
A Deep Analysis of Brain Tumor Detection from MR Images Using Deep Learning Networks


Abstract
:1. Introduction
- Primary brain tumors: Primary brain tumors are those that develop in the brain. A primary brain tumor may develop from the brain cells and may be encased in nerve cells that surround the brain. This type of brain tumor can be benign or malignant [18].
- Secondary brain tumors: The majority of brain malignancies are secondary brain tumors, which are cancerous and fatal. Breast cancer, kidney cancer, or skin cancer are examples of conditions that begin in one area of the body and progress to the brain. Although benign tumors do not migrate from one section of the body to the other, secondary brain tumors are invariably cancerous [19].
2. Related Works
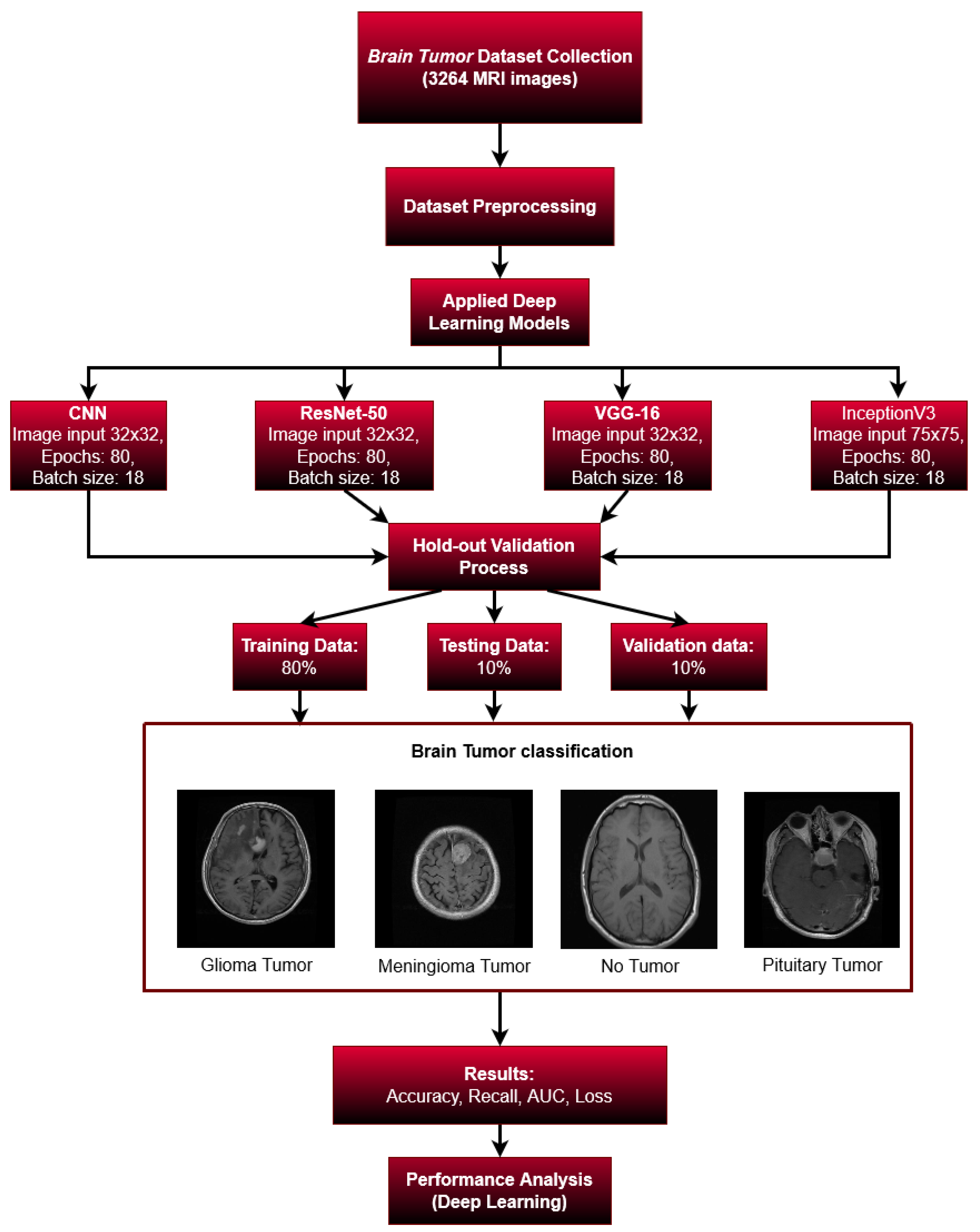
3. Methodology
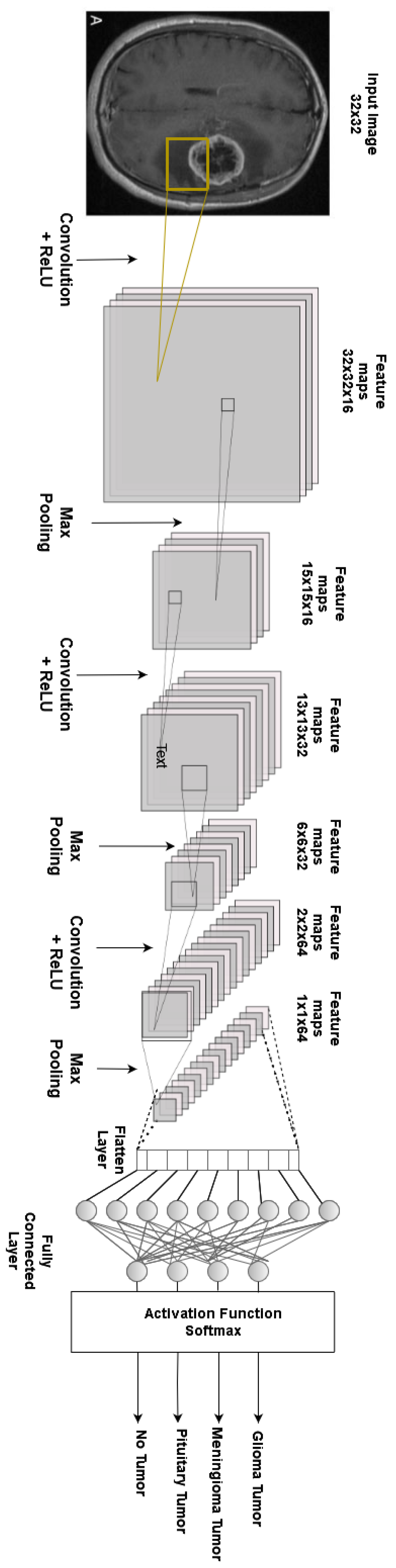
3.1. Proposed Architecture
3.2. Environment Setup
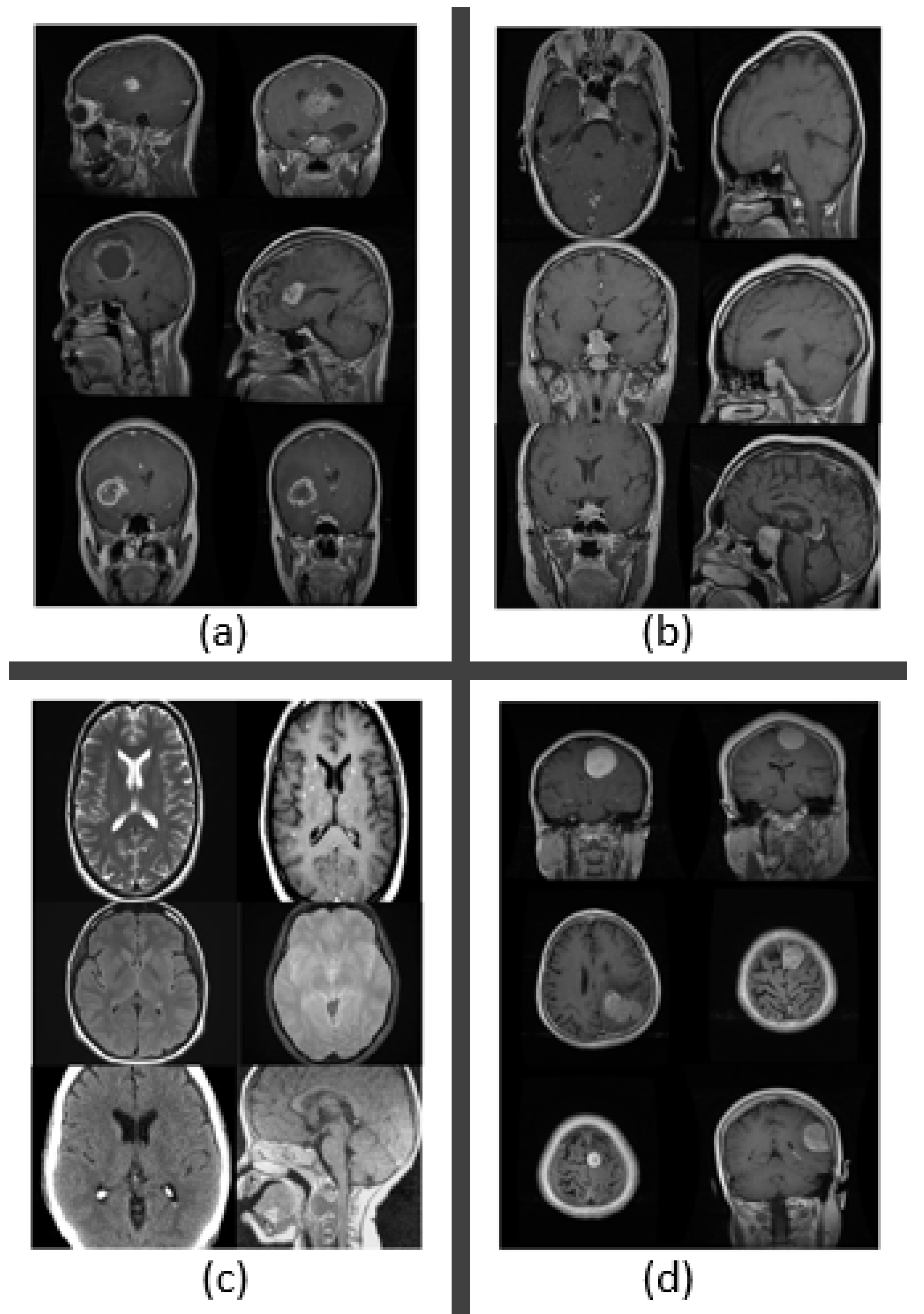
3.3. Dataset Collection
3.4. Pre-Processing of the Dataset
3.5. Data Division and Augmentation
3.6. Validation Process
3.7. Performance Metrics
3.7.1. Accuracy
- TP = True positive;
- TN = True negative;
- FN = False negative;
