
Toxicological Risks of the Cobalt–Chromium Alloys in Dentistry: A Systematic Review

 , ,
, , 
Abstract
:1. Introduction
2. Methods
2.1. Data Sources and Search Strategy
2.2. Study Selection
2.3. Inclusion and Exclusion Criteria
2.4. Data Extraction and Study Quality Assessment
3. Results
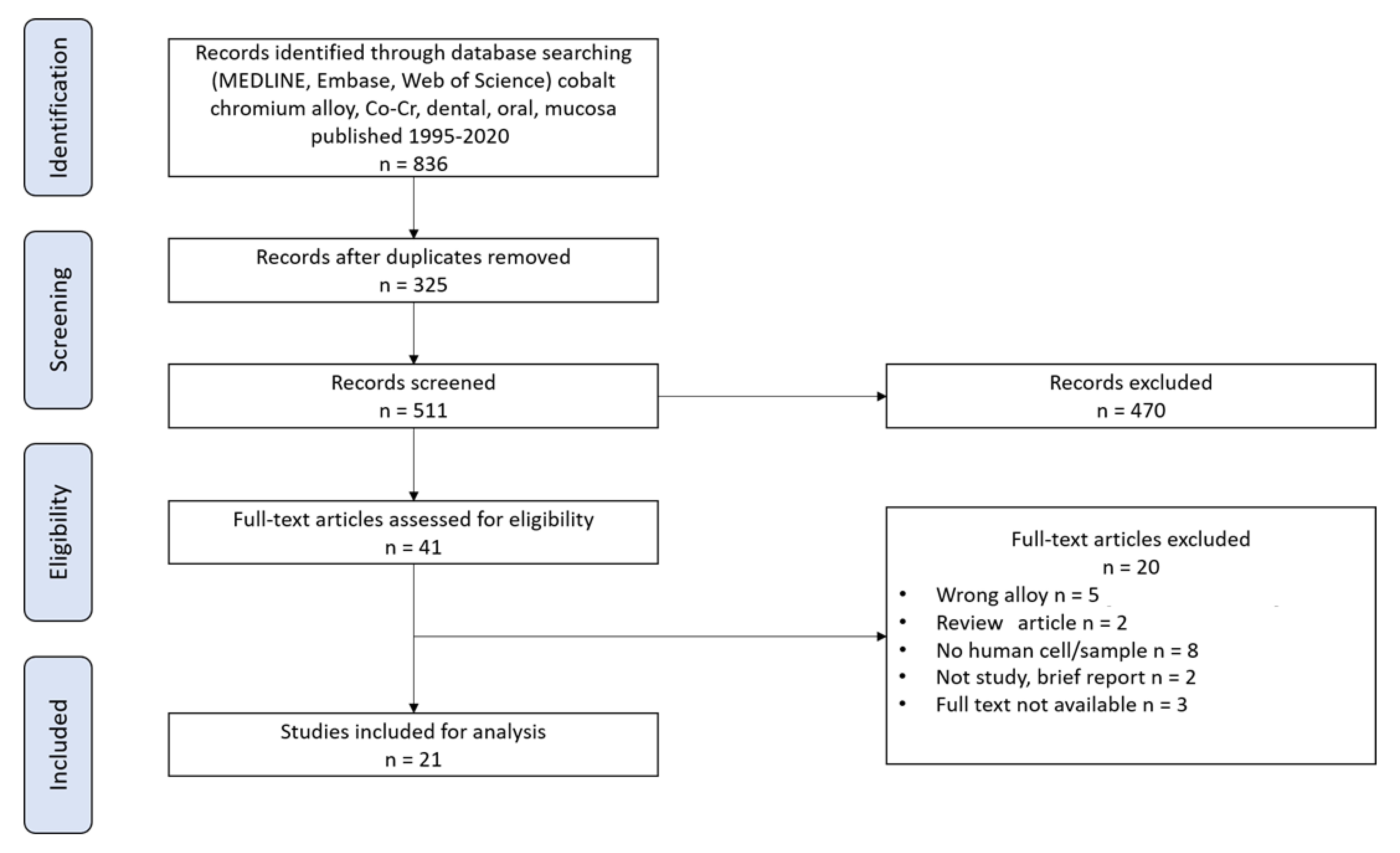
3.1. Study Selection
3.2. Cytotoxicity of Co-Cr Alloys Based on In Vitro Studies
3.3. Cytotoxicity of Co-Cr Alloys Based on in Vivo Studies
3.4. Sensitization and Irritation to Co-Cr Alloys
3.5. Type IV Hypersensitivity Reaction to Co-Cr Alloys
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kassapidou, M.; Stenport, V.F.; Hjalmarsson, L.; Johansson, C.B. Cobalt-chromium alloys in fixed prosthodontics in Sweden. Acta Biomater. Odontol. Scand. 2017, 3, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Al-Imam, H.; Benetti, A.R.; Øzhayat, E.B.; Pedersen, A.M.L.; Johansen, J.D.; Thyssen, J.P.; Jellesen, M.S.; Gotfredsen, K. Cobalt release and complications resulting from the use of dental prostheses. Contact Dermat. 2016, 75, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Han, X.; Sawada, T.; Schille, C.; Schweizer, E.; Scheideler, L.; Geis-Gerstorfer, J.; Rupp, F.; Spintzyk, S. Comparative Analysis of Mechanical Properties and Metal-Ceramic Bond Strength of Co-Cr Dental Alloy Fabricated by Different Manufacturing Processes. Materials 2018, 11, 1801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaicelyte, A.; Janssen, C.; Le Borgne, M.; Grosgogeat, B. Cobalt–Chromium Dental Alloys: Metal Exposures, Toxicological Risks, CMR Classification, and EU Regulatory Framework. Crystals 2020, 10, 1151. [Google Scholar] [CrossRef]
- Kim, T.-W.; Kim, W.-I.; Mun, J.-H.; Song, M.; Kim, H.-S.; Kim, B.-S.; Kim, M.-B.; Ko, H.-C. Patch Testing with Dental Screening Series in Oral Disease. Ann. Dermatol. 2015, 27, 389–393. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Babineau, J. Product Review: Covidence (Systematic Review Software). J. Can. Heal. Libr. Assoc. 2014, 35, 68–71. [Google Scholar] [CrossRef]
- Ryan, R.; Hill, S. How to GRADE the Quality of the Evidence. Cochrane Consumers and Communication Group. Version 3.0. December 2016. December 2016. Available online: http://cccrg.cochrane.org/author-resources (accessed on 6 December 2021).
- Fonseca, J.; Troconis, C.; Palmier, N.; Gomes-Silva, W.; Paglioni, M.-D.; Araújo, A.; Arboleda, L.; Filho, A.; González-Arriagada, W.; Goes, M.; et al. The impact of head and neck radiotherapy on the dentine-enamel junction: A systematic review. Med. Oral Patol. Oral Cir. Bucal. 2020, 25, e96–e105. [Google Scholar] [CrossRef]
- Pavan, L.M.C.; Rêgo, D.F.; Elias, S.; Canto, G.D.L.; Guerra, E.N.S. In Vitro Anti-Tumor Effects of Statins on Head and Neck Squamous Cell Carcinoma: A Systematic Review. PLoS ONE 2015, 10, e0130476. [Google Scholar] [CrossRef] [Green Version]
- Lin, H.L.; Wang, Y.Y.; Lu, Y. Different removable partial dentures in repair of dentition defects: A biocompatibility analysis. Chin. J. Tissue Eng. Res. 2016, 20, 1171–1176. [Google Scholar] [CrossRef]
