RETRACTED: Attenuation of Benign Prostatic Hyperplasia by Optimized Tadalafil Loaded Pumpkin Seed Oil-Based Self Nanoemulsion: In Vitro and In Vivo Evaluation


Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Design TDL-PSO SNEDDS
2.1.1. TDL-PSO SNEDDS Formulation
2.1.2. TDL-PSO SNEDDS Evaluation
2.1.3. Vesicular Size and Zeta Potential
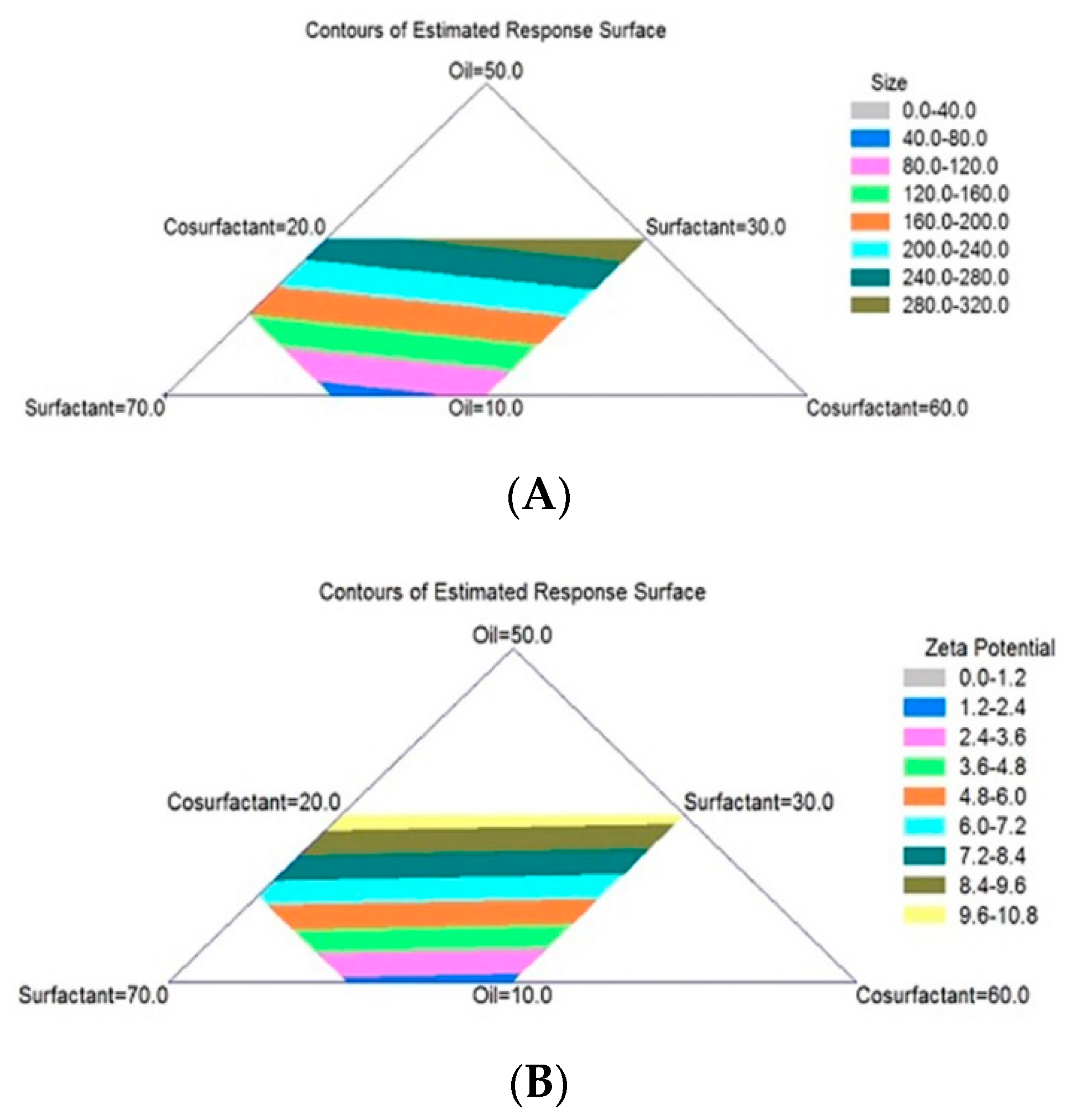
2.1.4. TDL-PSO SNEDDS Mixture Design Analysis
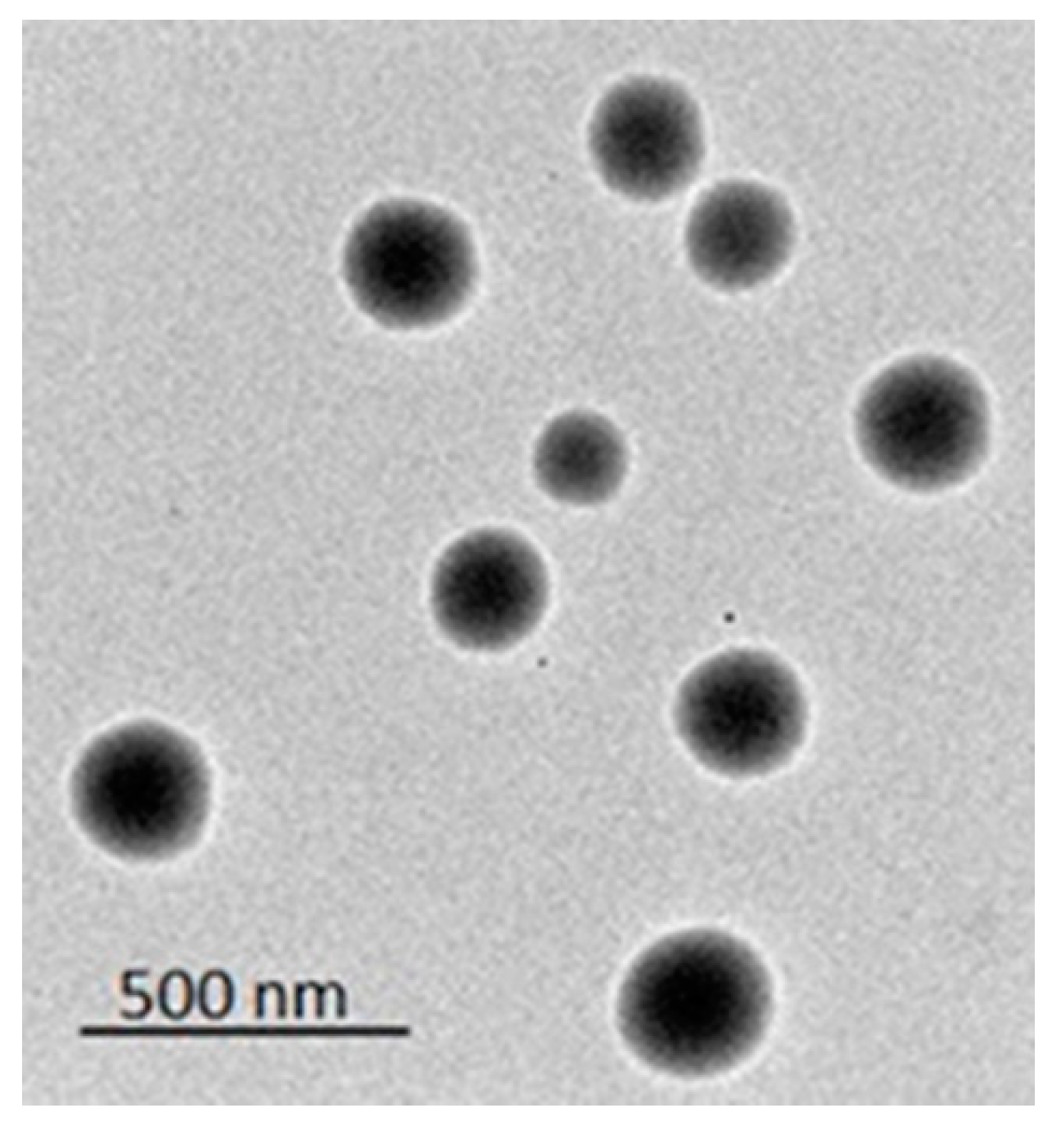
2.1.5. TDL-PSO SNEDDS Examination by Transmission Electron Microscopy
2.2. TDL-PSO SNEDDS Formulation In Vivo Studies
2.2.1. Design of In Vivo Study Protocol for the Evaluation of TDL-PSO SNEDDS Effects
2.2.2. Chromatographic Analysis of TDL Quantitation in Rat Prostates
2.2.3. Prostate Weight and Prostate Index
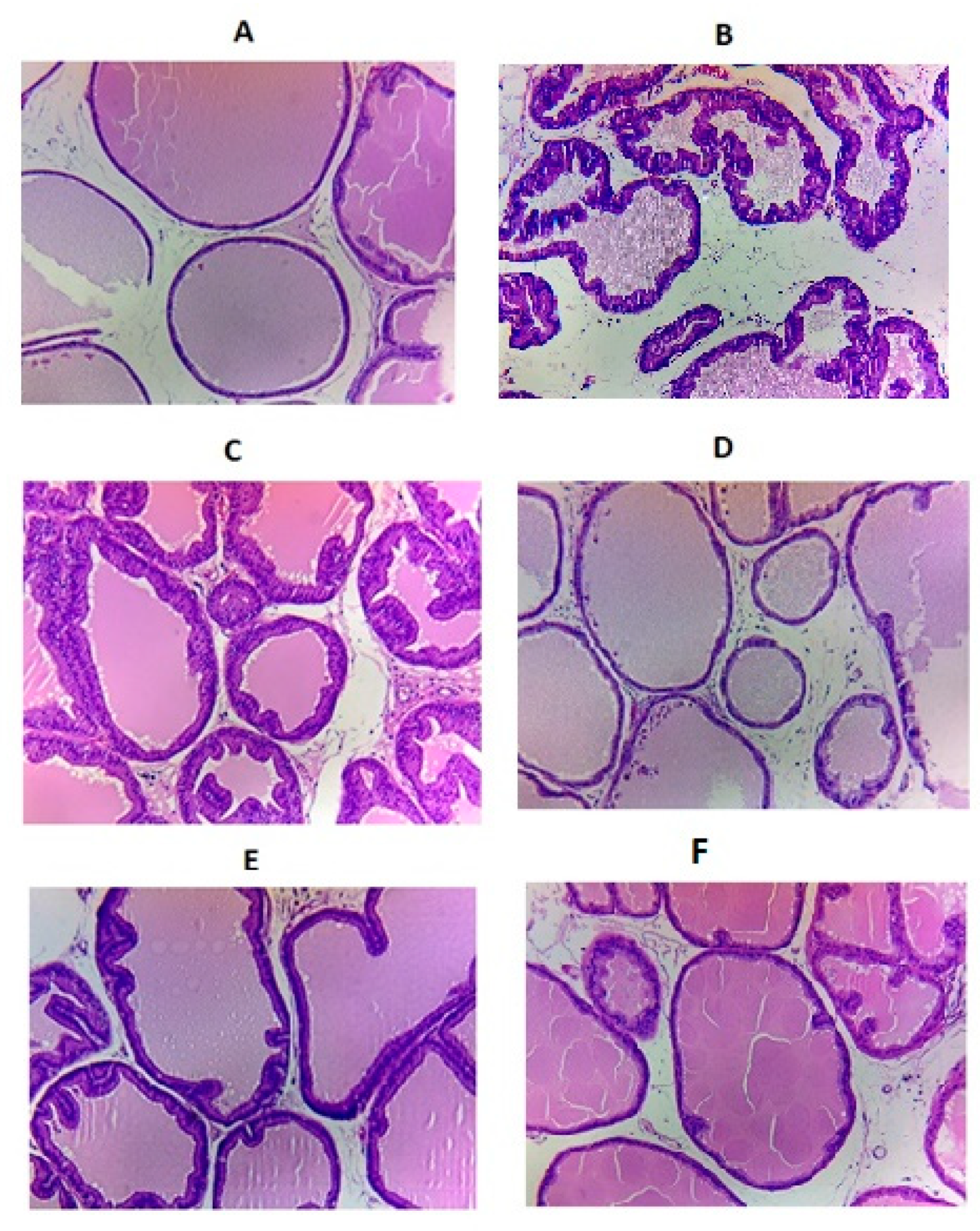
2.2.4. Histopathology
2.2.5. Pharmacokinetic Analysis
2.3. Statistical Analysis
3. Results and Discussion
3.1. Formulation and Characterization of TDL-PSO SNEDDS
3.1.1. Evaluation of TDL-PSO SNEDDS Formulation Globule Size
3.1.2. Evaluation of the TDL-PSO SNEDDS Formulation Zeta Potential
3.1.3. TDL-PSO SNEDDS Mixture Design Analysis for an Optimized Formula
3.1.4. Vesicles Examination by TEM
3.2. TDL-PSO SNEDDS Formulation In Vivo Studies
3.2.1. Prostate Weight and Prostate Index
3.2.2. Histopathological Examination
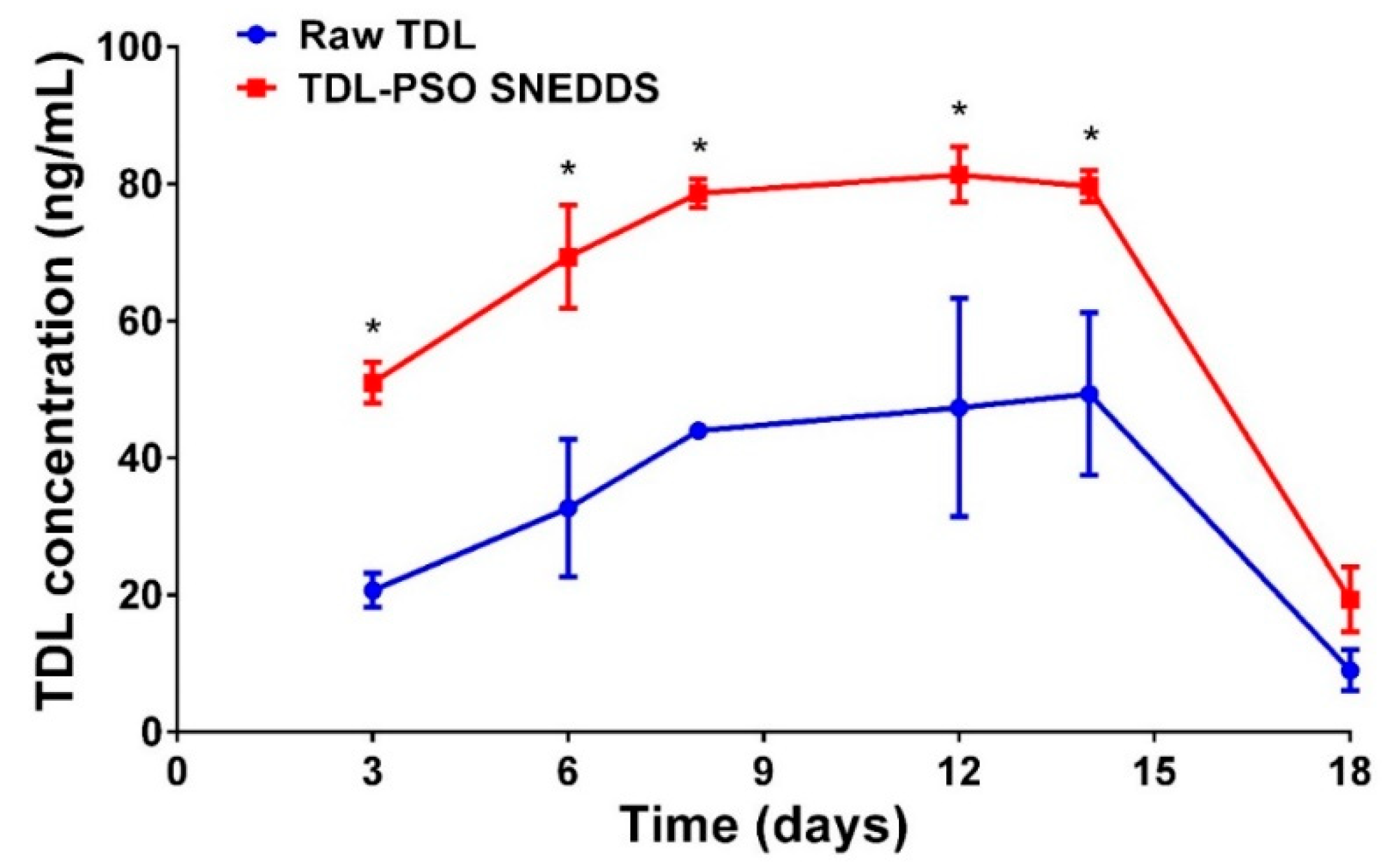
3.2.3. TDL Prostate Levels
3.2.4. In Vivo Pharmacokinetics in Prostate Tissue
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Amano, T.; Earle, C.; Imao, T.; Matsumoto, Y.; Kishikage, T. Administration of daily 5 mg tadalafil improves endothelial function in patients with benign prostatic hyperplasia. Aging Male 2018, 21, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Damiano, R.; Cai, T.; Fornara, P.; Franzese, C.A.; Leonardi, R.; Mirone, V. The role of Cucurbita pepo in the management of patients affected by lower urinary tract symptoms due to benign prostatic hyperplasia: A narrative review. Arch. Ital. Di Urol. E Androl. 