation of Antiretroviral Therapy among Adults Receiving HIV Care in the United States. JAIDS J. Acquir. Immune Defic. Syndr. 2014, 66, 80–89. [Google Scholar] [CrossRef] [Green Version]
- Markowitz, M.; Zolopa, A.; Squires, K.; Ruane, P.; Coakley, D.; Kearney, B.; Zhong, L.; Wulfsohn, M.; Miller, M.D.; Lee, W.A. Phase I/II study of the pharmacokinetics, safety and antiretroviral activity of tenofovir alafenamide, a new prodrug of the HIV reverse transcriptase inhibitor tenofovir, in HIV-infected adults. J. Antimicrob. Chemother. 2014, 69, 1362–1369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merck Sharp & Dohme Corp. A Study of Islatravir (MK-8591) in Anti-Retroviral Therapy-Naive, Human Immunodeficiency Virus-1 Infected Participants (MK-8591-003). Available online: https://ClinicalTrials.gov/show/NCT02217904 (accessed on 22 April 2020).
- Schürmann, D.; Rudd, D.J.; Zhang, S.; De Lepeleire, I.; Robberechts, M.; Friedman, E.; Keicher, C.; Hüser, A.; Hofmann, J.; Grobler, J.A.; et al. Safety, pharmacokinetics, and antiretroviral activity of islatravir (ISL, MK-8591), a novel nucleoside reverse transcriptase translocation inhibitor, following single-dose administration to treatment-naive adults infected with HIV-1: An open-label, phase 1b, consecutive-panel trial. Lancet HIV 2020, 7, e164–e172. [Google Scholar] [CrossRef] [PubMed]
- Margolis, D.A.; Gonzalez-Garcia, J.; Stellbrink, H.-J.; Eron, J.J.; Yazdanpanah, Y.; Podzamczer, D.; Lutz, T.; Angel, J.B.; Richmond, G.J.; Clotet, B.; et al. Long-acting intramuscular cabotegravir and rilpivirine in adults with HIV-1 infection (LATTE-2): 96-week results of a randomised, open-label, phase 2b, non-inferiority trial. Lancet 2017, 390, 1499–1510. [Google Scholar] [CrossRef]
- ViiV Healthcare. A Phase IIb Study to Evaluate a Long-Acting Intramuscular Regimen for Maintenance of Virologic Suppression (Following Induction With an Oral Regimen of GSK1265744 and Abacavir/Lamivudine) in Human Immunodeficiency Virus Type 1 (HIV-1) Infected, Antiretroviral Therapy-Naive Adult Subjects. Available online: https://ClinicalTrials.gov/show/NCT02120352 (accessed on 22 April 2020).
- Gilead Sciences. Study to Evaluate the Safety and Efficacy of Lenacapavir in Combination With Other Antiretroviral Agents in People Living With HIV. 2020. Available online: https://ClinicalTrials.gov/show/NCT04143594 (accessed on 9 September 2020).
- Gilead Sciences. Study to Evaluate the Safety and Efficacy of Lenacapavir in Combination With an Optimized Background Regimen in Heavily Treatment Experienced Participants Living With HIV-1 Infection With Multidrug Resistance. 2020. Available online: https://ClinicalTrials.gov/show/NCT04150068 (accessed on 9 September 2020).
