
Adhesion of Different Resin Cements to Zirconia: Effect of Incremental versus Bulk Build Up, Use of Mould and Ageing †


Abstract
:1. Introduction
2. Materials and Methods
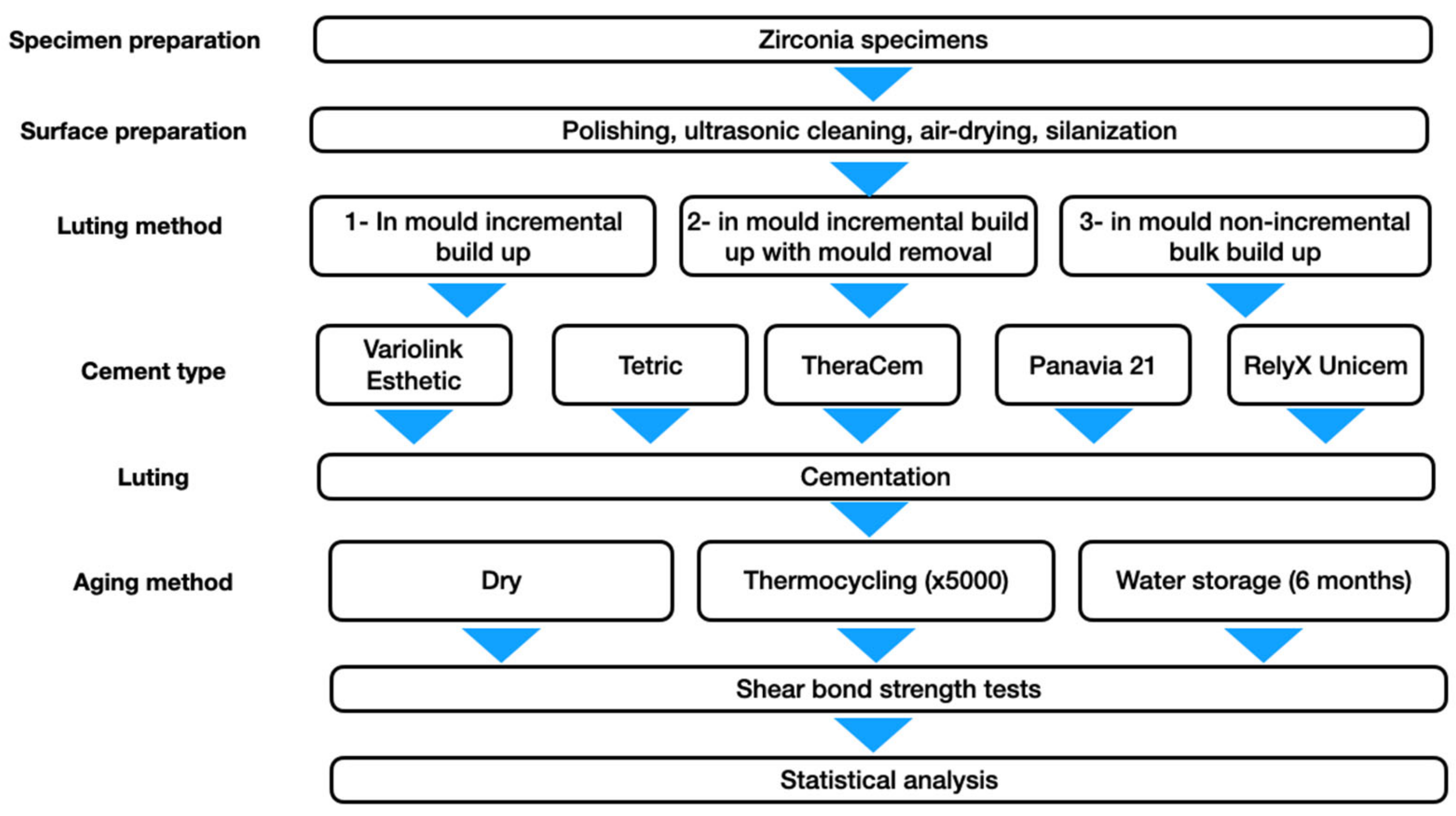
2.1. Specimen Preparation
2.2. Luting Methods
- Protocol 1: in mould incremental build up;
- Protocol 2: in mould incremental build up with subsequent mould removal;
- Protocol 3: in mould non-incremental bulk build up.