2016, 88, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Egan, K.B. The Epidemiology of Benign Prostatic Hyperplasia Associated with Lower Urinary Tract Symptoms: Prevalence and Incident Rates. Urol. Clin. North Am. 2016, 43, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Vignozzi, L.; Gacci, M.; Cellai, I.; Morelli, A.; Maneschi, E.; Comeglio, P.; Santi, R.; Filippi, S.; Sebastianelli, A.; Nesi, G.; et al. PDE5 inhibitors blunt inflammation in human BPH: A potential mechanism of action for PDE5 inhibitors in LUTS. Prostate 2013, 73, 1391–1402. [Google Scholar] [CrossRef]
- Jin, S.; Xiang, P.; Liu, J.; Yang, Y.; Hu, S.; Sheng, J.; He, Q.; Yu, W.; Han, W.; Jin, J.; et al. Activation of cGMP/PKG/p65 signaling associated with PDE5-Is downregulates CCL5 secretion by CD8 + T cells in benign prostatic hyperplasia. Prostate 2019, 79, 909–919. [Google Scholar] [CrossRef]
- Zenzmaier, C.; Kern, J.; Sampson, N.; Heitz, M.; Plas, E.; Untergasser, G.; Berger, P. Phosphodiesterase type 5 inhibition reverts prostate fibroblast-to- myofibroblast Trans-differentiation. Endocrinology 2012, 153, 5546–5555. [Google Scholar] [CrossRef]
- Fibbi, B.; Morelli, A.; Vignozzi, L.; Filippi, S.; Chavalmane, A.; De Vita, G.; Marini, M.; Gacci, M.; Vannelli, G.B.; Sandner, P.; et al. Characterization of phosphodiesterase Type 5 expression and functional activity in the human male lower urinary tract. J. Sex. Med. 2010, 7, 59–69. [Google Scholar] [CrossRef]
- Lin, C.S.; Albersen, M.; Xin, Z.; Namiki, M.; Muller, D.; Lue, T.F. Phosphodiesterase-5 expression and function in the lower urinary tract: A critical review. Urology 2013, 81, 480–487. [Google Scholar] [CrossRef]
- Roehrborn, C.G.; Casabé, A.; Glina, S.; Sorsaburu, S.; Henneges, C.; Viktrup, L. Treatment satisfaction and clinically meaningful symptom improvement in men with lower urinary tract symptoms and prostatic enlargement secondary to benign prostatic hyperplasia: Secondary results from a 6-month, randomized, double-blind study comparing finasteride. Int. J. Urol. 2015, 22, 582–587. [Google Scholar]