- Spreen, W.R.; Margolis, D.A.; Pottage, J.C. Long-acting injectable antiretrovirals for HIV treatment and prevention. Curr. Opin. HIV AIDS 2013, 8, 565–571. [Google Scholar] [CrossRef]
- Pons-Faudoa, F.P.; Ballerini, A.; Sakamoto, J.; Grattoni, A. Advanced implantable drug delivery technologies: Transforming the clinical landscape of therapeutics for chronic diseases. Biomed. Microdevices 2019, 21, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Barrett, S.E.; Teller, R.S.; Forster, S.P.; Li, L.; Mackey, M.A.; Skomski, D.; Yang, Z.; Fillgrove, K.L.; Doto, G.J.; Wood, S.L.; et al. Extended-Duration MK-8591-Eluting Implant as a Candidate for HIV Treatment and Prevention. Antimicrob. Agents Chemother. 2018, 62, e01058-18. [Google Scholar] [CrossRef] [Green Version]
- Pons-Faudoa, F.P.; Sizovs, A.; Di Trani, N.; Paez-Mayorga, J.; Bruno, G.; Rhudy, J.; Manohar, M.; Gwenden, K.; Martini, C.; Chua, C.Y.X.; et al. 2-Hydroxypropyl-β-cyclodextrin-enhanced pharmacokinetics of cabotegravir from a nanofluidic implant for HIV pre-exposure prophylaxis. J. Control. Release 2019, 306, 89–96. [Google Scholar] [CrossRef]
- Chua, C.Y.X.; Jain, P.; Ballerini, A.; Bruno, G.; Hood, R.L.; Gupte, M.; Gao, S.; Di Trani, N.; Susnjar, A.; Shelton, K.; et al. Transcutaneously refillable nanofluidic implant achieves sustained level of tenofovir diphosphate for HIV pre-exposure prophylaxis. J. Control. Release 2018, 286, 315–325. [Google Scholar] [CrossRef]
- Pons-Faudoa, F.P.; Sizovs, A.; Shelton, K.A.; Momin, Z.; Bushman, L.R.; Xu, J.; Grattoni, A.; Nichols, J.E.; Hawkins, T.; Rooney, J.F.; et al. Preventive Efficacy of a Tenofovir Alafenamide Fumarate Nanofluidic Implant in SHIV-Challenged Nonhuman Primates. bioRxiv Preprint Server 2020. [Google Scholar] [CrossRef]
- Gunawardana, M.; Remedios-Chan, M.; Miller, C.S.; Fanter, R.; Yang, F.; Marzinke, M.A.; Hendrix, C.W.; Beliveau, M.; Moss, J.A.; Smith, T.J.; et al. Pharmacokinetics of Long-Acting Tenofovir Alafenamide (GS-7340) Subdermal Implant for HIV Prophylaxis. Antimicrob. Agents Chemother. 2015, 59, 3913–3919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, L.M.; Krovi, S.A.; Li, L.; Girouard, N.; Demkovich, Z.R.; Myers, D.; Creelman, B.; Van Der Straten, A. Characterization of a Reservoir-Style Implant for Sustained Release of Tenofovir Alafenamide (TAF) for HIV Pre-Exposure Prophylaxis (PrEP). Pharmaceutics 2019, 11, 315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schlesinger, E.; Johengen, D.; Luecke, E.; Rothrock, G.; McGowan, I.; Van Der Straten, A.; Desai, T.A. A Tunable, Biodegradable, Thin-Film Polymer Device as a Long-Acting Implant Delivering Tenofovir Alafenamide Fumarate for HIV Pre-exposure Prophylaxis. Pharm. Res. 2016, 33, 1649–1656. [Google Scholar] [CrossRef]
- Su, J.T.; Simpson, S.M.; Sung, S.; Tfaily, E.B.; Veazey, R.; Marzinke, M.; Qiu, J.; Watrous, D.; Widanapathirana, L.; Pearson, E.; et al. A Subcutaneous Implant of Tenofovir Alafenamide Fumarate Causes Local Inflammation and Tissue Necrosis in Rabbits and Macaques. Antimicrob. Agents Chemother. 2019, 64, 775452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Trani, N.; Silvestri, A.; Sizovs, A.; Wang, Y.; Erm, D.R.; Demarchi, D.; Liu, X.; Grattoni, A. Electrostatically gated nanofluidic membrane for ultra-low power controlled drug delivery. Lab Chip 2020, 20, 1562–1576. [Google Scholar] [CrossRef]
- Di Trani, N.; Silvestri, A.; Wang, Y.; Demarchi, D.; Liu, X.; Grattoni, A. Silicon Nanofluidic Membrane for Electrostatic Control of Drugs and Analytes Elution. Pharmaceutics 2020, 12, 679. [Google Scholar] [CrossRef]
- Anderson, P.L.; Glidden, D.V.; Liu, A.; Buchbinder, S.; Lama, J.R.; Guanira, J.V.; Mcmahan, V.; Bushman, L.R.; Casapía, M.; Montoya-Herrera, O.; et al. Emtricitabine-Tenofovir Concentrations and Pre-Exposure Prophylaxis Efficacy in Men Who Have Sex with Men. Sci. Transl. Med. 2012, 4, 151ra125. [Google Scholar] [CrossRef] [Green Version]
- Bushman, L.R.; Kiser, J.J.; Rower, J.E.; Klein, B.; Zheng, J.-H.; Ray, M.L.; Anderson, P.L. Determination of nucleoside analog mono-, di-, and tri-phosphates in cellular matrix by solid phase extraction and ultra-sensitive LC–MS/MS detection. J. Pharm. Biomed. Anal. 2011, 56, 390–401. [Google Scholar] [CrossRef] [Green Version]
- Shieh, E.; Marzinke, M.A.; Fuchs, E.J.; Hamlin, A.; Bakshi, R.P.; Aung, W.; Breakey, J.; Poteat, T.; Brown, T.T.; Bumpus, N.N.; et al. Transgender women on oral HIV pre-exposure prophylaxis have significantly lower tenofovir and emtricitabine concentrations when also taking oestrogen when compared to cisgender men. J. Int. AIDS Soc. 2019, 22, e25405. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services; Food and Drug Administration; Center for Drug Evaluation and Research; Medicine, C. f. V. Bioanalytical Method Validation: Guidance for Industry U.S.; Department of Health and Human Services, U.S. Food and Drug Administration: Rockville, MD, USA, 2018; p. 44.