- Hamano, H.; Uoshima, K.; Miao, W.-P.; Masuda, T.; Matsumura, M.; Hani, H.; Kitazaki, H.; Inoue, M. Investigation of metal allergy to constituent elements of intraoral restoration materials. J. Stomatol. Soc. 1998, 65, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Fujii, H. Metal elements from intraoral metal restorations. Shanghai J. Stomatol. 2004, 13, 189–192. [Google Scholar]
- Ren, L.; Memarzadeh, K.; Zhang, S.; Sun, Z.; Yang, C.; Ren, G.; Allaker, R.P.; Yang, K. A novel coping metal material CoCrCu alloy fabricated by selective laser melting with antimicrobial and antibiofilm properties. Mater. Sci. Eng. C 2016, 67, 461–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puskar, T.; Jevremovic, D.; Williams, R.J.; Eggbeer, D.; Vukelic, D.; Budak, I. A Comparative Analysis of the Corrosive Effect of Artificial Saliva of Variable pH on DMLS and Cast Co-Cr-Mo Dental Alloy. Materials 2014, 7, 6486–6501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, Y.; Jiang, L.; Lin, H.; Cheng, H. Cell death affected by dental alloys: Modes and mechanisms. Dent. Mater. J. 2017, 36, 82–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okazaki, Y.; Gotoh, E. Comparison of metal release from various metallic biomaterials In Vitro. Biomaterials 2005, 26, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Martín-Cameán, A.; Jos, A.; Calleja, A.; Gil, F.; Iglesias-Linares, A.; Solano, E. Development and validation of an inductively coupled plasma mass spectrometry (ICP-MS) method for the determination of cobalt, chromium, copper and nickel in oral mucosa cells. Microchem. J. 2014, 114, 73–79. [Google Scholar] [CrossRef]
- Machado, M.I.P.; Gomes, A.M.; Rodrigues, M.F.; Pinto, T.S.; Fernandes, C.J.D.C.; Bezerra, F.J.; Zambuzzi, W.F. Cobalt-chromium-enriched medium ameliorates shear-stressed endothelial cell performance. J. Trace Elem. Med. Biol. 2019, 54, 163–171. [Google Scholar] [CrossRef]
- Lucchetti, M.C.; Fratto, G.; Valeriani, F.; De Vittori, E.; Giampaoli, S.; Papetti, P.; Spica, V.R.; Manzon, L. Cobalt-chromium alloys in dentistry: An evaluation of metal ion release. J. Prosthet. Dent. 2015, 114, 602–608. [Google Scholar] [CrossRef]
- Leinfelder, K.F. An Evaluation of Casting Alloys Used for Restorative Procedures. J. Am. Dent. Assoc. 1997, 128, 37–45. [Google Scholar] [CrossRef]
- Kusy, R.P. Types of corrosion in removable appliances: Annotated cases and preventative measures. Clin. Orthod. Res. 2000, 3, 230–239. [Google Scholar] [CrossRef] [PubMed]
- Kusy, R.P. Clinical response to allergies in patients. Am. J. Orthod. Dentofac. Orthop. 2004, 125, 544–547. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.R.; Kim, Y.K.; Son, J.S.; Min, B.K.; Kim, K.-H.; Kwon, T.-Y. Comparison of in vitro biocompatibility of a Co–Cr dental alloy produced by new milling/post-sintering or traditional casting technique. Mater. Lett. 2016, 178, 300–303. [Google Scholar] [CrossRef]
- Kettelarij, J.A.B.; Lidén, C.; Axén, E.; Julander, A. Cobalt, nickel and chromium release from dental tools and alloys: Metal release from dental items. Contact Dermat. 2014, 70, 3–10. [Google Scholar] [CrossRef]