- Gacci, M.; Corona, G.; Salvi, M.; Vignozzi, L.; McVary, K.T.; Kaplan, S.A.; Roehrborn, C.G.; Serni, S.; Mirone, V.; Carini, M.; et al. A systematic review and meta-analysis on the use of phosphodiesterase 5 inhibitors alone or in combination with α-blockers for lower urinary tract symptoms due to benign prostatic hyperplasia. Eur. Urol. 2012, 61, 994–1003. [Google Scholar] [CrossRef]
- Pisco, J.M.; Bilhim, T.; Pinheiro, L.C.; Fernandes, L.; Pereira, J.; Costa, N.V.; Duarte, M.; Oliveira, A.G. Medium- and Long-Term Outcome of Prostate Artery Embolization for Patients with Benign Prostatic Hyperplasia: Results in 630 Patients. J. Vasc. Interv. Radiol. 2016, 27, 1115–1122. [Google Scholar] [CrossRef] [PubMed]
- Brock, G.; Broderick, G.; Roehrborn, C.G.; Xu, L.; Wong, D.; Viktrup, L. Tadalafil once daily in the treatment of lower urinary tract symptoms (LUTS) suggestive of benign prostatic hyperplasia (BPH) in men without erectile dysfunction. BJU Int. 2013, 112, 990–997. [Google Scholar] [CrossRef] [PubMed]
- Carson, C.C.; Rosenberg, M.; Kissel, J.; Wong, D.G. Tadalafil—A therapeutic option in the management of BPH-LUTS. Int. J. Clin. Pract. 2014, 68, 94–103. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.T.; Wang, Y.Y.; Liu, W.S.; Cheng, C.M.; Chiu, K.H.; Liu, L.L.; Liu, X.Z.; Wen, Z.H.; Chen, Y.H.; Chen, T.M. Rhodobacter sphaeroides extract lycogenTM attenuates testosterone-induced benign prostate hyperplasia in rats. Int. J. Mol. Sci. 2018, 19, 1137. [Google Scholar] [CrossRef]
- Nawirska-Olszańska, A.; Kita, A.; Biesiada, A.; Sokół-ŁĘtowska, A.; Kucharska, A.Z. Characteristics of antioxidant activity and composition of pumpkin seed oils in 12 cultivars. Food Chem. 2013, 139, 155–161. [Google Scholar] [CrossRef]
- Bardaa, S.; Ben Halima, N.; Aloui, F.; Ben Mansour, R.; Jabeur, H.; Bouaziz, M.; Sahnoun, Z. Oil from pumpkin (Cucurbita pepo L.) seeds: Evaluation of its functional properties on wound healing in rats. Lipids Health Dis. 2016, 15, 73. [Google Scholar] [CrossRef]