- Biesinger, T.; White, R.; Kimata, M.T.Y.; Wilson, B.K.; Allan, J.S.; Kimata, J.T. Relative replication capacity of phenotypic SIV variants during primary infections differs with route of inoculation. Retrovirology 2010, 7, 88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polacino, P.; Cleveland, B.; Zhu, Y.; Kimata, J.T.; Overbaugh, J.; Anderson, D.; Hu, S.-L. Immunogenicity and protective efficacy of Gag/Pol/Env vaccines derived from temporal isolates of SIVmne against cognate virus challenge. J. Med Primatol. 2007, 36, 254–265. [Google Scholar] [CrossRef] [PubMed]
- WHO. Expert Committee on Biological Standardization: Sixty-Sixth Report; WHO: Geneva, Switzerland, 2016; Volume 999. [Google Scholar]
- Di Trani, N.; Pimpinelli, A.; Grattoni, A. Finite-Size Charged Species Diffusion and pH Change in Nanochannels. ACS Appl. Mater. Interfaces 2020, 12, 12246–12255. [Google Scholar] [CrossRef] [PubMed]
- Di Trani, N.; Jain, P.; Chua, C.Y.X.; Ho, J.S.; Bruno, G.; Susnjar, A.; Pons-Faudoa, F.P.; Sizovs, A.; Hood, R.L.; Smith, Z.W.; et al. Nanofluidic microsystem for sustained intraocular delivery of therapeutics. Nanomedicine: Nanotechnol. Biol. Med. 2019, 16, 1–9. [Google Scholar] [CrossRef]
- Di Trani, N.; Silvestri, A.; Bruno, G.; Geninatti, T.; Grattoni, A.; Gilbert, A.; Rizzo, G.; Filgueira, C.S.; Demarchi, D.; Grattoni, A. Remotely controlled nanofluidic implantable platform for tunable drug delivery. Lab Chip 2019, 19, 2192–2204. [Google Scholar] [CrossRef]
- Bruno, G.; Di Trani, N.; Hood, R.L.; Zabre, E.; Filgueira, C.S.; Canavese, G.; Jain, P.; Smith, Z.; Demarchi, D.; Hosali, S.; et al. Unexpected behaviors in molecular transport through size-controlled nanochannels down to the ultra-nanoscale. Nat. Commun. 2018, 9, 1682. [Google Scholar] [CrossRef] [Green Version]
- Ferrati, S.; Fine, D.; You, J.; De Rosa, E.; Hudson, L.; Zabre, E.; Hosali, S.; Zhang, L.; Hickman, C.; Bansal, S.S.; et al. Leveraging nanochannels for universal, zero-order drug delivery in vivo. J. Control. Release 2013, 172, 1011–1019. [Google Scholar] [CrossRef]
- Sizovs, A.; Pons-Faudoa, F.P.; Malgir, G.; Shelton, K.A.; Bushman, L.R.; Chua, C.Y.X.; Anderson, P.L.; Nehete, P.N.; Sastry, K.J.; Grattoni, A. Trans-urocanic acid enhances tenofovir alafenamide stability for long-acting HIV applications. Int. J. Pharm. 2020, 587, 119623. [Google Scholar] [CrossRef]
- Grattoni, A.; De Rosa, E.; Ferrati, S.; Wang, Z.; Gianesini, A.; Liu, X.; Hussain, F.; Goodall, R.; Ferrari, M. Analysis of a nanochanneled membrane structure through convective gas flow. J. Micromech. Microeng. 2009, 19, 115018. [Google Scholar] [CrossRef]
- Scorrano, G.; Bruno, G.; Di Trani, N.; Ferrari, M.; Pimpinelli, A.; Grattoni, A. Gas Flow at the Ultra-nanoscale: Universal Predictive Model and Validation in Nanochannels of Ångstrom-Level Resolution. ACS Appl. Mater. Interfaces 2018, 10, 32233–32238. [Google Scholar] [CrossRef] [PubMed]
- Oliveros, A.; Guiseppi-Elie, A.; Saddow, S.E. Silicon carbide: A versatile material for biosensor applications. Biomed. Microdevices 2013, 15, 353–368. [Google Scholar] [CrossRef]