2.3. Macroshear Test
2.4. Statistical Analysis
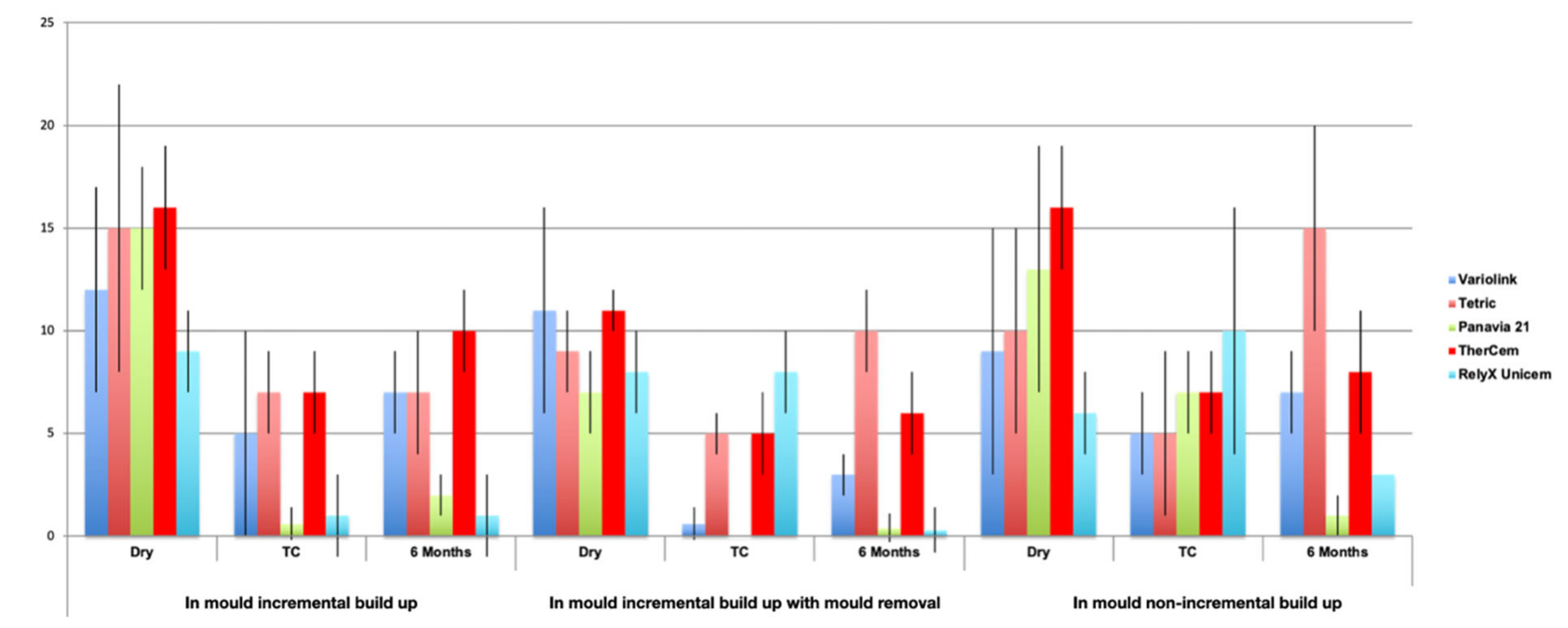
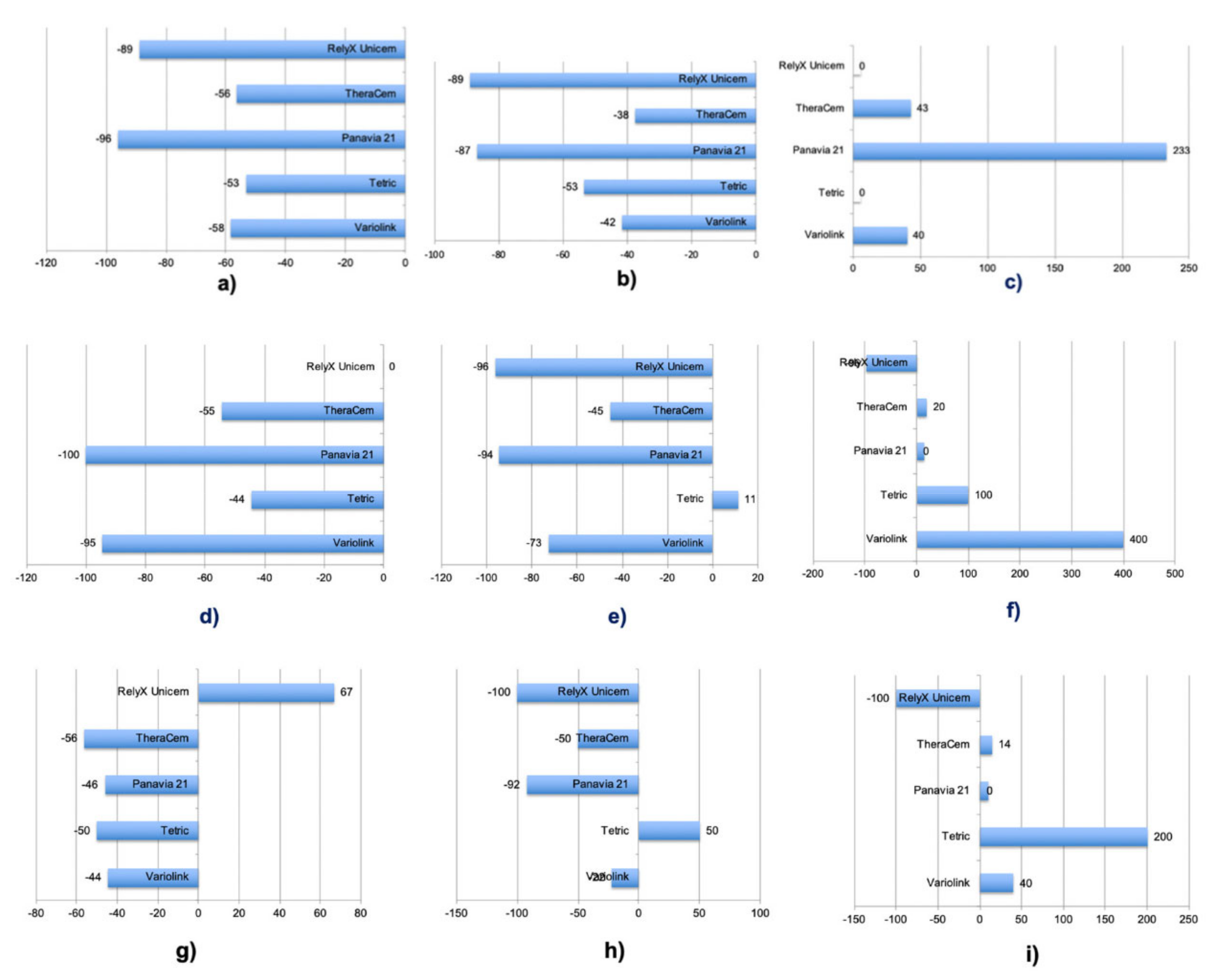
3. Results
4. Discussion
5. Conclusions
- The adhesion of the tested resin cements to zirconia was influenced by the cement type, luting protocol and ageing.
- In dry conditions, the MDP-based cement TheraCem performed the best in all the adhesion protocols.
- After ageing, a reduction in bond strength was observed among most cement types, as a result of hydrolytic degradation. As an exception, Tetric showed an increase in bond strength, possibly due to further polymerization and a higher degree of conversion.