- Rabrenović, B.B.; Dimić, E.B.; Novaković, M.M.; Tešević, V.V.; Basić, Z.N. The most important bioactive components of cold pressed oil from different pumpkin (Cucurbita pepo L.) seeds. LWT-Food Sci. Technol. 2014, 55, 521–527. [Google Scholar] [CrossRef]
- Procida, G.; Stancher, B.; Cateni, F.; Zacchigna, M. Chemical composition and functional characterisation of commercial pumpkin seed oil. J. Sci. Food Agric. 2013, 93, 1035–1041. [Google Scholar] [CrossRef]
- Heim, S.; Seibt, S.; Stier, H.; Moré, M.I. Uromedic® Pumpkin Seed Derived Δ7-Sterols, Extract and Oil Inhibit 5α-Reductases and Bind to Androgen Receptor in Vitro. Pharmacol. Pharm. 2018, 9, 193–207. [Google Scholar] [CrossRef]
- Vahlensieck, W.; Theurer, C.; Pfitzer, E.; Patz, B.; Banik, N.; Engelmann, U. Effects of pumpkin seed in men with lower urinary tract symptoms due to benign prostatic hyperplasia in the one-year, randomized, placebo-controlled GRANU study. Urol. Int. 2015, 94, 286–295. [Google Scholar] [CrossRef]
- Hong, H.; Kim, C.-S.; Maeng, S. Effects of pumpkin seed oil and saw palmetto oil in Korean men with symptomatic benign prostatic hyperplasia. Nutr. Res. Pract. 2009, 3, 323. [Google Scholar] [CrossRef]
- Curtis Nickel, J.; Shoskes, D.; Roehrborn, C.G.; Moyad, M. Nutraceuticals in Prostate Disease: The Urologist’s Role. Rev. Urol. 2008, 10, 192–206. [Google Scholar]
- Leibbrand, M.; Siefer, S.; Schön, C.; Perrinjaquet-Moccetti, T.; Kompek, A.; Csernich, A.; Bucar, F.; Kreuter, M.H. Effects of an Oil-Free Hydroethanolic Pumpkin Seed Extract on Symptom Frequency and Severity in Men with Benign Prostatic Hyperplasia: A Pilot Study in Humans. J. Med. Food 2019, 22, 551–559. [Google Scholar] [CrossRef]
- Ejike, C.E.C.C.; Ezeanyika, L.U.S. Inhibition of the experimental induction of benign prostatic hyperplasia: A possible role for fluted pumpkin (Telfairia occidentalis Hook f.) seeds. Urol. Int. 2011, 87, 218–224. [Google Scholar] [CrossRef]
- Berges, R.; Oelke, M. Age-stratified normal values for prostate volume, PSA, maximum urinary flow rate, IPSS, and other LUTS/BPH indicators in the German male community-dwelling population aged 50 years or older. World J. Urol. 2011, 29, 171–178. [Google Scholar] [CrossRef]