- Zorman, C.A.; Eldridge, A.; Du, J.G.; Johnston, M.; Dubnisheva, A.; Manley, S.; Fissell, W.; Fleischman, A.; Roy, S. Amorphous silicon carbide as a non-biofouling structural material for biomedical microdevices. In Materials Science Forum; Trans Tech Publications Ltd.: Stafa-Zurich, Switzerland, 2012; pp. 537–540. [Google Scholar]
- Cogan, S.F.; Edell, D.J.; Guzelian, A.A.; Liu, Y.P.; Edell, R. Plasma-enhanced chemical vapor deposited silicon carbide as an implantable dielectric coating. J. Biomed. Mater. Res. 2003, 67, 856–867. [Google Scholar] [CrossRef]
- Ballerini, A.; Chua, C.Y.X.; Rhudy, J.; Susnjar, A.; Di Trani, N.; Jain, P.R.; Laue, G.; Lubicka, D.; Shirazi-Fard, Y.; Ferrari, M.; et al. Counteracting Muscle Atrophy on Earth and in Space via Nanofluidics Delivery of Formoterol. Adv. Ther. 2020, 2000014. [Google Scholar] [CrossRef]
- Chua, C.Y.X.; Ho, J.; Susnjar, A.; Lolli, G.; Di Trani, N.; Pesaresi, F.; Zhang, M.; Nance, E.; Grattoni, A. Intratumoral Nanofluidic System for Enhancing Tumor Biodistribution of Agonist CD40 Antibody. Adv. Ther. 2020. [Google Scholar] [CrossRef]
- Chua, C.Y.X.; Jain, P.; Susnjar, A.; Rhudy, J.; Folci, M.; Ballerini, A.; Gilbert, A.; Singh, S.; Bruno, G.; Filgueira, C.S.; et al. Nanofluidic drug-eluting seed for sustained intratumoral immunotherapy in triple negative breast cancer. J. Control. Release 2018, 285, 23–34. [Google Scholar] [CrossRef] [PubMed]
- Filgueira, C.S.; Nicolov, E.; Hood, R.L.; Ballerini, A.; Garcia-Huidobro, J.; Lin, J.Z.; Fraga, D.; Webb, P.; Sabek, O.M.; Gaber, A.O.; et al. Sustained zero-order delivery of GC-1 from a nanochannel membrane device alleviates metabolic syndrome. Int. J. Obes. 2016, 40, 1776–1783. [Google Scholar] [CrossRef]
- Grattoni, A.; Fine, D.; Zabre, E.; Ziemys, A.; Gill, J.; Mackeyev, Y.; Cheney, M.A.; Danila, D.C.; Hosali, S.; Wilson, L.J.; et al. Gated and Near-Surface Diffusion of Charged Fullerenes in Nanochannels. ACS Nano 2011, 5, 9382–9391. [Google Scholar] [CrossRef]
- Ferrati, S.; Nicolov, E.; Zabre, E.; Geninatti, T.; Shirkey, B.A.; Hudson, L.; Hosali, S.; Crawley, M.; Khera, M.; Palapattu, G.; et al. The Nanochannel Delivery System for Constant Testosterone Replacement Therapy. J. Sex. Med. 2015, 12, 1375–1380. [Google Scholar] [CrossRef] [Green Version]
- Fletcher, C.V.; Staskus, K.; Wietgrefe, S.W.; Rothenberger, M.; Reilly, C.; Chipman, J.G.; Beilman, G.J.; Khoruts, A.; Thorkelson, A.; Schmidt, T.E.; et al. Persistent HIV-1 replication is associated with lower antiretroviral drug concentrations in lymphatic tissues. Proc. Natl. Acad. Sci. USA 2014, 111, 2307–2312. [Google Scholar] [CrossRef] [Green Version]
- Kzhyshkowska, J.; Gudima, A.; Riabov, V.; Dollinger, C.; LaValle, P.; Vrana, N.E. Macrophage responses to implants: Prospects for personalized medicine. J. Leukoc. Biol. 2015, 98, 953–962. [Google Scholar] [CrossRef] [Green Version]