- FP = False positive.
3.7.2. Recall
3.7.3. Area under the Curve
4. Machine Learning Models
4.1. Transfer Learning Models
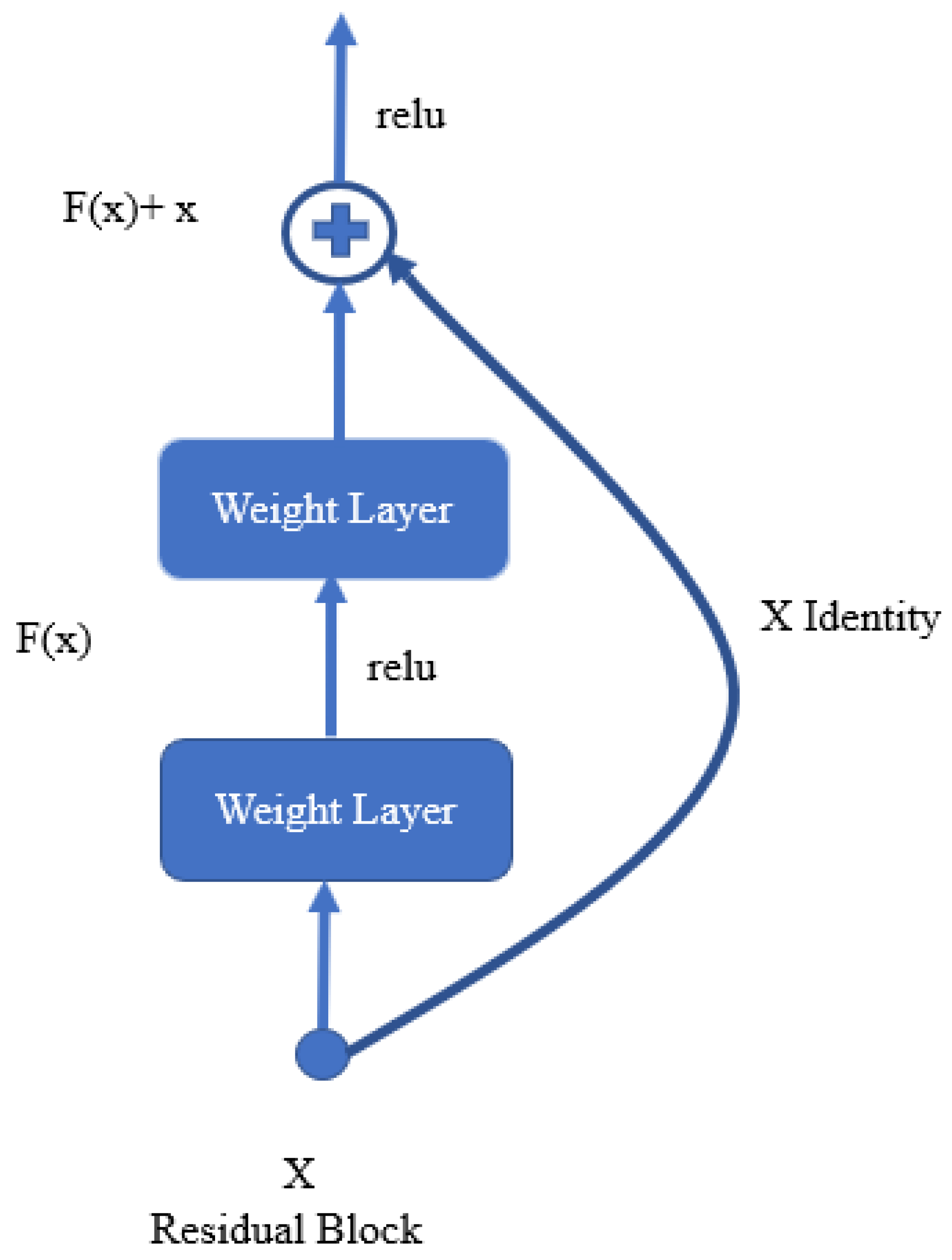
4.1.1. ResNet-50
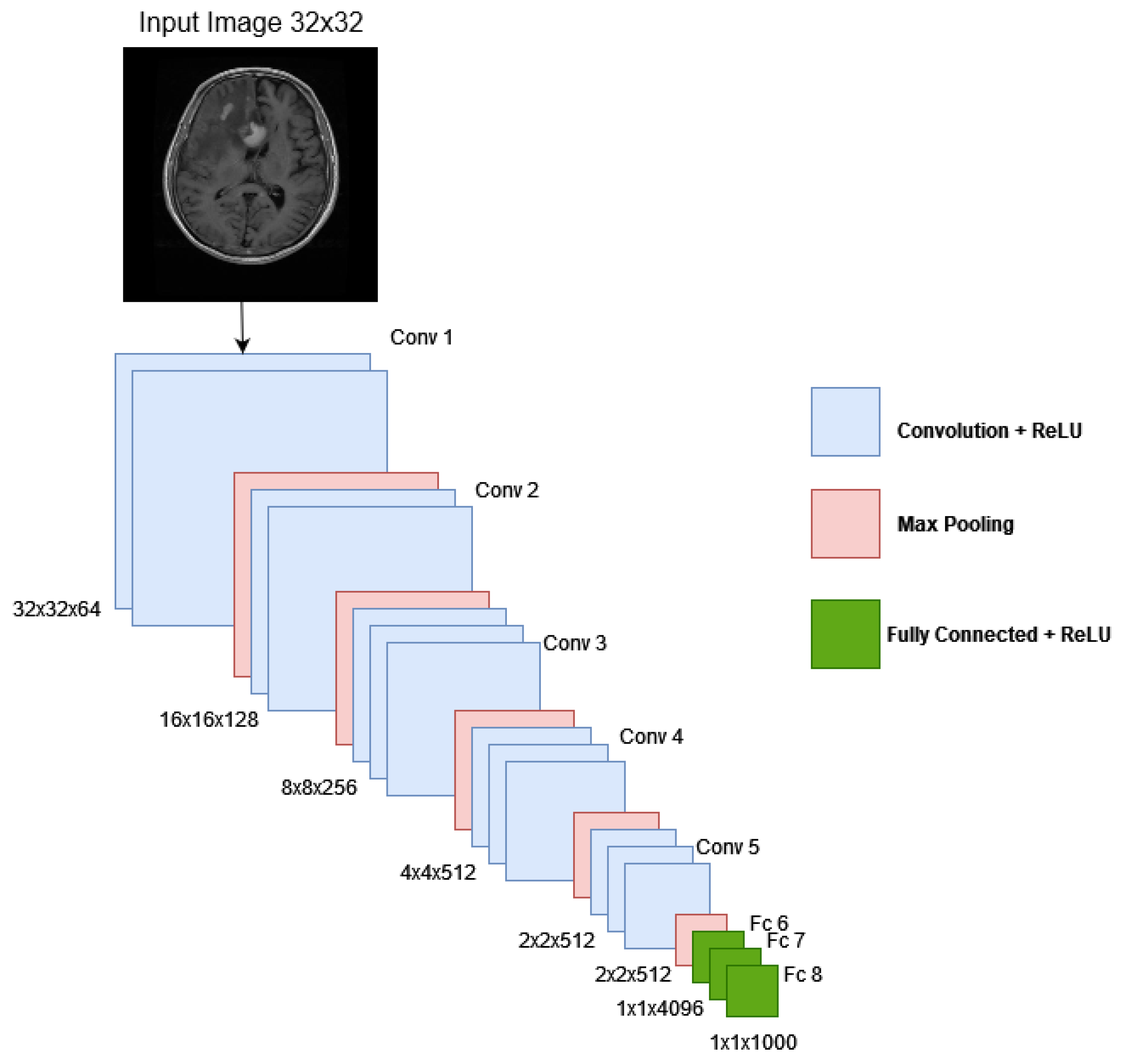
4.1.2. VGG16
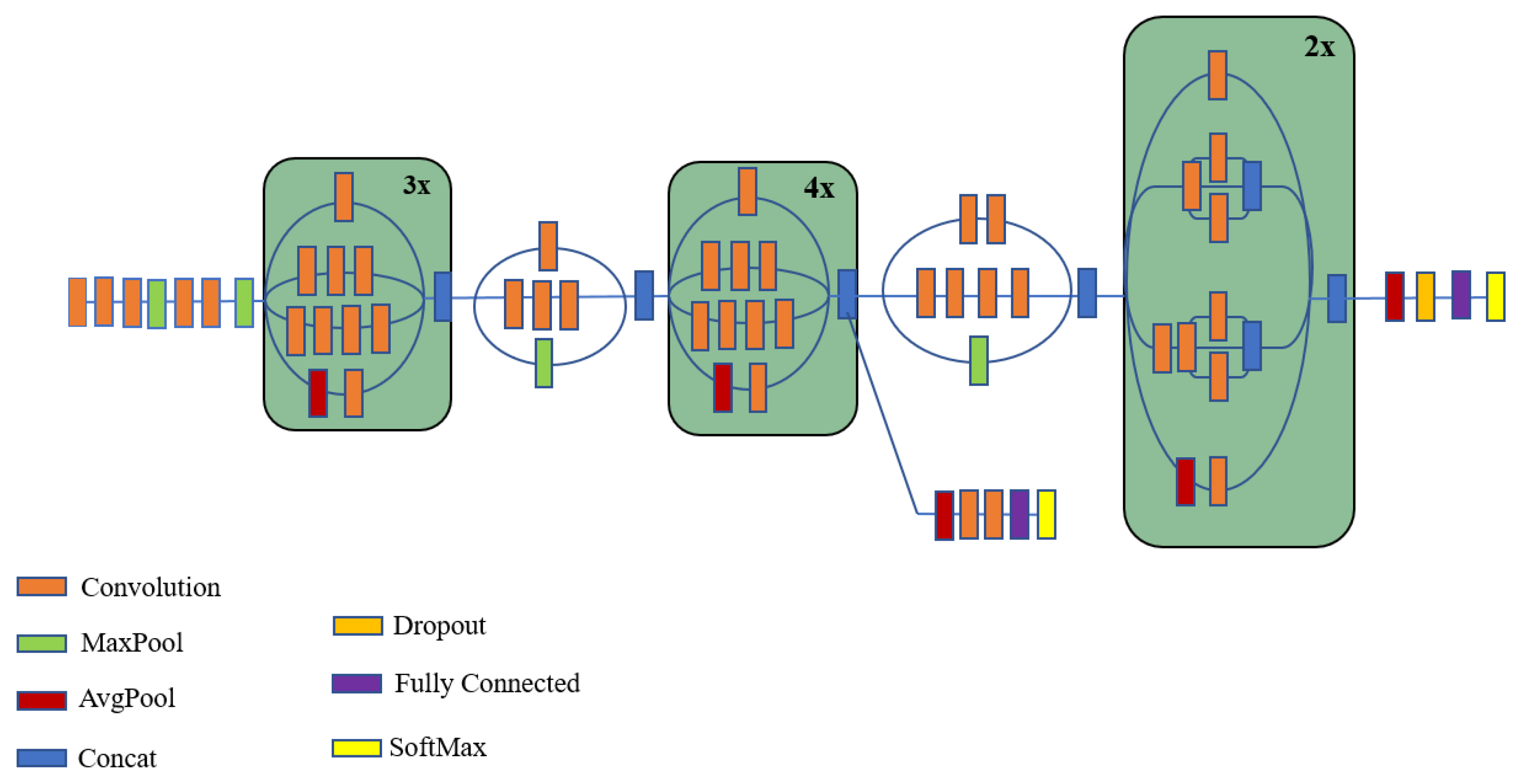
4.1.3. Inception V3
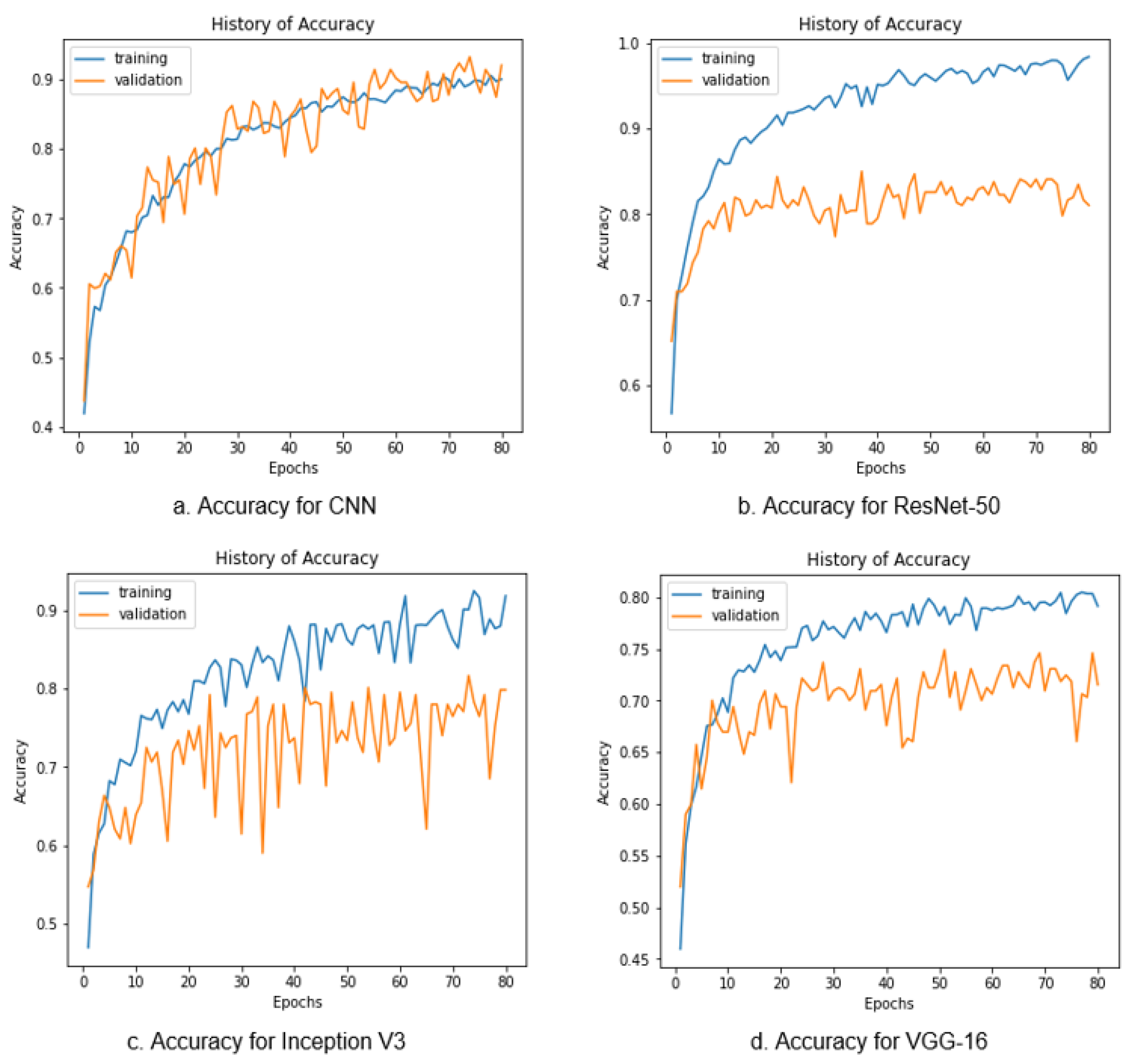
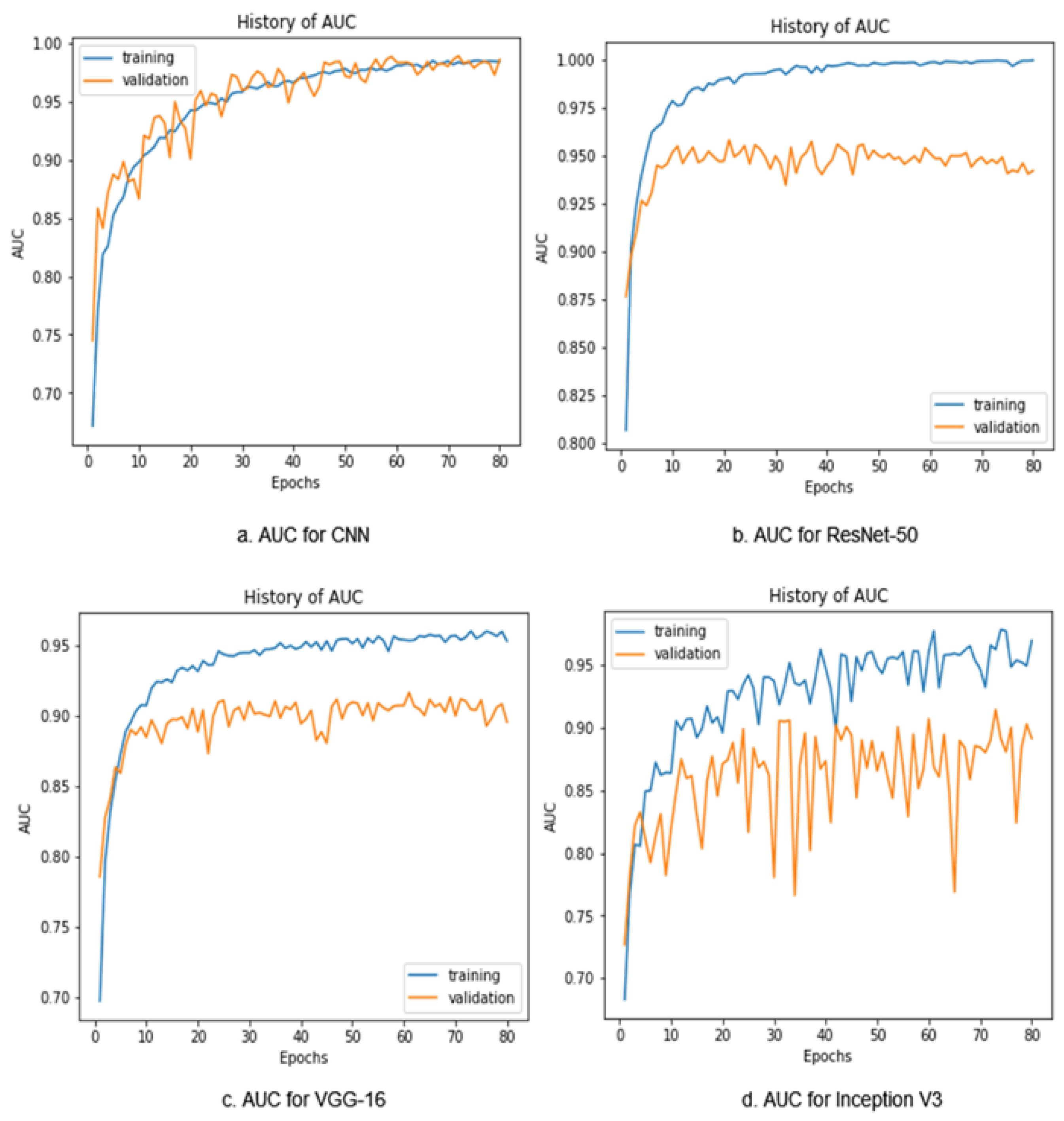
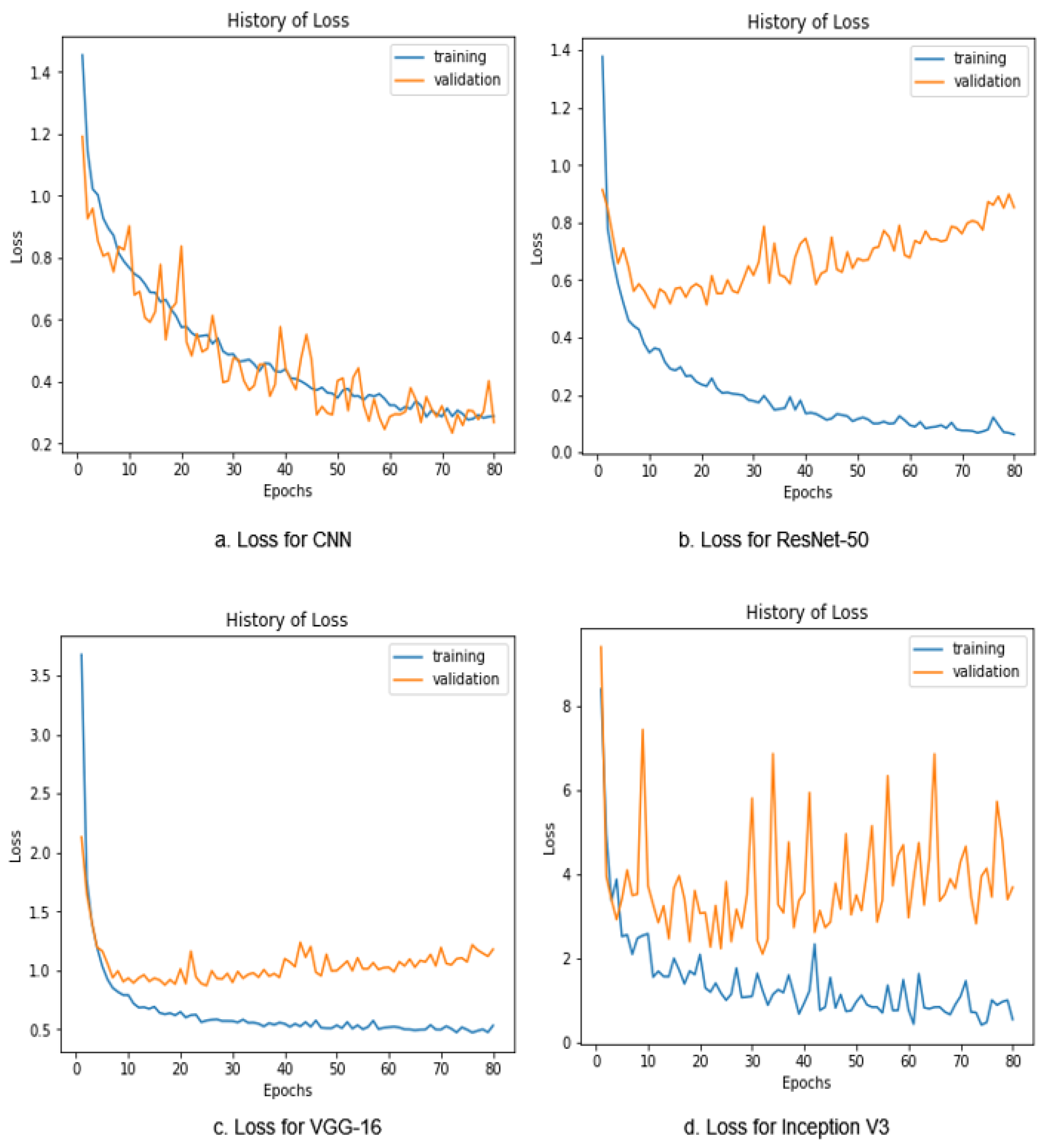
5. Results’ Analysis and Discussion
6. Conclusions and Future Works
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Qureshi, S.A.; Raza, S.E.A.; Hussain, L.; Malibari, A.A.; Nour, M.K.; Rehman, A.U.; Al-Wesabi, F.N.; Hilal, A.M. Intelligent Ultra-Light Deep Learning Model for Multi-Class Brain Tumor Detection. Appl. Sci. 2022, 12, 3715. [Google Scholar] [CrossRef]
- Zahoor, M.M.; Qureshi, S.A.; Bibi, S.; Khan, S.H.; Khan, A.; Ghafoor, U.; Bhutta, M.R. A New Deep Hybrid Boosted and Ensemble Learning-Based Brain Tumor Analysis Using MRI. Sensors 2022, 22, 2726. [Google Scholar] [CrossRef] [PubMed]
- Arabahmadi, M.; Farahbakhsh, R.; Rezazadeh, J. Deep Learning for Smart Healthcare—A Survey on Brain Tumor Detection from Medical Imaging. Sensors 2022, 22, 1960. [Google Scholar] [CrossRef] [PubMed]