- Jevremovic, D.; Kojic, V.; Bogdanovic, G.; Puskar, T.; Eggbeer, D.; Thomas, D.; Williams, R. A selective laser melted Co-Cr alloy used for the rapid manufacture of removable partial denture frameworks: Initial screening of biocompatibility. J. Serbian Chem. Soc. 2011, 76, 43–52. [Google Scholar] [CrossRef]
- Hryniewicz, T.; Rokicki, R.; Rokosz, K. Co–Cr alloy corrosion behaviour after electropolishing and “magnetoelectropolishing” treatments. Mater. Lett. 2008, 62, 3073–3076. [Google Scholar] [CrossRef]
- Chang, H.; Tomoda, S.; Silwood, C.J.; Lynch, E.; Grootveld, M. 1H NMR investigations of the molecular nature of cobalt(II) ions in human saliva. Arch. Biochem. Biophys. 2012, 520, 51–65. [Google Scholar] [CrossRef]
- Angelieri, F.; Carlin, V.; Martins, R.A.; Ribeiro, D.A. Biomonitoring of mutagenicity and cytotoxicity in patients undergoing fixed orthodontic therapy. Am. J. Orthod. Dentofac. Orthop. 2011, 139, e399–e404. [Google Scholar] [CrossRef]
- Alnazzawi, A.A. Oral diseases associated with fixed prosthodontic restorations. Saudi Med. J. 2017, 38, 322–324. [Google Scholar] [CrossRef]
- Könönen, M.; Rintanen, J.; Waltimo, A.; Kempainen, P. Titanium framework removable partial denture used for patient allergic to other metals: A clinical report and literature review. J. Prosthet. Dent. 1995, 73, 4–7. [Google Scholar] [CrossRef]
- Selden, A.I.; Persson, B.; I Bornberger-Dankvardt, S.; Winstrom, L.E.; Bodin, L.S. Exposure to cobalt chromium dust and lung disorders in dental technicians. Thorax 1995, 50, 769–772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seldén, A.; Sahle, W.; Johansson, L.; Sörenson, S.; Persson, B. Three Cases of Dental Technician’s Pneumoconiosis Related to Cobalt-Chromium-Molybdenum Dust Exposure. Chest 1996, 109, 837–842. [Google Scholar] [CrossRef] [PubMed]
- Katsoulis, J.; Fischer, J.; Huber, S.; Balmer, S.; Mericske-Stern, R. Titanlegierung vs. CoCr-Legierung in der Teilprothetik: Eine klinische Studie. Schweiz. Monatsschr. Zahnmed. 2008, 118, 1040–1046. [Google Scholar] [CrossRef] [PubMed]
- Song, H.; Yin, W.; Ma, Q. Allergic palmoplantar pustulosis caused by cobalt in cast dental crowns: A case report, Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2011, 111, E8–E10. [Google Scholar] [CrossRef]
- Imirzalioglu, P.; Alaaddinoglu, E.; Yilmaz, Z.; Oduncuoglu, B.; Yilmaz, B.; Rosenstiel, S. Influence of recasting different types of dental alloys on gingival fibroblast cytotoxicity. J. Prosthet. Dent. 2012, 107, 24–33. [Google Scholar] [CrossRef]
- Baričević, M.; Ratkaj, I.; Mladinić, M.; Želježić, D.; Kraljević, S.P.; Lončar, B.; Mravak-Stipetić, M. In Vivo assessment of DNA damage induced in oral mucosa cells by fixed and removable metal prosthodontic appliances. Clin. Oral Investig. 2012, 16, 325–331. [Google Scholar] [CrossRef]
- Łukomska-Szymańska, M.; Brzeziński, P.M.; Zielinśki, A.; Sokołowski, J. Cytological response of palatal epithelium to TiN-coated CoCr alloy denture. Folia Histochem. Cytobiol. 2012, 50, 104–110. [Google Scholar] [CrossRef] [Green Version]
- McGinley, E.; Moran, G.; Fleming, G. Base-metal dental casting alloy biocompatibility assessment using a human-derived three-dimensional oral mucosal model. Acta Biomater. 2012, 8, 432–438. [Google Scholar] [CrossRef]