- Considering the higher bond strength values overall, MDP-based cements may adhere to a zirconium surface more reliably by using a universal primer based on MDP and MPS, and this can be suggested as an option for bonding to zirconia without air abrasion.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ichikawa, Y.; Akagawa, Y.; Nikai, H.; Tsuru, H. Tissue compatibility and stability of a new zirconia ceramic in vivo. J. Prosthet. Dent. 1992, 68, 322–326. [Google Scholar] [CrossRef]
- Guazzato, M.; Albakry, M.; Ringer, S.; Swain, M. Strength, fracture toughness and microstructure of a selection of all-ceramic materials. Part II. Zirconia-based dental ceramics. Dent. Mater. 2004, 20, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Sailer, I.; Fehér, A.; Filser, F.; Gauckler, L.J.; Lüthy, H.; Hämmerle, C.H.F. Five-year clinical results of zirconia frameworks for posterior fixed partial dentures. Int. J. Prosthodont. 2007, 20, 383–388. [Google Scholar] [PubMed]
- Beuer, F.; Schweiger, J.; Edelhoff, D. Digital dentistry: An overview of recent developments for CAD/CAM generated restorations. Br. Dent. J. 2008, 204, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Denry, I.; Kelly, J. Emerging Ceramic-based Materials for Dentistry. J. Dent. Res. 2014, 93, 1235–1242. [Google Scholar] [CrossRef] [Green Version]
- Albert, F.E.; El-Mowafy, O.M. Marginal adaptation and microleakage of Procera AllCeram crowns with four cements. Int. J. Prosthodont. 2004, 17, 529–535. [Google Scholar] [CrossRef]
- Inokoshi, M.; De Munck, J.; Minakuchi, S.; Van Meerbeek, B. Meta-analysis of Bonding Effectiveness to Zirconia Ceramics. J. Dent. Res. 2014, 93, 329–334. [Google Scholar] [CrossRef]
- Özcan, M.; Bernasconi, M. Adhesion to zirconia used for dental restorations: A systematic review and meta-analysis. J. Adhes. Dent. 2015, 17, 7–26. [Google Scholar] [CrossRef]
- Thompson, J.Y.; Stoner, B.R.; Piascik, J.R.; Smith, R. Adhesion/cementation to zirconia and other non-silicate ceramics: Where are we now? Dent. Mater. 2011, 27, 71–82. [Google Scholar] [CrossRef] [Green Version]
- Aida, M.; Hayakawa, T.; Mizukawa, K. Adhesion of composite to porcelain with various surface conditions. J. Prosthet. Dent. 1995, 73, 464–470. [Google Scholar] [CrossRef]
- Özcan, M.; Vallittu, P.K. Effect of surface conditioning methods on the bond strength of luting cement to ceramics. Dent. Mater. 2003, 19, 725–731. [Google Scholar] [CrossRef] [Green Version]
- Della Bona, A.; Donassollo, T.A.; Demarco, F.F.; Barrett, A.A.; Mecholsky, J.J. Characterization and surface treatment effects on topography of a glass-infiltrated alumina/zirconia-reinforced ceramic. Dent. Mater. 2007, 23, 769–775. [Google Scholar] [CrossRef] [PubMed]
- Pozzobon, J.L.; Pereira, G.K.R.; Wandscher, V.F.; Dorneles, L.S.; Valandro, L.F. Mechanical behavior of yttria-stabilized tetragonal zirconia polycrystalline ceramic after different zirconia surface treatments. Mater. Sci. Eng. C 2017, 77, 828–835. [Google Scholar] [CrossRef] [PubMed]
- Matinlinna, J.P.; Heikkinen, T.; Ozcan, M.; Lassila, L.V.J.; Vallittu, P.K. Evaluation of resin adhesion to zirconia ceramic using some organosilanes. Dent. Mater. 2006, 22, 824–831. [Google Scholar] [CrossRef] [PubMed]
- Marsden, J.G. Organofunctional Silane Coupling Agents. In Handbook of Adhesives; Springer: Berlin/Heidelberg, Germany, 1990; pp. 536–548. [Google Scholar]
- Özcan, M. The use of chairside silica coating for different dental applications: A clinical report. J. Prosthet. Dent. 2002, 87, 469–472. [Google Scholar] [CrossRef] [PubMed]
- Paschoalino, V.M.; Paschoalino, B.J.; Özcan, M.; de Carvalho, R.L.A.; De Carvalho, R.F.; Husain, N.A.-H.; Leite, F.P.P. Effect of different air-abrasion protocols on topography, surface wettability and adhesion of MDP monomer-based resin cement to zirconia. J. Adhes. Sci. Technol. 2019, 33, 1948–1958. [Google Scholar] [CrossRef]