- Tandel, G.S.; Biswas, M.; Kakde, O.G.; Tiwari, A.; Suri, H.S.; Turk, M.; Laird, J.R.; Asare, C.K.; Ankrah, A.A.; Khanna, N.; et al. A review on a deep learning perspective in brain cancer classification. Cancers 2019, 11, 111. [Google Scholar] [CrossRef] [Green Version]
- Gore, D.V.; Deshpande, V. Comparative study of various techniques using deep Learning for brain tumor detection. In Proceedings of the 2020 IEEE International Conference for Emerging Technology (INCET), Belgaum, India, 5–7 June 2020; pp. 1–4. [Google Scholar]
- DeAngelis, L.M. Brain tumors. N. Engl. J. Med. 2001, 344, 114–123. [Google Scholar] [CrossRef] [Green Version]
- Borole, V.Y.; Nimbhore, S.S.; Kawthekar, D.S.S. Image processing techniques for brain tumor detection: A review. Int. J. Emerg. Trends Technol. Comput. Sci. (IJETTCS) 2015, 4, 2. [Google Scholar]
- Amin, J.; Sharif, M.; Yasmin, M.; Fernandes, S.L. Big data analysis for brain tumor detection: Deep convolutional neural networks. Future Gener. Comput. Syst. 2018, 87, 290–297. [Google Scholar] [CrossRef]