- McGinley, E.L.; Moran, G.P.; Fleming, G.J. Biocompatibility effects of indirect exposure of base-metal dental casting alloys to a human-derived three-dimensional oral mucosal model. J. Dent. 2013, 41, 1091–1100. [Google Scholar] [CrossRef]
- Rusu, L.C.; Borţun, C.M.; Tănăsie, G.; Podariu, A.C.; Baderca, F.; Solovan, C.; Ardelean, L. The cytotoxicity of dental alloys studied on cell culture. Rom. J. Morphol. Embryol. 2014, 55, 111–115. [Google Scholar]
- Forster, A.; Ungvári, K.; Györgyey, Á.; Kukovecz, Á.; Turzó, K.; Nagy, K. Human epithelial tissue culture study on restorative materials. J. Dent. 2014, 42, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Martín-Cameán, A.; Jos, A.; Puerto, M.; Calleja, A.; Iglesias-Linares, A.; Solano, E.; Cameán, A.M. In Vivo determination of aluminum, cobalt, chromium, copper, nickel, titanium and vanadium in oral mucosa cells from orthodontic patients with mini-implants by Inductively coupled plasma-mass spectrometry (ICP-MS). J. Trace Elements Med. Biol. 2015, 32, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Puskar, T.; Lapcevic, A.; Jevremovic, D.; Arandjelovic, S.; Radulovic, S.; Budak, I.; Vukelic, D. Comparative study of cytotoxicity of direct metal laser sintered and cast Co-Cr-Mo dental alloy. Metalurgija 2015, 54, 481–484. [Google Scholar]
- Comăneanu, R.M.; Hancu, V.; Barbu, H.M.; Coman, C.; Cotrut, M.C.; Tarcolea, M.; Holicov, A.M.; Ormenisan, A. Comparative assessment of biocompatibility of NiCr and CoCr alloys used in metal-fused-to-ceramic technology. Rev. Chim. 2015, 66, 312–315. [Google Scholar]
- Gălăţeanu, B.; Golgovici, F.; Hudita, A.; Stan, M.; Dinescu, S.; Costache, M.; Demetrescu, I.; Popescu, A. About electrochemical stability and biocompatibility of two types of CoCr commercial dental alloys. Mater. Corros. 2016, 67, 1096–1104. [Google Scholar] [CrossRef]
- Yu, S.-J.; Shan, W.-L.; Liu, Y.-X.; Huang, X.-Y.; Zhu, G.-X. Effects of Four Different Crown Materials on the Peri-Implant Clinical Parameters and Composition of Peri-Implant Crevicular Fluid. J. Oral Implant. 2017, 43, 337–344. [Google Scholar] [CrossRef]
- Ganbold, B.; Heo, S.-J.; Koak, J.-Y.; Kim, S.-K.; Cho, J. Human Stem Cell Responses and Surface Characteristics of 3D Printing Co-Cr Dental Material. Materials 2019, 12, 3419. [Google Scholar] [CrossRef] [Green Version]
- Kettelarij, J.; Nilsson, S.; Midander, K.; Lidén, C.; Julander, A. Snapshot of cobalt, chromium and nickel exposure in dental technicians: Metal exposure in dental technicians. Contact Derm. 2016, 75, 370–376. [Google Scholar] [CrossRef] [Green Version]
- Kim, E.-C.; Kim, M.-K.; Leesungbok, R.; Lee, S.-W.; Ahn, S.-J. Co–Cr dental alloys induces cytotoxicity and inflammatory responses via activation of Nrf2/antioxidant signaling pathways in human gingival fibroblasts and osteoblasts. Dent. Mater. 2016, 32, 1394–1405. [Google Scholar] [CrossRef]


{kind=link}
| Author Year | Type Duration | Assessed Criteria | Main Results/Conclusion |
|---|---|---|---|