- Yildirim, B.; Kümbüloğlu, Ö.; Saraçoğlu, A.; Al-Haj Husain, N.; Özcan, M. An investigation of atomic force microscopy, surface topography and adhesion of luting cements to zirconia: Effect of silica coating, zirconia primer and laser. J. Adhes. Sci. Technol. 2019, 33, 2047–2060. [Google Scholar] [CrossRef]
- Pereira, G.; Fraga, S.; Montagner, A.; Soares, F.; Kleverlaan, C.; Valandro, L. The effect of grinding on the mechanical behavior of Y-TZP ceramics: A systematic review and meta-analyses. J. Mech. Behav. Biomed. Mater. 2016, 63, 417–442. [Google Scholar] [CrossRef]
- Curtis, A.R.; Wright, A.J.; Fleming, G.J.P. The influence of surface modification techniques on the performance of a Y-TZP dental ceramic. J. Dent. 2006, 34, 195–206. [Google Scholar] [CrossRef]
- Guazzato, M.; Quach, L.; Albakry, M.; Swain, M. Influence of surface and heat treatments on the flexural strength of Y-TZP dental ceramic. J. Dent. 2005, 33, 9–18. [Google Scholar] [CrossRef]
- Kosmač, T.; Oblak, C.; Jevnikar, P.; Funduk, N.; Marion, L. The effect of surface grinding and sandblasting on flexural strength and reliability of Y-TZP zirconia ceramic. Dent. Mater. 1999, 15, 426–433. [Google Scholar] [CrossRef]
- Kosmač, T.; Oblak, Č.; Marion, L. The effects of dental grinding and sandblasting on ageing and fatigue behavior of dental zirconia (Y-TZP) ceramics. J. Eur. Ceramic Soc. 2008, 28, 1085–1090. [Google Scholar] [CrossRef]
- Özcan, M.; Melo, R.; Souza, R.; Machado, J.P.; Valandro, L.F.; Botttino, M.A. Effect of air-particle abrasion protocols on the biaxial flexural strength, surface characteristics and phase transformation of zirconia after cyclic loading. J. Mech. Behav. Biomed. Mater. 2013, 20, 19–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Passos, S.P.; Linke, B.; Major, P.W.; Nychka, J.A. The effect of air-abrasion and heat treatment on the fracture behavior of Y-TZP. Dent. Mater. 2015, 31, 1011–1021. [Google Scholar] [CrossRef]
- Jevnikar, P.; Krnel, K.; Kocjan, A.; Funduk, N.; Kosmač, T. The effect of nano-structured alumina coating on resin-bond strength to zirconia ceramics. Dent. Mater. 2010, 26, 688–696. [Google Scholar] [CrossRef]
- Magne, P.; Paranhos, M.P.; Burnett, L.H., Jr. New zirconia primer improves bond strength of resin-based cements. Dent. Mater. 2010, 26, 345–352. [Google Scholar] [CrossRef]
- Pilo, R.; Kaitsas, V.; Zinelis, S.; Eliades, G. Interaction of zirconia primers with yttria-stabilized zirconia surfaces. Dent. Mater. 2016, 32, 353–362. [Google Scholar] [CrossRef] [PubMed]
- Standards IOf. ISO 6872: 2008; Dentistry: Ceramic Materials. International Organization for Standards: Geneva, Switzerland, 2008.
- Standards IOf. ISO 11405: 2015; Dentistry—Testing of Adhesion to Tooth Structure. ICS: Geneva, Switzerland, 2015.
- Della Bona, A.; Van Noort, R. Shear vs. Tensile Bond Strength of Resin Composite Bonded to Ceramic. J. Dent. Res. 1995, 74, 1591–1596. [Google Scholar] [CrossRef]
- Valandro, L.F.; Özcan, M.; Amaral, R.; Vanderlei, A.; Bottino, M.A. Effect of testing methods on the bond strength of resin to zirconia-alumina ceramic: Microtensile versus shear test. Dent. Mater. J. 2008, 27, 849–855. [Google Scholar] [CrossRef] [Green Version]
- DeHoff, P.H.; Anusavice, K.J.; Wang, Z. Three-dimensional finite element analysis of the shear bond test. Dent. Mater. 1995, 11, 126–131. [Google Scholar] [CrossRef]
- Betamar, N.; Cardew, G.; Van Noort, R. Influence of Specimen Designs on the Microtensile Bond Strength to Dentin. Doctoral Dissertation, University of Sheffield, Department of Adult Dental Care, Sheffield, UK, 2007. [Google Scholar]
- ISO 10477; Dentistry-Polymer-Based Crown and Bridge Materials. International organization for Standardization: Geneva, Switzerland, 1996.