- Iorgulescu, J.B.; Sun, C.; Neff, C.; Cioffi, G.; Gutierrez, C.; Kruchko, C.; Ruhl, J.; Waite, K.A.; Negoita, S.; Hofferkamp, J.; et al. Molecular biomarker-defined brain tumors: Epidemiology, validity, and completeness in the United States. Neuro-Oncology 2022, 24, 1989–2000. [Google Scholar] [CrossRef]
- Mabray, M.C.; Barajas, R.F.; Cha, S. Modern brain tumor imaging. Brain Tumor Res. Treat. 2015, 3, 8–23. [Google Scholar] [CrossRef] [Green Version]
- Cha, S. Update on brain tumor imaging: From anatomy to physiology. Am. J. Neuroradiol. 2006, 27, 475–487. [Google Scholar]
- Ranjbarzadeh, R.; Bagherian Kasgari, A.; Jafarzadeh Ghoushchi, S.; Anari, S.; Naseri, M.; Bendechache, M. Brain tumor segmentation based on deep learning and an attention mechanism using MRI multi-modalities brain images. Sci. Rep. 2021, 11, 10930. [Google Scholar] [CrossRef] [PubMed]
- Tiwari, P.; Pant, B.; Elarabawy, M.M.; Abd-Elnaby, M.; Mohd, N.; Dhiman, G.; Sharma, S. CNN Based Multiclass Brain Tumor Detection Using Medical Imaging. Comput. Intell. Neurosci. 2022, 2022, 1830010. [Google Scholar] [CrossRef] [PubMed]
- Anaya-Isaza, A.; Mera-Jiménez, L. Data Augmentation and Transfer Learning for Brain Tumor Detection in Magnetic Resonance Imaging. IEEE Access 2022, 10, 23217–23233. [Google Scholar] [CrossRef]