| Könönen et al. (1995) [31] | In vivo 5 y | n = 1 Effects of RPD with Ti on oral cavity (case report). |
|
| Seldén et al. (1995) [32] | In vivo | n = 37 Effect of Co-Cr-Mo exposure to lung disorders. | The dust from Co-Cr-Mo dental constructions can cause pneumoconiosis. Six patients exhibited radiological parameters associated with alloys. The risk can be reduced with local exhaust ventilation. |
| Seldén et al. (1996) [33] | In vivo 5 y | n = 3 Effect of Co-Cr-Mo exposure to lung disorders (a follow-up study of confirmed pneumoconiosis cases in dental technicians working with the alloys). | Pneumoconiosis is associated with inorganic dusts arising in production of Co-Cr-Mo dental constructions. However, the primary causes of 2 reported cases cannot be reduced to alloys because patients already had lung problems. |
| Katsoulis et al. (2008) [34] | In vivo 12 months | n = 10 Effects of using Ti in RPDs of the Ti6A17Nb-alloy. | After 6 months, significant biological differences were not observed. The Ti6A17Nb-alloy (Girotan L) for RPDs can be regarded as equivalent to RPDs made from Co-Cr-alloy. |
| Song et al. (2011) [35] | In vivo | n = 1 Allergic reaction to Co in cast dental crowns (case report). | 58-year-old male patient wearing crowns developed palmoplantar pustulosis in the hands and feet. Symptoms include redness, pustules, vesicles, and scaly erythema on hands and feet. It appeared 1 month after Co-Cr application on molar teeth. Symptoms disappeared with the crown removal, confirming allergic reaction to the material. |
| Imirzalioglu et al. (2012) [36] | In vitro | Effect of repeated casting of alloys on gingival fibroblast cytotoxicity. | Recasting significantly increased elemental release in Co-Cr and Ni-Cr alloys (p < 0.001), but Ni-Cr alloys were associated with higher cytotoxicity, especially after recasting Ni-Cr alloys with 65% surplus metal (significant increase). |
| Baričević et al. (2012) [37] | In vivo >5 y | n = 55 Genotoxicity of Co-Cr-Mo and Ni-Cr alloys when exposed to contact with oral cavity. | Comet assay parameters (tail length and percentage DNA in the tail) were significantly higher in the group wearing prosthodontic appliances:
|
| Łukomska-Szymańska et al. (2012) [38] | In vivo >5 y | n = 120 Effect of TiN coatings on Co-Cr alloy in framework dentures on human palatal epithelium cytology in comparison to:
| Co-Cr alloys did not have protective qualities for the oral cavity. Each prosthesis disturbed palatal epithelium keratinization, but Co-Cr alloys were associated with significantly higher perturbation of keratinization in comparison to acrylic dentures. |
| McGinley et al. (2012) [39] | In vitro 72 h | Ni-Cr alloys cytocompatibility and effect on human-derived oral mucosa. | Co-Cr had significantly better cytocompatibility than Ni-Cr alloy. Ni-Cr alloy-treated oral mucosal models were associated with (i) significant reductions in cell viability and (ii) significant increases in oxidative stress, inflammatory cytokine expression, and cellular toxicity (in comparison to untreated oral mucosal models). The higher the Ni, the higher the effects. |