- Yoshida, K.; Yamashita, M.; Atsuta, M. Zirconate coupling agent for bonding resin luting cement to pure zirconium. Am. J. Dent. 2004, 17, 249–252. [Google Scholar] [PubMed]
- Yoshida, K.; Tsuo, Y.; Atsuta, M. Bonding of dual-cured resin cement to zirconia ceramic using phosphate acid ester monomer and zirconate coupler. J. Biomed. Mater. Res. Part B Appl. Biomater. 2006, 77, 28–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, L.; Suh, B.I.; Brown, D.; Chen, X. Bonding of primed zirconia ceramics: Evidence of chemical bonding and improved bond strengths. Am. J. Dent. 2012, 25, 103–108. [Google Scholar] [PubMed]
- Inokoshi, M.; Vanmeensel, K.; Zhang, F.; De Munck, J.; Eliades, G.; Minakuchi, S.; Naert, I.; Van Meerbeek, B.; Vleugels, J. Aging resistance of surface-treated dental zirconia. Dent. Mater. 2015, 31, 182–194. [Google Scholar] [CrossRef] [PubMed]
- de Oyagüe, R.C.; Monticelli, F.; Toledano, M.; Osorio, E.; Ferrari, M.; Osorio, R. Influence of surface treatments and resin cement selection on bonding to densely-sintered zirconium-oxide ceramic. Dent. Mater. 2009, 25, 172–179. [Google Scholar] [CrossRef] [PubMed]
- Miller, J.D.; Hoh, K.-P.; Ishida, H. Studies of the simulation of silane coupling agent structures on particulate fillers; the pH effect. Polym. Compos. 1984, 5, 18–28. [Google Scholar] [CrossRef]
- Park, J.; Chang, J.; Ferracane, J.; Lee, I.B. How should composite be layered to reduce shrinkage stress: Incremental or bulk filling? Dent. Mater. 2008, 24, 1501–1505. [Google Scholar] [CrossRef] [PubMed]
- Gale, M.; Darvell, B. Thermal cycling procedures for laboratory testing of dental restorations. J. Dent. 1999, 27, 89–99. [Google Scholar] [CrossRef]
- Valandro, L.F.; Özcan, M.; Amaral, R.; Leite, F.P.P.; Bottino, M.A. Microtensile Bond Strength of a Resin Cement to Silica-Coated and Silanized In-Ceram Zirconia Before and After Aging. Int. J. Proshtodont. 2007, 20, 70–72. [Google Scholar]
- Qeblawi, D.M.; Muñoz, C.A.; Brewer, J.D.; Monaco, E.A., Jr. Theeffectof zirconia surface treatment on flexural strength and shear bond strength to a resin cement. J. Prosthet. Dent. 2010, 103, 210–220. [Google Scholar] [CrossRef]
- Kern, M.; Wegner, S.M. Bonding to zirconia ceramic: Adhesion methods and their durability. Dent. Mater. 1998, 14, 64–71. [Google Scholar] [CrossRef]
- Tanaka, R.; Fujishima, A.; Shibata, Y.; Manabe, A.; Miyazaki, T. Cooperation of Phosphate Monomer and Silica Modification on Zirconia. J. Dent. Res. 2008, 87, 666–670. [Google Scholar] [CrossRef] [PubMed]
- Özcan, M.; Kumbuloglu, O. Effect of composition, viscosity and thickness of the opaquer on the adhesion of resin composite to titanium. Dent. Mater. 2009, 25, 1248–1255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edelhoff, D.; Özcan, M. To what extent does the longevity of fixed dental prostheses depend on the function of the cement? Working Group 4 materials: Cementation. Clin. Oral Implant. Res. 2007, 18, 193–204. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material | Chemical Composition | Manufacturer |