- Vesely, S.; Knutson, T.; Damber, J.E.; Dicuio, M.; Dahlstrand, C. Relationship between age, prostate volume, prostatespecific antigen, symptom score and uroflowmetry in men with lower urinary tract symptoms: Does prostate size matter? Scand. J. Urol. Nephrol. 2003, 37, 322–328. [Google Scholar] [CrossRef]
- Gratzke, C.; Bachmann, A.; Descazeaud, A.; Drake, M.J.; Madersbacher, S.; Mamoulakis, C.; Oelke, M.; Tikkinen, K.A.O.; Gravas, S. EAU guidelines on the assessment of non-neurogenic male lower urinary tract symptoms including benign prostatic obstruction. Eur. Urol. 2015, 67, 1099–1109. [Google Scholar] [CrossRef]
- Cherniakov, I.; Domb, A.J.; Hoffman, A. Self-nano-emulsifying drug delivery systems: An update of the biopharmaceutical aspects. Expert Opin. Drug Deliv. 2015, 12, 1121–1133. [Google Scholar] [CrossRef]
- Zhang, J.; Wen, X.; Dai, Y.; Xia, Y. Mechanistic studies on the absorption enhancement of a self-nanoemulsifying drug delivery system loaded with norisoboldine-phospholipid complex. Int. J. Nanomed. 2019, 14, 7095–7106. [Google Scholar] [CrossRef]
- Fahmy, U.A.; Ahmed, O.A.; Hosny, K. Development and Evaluation of Avanafil Self-nanoemulsifying Drug Delivery System with Rapid Onset of Action and Enhanced Bioavailability. AAPS PharmSciTech 2014, 16, 53–58. [Google Scholar] [CrossRef]
- Ahmed, O.A.A.; Badr-Eldin, S.M.; Tawfik, M.K.; Ahmed, T.A.; El-Say, K.M.; Badr, J.M. Design and optimization of self-nanoemulsifying delivery system to enhance quercetin hepatoprotective activity in paracetamol-induced hepatotoxicity. J. Pharm. Sci. 2014, 103, 602–612. [Google Scholar] [CrossRef]
- El-Say, K.M.; Ahmed, T.A.; Ahmed, O.A.A.; Hosny, K.M.; Abd-Allah, F.I. Self-Nanoemulsifying Lyophilized Tablets for Flash Oral Transmucosal Delivery of Vitamin K: Development and Clinical Evaluation. J. Pharm. Sci. 2017, 106, 2447–2456. [Google Scholar] [CrossRef]