- Lotlikar, V.S.; Satpute, N.; Gupta, A. Brain Tumor Detection Using Machine Learning and Deep Learning: A Review. Curr. Med. Imaging 2022, 18, 604–622. [Google Scholar] [CrossRef]
- Xie, Y.; Zaccagna, F.; Rundo, L.; Testa, C.; Agati, R.; Lodi, R.; Manners, D.N.; Tonon, C. Convolutional neural network techniques for brain tumor classification (from 2015 to 2022): Review, challenges, and future perspectives. Diagnostics 2022, 12, 1850. [Google Scholar] [CrossRef]
- Almadhoun, H.R.; Abu-Naser, S.S. Detection of Brain Tumor Using Deep Learning. Int. J. Acad. Eng. Res. (IJAER) 2022, 6, 29–47. [Google Scholar]
- Sapra, P.; Singh, R.; Khurana, S. Brain tumor detection using neural network. Int. J. Sci. Mod. Eng. (IJISME) ISSN 2013, 1, 2319–6386. [Google Scholar]
- Soomro, T.A.; Zheng, L.; Afifi, A.J.; Ali, A.; Soomro, S.; Yin, M.; Gao, J. Image Segmentation for MR Brain Tumor Detection Using Machine Learning: A Review. IEEE Rev. Biomed. Eng. 2022, 16, 70–90. [Google Scholar] [CrossRef]
- Cancer-Types. Brain Tumor: Statistics. 2022. Available online: https://www.cancer.net/cancer-types/brain-tumor/statistics (accessed on 15 November 2022).