| McGinley et al. (2013) [40] | In vitro 72 h | Cytocompatibility of base-metal dental casting alloys (Ni-Cr and Co-Cr) in fixed prosthodontic and orthodontic dentistry. | Ni-Cr base-metal alloy immersion solutions shown significantly lower cytocompatibility than Co-Cr alloys. In comparison to controls, Ni alloy was associated with significantly decreased cell viability, increased oxidative stress, inflammatory cytokine expression, and cellular toxicity levels. Co-Cr alloy did not increase oxidative stress or cellular toxicity when compared to controls. |
| Rusu et al. (2014) [41] | In vitro 7 days | Cytotoxicity of Ni-Cr and Co-Cr alloys. | The cytotoxicity of both alloys was similar, suggesting non-cytotoxic effect. After 7 days of inoculation, the cells grew well for both alloys and had a relatively high confluence. They observed no fragments detached with the eluates. |
| Forster et al. (2014) [42] | In vitro 72 h | Attachment and proliferation rate of cultured human epithelial cells on these materials:
| All surfaces exhibited significant cell proliferation in comparison to control plate (Li-disilicate, zirconia, Co-Cr). Li-disilicate exhibited the highest cell attachment and zirconia the lowest. It revealed that all restorative materials were equally suitable for subgingival restorations, but Li-disilicate had the best cytocompatibility. |
| Martín-Cameán et al. (2015) [43] | In vivo 15 months | n = 60 Determination of the content of metals (Al, Cu, Cr, Mn, Ni, Ti, and V) in oral mucosa cells from patients treated with conventional orthodontic appliances (brackets, arch wires, and bands) in comparison to:
| Only few traces of Co and V release were observed. The rest can be summarized in such order: Cr < Ni < Ti < Cu < Al. Significant differences in metal release compared to the control group were observed:
|
| Puskar et al. (2015) [44] | In vitro | Cytotoxicity of DMLS and cast Co-Cr-Mo dental alloy on human MRC-5 fibroblast cells. | Corresponding alloy did not have negative cytotoxic effect and could be used for application in dentistry. Cytotoxic effect was observed in neither conventionally cast nor DMLS Co-Cr-Mo alloy. There was no statistically significant difference between samples. |
| Comăneanu et al. (2015) [45] | In vitro | Cytocompatibility of Ni-Cr (N1, N2, N3) and Co-Cr (C1, C2, C3) alloys. | Cytocompatibility of the alloys examined can be summarized in the following descending order: C1 > C3 > N2 > N3 > C2 > N1. Co-Cr alloys were associated with better cell adhesion. |
| Al-Imam et al. (2016) [2] | In vivo 1–5 y | n = 66
|
|
| Gălăţeanu et al. (2016) [46] | In vitro 24 h | Electrochemical behavior of two Co-Cr dental alloys:
| Wirobond 280 exhibits best qualities:
|
| Kettelarij et al. (2016) [25] | In vivo 24 h | n = 13 Co, Cr, and Ni exposure on the skin, in the air, and urine levels for dental technicians. | Co, Cr, and Ni exposure after work (2 h) were observed on skin and through the air:
|
| Kim et al. (2016) [24] | In vitro 24 h | Effects of Co-Cr alloys on HGF and osteoblasts. | Few Co-Cr alloy cytotoxic and inflammatory effects via activation of Nrf2/ARE were examined:
|