- Ahmed, O.A.A.; Afouna, M.I.; El-Say, K.M.; Abdel-Naim, A.B.; Khedr, A.; Banjar, Z.M. Optimization of self-nanoemulsifying systems for the enhancement of in vivo hypoglycemic efficacy of glimepiride transdermal patches. Expert Opin. Drug Deliv. 2014, 11, 1005–1013. [Google Scholar] [CrossRef]
- Fahmy, U.A.; Aljaeid, B.M. Tadalafil transdermal delivery with alpha-lipoic acid self nanoemulsion for treatment of erectile dysfunction by diabetes mellitus. Int. J. Pharmacol. 2018, 14, 945–951. [Google Scholar] [CrossRef]
- Abdel-Naim, A.B.; Neamatallah, T.; Eid, B.G.; Esmat, A.; Alamoudi, A.J.; Abd El-Aziz, G.S.; Ashour, O.M. 2-Methoxyestradiol attenuates testosterone-induced benign prostate hyperplasia in rats through inhibition of HIF-1 α /TGF- β /Smad2 Axis. Oxid. Med. Cell. Longev. 2018, 2018, 4389484. [Google Scholar] [CrossRef]
- Pappula, N.; Kodali, B.; Datla, P.V. Selective and rapid determination of tadalafil and finasteride using solid phase extraction by high performance liquid chromatography and tandem mass spectrometry. J. Pharm. Biomed. Anal. 2018, 152, 215–223. [Google Scholar] [CrossRef]
- Oh, N.; Park, J.H. Endocytosis and exocytosis of nanoparticles in mammalian cells. Int. J. Nanomed. 2014, 9, 51–63. [Google Scholar]
- Zaki, N.M.; Tirelli, N. Gateways for the intracellular access of nanocarriers: A review of receptor-mediated endocytosis mechanisms and of strategies in receptor targeting. Expert Opin. Drug Deliv. 2010, 7, 895–913. [Google Scholar] [CrossRef]
- Liu, C.; Lv, L.; Guo, W.; Mo, L.; Huang, Y.; Li, G.; Huang, X. Self-Nanoemulsifying Drug Delivery System of Tetrandrine for Improved Bioavailability: Physicochemical Characterization and Pharmacokinetic Study. BioMed Res. Int. 2018, 2018, 6763057. [Google Scholar] [CrossRef]
- Basalious, E.B.E.B.; Shawky, N.; Badr-Eldin, S.M.S.M. SNEDDS containing bioenhancers for improvement of dissolution and oral absorption of lacidipine. I: Development and optimization. Int. J. Pharm. 2010, 391, 203–211. [Google Scholar] [CrossRef]
- European Medicines Agency. Cialis. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/cialis (accessed on 16 November 2019).