- Zhang, Y.; Li, A.; Peng, C.; Wang, M. Improve glioblastoma multiforme prognosis prediction by using feature selection and multiple kernel learning. IEEE/ACM Trans. Comput. Biol. Bioinform. 2016, 13, 825–835. [Google Scholar] [CrossRef]
- Vaishnav, P.K.; Sharma, S.; Sharma, P. Analytical review analysis for screening COVID-19 disease. Int. J. Mod. Res. 2021, 1, 22–29. [Google Scholar]
- Mamun, M.; Bin Shawkat, S.; Ahammed, M.S.; Uddin, M.M.; Mahmud, M.I.; Islam, A.M. Deep Learning Based Model for Alzheimer’s Disease Detection Using Brain MRI Images. In Proceedings of the 2022 IEEE 13th Annual Ubiquitous Computing, Electronics, and Mobile Communication Conference (UEMCON), New York, NY, USA, 26–29 October 2022; pp. 510–516. [Google Scholar] [CrossRef]
- Chatterjee, I. Artificial intelligence and patentability: Review and discussions. Int. J. Mod. Res. 2021, 1, 15–21. [Google Scholar]
- Mamun, M.; Mahmud, M.I.; Hossain, M.I.; Islam, A.M.; Ahammed, M.S.; Uddin, M.M. Vocal Feature Guided Detection of Parkinson’s Disease Using Machine Learning Algorithms. In Proceedings of the 2022 IEEE 13th Annual Ubiquitous Computing, Electronics, and Mobile Communication Conference (UEMCON), New York, NY, USA, 26–29 October 2022; pp. 566–572. [Google Scholar] [CrossRef]
- Mamun, M.; Uddin, M.M.; Kumar Tiwari, V.; Islam, A.M.; Ferdous, A.U. MLHeartDis:Can Machine Learning Techniques Enable to Predict Heart Diseases? In Proceedings of the 2022 IEEE 13th Annual Ubiquitous Computing, Electronics, and Mobile Communication Conference (UEMCON), New York, NY, USA, 26–29 October 2022; pp. 561–565. [Google Scholar] [CrossRef]
- Mahmud, M.I.; Mamun, M.; Abdelgawad, A. A Deep Analysis of Textual Features Based Cyberbullying Detection Using Machine Learning. In Proceedings of the 2022 IEEE Global Conference on Artificial Intelligence and Internet of Things (GCAIoT), Maidu, Egypt, 18–21 December 2022; pp. 166–170. [Google Scholar] [CrossRef]
- Usman, K.; Rajpoot, K. Brain tumor classification from multi-modality MRI using wavelets and machine learning. Pattern Anal. Appl. 2017, 20, 871–881. [Google Scholar] [CrossRef] [Green Version]
- Shao, C.; Yang, Y.; Juneja, S.; GSeetharam, T. IoT data visualization for business intelligence in corporate finance. Inf. Process. Manag. 2022, 59, 102736. [Google Scholar] [CrossRef]
- Dhankhar, A.; Juneja, S.; Juneja, A.; Bali, V. Kernel parameter tuning to tweak the performance of classifiers for identification of heart diseases. Int. J. E-Health Med. Commun. (IJEHMC) 2021, 12, 1–16. [Google Scholar] [CrossRef]
- Lin, T.Y.; RoyChowdhury, A.; Maji, S. Bilinear CNN models for fine-grained visual recognition. In Proceedings of the IEEE International Conference on Computer Vision, Santiago, Chile, 7–13 December 2015; pp. 1449–1457. [Google Scholar]
- Acharya, U.R.; Oh, S.L.; Hagiwara, Y.; Tan, J.H.; Adam, M.; Gertych, A.; San Tan, R. A deep convolutional neural network model to classify heartbeats. Comput. Biol. Med. 2017, 89, 389–396. [Google Scholar] [CrossRef] [PubMed]
- Demir, F.; Abdullah, D.A.; Sengur, A. A new deep CNN model for environmental sound classification. IEEE Access 2020, 8, 66529–66537. [Google Scholar] [CrossRef]
- Musallam, A.S.; Sherif, A.S.; Hussein, M.K. A New Convolutional Neural Network Architecture for Automatic Detection of Brain Tumors in Magnetic Resonance Imaging Images. IEEE Access 2022, 10, 2775–2782. [Google Scholar] [CrossRef]
- Woźniak, M.; Siłka, J.; Wieczorek, M. Deep Neural Network Correlation Learning Mechanism for CT Brain Tumor Detection. Neural Comput. Appl. 2021, 1–16. Available online: https://link.springer.com/article/10.1007/s00521-021-05841-x (accessed on 15 November 2022).
- Amin, J.; Sharif, M.; Haldorai, A.; Yasmin, M.; Nayak, R.S. Brain tumor detection and classification using machine learning: A comprehensive survey. Complex Intell. Syst. 2022, 8, 3161–3183. [Google Scholar] [CrossRef]
- Nayak, D.R.; Padhy, N.; Mallick, P.K.; Zymbler, M.; Kumar, S. Brain Tumor Classification Using Dense Efficient-Net. Axioms 2022, 11, 34. [Google Scholar] [CrossRef]
- Obeidavi, M.R.; Maghooli, K. Tumor Detection in Brain MRI using Residual Convolutional Neural Networks. In Proceedings of the 2022 IEEE International Conference on Machine Vision and Image Processing (MVIP), Ahvaz, Iran, 23–24 February 2022; pp. 1–5. [Google Scholar]
- Khalil, H.A.; Darwish, S.; Ibrahim, Y.M.; Hassan, O.F. 3D-MRI brain tumor detection model using modified version of level set segmentation based on dragonfly algorithm. Symmetry 2020, 12, 1256. [Google Scholar] [CrossRef]
- Sajid, S.; Hussain, S.; Sarwar, A. Brain tumor detection and segmentation in MR images using deep learning. Arab. J. Sci. Eng. 2019, 44, 9249–9261. [Google Scholar] [CrossRef]
- Attallah, O.; Sharkas, M.A.; Gadelkarim, H. Deep learning techniques for automatic detection of embryonic neurodevelopmental disorders. Diagnostics 2020, 10, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stadlbauer, A.; Marhold, F.; Oberndorfer, S.; Heinz, G.; Buchfelder, M.; Kinfe, T.M.; Meyer-Bäse, A. Radiophysiomics: Brain Tumors Classification by Machine Learning and Physiological MRI Data. Cancers 2022, 14, 2363. [Google Scholar] [CrossRef] [PubMed]
- Aamir, M.; Rahman, Z.; Dayo, Z.A.; Abro, W.A.; Uddin, M.I.; Khan, I.; Imran, A.S.; Ali, Z.; Ishfaq, M.; Guan, Y.; et al. A deep learning approach for brain tumor classification using MRI images. Comput. Electr. Eng. 2022, 101, 108105. [Google Scholar] [CrossRef]
- Haq, A.u.; Li, J.P.; Khan, S.; Alshara, M.A.; Alotaibi, R.M.; Mawuli, C. DACBT: Deep learning approach for classification of brain tumors using MRI data in IoT healthcare environment. Sci. Rep. 2022, 12, 15331. [Google Scholar] [CrossRef]
- Sayedgomaa. Brain Tumor Kaggle. Available online: https://www.kaggle.com/code/sayedgomaa/brain-tumor/notebook (accessed on 21 December 2022).