- Ruane, P.J.; DeJesus, E.; Berger, D.; Markowitz, M.; Bredeek, U.F.; Callebaut, C.; Zhong, L.; Ramanathan, S.; Rhee, M.S.; Fordyce, M.W.; et al. Antiviral Activity, Safety, and Pharmacokinetics/Pharmacodynamics of Tenofovir Alafenamide as 10-Day Monotherapy in HIV-1–Positive Adults. JAIDS J. Acquir. Immune Defic. Syndr. 2013, 63, 449–455. [Google Scholar] [CrossRef] [Green Version]
- Polis, M.; Sidorov, I.; Yoder, C.; Jankelevich, S.; Metcalf, J.; Mueller, B.; Dimitrov, M.; Pizzo, P.; Yarchoan, R.; Dimitrov, D.; et al. Correlation between reduction in plasma HIV-1 RNA concentration 1 week after start of antiretroviral treatment and longer-term efficacy. Lancet 2001, 358, 1760–1765. [Google Scholar] [CrossRef]
- Mittler, J.; Essunger, P.; Yuen, G.J.; Clendeninn, N.; Markowitz, M.; Perelson, A.S. Short-Term Measures of Relative Efficacy Predict Longer-Term Reductions in Human Immunodeficiency Virus Type 1 RNA Levels following Nelfinavir Monotherapy. Antimicrob. Agents Chemother. 2001, 45, 1438–1443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shao, J.; Kraft, J.C.; Li, B.; Yu, J.; Freeling, J.; Koehn, J.; Ho, R.J.Y. Nanodrug formulations to enhance HIV drug exposure in lymphoid tissues and cells: Clinical significance and potential impact on treatment and eradication of HIV/AIDS. Nanomedicine 2016, 11, 545–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ho, R.J.; Yu, J.; Li, B.; Kraft, J.C.; Freeling, J.P.; Koehn, J.; Shao, J. Systems Approach to targeted and long-acting HIV/AIDS therapy. Drug Deliv. Transl. Res. 2015, 5, 531–539. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| nTAFt (NHP #) | TAF Loaded (mg) | Residual TAF * (mg) | TAF Stability (%) | TAF Release Rate (mg/day) |
|---|---|---|---|---|
| 1 | 244.1 | 173.36 | 61.86 | 2.53 |
| 2 | 257.4 | 191.64 | 41.29 | 2.35 |
| 3 | 244.1 | 110.61 | 47.50 | 4.77 |
| 4 | 248.5 | 149.06 | 55.42 | 3.55 |
| 5 | 253.0 | 193.15 | 48.27 | 2.14 |
| 6 | 276.3 | 270.41 | 96.71 | 0.21 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pons-Faudoa, F.P.; Trani, N.D.; Sizovs, A.; Shelton, K.A.; Momin, Z.; Bushman, L.R.; Xu, J.; Lewis, D.E.; Demaria, S.; Hawkins, T.; et al. Viral load Reduction in SHIV-Positive Nonhuman Primates via Long-Acting Subcutaneous Tenofovir Alafenamide Fumarate Release from a Nanofluidic Implant. Pharmaceutics 2020, 12, 981. https://doi.org/10.3390/pharmaceutics12100981
Pons-Faudoa FP, Trani ND, Sizovs A, Shelton KA, Momin Z, Bushman LR, Xu J, Lewis DE, Demaria S, Hawkins T, et al. Viral load Reduction in SHIV-Positive Nonhuman Primates via Long-Acting Subcutaneous Tenofovir Alafenamide Fumarate Release from a Nanofluidic Implant. Pharmaceutics. 2020; 12(10):981. https://doi.org/10.3390/pharmaceutics12100981
Chicago/Turabian StylePons-Faudoa, Fernanda P., Nicola Di Trani, Antons Sizovs, Kathryn A. Shelton, Zoha Momin, Lane R. Bushman, Jiaqiong Xu, Dorothy E. Lewis, Sandra Demaria, Trevor Hawkins, and et al. 2020. "Viral load Reduction in SHIV-Positive Nonhuman Primates via Long-Acting Subcutaneous Tenofovir Alafenamide Fumarate Release from a Nanofluidic Implant" Pharmaceutics 12, no. 10: 981. https://doi.org/10.3390/pharmaceutics12100981