| Yu et al. (2017) [47] | In vivo 12 months | n = 196 The peri-implant clinical parameters (PI) and the concentrations of RANKL, OPG, and calcium in PICF with four different crown materials (Co-Cr, Au-Pt, Ti, Zi). | All materials affected the concentrations of OPG, RANKL, calcium ion, and RANKL/OPG ratio. 12 months after restoration, PD and GCF volumes for all groups were significantly higher when compared to control group. Zi and Ti had the best parameters. Ti group had the highest OPG concentration; Ti and Zi groups had smallest concentrations of RANKL and calcium ion, as well as smallest RANKL/OPG ratio. |
| Ganbold et al. (2019) [48] | In vitro | hADSC behavior on a 3D printed Co-Cr alloy in comparison to other Co-Cr alloys (made by casting or milling) and Ni-Cr alloy. | Ni-Cr alloy was associated with significantly lower cell proliferation and viability. OD values for all Co-Cr groups (casting, milling, and 3D) were higher than that of the Ni-Cr group. It reveals that all Co-Cr alloys are more cytocompatible than Ni-Cr alloy. |
| Author | Study Limitations | Inconsistency | Indirectness | Imprecision | Publication Bias | Overall Quality |
|---|---|---|---|---|---|---|
| Könönen (1995) [31] | V | V | V | X | V | +++ |
| Seldén (1995) [32] | V | XX | V | V | V | ++ |
| Seldén (1996) [33] | V | XX | V | X | V | + |
| Katsoulis (2008) [34] | X | V | V | X | V | ++ |
| Song (2011) [35] | V | V | V | X | V | +++ |
| Łukomska-Szymańska (2012) [38] | V | V | X | V | V | +++ |
| Baričević (2012) [37] | V | V | X | V | V | +++ |
| Martín-Cameán (2015) [43] | V | V | X | V | V | +++ |
| Kettelarij (2016) [49] | V | XX | V | X | V | + |
| Al-Imam (2016) [2] | V | V | V | V | V | ++++ |
| Yu (2017) [47] | V | X | X | V | V | ++ |
| Author | Study Limitations | Inconsistency | Indirectness | Imprecision | Publication Bias | Overall Quality |
|---|---|---|---|---|---|---|
| McGinley (2012) [39] | V | V | V | V | V | ++++ |
| Imirzalioglu (2012) [36] | V | V | V | V | V | ++++ |
| McGinley (2013) [40] | V | V | V | V | V | ++++ |
| Rusu (2014) [41] | X | V | V | X | V | ++ |
| Forster(2014) [42] | V | V | V | X | V | +++ |
| Puskar (2015) [44] | V | V | X | X | V | ++ |
| Comăneanu (2015) [45] | X | V | V | X | V | ++ |
| Gălăţeanu (2016) [46] | V | V | X | V | V | +++ |
| Kim (2016) [24] | V | X | X | V | V | ++ |
| Ganbold(2019) [48] | V | V | V | V | V | ++++ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grosgogeat, B.; Vaicelyte, A.; Gauthier, R.; Janssen, C.; Le Borgne, M. Toxicological Risks of the Cobalt–Chromium Alloys in Dentistry: A Systematic Review. Materials 2022, 15, 5801. https://doi.org/10.3390/ma15175801
Grosgogeat B, Vaicelyte A, Gauthier R, Janssen C, Le Borgne M. Toxicological Risks of the Cobalt–Chromium Alloys in Dentistry: A Systematic Review. Materials. 2022; 15(17):5801. https://doi.org/10.3390/ma15175801
Chicago/Turabian StyleGrosgogeat, Brigitte, Alina Vaicelyte, Rémy Gauthier, Christine Janssen, and Marc Le Borgne. 2022. "Toxicological Risks of the Cobalt–Chromium Alloys in Dentistry: A Systematic Review" Materials 15, no. 17: 5801. https://doi.org/10.3390/ma15175801