- Dwork, C.; Feldman, V.; Hardt, M.; Pitassi, T.; Reingold, O.; Roth, A. The reusable holdout: Preserving validity in adaptive data analysis. Science 2015, 349, 636–638. [Google Scholar] [CrossRef] [Green Version]
- Cao, B.; Pan, S.J.; Zhang, Y.; Yeung, D.Y.; Yang, Q. Adaptive transfer learning. In Proceedings of the AAAI Conference on Artificial Intelligence, Atlanta, GA, USA, 11–15 July 2010; Volume 24, pp. 407–412. [Google Scholar]
- Zhuang, F.; Qi, Z.; Duan, K.; Xi, D.; Zhu, Y.; Zhu, H.; Xiong, H.; He, Q. A comprehensive survey on transfer learning. Proc. IEEE 2020, 109, 43–76. [Google Scholar] [CrossRef]
- Loey, M.; Manogaran, G.; Taha, M.H.N.; Khalifa, N.E.M. A hybrid deep transfer learning model with machine learning methods for face mask detection in the era of the COVID-19 pandemic. Measurement 2021, 167, 108288. [Google Scholar] [CrossRef] [PubMed]
- Peirelinck, T.; Kazmi, H.; Mbuwir, B.V.; Hermans, C.; Spiessens, F.; Suykens, J.; Deconinck, G. Transfer learning in demand response: A review of algorithms for data-efficient modelling and control. Energy 2022, 7, 100126. [Google Scholar] [CrossRef]
- Ahsan, M.; Gomes, R.; Denton, A. Application of a convolutional neural network using transfer learning for tuberculosis detection. In Proceedings of the 2019 IEEE International Conference on Electro Information Technology (EIT), Brookings, SD, USA, 20–22 May 2019; pp. 427–433. [Google Scholar]
- Thenmozhi, K.; Reddy, U.S. Crop pest classification based on deep convolutional neural network and transfer learning. Comput. Electron. Agric. 2019, 164, 104906. [Google Scholar] [CrossRef]
- Heidari, M.; Rafatirad, S. Using transfer learning approach to implement convolutional neural network model to recommend airline tickets by using online reviews. In Proceedings of the 2020 15th IEEE International Workshop on Semantic and Social Media Adaptation and Personalization (SMA), Zakynthos, Greece, 29–30 October 2020; pp. 1–6. [Google Scholar]
- Rahman, T.; Chowdhury, M.E.; Khandakar, A.; Islam, K.R.; Islam, K.F.; Mahbub, Z.B.; Kadir, M.A.; Kashem, S. Transfer learning with deep convolutional neural network (CNN) for pneumonia detection using chest X-ray. Appl. Sci. 2020, 10, 3233. [Google Scholar] [CrossRef]
- Akiba, T.; Suzuki, S.; Fukuda, K. Extremely large minibatch sgd: Training resnet-50 on imagenet in 15 minutes. arXiv 2017, arXiv:1711.04325. [Google Scholar]
- Almourish, M.H.; Saif, A.A.; Radman, B.M.; Saeed, A.Y. COVID-19 diagnosis based on CT images using pre-trained models. In Proceedings of the 2021 IEEE International Conference of Technology, Science and Administration (ICTSA), Taiz, Yemen, 22–24 March 2021; pp. 1–5. [Google Scholar]
- Wu, P.; Tan, Y. Estimation of economic indicators using residual neural network ResNet-50. In Proceedings of the 2019 IEEE International Conference on Data Mining Workshops (ICDMW), Beijing, China, 8–11 November 2019; pp. 206–209. [Google Scholar]
- Theckedath, D.; Sedamkar, R. Detecting affect states using VGG16, ResNet-50 and SE-ResNet-50 networks. Comput. Sci. 2020, 1, 79. [Google Scholar]
- Al-Haija, Q.A.; Manasra, G.F. Development of Breast Cancer Detection Model Using Transfer Learning of Residual Neural Network (ResNet-50). Am. J. Sci. Eng. 2020, 1, 30–39. [Google Scholar] [CrossRef]
- Setiawan, A.W. The Effect of Image Dimension and Exposure Fusion Framework Enhancement in Pneumonia Detection Using Residual Neural Network. In Proceedings of the 2022 IEEE International Seminar on Application for Technology of Information and Communication (iSemantic), Wuhan, China, 4–6 Feburary 2022; pp. 41–45. [Google Scholar]
- Jiang, T.; Zhang, Q.; Yuan, J.; Wang, C.; Li, C. Multi-Type Object Tracking Based on Residual Neural Network Model. Symmetry 2022, 14, 1689. [Google Scholar] [CrossRef]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- da Rocha, D.A.; Ferreira, F.M.F.; Peixoto, Z.M.A. Diabetic retinopathy classification using VGG16 neural network. Res. Biomed. Eng. 2022, 38, 761–772. [Google Scholar] [CrossRef]
- Pravitasari, A.A.; Iriawan, N.; Almuhayar, M.; Azmi, T.; Irhamah, I.; Fithriasari, K.; Purnami, S.W.; Ferriastuti, W. UNet-VGG16 with transfer learning for MRI-based brain tumor segmentation. TELKOMNIKA (Telecommun. Comput. Electron. Control.) 2020, 18, 1310–1318. [Google Scholar] [CrossRef]
- Deng, J.; Dong, W.; Socher, R.; Li, L.J.; Li, K.; Fei-Fei, L. ImageNet: A large-scale hierarchical image database. In Proceedings of the 2009 IEEE Conference on Computer Vision and Pattern Recognition, Miami, FL, USA, 20–25 June 2009; pp. 248–255. [Google Scholar] [CrossRef] [Green Version]
- Wang, H. Garbage recognition and classification system based on convolutional neural network VGG16. In Proceedings of the 2020 3rd IEEE International Conference on Advanced Electronic Materials, Computers and Software Engineering (AEMCSE), Shenzhen, China, 24–26 April 2020; pp. 252–255. [Google Scholar]
- Yan, J.; Wang, Z. YOLO V3+ VGG16-based automatic operations monitoring and analysis in a manufacturing workshop under Industry 4.0. J. Manuf. Syst. 2022, 63, 134–142. [Google Scholar] [CrossRef]
- Liu, M.; Yi, M.; Wu, M.; Wang, J.; He, Y. Breast Pathological Image Classification Based on VGG16 Feature Concatenation. J. Shanghai Jiaotong Univ. (Sci.) 2022, 27, 473–484. [Google Scholar] [CrossRef]