- U.S. Food and Drug Administration. Drug Approval Package: Cialis (tadalafil) NDA #021368. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2003/21-368_cialis.cfm (accessed on 16 November 2019).
- Cruz, R.C.B.; Meurer, C.D.; Silva, E.J.; Schaefer, C.; Santos, A.R.S.; Bella Cruz, A.; Cechinel Filho, V. Toxicity evaluation of Cucurbita maxima seed extract in mice. Pharm. Biol. 2006, 44, 301–303. [Google Scholar] [CrossRef]
- Abou-Zeid, S.M.; AbuBakr, H.O.; Mohamed, M.A.; El-Bahrawy, A. Ameliorative effect of pumpkin seed oil against emamectin induced toxicity in mice. Biomed. Pharmacother. 2018, 98, 242–251. [Google Scholar] [CrossRef]
- Sayed, F.; Aal, A. The Protective Effect of Pumpkin Seed Oil on Azathioprine–Induced Hepatic Toxicity in Adult Male Albino Rats: Histological and Immunohistochemical Study. Basic Sci. Med. 2014, 3, 85–100. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factors | Levels | ||
| Low | High | ||
| PSO (%) | 10 | 30 | |
| Tween 80 (%) | 30 | 60 | |
| PEG 200 (%) | 20 | 40 | |
| Responses | Low | High | Goal |
| Globule size (nm) | 55 | 324 | Minimize |
| Zeta potential (mV) | 1.45 | 13.75 | Maximize |
| TDL-PSO SNEDDS Formula | Factors (X1–X3) | Responses (Y1–Y2) | |||||
|---|---|---|---|---|---|---|---|
| PSO (%) | Tween 80 (%) | PEG 200 (%) | Globule Size (nm) | Zeta Potential (mV) | |||
| Observed | Fitted | Observed | Fitted | ||||
| 1 | 30 | 50 | 20 | 287.0 | 269.65 | 13.75 | 10.36 |
| 2 | 30 | 30 | 40 | 324.0 | 313.99 | 10.70 | 10.03 |
| 3 | 20 | 60 | 20 | 160.0 | 155.00 | 5.98 | 6.35 |
| 4 | 10 | 60 | 30 | 55.0 | 62.53 | 1.45 | 2.17 |
| 5 | 10 | 50 | 40 | 89.0 | 84.70 | 0.76 | 2.01 |
| 6 | 25 | 50 | 25 | 197.0 | 223.41 | 6.22 | 8.27 |
| 7 | 25 | 40 | 35 | 209.0 | 245.58 | 4.70 | 8.11 |
| 8 | 20 | 55 | 25 | 183.0 | 166.09 | 7.6 | 6.26 |
| 9 | 15 | 55 | 30 | 135.0 | 119.85 | 6.89 | 4.18 |
| 10 | 15 | 50 | 35 | 145.0 | 130.94 | 6.10 | 4.09 |
| 11 | 30 | 40 | 30 | 324.0 | 291.82 | 9.50 | 10.20 |
| 12 | 25 | 55 | 20 | 189.0 | 212.32 | 7.10 | 8.35 |