|---|---|---|
| Monobond Plus | Alcohol solution of silane methacrylate, phosphoric acid methacrylate and sulphide methacrylate | Ivoclar Vivadent, Schaan, Liechtenstein |
| Oxyguard II | Glycerol 50–70 wt.%, polyethylene glycol, catalysts, accelerators, dyes | Kuraray, Osaka, Japan |
| RelyX Unicem (REL) | Phosphoric acid methacrylates, dimethacrylates, silanated fillers, inorganic fillers (72 wt.%), initiators, stabilizers, rheologic additives | 3M ESPE, St. Paul, MN, USA |
| Tetric (TET) | F3Yb, Bis-GMA, urethandimethacrylate, triethylenglycoldimetharcylate | Ivoclar Vivadent, Schaan, Lichtenstein |
| TheraCem (THC) | Paste A: Portland Cement, Yb with barium glass, F3Yb, BisGMA Paste B: MDP, HEMA, tert-butyl perbenzoate | BISCO Inc., Schaumburg, IL, USA |
| Panavia 21 (PAN) | Paste A: BPEDMA, MDP, DMA, silanated silica filler silanated colloidal silica Paste B: DMA, pigments, accelerators | Kuraray, Osaka, Japan |
| Variolink esthetic (VAR) | Monomer matrix: UDMA, methacrylates Inorganic filler: YbF3, spheroid mixed oxide, inorganic Fillers (38 wt.%: particle size: 0.04–0.2 mm, mean: 0.1 mm) | Ivoclar Vivadent, Schaan, Lichtenstein |
| Protocol 1 | P1-PAN | P1-THC | P1-VAR | P1-TET | P1-REL | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| P1-PAN | 0.000 | 0.005 | 0.000 | n.s. | ||||||
| P1-THC | 0.000 | 0.000 | n.s. | 0.000 | ||||||
| P1-VAR | 0.005 | 0.000 | 0.001 | 0.000 | ||||||
| P1-TET | 0.000 | n.s. | 0.001 | 0.000 | ||||||
| P1-REL | n.s. | 0.000 | 0.000 | 0.000 | ||||||
| Protocol 2 | P2-PAN | P2-THC | P2-VAR | P2-TET | P2-REL | |||||
| P2-PAN | 0.000 | 0.000 | 0.000 | n.s. | ||||||
| P2-THC | 0.000 | 0.001 | n.s. | 0.000 | ||||||
| P2-VAR | 0.005 | 0.001 | 0.000 | n.s. | ||||||
| P2-TET | 0.000 | n.s. | 0.000 | 0.000 | ||||||
| P2-REL | n.s. | 0.000 | n.s. | 0.000 | ||||||
| Protocol 3 | P3-PAN | P3-THC | P3-VAR | P3-TET | P3-REL | |||||
| P3-PAN | 0.000 | n.s. | 0.000 | n.s. | ||||||
| P3-THC | 0.000 | 0.000 | n.s. | 0.000 | ||||||
| P3-VAR | n.s. | 0.000 | 0.000 | n.s. | ||||||
| P3-TET | 0.000 | n.s. | 0.000 | 0.000 | ||||||
| P2-REL | n.s. | 0.000 | n.s. | 0.000 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Müller, N.; Al-Haj Husain, N.; Chen, L.; Özcan, M. Adhesion of Different Resin Cements to Zirconia: Effect of Incremental versus Bulk Build Up, Use of Mould and Ageing. Materials 2022, 15, 2186. https://doi.org/10.3390/ma15062186
Müller N, Al-Haj Husain N, Chen L, Özcan M. Adhesion of Different Resin Cements to Zirconia: Effect of Incremental versus Bulk Build Up, Use of Mould and Ageing. Materials. 2022; 15(6):2186. https://doi.org/10.3390/ma15062186
Chicago/Turabian StyleMüller, Nicolas, Nadin Al-Haj Husain, Liang Chen, and Mutlu Özcan. 2022. "Adhesion of Different Resin Cements to Zirconia: Effect of Incremental versus Bulk Build Up, Use of Mould and Ageing" Materials 15, no. 6: 2186. https://doi.org/10.3390/ma15062186