- Nie, H. Face Expression Classification Using Squeeze-Excitation Based VGG16 Network. In Proceedings of the 2022 2nd IEEE International Conference on Consumer Electronics and Computer Engineering (ICCECE), Guangzhou, China, 14–16 January 2022; pp. 482–485. [Google Scholar]
- Jignesh Chowdary, G.; Punn, N.S.; Sonbhadra, S.K.; Agarwal, S. Face mask detection using transfer learning of inceptionv3. In Big Data Analytics, Proceedings of the 8th International Conference, BDA 2020, Sonepat, India, 15–18 December 2020; Proceedings 8; Springer: Berlin/Heidelberg, Germany, 2020; pp. 81–90. [Google Scholar]
- Xia, X.; Xu, C.; Nan, B. Inception-v3 for flower classification. In Proceedings of the 2017 2nd IEEE International Conference on Image, Vision and Computing (ICIVC), Chengdu, China, 2–4 June 2017; pp. 783–787. [Google Scholar]
- Tio, A.E. Face shape classification using inception v3. arXiv 2019, arXiv:1911.07916. [Google Scholar]
- Mujahid, M.; Rustam, F.; Álvarez, R.; Luis Vidal Mazón, J.; Díez, I.d.l.T.; Ashraf, I. Pneumonia Classification from X-ray Images with Inception-V3 and Convolutional Neural Network. Diagnostics 2022, 12, 1280. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Chen, D.; Hao, L.; Liu, X.; Zeng, Y.; Chen, J.; Zhang, G. Pulmonary image classification based on inception-v3 transfer learning model. IEEE Access 2019, 7, 146533–146541. [Google Scholar] [CrossRef]
- Liu, Z.; Yang, C.; Huang, J.; Liu, S.; Zhuo, Y.; Lu, X. Deep learning framework based on integration of S-Mask R-CNN and Inception-v3 for ultrasound image-aided diagnosis of prostate cancer. Future Gener. Comput. Syst. 2021, 114, 358–367. [Google Scholar] [CrossRef]
- Andrew, A.; Santoso, H. Compare VGG19, ResNet-50, Inception-V3 for review food rating. Sink. J. Dan Penelit. Tek. Inform. 2022, 7, 845–494. [Google Scholar]
- Al Husaini, M.A.S.; Habaebi, M.H.; Gunawan, T.S.; Islam, M.R.; Elsheikh, E.A.; Suliman, F. Thermal-based early breast cancer detection using inception V3, inception V4 and modified inception MV4. Neural Comput. Appl. 2022, 34, 333–348. [Google Scholar] [CrossRef]
- Chang, W.J.; Chen, L.B.; Hsu, C.H.; Lin, C.P.; Yang, T.C. A Deep Learning-Based Intelligent Medicine Recognition System for Chronic Patients. IEEE Access 2019, 7, 44441–44458. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Dataset | Models | Performance | Limitations |
|---|---|---|---|---|
| [17], 2022 | 10,000 MR images | Deep educational model (proposed), VGG16, ResNet-50, MobileNet, Inception V3 | Deep educational model: accuracy 98% | Need to apply image augmentation methods |
| [34], 2022 | 3394 MR images | Deep convolutional neural network (DCNN) (proposed), VGG16, VGG19, CNN-SVM | DCNN: accuracy 97.72% | Should consider more datasets and various types of images |
| [35], 2021 | 3064, CT brain scan images | Correlation learning mechanism (CLM) with CNN | CLM model: accuracy 96%, precision and recall 95% | Should consider more datasets to obtain more accurate and promising results |
| [36], 2021 | 2556 brain tumor images | Hybrid ensemble classifier (KNN-RF-DT) (proposed), naive Bayes, random forest, neural network, KNN, and decision tree | Hybrid ensemble classifier (KNN-RF-DT): accuracy 97.305%, precision 97.73%, specificity 97.60%, sensitivity 97.04%, Youden index 94.71%, and F1-score 97.41% | Should consider more datasets to obtain more accurate and promising results |
| [37], 2022 | 3260 MRI brain images | Dense EfficientNet (proposed), ResNet 50, MobileNet, MobileNetV2 | Dense EfficientNet: accuracy 98.78%, F1-score 98% | Higher number of parameters and evaluation time |
| [38], 2022 | BRATS 2015 dataset, 2000 MR images | Residual network | Residual network: accuracy of 97.05% | Lack of performance metrics evaluation |
| [39], 2020 | BRATS 2017, 3D image dataset | Modified two-step dragonfly method (proposed), random forest, SVM, fuzzy C-means | Accuracy: 98.20%, recall: 95.13%, and precision: 93.21% | Data processing and over-fitting |
| [40], 2019 | BRATS 2013 MRI tumor dataset | Hybrid CNN models | Dice score of 86%, sensitivity of 86%, and specificity of 91% | Only one tumor per slice was evaluated |
| [15], 2019 | 227 MR images | KNN classifier (proposed), RF, NB, and RBF | Accuracy of 95.6% and AUC of 99% | Lack of MR images |
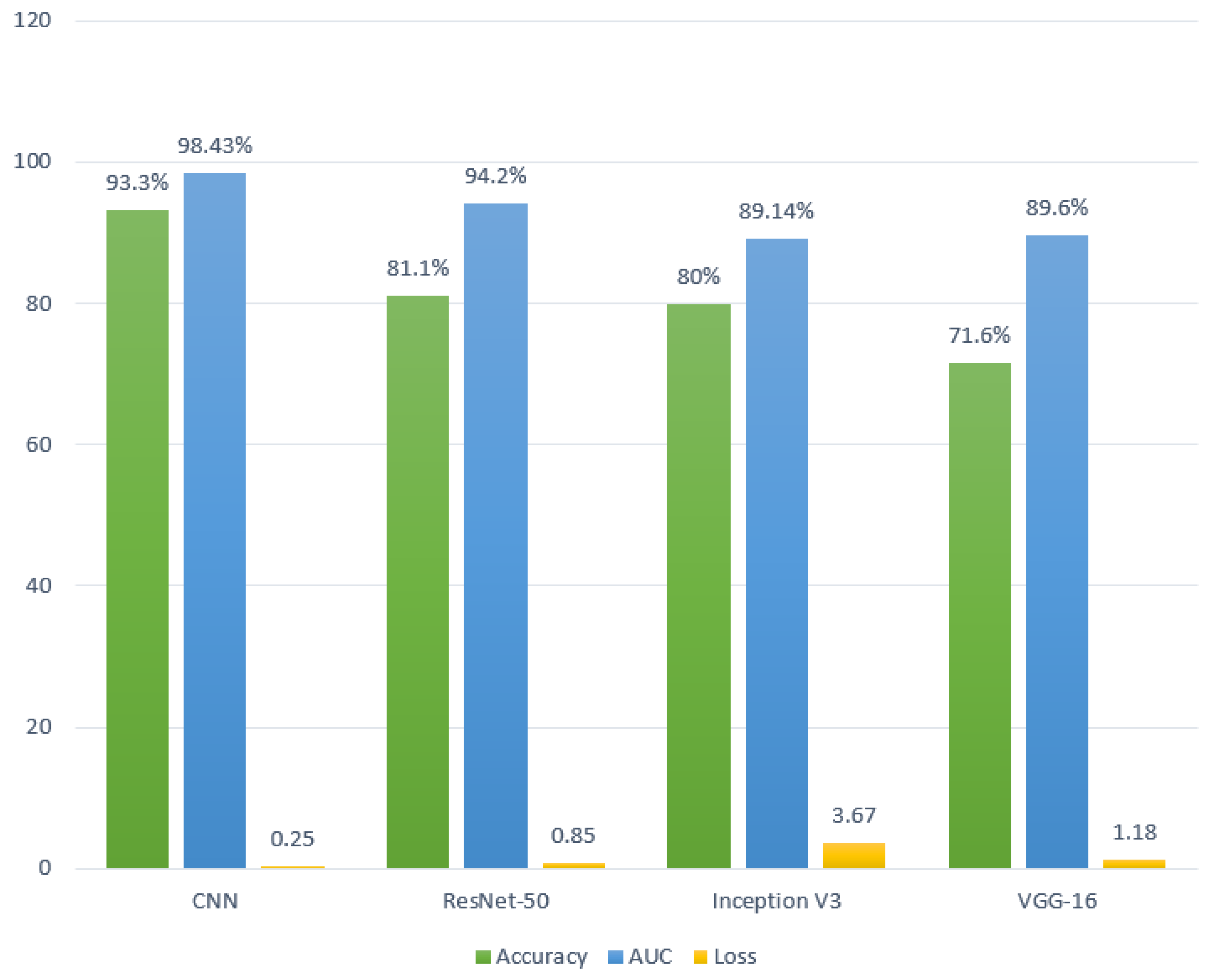
| Our work | 3264 MR images | CNN (proposed), ResNet-50, VGG16, and Inception V3 | Accuracy of 93.30%, AUC of 98.43%, recall of 91.13%, and loss of 0.25 | — |
| Brain Tumor Type | Count |
|---|---|
| Glioma Tumor | 926 |
| Meningioma Tumor | 937 |
| No Tumor | 500 |
| Pituitary Tumor | 901 |
| Total | 3264 |
| Models | Accuracy (%) | AUC (%) | Recall (%) | Loss |
|---|---|---|---|---|
| CNN | 93.30 | 98.43 | 91.13 | 0.25 |
| ResNet-50 | 81.10 | 94.20 | 81.04 | 0.85 |
| VGG16 | 71.60 | 89.60 | 70.03 | 1.18 |
| Inception V3 | 80.00 | 89.14 | 79.81 | 3.67 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahmud, M.I.; Mamun, M.; Abdelgawad, A. A Deep Analysis of Brain Tumor Detection from MR Images Using Deep Learning Networks. Algorithms 2023, 16, 176. https://doi.org/10.3390/a16040176
Mahmud MI, Mamun M, Abdelgawad A. A Deep Analysis of Brain Tumor Detection from MR Images Using Deep Learning Networks. Algorithms. 2023; 16(4):176. https://doi.org/10.3390/a16040176
Chicago/Turabian StyleMahmud, Md Ishtyaq, Muntasir Mamun, and Ahmed Abdelgawad. 2023. "A Deep Analysis of Brain Tumor Detection from MR Images Using Deep Learning Networks" Algorithms 16, no. 4: 176. https://doi.org/10.3390/a16040176