| 13 | 20 | 50 | 30 | 167.0 | 177.17 | 6.29 | 6.18 |
| 14 | 20 | 40 | 40 | 189.0 | 199.34 | 8.30 | 6.02 |
| 15 | 15 | 60 | 25 | 110.0 | 108.76 | 3.45 | 4.26 |
| 16 | 10 | 55 | 35 | 78.0 | 73.61 | 2.10 | 2.09 |
| 17 | 20 | 50 | 30 | 171.0 | 177.17 | 4.30 | 6.18 |
| Group | Rat Weight | Prostate Weight | Prostate Index (× 103) |
|---|---|---|---|
| Group 1 (Normal) | 267.4 ± 4.72 | 0.68 ± 0.04 | 2.54 ± 0.15 |
| Group 2 (Testosterone only) | 265.2 ± 21.99 | 1.07 ± 0.13 | 4.03 ± 0.39 |
| Group 3 (Plain formula) | 270.0 ± 16.60 | 1.09 ± 0.15 | 4.04 ± 0.49 |
| Group 4 optimized (TDL-PSO SNEDDS) | 270.6 ± 15.77 | 0.69 ± 0.04 *$#& | 2.55 ± 0.20 *$#& |
| Group 5 (TDL) | 257.4 ± 21.97 | 0.85 ± 0.04 | 3.30 ± 0.39 |
| Group 6 (PSO) | 280.2 ± 13.81 | 0.86 ± 0.08 | 3.07 ± 0.35 |
| Parameter | Unit | TDL | TDL-PSO SNEDDS |
|---|---|---|---|
| Cmax | ng/mL | 38.69 ± 6.5 | 88.10 ± 7.6 * |
| AUC 0–t | ng/mL *d | 494.96 ± 34.2 | 1187.81 ± 89.2 * |
| Ke | 1/d | 0.43 ± 0.06 | 0.36 ± 0.06 |
| t1/2 | d | 1.63 ± 0.20 | 1.96 ± 0.30 |
| Tmax | d | 11.3 ± 3.05 | 12.7 ± 1.15 |
| MRT 0–inf_obs | d | 10.45 ± 0.41 | 10.12 ± 0.21 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alhakamy, N.A.; Fahmy, U.A.; Ahmed, O.A.A. RETRACTED: Attenuation of Benign Prostatic Hyperplasia by Optimized Tadalafil Loaded Pumpkin Seed Oil-Based Self Nanoemulsion: In Vitro and In Vivo Evaluation. Pharmaceutics 2019, 11, 640. https://doi.org/10.3390/pharmaceutics11120640
Alhakamy NA, Fahmy UA, Ahmed OAA. RETRACTED: Attenuation of Benign Prostatic Hyperplasia by Optimized Tadalafil Loaded Pumpkin Seed Oil-Based Self Nanoemulsion: In Vitro and In Vivo Evaluation. Pharmaceutics. 2019; 11(12):640. https://doi.org/10.3390/pharmaceutics11120640
Chicago/Turabian StyleAlhakamy, Nabil A., Usama A. Fahmy, and Osama A. A. Ahmed. 2019. "RETRACTED: Attenuation of Benign Prostatic Hyperplasia by Optimized Tadalafil Loaded Pumpkin Seed Oil-Based Self Nanoemulsion: In Vitro and In Vivo Evaluation" Pharmaceutics 11, no. 12: 640. https://doi.org/10.3390/pharmaceutics11120640